


Introduction
To adapt to the environment and survive, humans adjust various biological systems, such as the endocrine and autonomic nervous systems. Reference Hales and Barker1,Reference Hales and Barker2 These adaptations work effectively as long as the environment remains similar. However, when the environment undergoes significant change, a mismatch occurs between the adaptation and the new conditions, which can potentially result in health problems. The Developmental Origins of Health and Disease (DOHaD) hypothesis argues that the environment before and immediately after birth can affect future health and the risk of some diseases. Reference Hales and Barker1,Reference Barker, Bull, Osmond and Simmonds3,Reference Barker, Winter, Osmond, Margetts and Simmonds4 For example, fetuses exposed to undernutrition in utero undergo behavioral adaptations to increase their chance of survival. Intrauterine growth restriction (IUGR) can alter food seeking behaviors (e.g., impulsive snacking) and lead to children’s preferences for high-sugar and high-fat diets. Reference Ayres, Agranonik, Portella, Filion, Johnston and Silveira5–Reference Silveira, Agranonik, Faras, Portella, Meaney and Levitan8 These adaptations arise from the fetus being programmed to seek more resources, a result of resource deprivation in the uterus. However, when fetuses are placed in a nutrient-rich environment after birth, the risk of non-communicable diseases, such as obesity and diabetes, is increased. Reference Hales and Barker1–Reference Barker, Winter, Osmond, Margetts and Simmonds4,Reference Gluckman, Hanson, Cooper and Thornburg9–Reference McMillen and Robinson12
From a behavioral economics perspective, both time and total benefits must be considered to examine the tendency to seek more resources. Reference Weinsztok, Brassard, Balodis, Martin and Amlung13 In general, people prefer to get smaller immediate rewards than to wait for larger future ones, Reference da Matta, Gonçalves and Bizarro14 a phenomenon called delay discounting (DD). Reference da Matta, Gonçalves and Bizarro14 High DD is considered an indicator of a person’s impulsivity and low self-control Reference Epstein, Richards, Saad, Paluch, Roemmich and Lerman15,Reference Shamosh and Gray16 and a predictor of several negative life outcomes, including worse academic performance, poor social relationships, and higher rates of criminal behavior and substance use. Reference Golsteyn, Grönqvist and Lindahl17,Reference Kang and Ikeda18 To our knowledge, no research to date has reported on the tendency of low birthweight (LBW) infants to seek more resources in the context of DD.
The development of DD in childhood may be influenced by prenatal factors such as LBW. Reference Lynn, Cuskelly and Gray19,Reference Schlotz, Godfrey and Phillips20 A study of 30 extremely-low-birthweight (ELBW) children and 29 normal birth weight children ages two to four experimented with self-regulatory tasks, where children had to decide between receiving a small reward instantly or waiting for a larger one. Reference Lynn, Cuskelly and Gray19 In this study, ELBW children showed significantly higher DD than normal birthweight children. However, the study did not report the duration they needed to wait to obtain the larger reward (indicating their level of patience). It is important to note that DD is not merely behavioral inhibition but also represents choice preference, a higher cognitive process of evaluating rewards subjectively under conditions of uncertainty. Reference Reynolds and Schiffbauer21 Therefore, to accurately assess DD, the influence of postnatal environmental factors must be considered.
In addition, children raised in toxic environments, e.g., experiencing adverse childhood experiences (ACEs), show high DD. Reference Acheson, Vincent, Cohoon and Lovallo22,Reference Shain, Nguyen and Meadows23 For example, in a study of 227 adult diabetic patients, aged 18–77 years in the US, Shain et al used the Monetary Choice Questionnaire (MCQ-27). In the MCQ-27, participants are presented with 27 combinations and asked to choose between two monetary rewards: a smaller, immediate reward or a larger, delayed one. Results showed a significant positive association between ACEs and DD. Reference Shain, Nguyen and Meadows23 Another study of 1176 young adults, aged 18–30 years, showed that ACEs were associated with high DD measured by the MCQ-27. Reference Acheson, Vincent, Cohoon and Lovallo22 However, to the best of our knowledge, there has been no research examining the impact of ACEs, which were assessed by caregivers, on DD in children. That is, both previous studies assessed ACEs as self-reported, which induces common method bias, and assessed them in adults retrospectively, which induces recall bias. To reach that goal, like with the marshmallow test Reference Mischel, Ayduk and Berman24,Reference Mischel, Shoda and Rodriguez25 , an experimental study to assess DD among children is needed, rather than assessment using a questionnaire.
