


Introduction
Childhood trauma is a global issue with severe, long-lasting consequences. Approximately one in four children suffer from child abuse or neglect (Massullo et al., Reference Massullo, De Rossi, Carbone, Imperatori, Ardito, Adenzato and Farina2023). These early adverse experiences can significantly affect both developmental trajectories in childhood (Putnam, Reference Putnam2006) and overall well-being in adulthood (Dye, Reference Dye2018; Mersky et al., Reference Mersky, Topitzes and Reynolds2013). Moreover, childhood trauma is linked to poor mental health outcomes and strongly associated with the development of psychiatric disorders (McLaughlin & Lambert, Reference McLaughlin and Lambert2017).
Among psychiatric outcomes, psychosis has a robust connection to early adverse experiences (Stanton et al., Reference Stanton, Denietolis, Goodwin and Dvir2020). Individuals who report traumatic experiences during childhood are approximately three times more likely to develop a psychotic disorder than those without such experiences (Stanton et al., Reference Stanton, Denietolis, Goodwin and Dvir2020; Giannopoulou et al., Reference Giannopoulou, Georgiades, Stefanou, Spandidos and Rizos2023). Importantly, psychosis risk increases with the number of trauma types reported, reaching nearly 4.7 times higher for those endorsing three or more traumatic exposures (Stanton et al., Reference Stanton, Denietolis, Goodwin and Dvir2020). In addition to cumulative burden, the specific nature of trauma may also differentially shape psychosis risk. Croft et al. (Reference Croft, Heron, Teufel, Cannon, Wolke, Thompson and Zammit2019) reported that sexual abuse carried the highest risk for psychosis (OR = 2.5), while physical abuse had the lowest (OR = 1.69); however, these associations changed after adjusting for co-occurring traumatic experiences.
Trauma-related effects are not limited to psychosis. Childhood trauma is associated with a wide range of nonpsychotic psychiatric diagnoses (NPDs) and symptom domains (Van Nierop et al., Reference Van Nierop, Viechtbauer, Gunther, Van Zelst, De Graaf, Ten Have and Van Winkel2015), including anxiety, depression, externalizing behaviors, and substance use (Barzilay et al., Reference Barzilay, Calkins, Moore, Wolf, Satterthwaite, Cobb Scott and Gur2019; McLaughlin & Lambert, Reference McLaughlin and Lambert2017). While trauma effects in these disorders are important in their own right, they are particularly relevant to psychosis, as psychotic disorders rarely occur without additional comorbidities (Altamura et al., Reference Altamura, Serati, Albano, Paoli, Glick and Dell’Osso2011; Hartz et al., Reference Hartz, Pato, Medeiros, Cavazos-Rehg, Sobell, Knowles and Pato2014; Mollon et al., Reference Mollon, Lanzagorta, Mathias, Rodrigue, Knowles, Deaso and Glahn2025; Strålin & Hetta, Reference Strålin and Hetta2021). Most studies of psychosis fail to account for such comorbidities, leaving it unclear whether trauma effects are specific to psychosis or cross-diagnostic, and whether associations between trauma and NPDs differ based on psychosis status. Furthermore, trauma has been linked with greater diagnostic complexity in adulthood as evidenced by increases in the number of psychiatric diagnoses in those with higher traumatic exposures (Copeland et al., Reference Copeland, Shanahan, Hinesley, Chan, Aberg, Fairbank and Costello2018; Dorrington et al., Reference Dorrington, Zavos, Ball, McGuffin, Rijsdijk, Siribaddana and Hotopf2014). Evidence, however, is lacking whether the association between trauma and diagnostic complexity differs by psychosis status, despite its relevance for understanding clinical heterogeneity in psychosis.
Beyond diagnostic risk, trauma may also contribute to the severity and broader clinical consequences of psychiatric illness. For example, in psychosis, childhood trauma is associated with significantly reduced global functioning, more severe clinical symptoms (Aas et al., Reference Aas, Andreassen, Aminoff, Færden, Romm, Nesvåg and Melle2016; Bailey et al., Reference Bailey, Alvarez-Jimenez, Garcia-Sanchez, Hulbert, Barlow and Bendall2018), poorer cognitive functioning (Dauvermann & Donohoe, Reference Dauvermann and Donohoe2019), and elevated risk for suicide attempts (Hassan et al., Reference Hassan, Stuart and De Luca2016). Similar associations between trauma exposure and adverse outcomes have also been observed across nonpsychotic psychiatric diagnoses (Barczyk et al., Reference Barczyk, Foulds, Porter and Douglas2023; Copeland et al., Reference Copeland, Shanahan, Hinesley, Chan, Aberg, Fairbank and Costello2018; Zhao et al., Reference Zhao, Tang, Wang, Liu, Zhao, Xie and Zeng2025), as well as individuals without a psychiatric diagnosis (Downey & Crummy, Reference Downey and Crummy2022; Flechsenhar et al., Reference Flechsenhar, Seitz, Bertsch and Herpertz2024; Kuzminskaite et al., Reference Kuzminskaite, Vinkers, Milaneschi, Giltay and Penninx2022). The consistency of findings across psychosis, other clinical conditions, and nonclinical populations raises a central question of which trauma-related effects, if any, are specific to psychosis, and which reflect broader transdiagnostic processes.
