

Background
Community-engaged research (CEnR) is increasingly recognized as a critical component of effective clinical and translational science, particularly for improving the relevance, equity, and impact of research conducted at academic medical centers [Reference Eder, Evans and Funes1–Reference Martinez, Russell, Rubin, Leslie and Brugge3]. By fostering bi-directional partnerships between academic institutions and the communities that they serve, CEnR supports translational goals such as improved uptake of evidence, responsiveness to community priorities, and reductions in health disparities, grounded in the principles of community-based participatory research [Reference Wallerstein, Duran, Oetzel and Minkler4, Reference Carney, Maltby, Mackin and Maksym5]. Despite this recognition, many academic health centers continue to face challenges in systematically supporting and sustaining CEnR.
Prior studies have documented persistent institutional barriers including misaligned incentive structures, limited administrative flexibility, inadequate financial mechanisms to support community partners, and variability in leadership support [Reference Selker and Wilkins2, Reference Carter-Edwards, Grewe and Fair6, Reference Drahota, Meza and Brikho7]. These challenges reflect the fact that CEnR represents a shift from traditional, investigator-driven research models towards partnership-based approaches that requires different organizational competencies, policies, and workflows. As a result, existing institutional infrastructures may be insufficiently equipped to support CEnR.
Recent scholarship has advanced the science of community engagement by centering on community partner perspectives [Reference Bustos, Simkani and Reichel8], emphasizing process of co-creation [Reference Pérez Jolles, Willging and Stadnick9], shared power [Reference Popay, Whitehead, Ponsford, Egan and Mead10], reflexivity [Reference Finlay and Gough11], and collective empowerment [Reference Burns12,Reference Oetzel, Boursaw and Magarati13] as central to community-academic partnerships producing meaningful research outcomes. This literature, situated largely at the partnership or the project level, has been instrumental in articulating how engagement processes contribute to trust and relevance in CEnR. At the same time, these partnership processes do not occur in isolation; they are influenced by institutional environment that can either enable or constrain their enactment [Reference Wallerstein, Oetzel and Sanchez-Youngman14]. There is also a need to examine the roles of community outreach and engagement offices/centers, supported in recent years through Clinical and Translational Science Centers [Reference Eder, Evans and Funes1] and Cancer Centers [Reference Paskett and Hiatt15] with goals to engage communities served by the academic medical centers, disseminate research activities, and conduct outreach and education for the community. Building on the strong foundation in community engagement science, we highlight the critical need for an institutional understanding of the assets and opportunities to support CEnR. Much of the existing literature, however, has examined these barriers from a single interest holder perspective or has relied on qualitative or quantitative methods alone which limits the ability to fully characterize institutional context and identify actionable opportunities for improvements meaningful to both academic and community partners.
Supported by the Patient Centered Outcomes Research Institute (PCORI) Engagement Award, we previously tested the feasibility of a data-driven, partnership-engaged, Engage for Equity PLUS (E2PLUS) intervention to understand and enhance institutional internal capacity to support CEnR, strengthen internal and external structures and processes to enhance institutional commitment to health equity through joint patient and community decision-making, and shared governance in research [Reference Sanchez-Youngman, Adsul and Gonzales16].
In this paper, we present a mixed-methods approach to integrate measurable institutional conditions with partner experiences. Using a sequential exploratory mixed-methods design, this study examined institutional support for CEnR across three geographic sites of an academic medical center. The qualitative research objective was to explore how academic investigators, institutional staff, and community partners perceive and experience institutional structures, policies, processes, and relational dynamics that influence CEnR. The quantitative objective was to assess across a broader sample of academic and community partners the perceptions of institutional commitment, trustworthiness, leadership support, policies, and infrastructure for CENR, informed by domains identified in the qualitative phase. The mixed-methods objective was to identify areas of convergence and divergence between academic and community perspectives, deepen understanding of site-specific institutional context, and inform actionable strategies to strengthen institutional support for CEnR within academic medical centers.
Materials and methods
Study design
This was a sequential exploratory mixed-methods study design for a pragmatic inquiry into the context of the academic medical center in order to identify strategies that can support institutional learning and translation impact [Reference Creswell and Creswell17]. In the first phase, we collected qualitative data through interviews with institutional academic leaders, community-engaged researchers and staff from community-facing offices, and focus groups with community members. In the second phase, we used the qualitative data to inform the adaptation of a quantitative data collection instrument [Reference Dickson, Kuhlemeier and Adsul18], using an online REDCap survey of academic and community members. Qualitative findings were used to refine survey domains, ensure contextual relevance, and incorporate community and academic partner-identified priorities related to the institutional and operational support for CEnR. Quantitative survey data were subsequently used to examine the distribution of perceptions identified qualitatively and to assess differences between academic and community respondents. Integration occurred at multiple points: during survey development, through comparison of qualitative themes and quantitative patterns, and interpretation of findings to generate institutional-level recommendations.
