


Introduction
Depression and anxiety – referred to as common mental disorders (CMDs) – are the most prevalent mental health conditions among older adults (Curran, Rosato, Ferry, & Leavey, Reference Curran, Rosato, Ferry and Leavey2020; Jalali et al., Reference Jalali, Ziapour, Karimi, Rezaei, Emami, Kalhori, Khosravi, Sameni and Kazeminia2024), with a significant impact on health (Chen, Lee, Su, Mullan, & Chiu, Reference Chen, Lee, Su, Mullan and Chiu2017). CMDs are associated with greater functional impairment and physical illness, slower recovery from medical conditions, elevated suicide risk, and more frequent and longer hospitalizations (Berk et al., Reference Berk, Köhler-Forsberg, Turner, Penninx, Wrobel, Firth, Loughman, Reavley, McGrath, Momen, Plana-Ripoll, O’Neil, Siskind, Williams, Carvalho, Schmaal, Walker, Dean, Walder and Marx2023; Webb & Chen, Reference Webb and Chen2022).
First-line treatments for CMDs include pharmacotherapy and psychotherapy, with cognitive behavioral therapy (CBT) being the most common. Problem-solving strategies are also particularly effective with older adults (Simon, Moise, & Mohr, Reference Simon, Moise and Mohr2024). Adding mindfulness-based approaches has also shown significant benefits for older adults with comorbid anxiety and depression (Wang et al., Reference Wang, Wang, Liu, Tang, Huang and Huang2024; Wuthrich et al., Reference Wuthrich, Dickson, Pehlivan, Chen, Zagic, Ghai, Neelakandan and Johnco2024). Strikingly, the prevalence of CMDs has not significantly decreased over the years, despite the increased availability of treatment options (Jorm, Patten, Brugha, & Mojtabai, Reference Jorm, Patten, Brugha and Mojtabai2017).
For this reason, preventive interventions may offer a valuable approach for protecting against CMDs, especially in older adults (Cuijpers, Van Straten, & Smit, Reference Cuijpers, Van Straten and Smit2005; Singh, Kumar, & Gupta, Reference Singh, Kumar and Gupta2022). Evidence supports the efficacy of such interventions in treating preclinical levels of CMDs in older adults (de Oliveira, Dornelles, Gosmann, & Camozzato, Reference de Oliveira, Dornelles, Gosmann and Camozzato2023; Dworschak, Heim, & Maercker, Reference Dworschak, Heim and Maercker2022; Scazufca et al., Reference Scazufca, Nakamura, Seward, Didone, Moretti, Oliveira da Costa, Queiroz de Souza, Macias de Oliveira, Souza dos Santos, Pereira, Mendes de Sá Martins, van de Ven, Hollingworth, Peters and Araya2024). However, the exact intervention effectiveness has not been determined. Previous meta-analyses have assessed the efficacy of psychosocial interventions (Forsman, Schierenbeck, & Wahlbeck, Reference Forsman, Schierenbeck and Wahlbeck2011), CBT (Vedel, Larsen, & Aamand, Reference Vedel, Larsen and Aamand2020; Wang et al., Reference Wang, Wang, Liu, Tang, Huang and Huang2024; Wuthrich et al., Reference Wuthrich, Meuldijk, Jagiello, Robles, Jones and Cuijpers2021; Wuthrich et al., Reference Wuthrich, Dickson, Pehlivan, Chen, Zagic, Ghai, Neelakandan and Johnco2024), educational programs (Conejo-Cerón et al., Reference Conejo-Cerón, Moreno-Peral, Rodríguez-Morejón, Motrico, Navas-Campaña, Rigabert, Martín-Pérez, Rodríguez-Bayón, Ballesta-Rodríguez, Luna, García-Campayo, Roca and Bellón2017), mind–body interventions such as yoga (Dong et al., Reference Dong, Zhang, Zhao, Cao, Kuang and Yao2024), and physical activity interventions (Ahmad, Syam, & Saleh, Reference Ahmad, Syam and Saleh2023; Podolski et al., Reference Podolski, Whitfield, Schaaf, Cornaro, Köbe, Koch and Wirth2023) in reducing CMD symptoms in older adults. However, such endeavors present several limitations, namely, they (1) focus on specific interventions, (2) often mix community-dwelling samples with those diagnosed with clinical depression/anxiety; (3) do not account for potential interactions between moderating variables, and (4) mix RCT findings with noncontrolled trials.
Thus, this meta-analysis aims to define the effects of preventive psychosocial interventions for older adults with nonclinical levels of CMD symptoms. Secondary objectives include identifying factors that may influence the effectiveness of these interventions, such as intervention type (e.g., mind–body, psychology-based, multi-component), length, delivery modality (group versus individual), and comparison group type (e.g., treatment as usual (TAU), waiting list/no treatment, active comparator, nonspecific factor component control).
