


The UK academic psychiatry workforce has contracted substantially over past two decades, reducing the profession’s capacity to lead innovation, train future clinicians, influence policy and translate scientific advances into clinical practice. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1–Reference Craddock, Antebi, Attenburrow, Bailey, Carson and Cowen3 A good example is the recent study highlighting the fact that, despite increased policy attention and funding for young people’s mental health, child and adolescent psychiatry remains markedly underrepresented academically compared with neurology despite similar specialist workforce numbers, with consequences for research, training, innovation and service development. Reference Kelleher, Poziemska, Kieseppä, Thapar, Dubicka and Lockhart4
In this paper, the Royal College of Psychiatrists’ (RCPsych) Academic Psychiatry Strategy (‘strategy’) defines a coordinated national recovery plan, suggesting specific recommendations which, although possibly challenging to implement, are essential for our discipline to underpin the future of our profession.
A Lancet Commission highlighted that mental disorders contribute an increasing share of the global disease burden, yet mental health research remains severely underfunded. Despite the growing impact of mental illness, investment in mental health research continues to lag far behind both the scale of the problem and funding levels for other major diseases. Reference Patel, Saxena, Lund, Thornicroft, Baingana and Bolton5
Simultaneously, the UK academic psychiatry workforce has contracted substantially, with the total number of full-time-equivalent psychiatrists employed by medical schools declining by over a third over the past two decades. 6 The decline of UK academic psychiatry is especially worrying at a time when advances in neuroscience, digital health, precision medicine, artificial intelligence, genomics and real-world data science are creating major global opportunities for scientific transformation. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1 This decline is driven by interconnected and reinforcing barriers, including low grant application rates among academic psychiatrists, limited research training opportunities, increasing administrative burdens, National Health Service (NHS) service pressures that restrict research time and insufficient university support and resources. Together, these structural, institutional and workforce-related challenges limit the capacity of psychiatrists to actively engage in research, and risk UK psychiatry falling behind in major developments in science and technology. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1
This Editorial examines the College academic strategy in the light of these challenges. The strategy seeks to create a sustainable framework for rebuilding academic psychiatry across the UK and is accordingly structured around seven pillars: (a) workforce and careers, (b) training and pipeline development, (c) funding and research impact, (d) regional networks, (e) diversity and mentorship, (f) innovation and translation and (g) governance and accountability. Importantly, the strategy recognises that academic psychiatry cannot remain confined to just a few tenured academics or a small number of traditional centres of institutional concentration. Instead, it proposes a broader national ecosystem of research-active services, networked collaborations and equitable academic opportunity across region, grades, gender and ethnicity.
Why academic psychiatry matters
Academic psychiatry is not a niche adjunct to clinical practice: it is a fundamental part of psychiatry for the advancement of mental healthcare. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1 Clinical academics bridge scientific discovery, critical appraisal, education, service delivery and policy. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1 They train medical students and resident doctors, develop and test interventions, lead clinical trials, influence national guidance and facilitate translation of evidence into practice.
Research-active, learning healthcare systems consistently demonstrate better patient outcomes, improved staff recruitment and retention, strengthening of organisational cultures and enhanced innovation. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1,6 Academic psychiatrists also play a pivotal role in reducing stigma around mental illness by embedding psychiatry within mainstream scientific medicine.
Recent literature has highlighted the decline of posts in this specialty, which affects not only universities and research institutions but also the entire mental health system. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1 The number of full-time academic psychiatrists in the UK declined from approximately 330 in 2004 to just over 200 by 2023. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1 This reduction has occurred despite increasing medical school and student numbers, rising mental health demand, escalating complexity within psychiatric practice and growing mental healthcare resource pressures. The consequences of reduced academic capacity extend into workforce recruitment, quality of training, updating plus implementation of evidence-based care and the ability of psychiatry to compete for research investment. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1
The concern is long-standing. A ‘wake-up call for British psychiatry’ nearly two decades ago, warning that academic psychiatry faced structural collapse without decisive interventions, was not undertaken. Reference Craddock, Antebi, Attenburrow, Bailey, Carson and Cowen3 The result is a paradoxical situation in which the need for psychiatric research and academic leadership has grown, although the workforce responsible for delivering it has diminished.
Why the decline persists
Part of the decline reflects societal factors, including persistent underinvestment in mental health research, stigma surrounding mental illness and the complexity of psychiatry’s scientific identity compared with other medical specialties. Psychiatry works at the intersection of medicine, psychology, sociology, philosophy and law, making its scientific identity more contested and less easily reducible to conventional biomedical models than many other specialties. Although this plurality is a strength, it has also contributed to ambivalence towards academic medicine and weakened the integration of research within routine psychiatric practice.
