

Introduction
Multisite studies are fundamental to clinical and translational research, providing high-quality scientific evidence [1,Reference Greenberg2]. By leveraging research networks across multiple institutions under a shared protocol, such studies accelerate participant recruitment from diverse populations, thereby enhancing the generalizability of findings and providing the statistical power and precision needed for reliable inference [Reference Unverzagt, Prondzinsky and Peinemann3]. However, early multisite studies also revealed that achieving consistent study implementation and reliable data across sites required dedicated coordination. In the mid-1960s, when the National Heart Institute initiated a series of large interventional studies, centralized coordination was recognized as essential to ensure data consistency, analytic validity, timely reporting, and effective communication across clinical sites, which later became core responsibilities of Data Coordinating Centers (DCCs) [Reference Greenberg2,Reference Cook and DeMets4–Reference DuChene, Hultgren and Neaton8].
In the 1990s, the introduction of the International Conference on Harmonization Good Clinical Practice (ICH-GCP) guidelines and the US Food and Drug Administration (FDA) 21 Code of Federal Regulations (CFR) Part 11 rule on electronic records and signatures substantially expanded the scope of study coordination and the responsibilities of DCCs [9,10]. These international guidelines and national mandates formalized expectations for data quality, documentation, monitoring, and oversight, elevating many coordination efforts that had previously followed scientific best practices to regulatory and compliance requirements [Reference Cook and DeMets4,Reference Gallin, Ognibene and Johnson11].
In contemporary clinical and translational research, multisite studies are increasingly coordinated through research consortia that span multiple countries, institutions, disciplines, and data environments [Reference Austin12,Reference Goodlett, Hung and Feriozzi13]. Correspondingly, the coordination challenges that initially motivated the creation of DCCs have further intensified and diversified. Coordinating across institutions now routinely involves managing heterogeneous data sources and data types, often collected using different systems and standards, which complicates data harmonization and quality assurance processes [Reference Austin12,Reference Castano and De Antonellis14,Reference Le Sueur, Bruce and Geifman15]. Additionally, DCCs for multisite studies must navigate organizational constraints, including variable institutional policies and contractual requirements, as well as cultural and national boundaries, that affect data access and sharing [Reference Austin12,Reference Gudi, Kamath and Chakraborty16,Reference Lidz, Pivovarova and Appelbaum17]. These challenges are further compounded by the need to integrate multidisciplinary expertise across clinical, statistical, and informatics expertise [Reference Austin12,Reference Ohmann, Banzi and Canham18].
Moreover, the COVID-19 pandemic accelerated the adoption of technological solutions across many multisite studies, including remote informed consent, patient engagement, decentralized data collection, virtual study operations, and artificial intelligence (AI) in diagnostic devices [Reference Cummins, Soni and Ivanova19]. This further expanded the scope of DCC responsibilities, requiring coordination of technology-enabled study workflows while navigating evolving regulatory requirements in patient recruitment and retention, intervention delivery, and data coordination [Reference Rosa, Marsch and Winstanley20,Reference Dorsey, Kluger and Lipset21]. As a result, these factors have contributed to increasingly complex study workflows, placing substantial organizational and operational demands on DCCs.
Despite the growing recognition of these challenges, the existing literature on DCCs remains fragmented, primarily confined to descriptions of individual studies or specific research programs. Although federal funders, such as the National Institutes of Health (NIH), have issued guidance outlining best practices for DCCs [22,23], these materials largely reflect the expectations and requirements rather than synthesized empirical experience from DCC practices. In particular, existing work has not systematically characterized the organizational and operational challenges DCCs face, nor how DCCs have adapted through changes in technology, governance, workflows, and infrastructure. Given the heterogeneous and evolving nature of the multisite studies DCCs coordinate, this gap warrants a scoping review to consolidate current evidence and experiences. By mapping reported challenges, solutions, and opportunities, this review aims to inform DCC practices that meet current demands and are positioned to adapt to evolving multisite research needs.
Objective and review question
The objective of this scoping review is to map existing knowledge and experiences on the organizational and operational aspects of DCCs in multisite studies. Specifically, we focus on two interrelated research questions: (i) What key organizational (e.g., governance, resources, workforce) and operational (e.g., data quality, compliance, workflow) challenges have been reported for DCCs? (ii) What solutions, best practices, and emerging technologies have been adopted by DCCs as contemporary adaptations to these challenges?
A preliminary search of PROSPERO, MEDLINE, the Cochrane Database of Systematic Reviews, Open Science Framework, and JBI Evidence Synthesis was conducted, and no current or in-progress scoping reviews or systematic reviews on the topic were identified.
Materials and methods
This rapid scoping review was conducted and reported in accordance with the PRISMA-ScR guidelines [Reference Tricco, Lillie and Zarin24], with a protocol registered on the Open Science Framework (osf.io/chtdw) [Reference Zhang, Lal and Kim25].
Eligibility criteria
Eligibility criteria were defined following the Population, Concept, and Context (PCC) framework. We included publications describing academic DCCs or equivalent entities with a centralized data management function, such as statistical coordinating centers and data management centers. We excluded disease registries, biobanks, and data repositories without active study coordination, as well as DCCs operated by commercial entities, such as contract research organizations.
The review focused on organizational and operational aspects of DCCs, including reported challenges, barriers, lessons learned, governance, compliance, collaboration, data quality, workforce development, and the adoption of emerging technologies. Publications limited to study protocols or methodological innovations without substantive discussion of DCC practice were excluded. Eligible articles described DCCs in multisite settings (with at least two clinical sites) on behalf of research consortia or clinical study networks. Studies limited to single-site, purely local settings or research networks without a specific study were excluded.
Publications reported in English between January 1, 2010, and August 31, 2025, were included. Peer-reviewed journal articles were eligible for inclusion. Editorials, letters, white papers, news briefs, and abstracts without full text were excluded.
Information sources and selection
Following a pilot test of eligibility criteria, we conducted a systematic search of PubMed (US National Library of Medicine), Scopus (Elsevier), and Web of Science Core Collection (Clarivate Analytics) to identify relevant publications. Full search strategies for each database are listed in the Supplementary Material. Reference lists of included reports were screened and searched manually to identify additional eligible publications. One author (YZ) conducted title and abstract screening, as well as full-text review, to identify potentially eligible records. To ensure the reliability of the screening process, any record whose eligibility was uncertain was elevated for full-text review and discussed with the research team. The screening was managed using Rayyan, a web-based systematic review management platform [Reference Ouzzani, Hammady and Fedorowicz26].
Data charting and synthesis
YZ, LSL, and SK conducted data charting using a data extraction form developed based on the DCC best practices checklist by the National Heart, Lung, and Blood Institute (NHLBI) [23]. YZ extracted data from all included sources, while LSL and SK independently charted subsets of sources, such that each source was charted by two reviewers. Multiple publications on the same DCC were combined into one entry to prevent duplication, with discrepancies resolved through research team discussions.