Methods
This meta-analysis was registered at PROSPERO (CRD463398) and prepared according to the PRISMA guidelines (Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson, McDonald and Moher2021; see Supplementary File 1).
Literature search
A systematic search was performed in PubMed/MEDLINE, PsycINFO, Web of Science, Scopus, and The Cochrane Library. The search ran until December 2024, comprising search terms related to the population (elderly), intervention type (preventive interventions against anxiety/depression), and study design (RCT) and was based on abstract, title, and keywords. Hits were restricted in publications in English and Spanish. The search string and strategies can be seen in Supplementary File 2.
Inclusion and exclusion criteria
To be eligible, primary studies needed to (i) follow an RCT design, (ii) study older adults (mean age > 60 years old), (iii) include a valid instrument measuring depression and/or anxiety, (iv) focus on people attending any outpatient mental health or community setting; (v) test the effectiveness of a psychosocial intervention (that is, mind–body-based; psychology-based; multicomponent; other) delivered with human component (that is clinician, trainer), (vi) target, or measure as an outcome, depression and/or anxiety through any standardized instrument, (vii) include a control group of users receiving TAU, being on the waiting list/no treatment, receiving a specific/active control, or a nonspecific control; and (viii) report sufficient statistical parameters to allow effect size calculation or provide the data upon request. The following were excluded: (i) non-RCTs, publications on the same data, and insufficient reporting; (ii) non-English/Spanish publications; (iii) studies applying pharmacological, treatment, or recovery programs; (iv) studies applying interventions not including a human provider (that is, apps, self-help); and (v) samples with diagnosed mental disorders (including major depression/anxiety), substance abuse, or dementia.
Screening and data extraction
Three researchers (JA, AC, and EP) performed the database searches; two of them (JA and AC) removed duplicates. Two of them (JA and AC) screened the search output independently based on titles/abstracts and accessed and screened the potentially eligible full-texts. Discrepancies were discussed with two reviewers (SS and EP). Extracted data are available at https://osf.io/e7vxz/. In all, 21 corresponding authors were contacted, and 14 provided missing information for eligible studies (66%).
The following data were coded: title, author, publication date, location, language; study design: intervention duration, follow-up periods; participant demographics: age, sex; sample size for intervention and control group; intervention characteristics: type (mind–body based, psychology-based, multicomponent, other), duration (in weeks), modality (group/individual); control group intervention/condition (TAU, waiting list/no treatment, active comparator/specific factor component, non-specific factor component); outcomes: depressive/anxiety symptoms; statistical parameters: means, standard deviations for intervention and control groups.
Interventions were grouped into four categories based on their content as described in the primary studies:
-
(1) Mind–body-based: including physical exercise activities (i.e., Tai-Chi, aerobic and resistance training, Xbox Kinect exercise training, home-based exergame program, walking, yoga).
-
(2) Psychology-based: based on a theory-driven psychological approach (i.e., CBT, behavioral activation, cognitive training, mindfulness, life story review, psychoeducation).
-
(3) Multicomponent: combining components of several approaches (i.e., social activities with psychoeducation; psychoeducation with mindfulness; exercises and diet; exercises and social activities; physical, cognitive, and social activities).
-
(4) Other: interventions not fitting suitably in the previous categories (i.e., pet support, attending sports activities, photograph appreciation).
Control group conditions were grouped into four groups based on the Gold et al. (Reference Gold, Enck, Hasselmann, Friede, Hegerl, Mohr and Otte2017) approach adjusted to the eligible studies content:
-
(1) TAU: care as usual.
-
(6) Waitlist control/no treatment: no treatment during the intervention period – could be offered after the trial.
-
(7) Active control: evidence-based treatment different from the experimental condition; may include structured activities or techniques that are considered therapeutic.
-
(8) Nonspecific factor component control: structured programs with the same duration and frequency as the experimental condition but not including activities or techniques considered therapeutic.
Outcome and quality assessment
The primary outcome was the depression and/or anxiety symptom change. Symptoms were measured through standardized instruments (e.g., Geriatric Depression Scale-GDS/Patient Health Questionnaire-PHQ for depression; Geriatric Anxiety Inventory-GAI/Hospital Anxiety Depression Scale-HADSHADS for anxiety). Two reviewers (JA and AC) assessed the study quality using the Effective Public Health Practice Project Quality Assessment Tool (EPHPP; Thomas, Ciliska, Dobbins, and Micucci (Reference Thomas, Ciliska, Dobbins and Micucci2004)). Studies were rated based on study design, blinding, confounders, instruments, psychometric characteristics, and withdrawals/dropouts. The GRADE system was applied to assess certainty of evidence for depressive and anxiety symptoms, based on study design, risk of bias, inconsistency, imprecision, and publication bias (Atkins et al., Reference Atkins, Eccles, Flottorp, Guyatt, Henry, Hill, Liberati, O’Connell, Oxman, Phillips, Schünemann, Edejer, Vist, Williams and The2004).