Another important limitation of the existing literature is that most evidence linking trauma to psychosis is drawn from adult-onset (AOP) samples. Far less is known about whether these associations generalize to early-onset psychosis (EOP) (onset before age 18 years). Although early-onset cases are neurobiologically and clinically similar, they are often regarded as a more severe subtype of psychosis (Driver et al., Reference Driver, Thomas, Gogtay and Rapoport2020; Jacobsen & Rapoport, Reference Jacobsen and Rapoport1998). In reference to trauma, greater exposure has been associated with earlier psychosis onset (Rosenthal et al., Reference Rosenthal, Meyer, Mayo, Tully, Patel, Ashby and Niendam2020; Trovão et al., Reference Trovão, Alves, Carrilho, Ricci, Bittencourt, Alves and Veras2022). EOP, however, is rare (Lemmers et al., Reference Lemmers, Tawil, Petek, Balog, Block, Santen and van der Maarel2012), resulting in limited information about how trauma exposure and its effects on outcomes might differ in early-onset versus adult-onset cases.
The aim of the current study was to clarify whether the patterns of trauma exposure and their relationships to psychiatric outcomes are different in psychosis relative to other psychiatric conditions and whether this pattern differs between EOP and AOP cases. We approach these aims via a series of regression analyses. First, we assessed trauma exposure as a function of psychosis status alone to align with prior literature and establish a baseline comparison. We then extended this framework by incorporating NPDs, modeling trauma exposure across finer-grained diagnostic subgroups to disentangle the relative contributions of psychosis and comorbid psychopathology. Next, we examined whether trauma exposure corresponded with overall psychiatric burden (indexed by the number of NPDs) to further evaluate whether trauma exposure scales with diagnostic complexity and whether this differs for those with psychosis. We also examine the impact of trauma exposure on functional, symptomatic, and cognitive outcomes beyond psychiatric diagnosis status, and again whether these impacts differ for those with psychosis. Finally, we qualitatively compare the overall pattern of results between the EOP and AOP samples, providing insight into potential differences in psychosis related to age of onset.
If trauma effects are more strongly associated with psychosis, we hypothesize that trauma exposure will be higher in individuals with psychosis than in those without, and that co-occurring nonpsychotic psychiatric diagnoses (NPDs) may further amplify this exposure more strongly than in nonpsychosis groups. We also expect trauma to be linked to a greater number of NPDs, particularly among those with psychosis, and to show stronger associations with clinical, functional, and cognitive outcomes in the psychosis group.
Methods
Sample
We used data from two psychosis samples: an early-onset psychosis (EOP) sample (see Table 1 and Supplementary Material sTable 1) and an adult-onset psychosis (AOP) sample (see Table 1 and Supplementary Material sTable 2). For each sample, psychosis diagnoses included the following: schizophrenia, schizoaffective, schizophreniform, brief psychotic disorder, psychosis NOS, delusional disorder, major depressive disorder (MDD) with psychosis, or bipolar disorder with psychosis. Controls were considered those without a psychosis diagnosis but could have one or more NPDs. Diagnoses were confirmed via case conferences using a consensus approach with experienced psychiatrists and clinical psychologists, with the instruments described for each sample below. All subjects were outpatients or part of the general population at the time of testing.
Sample demographics

Note: Demographic and phenotypic information for EOP and AOP samples by psychosis status. Values are means (standard deviation) unless otherwise specified. *Means were calculated only among participants with NPDs.
EOP cohort
Subjects in the EOP sample (N = 1341) were Mexican and part of the Early Psychosis Investigation Center in Mexico City (EPIMex). The EPIMex study was established to discover psychosocial, biological, and genetic mechanisms predisposing individuals to the onset of psychosis before the age of 18 years. Control and psychosis participants were recruited from three medical facilities in Mexico City (Child Psychiatric Hospital Dr. Juan N Navarro, Carracci Medical Group, Centros de Integración Juvenil) and through local schools and advertising (https://www.epimex.net/). Diagnoses were ascertained for all participants using the Structured Clinical Interview for the DSM-V (SCID-5) and the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS) for participants under the age of 18 years. KSADS modules included separation anxiety, elimination disorders (enuresis and encopresis), externalizing disorders (oppositional defiant disorder, conduct disorder, and disruptive mood dysregulation), and tic disorders. Subjects were between the ages of 6–21 years and were excluded if they reported a history of severe developmental disorders that would impact their ability to participate or a history of a neurodegenerative disorder or brain infection.
Controls were not excluded for nonpsychotic psychiatric disorders, but did not possess any lifetime psychosis diagnosis and could not have a first or second degree relative with a psychotic illness.
The protocol was approved by the institutional review board at Boston Children’s Hospital. All participants provided written informed consent. For individuals under the age of 18 years, guardians provided written informed consent.
AOP cohort
Subjects in the AOP sample (N = 392) were part of a larger study examining brain dysconnectivity in psychosis in African Americans. Control and psychosis participants were recruited from Hartford, Connecticut area, via flyers, advertisements in local newspapers, and Craigslist. Diagnoses were ascertained for all participants using the Structured Clinical Interview for the DSM-IV-TR. Subjects were between the ages of 18 and 70 years and were excluded if they reported a history of major medical disorders or severe head injury, or if they had an IQ (as assessed by the WASI or WTAR) <70. Subjects who tested positive for illicit drugs (excluding THC) via urine screening or were intoxicated on the day of testing were also excluded.
As in in EPIMEX, controls were not excluded for nonpsychotic psychiatric disorders, but did not possess any lifetime psychosis diagnosis and could not have a first or second degree relative with a psychotic disorder.
The protocol was approved by institutional review boards at Hartford Hospital and Yale University. All participants provided written informed consent.