The data extraction form captured the following information: (1) source metadata (author, year, and journal), (2) study contextual information (country/region of study, research consortium/network, number of clinical sites, and funding source), (3) DCC characteristics (personnel components, organizational setting, and reported responsibilities), (4) challenges, adaptations, and technologies reported for each item outlined in the NHLBI DCC best practices checklist, categorized into four domains: Clinical Study/Trial Operations, Data Management, Quality Assurance/Quality Control, and Human Subjects Protections and Regulatory Affairs [23]. When information was unclear or insufficiently reported, this was documented rather than inferred.
Extracted data were summarized using descriptive tables to identify patterns in DCC characteristics, key challenges, and implemented adaptations across the four domains of NHLBI DCC best practices checklist [23]. To synthesize findings, a narrative synthesis was conducted to organize reported challenges and adaptations into broader organizational and operational categories, facilitating the identification of recurring challenges and potential opportunities.
Results
Document selection and characteristics
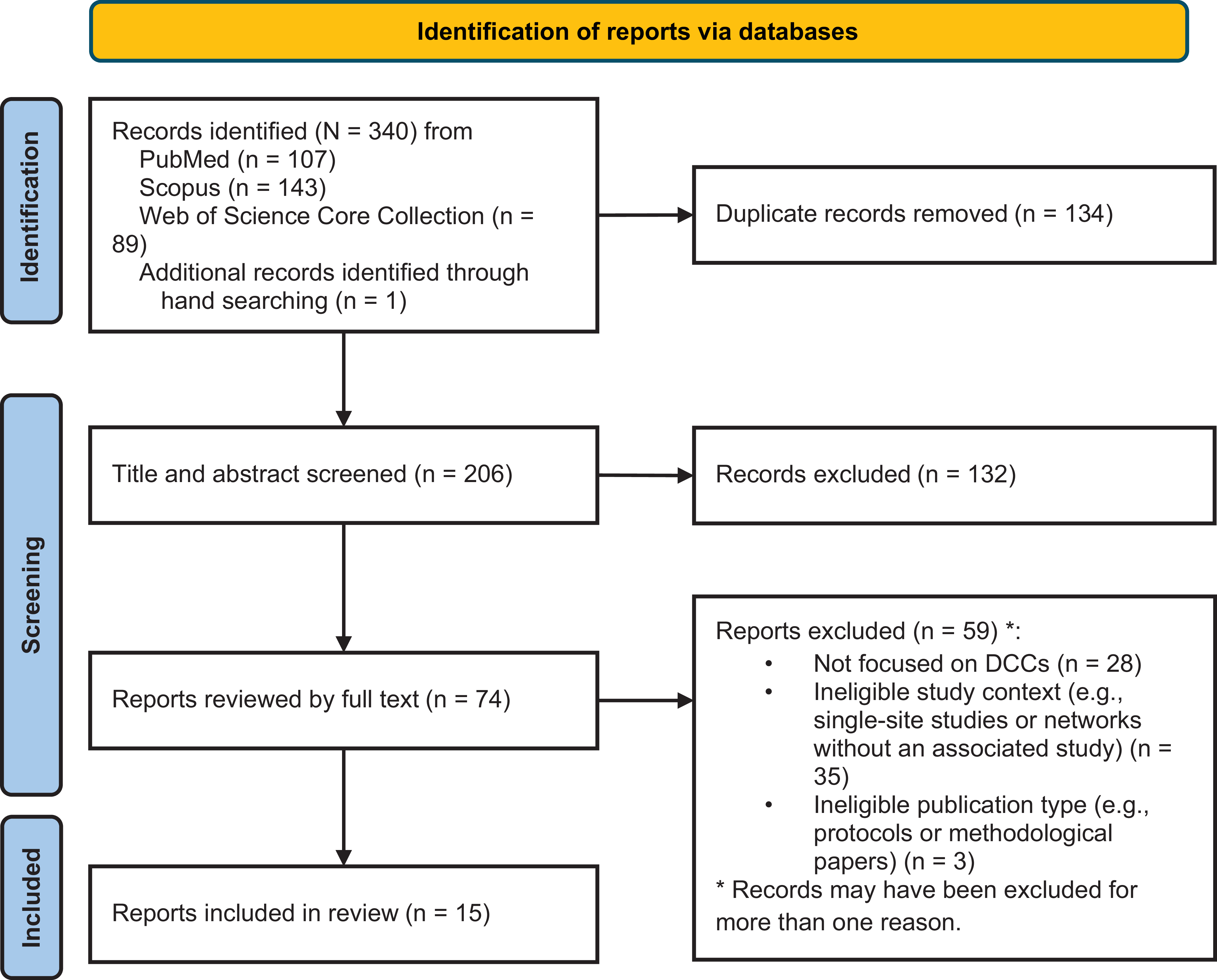
A total of 340 records were identified from PubMed (n = 107), Scopus (n = 143), Web of Science Core Collection (n = 89), and hand searching (n = 1). After deduplication, 206 records remained for title and abstract screening, of which 132 did not meet the inclusion criteria. Following a full-text review of the remaining 74 records, 59 ineligible reports were excluded for the following reasons: (i) not focused on DCCs (n = 28), (ii) ineligible study context, such as single-site studies or networks without an associated study (n = 35), and (iii) ineligible publication type, including protocols and methodological papers (n = 3). This resulted in the inclusion of 15 reports describing experiences from 16 DCCs, two of which described the same DCC [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28], and one that described three separate DCCs [Reference Cummins, Burr and Young29]. Figure 1 presents the PRISMA flow diagram for report selection [Reference Page, McKenzie and Bossuyt30].
PRISMA flowchart illustrating the search and selection process results for the scoping review.

Figure 1. Long description
The flowchart begins with the identification phase, where 340 records are identified from various databases: 107 from PubMed, 143 from Scopus, 89 from Web of Science Core Collection, and 1 additional record through hand searching. Duplicate records, totaling 134, are removed. The next phase involves screening titles and abstracts of 206 records, excluding 132 records. Reports are then reviewed by full text, with 74 reports assessed. In the final phase, 59 reports are excluded for various reasons: 28 not focused on Data Coordinating Centers, 35 with ineligible study context, and 3 with ineligible publication type. Ultimately, 15 reports are included in the review.