Experiencing traumatic events, such as a natural disaster, can also influence DD due to a perception of future unpredictability following such events. In 2011, the Great East Japan Earthquake (GEJE) occurred, which was one of the largest earthquakes in Japan. The earthquake, followed by a massive tsunami, resulted in the direct and indirect deaths of over 22,000 people. Reference Zheng, Feng and Ishiwatari26 Research on children aged 3–5 years experiencing the GEJE found that those whose houses were destroyed showed high rates of DD. Reference Matsuyama, Fujiwara, Sawada, Yagi, Mashiko and Kawachi27
Based on this literature, it is essential to consider both prenatal factors, such as LBW, and postnatal environmental exposures, such as ACEs and natural disasters, when examining DD in children. However, no studies have examined or compared the effects of prenatal factors and postnatal experiences on DD simultaneously. Thus, we explored the impacts of LBW, ACEs before and after the GEJE, and trauma related to the GEJE on DD in children. We also aimed to clarify how specific ACEs and their timing are associated with DD, based on an experiment conducted among preschool-aged children living in the four tsunami-affected prefectures associated with the GEJE.
Method
Participants
This study used data from the Great East Japan Earthquake Follow-up for Children (GEJE-FC) study (see Fujiwara et al. Reference Fujiwara, Yagi, Homma, Mashiko, Nagao and Okuyama28 for details of the study protocol). In brief, the GEJE-FC enrolled children and their caregivers residing in three affected geographical areas (Iwate, Miyagi, and Fukushima prefectures), who experienced the GEJE when the children were between 3 and 5 years old. Participants completed the baseline survey between September 2012 and June 2013 (N = 269) and were subsequently followed annually. DD was assessed in the third follow-up survey of this study in 2014, in which 168 children participated. After excluding one child who lacked the experiment outcome, a total of 167 children were analyzed (Supplementary Figure S1).
Outcome
We examined DD using an incentivized experiment based on the time-investment exercise developed by Angerer et al. Reference Angerer, Lergetporer, Glätzle-Rützler and Sutter29 Details of the procedure can be found elsewhere. Reference Matsuyama, Fujiwara, Sawada, Yagi, Mashiko and Kawachi27 In this exercise, children were initially given 5 tokens. They were asked to decide how many tokens to exchange immediately (for an equivalent number of candies) or to invest in the future, as each invested token would be doubled and paid out 4 weeks later. For example, if a child chose to allocate one token now and four tokens in the future, she/he would receive one candy immediately and eight candies four weeks later, resulting in a total gain of nine candies (Figure 1). A higher allocation of tokens for immediate reward indicates a greater tendency of the child to discount future rewards, reflecting a preference for smaller, more immediate rewards over larger, delayed ones. The dependent variable in our analysis was the number of tokens allocated immediately (i.e., range 0–5).
Instructions and examples of the experiment.

Exposure
We investigated four exposure variables: low birth weight (LBW), ACEs before the GEJE, traumatic experiences related to the GEJE, and ACEs after the GEJE.
Information on child birthweight was reported by caregivers based on information collected from their Mother-Child Handbook at baseline. Reference Fujiwara, Nawa and Matsuyama30 We categorized birthweight of less than 2,500 g as LBW. Self-reported LBW in the Mother-Child Handbooks has been reported to have 93% agreement with birth certificates, with a sensitivity and specificity of 92.5% and 99.7%, respectively. Reference Wise, Wang and Wesselink31
ACEs before or after the GEJE were reported by caregivers on the baseline questionnaire. ACEs reported by caregivers included whether the child: (1) was involved in a serious accident, (2) witnessed a serious accident, (3) was attacked by a dog or other animal, (4) had a close friend or family member with a serious illness, (5) experienced the death of a close friend or family member, (6) visited the hospital due to a serious disease/injury or underwent a serious medical procedure or was admitted to the hospital, (7) was separated from a caregiver, (8) experienced sexual assault, (9) experienced other criminal assault, (10) was bullied by peers in preschool or in the neighborhood, (11) experienced violence perpetrated by a close friend or family member, (12) witnessed a violent incident involving a close friend or family member, (13) had a close friend or family member who attempted suicide, (14) experienced a previous natural disaster, and (15) experienced other stressful events. We calculated the total number of these experiences and categorized them as 0, 1, 2, and 3 or more based on their distribution.
Child psychiatrists or clinical psychologists conducted semi-structured interviews with children to evaluate traumatic experiences related to the GEJE. Based on topics in other studies examining the mental health of children following a tsunami, Reference Thienkrua, Cardozo and Chakkraband32 the evaluation included assessment of: (1) separation from the caregiver, (2) the loss (death) of close family members or relatives, (3) the loss (death) of distant relatives or friends, (4) witnessing a tsunami, (5) witnessing a fire, (6) observing someone being swept away by a tsunami, (7) encountering a dead body, and (8) having their house damaged (destroyed or flooded). Interviewers refrained from inquiring further when children were unable to recall their experiences from the disaster, as additional probing had the potential to evoke painful and traumatic memories. We counted the number of traumatic experiences reported and categorized them as 0, 1, 2, and 3 or more.