Theoretical framework
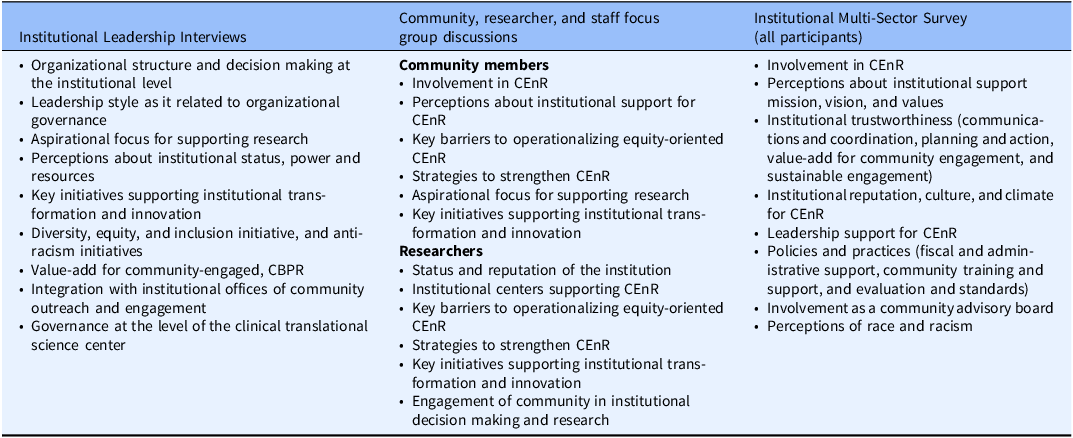
The institutional assessment was informed by an aggregation of constructs from two key frameworks: the CBPR model [Reference Belone, Lucero and Duran19] and the Assessing Community Engagement Model by the National Academies of Science, Engineering, and Medicine [Reference Aguilar-Gaxiola, Ahmed and Anise20]. In addition, the assessment was guided by an in-depth understanding of contextual assessments common in the implementation science literature and often included in its theories, models and frameworks [Reference Nilsen and Bernhardsson21]. Detailed information about the underlying theoretical framework is presented elsewhere [Reference Adsul, Sanchez-Youngman and Dickson22]. Together, these frameworks informed the development of the qualitative data collection instruments with specified domains outlined in Table 1. The qualitative findings then supported the adaptation of a published institutional survey [Reference Dickson, Kuhlemeier and Adsul18] that was refined for this project.
Domains of inquiry for the qualitative and quantitative data

Participant recruitment and data collection
The research team from University of New Mexico (UNM) led the design and development of the data collection instruments with leaders from the institutional Clinical and Translational Science Award center, which operates in three geographically distinct sites in the United States. Together the UNM team and the CTSA leaders formed a core champion team that also included community members, researchers, and staff. The champion team collectively served in an advisory role to the data collection protocols as well as throughout the data interpretation phase. All data collection instruments (i.e., interview guides, focus group discussion guides, and survey) were adapted from prior work on barriers and facilitators embedded in institutional contexts to be more congruent with this academic medical center and the evaluation goals [Reference Dickson, Kuhlemeier and Adsul18,Reference Adsul, Sanchez-Youngman and Dickson22]. In addition, we added 20 items that were generated from the Principles of Trustworthiness put forth by the American Association of Medical Colleges, Center for Health Justice.[23] While data collection was led by the UNM team, the champion team led the participant recruitment based on existing relationships with senior leadership, community-engaged researchers, staff from community-facing offices, and community partners from institutional advisory boards and from CEnR partnerships. Study protocol and all data collection instruments were approved by the institutional review boards of the University of New Mexico Health Sciences Center and the academic medical center.
Data were collected from August through October 2023. Interviews and focus groups were conducted both in-person and on video-conferencing platforms. We conducted in-depth interviews with academic leaders, researchers, and staff (n = 54) and focus groups’ discussions (N = 4) with community members (n = 33). Using rapid analytic approaches, the themes from these qualitative data informed the adaptation of the institutional survey which was administered through REDCap [Reference Harris, Taylor, Thielke, Payne, Gonzalez and Conde24]. Survey invitations were sent to 175 leaders, investigators, and community partners affiliated (i.e., those serving on institutional advisory boards or engaged in a CEnR partnership) with the academic medical center. A total of five rounds of invitations were sent between September 20, 2023, and October 6, 2023. We received 85 responses, for a response rate of 49%. Community participants received an electronic gift card for participation whereas academic participants were not remunerated.
Data analyses
We conducted rapid qualitative analysis [Reference Hamilton and Finley25] on the qualitative data from 87 people affiliated with the academic medical center that were collected through leadership interviews, researcher, staff, and community focus groups. Following interviews and focus groups at each of the three sites, trained members of the research team (PA, AK, NW) generated analytic memos that synthesized key points related to theory-informed domains, documented emergent insights, and captured illustrative quotations. To enhance analytic rigor, participatory sense-making discussions were held with additional members of the academic health center team (IS, MLW) to compare interpretations and resolve differences through consensus. Findings from the qualitative phase were used to adapt and refine the institutional survey instrument. All individuals consenting to the survey were included in the analysis. Descriptive statistics were calculated for all survey items, including frequencies for Likert-type responses, stratified by community versus academic respondents. Group differences in response distributions were examined using Mann–Whitney U tests, excluding missing and “don’t know” responses. To facilitate interpretability, we present z-statistics for significance tests. A negative z-statistic indicates that the ranked sum for community members was higher than that of institutional members. Positive z-scores, on the other hand, indicate higher ranked sums among institutional participants. Depending on the response options for each question, higher values for each item is either associated with a higher level of agreement (e.g., “Strongly Agree”) or frequency (e.g., “Always”). Following survey data analyses, qualitative data were revisited to examine how interview and focus group findings explained or contextualized. This interpretive return to the data supported the mixed methods integration during the interpretation phase.
Results
Findings from the interviews and focus groups
Theme 1: Establishing a linkage between clinical care and research
“[The institution] does have a good reputation, and most people feel like physicians know what they are doing” which people said helps with cross-institutional collaborations and trust in clinical care, though many community members suggested the need for the institution to still invest more in relationships with organizations so that uninsured patients can receive high-quality care, which would also impact the support for research.
Data from researchers and staff indicate that the institution doesn’t yet see CEnR as a part of the “continuum of care” for what is delivered in the clinic. According to community members, it is important to invest not just in research but, “in its people so that people can see that [the institution] will honor the community and not just go get blood [for the research]” – (Community member) Staff relayed anecdotes of conversations with individuals recruited into research studies who perceive that they did not have access to the clinical practice: “I’m good enough for research, but not good enough for care” (Staff member) These clinical barriers have made recruiting for research more difficult.