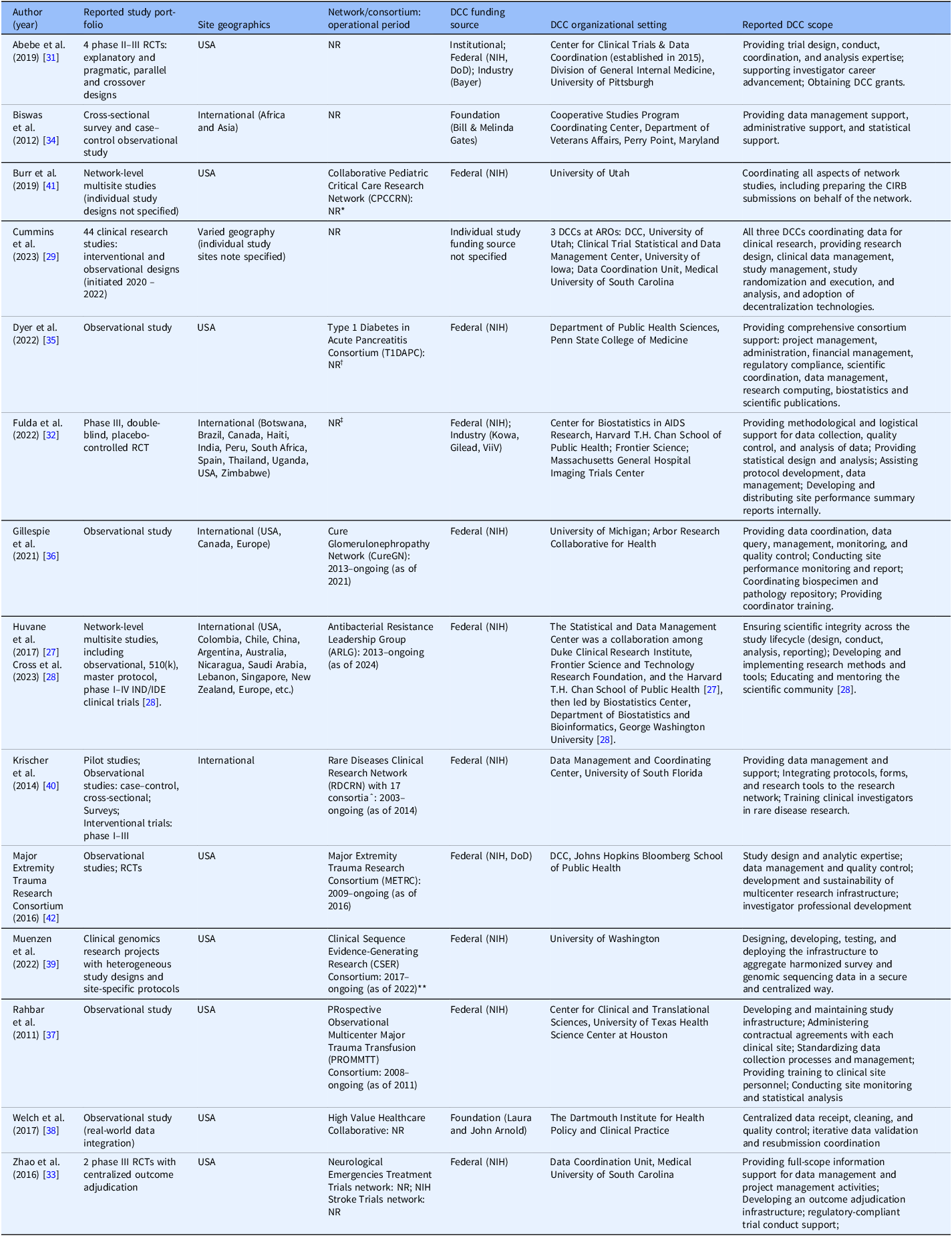
As summarized in Table 1, these DCCs support multisite clinical research across diverse study portfolios, organizational settings, and funding contexts. The study portfolios were heterogeneous, ranging from late-phase interventional trials, for example, phase III randomized clinical trials (RCTs) [Reference Abebe, Althouse and Comer31–Reference Zhao and Pauls33], and large-scale observational studies [Reference Biswas, Carty and Horney34–Reference Welch, von Recklinghausen and Taenzer38], to mixed portfolios encompassing both designs [Reference Huvane, Komarow and Hill27–Reference Cummins, Burr and Young29,Reference Muenzen, Amendola and Kauffman39,Reference Krischer, Gopal-Srivastava and Groft40]. Geographically, eight DCCs were based in the USA [Reference Abebe, Althouse and Comer31,Reference Zhao and Pauls33,Reference Dyer, Baab and Merchlinski35,Reference Rahbar, Fox and del Junco37–Reference Muenzen, Amendola and Kauffman39,Reference Burr, Johnson and Vasenina41,42], while five coordinated international studies across multiple continents [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28,Reference Fulda, Fichtenbaum and Kileel32,Reference Biswas, Carty and Horney34,Reference Gillespie, Laurin and Zinsser36,Reference Krischer, Gopal-Srivastava and Groft40]. Three DCCs described in one report did not specify their study locations [Reference Cummins, Burr and Young29].
Characteristics of DCCs described in the included reports

Table 1. Long description
A table comparing characteristics of Data Coordinating Centers (DCCs) in clinical research. The table has eleven rows and eight columns, detailing reported study design, site geography, network consortium, funding source, DCC organizational setting, DCC organizational structure, reported DCC scope, and references. Each row provides specific details for different DCCs, including study types such as phase III randomized clinical trials and large-scale observational studies, geographical locations ranging from the USA to international settings, and various funding sources. The table highlights the diversity in study portfolios, organizational settings, and funding contexts supported by these DCCs.
Note: RCT = randomized clinical trial; NIH = National Institute of Health; DCC = Data Coordinating Center; DoD = Department of Defense; CIRB = Centralized Institutional Review Board (IRB); ARO = Academic Research Organization; IND/IDE = Investigational New Drug and Investigational Device Exemption; SC = steering committee;, sIRB = single IRB.
* CIRB development initiated in 2012; full operational period not reported [Reference Burr, Johnson and Vasenina41].
†Recruitment started in 2022; full operational period not reported [Reference Dyer, Baab and Merchlinski35].
‡Enrollment started in 2015; full operational period not reported [Reference Fulda, Fichtenbaum and Kileel32].
ˆ17 consortia under the RDCRN: Angelman, Rett and Prader–Willi Syndromes Consortium, Autonomic Rare Diseases Clinical Research Consortium, Brain Vascular Malformation Consortium, Chronic Graft Versus Host Disease Consortium, Dystonia Coalition, Genetic Disorders Mucociliary Clearance Consortium, Inherited Neuropathies Consortium, Lysosomal Disease Network, Nephrotic Syndrome Study Network, North American Mitochondrial Disease Consortium, Porphyrias Consortium, Primary Immune Deficiency Treatment Consortium, Rare Kidney Stone Consortium, Salivary Gland Carcinomas Consortium, Salivary Gland Carcinomas Consortium, Sterol and Isoprenoid Diseases Consortium, Urea Cycle Disorders Consortium, Vasculitis Clinical Research Consortium. Operational period of each consortium not reported [Reference Krischer, Gopal-Srivastava and Groft40].
** The CSER phase 2 data coordination and analysis was operated between 2017 and 2023, with its DCC starting in 2019 [Reference Muenzen, Amendola and Kauffman39].