Covariates
We selected potential confounders from the baseline survey with caregivers based on previous research. Reference Matsuyama, Fujiwara, Sawada, Yagi, Mashiko and Kawachi27 These included the child’s age at the time of the experiment, the child’s sex, maternal educational attainment (high school or less, some college, and college or more), and household subjective economic status before the GEJE (not stable, fairly stable, and stable).
Statistical analysis
We used multivariable Poisson regression models to examine LBW, ACEs before the GEJE, traumatic experiences related to the GEJE, and ACEs after the GEJE in relation to token allocation for immediate rewards (i.e., greater DD). This analysis yielded incident rate ratios (IRR), because our outcome (the number of allocated coins) is count data. In addition to the crude models, Models 1–4 estimated the associations between each exposure (i.e., LBW, ACEs before the GEJE, traumatic experiences related to the GEJE, and ACEs occurring after the GEJE) and the number of tokens separately, adjusting for potential confounders. In Model 5, each adversity was simultaneously added to the model, adjusting for potential confounders. A correlation matrix showed low correlations among the variables, with the highest correlation observed between ACEs before and after the GEJE (r = 0.336) (Supplementary Table S1), suggesting that multicollinearity is unlikely to be a significant issue in Model 5.
Multiple imputation by chained equations was applied to generate 20 imputed datasets to handle missing values in the covariates. To assess the potential for selection bias, we used inverse probability weighting (IPW) with stabilized weights. First, a logistic regression model was used to estimate the propensity score of selection based on relevant covariates, which were truncated at a minimum value of 0.01 to prevent extreme weights. Stabilized weights were then calculated by taking the ratio of the average probability of selection to each individual’s propensity score. Additionally, given that the study included 167 children from 143 families, we took into account the within-family correlation in order to estimate the standard error due to clustering within the household.
To address the potential confounding effects of hyperactivity traits, we conducted a sensitivity analysis by adding a hyperactivity trait variable, which may serve as a proxy for attention-deficit hyperactivity disorder. The trait was assessed based on behavior observed during a semi-structured interview and categorized as normal, hyperactive, or hypoactive.
We conducted exploratory analyses to examine the association of each ACE occurring before and after the GEJE, as well as each traumatic experience related to the GEJE, with DD. Due to convergence issues, multiple imputation could not be applied in this analysis, and therefore, missing cases for each adversity were excluded. Additionally, to explore the cumulative effect of all stressors, we calculated an adversity count, which represented the total number of ACEs before and after the GEJE, as well as traumatic experiences related to the GEJE. This count was used to examine the association between the cumulative effect of adversity and DD. Furthermore, we also examined the cumulative effects of LBW, ACEs before the GEJE, and traumatic experiences related to the GEJE by dichotomizing each variable (present or absent) and summing them to create a cumulative score ranging from 0 to 3. Lastly, we used structural equation modeling (SEM) to examine adversity over time, with the goodness of fit indices including the chi-square/degree of freedom ratio (χ 2/df), the comparative fit index (CFI), and the root mean square error of approximation (RMSEA). Acceptable critical values were defined as χ 2/df <5, CFI >0.95, and RMSEA <0.06.
All statistical analyses were performed using STATA version 16.0 (StataCorp., College Station, TX, USA).
Written informed consent was obtained from all participants, with parents or legal guardians providing consent for their children. The study protocols received approval from the Research Ethics Committee at the National Center for Child Health and Development and Tokyo Medical and Dental University.
Results
Child and caregiver characteristics are presented in Table 1. The mean ages of children were 4.8 (SD = 1.4) years old when they were exposed to the GEJE and 8.3 (SD = 1.4) years old when they participated in the DD experiment. Approximately 8% were born LBW. The prevalence of 3 or more ACEs before the GEJE was 7%, while after the GEJE, it increased to 13%. A total of 29 (17.4%) children reported having experienced 3 or more traumatic events related to the GEJE. The mean number of tokens allocated immediately was 2.7 (SD = 1.3), with approximately 63% of children allocating two or three tokens to receive an immediate reward.
