


Case presentation
A 28-year-old woman underwent prenatal ultrasonography at 20 weeks of gestation, revealing a suspected aortic arch anomaly. Serial fetal evaluations confirmed an isolated arch abnormality. At 38 weeks of gestation, a male infant was delivered by caesarean section (birth weight 3380 g, Apgar scores 8/9) and admitted for cardiac evaluation.
Echocardiographic findings
Day 1 of life
Transthoracic echocardiography demonstrated an abnormal aortic arch configuration. A single large vessel arose from the descending aorta (later confirmed as a Kommerell diverticulum by CT), extending superiorly with retrograde flow and bifurcating into rightward and leftward branches; the leftward branch connected to a markedly dilated structure measuring 8–9 mm at its mid-portion, with continuous left-to-right shunt flow into the left pulmonary artery, confirming a patent ductus arteriosus. The patent ductus arteriosus demonstrated unusual fusiform aneurysmal dilatation at its mid-portion, while the aortic and pulmonary ends appeared normal in calibre (pulmonary end 3.5 mm). A small atrial septal defect (2–3 mm) was also identified.
Day 2 of life
Repeat echocardiography showed progressive patent ductus arteriosus closure. The pulmonary end narrowed to 2 mm, while the aneurysmal mid-portion remained dilated at 8 mm with persistent shunt flow.
Day 4 of life
Follow-up echocardiography demonstrated complete functional patent ductus arteriosus closure with no detectable flow. The aneurysmal mid-portion contained heterogeneous echogenic material consistent with intraluminal thrombosis (Figure 1).
Serial echocardiographic findings demonstrating spontaneous closure of aneurysmal patent ductus arteriosus ( a ) Day 1 of life: High parasternal short axis view demonstrates markedly dilated mid-portion of the patent ductus arteriosus (asterisk) measuring 8–9 mm, appearing as a hypoechoic structure adjacent to the left pulmonary artery. The patent lumen indicates ongoing ductal flow. ( b ) Day 4 of life: Follow-up imaging at the same level demonstrates complete functional closure of the ductus arteriosus. The previously patent lumen is now filled with heterogeneous echogenic material (arrowhead) consistent with intraluminal thrombosis. AV = aortic valve; LPA = left pulmonary artery.

CT angiography
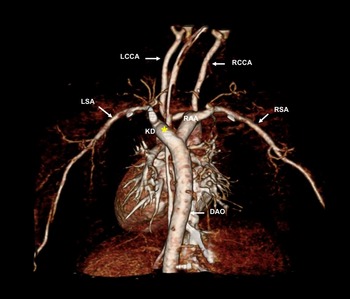
Multi-detector CT on day 4 confirmed a right-sided aortic arch with sequential branching of the left common carotid artery, right common carotid artery, and right subclavian artery. Approximately 10 mm distal to the right subclavian artery origin, a prominent diverticulum arose from the descending aorta, extending superiorly 5–6 mm in a retroesophageal course before giving rise to the left subclavian artery, consistent with a Kommerell diverticulum (Figure 2). The patent ductus arteriosus was no longer visible, confirming anatomical closure.
Three-dimensional reconstruction CT angiography demonstrating right aortic arch with Kommerell diverticulum. Posterior view demonstrates right aortic arch (RAA) with Kommerell diverticulum (KD, asterisk) arising from the descending aorta (DAO). The left subclavian artery (LSA) originates from the diverticulum. Sequential branching of the left common carotid artery (LCCA), right common carotid artery (RCCA), and right subclavian artery (RSA) from the aortic arch is shown.