Trauma assessment
Trauma exposure was assessed using different measures in each sample. Subjects in the EOP sample completed the Spanish version of the Adverse Childhood Experiences (ACEs) questionnaire (Oláh et al., Reference Oláh, Fekete, Kuritárné Szabó and Kovács-Tóth2023). The Spanish translation of the ACEs questionnaire has demonstrated strong construct validity and reliability in empirical studies in Mexico (Casas-Muñoz et al., Reference Casas-Muñoz, Velasco-Rojano, Rodríguez-Caballero, Prado-Solé and Álvarez2024). The ACEs is a 10-item (yes/no) questionnaire to assess traumatic experiences in childhood; scoring is the sum across all items. Subjects in the AOP sample completed the Childhood Trauma Questionnaire (CTQ) (Bernstein et al., Reference Bernstein, Ahluvalia, Pogge and Handelsman1997) in English. The CTQ is a 28 ordinal (1 = Never true, 2 = Rarely true, 3 = Sometimes true, 4 = Often true, 5 = Very often true) item questionnaire quantifying the frequency of stressful environmental events in childhood. Item subsets can be summed to generate subscale scores reflecting physical and emotional neglect, physical and emotional abuse, and sexual abuse, or summed across all items for a total CTQ score. Prior research demonstrates strong concordance between ACEs items and corresponding CTQ subscales (Schmidt et al., Reference Schmidt, Narayan, Atzl, Rivera and Lieberman2020; Xu et al., Reference Xu, Li, Cai, Yuan, He, Liu and Wang2023).
We constructed a conceptually comparable trauma measure between EOP and AOP samples by identifying items from each that addressed the same type of trauma (i.e. physical, sexual, and emotional abuse; physical and emotional neglect; and parental substance use) (see Supplementary Material sTable 3). For the ACEs, this resulted in six binary items (0/1), one per trauma type; we then summed across endorsed trauma types to get a score ranging from 0 to 6. For the CTQ, several items could index a particular trauma type. As such, if subjects endorsed any item (CTQ response of ≥2) within a trauma type, that type received a 1. Like the ACEs, we summed across trauma types for a score ranging from 0 to 6. This method allowed us to conduct parallel analyses in each sample with a more comparable measure. To ensure results were not solely a consequence of our restricted trauma measure, we also performed all analyses with complete trauma measures within each sample using the measure’s respective scoring procedure.
Outcome measures
Outcomes included global functioning, symptom severity, and cognition. Outcomes were assessed with identical procedures and measures for EOP and AOP samples unless otherwise indicated.
Global functioning was measured using the Global Assessment of Functioning (GAF) scale (Blake et al., Reference Blake, Cangelosi, Johnson-Brooks and Belcher2007). For participants in the EOP sample under the age of 18 years, we used the Children’s Global Assessment Scale (CGAS) (Blake et al., Reference Blake, Cangelosi, Johnson-Brooks and Belcher2007). For both measures, scores range from 1 to 100, with higher scores indicating better global function. Values around 70 generally reflect mild difficulties with overall functioning, scores between 51 and 70 indicate moderate symptoms or impairment, and scores between 31 and 50 suggest serious impairment in social, school, or occupational functioning. Scores below 30 are typically associated with severe dysfunction requiring substantial support.
Symptom severity was measured using the total score on the Brief Psychiatric Rating Scale (BPRS). This measure assesses psychopathology in several psychiatric diagnoses looking at symptom domains such as anxiety, emotional withdrawal, and bizarre behavior (Hofmann et al., Reference Hofmann, Schmid, Jabat, Brackmann, Noboa, Bobes and Egger2022).
Cognition was assessed with three measures: digit symbol (indexing processing speed) (Mathias et al., Reference Mathias, Knowles, Barrett, Leach, Buccheri, Beetham and Glahn2017, the Controlled Word Association Test (COWAT) (indexing verbal fluency) (Spreen & Strauss, Reference Spreen and Strauss1998), and letter-number sequencing (indexing verbal working memory) (Corporation, Reference Corporation1997). We chose cognitive measures based on two criteria: (1) Availability and comparability in our EOP and AOP samples and (2) Consistent evidence of disrupted performance in psychosis (Bora et al., Reference Bora, Binnur Akdede and Alptekin2017; Catalan et al., Reference Catalan, McCutcheon, Aymerich, Pedruzo, Radua, Rodríguez and Fusar-Poli2024). EOP participants completed cognitive testing with a computerized battery on Gorilla (https://gorilla.sc, Mathias et al., Reference Mathias, Knowles, Barrett, Leach, Buccheri, Beetham and Glahn2017), whereas AOP participants completed cognitive testing with a computerized battery called “Charlie” (https://github.com/sammosummo/Charlie, Mathias et al., Reference Mathias, Knowles, Barrett, Leach, Buccheri, Beetham and Glahn2017). Cognitive tests were identical across platforms and were administered at in-person visits with a moderator.
Statistical analyses
We used R version 4.4.1 to conduct all statistical analyses.
Sample comparisons
Within each study, demographic variables were compared across control and psychosis groups. Chi-square tests were used to assess differences in sex distribution and ANCOVAs were used to evaluate differences in age and number of nonpsychotic diagnoses (in NPD subjects only). To characterize similarities and differences between samples, the same analyses were conducted across studies, excluding age, which differed by design.
Trauma analyses
All analyses related to trauma were performed separately in EOP and AOP samples with restricted and complete trauma measures (ACEs total and CTQ total scores). No formal statistical comparisons were made between samples. In all models described below, sex and age were used as covariates and all continuous measures were standardized across all individuals within each sample.
