


Introduction
Persistent regional inequalities in radiotherapy access remain a major concern across the United Kingdom (UK). 1 The term ‘postcode lottery’ refers to the unequal availability and quality of health services across different postcodes. In the context of health and social care, it originated around 1997 to describe regional variation in access to care and treatments. Reference Redhead and Lynch2 The NHS Constitution asserts equal access to services regardless of location, yet studies indicate notable regional disparities in cancer diagnosis and treatment. Reference Chamberlain, Owen-Smith and Donovan3 Recent evidence confirms that a substantial proportion of UK cancer patients feel disadvantaged by local variations; Macmillan reports that ∼40% of people with cancer have struggled to get appropriate care simply because of where they live, 4 and a survey of UK genetics services found ∼48% of England’s population lacked full implementation of familial breast cancer screening guidelines due to region-to-region differences. Reference Evans, Edwards and Duffy5 In Wales, these regional disparities have manifested in cancer outcomes; a Royal College of Physicians report found five-year cancer survival is lower in Swansea Bay (55%) than in Cardiff (58.9%) or Powys (59.3%), underlining significant local differences, 6 with women living in the most deprived parts of Wales living nearly 6 years less than those in the least deprived areas.
Cancer services in Wales are delivered by the seven local health boards, with three specialist oncology centres. In South-West Wales, Swansea Bay University Health Board (UHB) covers Swansea, Neath and Port Talbot, while Hywel Dda UHB covers Carmarthenshire, Pembrokeshire and Ceredigion, serving roughly one-third of Wales’ population. SWWCC at Singleton Hospital in Swansea serves as the specialist oncology hub for these regions, as well as a small portion of Powys UHB, meaning many patients must travel significant distances to receive treatment. Reference Purden, Jackson and Lewis7
Delays between surgery and radiotherapy can be critical; national guidance recommends adjuvant breast radiotherapy begin within 4–8 weeks post-surgery. 8 If radiotherapy resources are limited (e.g., machine capacity or staffing shortages), these intervals can lengthen, potentially affecting outcomes. Further, if patients find it challenging to travel for appointments, the time between key steps in the pathway will be extended. Staffing shortages exacerbate the issue: Wales has one of the most significant cancer workforce gaps in the UK. The Royal College of Radiologists reported that 30% of Welsh radiologists were due to retire by 2021, with only three new oncology consultant posts created between 2013 and 2019. As of 2024, Wales faces a 32% shortfall, 3% higher than the UK average. 9 To mitigate this, Swansea Bay UHB has begun training consultant radiographers to expand oncology capacity.
Early detection depends on screening and timely diagnosis. In Wales, women aged 50–70 are invited for breast screening every three years. Uptake in 2021–2022 reached 70.0%, meeting the national standard for the first time, but remains regionally uneven 10 : South-West Wales recorded the highest rate (72.5%), while North and South-East Wales were below target. COVID-19 disruptions reduced screening activity, and Audit Wales (2024) notes that uptake has remained below pre-pandemic levels. 11 Such variation suggests postcode effects, with rural areas of higher deprivation showing lower participation and later diagnosis.
After referral, either due to screening abnormality or General Practitioner suspicion, diagnosis involves imaging and biopsy. Unlike England, Wales has not adopted the 28-day Faster Diagnosis Standard; instead, it applies a Single Cancer Pathway (since 2019), combining urgent and routine referrals under a 62-day standard for diagnosis and treatment. 12 The national target is for ≥75% of patients to begin treatment within 62 days of first suspicion, though performance remains below this level (Figure 1). Nonetheless, Swansea Bay UHB performs strongly, with no therapy pathways exceeding the 14-week target and no waits over one or two years. In July 2025, 87.9% of Swansea Bay UHB breast cancer patients began treatment within 62 days, the highest in Wales by 12.4%. 13 Historically, Wales met the previous 31-day target (∼98% in 2016) but routinely missed the 62-day standard. 14
Percentage of patients starting first definitive treatment within target time, all cancer sites, Swansea Bay (blue), Wales (yellow), December 2020 to July 2025 15 .