Statistical analyses
We calculated the summary effects of standardized mean differences (Cohens d) using the means of random effect calculations following current recommendations (Borenstein, Hedges, Higgins, & Rothstein, Reference Borenstein, Hedges, Higgins and Rothstein2021). Heterogeneity was assessed by calculating I-squared values, which we interpreted in terms of well-established thresholds, with values from 0 to 25% indicating no, 25 to 50% indicating little, 50 to 75% indicating moderate and 75 to 100% indicating strong between-studies heterogeneity (Higgins, Thompson, Deeks, & Altman, Reference Higgins, Thompson, Deeks and Altman2003).
We used single precision-weighted regression models to assess the effects of intervention type (a subgroup summary effect was calculated for each distinct intervention, i.e., mind–body-based, psychology-based, multicomponent program, other), modality (group versus Individual versus mixed), control group interventions (TAU, being in waiting list or no intervention, specific or nonspecific intervention), cognitive function change, age, sex, outcome being primary or secondary, publication year, and study quality. For categorical variables, categories were dummy-coded to allow comparisons. Effect sizes were interpreted based on Cohen’s (Reference Cohen2013) well-established thresholds (i.e., ds = 0.2, 0.5, and 0.8 represent the lower thresholds of small, moderate, and large effects, respectively). Analyses were performed in the open-source software environment R 4.2.0 (R Core Team, 2022) by means of the package metafor (Viechtbauer, Reference Viechtbauer2010).
Dissemination bias
We visually inspected funnel plots for asymmetry indications, and we used four formal publication bias-detection methods. First, we used trim and fill analyses that allow a formal assessment of funnel plot asymmetry by iteratively trimming excess studies on one side of an asymmetric funnel and re-estimating the summary effect until funnel plot symmetry is observed. Subsequently, trimmed studies are re-entered into the funnel and studies with equivalent weights and effect sizes are added on the opposite side of the funnel. This method can be interpreted in terms of a sensitivity analysis (Duval & Tweedie, Reference Duval and Tweedie2000). Second, we used the Begg and Mazumdar (Reference Begg and Mazumdar1994) rank correlation method that assesses correlations between effect sizes and their sampling variances, where significant associations are indicative of confounding bias. Third, we calculated Sterne and Egger’s regression method (Sterne & Egger, Reference Sterne, Egger, Rothstein, Sutton and Borenstein2005) in which effect sizes are regressed on their precision estimates, with significant results indicating bias. Finally, we assessed evidence for possible excess significance of the number of observed primary study effects (Ioannidis & Trikalinos, Reference Ioannidis and Trikalinos2007). We interpreted all results according to current standards as outlined by Siegel, Eder, Wicherts, and Pietschnig (Reference Siegel, Eder, Wicherts and Pietschnig2022).
Multiverse analyses
Different (reasonable) choices of researchers in approaching the design of the studies and the data analysis (i.e., the so-called researcher degrees of freedom) have been shown to have, in many cases, considerable impact on the outcome of the study (Simonsohn, Simmons, & Nelson, Reference Simonsohn, Simmons and Nelson2020) In the meta-analytical context, these choices pertain typically to the questions about which data to analyze (the so-called ‘which factors’) and which analytical methods to use (the so-called ‘how factors’; (Voracek, Kossmeier, & Tran, Reference Voracek, Kossmeier and Tran2019). Some effects may only be observable under very specific circumstances or, in the worst case, may even represent a spurious finding that is only observable due to chance in a certain dataset after specific choices have been made, whereas other effects show a large generality by manifesting themselves regardless of the choices that have been made. Specification curve analysis and combinatorial meta-analyses are useful to show the meaningfulness, generality, and specificity of effects under scrutiny.
Specification curve
In specification curve analyses, one aims to assess all possible summary effects that can be calculated based on reasonable analytical choices that can be made in subsetting (‘which factors’) and analyzing (‘how factors’) the available data. We presently account for five which factors, namely control group type (nonspecific versus specific versus TAU, versus waitlist versus either control type), intervention type (multicomponent versus psychology-based versus mind–body-based versus other versus either intervention), quality assessment (weak versus moderate versus strong versus any), primary outcome (no versus yes versus either), treatment setting (group versus individual versus mixed versus any) and one how factor, namely, the calculation method (REML: random effects maximum likelihood versus RE-DL: random effects DerSimonian-Laird versus FE: fixed effect). This resulted in 5*5*3*4*4*3 = 3,600 reasonable ways (i.e., specifications) to calculate a summary effect in our present meta-analysis. However, we considered only those specifications that included at least two primary studies for summary effect calculations, thus reducing the number of outcomes accordingly.