We conducted a series of regression analyses to systematically examine trauma exposure and its clinical relevance. First, to align with prior literature and establish a baseline comparison, we used multiple linear regression to assess trauma exposure as a function of psychosis status alone, treating psychosis as a binary predictor and trauma score as the dependent variable.
We then extended this model to more precisely characterize the contribution of nonpsychotic diagnoses (NPDs) to trauma exposure. Using multiple regression, trauma exposure was modeled as a function of psychosis and NPD status by dividing the sample into finer-grained diagnostic groups: controls without psychiatric diagnoses (C), controls with nonpsychotic diagnoses (Cdx), individuals with psychosis only (PSY), and individuals with psychosis and nonpsychotic diagnoses (PSYdx). Group membership was dummy coded with C as the reference group. Follow-up pairwise contrasts (Cdx vs. PSY, Cdx vs. PSYdx, PSY vs. PSYdx) were conducted with false discovery rate (FDR) correction (Benjamini & Hochberg, Reference Benjamini and Hochberg1995). This approach allowed us to disentangle the relative contributions of psychosis and psychiatric comorbidity to trauma exposure.
To further evaluate whether trauma exposure scaled with overall psychiatric burden, we conducted a follow-up regression examining the association between the number of NPDs and trauma exposure. In this model, trauma score was the dependent variable, number of NPDs was the primary predictor, with psychosis status included as a covariate; the interaction between psychosis status and number of NPDs was also tested. This analysis assessed whether trauma exposure varied as a function of cumulative nonpsychotic comorbidity and whether this relationship differed by psychosis status.
Finally, we examined the clinical and cognitive consequences of trauma. Multiple linear regression models were used to test the effects of trauma score, psychosis status (binary), and NPD status (binary) (predictor variables) on functional, symptomatic, and cognitive outcomes (dependent variables). The interaction between trauma and psychosis status was also tested. Separate models were estimated for each dependent variable with multiple testing controlled using the false discovery rate (Benjamini & Hochberg, Reference Benjamini and Hochberg1995). This analytic sequence allowed us to assess whether trauma exposure contributes to outcomes and if this effect differs by psychosis status.
Results
Sample characteristics
Within samples
There were no significant differences in age across psychosis and control groups for either the EOP (F[1, 1338] = 0.94, p = 0.33) or the AOP (F[1, 389] = 0.34, p = 0.56) sample. For the EOP sample, there were significantly more males in the control group than in the psychosis group (χ2(1) = 10.3, p = 0.001); there were no significant differences in sex distribution across groups for the AOP sample (χ 2(1) = 0.16, p = 0.69). EOP control and psychosis participants did not significantly differ in the number of NPDs (F[1, 1052] = 0.03, p = 0.85), whereas AOP psychosis participants had significantly more NPDs than AOP controls (F[1, 276] = 13.3, p = 0.0003] (see Figure 1A).
(A). Bars show the number of nonpsychotic diagnoses by study (panels) and psychosis status (bars). (B). Diagnostic complexity in controls (red) and those with psychosis (blue) in EOP (left) and AOP (right) samples. Dots connected by a vertical line indicate the specified pattern of comorbidity, whereas bars indicate how frequently that pattern appears in the sample. *Disorders assessed with the KSADS for the EOP sample only. Separation anxiety is included in the anxiety category for the EOP sample.

Between samples
The AOP sample contained significantly more males than the EOP sample (χ 2(1) = 5.8, p = 0.02). EOP control and psychosis participants had significantly more NPDs than AOP control and psychosis participants (control: F[1, 658] = 30.9, p = 3.9 × 10−8; psychosis: F [1, 670] = 5.4, p = 0.02), although this is likely due to the addition of the KSADS in the EOP sample only. Regarding the nature of NPDs, those related to anxiety and depression were common for both EOP and AOP samples. Substance-related disorders were more frequently reported in the AOP group (see Figure 1B).
Trauma
Trauma-related results in the main text pertain to analyses with restricted trauma measures unless otherwise indicated. See Supplementary Material sTables 4 and 5 for comparison of effects between restricted and complete trauma measures. Overall, conclusions were unchanged regardless of trauma measures used. Reported effect sizes are standardized.