The time it takes to get to a radiotherapy centre by private car or public transport can affect a patient’s decision to access radiotherapy treatment. Reference Han, Sullivan and Tree16 In 2007, the National Radiotherapy Advisory Group stated that the recommended travel time to/from a radiotherapy centre should be no more than 45 minutes. 17 Recent analysis, based on travel times to a 1 pm appointment when driving a private car, found that 7.4 million people in the UK are more than 45 minutes from their closest radiotherapy centre, and 2.4 million are more than 1 hour away. Reference Purden, Jackson and Lewis7,18 When taking public transport to a radiotherapy appointment at 1 pm, the number of people more than 45 minutes away is 49.6 million, and those more than 1 hour from a centre are 39.9 million. 19 The analysis highlights geographical areas across the UK where access to radiotherapy is extremely limited, especially for those reliant on public transport. In Wales, the Cameron Report (1996) recommends a travel time of 60 minutes to access therapy, given the country’s varied physical, population and health service distributions. Reference Cameron20
These systemic differences translate into uneven patient experiences and outcomes. Patients in South-West Wales may have more complex journeys or need to attend multiple hospitals as part of their care, compared to those near more centralised services. In practice, this means a breast cancer patient’s access to treatment and support services, such as psychological counselling or educational sessions, may depend on where they live.
This study aims to examine whether distance from SWWCC influences access to, or timing of, breast cancer radiotherapy and how service developments have mitigated geographic inequity.
Methods
Retrospective data were extracted from the institutional MOSAIQ (Elekta AB, Stockholm, Sweden) oncology information system using custom Python code (Python 3.12, pyodbc, pandas). A secure Structured Query Language connection was established to the MOSAIQ database, and multiple queries were executed to obtain clinical, planning and scheduling information for patients treated for breast cancer since 2017. These data were integrated into a hierarchical structure linking each patient to their associated treatment sites, fields and fraction deliveries.
Quality Checklist (QCL) data, encompassing completed tasks relevant to breast radiotherapy (e.g., Computed Tomography (CT) simulation, plan approval and plan checking), were grouped into temporal ‘sessions’ based on task timestamps. All retrieved information was consolidated into a nested Python dictionary indexed by patient identifier and subsequently flattened into a structured tabular dataset containing demographic, diagnostic, treatment and scheduling fields. The final dataset was exported in Microsoft Excel format for downstream analysis of the time between key steps in the pathway.
Travel distances and times were calculated using RTInsight, a Python-based geospatial analysis tool developed at SWWCC and used to support business cases. Patient postcodes were geocoded using the Ordnance Survey Code-Point Open dataset, 21 providing high-precision spatial coordinates, which were then converted to latitude and longitude using the WGS84 reference system for routing compatibility. These coordinates were used to model travel to SWWCC under different transport scenarios. Driving distances and times were calculated using a locally deployed openrouteservice engine, drawing on OpenStreetMap road network data to reflect real-world routing, road topology and speed limits and modelling travel at 13:30 on a Wednesday. 22,23 RTInsight calculates network-based driving distance rather than straight-line distance, which is particularly important in the rural and geographically complex road networks of South-West Wales. To validate RTInsight, estimated travel times were compared with those generated by Google Maps, used as an established commercial benchmark. Random pairs of Welsh postcodes were processed by RTInsight and manually entered into Google Maps for comparison. A Wilcoxon signed-rank test showed no statistically significant difference between the two methods (W = 1,736, n = 100, p = .12). In addition, RTInsight’s data handling and analytical pipeline are routinely verified using an automated test suite implemented with the pytest framework.