Combinatorial meta-analysis
It can be highlighted that the specification curve falls short of assessing the generality and salience of a given effect, because not all factors that can influence the manifestation of a summary effect may necessarily be known. To account for this possibility, the combinatorial meta-analytical approach has been introduced (Olkin, Dahabreh, & Trikalinos, Reference Olkin, Dahabreh and Trikalinos2012. By means of this method, not only the reasonable but all 2 k-1 possible combinations of the available studies are considered to yield potentially meaningful representations of the scrutinized effect. In our analyses, this approach yields 259 = 576,460,752,303,423,488 and 223 = 8,388,608 combinations for pre-to-post as well as pre-to-follow-up comparisons, respectively, in depression and 229 = 536,870,912 and 218 = 262,144 combinations, respectively, in anxiety. As these numbers of effect estimations exceed the computational power of most standard equipment, we drew a random sample of 100,000 combinations within each of these calculations. This approach allowed us to inspect the potential systematic patterns in terms of the relation of summary effect sizes with their associated between-studies heterogeneity by means of GOSH plots (Graphic Display of Heterogeneity; (Olkin et al., Reference Olkin, Dahabreh and Trikalinos2012).
Results
Final sample
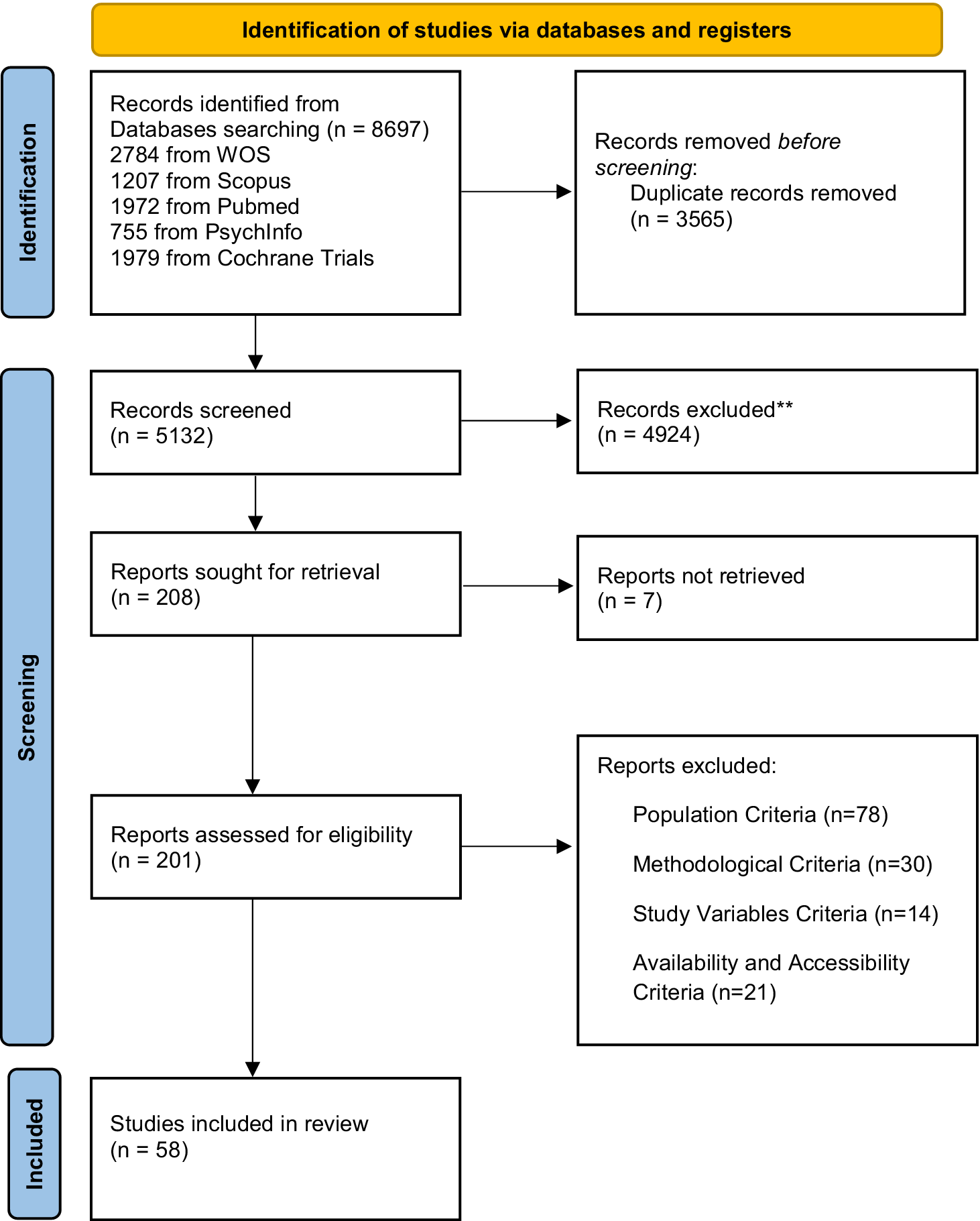
The inclusion criteria were met by 58 independent studies (56 on depression and 26 on anxiety, i.e., almost half of the studies including both outcomes), reporting k = 60 effect sizes for depression and k = 30 effect sizes for anxiety comparing pre-to-post intervention levels. Also, k = 24 effect sizes were reported for depression and k = 19 effect sizes for anxiety comparing pre-intervention to follow-up (Check Figure 1 for the PRISMA flowchart for study inclusion; References are displayed in Supplementary File 14.).