Exposure
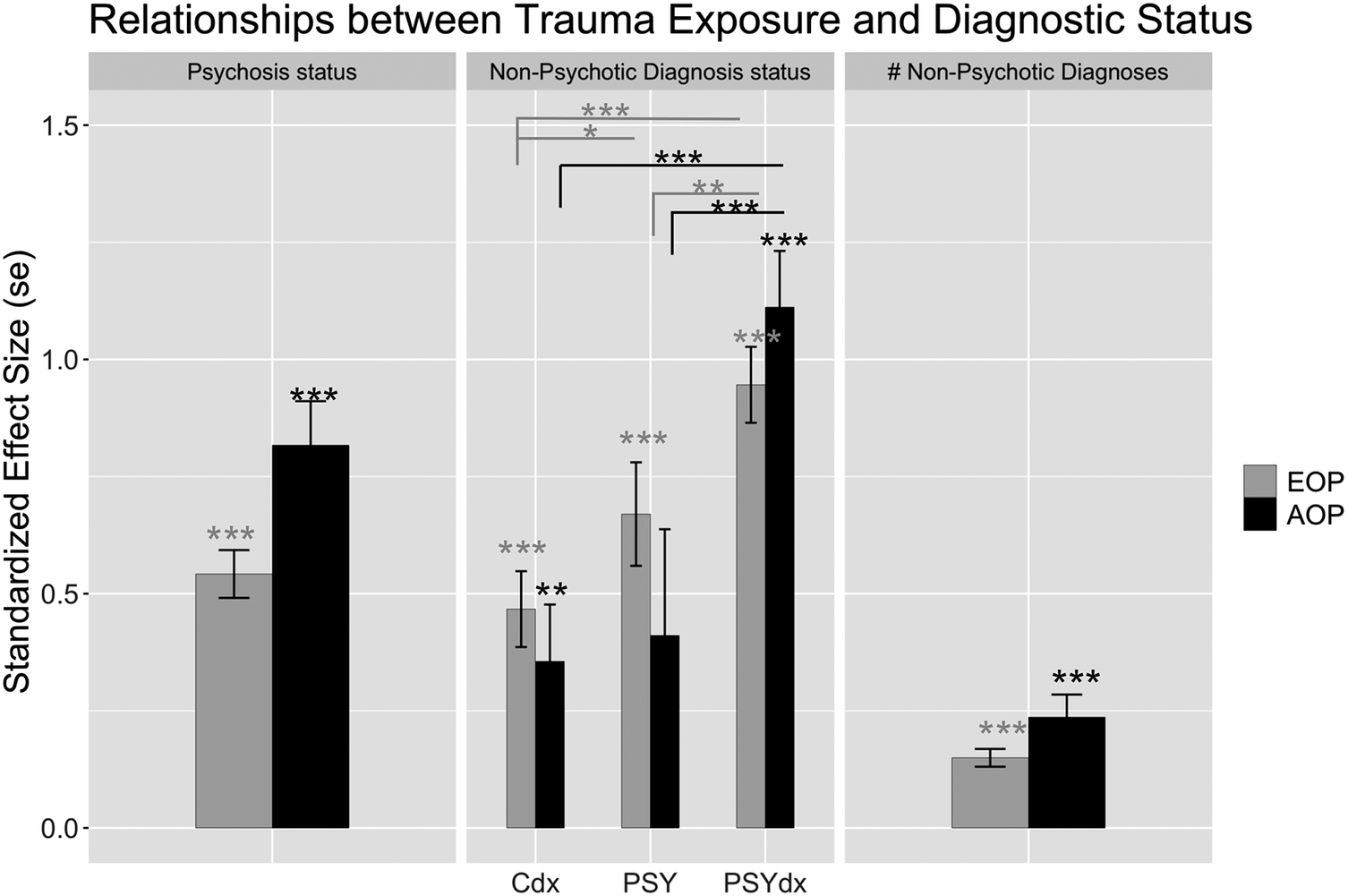
Figure 2 illustrates the distribution of restricted trauma scores (i.e. proportion of participants by the total number of trauma types endorsed). Disregarding NPD status, individuals with psychosis in both samples reported greater trauma exposure than those without psychosis (Figure 3, Panel 1; Supplementary Material sTable 4, Model 1); effect sizes were somewhat larger in the AOP (
 $ \beta $
= 0.81 [0.09]) versus the EOP sample (
$ \beta $
= 0.81 [0.09]) versus the EOP sample (
 $ \beta $
= 0.54 [0.05]).
$ \beta $
= 0.54 [0.05]).
Bars show the distribution of restricted trauma scores by those with psychosis (hashed bars) and without psychosis (solid bars) in EOP (gray bars) and AOP (black bars) samples.

Panels show standardized effect sizes and standard errors from the following models from left to right: trauma exposure by psychosis status (Supplementary Material sTable 4, Model 1), trauma exposure by psychosis status and NPD status (effect sizes are in reference to controls with no NPDs) (Supplementary Material sTable 4, Model 2), and trauma exposure by number of NPDs controlling for psychosis status (Supplementary Material sTable 4, Model 3). In each model, age and sex were included as covariates. N’s for the first and second panels are located in Table 1 and Supplementary Material sTables 1 and 2, respectively. EOP = early-onset psychosis; AOP = adult-onset psychosis, Cdx = controls with NPDs, PSY = individuals with psychosis only, PSYdx = individuals with psychosis and NPDs. *p < 0.05, **p < 0.01, ***p < 0.001.

When NPD status was considered alongside psychosis, an additive effect emerged: trauma scores increased linearly across Cdx (EOP:
 $ \beta $
= 0.47 [0.08]; AOP:
$ \beta $
= 0.47 [0.08]; AOP:
 $ \beta $
= 0.36 [0.12]), PSY (EOP:
$ \beta $
= 0.36 [0.12]), PSY (EOP:
 $ \beta $
= 0.67 [0.11]; AOP:
$ \beta $
= 0.67 [0.11]; AOP:
 $ \beta $
= 0.41 [0.23]), and PSYdx groups (EOP:
$ \beta $
= 0.41 [0.23]), and PSYdx groups (EOP:
 $ \beta $
= 0.95 [0.08]; AOP:
$ \beta $
= 0.95 [0.08]; AOP:
 $ \beta $
= 1.1 [0.12]) relative to controls with no psychiatric diagnoses (Figure 3, Panel 2; Supplementary Material sTable 2, Model 2). In the EOP sample, there were also significant differences between the Cdx and PSY, Cdx and PSYdx, and PSY and PSYdx groups (Supplementary Material sTable 2, Model 2). A similar pattern was observed in the AOP sample, but there was no significant difference between the Cdx and PSY groups, nor the PSY and control groups. The latter comparison, however, did reach significance when using the complete trauma measure (Supplementary Material sTable 2, Model 2). Given the limited size of the PSY group in the AOP sample, we view the initial null findings as more consistent with underpowered analyses than with a true absence of effect.