Clinical course
Screening studies (abdominal/cranial ultrasonography, chromosomal microarray) revealed no abnormalities. The infant remained asymptomatic throughout hospitalisation without respiratory distress, stridor, or feeding difficulties. Close surveillance with serial imaging was initiated, with surgical intervention planned if risk signs develop. The infant was discharged on day 11 with cardiology follow-up. At 1-month follow-up, the infant thrived with normal growth and development.
Discussion
Kommerell diverticulum is an uncommon congenital vascular anomaly representing a persistent remnant of the embryonic fourth aortic arch.Reference Worhunsky, Levy, Stephens and Backer1 In patients with a right aortic arch and an aberrant left subclavian artery, the diverticulum arises from the descending aorta and gives rise to the left subclavian artery in a retroesophageal course. Combined with a left-sided ligamentum arteriosum, this anatomy creates a complete vascular ring that can compress the trachea and oesophagus.Reference Bae, Kang and Choo2
Early recognition of Kommerell diverticulum, particularly through prenatal diagnosis, has important clinical implications for perinatal management and postnatal surveillance. Prenatal echocardiography can identify aortic arch sidedness and raise suspicion of associated arch anomalies during routine screening.Reference Suzuki, Sasaki and Kunugi3 Although the complete vascular anatomy, including the presence of a Kommerell diverticulum, is best delineated by postnatal CT or cardiac MRI, prenatal suspicion allows for planned delivery at tertiary centres with paediatric cardiac surgery expertise and enables timely evaluation and longitudinal follow-up.
This case demonstrates an exceptionally early diagnosis combined with unique morphologic features. While a right aortic arch with an aberrant left subclavian artery occurs in 0.04 to 0.4% of the population,Reference Cinà, Althani, Pasenau and Abouzahr4 diagnosis on the first day of life is exceptional. Among 212 reported cases, the youngest patient was 18 days old, with mean age at diagnosis of 41.8 years.Reference Tanaka, Milner and Ota5 Our day 1 diagnosis represents one of the youngest documented cases and is further distinguished by selective mid-ductal aneurysmal dilatation of the patent ductus arteriosus. Serial imaging documented ductal evolution from patency to thrombosis over four days, providing insight into the natural history of this rare variant.
The most distinctive feature was the unusual fusiform mid-ductal aneurysmal dilatation. We propose that this reflects high ductal flow volume in right aortic arch anatomy (where the left-sided ductus carries the predominant fetal blood flow) and inherent structural characteristics of the mid-ductal segment, which consists of ductal tissue without structural reinforcement from adjacent great vessel walls.
Management of asymptomatic Kommerell diverticulum in paediatric patients remains controversial. The 2022 American College of Cardiology/American Heart Association Aortic Disease Guideline suggests repair may be reasonable for diverticulum diameter ≥3 cm in adults (Class 2b recommendation),Reference Isselbacher, Preventza and Hamilton Black Iii6 but no paediatric guidelines exist.
Luciano et al. advocate for prophylactic surgical resection based on cystic medial necrosis in 67% of resected diverticula, even in infants as young as 11 months.Reference Luciano, Mitchell, Fraisse, Lepidi, Kreitmann and Ovaert7 Cystic medial necrosis predisposes to aneurysmal dilatation, dissection, and rupture, suggesting the diverticulum represents inherently abnormal vascular tissue supporting early intervention.Reference Kim, Cambria and Isselbacher8 Conversely, Erben et al. reported very slow growth rates (mean 1.45 mm/year), with most patients remaining asymptomatic and rupture being rare,Reference Erben, Brownstein and Velasquez9 supporting conservative management with surveillance.
However, vigilant long-term follow-up is essential. The persistent ligamentum arteriosum maintains the potential for vascular ring compression as the child grows, and progressive diverticulum enlargement could cause compression. Regular surveillance with serial echocardiography and cross-sectional imaging is essential. Surgical intervention should be considered if symptoms develop or significant diverticulum enlargement occurs.
In conclusion, this case provides valuable documentation of spontaneous ductal closure in neonatal Kommerell diverticulum and highlights the management dilemma in asymptomatic paediatric patients. The absence of paediatric guidelines underscores the need for long-term natural history data. Serial imaging documentation in cases like ours contributes important information to guide future recommendations.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Competing interests
The authors declare none.
Ethical standard
This research does not involve any human and/or animal experimentation.


 Open access
Open access