PRISMA Flowchart
Source: Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson, McDonald and Moher2021. This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.

For studies focusing on depression, there were 5,517 participants, whereas for anxiety there were 2,999 participants. Of those, there were 2,449 participants with available data on follow-ups for depression and 2,080 for anxiety.
The mean participant age for studies focusing on depression was M = 72.07 (SD = 4.27) and for anxiety, it was M = 71.40 (SD = 4.07). For studies focusing on depression, 70.14% were female, whereas for anxiety, the percentage was 68.02%.
There were 27 studies from the United States, Canada, Australia, and Europe, 23 studies from South Asia, and 4 studies from South America and the Middle East.
Interventions and controls description
Out of the 56 studies comparing the effects of an intervention on depression levels, 34 studies use psychology-based interventions, 12 use mind–body-based interventions, five use multicomponent therapy, and five use other therapies.
In terms of comparisons, 21 studies compared the interventions’ effectiveness with TAU, 16 studies with waitlist, 12 studies with specific comparators, and 7 studies with nonspecific controls. Studies reporting follow-ups would most commonly follow up patients for 52 weeks, with the longest follow-up being 192 weeks.
When it comes to anxiety, out of 26 studies, 19 applied psychology-based interventions, t3 applied mind–body-based interventions, 3 multicomponent interventions, and 1 applied other intervention. There were 12 studies comparing the control groups with TAU, 5 with waitlist, 6 with specific comparator, and 2 with the nonspecific comparator. The longest follow-up time was 192 weeks. (See Table 1 for study characteristics.)
Characteristics of included studies

Depression and anxiety instruments
Most studies measured changes in depressive symptoms assessed by the GDS (=35), with seven using PHQ-9, six using CES-D, five using HADS, three using BDI, and one using DASS (the depression subscale), MADRS, and HSCL-90, respectively.
Similarly, for anxiety changes, 14 studies used GAD-7, three studies used STAI (only the state subscale was extracted), four used DASS, five used HADS, one used the SCL-90 (the anxiety subscale), and three studies used BAI (See Table 1).
Intervention effectiveness on depressive symptom reduction
Interventions targeting depressive symptoms showed a significant moderate effect compared to controls (k = 60; d = −0.530; p < .001) pre-to-post. When removing two outliers, the effect remained significant although it was somewhat lower (k = 58; d = −0.474; p < .001).
There was also a significant small-to-moderate effect comparing symptom levels pre-to-follow-up (k = 24; d = −0.386; p = .002; Supplementary file 3). Given the large heterogeneity (I 2 = 84.51 for pre-to-post and I 2 = 87.24 for pre-to-follow-up), several factors were examined as potential moderators of these findings. Specifically, for pre-to-post and pre-to-follow-up depressive levels, the findings revealed an effect of mean age, with younger participants showing higher reductions of depressive symptoms when receiving an intervention (b = 0.055; p < .001, b = 0.075; p < .007). Targeting depression as the primary outcome also seems to moderate both pre-to-post and pre-to-follow-up comparisons (b = −0.313; p < .042, b = −0.490; p < .036). On the other hand, when comparing intervention types (psychology-based, mind–body-based, multicomponent, other), no significant differences emerged. Likewise, there was no difference when comparing types of control (specific, TAU, waitlist, other nonspecific; Table 2) across both pre-to-post and pre-to-follow-up comparisons.
Single precision-weighted regression models

a Referenced to nonspecific controls.
b Referenced to multicomponent therapy.
c 0 = No, 1 = Yes.
d Referenced to weak quality.
e Referenced to group treatment.
f sensitivity analyses show that this effect is driven by a leverage point – removal of one outlier, yielding a 7.5 more extreme value compared to its adjacent value leads to nonsignificance of this effect (k = 12; b = 0.135; SE = 0.156: p = .386).