In leadership interviews, several leaders mentioned that the institution differentiates itself from other academic health centers in that, “we really view research and discovery as way to improve patient care.” Many interviewees brought up the fact that it is a physician-led organization, operating like “a tricycle with clinical care being the big front wheel, supported by research and education.” To integrate into the Clinic, there is a need to examine the intersection of CEnR with the concept of a “learning healthcare system” where community engagement and health equity research can play an important role in addressing the main focus of unmet patient needs as described by a leader below,
We also talk about the needs of the patient come first. That’s our primary values. That’s what roots us. When we think about research, we think about unmet patient needs. (Institutional Leader)
Theme 2: Leveraging the institutional reputation in the community
Many community members stated that the institution has to balance the needs of patients seeking care from around the world and the needs of communities in the institution’s back yard: “There is still a lot of mistrust in healthcare.” (community member). “There’s two perspectives, there is the [institutional] perspective and the community health perspective, and they are too far apart” said a community member, encouraging the institution’s approach to the community to be less transactional. They also encourage the clinic to invest in continuous engagement with community organizations that have been working hard to build trust in the community.
Many researchers and leaders in the institution agreed with the community members perceptions that, “The main thrust of [the institution] is serious and complex disease” and “Our DNA is still in serious and complex care.” Several staff members mentioned that there is a lot of “brand name” trust that the [institution] generates in the community, “If you google anything about medicine, [the institution] pops up first.” Some researchers indicated that this focus on complexity sometimes makes it difficult to collaborate with local communities on research and practice priorities. One leader said, “If [the institution] leads, others will follow” while another mentioned “If anyone can figure out how to make sure people have access to care, it’s [the institution]” – (Institutional Leader).
Theme 3: Going beyond community engagement as a grant mandate
Many community members questioned, “How much is the institution genuinely interested in community participation and how much of it is done simply to check a box?” Several thought that the community engagement activities were happening because it is required of them through federal grants. Community members perceived that the institution is not always prepared to support CEnR and were not sure that the work is being “translated to a larger institutional policy and really being institutionalized in ways that can be felt outside research.” Authentic and meaningful approach to CEnR would mean that the institution invests in building community capacity through research outcomes and provide sustainable solutions through CEnR. They also encouraged, genuine and authentic interactions including “breaking bread with the community,” showing up in-person and “looking people in the eye” which was hard to do online, although many community members also supported hybrid approaches. Community members shared that researchers who have a passion for a certain field are important, but other times it would be great for them to look at ways in which they could address community priorities; often it seemed that “[the institution] is not asking what new research should be done.” (Community member).
For authentic engagement, some researchers suggested that the institution should create space for the community to define their needs and assets and generate a sustained presence in the community after the research is over through newsletters and communications. Leadership agreed that community engagement was a key priority for federal research which meant that these activities were happening across the institution, but they also acknowledged that “it was typical of the institution to have all these activities siloed and not coordinated in a larger effort… “where is the front door?” Some leaders acknowledged that CEnR was a “field in itself” and they had to learn a lot; most investigators “don’t really understand the field, and so they bring on someone else, and they don’t understand it either” acknowledging that there was a lot to learn about CEnR. One leader acknowledged the need to move beyond the grants, as stated below:
We like grants…but it is instantly wrong for me to say, ‘well, this is what [federal grants] require, therefore this is what we should do’ and really that’s not what we should be doing at all… We should align when we can but we should be driven by what [the institution] …is well-suited to do. If that aligns with [federal grants], fine. If it doesn’t, we are going to have to figure out how to do both and keep our grants. (Institutional Leader)
Theme 4: Addressing complexity around health equity in CEnR
Addressing the complexity around promoting health equity and prioritizing community is “more than any one health system can do” given the mistrust and fear in the community which would require a “360-degree approach” according to community member participants. Addressing community priorities requires an awareness of “issues of trust and communication and transparency” which is lacking when community engagement is conducted “in a very superficial manner for research” Community members mentioned that CEnR investigators have “to meet the community where the community is” and be transparent with what you want from the community; they also need to develop communication skills and “a humility that needs to be embedded in the process” of community engagement, further elucidating the complexity.
Several researchers pointed out that conducting CEnR requires a lot more intentionality and effort than other research approaches. There is a need to address historical tensions in the community, rebuilding trust, and yet this doesn’t support their promotion and tenure, as noted by an investigator below,
So the entire structure down to even how we are rated in performance of our job does not align with community-based research. It’s a heavy emphasis on timelines for basic scientists to get things out, which is typically faster than it takes people like us who have to build these relationships in the community. It becomes even more challenging when there have been some historic circumstances that have caused tension with us in the community, and we have to now go back in and try to rebuild that structure. [Investigator]
Per one investigator, “there is nothing more complex…than social determinants of health in the context of chronic disease,” while mentioning the opportunity for the institution to leverage its reputation in the community and expertise towards community health. Leadership perceived the complexity around health equity research in relation to social determinants of health by noting the need to address the research to practice gap, which would require coordination with other community-based organizations. One leader noted the need to encourage scientists to undertake research that “allows you to change paradigms vs research that is there to confirm what most of us already knew, 20 years ago.”
Theme 5: Institutionalized prioritization and support for CEnR
Community members noted that there are many investigators driven by genuine interest in the community, but the “institution as a whole is driven by other factors.” Many community members noted themselves to be, “trusted messengers for the community” which is a reputation that has taken them years to build in the community and they needed to see institutional investment in CEnR outside of waiting for NIH funding. “You can’t do lip service to community engagement;” community members said it needed to be “central, until every department must look at itself and say, “How are we involved in the community? What are we doing to improve health outcomes of the minority populations in the community?” They encouraged the institution to “take risks and invest where it matters” for more impactful change and sustainable community solutions that showcase their intentions. Although, many noted that changing for organizations can be hard, “we as humans, don’t do it naturally, so how would a big organization do it naturally?”
Researchers mentioned primarily relying on their own grant success to convince leadership of the value of CEnR. They suggested that institutionalization of CEnR is possible by giving voice and infrastructure support to the investigators leading this work, including sustained fiscal support for ongoing partnerships between funding cycles and addressing internal structural barriers (IRB approvals, mechanics of compensation for community partners, etc.) to reduce impact on fragile relationships in the community for researchers.