However, part of the paradox also lies within the profession itself. Some psychiatrists strongly identify with neuroscience, translational medicine and quantitative research whereas others prioritise psychotherapeutic, social, cultural or phenomenological approaches to mental distress. Unlike many medical specialties, psychiatry has not always reached consensus, including within parts of the RCPsych, that research, particularly biologically or technologically driven research, should be central to the profession’s future. This has created a self-reinforcing cycle: when research is seen as peripheral to clinical psychiatry, academic careers become less attractive and visible, weakening research culture, mentorship, scientific confidence and institutional influence. NHS service pressures have further widened this divide by framing research as optional rather than integral to high-quality care. Doctors should be encouraged to undertake research in the same way they are expected to complete audits, a point that the General Medical Council (GMC) has highlighted clearly.
Importantly, this is not simply a workforce problem but a cultural and structural one. The ‘treatment’ therefore cannot rely solely on increasing funding or creating more academic posts. It requires reintegration of scientific inquiry into the professional identity of psychiatry itself while preserving the specialty’s biopsychosocial breadth. The strategy therefore implicitly represents not only a workforce recovery plan, but also a cultural repositioning of psychiatry: reframing research, innovation and critical inquiry as core components of psychiatric practice rather than as optional academic pursuits undertaken by a small minority.
Why the strategy is needed now
Several converging pressures explain why the current moment is particularly critical.
First, the academic workforce pipeline is fragile. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1 Academic career pathways remain difficult to navigate, especially for early-career psychiatrists attempting to balance research, training and clinical responsibilities. Limited protected time, insecure funding pathways and the perception that academic careers are incompatible with work–life balance all deter recruitment.
Second, there are significant inequities in participation and representation. Reference Hassiotis, Sinclair, Lingford Hughes, Young, Korszun and Lagunes-Cordoba7 Clinicians from minoritised groups, such as women and those from ethnic backgrounds, as well as specialty and specialist doctors and psychiatrists with caring responsibilities, continue to encounter barriers to progression. The importance of structured, solution-focused approaches to supporting women in academic psychiatry, emphasising mentorship, sponsorship, flexibility and structural reform, is neglected. Reference Hassiotis, Sinclair, Lingford Hughes, Young, Korszun and Lagunes-Cordoba7 Without targeted intervention, the academic workforce risks becoming progressively narrower and even less representative.
Third, academic activity remains geographically concentrated. Reference Laugharne, Tracy, Bhugra and Shankar8 The Oxford–Cambridge–London ‘golden triangle’ dominates research infrastructure and funding. These internationally recognised centres remain essential, but large parts of the country still lack meaningful participation in psychiatric research, requiring proactive strategies for geographic inclusion and ‘levelling-up’.
Fourth, psychiatry faces increasing competition for research investment. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1 Mental health research remains underfunded relative to disease burden, whereas pharmaceutical investment in psychiatric therapeutics has historically lagged behind areas such as oncology and cardiovascular medicine. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1 Without strong academic leadership and coordinated advocacy, psychiatry risks further marginalisation.
Finally, psychiatry is now entering a transformative scientific era. Reference Shankar, Terry, James, Laugharne, Ali and Anil9 Advances in artificial intelligence, digital therapeutics, biomarkers, computational psychiatry and precision medicine require robust academic infrastructure capable of evaluating innovation safely, ethically and rigorously. Reference Shankar, Terry, James, Laugharne, Ali and Anil9 Without a strong academic base, psychiatry risks becoming a passive recipient rather than an active leader in these developments.
