


Impact statement
This study provides novel insights into the preferences and concerns of people with human immunodeficiency virus (HIV) in Lesotho regarding behavioral treatment strategies for addressing depression and harmful alcohol use. Key results are organized in a preference chart of different treatment components based on feedback from potential service users, which other implementers may adapt as a formative step before real-world adaptation and implementation of an evidence-based intervention. By highlighting the perceived benefits and limitations of phone-based interventions and the inclusion of trusted individuals in care, the findings underscore the importance of tailoring approaches to the unique sociocultural and infrastructural contexts in Lesotho. The emphasis on trusted HIV providers and preferences for face-to-face treatment offers guidance for integrating mental health care into HIV services in this setting. These results contribute to the evidence base for developing contextually relevant behavioral treatment programs to improve the well-being of people with HIV in similar settings.
Introduction
Despite global efforts to reduce the mental health burden, identifying and developing appropriate treatments for low-resource settings remain a challenge (WHO, MSD, 2022; Nadkarni et al., Reference Nadkarni, Gandhi, Bhatia and Velleman2023). In high-income countries, patient-centered approaches and personalized treatment regimens are being developed and assessed, aiming to answer the questions of what works for whom, in which settings and under what conditions (Deif and Salama, Reference Deif and Salama2021; Sampogna et al., Reference Sampogna, Della Rocca, Di Vincenzo, Catapano, Del Vecchio, Volpicelli, Martiadis, Signorelli, Ventriglio and Fiorillo2024). This also holds relevance in low- and middle-income countries (LMICs), where 82% of people with mental health symptoms or substance use problems (hereafter referred to as behavioral health problems) live. Despite the growing burden of behavioral health problems in these settings, only a limited number of treatment modalities have been evaluated.
Most interventions evaluated for behavioral health in LMICs focus on in-person, individually delivered care (Fu et al., Reference Fu, Burger, Arjadi and Bockting2020; Nakimuli-Mpungu et al., Reference Nakimuli-Mpungu, Musisi, Smith, Von Isenburg, Akimana, Shakarishvili, Nachega, Mills, Chibanda, Ribeiro, Williams and Joska2021; Abba Hassan et al., Reference Abba Hassan, Ibrahim and Nadkarni2024). While several digital interventions – most of which are delivered via smartphone applications or websites – have been evaluated in these settings, few have emphasized phone-based modalities, such as short message services (SMSs) or voice calls, which are more readily accessible technologies in LMICs (Fu et al., Reference Fu, Burger, Arjadi and Bockting2020; Eze et al., Reference Eze, Mbachu, Azuogu, Ossai, Unah, Akamike and Onwasigwe2021; Staton et al., Reference Staton, Friedman, Phillips, Minnig, Sakita, Ngowi, Suffoletto, Hirshon, Swahn, Mmbaga and Vissoci2023). Moreover, few interventions have engaged trusted individuals (e.g., romantic partners and family members) as part of the treatment process, despite the evidence that loved ones can play a key role in maintaining or improving behavioral health problems (Baucom et al., Reference Baucom, Fischer, Worrell, Corrie, Belus, Molyva and Boeding2018; Regenauer et al., Reference Regenauer, Belus, Ndamase, Rose, Gordon, Majokweni, Kotelo, Myers, Joska, Safren and Magidson2020). A better understanding of the potential use of these treatment strategies could improve delivery and enhance social support.
Although these strategies have not been assessed extensively in LMICs for behavioral health problems, including trusted individuals in terms of treatment and phone-based treatment delivery, they are hailed for their efficiency. The involvement of trusted individuals is a resource-intensive strategy but has the potential to improve the behavioral health outcomes of those involved (Baucom et al., Reference Baucom, Fischer, Worrell, Corrie, Belus, Molyva and Boeding2018), which may be more cost-effective (Belus et al., Reference Belus, Van Heerden, Hines, Pita, Mdakane, Magidson, Van Rooyen and Barnabas2025). Moreover, delivering intervention content via technology has greater dissemination potential than does using human resources (Bock et al., Reference Bock, Barnett, Thind, Rosen, Walaska, Traficante, Foster, Deutsch, Fava and Scott-Sheldon2016; Muñoz et al., Reference Muñoz, Chavira, Himle, Koerner, Muroff, Reynolds, Rose, Ruzek, Teachman and Schueller2018). As of 2024, in LMICs, 77% of men and 66% of women own mobile phones, and 54% of individuals use the internet on a regular basis (World Bank, 2024). Specialized health services, such as behavioral health treatment, are concentrated in urban areas like capital cities. Given that most individuals in LMICs still live outside urban areas (United Nations, 2021), the increasing penetration of mobile technology in rural areas presents a significant opportunity to enhance behavioral health care for populations that might otherwise lack access to such treatment. Therefore, testing various treatment delivery strategies involving SMSs, phone calls and trusted individuals has the potential to increase the availability of effective behavioral treatment strategies in LMICs.