$ \beta $
= 1.1 [0.12]) relative to controls with no psychiatric diagnoses (Figure 3, Panel 2; Supplementary Material sTable 2, Model 2). In the EOP sample, there were also significant differences between the Cdx and PSY, Cdx and PSYdx, and PSY and PSYdx groups (Supplementary Material sTable 2, Model 2). A similar pattern was observed in the AOP sample, but there was no significant difference between the Cdx and PSY groups, nor the PSY and control groups. The latter comparison, however, did reach significance when using the complete trauma measure (Supplementary Material sTable 2, Model 2). Given the limited size of the PSY group in the AOP sample, we view the initial null findings as more consistent with underpowered analyses than with a true absence of effect.
A greater number of NPDs was significantly associated with a higher trauma score (EOP:
 $ \beta $
= 0.15 [0.02]; AOP:
$ \beta $
= 0.15 [0.02]; AOP:
 $ \beta $
= 0.24 [0.05]) (see Figure 3, Panel 3 and Supplementary Material sTable 4, Model 3). This effect was similar regardless of an individual’s psychosis status (no significant psychosis by number of NPDs interaction), although those with psychosis consistently showed higher trauma scores regardless of number of NPDs (significant main effect of psychosis) (EOP:
$ \beta $
= 0.24 [0.05]) (see Figure 3, Panel 3 and Supplementary Material sTable 4, Model 3). This effect was similar regardless of an individual’s psychosis status (no significant psychosis by number of NPDs interaction), although those with psychosis consistently showed higher trauma scores regardless of number of NPDs (significant main effect of psychosis) (EOP:
 $ \beta $
= 0.57 [0.08]; AOP:
$ \beta $
= 0.57 [0.08]; AOP:
 $ \beta $
= 0.69 [0.15]).
$ \beta $
= 0.69 [0.15]).
Effect on outcomes
We examined the relationship between trauma exposure and diagnostic status (psychosis and NPD) on outcomes such as global functioning, symptom severity, and cognition. Figure 4 and Supplementary Material sTable 5 show the standardized effect sizes for trauma, psychosis status, NPD status, and the interaction between trauma and psychosis for each outcome measure model in EOP and AOP samples. In both samples, trauma scores were significantly associated with lower global functioning (EOP:
 $ \beta $
= -0.21 [0.04]; AOP:
$ \beta $
= -0.21 [0.04]; AOP:
 $ \beta $
= -0.13 [0.05]) and higher symptom severity (EOP:
$ \beta $
= -0.13 [0.05]) and higher symptom severity (EOP:
 $ \beta $
= 0.13 [0.04]; AOP:
$ \beta $
= 0.13 [0.04]; AOP:
 $ \beta $
= 0.14 [0.05]). There were no significant effects of trauma on cognition. Additionally, trauma score did not differentially affect outcomes based on psychosis status (no significant psychosis by trauma interactions). Psychosis status was significantly associated with worse global functioning (EOP:
$ \beta $
= 0.14 [0.05]). There were no significant effects of trauma on cognition. Additionally, trauma score did not differentially affect outcomes based on psychosis status (no significant psychosis by trauma interactions). Psychosis status was significantly associated with worse global functioning (EOP:
 $ \beta $
= -0.86 [0.05]; AOP:
$ \beta $
= -0.86 [0.05]; AOP:
 $ \beta $
= -1.3 [0.07]), higher symptom severity (EOP:
$ \beta $
= -1.3 [0.07]), higher symptom severity (EOP:
 $ \beta $
= 1.0 [0.05]; AOP:
$ \beta $
= 1.0 [0.05]; AOP:
 $ \beta $
= 1.1 [0.08]), and poorer cognitive function (average effect sizes across cognitive tasks EOP:
$ \beta $
= 1.1 [0.08]), and poorer cognitive function (average effect sizes across cognitive tasks EOP:
 $ \beta $
= -0.21; AOP:
$ \beta $
= -0.21; AOP:
 $ \beta $
= -0.34) regardless of trauma exposure. NPD status was also significantly associated with worse global functioning (EOP:
$ \beta $
= -0.34) regardless of trauma exposure. NPD status was also significantly associated with worse global functioning (EOP:
 $ \beta $
= -0.48 [0.06]; AOP:
$ \beta $
= -0.48 [0.06]; AOP:
 $ \beta $
= -0.56 [0.07]) and higher symptom severity (EOP:
$ \beta $
= -0.56 [0.07]) and higher symptom severity (EOP:
 $ \beta $
= 0.26 [0.06]; AOP:
$ \beta $
= 0.26 [0.06]; AOP:
 $ \beta $
= 0.32 [0.08]), albeit to a lesser degree than psychosis status, and was associated with better verbal fluency in the EOP sample only (
$ \beta $
= 0.32 [0.08]), albeit to a lesser degree than psychosis status, and was associated with better verbal fluency in the EOP sample only (
 $ \beta $
= 0.18 [0.07]).
$ \beta $
= 0.18 [0.07]).