Among the 13 DCCs that reported funding sources, most reported experiences from federally funded research, including 11 supported by the NIH [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28,Reference Abebe, Althouse and Comer31–Reference Zhao and Pauls33,Reference Dyer, Baab and Merchlinski35–Reference Rahbar, Fox and del Junco37,Reference Muenzen, Amendola and Kauffman39–42] and two by the Department of Defense (DoD) [Reference Abebe, Althouse and Comer31,42]. In addition, two DCCs reported foundation funding [Reference Biswas, Carty and Horney34,Reference Welch, von Recklinghausen and Taenzer38], and two reported industry funding [Reference Abebe, Althouse and Comer31,Reference Fulda, Fichtenbaum and Kileel32]. One DCC also reported receiving initial institutional funding to support the infrastructure development [Reference Abebe, Althouse and Comer31]. Although all DCCs were situated within academic environments, organizational structures varied. Three DCCs were jointly operated by multiple institutions [Reference Huvane, Komarow and Hill27,Reference Fulda, Fichtenbaum and Kileel32,Reference Gillespie, Laurin and Zinsser36], while many were embedded within an institutional center that may concurrently coordinate multiple studies or research programs [Reference Huvane, Komarow and Hill27–Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31–Reference Biswas, Carty and Horney34,Reference Rahbar, Fox and del Junco37,Reference Krischer, Gopal-Srivastava and Groft40,42].
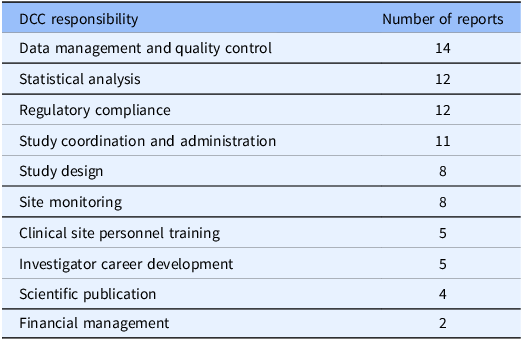
The reported responsibilities of these DCCs, as summarized in Table 2, extended beyond centralized data management. Although some reports focused on specific DCC functions and may not reflect the full scope of activities, DCC responsibilities consistently spanned the research lifecycle. Data management and quality control was the most commonly reported responsibility (n = 14) [Reference Huvane, Komarow and Hill27–Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31–Reference Krischer, Gopal-Srivastava and Groft40,42], followed by statistical analysis (n = 12) [Reference Huvane, Komarow and Hill27–Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31,Reference Fulda, Fichtenbaum and Kileel32,Reference Biswas, Carty and Horney34–Reference Rahbar, Fox and del Junco37,Reference Muenzen, Amendola and Kauffman39,Reference Krischer, Gopal-Srivastava and Groft40,42], regulatory compliance (n = 12) [Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31–Reference Rahbar, Fox and del Junco37,Reference Muenzen, Amendola and Kauffman39–42], and study coordination and administration (n = 11) [Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31,Reference Zhao and Pauls33–Reference Rahbar, Fox and del Junco37,Reference Muenzen, Amendola and Kauffman39–42]. Additional responsibilities included study design (n = 8) [Reference Huvane, Komarow and Hill27–Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31,Reference Fulda, Fichtenbaum and Kileel32,Reference Dyer, Baab and Merchlinski35,Reference Rahbar, Fox and del Junco37,42], site monitoring (n = 8) [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28,Reference Fulda, Fichtenbaum and Kileel32,Reference Dyer, Baab and Merchlinski35–Reference Rahbar, Fox and del Junco37,Reference Krischer, Gopal-Srivastava and Groft40,42], clinical site personnel training (n = 5) [Reference Dyer, Baab and Merchlinski35–Reference Rahbar, Fox and del Junco37,Reference Krischer, Gopal-Srivastava and Groft40,42], investigator career development (n = 5) [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28,Reference Abebe, Althouse and Comer31,Reference Krischer, Gopal-Srivastava and Groft40,42], scientific publication (n = 4) [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28,Reference Dyer, Baab and Merchlinski35,Reference Rahbar, Fox and del Junco37], and financial management (n = 2) [Reference Dyer, Baab and Merchlinski35,42].