Characteristics of the study participants (N = 167)

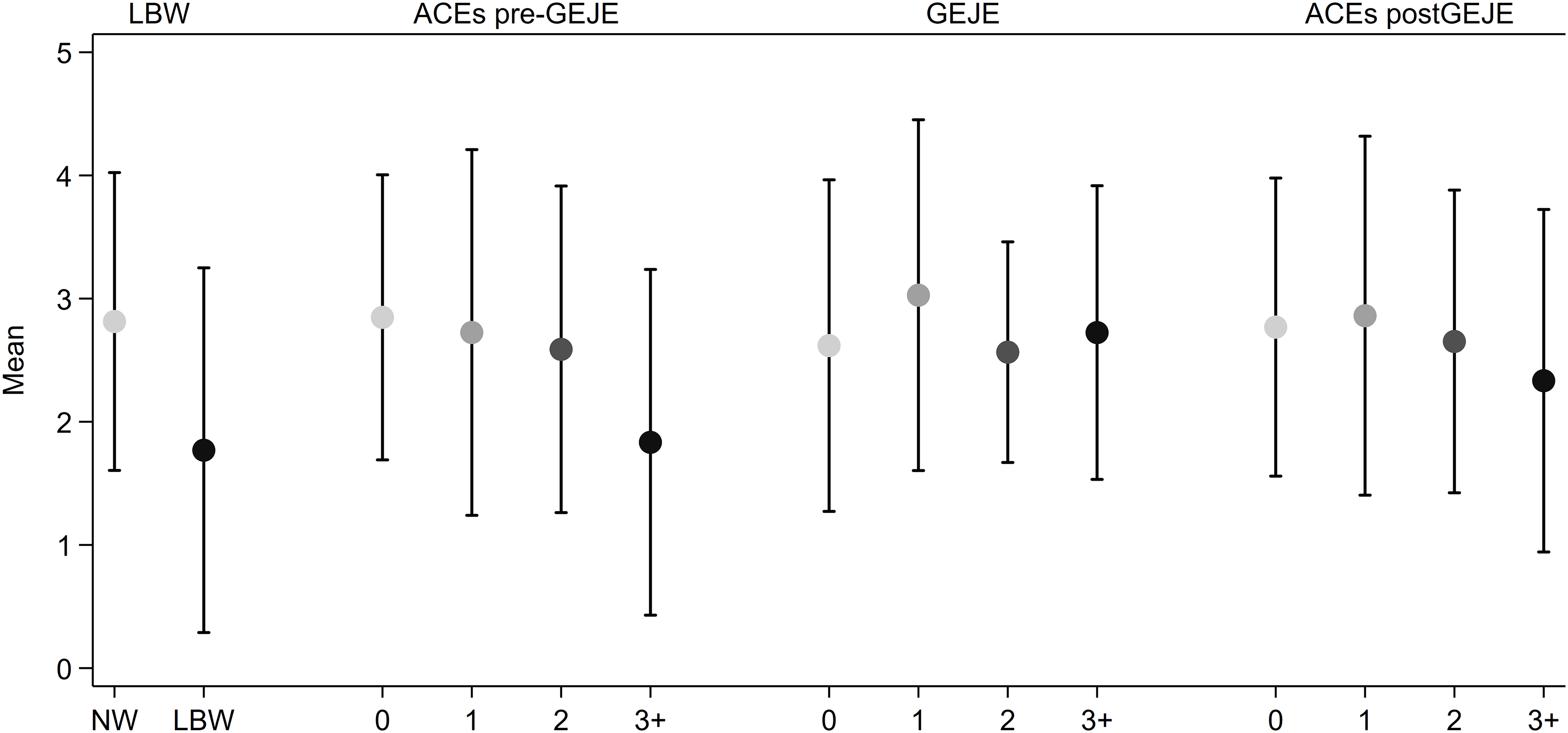
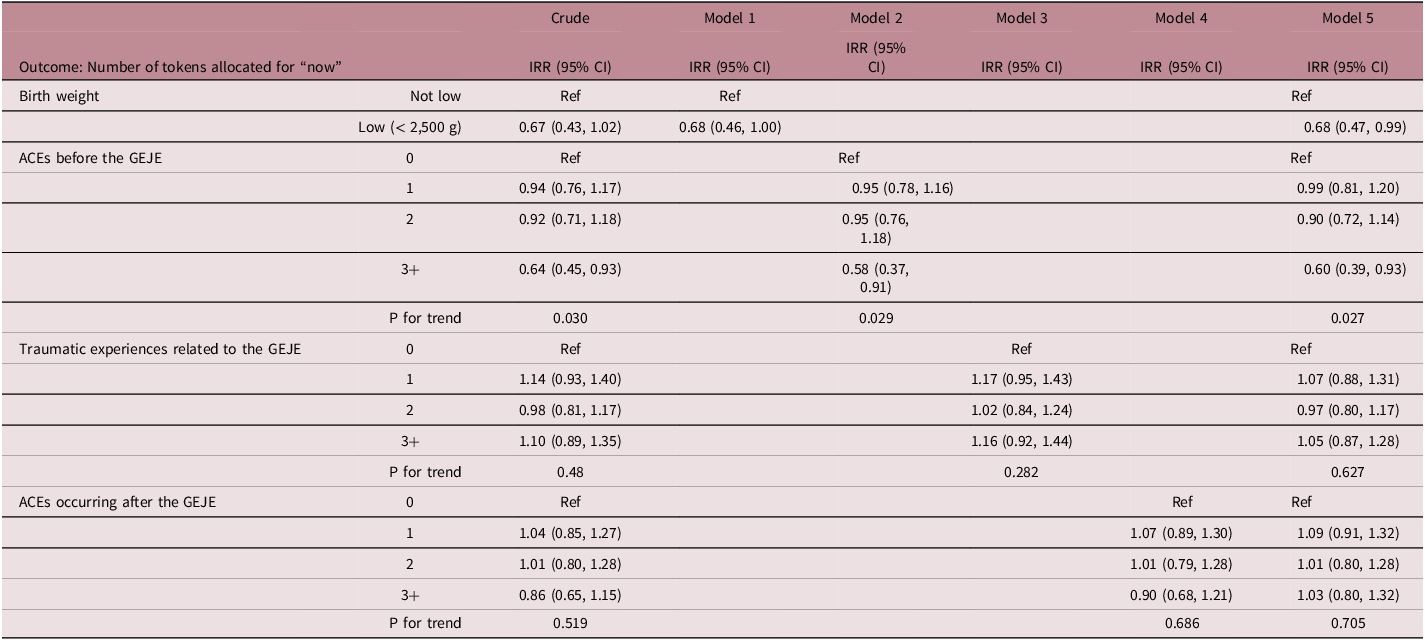
Figure 2 shows the number of tokens allocated “now” by each exposure, and Table 2 shows the results of the Poisson regression models examining the association between each adversity and children’s DD behavior. Children born LBW were 0.68 times less likely to allocate tokens for immediate rewards compared to children born with normal weight, indicating a lower likelihood of DD (95% CI: 0.46, 1.00). Similarly, children born with 3 or more ACEs before the GEJE were 0.58 times less likely to allocate tokens for “now” (95% CI: 0.37, 0.91). There was an inverse dose-response association observed between the number of ACEs occurring before the GEJE and DD (P for trend = 0.029). In contrast, child traumatic experiences related to the GEJE or ACEs after the GEJE were not associated with DD. The results were comparable to those obtained before multiple imputation, using dummy variables for missing data (Supplementary Table S2).
Distribution of tokens allocated immediately by each adversity experience. This figure illustrates the mean number of tokens allocated immediately by children who experienced adversities compared to those who did not. Each dot represents the number of tokens allocated immediately and the bars indicate the standard deviations. LBW, low birthweight; BW, normal weight; ACE, adverse childhood experience; GEJE, great East Japan Earthquake.

Results of multivariable Poisson regression models examining low birth weight, adverse childhood experiences, and natural disaster in relation to delay discounting (N = 167)

IRR, incidence rate ratio; CI, confidence interval; ACE, adverse childhood experience; GEJE, Great East Japan Earthquake. Model 1–4 separately estimate each stressor, adjusted for age, sex, education, and household subjective economic status before the GEJE.
Model 5 included all stressors simultaneously, controlling for the same confounders as in Model 1–4.