What the strategy proposes
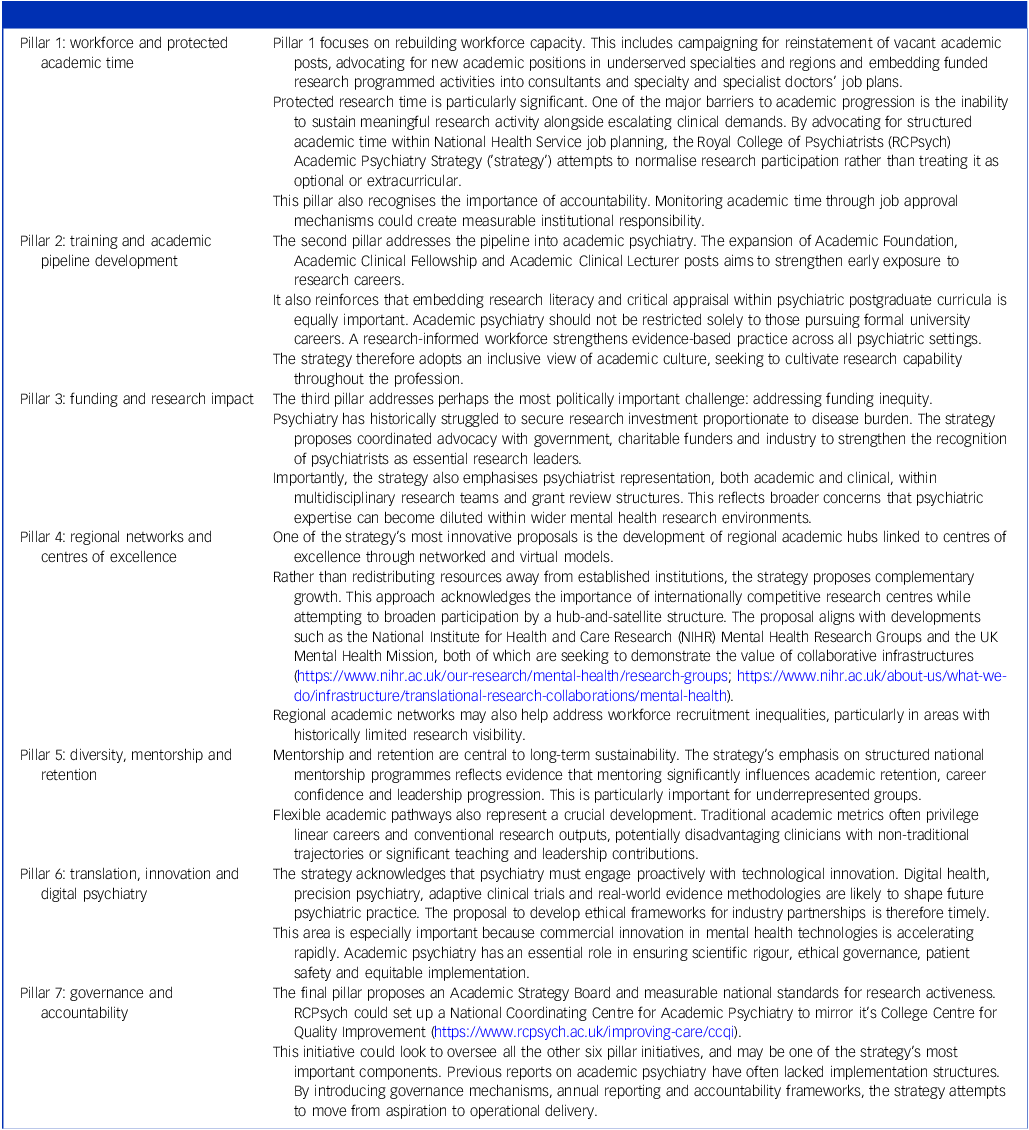
The RCPsych strategy proposes to move beyond problem description towards system-wide implementation. Table 1 describes the seven pillars of the strategy. Supplementary Information 1 provides an example of implementation.
The seven pillars of the RCPsych Academic Strategy

The strategy’s principal strength lies in its breadth and coherence; rather than focusing solely on workforce numbers, it recognises academic psychiatry as an interconnected ecosystem involving training, mentorship, infrastructure, diversity, regional collaboration, innovation and leadership. Importantly, it balances ambition with pragmatism by building on existing structures within the College, The National Institute for Health and Care Research (NIHR) and universities, while also positioning psychiatry within emerging fields such as digital health, artificial intelligence and translational science. The emphasis on inclusion, regional equity and the framework known as ‘outcome, situation, choices, actions, review’ further strengthens the strategy by framing sustainability as dependent on opportunity, support, capability, accountability and representation. However, implementation will be challenging. Many proposals require sustained funding, protected research time and long-term institutional commitment at a time of considerable NHS workforce pressure. Success will also depend on effective coordination among universities, NHS organisations, funders and regulators, with the additional risk that poorly resourced expansion could inadvertently widen existing inequalities. As with many long-term workforce strategies, outcomes may take years to materialise and there remains a danger that, without clear accountability and sustained momentum, the vision may become diffuse and fail to translate into meaningful change.
Implementation of the RCPsych strategy
As stated at the outset, the ‘wake-up’ time is now and rebuilding academic psychiatry cannot be deferred any longer. Through the seven pillars, there will be immediate opportunities that can be built upon. However, if this is not enacted in a timely manner, and in the manner we have suggested, we fear that there will be significant problems ahead.