People with human immunodeficiency virus (HIV) are disproportionately affected by behavioral and mental health problems (National Institute of Mental Health, 2019; Di Gennaro et al., Reference Di Gennaro, Papagni, Segala, Pellegrino, Panico, Frallonardo, Diella, Belati, Santoro, Brindicci, Balena, Bavaro, Montalbò, Guido, Calluso, Di Tullio, Sgambati, Fiordelisi, De Gennaro and Saracino2024). It is well established that targeting the behavioral needs of people with HIV is imperative for improving their overall health outcomes (Sikkema et al., Reference Sikkema, Dennis, Watt, Choi, Yemeke and Joska2015; Godfrey and Nkengasong, Reference Godfrey and Nkengasong2023; Wainberg et al., Reference Wainberg, Wolvaardt, Gouveia and Ferenchick2023). The integration of behavioral health services into HIV clinical care appears to be a feasible and effective strategy to improve behavioral health outcomes (Goldhammer et al., Reference Goldhammer, Marc, Chavis, Psihopaidas, Massaquoi, Cahill, Bryant, Bourdeau, Mayer, Cohen and Keuroghlian2022). A recent meta-analysis of mental health interventions for people with HIV in LMICs revealed that interventions reporting stakeholder involvement were more effective than those that did not report involvement (Nakimuli-Mpungu et al., Reference Nakimuli-Mpungu, Bass, Alexandre, Mills, Musisi, Ram, Katabira and Nachega2012). Thus, interventions that are aligned with the community’s perceived needs of care should be proposed (Osborn et al., Reference Osborn, Kleinman and Weisz2021; Bemme et al., Reference Bemme, Roberts, Ae-Ngibise, Gumbonzvanda, Joag, Kagee, Machisa, Van Der Westhuizen, Van Rensburg, Willan, Wuerth, Aoun, Jain, Lund, Mathias, Read, Taylor Salisbury and Burgess2024). Lesotho is a lower-middle-income country where one-fifth of the population lives with HIV, and mortality by suicide is the highest globally (UNAIDS, 2023; World Bank Group, 2023). The comorbid behavioral health problems of people with HIV in Lesotho negatively impact their clinical outcomes, such as decreased medication adherence, worsening physical health and increased stigma and social isolation (Stahlman et al., Reference Stahlman, Grosso, Ketende, Sweitzer, Mothopeng, Taruberekera, Nkonyana and Baral2015; Cerutti et al., Reference Cerutti, Broers, Masetsibi, Faturiyele, Toti-Mokoteli, Motlatsi, Bader, Klimkait and Labhardt2016; Wendi et al., Reference Wendi, Stahlman, Grosso, Sweitzer, Ketende, Taruberekera, Nkonyana, Mothopeng and Baral2016; Mahlomaholo et al., Reference Mahlomaholo, Wang, Xia, Wang, Yang and Wang2021). A large treatment gap for behavioral health problems exists in this setting, with 90% of adults from the Butha-Buthe and Mokhotlong districts in community settings reporting untreated behavioral health problems (Fernández et al., Reference Fernández, Yoon, Firima, Gupta, Sematle, Khomolishoele, Molulela, Bane, Tlahani, Lee, Chammartin, Gerber, Lejone, Ayakaka, Labhardt, Amstutz and Belus2024). In the context of a few treatment options from the public health system, external efforts are being invested by global academic and health bodies to address this treatment gap (Partners in Health, 2018; Belus et al., Reference Belus, Msimango, Van Heerden, Magidson, Bradley, Mdakane, Van Rooyen and Barnabas2024). However, little is known about preferences for behavioral health treatment in the local community.
Therefore, the goal of this study was to understand the perspectives of potential behavioral treatment service users in Lesotho by focusing on people with HIV receiving HIV care in semi-rural or rural communities with unmet behavioral health needs. We explored individuals’ perspectives on (1) phone-based interventions, (2) involving trusted individuals in care and (3) preferred characteristics for providers of behavioral health treatments.
Methods
Setting
Lesotho is a mountainous enclave of South Africa with a high burden of communicable and noncommunicable diseases. Although the country has recently made significant strides in its HIV response (Lesotho Ministry of Health, 2022; Farahani et al., Reference Farahani, Farley, Smart, Ndagije, Maile, Longwe, Hoos and El-Sadr2025), the infrastructure for behavioral healthcare is underdeveloped, with one or two psychiatric nurses at every district hospital (WHO, MSD, 2014). As most people live in remote areas, accessing the health facilities where these nurses provide care is burdensome (Partners in Health, 2018).
Participants
Participants were recruited from a larger study testing a viral load-triggered, automated, differentiated service delivery model for people on antiretroviral therapy (ART) versus usual care (VIral Load Triggered ART Care in Lesotho, or VITAL). Participants were eligible for the parent study if they were adults living with HIV, on ART, registered for HIV care at a participating health facility and planned to remain in the area for 2 years of care (Tschumi et al., Reference Tschumi, Lerotholi, Kopo, Kao, Lukau, Nsakala, Chejane, Motaboli, Lee, Barnabas, Shapiro, van Heerden, Lejone, Amstutz, Brown, Heitner, Belus, Chammartin and Labhardt2022). For the current study, participants were eligible if they exhibited at least mild behavioral health needs in the past year, defined by the presence of at least mild depressive symptoms indicated by the Patient Health Questionnaire, a 9-item score of ≥5 (Kroenke and Spitzer, Reference Kroenke and Spitzer2002), and unhealthy alcohol use indicated by the Alcohol Use Disorder Identification Test for Consumption score of ≥3 for women or ≥4 for men (Bush et al., Reference Bush, Kivlahan, McDonell, Fihn and Bradley1998). We did not screen for use of other substances as a prior cross-sectional household survey demonstrated low prevalence of nonalcohol substance use in this community (Fernández et al., Reference Fernández, Yoon, Firima, Gupta, Sematle, Khomolishoele, Molulela, Bane, Tlahani, Lee, Chammartin, Gerber, Lejone, Ayakaka, Labhardt, Amstutz and Belus2024). Prospective participants were not rescreened before participation. The broad inclusion of those reporting depressive symptoms or unhealthy alcohol use within the past year reflects the exploratory aim of eliciting feedback from potential service users with lived experience of these symptoms.