The sensitivity analysis, which included a variable for hyperactivity traits, did not change the results substantially (see Supplementary Table S3). In particular, the associations for both LBW (IRR = 0.67, 95% CI: 0.45–0.98) and ACEs (3+) before the GEJE (IRR = 0.56, 95% CI: 0.35–0.90) remained significant, suggesting the robustness of the findings. The association of each ACE before and after the GEJE and each traumatic experience related to the GEJE with DD was heterogeneous (Supplementary Table S4). Some experiences, such as the experience of a previous natural disaster before the GEJE, tended to be associated with higher DD (IRR: 1.61, 95% CI 1.23, 2.10), while violence exposure perpetrated by a close friend or family member before the GEJE was associated with lower DD (IRR: 0.20, 95% CI: 0.05, 0.85). Supplementary Table S5 indicates that when the number of stressors – defined as the sum of ACEs before the GEJE, traumatic experiences related to the GEJE, and ACEs after the GEJE – was combined into an overall adversity count, no significant association was found with DD (P for trend = 0.335). Similarly, no clear cumulative effect on DD was observed when the number of dichotomized adversities was summed (P for trend = 0.266) (Supplementary Table S6). The SEM model indicated a poor fit with χ 2/df = 3.25, CFI = 0.862, and RMSEA = 0.122, suggesting an inadequate model fit (Supplementary Figure S1). Therefore, we did not use SEM as a primary analytical approach.
Discussion
Children born LBW as well as those who experienced 3+ ACEs before the GEJE allocated tokens to receive more future rewards, displaying lower rates of DD, compared to children who were not LBW and experienced <3 ACEs, respectively. An inverse dose-response association was observed between the number of ACEs before the GEJE and DD. In contrast, children who had traumatic experiences related to the GEJE or had ACEs occurring after the GEJE did not show a significant association with DD after adjustment of LBW and ACEs. This study is the first to simultaneously investigate and compare the impacts of prenatal factors like LBW and postnatal experiences like ACEs on DD. The results showed that LBW and ACEs during preschool had a significant inverse impact on DD. Furthermore, the type of traumatic event and ACE affected DD differently.