If implemented effectively, the strategy could have transformative results for psychiatry. A revitalised academic workforce could improve recruitment into psychiatry by increasing visibility, prestige and intellectual appeal, because exposure to research-active environments is associated with greater trainee engagement and career satisfaction. Reference Shankar, Bowater, Laugharne, Tracy, Critchley and Young1–Reference Craddock, Antebi, Attenburrow, Bailey, Carson and Cowen3
Improved academic infrastructure could strengthen the UK’s international leadership in psychiatric research at a time when global mental health demand is increasing rapidly. The strategy may also help position psychiatry more centrally within integrated healthcare systems, neuroscience and digital medicine.
Importantly, stronger academic psychiatry could accelerate the translation of innovation into clinical care. Advances in biomarkers, digital therapeutics, predictive analytics and personalised interventions require clinically informed psychiatric leadership. Additionally, improved psychiatric research capacity may contribute to reduced stigma, better public understanding of mental illness and more effective policy development, maintaining that intersectionality and plurality key to psychiatry.
The consequences of inaction may be profound. Without intervention, academic psychiatry posts and infrastructure are likely to continue declining. Workforce ageing, combined with insufficient recruitment, may create irreversible losses in expertise and mentorship. The UK risks losing international competitiveness in psychiatric science, which has historically contributed to its world-leading position in health and life science research.
Clinical services may also suffer indirectly. Reduced academic leadership will weaken evidence implementation, quality improvement and innovation within NHS systems. Failure to diversify the academic workforce risks perpetuating inequities in leadership and research priorities.
Perhaps most significantly, psychiatry itself risks marginalisation within medicine. Academic visibility strongly influences specialty prestige, undergraduate exposure and policy influence. A weakened academic base may reinforce misconceptions that psychiatry is less scientific or less innovative than other specialties.
Academic psychiatry is essential to ensuring that psychiatry remains scientifically rigorous, clinically innovative and relevant to future healthcare needs. To secure investment in an increasingly competitive funding environment, academic psychiatry must also demonstrate measurable clinical impact, innovation and entrepreneurial value, as should all areas of medical research.
The RCPsych strategy represents the first comprehensive attempt to address the long-standing crisis in UK academic psychiatry. It acknowledges that workforce decline, funding inequity, regional imbalance and barriers to inclusion are interconnected challenges requiring coordinated solutions.
Importantly, the strategy also reframes academic psychiatry as central to the future of clinical care rather than peripheral to it, in keeping with recent shifts in GMC perspectives and psychiatric training curricula requirements. In an era defined by digital transformation, precision medicine and escalating mental health demand, a strong academic psychiatric workforce is elemental in helping UK psychiatry reach its true potential.
The strategy is ambitious and implementation will undoubtedly be difficult, because financial constraints, workforce pressures and organisational fragmentation remain significant challenges. However, the greater risk may lie in failing to act.
The challenge now is whether the profession, the RCPsych, universities, NHS organisations and national funders (including charities) are prepared to match the problem with sustained collective action.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10735
Data availability
Not applicable.
Author contributions
R.S.: conceptualisation, investigation, methodology, project administration, resources, validation, visualisation, writing – original draft, review and editing. J.G.: conceptualisation, writing – review and editing. G.S.M.: conceptualisation, writing – review and editing. P.W.W. conceptualisation, writing – review and editing. E.L.C.: writing – review and editing. L.I.S.: writing – review and editing. S.F.: writing – review and editing. S.R.C.: writing – review and editing. I.V.: writing – review and editing. R.A.L.: writing – review and editing. S.D.: writing – review and editing. A.H.Y.: conceptualisation, validation, visualisation, writing – review and editing.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
There is no direct conflict of interest for any of the authors. R.S. is the Associate Dean for Academic Training for RCPsych, G.S.M. is the Editor-in-Chief of BJPsych, S.D. is the Dean of RCPsych and A.H.Y. the Chair of the Academic Faculty of RCPsych, none of whom took part in the review or decision-making process of this paper. R.S. has received institutional research, travel support and/or honoraria for talks and expert advisory boards from LivaNova, UCB, Eisai, Veriton Pharma, Bial, Angelini, UnEEG and Jazz/GW Pharma outside the submitted work. He holds, or has held, competitive grants from various national grant bodies including Innovate, Economic and Social Research Council, Engineering and Physical Sciences Research Council, National Institute for Health and Care Research (NIHR), National Health Service Small Business Research Initiative and other funding bodies, including charities all outside this work. S.R.C.’s work is supported by NIHR Applied Research Collaboration Wessex, UK. The views expressed are those of the authors and not necessarily those of the NIHR, NHS or Department of Health and Social Care. S.R.C. receives an honorarium for journal editorial work from Elsevier. No other author has any conflict of interest.



eLetters
No eLetters have been published for this article.