The target sample size for the current study was 30 participants, as calculated per existing guidelines for qualitative interviews (Malterud et al., Reference Malterud, Siersma and Guassora2016; Vasileiou et al., Reference Vasileiou, Barnett, Thorpe and Young2018). We purposively sampled to achieve similar proportions of males and females, but females were most common at the time of recruitment during normal business hours, which is reflected in the demographics of our final sample. The samples were also distributed among two clinics to diversify our sample among both Butha-Buthe and Mokhotlong districts. Participants were reimbursed for their transportation costs and provided with minor refreshments (e.g., water bottle) during the interview. No other remuneration was provided. Two participants’ data were excluded after data collection due to post hoc discovery of their ineligibility, resulting in a final sample size of N = 28.
Training and capacity building
Capacitating Basotho team members in qualitative research methods was a goal of the research project, as part of the larger implementing partnership between the Swiss team and the Lesotho team. Three training events were facilitated by two doctoral students (GHY and NEJ) during the study period, one of which was conducted specifically for the current study. During this training, attendees learned about major qualitative theories, common interviewing modalities and analytic approaches. Training events included interviewing, role-plays and sample transcript coding practice sessions. The training events were open to other staff members in the implementing partner organization, who were interested in learning about qualitative research but were not specifically involved in the current project. Team members involved in the current study also received separate training and supervision on the study’s interview guide and conducted pilot interviews with participants, after which they received feedback from the supervisor (JMB). One team member was also trained in codebook development. All team members were encouraged to provide meaningful input throughout the data collection and analysis period, including interpretation of the results for dissemination.
Positionality statement
The study team was composed of cisgender women and men, ranging from individuals new to research to experienced academics. This study was conceptualized by a clinical psychologist (JMB) and a public health researcher (AvH) originating from Canada and South Africa, respectively. Mosotho team members were consulted during the study’s conceptualization stage to further develop early ideas into a culturally relevant interview guide. Two female (MM and PM) and one male Mosotho interviewers, and one male Mosotho study coordinator conducted, recorded, transcribed and translated the interviews and performed audio fidelity checks. They also contributed to project management, translation of the interview guide, generation of the codebook and interpretation of the results for salience in the local context. Two American students completing their doctoral degrees in Switzerland (GHY and NEJ), who have lived experience and conducted prior qualitative research in Lesotho, oversaw the analyses.
Recruitment