Leaders described challenges in aggregating a common vision for CEnR across the three national sites. They mentioned the need for interagency coordination and communications to strengthen community engagement and, most importantly, to scale it across sites. Some mentioned that not all leaders understood community engagement and that “community engagement kind of needs to be one voice.” Many described the importance of structures such as the advisory boards, Community Engagement Studios, and the central offices for Community Engagement at the Cancer Center and the Clinical Translations Science Center. However, they also cautioned against over-reliance on these structures, mentioning the need for infrastructure investment to bolster the workforce with individuals that understand what it takes to engage, recruit, and retain participants since community engagement and CEnR is “joined at the hip,” according to a researcher.
Findings from the institutional survey
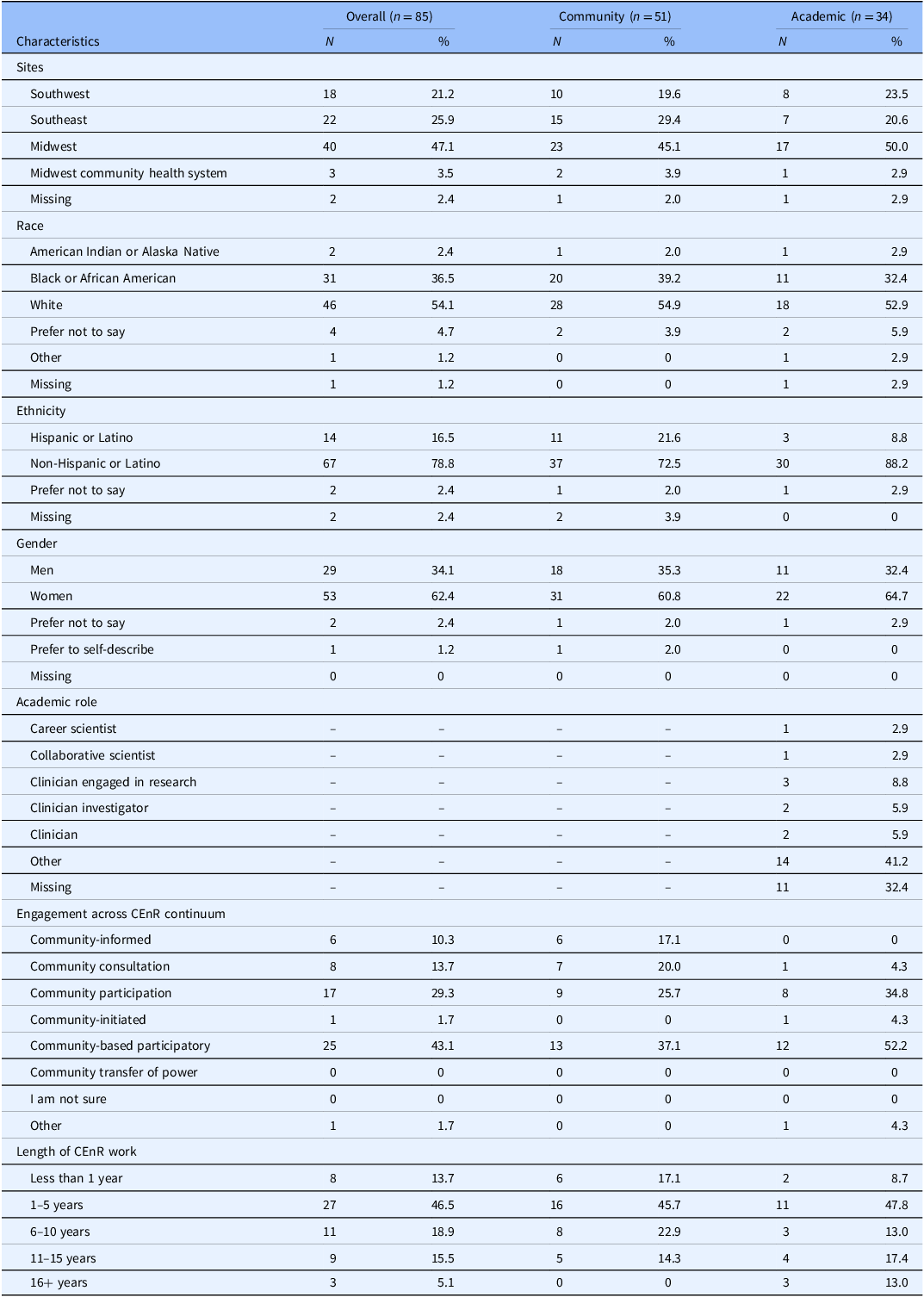
Of the 85 people who responded to the survey, 60% identified as members of communities that interacted with the institution, and 40% were members of the institution. Nearly half of respondents (43.1%) identified themselves as being involved in CBPR and having 1–5 years of experience in CEnR (46.5%). Detailed sample demographic information is presented in Table 2. Tables 3, 4, 5, and 6 provide descriptive statistics for the survey, including the results of Mann Whitney U tests to assess significant differences in response distributions between community and institutional members. Select findings that expand on the qualitative findings are summarized here.
