


Impact statement
This study presents the first nationally representative evidence on the prevalence and determinants of anxiety among Bangladeshi women of reproductive age, as well as both rural–urban disparities and the role of sociodemographic and reproductive health factors. Utilizing recent BDHS-2022 data and applying a validated GAD-7 scale, the findings underscore that anxiety is not only common but also patterned by structural inequities, such as education, occupation, region and gender norms. Identifying high-risk groups, including older women, those with limited education, women subjected to family pressure to conceive and those who justify domestic violence, provides a basis for targeted mental health screening and intervention programs. The study highlights the necessity of integrating mental health services within reproductive and primary healthcare systems, particularly in underserved rural regions. By demonstrating how reproductive autonomy, socioeconomic status and cultural practices intersect with women’s mental health, this work supports evidence-based strategies to reduce the mental health burden in low-resource settings. It also contributes to the global discourse on women’s health equity, positioning Bangladesh as a case study for other South Asian and low-income countries facing similar challenges.
Introduction
Anxiety is a common mental health disorder marked by excessive apprehension, worry and associated behavioral disturbances (Szuhany and Simon, Reference Szuhany and Simon2022). Globally, anxiety disorders affect millions of individuals across different sociodemographic backgrounds, making it one of the most significant public health concerns (WHO, 2025). In 2019, ~301 million people worldwide (4.05% of the global population) suffered from anxiety disorders, with women being 1.66 times more likely to be affected than men (Javaid et al., Reference Javaid, Hashim, Hashim, Stip, Samad and Al Ahbabi2023). These gender differences are particularly pronounced during the reproductive years, a life stage marked by unique biological, social and economic vulnerabilities that may elevate anxiety risk.
Women of reproductive age represent a critical population for mental health research due to the intersection of hormonal fluctuations, reproductive responsibilities, caregiving roles and gendered social expectations. Evidence suggests that pregnancy, childbirth, childcare demands and social role strain can significantly increase susceptibility to anxiety disorders (Gibson, Reference Gibson2016; Soyannwo et al., Reference Soyannwo, Adebayo and Sigbeku2020). Empirical studies from South Asia further demonstrate a substantial burden of anxiety among women in this age group; for example, a recent study in Nepal reported that 22.2% of women of reproductive age experienced moderate-to-severe anxiety (Tohan et al., Reference Tohan, Saha, Moon, Howlader and Md. Ashfikur2024). Despite this heightened vulnerability, women’s mental health during the reproductive years remains underexamined in many low- and middle-income countries, including Bangladesh.
Anxiety is shaped by multiple social determinants across the life course, including education, socioeconomic status (SES), chronic illness, relationship dynamics and social support (Curran et al., Reference Curran, Rosato, Ferry and Leavey2020; Shawahna et al., Reference Shawahna, Hattab, Al-Shafei and Tab’ouni2020). SES is a particularly influential determinant, as financial insecurity and limited access to healthcare services exacerbate psychological distress, especially among women during economically and socially demanding life stages (Sancako, Reference Sancako2012; Mst. Sadia et al., Reference Sultana, Khan, Hossain, Islam, Hasan, Ahmed, Li and Khan2021). In Bangladesh, evidence from the COVID-19 pandemic highlighted significantly higher anxiety and depression among individuals with monthly incomes below 30,000 BDT and those experiencing food insecurity (Sultana et al., Reference Sultana, Khan, Hossain, Islam, Hasan, Ahmed, Li and Khan2021). Nutritional status also plays an important, yet often overlooked, role in mental health, with research demonstrating a nonlinear association between body mass index (BMI) and anxiety symptoms (Haghighi et al., Reference Haghighi, Jahangard, Ahmadpanah, Bajoghli, Holsboer-Trachsler and Brand2016; Herhaus et al., Reference Herhaus, Kersting, Brähler and Petrowski2020). Studies from Bangladesh similarly indicate a positive association between obesity and anxiety-related outcomes (Hossain et al., Reference Hossain, Bhuiya and Ali2022).
In addition to individual-level risk factors, geographic context is increasingly recognized as a key determinant of mental health. Rural–urban disparities are particularly relevant in Bangladesh, where living environments shape exposure to stressors, availability of resources and access to mental healthcare. Urban populations may face heightened anxiety due to work-related pressures, social isolation, financial strain and environmental stressors, while rural populations often experience mental health challenges linked to poverty, limited healthcare infrastructure and persistent stigma surrounding mental illness (Robertson, Reference Robertson2019; Chebet, Reference Chebet2024). In Bangladesh, rural areas typically have fewer trained mental health professionals, lower mental health literacy and limited service availability, increasing the risk of underdiagnosed and untreated anxiety among women (Khan et al., Reference Khan, Akter, Rahman, Amin, Rahman and Winch2025). Conversely, urban women may encounter distinct stressors such as employment insecurity, gender-based violence and competing work–family demands, resulting in different patterns of anxiety prevalence and severity (Koly et al., Reference Koly, Tasnim, Ahmed, Saba, Mahmood, Farin, Choudhury, Ashraf, Hasan, Oloniniyi, Modasser and Reidpath2022; Moon et al., Reference Moon, Md. Shajahan, Md. Monjurul, Farhana Arefeen and Md. Sazzadur Rahman2024).
The mental health landscape in Bangladesh is particularly concerning, with 16.8% of the population experiencing mental disorders, among them 16.7% were men and 17% were women (WHO, 2019). The COVID-19 pandemic exacerbated these conditions, disproportionately affecting women, low-income individuals and those with limited access to essential services (Mst. Sadia et al., Reference Sultana, Khan, Hossain, Islam, Hasan, Ahmed, Li and Khan2021, Reference Sultana, Khan, Hossain, Ansar, Sikder and Hasan2023; Javaid et al., Reference Javaid, Hashim, Hashim, Stip, Samad and Al Ahbabi2023). Furthermore, recent research indicates a strong relationship between mental health distress and suicide rates, with female students being disproportionately affected. A retrospective study found that 61% of student suicides in Bangladesh involved female students, with 7% explicitly linked to anxiety and depression (Himel et al., Reference Himel, Siyam, Tanni, Rafiquzzaman, Alam, Hassan and Uddin2024). Bangladesh’s socioeconomic context, marked by persistent poverty, health disparities and a fragile mental health support system, creates a complex environment where multiple factors, including SES, chronic illness and nutrition, jointly influence anxiety outcomes among women. However, most existing studies have examined these factors in isolation, failing to address the compounding effects of rural–urban disparities on women’s mental health.