The study took place in two districts in Northern Lesotho, Butha-Buthe (peri-urban township with extended rural areas) and Mokhotlong (rural, mountainous region). We recruited participants using a purposive sampling approach from a list of VITAL participants based on their most recent depression and alcohol use scores in the past year. Trained study staff called individuals from this list and inquired about their interest in participating in the qualitative study. Interested participants were invited to their local health clinic to complete informed consent procedures and an individual semi-structured interview. Each interview lasted between 40 and 70 min, was conducted in Sesotho (local language) and was audio recorded. Local team members – a trained male Basotho psychologist and two female Basotho nurses – led the interviews. Participant activities took place in private rooms of local health facilities. Audio recordings were then transcribed and translated by an external professional bilingual (Sesotho and English) transcriber. Bilingual members of the research team performed fidelity checks on 15% of the randomly chosen transcripts. The Lesotho National Health Research and Ethics Committee approved the study (ID 220–2019).
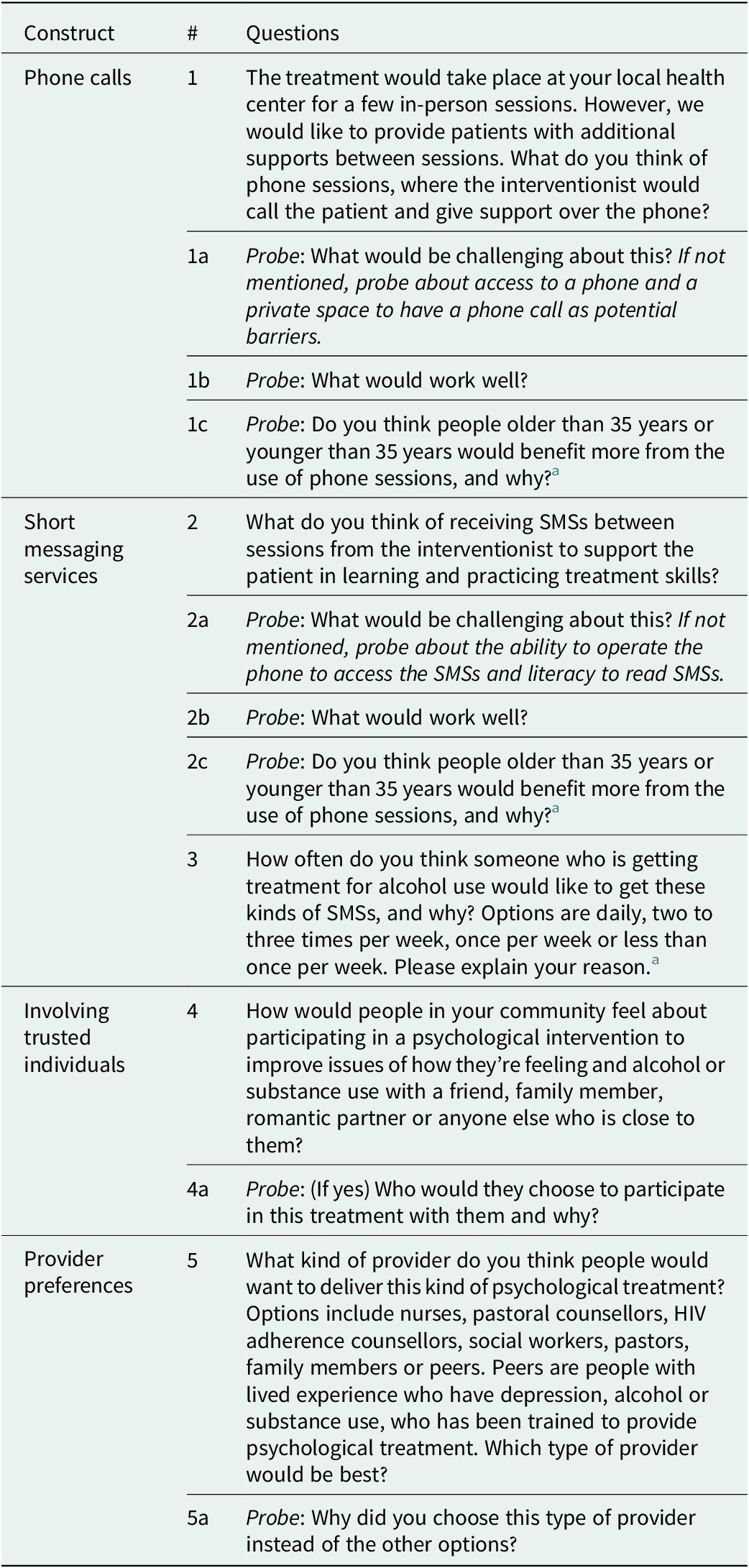
Interview guide
The semi-structured interview guide is shown in Appendix 1. Interview questions elicited participants’ preferences in supplementing health facility-based behavioral treatment (a) over the phone, via phone calls and text messages, overall and by age group and (b) by involving a trusted individual as a treatment supporter. Questions were framed using the term “psychological treatment” to refer to treatments for common mental and behavioral problems that were reported previously by participants in the same interview (e.g., depression and suicidal thoughts, stress and alcohol use). Although participants were only screened for unhealthy alcohol use, we also explored their treatment preferences with alcohol or “other substances” in the community. This was done to avoid limiting their responses to experiences only pertinent to alcohol, as prior evidence suggests the presence of other substances in the community, albeit infrequently (Gonzalez et al., 2024). The age threshold separating “younger” versus “older” adults and the frequency options given for SMS preferences were informed by e-health preferences elicited in the parent study.
Analysis
The study used a thematic analysis approach. The coding team involved two American doctoral students and one Mosotho team member. A preliminary codebook was generated after each of the coding team members reviewed the first three transcripts and agreed upon emerging themes and patterns. The rest of the transcripts were coded with Dedoose version 9.2.14 (Dedoose, 2016). The coding tree included up to three levels. The smallest code level contained specific examples of symptoms or words associated with the higher-level codes reported by participants. Perspectives on preferences for different service components were categorized into smaller groups based on age (younger vs. older adults) and factors influencing access (facilitators vs. barriers). Coders double-coded the first 30% of the transcripts. The interrater reliability was adequate at Cohen’s d = 0.87. The team employed an iterative process of codebook development throughout the coding process; the codebook was reconciled throughout. For validation, additional Mosotho study team members experienced in qualitative analysis reviewed the results to ensure the relevance and salience of findings in the local context.