Demographic characteristics of the multi-sector survey respondents

Mission, vision, and values for the institution

Institutional trustworthiness

Institutional reputation, culture, and climate for community-engaged research

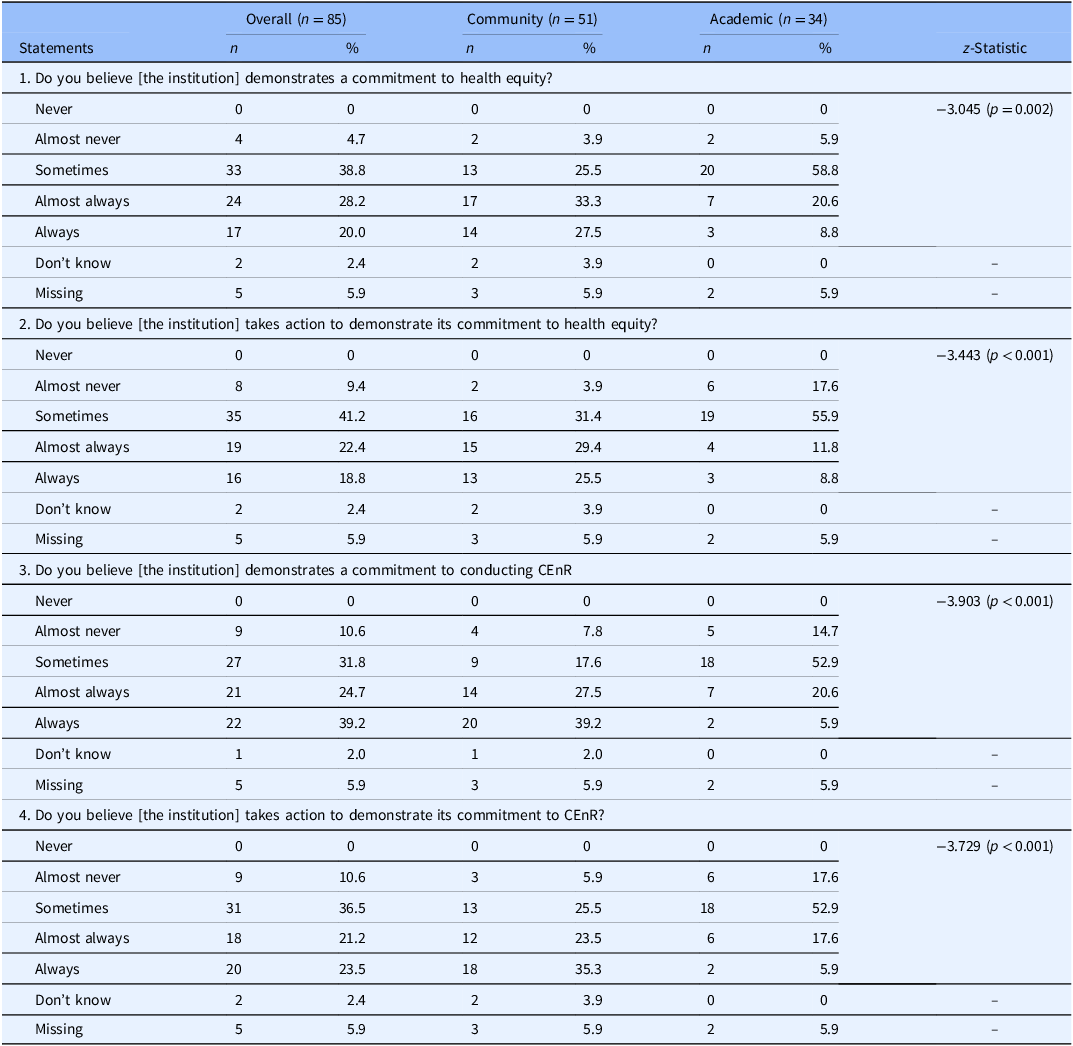
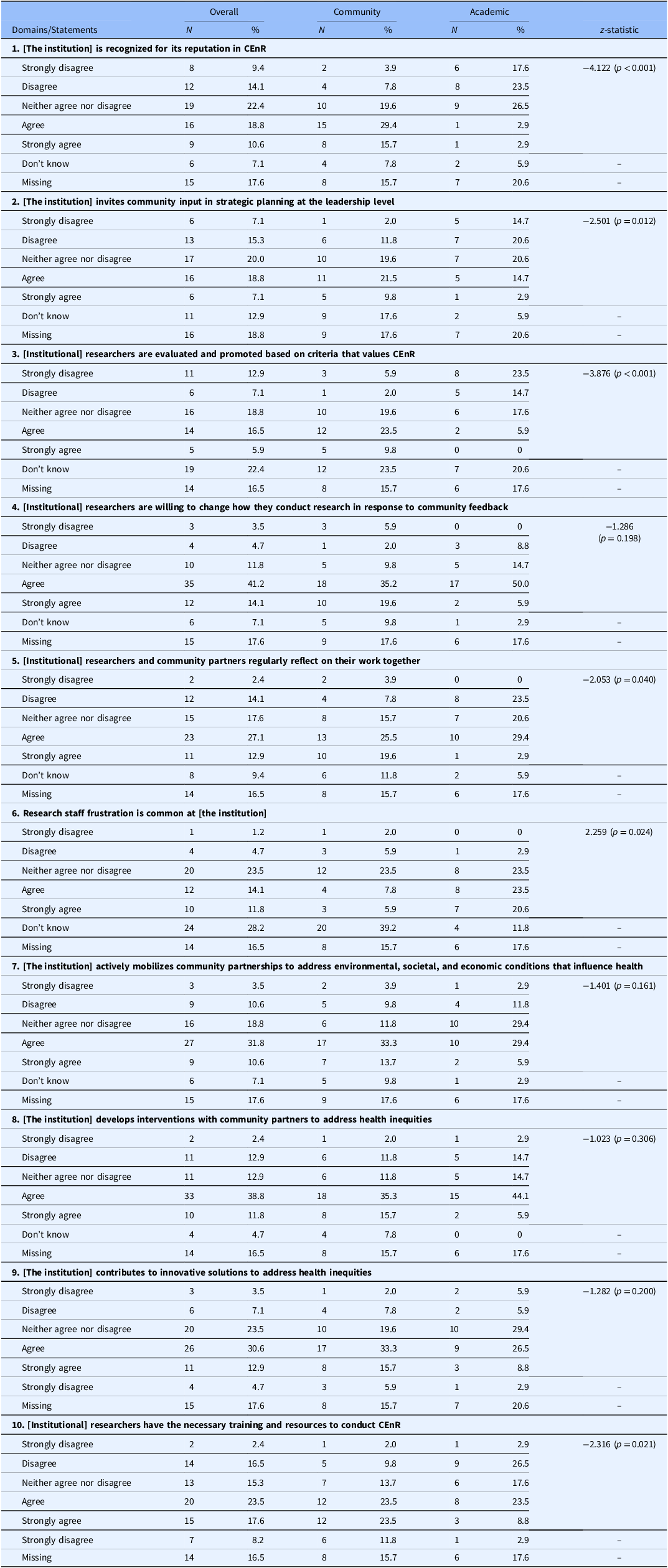
When asked about the institution’s commitment to health equity and CEnR, most respondents acknowledged the institution’s stated commitment for both health equity and CEnR. The discrepancy apparent between participants’ perception of the institution’s stated commitment to health equity (48.2% rated always or almost always; Table 3, Q1) and their action to demonstrate this commitment (41.2% rated always or almost always; Table 3, Q2) underscores the theme that emerged from the qualitative data regarding the complexity associated with addressing social determinants of health and promoting health equity. While community members were more likely than institutional respondents to perceive that these commitments were demonstrated in practice, institutional respondents may be more attuned to the challenges of translating aspirational values into actionable institutional strategies.