Patients were categorised based on transport type, travel time to the department (≤/>60 minutes) and treatment prescription.
Statistical Analysis
2,286 patients attending SWWCC for breast cancer radiotherapy between January 1st, 2018, and December 31st, 2023, were studied. Statistical analyses were performed using IBM SPSS Statistics version 30.0.0.0(15). Per the assumptions of the statistical tests, outliers in the data were identified by inspecting a boxplot for values more than 1.5 box lengths from the box edges. Outliers were scrutinised and removed from the analysis if indicated, e.g., if the patient’s postcode on MOSAIQ had changed since their treatment, indicating they had moved away. Levene’s test for equality of variances was used to assess homogeneity of variances, and Shapiro-Wilk’s test was used to determine the distribution of the data for the time between booking and delivery of the first fraction. A Kruskal-Wallis H test,
Reference Kruskal and Wallis24,25
and tests of its assumptions were performed to determine if there were statistically significant differences between groups, and Fisher’s exact test, with post hoc analysis involving pairwise comparisons using multiple Fisher’s exact tests (2
 $ \times \;$
2) with a Bonferroni correction, was used to assess differences in proportions between individual groups.
$ \times \;$
2) with a Bonferroni correction, was used to assess differences in proportions between individual groups.
Results
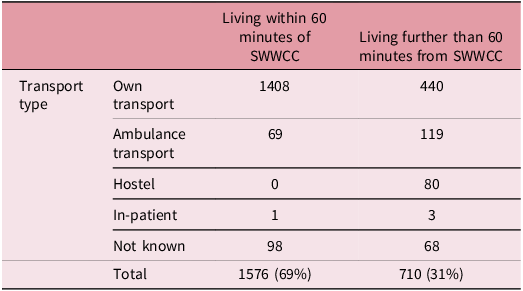
Descriptive statistics indicate that, among patients living more than 60 minutes from the hospital, 11.3% required a hostel for treatment, compared with 0% among those living within 60 minutes of the hospital. 16.8% of patients living outside the recommended travel area required outpatient ambulance transport, compared with just 4.4% within it. 62% of patients living outside the recommended travel area travelled independently, compared with 89.3% of those living within it. These are statistically significant differences in proportions, as assessed by Fisher’s exact test, p < .001. A statistically significant difference existed between the five independent binomial proportions (p < .001). All pairwise comparisons were statistically significant, indicating that patients’ methods of travel are influenced by how far they live from the department.
A Kruskal-Wallis test was conducted to determine whether there were differences in the timing of patient arrival for treatment between four groups of participants with different levels of travel independence: the ‘In Patient’, ‘Hostel Required’, ‘Ambulance Transport’ and ‘Own Transport’ patient groups. Distributions of arrival times were not similar for all groups, as assessed by visual inspection of a boxplot. Statistically significant differences were found between the different levels of travel independence, χ2(3) = 21.214, p < .001. Subsequently, pairwise comparisons were performed using Dunn’s procedure with a Bonferroni correction for multiple comparisons. Reference Dunn26 Adjusted p-values are presented. This post hoc analysis revealed statistically significant differences in arrival time between the Ambulance Transport (mean rank = 43.17) and Own Transport (mean rank = 32.41) (p < .001) groups, but not between any other group combination.
A Kruskal-Wallis H test was run to determine whether there were differences in time between booking and delivery of the first fraction between groups living within the 60-minute recommended travel time and those living farther. There was homogeneity of variances for patients’ wait between booking and delivery of the first fraction of treatment, as assessed by Levene’s test for equality of variances (p = .087), but the data were not normally distributed for each group, as assessed by Shapiro-Wilk’s test (p < .001). Median scores were not statistically significantly different between groups, p = .676.
Figure 3 visualises the 10-patient moving average of time from booking date to delivery of the first fraction for each prescription and treatment complexity. A large degree of variability is seen in 2018, with a small spike in early 2020, after which all active prescriptions converge to a 20–30 day wait.
Point density map, depicting SWWCC (H) radiotherapy patients’ postcode locations, 2018–2023. Map data from OpenStreetMap https://www.openstreetmap.org/copyright.