Although Bangladesh enacted the Mental Health Act in 2018 to replace the Lunacy Act of 1912, significant implementation challenges remain, including shortages of trained personnel, limited service coverage and inadequate budget allocation (Karim and Shaikh, Reference Karim and Shaikh2021; Barua, Reference Barua2024). As a result, mental health needs, particularly among vulnerable populations such as women of reproductive age, remain largely unmet. Importantly, most existing studies in Bangladesh have examined anxiety risk factors in isolation, with limited attention to how rural–urban disparities interact with socioeconomic and health-related determinants to shape women’s mental health outcomes. (Hasan et al., Reference Hasan, Anwar, Christopher, Hossain, Hossain, Koly, Saif-Ur-Rahman, Ahmed, Arman and Hossain2021).
To address this gap, the present study examines the prevalence and determinants of anxiety among women of reproductive age in Bangladesh, with a specific focus on rural–urban disparities. Using nationally representative data from the Bangladesh Demographic and Health Survey (BDHS) 2022, this study aims to identify key individual and contextual-level risk factors, assess geographic differences in anxiety burden and inform targeted mental health policies and interventions. A clearer understanding of these dynamics is essential for developing equitable, evidence-based strategies to improve women’s mental health across diverse socioeconomic and geographic settings in Bangladesh.
Methods
Study design and data source
To ensure comprehensive and accurate reporting of observational research, the study adhered to the STROBE guidelines (see Supplementary File 3). Data were derived from the 2022 Bangladesh Demographic and Health Survey (BDHS), a nationally representative survey that employed a two-stage stratified cluster sampling technique. The BDHS aimed to provide comprehensive data on population health and socioeconomic indicators. A total of 20,029 individuals aged 15–49 years were selected from both urban and rural areas of Bangladesh, via face-to-face interviews with validated questionnaires and trained data collectors. Details of the study design, sampling procedure and data collection strategies were stated in detail in the BDHS 2022 published report (NIPORT and ICF, 2023).
To facilitate statistical analysis, data are provided in separate files by unit of analysis. The dataset used in this study was derived from the Individual Recode File (IR), which contains individual-level information on adults in selected households. This dataset includes variables on socioeconomic factors, health status and mental health. Data on nutritional status (via BMI) and anxiety levels (measured using the GAD-7 scale) were analyzed. We focused on participants aged 15 years and older who could self-report information.
Variables and measures
The study examined the impact of socioeconomic characteristics and nutritional status on anxiety levels. Participants’ socioeconomic characteristics, nutritional status and mental health outcomes (specifically anxiety) were the primary variables of interest.
Dependent variable
The Generalized Anxiety Disorder-7 (GAD-7) scale, which includes the following items, was used to quantify anxiety: (a) feeling nervous, anxious or on edge; (b) not being able to stop or control worrying; (c) worrying too much about different things; (d) trouble relaxing; (e) being so restless that it is hard to sit still; (f) becoming easily annoyed or irritable; and (g) feeling afraid as if something awful might happen. The GAD-7’s total score is determined by adding the results of each of the seven items. A score of 0, 1, 2 or 3 is given to each symptom on the GAD-7 based on how often the respondent reported experiencing it in the 2 weeks before the survey: 1 = Seldom; 2 = Frequently; 3 = Always; 0 = Never. A GAD-7 score might be anywhere between 0 and 21. Anxiety symptoms are more severe when scores are higher. A GAD-7 score of 0–4 represents minimal anxiety, 5–9 represents mild anxiety, 10–14 represents moderate anxiety and 15–21 represents severe anxiety (Spitzer et al., Reference Spitzer, Kroenke, Janet and Löwe2006). Reliability analysis indicated high internal consistency for the GAD-7, with a Cronbach’s α of 0.834. In this study, GAD-7 scores from 0 to 9 were coded as 0, and scores from 10 to 21 were coded as 1, consistent with the validated cutoff of ≥10 (Kroenke et al., Reference Kroenke, Spitzer, Janet and Löwe2010; Muñoz-Navarro et al., Reference Muñoz-Navarro, Cano-Vindel, Moriana, Medrano, Ruiz-Rodríguez, Agüero-Gento, Rodríguez-Enríquez, Pizà and Ramírez-Manent2017) and supported by evidence from Bangladesh showing the same threshold (Raza et al., Reference Raza, Banik, Noor, Sayeed, Saha, Jahan, Ashiquzzaman, Siddique, Ahmed and Rahman2025).
Independent variables
The independent variables included the following socioeconomic characteristics: age (15–24, 25–34 and 35–49 years), division (Dhaka, Chittagong, Khulna, Rajshahi, Rangpur, Sylhet, Mymensingh, Barisal), residence (urban, rural), religion (Islam, others), education level (no education, secondary, higher), employment status (currently working: yes, no), occupation (not working, agriculture, skilled labor/professional, domestic labor), wealth index (poor, middle, rich), husband education (no education, primary, secondary and higher), husband occupation status (currently working: yes, no), household head sex (male, female), household family members (<3, >3), number of living children (no children, 1 or 2 children, more than 3 children) and mass media access (tv, radio, internet). Maternal characteristics were as follows: menstruation status in last 6 weeks (yes, no), fertility preference (undecided, no more, want more), decision-maker for using contraception (respondent, husband, joint decision), became pregnant by family pressure (yes, no), ever terminated pregnancy (yes, no), justifies wife beating if refuse to intercourse (yes, no) status were self-reported by the participants and death of any children (yes, no). For nutritional status, height and weight were measured during data collection, allowing the calculation of body mass index (BMI). Nutritional status was classified according to the World Health Organization (WHO) BMI categories: underweight (BMI < 18.5), normal weight (BMI 18.5–24.9), overweight (BMI 25–29.9) and obese (BMI ≥ 30) (World Health Organization, n.d.).
Data analysis
The analysis of data and visualization was performed using software: Stata version 17 and R version 4.4.2. Descriptive statistics were computed to summarize the socioeconomic, health and nutritional characteristics of the sample. Frequencies and percentages were used to represent categorical variables.