Frequency of reported DCC responsibilities across included reports

Table 2. Long description
The table presents the frequency of reported DCC responsibilities across included reports. It consists of two columns and eleven rows. The first column lists the DCC responsibilities, and the second column shows the number of reports for each responsibility. The responsibilities include data management and quality control with fourteen reports, statistical analysis with twelve reports, regulatory compliance with twelve reports, study coordination and administration with eleven reports, study design with eight reports, site monitoring with eight reports, clinical site personnel training with five reports, investigator career development with five reports, scientific publication with four reports, and financial management with two reports.
Note: Some reports focused on specific DCC functions, so the responsibilities shown here may not reflect the full scope of activities performed by the DCC.
DCC = Data Coordinating Center.
Reported key challenges and adaptations
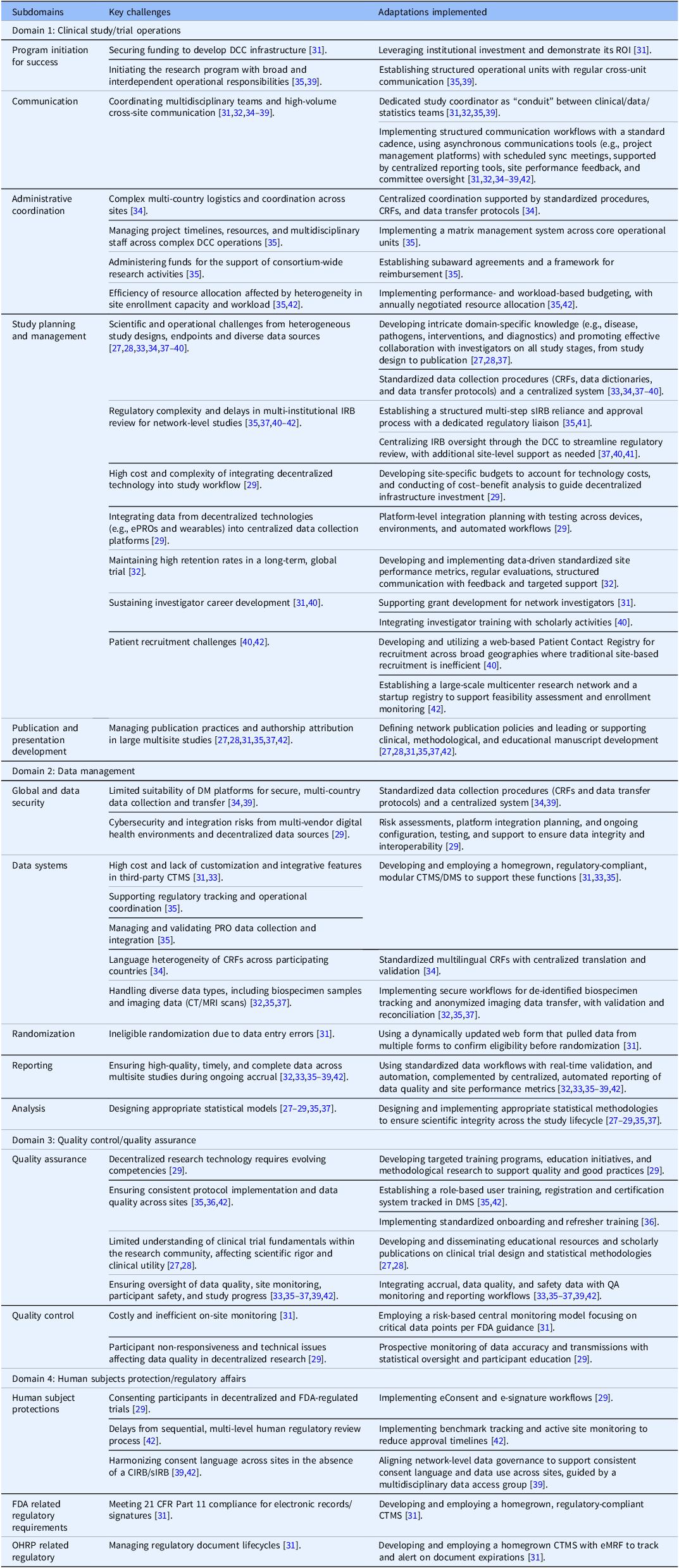
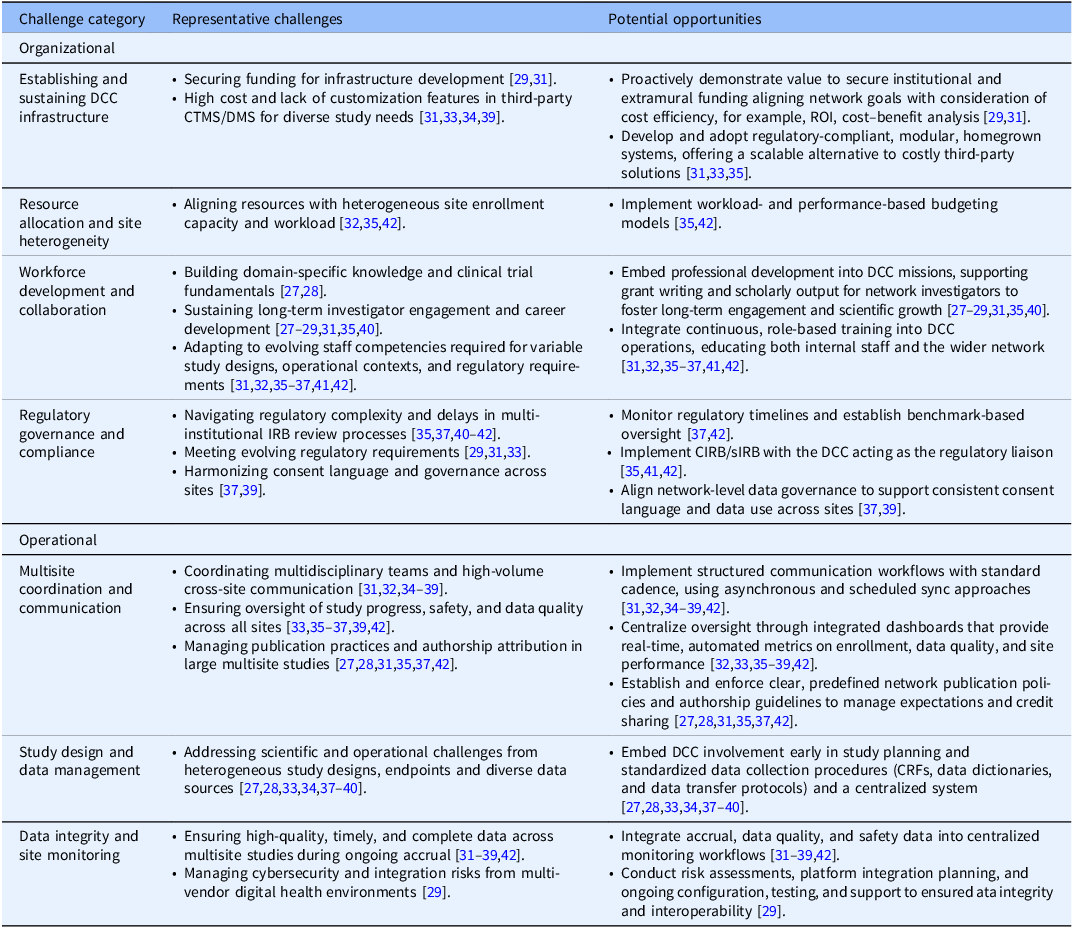
Table 3 presents a mapping of key DCC challenges and corresponding adaptations implemented across all included publications, aligned with the NHLBI domains and subdomains of the DCC best practices checklist [23]. Challenges were identified across all domains, with the clinical study and trial operations most commonly discussed. This mapping serves as a reference for DCCs encountering similar issues. Table 4 further synthesizes reported challenges into broader organizational and operational categories and distills the reported adaptations into forward-looking opportunities that DCCs may consider for future development and investment.
Key challenges and adaptations

Table 3. Long description
A table mapping key challenges and corresponding adaptations implemented across various publications, aligned with the NHLBI domains and subdomains of the DCC best practices checklist. The table highlights challenges identified in all domains, with a particular focus on clinical study and trial operations. It serves as a reference for Data Coordinating Centers encountering similar issues, and synthesizes reported challenges into broader organizational and operational categories, offering forward-looking opportunities for future development and investment.
ROI = return-on-investment; CIRB = Centralized Institutional Review Board (IRB); CRF = case report form; CTMS = clinical trial management system; eMRF = electronic master regulatory files; HRPP = Human Research Protection Program; DCC = Data Coordinating Center; DMS = data management system; ePRO = electronic patient-reported outcomes; OHRP = Office for Human Research Protection; CFR = Code of Federal Regulations.
Cross-domain synthesis of organizational and operational challenges and potential opportunities

Table 4. Long description
The table presents a detailed comparison of organizational and operational challenges and potential opportunities in DCC infrastructure. It includes categories such as establishing and sustaining DCC infrastructure, resource allocation, workforce development, regulatory governance, multisite coordination, study design, and data integrity. Each category lists representative challenges and potential opportunities. The table has multiple rows and columns, with headers indicating the challenge category, representative challenges, and potential opportunities. Notable trends include the need for securing funding, adapting to regulatory requirements, and implementing structured communication workflows.
CIRB = Centralized Institutional Review Board (IRB); CTMS = clinical trial management system; CRF = case report form; DCC = Data Coordinating Center; DMS = data management system; ROI = return-on-investment; sIRB = single IRB.