Time from booking date to delivery of 1st fraction, by prescription (10-patient moving average).

This reduction in waiting time between booking and delivery of the first fraction is correlated with a decrease in time between the 3D CT and the physics team completing the plan check, which has also decreased from an average of 27 days in early 2018 to <10 days by the end of 2023 (Figure 4).
Time from 3DCT to Phys Plan Checking Complete.

Discussion
There were no statistically significant differences in booking-to-treatment time between patients living locally to the treatment centre and those living more than 1 hour away. Overall booking-to-treatment time shrank by more than 50%, from ∼60 days to ∼20–25 days (Figure 3). Despite a wide geographical spread (Figure 2), the health board achieved equitable timeliness of care.
The data show that patients’ travel modality choices differed significantly by distance (Table 1). Patients residing more than one hour away were more likely to use the free non-emergency patient transport service, whereas those living locally predominantly travelled independently by car or public transport. Patients travelling independently face different travel burdens, including fuel and parking costs and the stress of timely navigation. Differences in transport modality highlight how geographic factors continue to shape the patient experience, with those travelling greater distances facing longer, less predictable treatment days. Notably, however, this travel-mode disparity did not translate into delays.
Patient travel type, by distance from SWWCC, for breast cancer radiotherapy patients 2018–2023

There was a statistically significant difference in arrival times between patients travelling independently and those travelling via non-emergency ambulance transport. This was expected, as there are usually two collection windows for non-emergency ambulance patients, at 8:30 am and 12:00 pm. When patients arrive via non-emergency ambulance for their radiotherapy, the department generally treats patients as soon as they arrive, rather than strictly within their scheduled treatment slot.
Substantial improvements in radiotherapy workflow were observed over the 6 years of study data: the time from CT simulation to completion of the physics team’s plan check fell from an average of 27 days in early 2018 to <10 days by the end of 2023 (Figure 4). These improvements coincide with streamlined pathways, dosimetrist plan approval and the adoption of hypofractionated regimens.
The accelerated uptake of 5-fraction (5#) breast radiotherapy has been central to patient and service capacity improvements. National guidance (NICE NG101) and RCR consensus now endorse 26 Gy in 5# over 1 week for most whole-breast cases. 8 This change has dramatically cut the number of hospital visits for many patients. The data suggest that each eligible patient saves roughly 20 one-way hospital trips under a 5# regime. Reference Purden, Jackson and Tales27 Fewer visits reduce travel time, costs and disruption to daily life. The National Institute for Health and Care Excellence (NICE) notes that shorter courses are ‘more convenient for patients’ and improve adherence and equality of access. 8 Locally, use of the patient hostel fell from 55 patients in 2018–2019 to only 8 in 2020–2021, with a slight rebound to 17 in 2022–2023. The pandemic partly drove this, due to infection-control restrictions on lodging and patients spending less time in the hospital each day for treatment, Reference Purden, Etheridge and Rose28 but the shift to 5# schedules also meant fewer patients required overnight stays near the hospital. For many rural patients, a one-week course meant they could travel from home each day instead of lodging. This suggests that treatment length is important for patient decision-making about travel and accommodation.
These efficiency and pathway changes have cost implications; reduced hostel occupancy and fewer fraction deliveries should lower NHS costs and reduce travel-related carbon emissions. Reference Purden, Jackson and Tales27 Streamlined planning and shorter regimens likely save staff time and equipment utilisation, freeing treatment machine capacity, but it should be noted that there are additional complexity costs associated with planning and delivery of 5# regimes: there is an increased demand on CT, more outlining may be required, online imaging is needed and takes longer, and there may also be slot length increases. Attention must be paid to ensure that efficiencies do not exacerbate inequalities. For instance, rural patients on limited incomes might disproportionately favour shorter treatments to minimise travel, a dynamic flagged by NICE as a potential ‘unintended consequence’. 8
Geographic inequity also affects access to optional supportive services such as the SWWCC radiotherapy open evening, which aims to improve patients’ understanding of their treatment and reduce anxiety by familiarising patients with the treatment environment. Patients living further away may be less likely to attend due to travel burden, particularly when the perceived benefit is supplementary. To address this, SWWCC introduced an online option that allows remote participation and some prerecorded content 29 ; however, virtual participation limits physical familiarity with treatment areas. Further, sessions are held monthly, meaning many patients will miss them altogether. This highlights both the potential and limitations of digital solutions in addressing geographic disparities in supportive care provision.
This retrospective, single-centre study uses routinely collected data and may not be fully generalisable to regions with different service configurations, workforce capacity or population characteristics. Its design limits control over data completeness and prevents the capture of key socioeconomic factors, such as deprivation, employment, transport access and caring responsibilities, that influence access to care. Reference McMaughan, Oloruntoba and Smith30 Measures of travel burden may underestimate patients’ lived experiences, as factors such as public transport availability, appointment timing, treatment frequency, physical fitness and reliance on informal support were not captured. In addition, residential location was derived from MOSAIQ records, which are updated if a patient moves after treatment; as a result, some patients may appear to live outside recommended travel time thresholds despite having lived closer at the time of treatment and vice versa.
Conclusion
Overall, these findings highlight a complex landscape: systemic improvements have reduced waiting times and enhanced efficiency, while changes in clinical practice, particularly the adoption of hypofractionated regimens, have eased some of the burden of travel. The data suggests that, no matter where you live in South-West Wales, patients have the same access to care, dispelling some concerns about a potential postcode lottery. However, inequities persist in the daily treatment experience, with patients dependent on hospital transport still experiencing less autonomy and greater disruption. This disparity illustrates that the postcode lottery in radiotherapy is not solely about waiting-time inequities but also about the lived experience of treatment. Addressing this residual disparity will require maintaining efficiency gains and improving patient-centred transport solutions and support for those living furthest from care.
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare none.





 Open access
Open access