Bivariate analyses (chi-square tests) were conducted to explore associations between independent variables (socioeconomic factors, nutritional status) and the outcome variable (anxiety). To account for the hierarchical structure of the BDHS data, with women nested within primary sampling units, univariate multilevel logistic regression was performed, and variables with a p-value <0.20 were selected for the adjusted model and a multivariable multilevel logistic regression model was used to estimate adjusted odds ratios (AORs) and 95% confidence intervals (CIs) for anxiety, adjusting for potential confounding variables, including age, gender and other factors. Sampling weights for the BDHS 2022 dataset were applied using Stata’s survey estimation procedures (the “svy” command) to obtain nationally representative estimates, accounting for sample clustering (StataCorp LLC, n.d.). Multicollinearity was assessed using the Variance Inflation Factor (VIF).
Model performance
The performance of the model was evaluated using the Receiver Operating Characteristic (ROC) curve and measured using the Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) values to assess the accuracy and goodness of fit. An AUROC value above 0.50 reflects the model’s ability to differentiate between two groups, and a lower p-value supports this discriminative capability (Cook and Rajbhandari, Reference Cook and Rajbhandari2018; Hasan et al., Reference Hasan, Md. Rashed, Chowdhury, Rahman, Hasan, Kabir and Uddin2023). Advanced statistical measures, including Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC), were also employed. These measures helped evaluate the variation at the community level and tested the robustness of the model. AIC and BIC values indicated a better balance between model complexity and fitness. Together, these evaluations ensured a comprehensive assessment of the model’s predictive and explanatory capabilities.
Ethical considerations
This study utilized the publicly available Bangladesh Demographic and Health Survey 2022 data. So, no ethical clearance was needed to conduct the study. The Bangladesh Demographic and Health Survey 2022 was conducted by NIPORT and ICF International, with ethical approval from the ICF Institutional Review Board in line with the Helsinki Declaration (1964). All participants provided informed verbal consent before the interview process. The data is publicly available on the DHS program website (https://dhsprogram.com/methodology/survey/survey-display-584.cfm) and permitted for use. Detailed information on participant selection, sample size and data collection methods is available in the BDHS reports (NIPORT and ICF, 2023).
Results
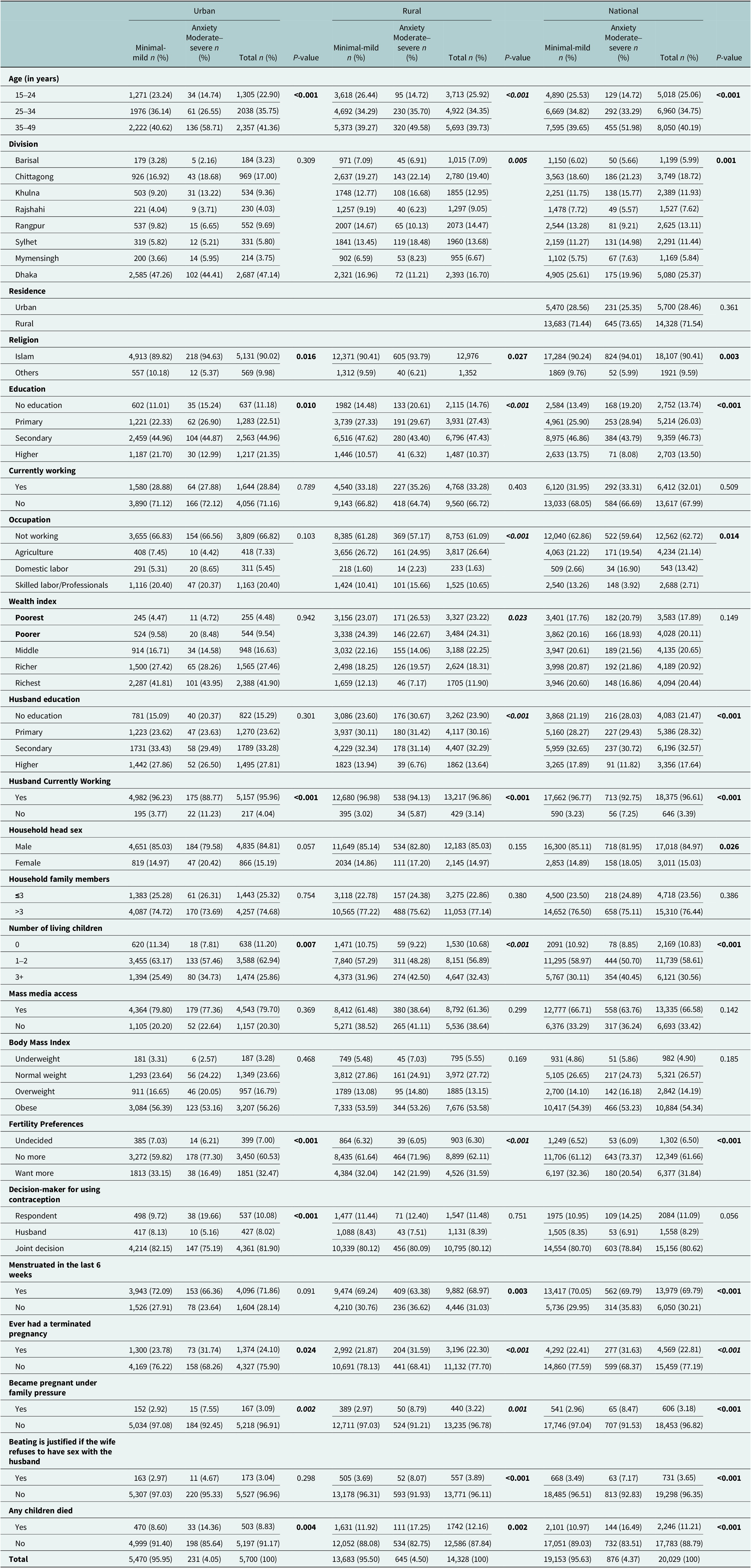
Table 1 depicts that the prevalence of anxiety symptoms varies across urban and rural areas in Bangladesh, influenced by sociodemographic status, chronic diseases and nutritional factors. Overall, 22.11% (n = 4,429) of respondents experienced mild anxiety symptoms, while 4.37% (n = 876) exhibited moderate-to-severe anxiety. The prevalence of mild anxiety was slightly higher among rural women at 22.63% (n = 3,243) compared to 20.81% (n = 1,186) in urban areas. Similarly, moderate-to-severe anxiety was more prevalent in rural areas at 4.5% (n = 645) than in urban settings at 4.05% (n = 231) (Figure 1).