A potential effect of cognitive function change was reported for pre-to-post comparisons but lost significance when two outliers were removed. There was no significant effect of any other potential moderator for the depressive symptoms change from pre-to-post or from pre-to-intervention to follow-up.
Intervention effectiveness on anxiety symptom reduction
For anxiety levels, the findings showed a small-to-moderate effect of interventions regarding pre-to-post changes compared to controls (k = 30; d = −0.333; p < .001) and a small, albeit nominally nonsignificant effect for pre-to-follow-up changes (k = 19; d = −0.205; p = .052). When examining potential moderators due to heterogeneity (I 2 = 81.92 for pre-to-post and I 2 = 79.38 for pre-to- follow-up), similarly to depression, younger participants showed higher symptom reduction for pre-to-post (b = 0.038; p = 0.020). No significant effects were observed for type of intervention, type of controls, or any other of the examined variables, both for pre-to-post and pre-to-follow-up changes in anxiety symptoms (Table 2).
Dissemination bias
Begg and Mazumdar’s rank correlation method indicated some evidence for funnel plot asymmetry in both anxiety calculations and in pre-to-post comparisons for depression. Moreover, trim-and-fill suggested asymmetry in the anxiety follow-up and Sterne and Egger’s regression in both depression calculations (see Supplementary file 5). All other methods were inconspicuous for the four meta-analytical subsets. In all, these results indicate that the calculated summary effects may be somewhat affected by effect inflation, but the possible confounding effects appear not to be substantial.
Study quality
Based on the EPHPP ratings, there were 11 studies with strong quality, 24 with moderate, and 23 with weak quality (Supplementary file 4). Dummy-coded precision-weighted single meta-regressions with low-quality studies as reference compared to moderate- and strong-quality studies did not show any systematic influences of study quality on the effect sizes for depression or anxiety. However, specification curves showed somewhat stronger summary effects for qualitatively weak studies in anxiety. Based on the GRADE system, certainty of evidence for both depressive and anxiety symptoms was moderate for psychology-based, mind–body-based, and other interventions, whereas it was low for multicomponent interventions. Certainty of evidence was downgraded mostly due to high unexplained heterogeneity. Further details can be found in Supplementary File 4.
Multiverse analyses findings
Specification curve
Out of 651 reasonable specifications for depression, 444 (68%) yielded significant negative summary effects, thus indicating treatment effectiveness. Merely 29 summary effects were positive, none of which reached nominal statistical significance. Treatment effects averaged d = −0.529 (Md = −0.475) with 50% of the most typical summary effect estimates (i.e., interquartile range) ranging from −0.701 to −0.264, thus suggesting a remarkable generality of the observed treatment effect. Effect sizes of more accurate estimates (i.e., with larger precision and smaller confidence intervals) appear to indicate numerically larger effects of mind–body-based interventions as well as waitlist controls (Figure 2). Removing two outliers from these analyses yielded somewhat numerically lower summary effect averages, yielding d = −0.463 (Md = −0.455, interquartile range = −0.634 to −0.242), but the effect generality and robustness of the observed meaningful treatment effect remained unaffected (Supplementary file 6). Depression follow-up results were similar in terms of interpretation to the pre-to-post comparisons, although effect sizes were numerically weaker. Out of 210 reasonable specifications, 80 (38%) yielded significant negative summary effects, while only 14 specifications led to positive effects, none of which were significant. Effects averaged at d = −0.356 (Md = −0.310) with an interquartile range from −0.476 to −0.119 (Supplementary file 7).
Effect sizes for depressive symptoms specification curve.

For anxiety, out of 309 reasonable specifications, 190 (61%) yielded significant negative summary effects with only 22 specifications leading to positive effects, all of which failed to reach significance. Summary effects averaged at d = −0.391 (Md = −0.354) with an interquartile range from −0.525 to −0.210. There was some indication that primary studies that had been rated to have weaker quality tended to show somewhat stronger effects, thus tentatively conforming to the results from our publication bias analyses. However, despite this observation, summary effect calculations showed in this case once more a remarkable generality of the treatment effect (Figure 3). Anxiety follow-up calculations supported results from pre-to-post comparisons, although, as expected, the effects were once again weaker. Out of 123 reasonable specifications, 78 (63%) yielded significant negative effects with 10 specifications leading to positive albeit nonsignificant summary effects. Summary effects averaged d = −0.265 (Md = −0.272) and the interquartile range showed values from −0.343 to −0.198 (Supplementary file 8).
Effect sizes for anxiety specification curve.