Standardized effect sizes and standard errors from models predicting outcomes from psychosis status (black), NPDs (gray), trauma (red), and the interaction between psychosis and trauma (dark red) in EOP (circle) and AOP (triangle) samples. Separate models were run for each outcome measure; FDR was used to correct for multiple comparisons across models. EOP = early-onset psychosis; AOP = adult-onset psychosis; WM = working memory; FDR = false discovery rate. *p < 0.05, **p < 0.01, ***p < 0.001.

Discussion
The current study aimed to examine whether the degree of trauma exposure or trauma’s impact on clinical outcomes were specific to psychosis, and whether patterns of results were consistent in EOP and AOP samples. The only indication for psychosis-specific effects was in the magnitude of trauma exposure, as those with psychosis (regardless of onset) had the greatest amount of trauma exposure. While both the presence and cumulative number of NPDs were associated with higher trauma exposure, these associations were similar regardless of psychosis status. Likewise, the effects of trauma on clinical outcomes did not appear to be psychosis-specific, as there were comparable patterns of effects for psychotic and nonpsychotic diagnostic groups. While some suggest childhood trauma is linked to earlier psychosis onset (Rosenthal et al., Reference Rosenthal, Meyer, Mayo, Tully, Patel, Ashby and Niendam2020; Trovão et al., Reference Trovão, Alves, Carrilho, Ricci, Bittencourt, Alves and Veras2022), we found no such evidence, as results were highly similar in EOP and AOP samples; in fact, effect sizes were numerically larger in the AOP than the EOP sample.
While elevated trauma exposure across psychiatric disorders is well established, our study examined the less explored relationship between trauma and NPDs in the context of psychosis. Consistent with prior work (Carr et al., Reference Carr, Martins, Stingel, Lemgruber and Juruena2013; Copeland et al., Reference Copeland, Shanahan, Hinesley, Chan, Aberg, Fairbank and Costello2018; Klinger-König et al., Reference Klinger-König, Erhardt, Streit, Völker, Schulze, Keil and Grabe2024), individuals with NPDs reported greater trauma exposure, and trauma increased with the number of NPDs, suggesting that greater childhood adversity may contribute to more complex psychopathology (Putnam, Reference Putnam2006). This effect was additive in psychosis, such that individuals with both psychosis and NPDs reported higher trauma exposure than those with psychosis alone. However, the effects of NPD presence and number were comparable among individuals with and without psychosis, as there were no significant psychosis-by-NPD interactions. These findings suggest that trauma may operate as a transdiagnostic risk factor contributing to a broad range of psychiatric disorders, potentially through shared mechanisms of vulnerability (Fischer & Gessler, Reference Fischer and Gessler2007). Furthermore, consistently elevated trauma exposure in psychosis aligns with evidence of dose–response relationships between cumulative childhood adversity and psychosis risk, with nonlinear trends indicating sharper increases in risk at higher levels of exposure (Flinn et al., Reference Flinn, Hefferman-Clarke, Parker, Allsopp, Zhou, Begemann and Varese2025). Further studies are needed to clarify how the type, timing, and cumulative load of trauma contribute to different patterns of psychopathology presentation. Nevertheless, the present findings underscore the importance of comprehensive trauma assessment when evaluating psychiatric risk and highlight the need for prevention strategies that limit cumulative exposure (particularly for those already at higher risk for psychosis), given its association with more severe and clinically complex psychiatric presentations in our sample.
Trauma exposure was associated not only with the presence of psychopathology but also with greater symptom severity and poorer global functioning. These findings support prior research indicating that trauma can negatively influence clinical features (Aas et al., Reference Aas, Andreassen, Aminoff, Færden, Romm, Nesvåg and Melle2016) and illness course (Kraan et al., Reference Kraan, Van Dam, Velthorst, De Ruigh, Nieman, Durston and De Haan2015). However, the impact of trauma on these outcomes did not vary by psychosis status, as reflected in the nonsignificant trauma-by-psychosis interaction. Thus, trauma is relevant to symptom and functional outcomes across all participants, regardless of psychopathology. Notably, trauma’s effect sizes on these outcomes were small – less than half the magnitude of those linked to a psychosis diagnosis (Figure 3) – suggesting that other psychosis-related factors (e.g. genetic [Pazoki et al., Reference Pazoki, Lin, Van Eijk, Schijven, De Zwarte and Luykx2021; Santoro et al., Reference Santoro, Ota, De Jong, Noto, Spindola, Talarico and Breen2018] or neurobiological [Brunner et al., Reference Brunner, Gajwani, Gross, Gumley, Krishnadas, Lawrie and Uhlhaas2022; Worker et al., Reference Worker, Berthert, Lawrence, Kia, Arango, Dinga and Marquand2023]) may contribute more substantially to poor outcomes than trauma exposure per se. This does not diminish the importance of trauma prevention and intervention efforts, which are likely to benefit many individuals, including those who never develop a diagnosable disorder.