Table 1. Distribution of anxiety prevalence in rural, urban area and in National across sociodemographic status, and nutritional status


Figure 1. Prevalence of anxiety in Bangladesh.
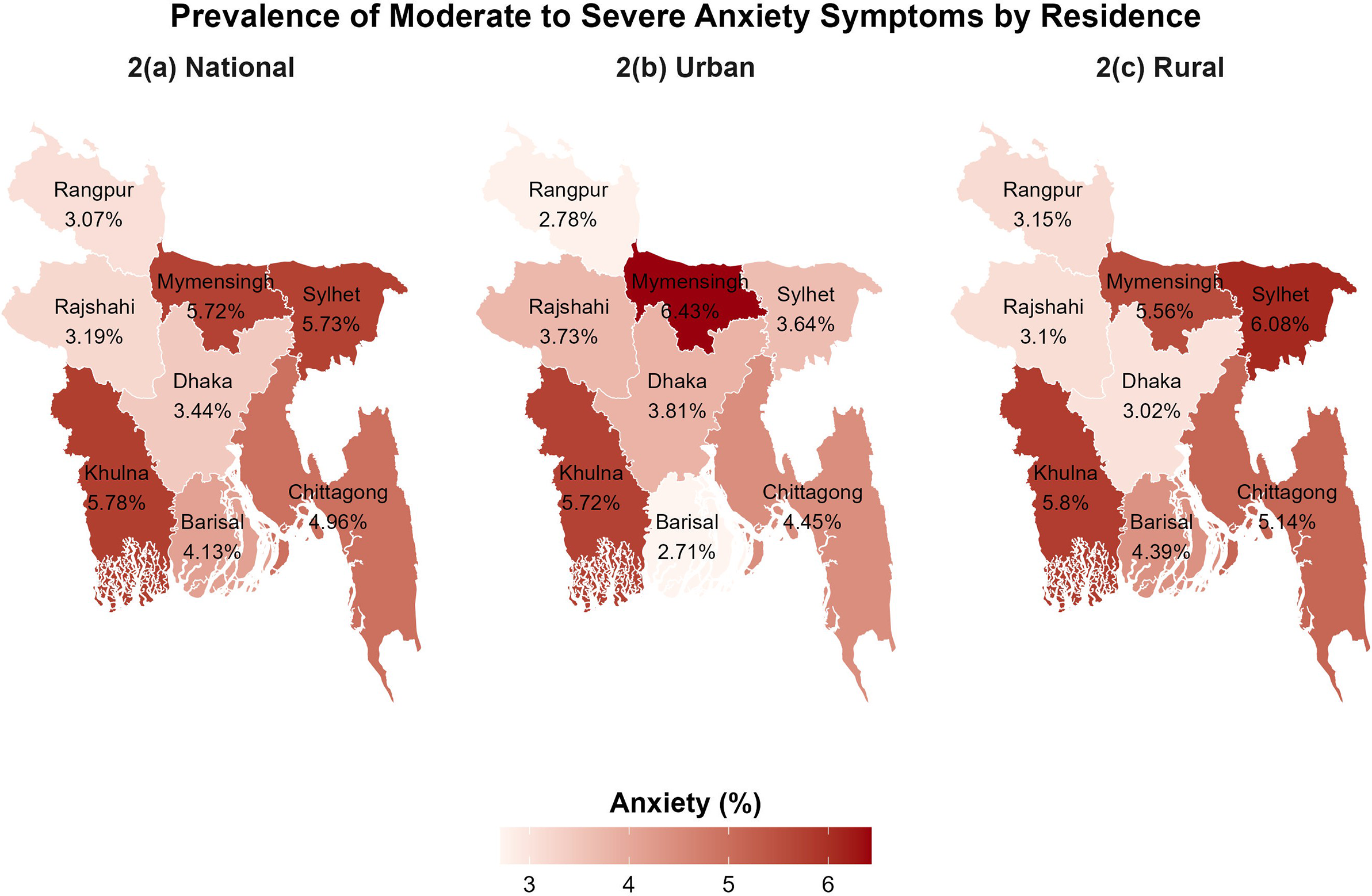
Age is significantly associated with anxiety (p < 0.001), with the highest proportion among those aged 35–49 years (51.98%), and the lowest among 15–24 years (14.72%). The spatial prevalence of anxiety is further illustrated in Figure 2. At the national level, Khulna (5.78%), Sylhet (5.73%) and Mymensingh (5.72%) exhibited the highest prevalence. In urban areas, Mymensingh recorded the highest prevalence (6.43%), followed by Khulna (5.72%) and Chittagong (4.45%). In rural settings, Sylhet showed the highest prevalence (6.08%), with Khulna (5.80%) and Mymensingh (5.56%) also demonstrating elevated levels. These patterns highlight persistent regional clustering of anxiety prevalence, with Mymensingh, Sylhet and Khulna emerging as consistently high-burden divisions. These regional disparities showed a statistically significant association with anxiety prevalence (p < 0.001 for rural and national).

Figure 2. Prevalence of moderate-to-severe anxiety symptoms at the division level in Bangladesh.
More detailed insights are provided, mapping the district-wise prevalence of moderate-to-severe anxiety symptoms (Supplementary File 1). Nationally, the highest prevalence of moderate-to-severe anxiety symptoms was observed in Kushtia (14.79%), followed by Nilphamari (12.18%) and Sirajganj (9.09%). In urban areas, the prevalence was highest in Magura (15.38%), Nilphamari (12.26%) and Chandpur (12.21%). In rural settings, the greatest prevalence was reported in Kushtia (15.38%), Lakshmipur (12.05%) and Nilphamari (12.17%). Anxiety symptoms were slightly more common among Muslim women compared to women of other religions, with the differences being significantly associated with anxiety across urban, rural and overall populations (p < 0.05). Among urban women experiencing moderate-to-severe anxiety, the largest shares had secondary (44.78%) and primary (26.90%) education. Rural trends were similar, with secondary education (43.40%) showing the highest percentage. Lower educational attainment overall was significantly associated with higher anxiety (p < 0.001). Occupation also played a role. The majority of cases in urban (66.56%) and rural (57.17%) areas were concentrated among unemployed individuals. Urban skilled laborers (20.37%) and rural individuals (24.95%) in agriculture showed a higher proportion, all statistically significant with anxiety (p < 0.001 for rural and in total and p = 0.014 for urban areas).