Organizational challenges and adaptations
At the organizational level, establishing and sustaining DCC infrastructure is a fundamental challenge, primarily due to the need to secure stable funding for infrastructure development and to the limited customization of third-party clinical trial management systems (CTMS) or data management systems (DMS) to meet diverse and evolving study needs [Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31,Reference Zhao and Pauls33,Reference Biswas, Carty and Horney34,Reference Muenzen, Amendola and Kauffman39]. Studies highlighted the importance of demonstrating institutional and network-level value through cost efficiency considerations to support long-term sustainability [Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31]. For example, the DCC at the University of Pittsburgh described intramural funding as supporting initial infrastructure development, with the expectation that the DCC would become self-sustaining through recurring projects over time [Reference Abebe, Althouse and Comer31]. As study needs evolve, DCCs often require continuous infrastructure enhancements, which may be constrained by limited budgets, underscoring the need for formal cost–benefit analyses to guide investment decisions [Reference Cummins, Burr and Young29]. Additionally, given the high cost and limited flexibility of commercial CTMS and DMS platforms [Reference Abebe, Althouse and Comer31,Reference Zhao and Pauls33,Reference Biswas, Carty and Horney34,Reference Muenzen, Amendola and Kauffman39], many DCCs reported developing and implementing regulatory-compliant, modular systems to support heterogeneous study portfolios [Reference Abebe, Althouse and Comer31,Reference Zhao and Pauls33,Reference Dyer, Baab and Merchlinski35]. The homegrown CTMS developed by the DCC at the University of Pittsburgh integrates multiple functional components, including electronic data capture, eligibility and randomization, drug and external data tracking, safety reporting, data and safety monitoring, statistical analysis and reporting, data sharing, and regulatory compliance [Reference Abebe, Althouse and Comer31]. Zhao and Pauls [Reference Zhao and Pauls33] described an outcome adjudication module within their homegrown CTMS. The DCC of the Type 1 Diabetes in Acute Pancreatitis Consortium (T1DAPC) also reported multiple core modules to meet study needs, including participant data and survey management, error tracking, document management, reimbursement tracking, sample tracking, and image data transmission [Reference Dyer, Baab and Merchlinski35].
Resource allocation is challenged by substantial heterogeneity in site environments, capacity, and workload. In coordinating a global trial, Fulda et al. highlighted geographic variation in personnel costs affecting site staffing and performance [Reference Fulda, Fichtenbaum and Kileel32]. In response, DCCs may consider implementing performance- and workload-based budgeting models. For example, the Major Extremity Trauma Research Consortium (METRC) negotiated budgets annually based on site performance and projected workload for the upcoming year [42], while the DMS used by the T1DAPC DCC overlays the visit structure defined in the study protocol with reimbursement rules to adjust payment and set grant limits, aligning payment with actual study activity and avoiding overpayment [Reference Dyer, Baab and Merchlinski35].
Workforce development represents another critical area for DCCs, encompassing both investigators and staff. For investigators, DCCs face challenges in building domain-specific knowledge and clinical trial fundamentals, as well as sustaining long-term investigator engagement and career development [Reference Huvane, Komarow and Hill27–Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31,Reference Dyer, Baab and Merchlinski35,Reference Krischer, Gopal-Srivastava and Groft40]. For staff members, DCCs must adapt to evolving competency requirements driven by diverse study designs, operational contexts, and regulatory requirements [Reference Abebe, Althouse and Comer31,Reference Fulda, Fichtenbaum and Kileel32,Reference Dyer, Baab and Merchlinski35–Reference Rahbar, Fox and del Junco37,Reference Burr, Johnson and Vasenina41,42]. Across included studies, reported adaptations pointed to opportunities to embed professional development into DCC missions, supporting grant writing and scholarly output for network investigators to foster long-term engagement and scientific growth [Reference Huvane, Komarow and Hill27–Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31,Reference Dyer, Baab and Merchlinski35,Reference Krischer, Gopal-Srivastava and Groft40]. For example, the Antibacterial Resistance Leadership Group (ARLG) DCC emphasized developing statistical methodology and disseminating educational resources to the scientific community [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28]. For staff members, DCCs may consider integrating continuous, role-based training and certification into their operations to ensure competency and protocol adherence across sites [Reference Abebe, Althouse and Comer31,Reference Fulda, Fichtenbaum and Kileel32,Reference Dyer, Baab and Merchlinski35–Reference Rahbar, Fox and del Junco37,Reference Burr, Johnson and Vasenina41,42]. The T1DAPC DCC embedded training and certification within its DMS to ensure that study activities were performed only by certified staff [Reference Dyer, Baab and Merchlinski35].
DCCs also face regulatory and governance challenges, particularly in multi-institutional and multinational IRB processes, evolving regulatory requirements, and heterogeneity in consent language and governance across sites [Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31,Reference Zhao and Pauls33,Reference Dyer, Baab and Merchlinski35,Reference Rahbar, Fox and del Junco37,Reference Muenzen, Amendola and Kauffman39–42]. Reports highlighted adaptations such as benchmark-based monitoring of regulatory approval timelines [Reference Rahbar, Fox and del Junco37,42], the use of centralized IRB (CIRB) or single IRB (sIRB) models with the DCC acting as a regulatory liaison [Reference Dyer, Baab and Merchlinski35,Reference Burr, Johnson and Vasenina41,42], and the development of harmonized, network-level data governance frameworks to promote consistency in consent language and data use across sites [Reference Rahbar, Fox and del Junco37,Reference Muenzen, Amendola and Kauffman39].
Operational challenges and adaptations
At the operational level, DCCs commonly reported challenges related to multisite coordination and communication, such as managing high-volume cross-site communication [Reference Abebe, Althouse and Comer31,Reference Fulda, Fichtenbaum and Kileel32,Reference Biswas, Carty and Horney34–Reference Muenzen, Amendola and Kauffman39], oversight of study progress, safety, and data quality [Reference Zhao and Pauls33,Reference Dyer, Baab and Merchlinski35–Reference Rahbar, Fox and del Junco37,Reference Muenzen, Amendola and Kauffman39,42], and managing publication practices and authorship attribution across research networks [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28,Reference Abebe, Althouse and Comer31,Reference Dyer, Baab and Merchlinski35,Reference Rahbar, Fox and del Junco37,42]. Across studies, implemented adaptations suggest opportunities to formalize communication workflows with standardized cadence, integrate asynchronous tools (e.g., email and project management platforms such as Basecamp) with scheduled synchronization to support consensus-building across sites, and use integrated dashboards to centralize real-time oversight of enrollment, data quality, and site performance [Reference Abebe, Althouse and Comer31–Reference Muenzen, Amendola and Kauffman39,42]. The emphasis on experienced study coordinators as central points of contact further indicates the importance and challenge of coordination roles in bridging multidisciplinary teams and heterogeneous site environments [Reference Abebe, Althouse and Comer31,Reference Fulda, Fichtenbaum and Kileel32,Reference Dyer, Baab and Merchlinski35,Reference Muenzen, Amendola and Kauffman39]. The matrix management system adopted by the T1DAPC DCC facilitates cross-unit communication within the DCC and project timeline management [Reference Dyer, Baab and Merchlinski35]. Additionally, the commonly adopted predefined publication policies and authorship guidelines underscore the importance of proactively managing the expectations and accountability for scholarly outputs [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28,Reference Abebe, Althouse and Comer31,Reference Dyer, Baab and Merchlinski35,Reference Rahbar, Fox and del Junco37,42].