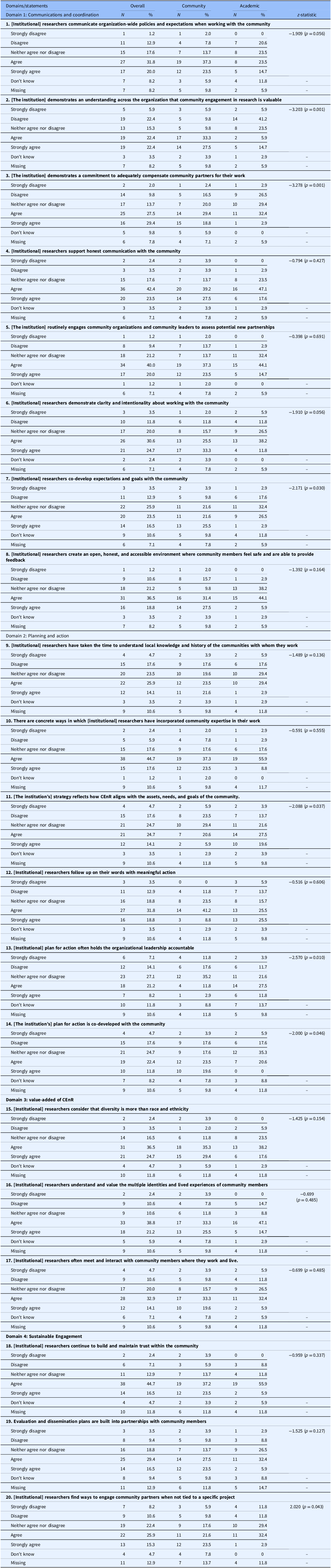
Institutional trustworthiness was assessed across four subdomains: communication practices, planning and action strategies, value assigned to community perspectives, and efforts to promote sustainable engagement. Items separately assessed perceptions of the trustworthiness of researchers and the trustworthiness of the institution, more broadly. Less than half of respondents (44.8%; Table 4, Q2) agreed or strongly agreed that the institution communicates the value of community engagement in research across the organization, and only one third (34.2%; Table 4, Q7) agreed or strongly agreed that the institution’s plan for action is co-developed with community members. Across these domains, institutional respondents expressed significantly greater skepticism than community members, echoing qualitative findings that emphasized the need for authentic and co-created engagement beyond grant-driven requirements.
In contrast, perceptions of individual researchers were consistently more favorable. Nearly two-thirds (65.9%; Table 4, Q4) of respondents agreed or strongly agreed that researchers support honest communication with the communities and over half (55.3%; Table 4, Q8) agreed or strongly agreed that researchers create an open, honest, and accessible environment where community members feel safe and able to provide feedback. These findings underscore the need to take a multifaceted focus on the institution’s reputation in the community, suggesting that institutional reputation is shaped not only by clinical excellence but also by individual clinicians’ and researchers’ commitment and embodiment of the institution’s mission, vision, and value with the way that they conduct themselves inside and outside the institution.
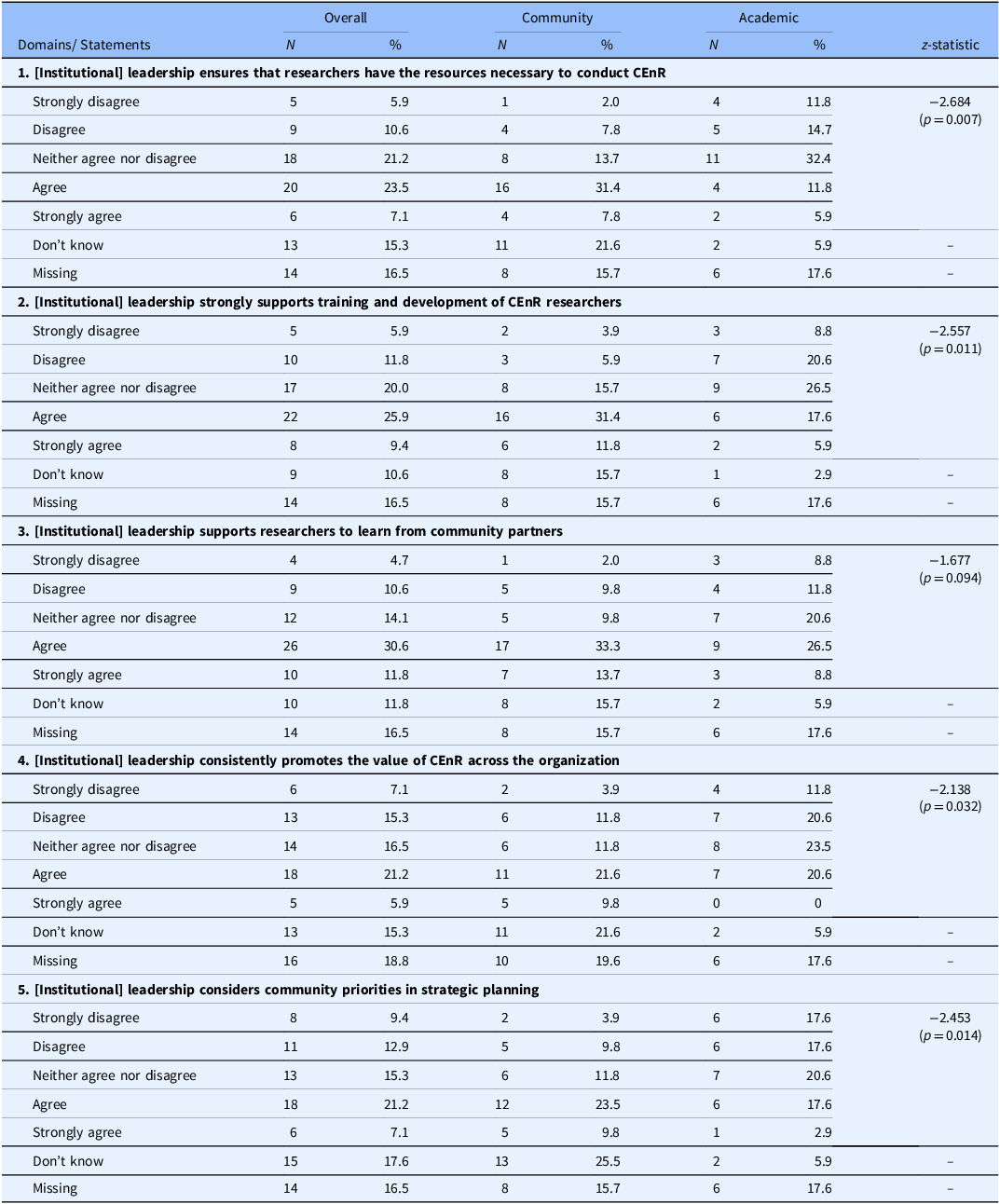
Finally, institution-based respondents were less likely than community-based respondents to perceive institutional leaders’ support for CEnR (17.7% of researchers compared to 39.2% community members; Table 6, Q1) or incorporates community priorities into strategic planning (20.5% of researchers compared to 33.3% community members; Table 6, Q5). Overall, community members perceived stronger institutional support for CEnR than did those working within the institution, underscoring knowledge about persistent internal constraints on prioritizing and sustaining engagement.
Perceptions of leadership engagement

Integration to generate actionable recommendations
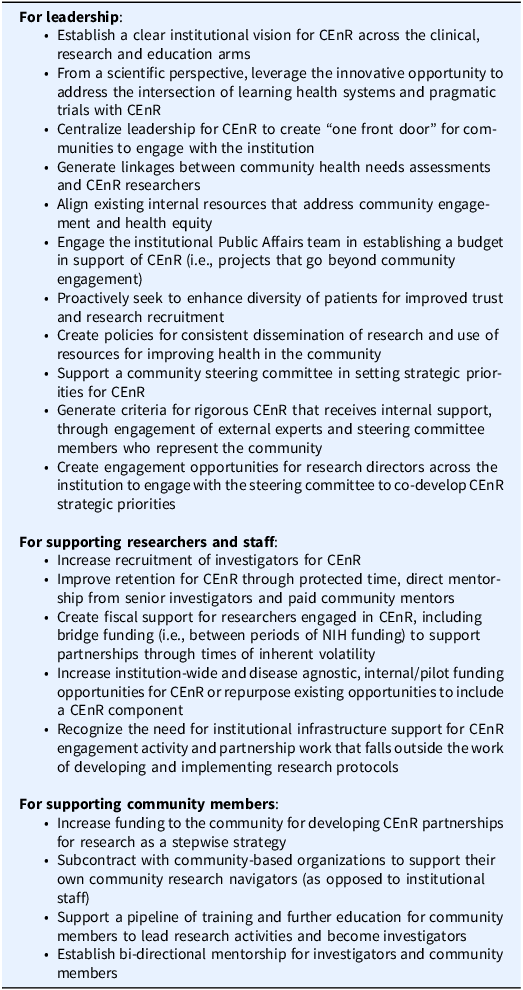