Combinatorial meta-analysis
Results from combinatorial meta-analyses were broadly in line with findings from our specification curve calculations, supporting the generality of our observed treatment effects. Depression analyses indicated an average effect size of d = −0.532 (Md = −0.532) and an interquartile range from −0.587 to −0.477 (Supplementary file 9). Removal of two outliers led to numerical changes with d = −0.475 (Md = −0.475; interquartile range = −0.523 to −0.426; Supplementary file 10). Depression follow-up calculations showed again numerically smaller but nonetheless meaningful effects (d = −0.421; Md = −0.420; interquartile range = −0.511 to −0.328; Supplementary file 11).
Anxiety analyses indicated effect averages of d = −0.359 (Md = −0.261) and an interquartile range from −0.423 to −0.292 (Supplementary file 12). Follow-up analyses showed an average of d = −0.386 (Md = −0.390; interquartile range = −0.480 to −0.279; Supplementary file 13). GOSH-plots did not indicate systematic patterns for depression or anxiety.
Discussion
This study provides the most comprehensive synthesis to date of randomized controlled trials (RCTs) evaluating preventive psychosocial interventions that aim to reduce subclinical depressive and anxiety symptoms in older adults. The meta-analysis includes primary studies that examine different intervention and control types and assesses both depression and anxiety outcomes to estimate prevention effectiveness against the most prevalent CMDs. A broad number of studies from different geographical regions is included, thus encompassing numerous samples experiencing their senior years in a variety of sociocultural contexts. Publication bias and multiverse analyses allowed for assessment of potential effect inflation and effect generality across potentially moderating variables and their interactions, allowing for robust conclusions.
Specifically, the findings indicate that such interventions are effective for reducing the participants’ depressive symptoms immediately after the intervention and at follow-up, thus demonstrating that the prevention effect is sustained in the long term. Findings are similar for anxiety; however, the prevention effects seem to be less sustainable at follow-up. Importantly, the observed effectiveness is independent of intervention or control condition types, suggesting that any preventive intervention is indeed effective for protecting older adults against CMDs. Only age seems to moderate these findings, with younger participants benefiting more substantially from preventive interventions. Moreover, mind–body-based interventions appeared to be somewhat superior and more effective when comparing interventions with waitlist controls. These results are robust and largely unaffected from publication bias and study quality, although the high unexplained heterogeneity observed somewhat limits the certainty of recommendations across the various intervention types.
This is the first meta-analysis to examine the generality of the intervention effect and the only one that accounts for different moderator effects and their interactions so far. Our findings are broadly in line with results of the only prior meta-analysis on preventive interventions against depression for older adults that encompassed all types of psychosocial interventions to date (Forsman et al., Reference Forsman, Schierenbeck and Wahlbeck2011). We update, expand, and refine these findings further; specifically, we included only trials that were randomized; we doubled the number of included studies with a wider sample; we included anxiety as an outcome to better encompass the CMDs in older adults; and we performed advanced meta-analytic procedures to refine the effectiveness effect size and to account for several moderators. This may also explain why our findings contrast with their results regarding social activity-based intervention effects, as we did not obtain superior results to other interventions. In fact, intervention effects showed remarkable generality across intervention types, with evidence suggesting somewhat more beneficial effects of mind–body-based interventions. This is consistent with recent studies that have supported the relevance of physical exercise to reducing depressive symptoms (Kim, Hong, & Choi, Reference Kim, Hong and Choi2022) and to improving health and well-being outcomes for older adults (Kappen, Pejman, & Nacke, Reference Kappen, Pejman and Nacke2019). However, determining which specific elements of mind–body-based interventions are responsible for these superior effects is challenging, because such interventions include a large variety of physical activities that differ in terms of intensity, modality (that is group-individual), frequency, or purpose. Furthermore, it seems that the effect sizes of more accurate estimates (that is smaller CIs) derive from studies that compare the intervention groups with waitlist controls, in line with previous findings indicating that waitlist controls groups are less effective than other types of control conditions, such as TAU (Plessen, Karyotaki, Miguel, Ciharova, & Cuijpers, Reference Plessen, Karyotaki, Miguel, Ciharova and Cuijpers2023).
Compared to depression, evidence for preventive interventions against anxiety is more limited and inconsistent, although there has been growth of the relevant literature in the last decade. Our results align with those of a recent meta-analysis examining the effect of remote CBT on self-reported anxiety (Ando et al., Reference Ando, Kao, Lee, Tai, Mendez, Sasaki, Tang and Papatheodorou2024) and contrast those of Dworschak et al. (Reference Dworschak, Heim and Maercker2022), where internet-based interventions did not seem to reduce anxiety symptoms. However, both meta-analyses were based on a limited number of primary studies ranging from two to six. Thus, the present meta-analysis based on 25 studies (that is, an amount four to twelve times larger) is the first to offer a more precise estimation of the effect on anxiety, encompassing a variety of intervention types and modalities.