Economic status, assessed by the wealth index, was associated with higher anxiety levels in rural (p = 0.023). Among anxious women, 24.31% were from poorer rural households. Husband’s education was also important; women whose husbands had lower or no education experienced higher anxiety, especially in rural areas (p < 0.001). Although most husbands were employed (linked to lower anxiety), a small but significant difference persisted overall (p < 0.001).
Male-headed households showed a greater share of anxiety cases among the urban residents (79.58%) and overall (81.95%), with the association being statistically significant (p = 0.026). The distribution of women with moderate-to-severe anxiety varied significantly by the number of living children across all residence types (p < 0.001). Most women with anxiety wanted no more children, whereas it was significantly lower among those who were undecided or wanted more children across all residence types (p < 0.001). Among women with anxiety, the majority reported joint decision-making regarding contraception (75.19% urban, 80.09% rural), whereas a smaller proportion made the decision independently (19.66% urban, 12.40% rural); the association was statistically significant only in urban areas (p < 0.001). As usual, menstruation showed a significant relationship with women’s overall anxiety level (p < 0.001); However, while the result showed an insignificant relationship with urban women and menstruation, rural women’s anxiety was significantly influenced by it (p = 0.004). Among the study sample, one-third of those who had experienced anxiety had ever terminated their pregnancy. In the regional analysis, similar trends were shown in the rural area. Though the number of women who had experienced anxiety and were pregnant due to in-laws’ family pressure was found to be minimal, the relationship between the two variables was found to be significant overall (p < 0.001), and in regional (p = 0.002 for urban, p = 0.001 for rural) analysis, rural women were the highest in number. In case of the women who justify being beaten by their husbands when they refused to engage in intercourse, the trends were almost similar (overall: p < 0.001; rural: p < 0.001). Women who had lost a child showed a higher rate of anxiety symptoms compared to those who had not, with this difference being significant in urban, rural and overall populations (p < 0.001).
In terms of health indicators, while BMI was not significantly associated with anxiety (p = 0.185), over half of the individuals with anxiety were classified as obese: 53.26% in rural areas, 53.16% in urban areas and 53.23% overall.
Table 2 presents the adjusted odds ratios (AORs) and 95% confidence intervals of various factors associated with anxiety across urban, rural and national populations, after adjusting for potential confounders. Age remained a significant factor at the rural and national levels. Compared to the reference group aged 15–24 years, individuals aged 25–34 and 35–49 years were more likely to report anxiety, with those aged 35–49 years having 1.89 times greater odds in rural areas (AOR = 1.89, 95% CI: [1.31–2.86], p < 0.001) and 1.75 times greater odds in the national analysis (AOR = 1.75, 95% CI: [1.24–2.46], p = 0.001). However, age did not show a significant association with anxiety in the urban subgroup.
Table 2. Multilevel logistic regression of anxiety prevalence in the rural, urban areas and across the country based on sociodemographic and reproductive health status

Geographical variations in anxiety were prominent. Compared to Dhaka, individuals residing in Khulna and Sylhet divisions had significantly higher odds of experiencing anxiety. The odds were highest in Khulna at the national level (AOR = 1.86, 95% CI: [1.22–2.86], p = 0.004), followed by Sylhet (AOR = 1.74, 95% CI: [1.14–2.65], p = 0.011). Additionally, women residing in urban areas of Mymensingh had higher odds of anxiety compared to those in Dhaka (AOR = 1.98, 95% CI: [1.08–3.64], p = 0.027).
Muslim women had significantly higher odds of experiencing anxiety compared to women of other religions, both in urban (AOR = 2.62, 95% CI: [1.268–3.64], p = 0.027), rural (AOR = 2.02, 95% CI: [1.32–2.69], p = 0.006) and overall (AOR = 2.13, 95% CI: [1.46–3.12], p < 0.001) analyses. Women with secondary education had significantly higher odds of anxiety in urban areas (AOR = 2.19, 95% CI: [1.03–4.65]; p = 0.042) compared to those with higher education, whereas no significant association was observed in rural or national level.
Occupational status was another important factor. Those engaged in agriculture were significantly less likely to experience anxiety than skilled laborers or professionals in urban, rural and national samples (Urban AOR = 0.36, 95%CI: [0.16–0.81], p = 0.014; Rural AOR = 0.51, 95% CI: [0.37–0.70], p < 0.001; National AOR = 0.56, 95% CI: [0.42–0.75], p < 0.001). Individuals not working also had slightly reduced odds for urban and national level (Rural AOR = 0.56, 95% CI: [0.41–0.76], p < 0.001; National AOR = 0.66, 95% CI: [0.51–0.85], p = 0.001). Across rural and national estimates, women in the richest households consistently had significantly lower odds of anxiety compared to the poorest group (Rural AOR = 0.48, 95% CI: [0.29–0.76], p = 0.002; National AOR = 0.65, 95% CI: [0.46–0.93], p = 0.002). Women whose husbands had no formal education had significantly higher odds of experiencing anxiety in rural areas (AOR = 1.68, 95% CI: [1.03–2.76], p = 0.034) compared to those whose husbands had higher education. Similar associations were found for primary (AOR = 1.63, 95% CI: [1.02–2.62], p = 0.043) and secondary education (AOR = 1.77, 95% CI: [1.10–2.84], p = 0.018), but only in rural settings. No significant association was observed in urban or overall analyses.
Additionally, women whose husbands were not currently working had significantly higher odds of anxiety compared to who were working across all settings: urban (AOR = 2.46, 95% CI: [1.37–4.35], p = 0.002), rural (AOR = 1.84, 95% CI: [1.21–2.80], p = 0.005) and overall (AOR = 2.14, 95% CI: [1.53–2.99], p < 0.001).