Operational challenges related to study design and data management are primarily driven by heterogeneity in study designs, endpoints, and data sources across multisite research networks, creating both scientific and operational complexity for DCCs [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28,Reference Zhao and Pauls33,Reference Biswas, Carty and Horney34,Reference Rahbar, Fox and del Junco37–Reference Krischer, Gopal-Srivastava and Groft40]. These challenges underscore opportunities for early and continuous DCC engagement to ensure methodological alignment and data harmonization. Specifically, reported adaptations highlight the use of centralized systems and standardized data collection tools, such as the development of case report forms (CRFs), data dictionaries, and data transfer protocols [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28,Reference Zhao and Pauls33,Reference Biswas, Carty and Horney34,Reference Rahbar, Fox and del Junco37–Reference Krischer, Gopal-Srivastava and Groft40]. Muenzen et al. further highlighted the importance of planning and budgeting for data coordination activities as early as possible to minimize downstream complications [Reference Muenzen, Amendola and Kauffman39]. When CRFs cannot be implemented, for example, data collection through electronic health records (EHRs), data specification documents were developed to define key elements, including case definitions, to support data consistency across sites [Reference Welch, von Recklinghausen and Taenzer38].
Moreover, ensuring protocol adherence requires high-quality, timely, and complete data during ongoing accrual, which poses another persistent operational challenge [Reference Fulda, Fichtenbaum and Kileel32,Reference Zhao and Pauls33,Reference Dyer, Baab and Merchlinski35–Reference Muenzen, Amendola and Kauffman39,42]. To address this, DCCs commonly develop centralized monitoring workflows that integrate accrual metrics, data quality indicators, and safety information [Reference Abebe, Althouse and Comer31,Reference Fulda, Fichtenbaum and Kileel32,Reference Biswas, Carty and Horney34–Reference Muenzen, Amendola and Kauffman39,42]. Such monitoring approaches are often implemented alongside adaptations for multisite coordination and communication [Reference Abebe, Althouse and Comer31,Reference Fulda, Fichtenbaum and Kileel32,Reference Biswas, Carty and Horney34–Reference Muenzen, Amendola and Kauffman39,42]. Furthermore, the adoption of decentralized technologies introduces distinct cybersecurity and data integration risks from multi-vendor digital health environments, posing data security challenges [Reference Cummins, Burr and Young29]. Mitigating these risks requires proactive technology governance, including risk assessments, platform integration planning, and ongoing configuration, testing, and technical support to ensure data integrity and interoperability from the local device to the central data infrastructure [Reference Cummins, Burr and Young29].
Discussion
In this scoping review, we synthesized published experiences from academic DCCs supporting multisite research and identified recurring organizational and operational challenges, corresponding adaptations, and emerging opportunities. In addition to their traditional coordination functions, many DCCs play leadership roles within consortia, particularly in facilitating data sharing, dissemination of results, and broader outreach activities. Accordingly, our findings highlight the expanding scope of DCC responsibilities and underscore the need for adaptive coordination that integrates governance, technology, and workforce capacity to support contemporary multisite clinical and translational studies.
At its core, the primary role of DCCs is to function as the central hub for communication and coordination across geographically dispersed studies. Effective coordination is foundational to consistent protocol implementation and adherence. Across the reviewed studies, this coordinating function has been increasingly supported by standardized workflows, centralized data platforms, and shared monitoring systems that collectively facilitate communication, data management, and site oversight. Notably, substantial heterogeneity in study designs, site capabilities, data sources, and regulatory environments was consistently reported, precluding a one-size-fits-all model for DCCs. In response, many DCCs have developed and adopted modular or scalable approaches that integrate components and leverage existing tools, rather than relying on a single comprehensive platform [Reference Abebe, Althouse and Comer31,Reference Zhao and Pauls33–Reference Dyer, Baab and Merchlinski35]. Such strategies allow DCCs to tailor infrastructure to meet study-specific needs while maintaining reproducible operational processes. Beyond the included literature, a recent report described a cost-effective, regulatory-compliant safety case management workflow that replaced specialized pharmacovigilance software that was incompatible with other clinical research software and required an annual license fee, thereby illustrating the value of workflow redesign to improve interoperability, efficiency, and effectiveness, while maintaining compliance [Reference Burson, Walter and Auman43].
Beyond coordination, regulatory governance represents a critical responsibility of DCCs. Navigating multi-institutional ethics review processes, meeting evolving regulatory requirements and standards (e.g., 21 CFR Parts 11 and 312, and ICH E6), and harmonizing consent language and data use across sites were commonly reported challenges [Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31,Reference Zhao and Pauls33,Reference Dyer, Baab and Merchlinski35,Reference Rahbar, Fox and del Junco37,Reference Muenzen, Amendola and Kauffman39–42]. Differences in funder requirements, state and institutional policies, and interoperability constraints across technology platforms at participating sites can make each DCC’s human-subjects protection landscape unique. In response, DCCs have spearheaded efforts to streamline compliance through developing CIRB or sIRB processes with the DCC as the regulatory liaison [Reference Dyer, Baab and Merchlinski35,Reference Burr, Johnson and Vasenina41,42], benchmarking regulatory timelines [Reference Rahbar, Fox and del Junco37,42], and aligning network-level data governance [Reference Rahbar, Fox and del Junco37,Reference Muenzen, Amendola and Kauffman39]. These governance structures not only supported regulatory compliance but also facilitated a more efficient study startup.
Technological advances present both opportunities and demands in conducting multisite studies. Technology-enabled workflows offer greater flexibility in coordination, communication, and data management [Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31–Reference Biswas, Carty and Horney34,Reference Rahbar, Fox and del Junco37,Reference Muenzen, Amendola and Kauffman39,Reference Krischer, Gopal-Srivastava and Groft40,42], and decentralized approaches, such as telemedicine, wearable devices, electronic patient-reported outcomes (ePROs), online recruitment portals, and eConsent, have extended engagement with populations that were previously hard to reach [Reference Cummins, Burr and Young29,Reference Krischer, Gopal-Srivastava and Groft40]. For example, telemedicine allows health services to be delivered to participants at remote locations without transportation, while wearable devices facilitate real-time patient monitoring and data collection [Reference Cummins, Soni and Ivanova19,Reference Cummins, Burr and Young29,Reference Zhang, Lin and Lal44]. However, these advances also introduce new operational demands, including increased requirements for data validation, system integration, cybersecurity, and regulatory oversight. For example, ePROs allow participants to report outcome data directly through web- or mobile-based applications, introducing additional requirements for data validation and quality control, while eConsent, which digitizes the informed consent process, must meet regulatory and compliance standards [Reference Cummins, Soni and Ivanova19,Reference Cummins, Burr and Young29]. These challenges underscore the need for DCCs to adapt their infrastructure, governance, and operational capacity to keep pace with evolving study needs. In this context, careful consideration of efficiency and cost efficiency becomes increasingly important when academic DCCs invest in and upgrade underlying infrastructure to support technology-enabled study workflows.