Qualitative and quantitative data were integrated at multiple points during survey development, through comparison of qualitative themes and quantitative patterns and interpretation of findings to generate institutional-level recommendations for institutional leadership, researchers and their staff, and community members. In collaboration with the institutional team, recommendations were grounded in partner experiences with the goal to identify pragmatic and contextually informed strategies to strengthen institutional capacity.
A consolidated recommendation for leaders was to establish and strengthen a clear institutional vision for CEnR through building a “learning health system” across all clinical, educational, and research arms. A concrete recommendation was for the leaders to centralize CEnR by creating “one front door” for communities to engage with investigators. For researchers and their staff, recommendations were to increase recruitment and retention of investigators for CEnR through protected time, bridge and pilot funding, and mentorship. Recommendations for communities were to increase funding for partnerships and for community-based organizations for their navigation staff as well as to support training for community members to lead research activities (see Table 7 for all recommendations).
Actionable recommendations for supporting community-engaged research at the institution

Discussion
This study presents findings from an evaluation of institutional support for CEnR at a multi-site academic medical center, with implications for other large, complex academic health systems. Building on prior scholarship [Reference Bustos, Simkani and Reichel8–Reference Burns12] that has largely examined CEnR at the partnership levels, this study shifts the analytic focus upstream to examine institutional conditions that shape whether such partnerships can be sustained in academic medical centers [Reference Sanchez-Youngman, Adsul and Gonzales16,Reference Dickson, Kuhlemeier and Adsul18,Reference Adsul, Sanchez-Youngman and Dickson22]. This mixed-methods study designed to capture perspectives from both community and academics and leaders expands the literature around translational sciences and community engagement infrastructure and describes how academic medical center structures, policies, and practices support CEnR. Guided by the domains from the community-based participatory research model [Reference Belone, Lucero and Duran19] and the National Academies, Assessing Meaningful Community Engagement model [Reference Aguilar-Gaxiola, Ahmed and Anise20], this study examined the alignment between the institutional mission, vision, and values; perceptions of the institutional trustworthiness and reputation; operational policies and practices related to CEnR; and leadership investment and prioritization of CEnR.