Reproductive health and gender-based attitudes also showed strong links to anxiety. Participants who reported not wanting any more children had significantly higher odds of experiencing anxiety in urban areas compared to those who wanted more children (AOR = 2.15, 95% CI: [1.22–3.77], p = 0.008). Regarding decision-making on contraception, women whose husbands were the sole decision-makers had significantly lower odds of anxiety in urban areas compared to those who made the decision themselves (AOR = 0.34, 95% CI: [0.15–0.75], p = 0.008), and those reporting joint decision-making also had lower odds (AOR = 0.59, 95% CI: [0.38–0.91], p = 0.009).
Women who menstruated in the last 6 weeks had significantly lower odds of anxiety compared to women who did not in rural (AOR = 0.81, 95% CI: [0.67–0.98], p = 0.028) and overall analyses (AOR = 0.81, 95% CI: [0.68–0.96], p = 0.01). Meanwhile, having a history of a terminated pregnancy showed significantly higher odds of anxiety in rural (AOR = 1.48, 95% CI: [1.20–1.81], p < 0.001) and overall samples (AOR = 1.46, 95% CI: [1.22–1.75], p < 0.001) compared to those without such history.
Women who conceived due to family pressure had significantly higher odds of anxiety in both regions, rural (AOR = 3.52, 95% CI: [2.26–5.48], p <0.001), urban (AOR = 2.94, 95% CI: [1.51–5.74], p = 0.001) and national samples (AOR = 3.41, 95% CI: [2.35–4.96], p < 0.001). Additionally, those who justified wife-beating in the context of refusing sex showed significantly higher odds of anxiety in the national sample (AOR = 2.10, 95% CI: [1.43–3.10], p < 0.001) and in the rural regions (AOR = 2.14, 95% CI: [1.41–3.23], p < 0.001) underscoring the mental health impact of internalized gender norms and coercion.
While assessing the robustness of the model, the area under the ROC curve (AUROC) was reported as 82.57% for the urban, 85.16%for rural and 84.47% for the overall model, with a 95% CI ranging from 83.23 to 85.71, which is higher than the cutoff value of 0.50 (Figure 3).

Figure 3. ROC curve of the multilevel logistic regression model for the national, urban, and rural populations, respectively.
The logistic regression models were evaluated using model selection and goodness-of-fit statistics. For model fit, both Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) values were lowest in the urban model (AIC = 1,550.185, BIC = 1774.027), indicating a relatively better fit compared to the rural (AIC = 4,311.504, BIC = 4,600.844) and overall models (AIC = 5,820.24, BIC = 6,149.294).
Discussion
This study examined the prevalence and determinants of anxiety among women of reproductive age in Bangladesh using nationally representative BDHS 2022 data, with analyses stratified by rural, urban and national settings. The findings demonstrate a substantial burden of anxiety and reveal marked disparities by geography, socioeconomic position and gender-related factors. Given the cross-sectional nature of the data, all findings should be interpreted as associations rather than causal relationships.
From a theoretical standpoint, the observed patterns align with frameworks of gendered social determinants of mental health and women’s autonomy, which emphasize that mental health outcomes are shaped by structural inequalities, power relations and socially prescribed gender roles rather than individual characteristics alone (Scheffer Lindgren and Renck, Reference Scheffer Lindgren and Renck2008; McAllister et al., Reference McAllister, Fritzell, Almroth, Harber-Aschan, Larsson and Burström2018; Wessells and Kostelny, Reference Wessells and Kostelny2022). In patriarchal contexts such as Bangladesh, constrained reproductive autonomy, economic dependence and exposure to coercive norms can cumulatively elevate psychological distress among women (Shahabuddin et al., Reference Shahabuddin, Nöstlinger, Delvaux, Sarker, Bardají, Brouwere and Broerse2016; Shahabuddin et al., Reference Shahabuddin, Nöstlinger, Delvaux, Sarker, Delamou, Bardají, Broerse and de Brouwere2017; Koly et al., Reference Koly, Tasnim, Ahmed, Saba, Mahmood, Farin, Choudhury, Ashraf, Hasan, Oloniniyi, Modasser and Reidpath2022).
Our analysis revealed that nationally, around 22.11%, or 22 in every 100 women of reproductive age, reported mild symptoms of anxiety. The total prevalence of mild anxiety at 22.11% among the reproductive age women is higher than the global estimate reported in the Global Burden of Disease report (7%) (IHME, 2024) and in the neighboring country – India (4%) (Annajigowda et al., Reference Annajigowda, Nirisha, Ganjekar, Rao, Gururaj, Varghese and Benegal2023) and Nepal (22.2%) (Tohan et al., Reference Tohan, Saha, Moon, Howlader and Md. Ashfikur2024). Notably, anxiety prevalence was consistently higher among rural women than urban women, diverging from global literature that often identifies urbanization as a major risk factor due to environmental stressors and social fragmentation (Gruebner et al., Reference Gruebner, Rapp, Adli, Kluge, Galea and Heinz2017; Solmi et al., Reference Solmi, Dykxhoorn, Kirkbride, Okkels, Kristiansen and Munk-Jørgensen2017; Javaid et al., Reference Javaid, Hashim, Hashim, Stip, Samad and Al Ahbabi2023). In Bangladesh, however, rural women may experience compounded vulnerabilities, including poverty, limited healthcare access, restricted mobility and entrenched gender norms, which together may intensify anxiety risk.