Ultimately, the ability of DCCs to ensure scientific integrity in large multisite clinical studies also depends on the strength and integration of their multidisciplinary workforce and the broader scientific community they engage with. As modern studies become more complex, expanding regulatory requirements and rapidly evolving data systems, combined with the enduring importance of methodological rigor, place increasing demands on workforce competence and statistical and methodological expertise [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28,Reference Freel, Snyder and Bastarache45,Reference Cagnazzo, Testoni and Speranza46]. Our review highlighted the critical role of experienced clinical research professionals in facilitating effective communication among multidisciplinary teams and across multiple sites [Reference Abebe, Althouse and Comer31,Reference Fulda, Fichtenbaum and Kileel32,Reference Dyer, Baab and Merchlinski35,Reference Muenzen, Amendola and Kauffman39]. It also underscored the importance of ongoing, role-based training and support for DCC internal staff and the wider research network [Reference Abebe, Althouse and Comer31,Reference Fulda, Fichtenbaum and Kileel32,Reference Dyer, Baab and Merchlinski35–Reference Rahbar, Fox and del Junco37,Reference Burr, Johnson and Vasenina41,42]. These findings align with prior work emphasizing the need to strengthen competencies among clinical research professionals who support clinical studies, including the development of competency-based frameworks, educational curricula, and mentorship programs [Reference Knapke, Jenkerson and Tsao47–Reference Samuels, Champagne and Lyden50]. Meanwhile, ensuring scientific rigor among DCC-supported research requires continued development and dissemination of statistical and methodological expertise, particularly as study designs, informatics, and analytic expectations evolve [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28]. Moreover, several reviewed DCCs emphasized the importance of engaging network investigators in manuscript and grant development [Reference Huvane, Komarow and Hill27–Reference Cummins, Burr and Young29,Reference Abebe, Althouse and Comer31,Reference Dyer, Baab and Merchlinski35,Reference Krischer, Gopal-Srivastava and Groft40]. This involvement not only promotes investigator career growth and ongoing engagement within the network but also reinforces the continuity of network research by creating a pipeline of investigators who continue to advance and expand the scientific agenda. Together, investments in workforce competence and methodological capacity enable DCCs to adapt to evolving research environments while maintaining scientific quality and supporting the continuity of network research.
Looking ahead, the role of DCCs is likely to further evolve with the rapid advancement of emerging technologies, including AI, robotics, and automation [Reference Rosa, Marsch and Winstanley20,Reference Kamel51]. These technologies are increasingly being integrated into biospecimen processing, medical devices, decentralized trials, and broader study infrastructure [Reference Rosa, Marsch and Winstanley20,Reference Dorsey, Kluger and Lipset21,Reference Unadkat, Gupta, Vinod, Gupta and Chaudhary52], contributing to growing complexity and heterogeneity in multisite research. In this context, DCCs will need to remain adaptive, developing robust workflows and infrastructure while meeting the regulatory requirements. DCC and clinical site workforce development will be essential to support the effective integration of emerging technologies in study implementation and DCC workflows. Moreover, academic DCCs are well positioned to contribute to the development of best practices and to work closely with investigators to translate emerging scientific and technological advances into practical research evidence. Collaborative initiatives such as the UNIversity data COoRdinating ceNters (UNICORN) Network provide an example of how academic DCCs can align efforts to support innovation, standardization, and knowledge sharing across institutions [53].
Limitations
This scoping review has several limitations. First, as a rapid scoping review, this study prioritized breadth and timeliness over exhaustive coverage. Although multiple databases were searched and reference lists were screened, relevant reports, particularly unpublished experiences, internal reports, or gray literature describing DCC practices, were not captured. Second, the included literature was heterogeneous in study context, scope, and level of detail, and all reports were descriptive. For example, reported DCC responsibilities varied depending on research network structures, particularly when clinical coordination was managed by entities separate from the DCC [Reference Huvane, Komarow and Hill27,Reference Cross, Greenwood-Quaintance and Souli28]. Third, our synthesis relied on reported experiences. Although the NHLBI DCC best practices checklist was used to guide data collection [23], the extracted data reflect the focus and scope of published reports and may not fully capture the complexity of day-to-day challenges or the implementation of adaptations in practice. This may introduce publication bias, whereby certain operational challenges are underrepresented. For example, cross-institutional email distribution may be unreliable due to evolving institutional email security policies, requiring an alternative communication infrastructure to ensure consistent coordination among teams. Such challenges are commonly encountered in the multi-institutional coordination but not described in the reviewed reports.
Conclusions
Multisite clinical studies emerged to generate robust evidence but quickly revealed the need for dedicated coordination, giving rise to DCCs as the “hub around which various clinical centers must revolve.” [Reference Greenberg2,Reference Cook and DeMets4–Reference DuChene, Hultgren and Neaton8,Reference Boyle, Fortner and Chinchilli54,Reference Overton55] As regulatory, technological, and methodological complexity have evolved, DCC responsibilities have expanded beyond centralized data management to encompass comprehensive study coordination, governance, and scientific support. In response to this evolution, this rapid scoping review synthesizes published experiences to characterize how academic DCCs have adapted. Our findings underscore the importance of adapting to study heterogeneity through modular infrastructure solutions, centralized and standardized workflows, proactive governance, and workforce investment, which is critical to operational feasibility and scientific integrity of contemporary multisite research.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cts.2026.10755.
Acknowledgments
During the preparation of this work, the first author used ChatGPT-5.1 and Grammarly to improve the readability and language of the manuscript. After using these tools, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Author contributions
Yunxi Zhang: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Validation, Visualization, Writing – original draft, Writing – review & editing; Lincy Lal: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – review & editing; Soeun Kim: Data curation, Formal analysis, Investigation, Validation, Writing – review & editing; John Michael Swint: Conceptualization, Investigation, Methodology, Writing – review & editing; David T. Mauger: Conceptualization, Investigation, Validation, Writing – review & editing; Aimee Merchlinski: Investigation, Validation, Writing – review & editing; Paula A. Valencia: Investigation, Validation, Writing – review & editing; Beth R. Holmes: Investigation, Validation, Writing – review & editing; Brenda Phillips: Investigation, Validation, Writing – review & editing; Kendall Thomas Baab: Investigation, Validation, Writing – review & editing; Vernon M. Chinchilli: Conceptualization, Investigation, Methodology, Supervision, Validation, Writing – review & editing.
Funding statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
All authors declare none.



 Open access
Open access