We found that children with LBW tended to allocate fewer tokens to immediate rewards, which is inconsistent with previous studies. Reference Lynn, Cuskelly and Gray19,Reference Schlotz, Godfrey and Phillips20,Reference Lynn, Cuskelly, Gray and OCallaghan33 However, we considered that this result supports the thrifty phenotype hypothesis, i.e., that intrauterine undernutrition can lead to the tendency to seek more resources. Reference Hales and Barker1,Reference Hales and Barker2,Reference Silveira, Agranonik, Faras, Portella, Meaney and Levitan8,Reference Levitan and Wendland34–Reference Prentice36 According to the thrifty phenotype hypothesis, the obesity risk among LBW children is not only due to metabolic and endocrine changes but also due to impulsivity and obesogenic eating behaviors, i.e., a preference for energy-dense foods, termed thrifty eating behavior. Reference Silveira, Agranonik, Faras, Portella, Meaney and Levitan8,Reference Levitan and Wendland34 Several previous studies showed that people who experienced IUGR prefer high-fat, high-carbohydrate diets after they grow up. Reference Bischoff, Portella and Paquet7,Reference Lussana, Painter, Ocke, Buller, Bossuyt and Roseboom35,Reference Ayres, Agranonik, Portella, Filion, Johnston and Silveira5,Reference Boone-Heinonen, Weeks, Sturza, Miller, Lumeng and Bauer37 Moreover, a study involving 160 children, including 35 with IUGR born after 35 weeks, reported that girls who had experienced IUGR had a strong tendency toward impulsive eating at age three. Reference Silveira, Agranonik, Faras, Portella, Meaney and Levitan8 These studies showed that LBW children have the tendency to seek additional resources to compensate for in utero deprivation, supporting our result that children with LBW in this study placed more tokens for a month later to acquire more resources, i.e., candy. We add to the literature that LBW children may show thrifty behaviors regardless of time scale, at least within one month.
However, the thrifty phenotype hypothesis alone may not fully explain the results of this study. Previous findings have shown contradictory results, that is, children with very low birthweight (VLBW) and ELBW showed higher DD, interpreted as poor self-control capabilities. Reference Lynn, Cuskelly and Gray19,Reference Schlotz, Godfrey and Phillips20,Reference Lynn, Cuskelly, Gray and OCallaghan33 A study examining brain MRI and temperament of 27 participants ages 15–16 found that LBW was associated with inhibitory control and small orbitofrontal cortex surface area, which correlates with low self-regulation. Reference Schlotz, Godfrey and Phillips20 Moreover, a study comparing 30 ELBW with 29 normal birthweight children found that at ages 2–4 years ELBW children had higher DD. Reference Lynn, Cuskelly and Gray19 These inconsistencies with previous research might be due to differences in the measurement of DD and age. The former study asked parents about their children’s temperament, which does not directly reflect the child’s responses or behavior. Reference Schlotz, Godfrey and Phillips20 In the latter study, DD was evaluated using the following self-regulation tasks; If a child could wait for the experimenter to return, they would receive two chocolates, if not, they would receive one. This experiment assessed the child’s ability to use self-control to obtain a delayed but larger reward, despite the fact that the waiting period was undisclosed. Reference Lynn, Cuskelly and Gray19 In contrast, our study used two distinct time points, and rewards could be obtained at different times: immediately or one month later. As a result, the task in our study required not only self-control but also the ability to perceive the passage of time (i.e., one month in this study) and the instability of the environment (i.e., the housing situation in the aftermath of the Great East Japan Earthquake). As the previous study included children aged 2–4, these children may not have fully understood the amount of chocolate. Reference Lynn, Cuskelly and Gray19 In contrast, our study included children with an average age of 8 (who could more fully comprehend the total reward amount), thus enabling them to show thrifty behaviors to try to obtain more rewards.