In contrast to clinical and functional outcomes, trauma was not significantly associated with cognitive outcomes in our sample, which included processing speed, verbal working memory, and verbal fluency. Although prior work has reported some trauma-related deficits in similar cognitive domains (Rosa et al., Reference Rosa, Scassellati and Cattaneo2023; Vargas et al., Reference Vargas, Lam, Azis, Osborne, Lieberman and Mittal2019), effect sizes are small, and results are inconsistent across psychiatric and nonpsychiatric populations. For example, a meta-analysis by Vargas et al. (Reference Vargas, Lam, Azis, Osborne, Lieberman and Mittal2019) reported effect sizes of −0.09 for working memory and −0.07 for processing speed, whereas a recent review by Rosa et al. (Reference Rosa, Scassellati and Cattaneo2023) noted mixed findings across studies of both psychotic and nonpsychotic psychiatric samples, with somewhat more consistent associations in nonpsychiatric populations, although these were based on fewer studies. These findings do not preclude the possibility that trauma may affect other cognitive domains not assessed here, such as executive functioning or general cognitive ability, although evidence in these domains is similarly inconsistent. Still another possibility may be the nature of our trauma measure, in that it captures the number of trauma types experienced rather than the frequency of events. However, we consider this unlikely, as analyses using the full CTQ, which more directly assesses trauma frequency, yielded the same results (Supplementary Material sTable 5). While trauma was not associated with cognitive outcomes in our sample, psychosis diagnosis was, underscoring that poor performance in our sample was primarily driven by other factors associated with the illness (McCleery & Nuechterlein, Reference McCleery and Nuechterlein2019; Mollon et al., Reference Mollon, David, Zammit, Lewis and Reichenberg2018) rather than trauma history.
There are several limitations to the present study. First, we focused specifically on childhood trauma, defined as exposure occurring before age 18 years by the ACEs and CTQ. However, trauma can also occur later in life, which may be especially relevant for individuals in the AOP group. In the EOP sample, we lacked information on the temporal relationship between trauma and psychosis onset. This is a key limitation because trauma may both precede and follow psychosis onset: individuals with psychosis are at increased risk for subsequent traumatic experiences (De Vries et al., Reference De Vries, Van Busschbach, Van Der Stouwe, Aleman, Van Dijk, Lysaker and Pijnenborg2019), and the illness and its treatment can be perceived as traumatic in and of itself (van Os et al., Reference van Os, Marsman, van Dam and Simons2017). Most of these studies, however, are conducted in adults and refer to trauma in adulthood. It is unclear if similar principles apply to those with EOP. Nevertheless, to acknowledge this limitation, we analyzed trauma in terms of exposure rather than risk or prediction. Additionally, we did not examine the effects of trauma subtypes (e.g. physical vs. sexual abuse), and our trauma measures varied across samples, which is suboptimal. However, prior research shows similar effects across subtypes (Croft et al., Reference Croft, Heron, Teufel, Cannon, Wolke, Thompson and Zammit2019), and our own findings were consistent whether using restricted or complete trauma measures, suggesting that trauma type and/or variation in trauma measurement was less critical in explaining our findings. Future research would benefit from the use of standardized trauma assessments across age groups to allow more direct comparisons between developmental periods, especially in reference to the effects of trauma subtype and timing. Ideally, longitudinal studies beginning in early childhood would provide clearer insight into how trauma contributes to psychosis risk and clinical trajectories over time. We are currently performing this work in an EOP sample collected in the United States. Finally, although BPRS and GAF scores offer complementary indicators of symptom severity and global functioning, they measure related but distinct constructs, and symptom severity does not always map directly onto functional impairment (Correll et al., Reference Correll, Brieden and Janetzky2023; Seitz-Holland et al., Reference Seitz-Holland, Jacobs, Reinen, Mathalon, Corcoran, Reichenberg and Pasternak2025). More detailed, domain-specific assessments of functioning and symptom domains would allow for a more nuanced understanding of how trauma influences clinical presentation and outcomes.
It is also true that the EOP and AOP samples differed in several demographic and clinical characteristics, including a higher proportion of males with psychosis in the AOP group and distinct ethnoracial and sociocultural contexts (Mexican youth in Mexico vs. African American adults in the United States). These differences may introduce heterogeneity and limit the comparison of patterns across groups. Even so, the overall pattern of findings was highly consistent across samples. Effect sizes for trauma exposure were larger in the AOP cohort, potentially reflecting the intersection of trauma with minority status, whereas the effect sizes for trauma’s impact on clinical outcomes were numerically similar across EOP and AOP groups. We, therefore, see the variability between samples as a strength rather than a limitation.
Our study has meaningful implications for clinical practice and underscores the urgency of integrating trauma-informed approaches across psychiatric care settings. The observation that trauma’s impact on symptom severity and global functioning was consistent regardless of psychosis status aligns with a growing body of evidence demonstrating that trauma operates as a transdiagnostic risk factor with pervasive downstream effects (Kessler et al., Reference Kessler, Birnbaum, Bromet, Hwang, Sampson and Shahly2010; Varese et al., Reference Varese, Smeets, Drukker, Lieverse, Lataster, Viechtbauer and Bentall2012). The equivalence of these effects across EOP and AOP samples further suggests that trauma-informed care is a consistent clinical imperative, not confined to a particular illness stage or age of onset. This is consistent with evidence that trauma-focused interventions are both feasible and effective in individuals with psychosis (Hardy, Reference Hardy2017; Van Den Berg et al., Reference Van Den Berg, De Bont, Van Der Vleugel, De Roos, De Jongh, Van Minnen and Van Der Gaag2015), challenging the historically held assumption that trauma processing is contraindicated in this population. Taken together, these results provide additional empirical support for integrated, trauma-sensitive frameworks that address the cumulative psychiatric burden experienced across diagnostic boundaries.
Supplementary material
To supplementary material for this article can be found at http://doi.org/10.1017/S0033291726104401.
Funding statement
Work in the early-onset psychosis sample was supported by the National Institute of Mental Health R01MH133621 and U01MH124962. Work in the adult-onset sample was supported by the National Institute of Mental Health MH106324.
Competing interests
The authors declare none.
Ethical standard
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guides on the care and use of laboratory animals.







 Open access
Open access