Results
Sample characteristics
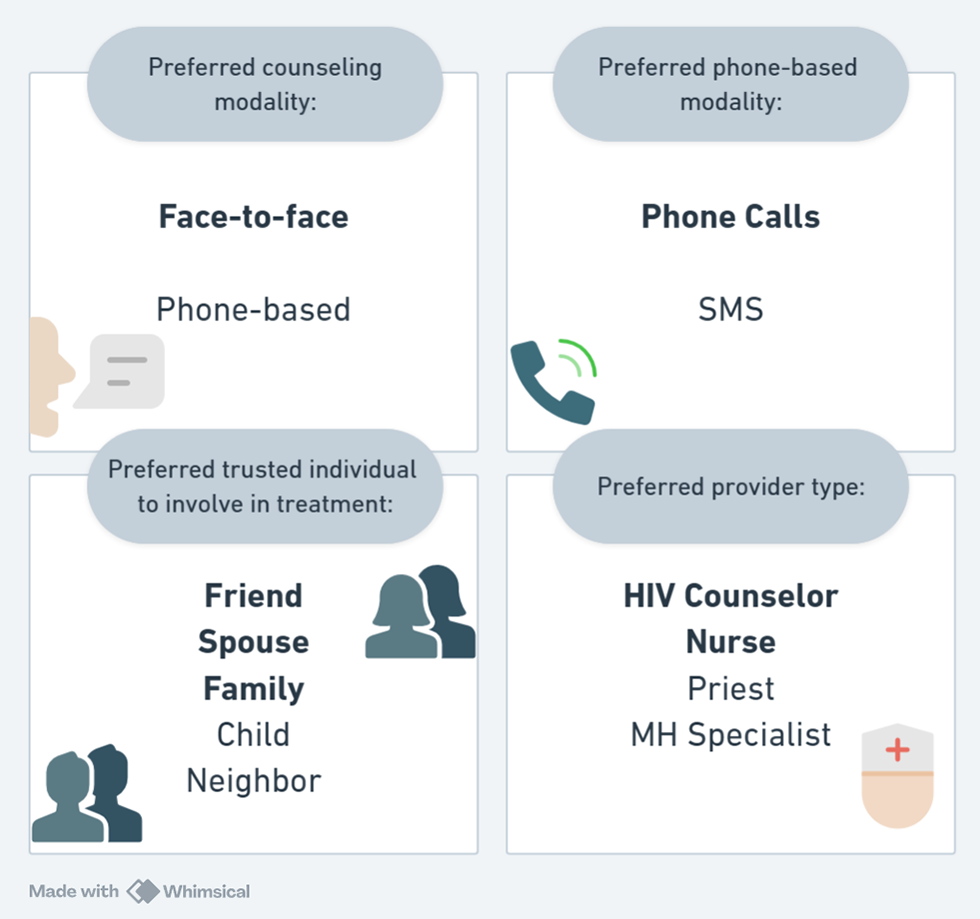
Twenty-eight participants with a median age of 44 years (range 28–68 years) participated in the study. Most lived in Butha-Buthe (77%) and were female (83%). Approximately two-thirds of the participants did not complete secondary school and were unemployed. Two-thirds of participants were married, one-fifth of participants reported that they were widowed, with the remaining participants being either unmarried or separated. The majority were eligible because they presented with a recent history of at least mild depressive symptoms, four participants were eligible due to harmful alcohol consumption levels and two participants were eligible on both depression and alcohol consumption levels. Below, we report how participants prefer potential behavioral treatment in these three domains: (1) phone-based treatment, (2) involving trusted individuals and (3) providers. Preferences are graphically summarized in Figure 1.
Preference chart for behavioral treatment for people with HIV in Lesotho (most frequently mentioned by participants are given in bold).

Phone-based treatment
Most participants expressed a preference for face-to-face treatment, despite the cost- and time-saving aspects presented by phone-based modalities. Participants believed that face-to-face sessions would promote understanding between the patient and provider.
I believe that would be easier for us to communicate effectively and understand each other when we are talking in person. You would be able to understand me better and so will I. When you counsel me in person, you are also able to see when and when I do not understand the things which you are saying.
- ID #15, age 40, female with depressive symptoms
Other participants cited specific logistical disadvantages for phone-based treatment, such as the need to have funds in their mobile account and access to a consistent signal and electricity (i.e., calls may drop unexpectedly), which may hinder the service user’s willingness to have prolonged conversations over the phone, limiting their verbal expression during phone counseling sessions.
Sometimes the child chews the SIM card just like they did right now. [Health care worker] struggled getting a hold of me so much, I just got lucky because my neighbors have her number.
- ID #7, age 37, female with depressive symptoms
When participants were asked to choose between two phone-based strategies, calls and text messages, they were heavily skewed toward phone calls. Phone calls were deemed more acceptable because participants believed they allowed for bidirectional communication while maintaining the convenience of reaching service users remotely. Participants suggested different clinical scenarios in which phone calls could be a good treatment delivery strategy, particularly for brief check-ins that require short updates, such as adherence check-ins or symptom changes that would warrant a physical visit. Participants believed that phone calls could be helpful in providing patients with timely counseling in times of need, without a lengthy wait until the patient could visit the facility.
I think that phone sessions can be very effective because sometimes I could be away […] at the time I am needed, and it would be easier if you were to just call me and have the conversation through the phone. I would personally find this very helpful, as my phone is always available.
-ID #21, age 42, male with depressive symptoms
Text messages garnered the least support among our middle- and older-aged participants. That said, participants viewed the approach as acceptable when it was presented as a potential brief counseling tool for the community. Primary concerns for the use of text messages were a lack of literacy, an issue prevalent among older participants. As such, participants endorsed the use of text messages for younger adults, who tend to be more literate and have more interest in using phones. Another concern was related to the perception that text messages are perceived as unimportant. In Lesotho, it is common for individuals to ignore them regardless of their purpose, as spam text messages have become pervasive from commercial subscriptions and social media.
Despite this concern, others saw the benefit of using text messages, regardless of the age of the recipient, owing to their ability to be stored and accessed later, even if the recipient is unavailable or if the phone is turned off. This is relevant in the current context, as electricity is not always available to charge phones, and it is common for multiple family members to share one mobile phone.
Text messages are reliable in that even if the phone is off at the time the message is sent, once I have charged it, I will be able to receive and access the message.
-ID #11, age 61, female with unhealthy alcohol use symptoms
In addition, one participant noted that phone calls and in-person visits may not be appropriate for heavy alcohol users, as they are less inclined to give up time and attention to behavioral treatment at a scheduled session. As such, text messages may be a low-touch, flexible treatment method where lessons can be read and digested at a time when they are sober and it can be shared with others while drinking:
I suspect that they would even hang up the phone call as soon as you tried to talk to them about such. They have been tried too many times […] He/she could pay attention and accept the information on the [text] messages when they are sober […] Now, he will be sharing this information with people who are drunk, and he will probably just be creating a conversation with this information; but you will hear that the message really did sink into him.