One’s perception of time requires the collaboration of multiple brain structures, such as the prefrontal cortex, parietal lobe, basal ganglia, and hippocampus. Reference Fontes, Ribeiro and Gupta38 Among these, the prefrontal cortex is deeply involved in executive function, including goal setting, task organization, and prospective planning; it is also a crucial brain structure for long-term decision-making. Reference Hiser and Koenigs39 A study of 55 preterm LBW infants and 81 controls reported that smaller cortical surface areas were associated with greater executive function deficits. Reference Østgård, Sølsnes and Bjuland40 Additionally, prior studies have reported that LBW children have smaller prefrontal cortex surface area and volume as well as score lower on tests of executive functioning than normal-weight-birth children. Reference Raznahan, Greenstein, Lee, Clasen and Giedd41,Reference van Houdt, Oosterlaan, van Wassenaer-Leemhuis, van Kaam and Aarnoudse-Moens42 A study of 139 twin pairs showed that birthweight was positively correlated with the surface area and the volume of the prefrontal cortex regardless of gestational age. Reference Raznahan, Greenstein, Lee, Clasen and Giedd41 A meta-analysis of 35 studies reported that normal-weight-birth children scored higher on executive functioning than children who were LBW, which was consistent across ages. Reference van Houdt, Oosterlaan, van Wassenaer-Leemhuis, van Kaam and Aarnoudse-Moens42 Previous studies have shown that LBW children tend to have poorer comprehension of the passage of time compared to normal-weight children. Reference Hüning, Assing, Weishaupt, Dransfeld, Felderhoff-Müser and Zmyj43,Reference Tinelli, Anobile and Gori44 In one study, 25 extremely LBW children and 26 normal-weight children took a test assessing the comprehension of time; in this test, three hourglasses containing different amounts of sand were flipped simultaneously. Children were asked to predict and justify which would empty first and last. Once the sand ran out, the hourglasses were randomly repositioned and the predictions repeated. The results indicated that LBW group had less accurate perceptions of time. Reference Hüning, Assing, Weishaupt, Dransfeld, Felderhoff-Müser and Zmyj43 Therefore, it is possible that due to their impaired perceptions of time, children with LBW seek more resources, regardless of the time needed to wait, leading to lower DD.
In our study, children who experienced 3+ ACEs before the GEJE also showed lower DD. Prior research suggests that childhood ACEs might lead to a thrifty phenotype. Reference Danese and Tan45–Reference Tyrka, Price, Marsit, Walters and Carpenter47 For example, people who have experienced maltreatment often have a smaller prefrontal cortex volume, which is potentially linked to impaired inhibitory control of eating behaviors. Reference McGowan, Sasaki and DAlessio46 Studies using functional magnetic resonance imaging (MRI) to examine brain structure have reported that ACEs appear to dull the response to rewards and feelings of satisfaction, which could lead individuals to take greater risks in order to get larger and more potent rewards. Reference Boecker, Holz and Buchmann48–Reference Herzberg and Gunnar50 Thus, similar to the explanation of LBW and high DD, children with ACEs may show more thrifty behaviors, that is, seeking more rewards, regardless of time scale.
However, other research has shown that ACEs may increase the risk of high DD in adulthood. Reference Acheson, Vincent, Cohoon and Lovallo22,Reference Shain, Nguyen and Meadows23 The inconsistency with previous studies might be due to the timing of assessment, that is, our study assessed DD and ACEs during childhood, by parents, while in the other studies they were assessed in adulthood, by self-report. Although there is a correlation between retrospective assessment of ACEs in adulthood and in childhood Reference Reuben, Moffitt and Caspi51 , ACEs should be assessed at the time of childhood, and objectively, to avoid common method bias and minimize the recall bias. Reference Fujiwara52 Thus, if we employ a more accurate assessment of ACEs, children who experienced ACEs showed thrifty behaviors, regardless of time scale, because of their impulsiveness. Children who experienced multiple ACEs during childhood may have a poor sense of time. A study involving 69 children, ranging from 8 to 14 years old, that used MRI scans to explore brain structure, indicated that children who experienced more severe trauma during childhood had a smaller hippocampus, Reference Rooij, Smith and Stenson53 a region of the brain which plays a crucial role in how we perceive the passage of time. Reference Fontes, Ribeiro and Gupta38,Reference Meck, Church and Matell54 This link between the size of the hippocampus and experiences of child maltreatment has been supported by a meta-analysis. Reference Riem, Alink, Out, Van Ijzendoorn and Bakermans-Kranenburg55 Therefore, in our study, it is likely that children with 3 or more ACEs might have allocated more tokens for a larger delayed reward (1 month later) without much concern for the one-month duration.
We found that trauma related to the GEJE and ACEs occurring after the GEJE did not affect DD. Interestingly, a prior study using the same cohort data indicated that trauma related to the GEJE, particularly severe housing destruction, contributed to higher DD across the whole population (including LBW and non-LBW children). Reference Matsuyama, Fujiwara, Sawada, Yagi, Mashiko and Kawachi27 In the current study, the effects of trauma related to the GEJE on DD became non-significant when LBW and pre-disaster ACEs were included as covariates in the multivariate analysis, indicating that LBW and pre-disaster ACEs might be confounders of the association between trauma related to the GEJE and DD. Since children with LBW or pre-disaster ACEs have difficulty in perceiving the passage of time and in understanding the instability of their environmental circumstances, it is possible that they may have underestimated the risk of waiting for delayed larger rewards and therefore delayed getting their rewards, i.e., showing lower DD.