Notably, age was the only factor moderating the intervention effectiveness on depressive and anxiety symptoms, as younger participants seem to benefit more from such interventions. A potential explanation for this finding may be related to how the decline in memory and learning capacity that come with age hinders the skills acquisition aimed at through the interventions. However, the exact impact of such decline on intervention outcomes is currently unknown (Wuthrich et al., Reference Wuthrich, Dickson, Pehlivan, Chen, Zagic, Ghai, Neelakandan and Johnco2024). Also, our analyses indicated no meaningful impact of mild cognitive decline on the interventions’ effectiveness, suggesting that other aging-related effects may be responsible for decreasing intervention effectiveness.
Despite the strengths of our study, the findings should be interpreted having in mind the following limitations. First, despite considering a comprehensive number of databases, we only included studies reported in English and Spanish, potentially introducing a language bias. However, the presently used publication bias detection methods should have picked up on publication language-based biases and indicate that such influences are modest at best. Second, given the focus on prevention studies, there is a possibility of a floor effect due to low symptom levels; this may suggest that in fact the intervention effectiveness may be even larger than detected. Third, there were only few studies including results based on intention to treat samples; thus, a completer-only bias may have influenced the findings. Fourth, the observed age moderation effect may be due to sample composition rather than genuine age differences in responsiveness to interventions, as there may have been an overrepresentation of younger participants, a common phenomenon observed in intervention studies focusing on the elderly. Fifth, it was not possible to define the effect size of specific intervention types (that is, CBT, yoga, mindfulness, etc.) due to the limited number of studies focusing on specific interventions and the heterogeneity among them in terms of procedures and format.
Given the overall moderate confidence on the observed effects of the included intervention types, continued investment in high-quality, large-scale RCTs is essential to guide policy and implementation. Future research should focus on the detection of the specific mechanisms that underlie psychosocial interventions, to determine how to optimize their impact, as this is a common gap in the literature addressing interventions destined to older adults (Iwano, Kambara, & Aoki, Reference Iwano, Kambara and Aoki2022; Qiu et al., Reference Qiu, Wu, Liu, Li, Yu, Zeng, Yang, Zhang and Chen2025). This may be particularly relevant in the context of digital and low-support interventions that seem to emerge as a potential future modus operandi (Wuthrich et al., Reference Wuthrich, Dickson, Pehlivan, Chen, Zagic, Ghai, Neelakandan and Johnco2024) in service provision. Importantly, given the exclusion of studies focusing on populations with physical illnesses, the high prevalence of mental symptoms in such populations (Berk et al., Reference Berk, Köhler-Forsberg, Turner, Penninx, Wrobel, Firth, Loughman, Reavley, McGrath, Momen, Plana-Ripoll, O’Neil, Siskind, Williams, Carvalho, Schmaal, Walker, Dean, Walder and Marx2023), and the comorbidity of such conditions in the elderly (Devita et al., Reference Devita, De Salvo, Ravelli, De Rui, Coin, Sergi and Mapelli2022), future endeavors should address this gap to guide the implementation of preventive strategies for older people with physical conditions and CMD symptoms.
According to our findings, preventive psychosocial interventions seem to be particularly beneficial for older individuals applied in a variety of delivery formats and settings, independent of its content or other characteristics. Given that the interventions seem to be more effective with younger participants, there is a need for primary care and mental health care professionals to reinforce early screening for depressive and anxiety symptomatology, to prevent further worsening of these conditions.
In conclusion, the present results clearly indicate the importance of early, nonpharmacological approaches in mental health prevention for aging populations. Low-cost and low-complexity preventive interventions would be a strong candidate for providing a cost-effective solution for common mental illness symptoms. Importantly, such interventions could be included in the main agenda of primary health care services and become part of routine care provision for older adults, if the aim is to protect them against the impact of mental disorders and to promote positive aging.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0033291726104607.
Data availability statement
Data and all other relevant materials are publicly available either at the website of Open Science Framework (www.osf.io) or upon request to the corresponding author.
Author contribution
The authors confirm contribution to the paper as follows: study design: all authors, data collection: SS, PE, AJ, CA; analysis of results: PE, PJ; interpretation of results: all authors; construction of final recommendation: all authors; draft of manuscript: SS, with input from PE, AJ, CA, PJ. All authors reviewed and approved the final version of the manuscript. PE, SS, AJ, CA, and PJ accessed and verified the underlying data.
Funding statement
This study was funded by the Chilean National Agency for Research and Development, ANID, with a FONDECYT Project grant 1241925.Funding for open access charge: Universidad de Málaga / CBUA.
Competing interests
All authors declare no competing interests.
Ethical standard
Ethical approval was not required as this is a systematic review.
Role of funding source
The funder of the study had no involvement in the study’s design, data collection, data analysis, data interpretation, or the writing of the report.







 Open access
Open access