-ID #12, age 52, male with unhealthy alcohol use symptoms
Involvement of trusted individuals
Many participants thought that their trusted individuals would accept the role of a treatment supporter and help address their behavioral symptoms. The participants reflected that behavioral symptoms in the community have become visibly problematic and predicted that their trusted individuals would be eager to accompany them because of the community’s empathetic attitude toward helping individuals who suffer from behavioral problems. A perceived benefit of this strategy for participants was that trusted individuals involved in behavioral health services can reinforce intervention strategies outside of core services and provide nuanced emotional support for participants to aid in their recovery outside of the services. Involving trusted individuals in behavioral treatment would allow accompanying individuals to better understand common behavioral problems and become better equipped to help:
I think they [trusted individuals] will be interested because they will have noticed that the said individual [with behavioral health needs] really does need help from them, and if they could take the necessary steps and precautions, that person would be okay.
-ID #4, age 36, female with unhealthy alcohol use and depressive symptoms
Another favorable aspect of involving trusted individuals in treatment is that it allows for vicarious learning of strategies to address behavioral health issues. The involvement of trusted individuals in treatment facilitates patient accountability for their progress, which will allow for real-time feedback as patients attempt to apply strategies from their treatment in their day-to-day lives. Thus, lessons learned from strategies to mitigate harmful behaviors by both the service user and their close supporters can be shared with the larger community, with the possibility of prompting an informal information campaign to increase awareness and promote the adoption of similar lessons for others:
[A close person] can hear what I have been taught there [from future behavioral treatment] and be able to see that I no longer do the things that I used to do. That will make it clear that I have been taught well. Many people will start to see that the person [with behavioral health issues] no longer does the [harmful] things that they used [to do] and from that, they will get ideas of approaching [the individual with behavioral health issues] so that they can know what she did to change.
-#ID9, age 56, female with unhealthy alcohol use symptoms
The most preferred trusted individuals to be involved in behavioral treatment were family members, especially spouses, as they were the main supporters of married individuals in major aspects of life. Friends were also preferred by several participants, especially by young people, who value camaraderie through shared experiences in living with HIV.
Most of us are living survivors of HIV, so we have come together in social settings and have had conversations that have helped us establish a genuine friendship with one another, regardless of our parents’ disputes.
-ID #5, age 28, female with depressive symptoms
Providers for behavioral treatment
One of the most preferred types of behavioral treatment providers among our participants was an HIV counselor. This provider type was preferred because of their reputation for maintaining confidentiality and existing familiarity within the local HIV community. They were also seen to have authority over the clinical and social knowledge of living with HIV. One participant alluded to the fact that people with HIV usually receive other non-HIV-related educational programs through them, so it would make sense that behavioral treatments also come from counselors. Other participants indicated that they already have a positive relationship with their HIV counselor in the context of HIV care, so it would also be someone that they would want to see for problems with behavioral health.
I would like […] HIV adherence counselors because I have observed that when I have problems, their approach makes me feel better after talking to them, so I believe even those who take alcohol in an unhealthy way will benefit.
-ID #14, age 41, female with depressive symptoms
For similar reasons, nurses were the next most preferred provider for future behavioral treatments. Participants preferred not to have behavioral treatment from peers or someone known to them for fear of their personal matters being exposed to the larger community. They strongly stated that peers who they know personally would not be suitable as providers due to the risk of gossip and fear of stigma surrounding behavioral symptoms. Another reason peers were not preferred is that, since they had similar problems, participants perceived peers as not being able to help others in similar situations.
We should not even consider a friend, a relative, a counselor or a family friend because lately, people are very quick to judge the next person. What would work best is a person who comes from a different place from where you reside, as they are most capable of empathizing with you to understand the kind of situation that you are in. I have discovered over the past years that I am the kind of person who likes to help other people, but I do not like to be assisted. I would come up with certain ideas, and people would shun then down only because they come from me.
-ID #5, age 28, female with depressive symptoms
Discussion
This qualitative study was a formative inquiry to understand potential service user preferences for behavioral treatment in a sample of people with HIV in Lesotho. Study findings suggest that potential service users prefer discreet, face-to-face treatment delivered by HIV-related health professionals. Participants favored face-to-face behavioral treatment and endorsed the utility of phone-based strategies for their privacy and flexibility. The involvement of trusted individuals in treatment, particularly family members, was viewed favorably, whereas the use of peers or other known community members as service providers was deemed less acceptable in this setting.