Age-specific trends indicated a peak in anxiety prevalence among individuals aged 35–49 years, aligning with findings from India (Annajigowda et al., Reference Annajigowda, Nirisha, Ganjekar, Rao, Gururaj, Varghese and Benegal2023), Nepal (Pandey et al., Reference Pandey, Adhikari, Bista, Lamichhane, Joshi, K, Sharma and Baral2024; Tohan et al., Reference Tohan, Saha, Moon, Howlader and Md. Ashfikur2024) and Brazil (Andrade et al., Reference Andrade, Wang, Andreoni, Silveira, Alexandrino-Silva, Siu, Nishimura, Anthony, Gattaz, Kessler and Viana2012), and even in the global trends study (Liu et al., Reference Liu, Luo, Huang, Tan, Cheng and Wu2024). Furthermore, a population-based study depicted a similar trend among older adults of the country (Sarker, Reference Sarker2021), which identified middle adulthood as a pivotal period due to heightened social and economic responsibilities and health issues. Generally, some studies show anxiety resilience among younger populations and argue that the younger individuals have greater flexibility and social support networks compared to older individuals who often face more responsibilities and health issues (Majnarić et al., Reference Majnarić, Bosnić, Guljaš, Vučić, Kurevija, Volarić, Martinović and Wittlinger2021; Shin and Park, Reference Shin and Park2022). The lack of a significant association in urban models suggests that age-related anxiety may be amplified by context-specific stressors, such as livelihood insecurity and weaker social protection mechanisms in rural areas (Folorunsho et al., Reference Folorunsho, Sanmori and Suleiman2025; Gu et al., Reference Gu, Tan, Guo, He and Zhang2025; Yang and Ge, Reference Yang and Ge2025) Pronounced regional clustering of anxiety was observed, with women residing in Khulna, Sylhet and Mymensingh divisions exhibiting significantly higher odds compared to those in Dhaka. Although urban Dhaka is frequently regarded as the focal point of mental health distress due to its population density and social fragmentation (Rahaman et al., Reference Rahaman, Kalam and Al-Mamun2023), our findings align with previous regional studies, indicating that peripheral divisions conceal significant mental health challenges stemming from persistent poverty, inadequate institutional support and widespread detrimental traditional practices (Arafat, Reference Arafat and Arafat2024; Arafat et al., Reference Arafat, Giasuddin, Mazumder, Arafat and Kar2024). Khulna is particularly vulnerable to climate-related stressors, such as salinity intrusion, livelihood disruption and displacement, which have been associated with psychological distress in affected populations (Kabir et al., Reference Kabir, Newnham, Dewan, Islam and Hamamura2024). Sylhet, despite substantial remittance inflows, is characterized by pronounced socioeconomic inequality and transnational family separation, placing caregiving and emotional burdens disproportionately on women (Silver, Reference Silver2014; Löbel, Reference Löbel2020; Galvan et al., Reference Galvan, Rusch, Rodríguez and Garcini2022; Salam et al., Reference Salam, Ahmad, Bristy and Chowdhury2024). Muslim women exhibited significantly higher odds of anxiety compared to women of other religions across rural, urban and national analyses. This association should not be interpreted as a religious effect per se but rather as reflecting broader social and structural contexts in which religious affiliation intersects with gender norms, family structures and expectations surrounding women’s reproductive and marital roles (Yellow Chair Collective, 2023; Dhaliwal, Reference Dhaliwal2025). Prior research in South Asia suggests that mental health disparities attributed to religion are often mediated by restricted autonomy, exposure to intimate partner violence and internalized gender norms rather than belief systems themselves (Niaz and Hassan, Reference Niaz and Hassan2006; Scheffer Lindgren and Renck, Reference Scheffer Lindgren and Renck2008). Educational attainment significantly predicted anxiety, with individuals lacking formal education exhibiting over twice the likelihood of suffering anxiety compared to those with greater education nationally. This aligns with previous research in India (Fahey et al., Reference Fahey, Soni, Allison, Vankar, Prabhakaran, Moore Simas, Byatt, Phatak, O’Keefe and Nimbalkar2017), Nepal (Tohan et al., Reference Tohan, Saha, Moon, Howlader and Md. Ashfikur2024) and Bangladesh (Islam, Reference Islam2019), which identified education as a protective factor, perhaps enhancing health literacy, coping strategies and economic prospects. Notably, urban women with secondary education had the highest anxiety rates, potentially indicating heightened stress due to aspirations for upward mobility and the pressures of navigating socioeconomic transitions (Sultan et al., Reference Sultan, Seager, Rashid, Haque and Khondaker2021; Das and Tampubolon, Reference Das and Tampubolon2022; Chlapecka et al., Reference Chlapecka, Wolfová, Fryčová and Cermakova2023).
The data on occupational status were inconclusive. Specifically, women engaged in agricultural work in rural areas were less likely to report anxiety than those in domestic labor or skilled professions. This echoes findings from studies suggesting that occupations involving natural environments, physical activity and lower levels of social isolation may offer mental health benefits (Coventry et al., Reference Coventry, Brown, Pervin, Brabyn, Pateman, Breedvelt, Gilbody, Stancliffe, McEachan and White2021). Conversely, those engaged in domestic labor often face isolation, long hours and less job security, factors that are linked with higher anxiety levels in research across various contexts, which were found in China (Hall et al., Reference Hall, Pangan, Edward and Huang2019), Pakistan (Husain et al., Reference Husain, Husain and Ijaz2022) and Turkey (Parlak et al., Reference Parlak, Çelebi and Yaman2022). Nevertheless, there is no study on the anxiety and depression levels of Bangladeshi domestic workers. For domestic laborers, especially women, isolation combined with a lack of control over working conditions can increase anxiety, suggesting that workplace policies and support systems could significantly impact mental health outcomes for individuals in these roles (Maeda et al., Reference Maeda, Nomura, Hiraike, Sugimori, Kinoshita and Osuga2019). However, the adjusted model revealed less consistent associations, suggesting possible mediating influences from education, income or familial dynamics.
The notable correlation between reproductive and gender-related characteristics and anxiety in Bangladeshi women highlights the substantial influence of patriarchal norms and restricted reproductive autonomy on mental health. Women who fell pregnant owing to familial coercion or legitimate domestic violence in the setting of sexual rejection had significantly elevated anxiety levels. The 2024 Abuse Against Women Survey indicates that 70% of Bangladeshi women had encountered some intimate partner abuse (IPV), with 41% experiencing it during the preceding year (UNFPA-Bangladesh, 2025). This widespread IPV, frequently grounded in deep-seated gender stereotypes, has been associated with negative mental health consequences, such as heightened anxiety and sadness (Scheffer Lindgren and Renck, Reference Scheffer Lindgren and Renck2008; Wessells and Kostelny, Reference Wessells and Kostelny2022). Women who reported menstruation within the last 6 weeks had significantly lower odds of experiencing anxiety compared to those who had not. Absence of recent menstruation may reflect underlying hormonal imbalances or reproductive disorders (e.g., PCOS), all of which have been linked to heightened anxiety in previous studies (Mueller et al., Reference Mueller, Grissom and Dohanich2014; Humeniuk et al., Reference Humeniuk, Dybciak, Raczkiewicz, Powrózek, Malecka-Massalska, Andrzejczyk, Suski and Bojar2025). Moreover, prior evidence suggests that irregular or infrequent menstruation is associated with a higher risk of anxiety (Abeputri et al., Reference Abeputri, Herlinawati and Arifandi2023).