Overall, survey findings indicate a clear opportunity to bridge the gap between institutional aspirations for community health and the operational realities of CEnR. There is some complexity in which community respondents distinguished between the academic medical center as an institution and the individual researchers with whom they’ve interacted, suggesting that a positive partnership-level experience may coexist with broader institutional constraints. This distinction mirrors prior work highlighting difference between interpersonal trust in researchers and trust in institutions more broadly [Reference Bustos, Simkani and Reichel8,Reference Lucero, Boursaw, Eder, Greene-Moton, Wallerstein and Oetzel26], requiring further study. Perspectives from respondents embedded within the institution further underscored the challenge of prioritizing CEnR within large academic medical centers whose dominant orientation remains complex, tertiary, clinical care, and is also noted as a tension in the evaluation of institutional readiness for community engagement across clinical and translational science centers [Reference Eder, Evans and Funes1].
The qualitative findings deepen and contextualize these survey patterns by illuminating the institutional dynamics through which CEnR is supported. Across five themes, participants described the need for stronger integration between research and clinical care, particularly in response to community members’ concerns about research participation without access to or utilization of clinical services. Conceptualizing CEnR as a part of a learning healthcare system [Reference Ellis, Sarkies and Churruca27], in which community priorities, clinical practice, and research mutually inform one another could be a promising strategy that addresses this disconnect and aligns with the calls in translational science to embed engagement within care delivery rather than treating it as a parallel activity [Reference Eder, Evans and Funes1,Reference Ellis, Sarkies and Churruca27].
Participants also highlighted how the institution’s global reputation creates both trust in research and clinical excellence while creating perceived distance from local community priorities. This reinforces the importance of sustained, place-based engagement beyond individual projects and is consistent with the prior literature, where community members emphasized the need for institutional commitment to CEnR that is proactive rather than in reaction to grant requirements, alongside intentional efforts to overcoming mistrust, historical tensions, and structural barriers that limit long-term community partnerships [Reference Wallerstein, Duran, Oetzel and Minkler4].
The participatory sense-making, based on CBPR principles, with the institutional team allowed for the translations of these complex contextual insights into actionable, role-specific recommendations targeting institutional leaders, researchers and staff, and community partners. Recommendations for leaders emphasize articulating a shared vision for CEnR across the clinical, educational, and research mission areas and reducing fragmentation through the centralized coordination or a “front door” for engagement. Recommendations for researchers and staff focus on strengthening institutional supports for CEnR through protected time, mentorship and trainings; bridge funding between awards to sustain community partnering processes; and reductions in administrative processes that strain community partnerships. Finally, recommendations for community partners underscore the direct investment in community-based organizations, research leadership development, and bi-directional mentorship to support equitable participation and shared governance. Collectively, these recommendations reinforce that effective CEnR is not solely the responsibility of individual partnerships and requires intentional support across the institution to achieve sustained community impact.
Several limitations should be considered when interpreting these findings. First, most community participants were engaged in advisory boards or existing community-engaged research partnerships and thus may represent individuals with a greater familiarity with research processes and a nuanced understanding of CEnR compared to community members not engaged in research activities. Future studies should intentionally include a broader range of community members, including those without prior research involvement to capture a wider spectrum of experiences with academic medical centers. Second, the survey responses from community members on some questions may reflect specific projects rather than perceptions of the institution as a whole, underscoring the need for further psychometric testing and refinement of institutional-level measures of CEnR support and trustworthiness. We also carefully considered the additional sub group analyses by years of CEnR experience and level of engagement across the CEnR continuum; however, given the modest sample size and the risk of over-stratification, we did not conduct these analyses and instead identify them as important areas for future research. Finally, the cross-sectional nature of assessment limits the ability to examine how institutional conditions and perceptions of support for CEnR evolve over time, particularly in response to organizational change or national context. We attempted to mitigate these limitations through a theory-guided analyses, team-based sense-making, and integration of qualitative and quantitative data for interpretation. This mixed-methods approach provides a robust understanding of contextual conditions shaping CEnR and informed the development of recommendations for how to improve structures, policies, and practices to enable institutions to realize their vision of supporting and growing their footprint in innovative CEnR.
Concomitant with the evaluation process and presently, evaluation findings are being used by community and academic partners to enhance and influence the institutional conditions to promote CEnR and health equity research. For example, a CEnR “playbook” of best practices for CEnR at the institutional level has been developed for community and academic audiences, with the dual objectives to outline best practices for CEnR and to shed light on institutional facilitators that are lacking or should be revised (e.g., around remuneration processes for community partners, IRB nuances for CEnR). The evaluation also led to a change in intramural CEnR grant-making processes to extend funding intervals for partnership development and funding amounts. The evaluation has also informed a CEnR strategic plan at the institutional level to promote health equity.
Findings from this study suggest that a systematic process of prioritizing the perspectives of academic leaders, researchers, community engagement staff, and community members can provide context-specific recommendations to support and promote CEnR at an institutional level. Actions on these recommendations can facilitate CEnR partnerships to promote health equity across the clinical translational science centers.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cts.2026.10771.
Acknowledgements
The authors thank the participants for their time, effort, and insight toward the study.
Author contributions
Prajakta Adsul: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing-original draft, Writing-review & editing, Alena Kuhlemeier: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing-original draft, Writing-review & editing, Mark Wieland: Conceptualization, Formal analysis, Investigation, Methodology, Writing-original draft, Writing-review & editing, Irene Sia: Conceptualization, Investigation, Methodology, Resources, Supervision, Writing-original draft, Writing-review & editing, Sagar Dugani: Investigation, Methodology, Writing-original draft, Writing-review & editing, Vesna Garovic: Supervision, Writing-original draft, Writing-review & editing, Nina Wallerstein: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing-original draft, Writing-review & editing.
Funding statement
This study was supported by the Mayo Clinic Center for Clinical and Translational Science (UL1 TR02377). S.B.D. was also supported by the National Institute on Minority Health and Health Disparities (NIMHD K23 MD016230).
Competing interests
Authors declare no competing interests.



 Open access
Open access