Participants in this study showed a strong preference for face-to-face treatment over phone-based treatment and phone calls over text messages. This may be partially explained by the notion of therapeutic alliance, which describes the collaborative and emotional relationship between a therapist and their client (Horvath and Luborsky, Reference Horvath and Luborsky1993). When envisioning remote behavioral treatment, participants expressed concern over the perceived absence of such an alliance with their provider. This finding is supported by prior research demonstrating consistent patient preferences for face-to-face rather than remote mental health treatment in rural Western settings, despite remote treatment having clear time- and resource-saving benefits (Renn et al., Reference Renn, Hoeft, Lee, Bauer and Areán2019; Sizer et al., Reference Sizer, Bhatta, Acharya and Paudel2022; Mazurka et al., Reference Mazurka, Vallis, Chen, Freeman, Langley, Ross, Arora, Kahn, Howard, Liu, Cumby, Brennan, Hickcox, Bagnell, Propper, Pavlova and Uher2024). Taken together, these findings suggest a preference for in-person delivered services globally, possibly because both providers and patients perceive stronger therapeutic alliances in in-person counseling than remote, enabling deeper empathy, more immediate support and greater personal connection (Sperandeo et al., Reference Sperandeo, Cioffi, Mosca, Longobardi, Moretto, Alfano, Scandurra, Muzii, Cantone, Guerriera, Architravo and Maldonato2021; Grondin et al., Reference Grondin, Lomanowska, Belleville, Yampolsky, M-PB and Jackson2024). Although findings from Lesotho corroborate existing literature, comparable evidence on empathy and therapeutic alliance in in-person versus remote treatment is scarce from other settings in Southern Africa, posing an opportunity for future research.
LMICs are known to have strengths in their supportive family and community structures, sharing the burden of psychological hardships (Rathod et al., Reference Rathod, Pinninti, Irfan, Gorczynski, Rathod, Gega and Naeem2017). This is reflected in our participants’ positive reactions to involving a trusted individual in treatment, many citing that community members would be willing to support others in need through treatment support. Specifically, participants liked that they would have accountability outside of the treatment sessions, and that their supporters would vicariously learn behavioral treatment components and spread this knowledge to others who may benefit in the community. There is a growing body of evidence demonstrating the efficacy of working with couples to improve HIV outcomes in both high- and low-resource settings (Remien et al., Reference Remien, Stirratt, Dolezal, Dognin, Wagner, Carballo-Dieguez, El-Bassel and Jung2005; Desgrées-du-Loû and Orne-Gliemann, Reference Desgrées-du-Loû and Orne-Gliemann2008; LaCroix et al., Reference LaCroix, Pellowski, Lennon and Johnson2013; Jiwatram-Negrón and El-Bassel, Reference Jiwatram-Negrón and El-Bassel2014; Wall et al., Reference Wall, Kilembe, Vwalika, Haddad, Lakhi, Onwubiko, Htee Khu, Brill, Chavuma, Vwalika, Mwananyanda, Chomba, Mulenga, Tichacek and Allen2017; Belus et al., Reference Belus, Baucom, Carney, Carrino and Wechsberg2019, Reference Belus, Msimango, Van Heerden, Magidson, Bradley, Mdakane, Van Rooyen and Barnabas2024; Belus, Reference Belus2020; Gutin et al., Reference Gutin, Ruark, Darbes, Neilands, Mkandawire and Conroy2023). However, the inclusion of romantic partners or other trusted individuals in behavioral treatment has not been widely evaluated in low-resource settings. To date, research has focused primarily on working with couples or families to reduce substance use (Wechsberg et al., Reference Wechsberg, Zule, El-Bassel, Doherty, Minnis, Novak, Myers and Carney2016; Sheikh et al., Reference Sheikh, Paul, Banda, Agath and Luty2017; Giusto et al., Reference Giusto, Green, Simmons, Ayuku, Patel and Puffer2020; Puffer et al., Reference Puffer, Friis Healy, Green, Giusto, Kaiser, Patel and Ayuku2020; Conroy et al., Reference Conroy, Hahn, Neilands, Darbes, Tebbetts, Mulauzi, Mkandawire and Ssewamala2024). Findings of the present study dovetail with the observed local norms of bringing a companion to health-related visits for moral support. Future research should evaluate this approach as a strategy to integrate behavioral treatment in routine HIV care.
Finally, the participants expressed preferences for their HIV counselors or nurses to deliver behavioral treatment, indicating that people with HIV in these communities are comfortable with such healthcare staff. Integration of behavioral health into chronic care has been extensively studied in the United States, and findings point to a consensus in adapting the integration of behavioral and mental health care with routine care into real-world practice (SAMHSA-HRSA, 2016; Goldhammer et al., Reference Goldhammer, Marc, Chavis, Psihopaidas, Massaquoi, Cahill, Bryant, Bourdeau, Mayer, Cohen and Keuroghlian2022; Conteh et al., Reference Conteh, Latona and Mahomed2023; McKinnon et al., Reference McKinnon, Lentz, Boccher-Lattimore, Cournos, Pather, Sukumaran, Remien and Mellins2024). Despite many calls for action to implement this strategy globally, evidence on such integration is scarce in LMICs and the Global South, especially in rural regions (Parcesepe et al., Reference Parcesepe, Mugglin, Nalugoda, Bernard, Yunihastuti, Althoff, Jaquet, Haas, Duda, Wester and Nash2018; Conteh et al., Reference Conteh, Latona and Mahomed2023). One study in Zimbabwe reported that a stepped-care integration model utilizing a mix of professionals, including nurses, community health workers and traditional providers, was acceptable to patients, and that all provider types were able to effectively screen for common mental health symptoms such as depression and alcohol use (Duffy et al., Reference Duffy, Sharer, Cornman, Pearson, Pitorak and Fullem2017). Despite encouraging evidence, providers who specialize in HIV or primary care often lack confidence in adding mental health treatment to their scope of care (Mall et al., Reference Mall, Sorsdahl, Swartz and Joska2012; Cele and Mhlongo, Reference Cele and Mhlongo2020; Ramokanate et al., Reference Ramokanate, Nyangu and Rathobei2023; Grimes et al., Reference Grimes, Ebasone, Dzudie, Nash, Wainberg, Pence, Barrington, Pefura, Yotebieng, Anastos, Nsame, Ajeh, Nyenti and Parcesepe2024). Adequate training and supervision programs are key to upskilling and supporting nonspecialist providers in delivering behavioral health care (Kemp et al., Reference Kemp, Petersen, Bhana and Rao2019).