The heightened anxiety levels in rural women underscore the persistent impact of entrenched patriarchal attitudes and insufficient autonomy as significant factors adversely influencing mental health. In rural areas, women’s agency in decision-making, particularly with reproductive choices, is frequently constrained, resulting in heightened susceptibility to mental health challenges (Shahabuddin et al., Reference Shahabuddin, Nöstlinger, Delvaux, Sarker, Bardají, Brouwere and Broerse2016; Koly et al., Reference Koly, Tasnim, Ahmed, Saba, Mahmood, Farin, Choudhury, Ashraf, Hasan, Oloniniyi, Modasser and Reidpath2022). The considerable influence of decision-making processes on contraceptive and anxiety forecasting corresponds with international research highlighting the significance of reproductive autonomy in mental health. Research reveals that women possessing greater decision-making autonomy over contraceptives are more likely to have improved mental health outcomes (Hall et al., Reference Hall, Steinberg, Marcus, Allen and Cwiak2014; Bawuah and Kodzo, Reference Bawuah and Kodzo2025; Swan et al., Reference Swan, Wasser and Cannon2025).
Although BMI was not significantly associated with anxiety after adjustment, descriptive patterns indicated elevated anxiety among underweight and overweight women. In rural settings, underweight women appeared particularly vulnerable, potentially reflecting food insecurity and compounded reproductive and socioeconomic stressors (Khudri et al., Reference Khudri, Osmani and Okunade2024). Unlike high-income settings where obesity-related stigma is a dominant pathway to anxiety, nutritional vulnerability in Bangladesh may operate through different psychosocial mechanisms (Herhaus et al., Reference Herhaus, Kersting, Brähler and Petrowski2020; Eik-Nes et al., Reference Eik-Nes, Tokatlian, Raman, Spirou and Kvaløy2022).
Strengths and limitations
This study has several strengths that contribute to its significance and robustness. First, it is a substantial, representative sample of individuals in Bangladesh, enhancing the generalizability of the findings to similar populations. The use of multivariable logistic regression allows adjustment for potential confounding variables, providing a more accurate assessment of the factors associated with anxiety. Additionally, the study draws on comprehensive BDHS 2022 data, ensuring high-quality data collection using validated measures. This approach strengthens the reliability of the findings and offers valuable insights for public health interventions targeting mental health.
However, the study also has some limitations. As a cross-sectional study, it establishes associations but cannot infer causation, making it difficult to determine the temporal relationship between the identified factors and anxiety. Self-reported information may be subject to social desirability bias or recall bias, which could compromise the accuracy of responses regarding lifestyle choices and mental health. Furthermore, the study may not capture all relevant contextual or cultural factors influencing anxiety, limiting a deeper understanding of the issue within specific subpopulations. Although the models adjusted for key sociodemographic and health-related variables, other potentially important factors, such as social support, life stressors and comorbid depression, were not available in the dataset and may have over-adjustment effects. Finally, although useful, the logistic regression model may not account for all nuances of complex human behaviors and mental health outcomes. Future research employing longitudinal and qualitative methods could help address these limitations, providing a more comprehensive view of the determinants of anxiety in this context.
Recommendations
Collectively, these findings underscore persistent rural–urban and regional disparities in anxiety among women of reproductive age in Bangladesh, rooted in socioeconomic vulnerability, gender inequality and constrained autonomy. Mental health policies should move beyond uniform approaches and adopt gender-responsive, region-specific strategies. In rural areas, interventions should prioritize women’s empowerment, reproductive autonomy and access to integrated mental and reproductive healthcare. Urban strategies should address employment-related stress, educational pressures and psychosocial support. At the national level, integrating mental health services into primary healthcare, particularly in underserved regions, remains essential for reducing inequities and improving women’s mental well-being.
Conclusion
This study highlights the prevalence of anxiety among Bangladeshi women of reproductive age, with 4.37% experiencing moderate-to-severe anxiety, and rural women experiencing the most. By identifying significant predictors using multivariable logistic regression, the research offers valuable insights into the sociodemographic, health and lifestyle factors contributing to anxiety. Key predictors include age (35–49 years), religion, occupation, geographic disparities (e.g., Sylhet region), husband’s education and employment status, abortion history, family pressure to conceive and justification of wife-beating.
These results underscore the imperative for context-specific mental health policies. In rural regions, comprehensive interventions aimed at women’s empowerment, maternal autonomy and context-specific health access are crucial. Conversely, urban mental health initiatives should emphasize chronic illness treatment, educationally associated psychosocial support and interventions addressing employment-related stress. National policy should move beyond uniform solutions and emphasize integrating regional mental health services into primary healthcare, particularly in underserved rural areas.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10170.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10170.
Data availability statement
This study used data from Bangladesh’s Demographic and Health Surveys (DHS), which can also be accessed on the DHS program’s website (www.dhsprogram.com). The Bangladesh Standard-DHS 2022 data set is available at https://dhsprogram.com/data/available-datasets.cfm
Author contributions
MHR: conceptualization, formal analysis, investigation, methodology, project administration, visualization, writing – original draft, writing – review and editing; KHP: data curation, formal analysis, visualization, investigation, software, resources, writing – original draft, writing – review and editing; MNH: formal analysis, visualization, software, investigation, methodology, writing – original draft, writing – review and editing; MABC: formal analysis, software, supervision, validation, writing – review and editing; MJU: supervision, validation, writing – review and editing.
Competing interests
The authors declare none.
Ethics approval and consent to participate
This study utilized the publicly available Bangladesh Demographic and Health Survey 2022 data. So, no ethical clearance was needed to conduct the study. The Bangladesh Demographic and Health Survey 2022 was conducted by NIPORT and ICF International, with ethical approval from the ICF Institutional Review Board in line with the Helsinki Declaration (1964). All participants provided informed verbal consent before the interview process. The data is publicly available on the DHS program website (https://dhsprogram.com/methodology/survey/survey-display-584.cfm) and is permitted for use. Detailed information on participant selection, sample size and data collection methods is available in the BDHS reports (NIPORT and ICF, 2023).






 Open access
Open access