There were several limitations to this study. The interviews were conducted during regular working hours, and the interviewees were recruited from a preselected cohort who were already receiving health care through the parent study. These factors present selection bias toward adults who are unemployed and have regular access to and engagement in healthcare. Our demographic skews toward older women, which means that the findings may not capture the preferences of younger individuals and men. We also did not explore perspectives on other known evidence-based strategies, such as community-based treatment, which may be relevant in rural settings such as Lesotho. Despite these limitations, the current study was the first to elicit potential service user preferences for different components of evidence-based approaches for behavioral treatment in Lesotho, taking the knowledge base one step closer to effective health programming for the local population. Contrary to what may be hypothesized for a low-resource setting, participants in Lesotho expressed clear preferences for time-intensive care (i.e., face-to-face and with the involvement of a trusted individual). The most important qualities of a treatment provider to our participants were expertise, anonymity and discretion, rather than peers, despite evidence of peer-to-peer care in HIV services in the Global South (Katz et al., Reference Katz, Bogart, Fitzmaurice, Staggs, Gwadz, Bassett, Cross, Courtney, Tsolekile, Panda, Steck, Bangsberg, Orrell and Goggin2021).
Current discourse on global health encourages feasible and acceptable adaptations of interventions for low-resource settings, factors that are still most often defined, developed and evaluated in Western settings by Western authors (Wagenaar et al., Reference Wagenaar, Hammett, Jackson, Atkins, Belus and Kemp2020). Instead, future work can give potential service users the direct power to determine feasibility and acceptability of an intervention in their own setting, and a voice to express what is the most desirable and necessary service component. Results from this study may inform the development and implementation of interventions aligned with the preferences of potential service users to establish high-quality, relevant and desirable standards of care for key populations in Lesotho and other LMICs.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2025.10017.
Data availability statement
The qualitative data analyzed are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank all the participants who spared their time and provided insight into their preferences for future interventions, as well as the study collaborators at SolidarMed Lesotho, for their logistical help in making the study possible.
Author contribution
Jennifer M. Belus and Alastair van Heerden conceptualized the project. Grace H. Yoon and Moleboheng Mokebe facilitated and managed the study activities. Palesa Mahlatsi and Moleboheng Mokebe conducted the interviews in Sesotho. Grace H. Yoon and Natalie E. Johnson undertook data analysis and cowrote the manuscript under the supervision of Irene Falgas-Bague and Jennifer M. Belus. All other authors, Malebanye Lerotholi, Niklaus D. Labhardt and Nadine Tschumi, reviewed the manuscript and provided substantive feedback.
Financial support
This study was funded by the Swiss National Science Foundation Ambizione grant [PZ00P1_201690; PI: Belus]. The views expressed are those of the authors and do not represent those of the funder.
Competing interests
Nadine D. Labhardt reports having received travel grants to attend scientific conferences from Gilead Sciences and ViiV Healthcare. In 2022 and 2023, his division at the University Hospital Basel received honoraria from ViiV Healthcare. All other authors declare that they have no conflicts of interest.
Ethics statement
The National Health Research Ethics Committee of Lesotho approved this study (NHREC ID #220–2019). Written informed consent, guided by the interviewer, was obtained from the participants before each interview.
Appendix 1. Semi-structured questionnaire
Prompt: We are interested in developing a psychological treatment to help people in your community who are feeling down, very stressed about life, or using alcohol or other substances in an unhealthy way. Someone who is experiencing these problems would meet with a trained provider and talk about their issues. The trained provider would help the person to make changes to feel better and/or reduce unhealthy alcohol or substance use. We would like to get some feedback from you on what approaches might work.


 Open access
Open access
Comments
February 4, 2025
Dear Professors Bass and Chibanda,
I am pleased to submit our manuscript, titled “ Face-to-Face, Confidential and Health Worker-Led: Understanding the Preferences for Behavioral Health Services Among People with HIV in Lesotho” for consideration for publication in Cambridge Prisms: Global Mental Health.
We believe that our study aligns with the scope of your journal, particularly given its focus on delivering locally informed evidence-based treatment options for global mental health in diverse settings. This manuscript presents a novel approach to engaging end-user preferences in implementing evidence-based interventions in a low-resource setting. Insights from our study have implications for behavioral treatment integration in routine HIV care for rural communities in Lesotho, a lower-middle-income country with a high HIV burden in Southern Africa.
This manuscript is original and has not been published or under consideration elsewhere. All authors have approved the submission. Please note the corresponding author for submission is Grace H. Yoon, co-first author, but the corresponding author to be listed for publication is Jennifer M. Belus, co-last author.
Thank you for your time in considering our manuscript, and please do not hesitate to contact us at grace.yoon@usb.ch should you require any further information.
Sincerely,
Grace H. Yoon, on behalf of all co-authors
Division of Clinical Epidemiology
University of Basel, University Hospital of Basel
Totengasslein 3, Basel 4051, Switzerland
grace.yoon@usb.ch
+41 78 256 5881