Exposure to ACEs can affect the development of the prefrontal cortex, which is involved in decision-making, impulse control, and foreseeing the consequences of one’s actions. Reference Hanson, Chung and Avants56,Reference Luby, Barch, Whalen, Tillman and Belden57 This leads to diminished judgment and a tendency to underestimate risks associated with behaviors. Reference Campbell, Walker and Egede58,Reference Hughes, Bellis and Hardcastle59 A mother-child cohort study involving 41 ELBW children and 128 controls showed that the former had a thinner cortex overall and insufficient development of the posterior corpus callosum, right pallidum, and right thalamus at ages 8 to 9. Reference Sripada, Bjuland and Solsnes60 These developmental deficiencies in brain structures are associated with reduced cognitive function and the ability to organize information for goal setting. Another possible explanation is that early ACEs attenuated sensitivity to earthquake-related trauma. Prior research found that experiencing the Great East Japan Earthquake increased PTSD risk only among individuals without ACEs. Reference Inoue, Stickley and Yazawa61
Life-course epidemiology also aids in the explanation of these findings, with models such as critical/sensitive periods, pathway models, and cumulative models explaining how ACEs lead to poor health in adulthood. Reference Fujiwara52 The critical/sensitive period model posits that there are critical or sensitive periods in brain development during childhood (including the prenatal period), and therefore, the detrimental effects of early life ACEs can persist into adulthood. A longitudinal study of 165 children and their mothers compared the impact of unpredictable events such as frequent changes in parents’ job status, housing, and parental remarriage or divorce during early childhood (0–5 years) and after (6–16 years) on sexual behavior and high-risk behavior. Reference Simpson, Griskevicius, Kuo, Sung and Collins62 The study found that unpredictability during early childhood significantly increased the risk of sexual and high-risk behaviors, while unpredictability after early childhood did not have the same effect.
Results of our study showed that children with LBW and multiple ACEs during early childhood had a tendency to seek more resources. In contrast, when all the stressors, including ACEs before and after the GEJE and traumatic experiences due to the GEJE, were summed to calculate an adversity count, no significant association was found between the adversity count and DD. Furthermore, we constructed a SEM including LBW, ACEs before and after the GEJE, and the GEJE-related trauma to examine the paths among these factors. However, the model fit was poor, and we found no significant association between LBW and ACEs before the GEJE. Only the paths from pre-disaster ACEs and LBW to DD reached significance. While a significant correlation between pre- and post-disaster ACEs may suggest a temporal or mediated structure, our initial model did not meet conventional fit criteria, and thus we did not further pursue refinement of the SEM. Results imply that the critical period for developing a thrifty phenotype may be in early childhood, up to age five, as our study participants experienced ACEs before age five. These results suggested that they can achieve low DD in adulthood if they receive appropriate training to enhance self-control and executive functioning. Reference Duncan, Gerner, Neel, Burton, Byrne and Warschausky63–Reference Wu, Hsieh and Hsu66
A systematic review of 35 studies on interventions to improve executive function in preschoolers up to age three in LBW or preterm-birth children demonstrated that some reported improved impulse control and self-regulation. Reference Duncan, Gerner, Neel, Burton, Byrne and Warschausky63–Reference Wu, Hsieh and Hsu66 In a study of 109 LBW children and 73 normal birth weight children, interventions to enhance parental responsiveness when LBW children were two years old showed catch-up in behavioral and mental development at age six among LBW children that matched that of normal birth weight children. Reference Walker, Chang, Younger and Grantham-McGregor65 Further research is warranted to determine if these interventions contribute to lower DD in LBW children as they get older, highlighting the ongoing nature of this important area of study.
This study has several limitations. Firstly, our experiment to study DD presented only one option without varying the amount of the rewards or delay times. Consequently, we could not quantitatively assess whether children’s choices varied with the discount rate or over time. However, it has been previously reported that single-choice experiments can produce results similar to multiple-choice experiments when repeated among the same children. Reference Angerer, Lergetporer, Glätzle-Rützler and Sutter29 Secondly, we did not provide multiple reward options (e.g., candies, stickers, pencils), but rather the reward was only candy, which might have been considered of minor value to some children. Thirdly, ACEs were measured retrospectively, introducing the possibility of recall bias. Furthermore, experiencing the disaster may have affected how participants recalled their ACEs. Reference ÖB67,Reference Dunn, Soare and Raffeld68 For example, it has been reported that individuals who have experienced trauma from a major earthquake tend to avoid recalling more distant negative experiences so as not to trigger associations with their traumatic event. Reference ÖB67 Additionally, some studies suggest that the psychosocial impact of ACEs may be stronger when they are more recent. Reference Dunn, Soare and Raffeld68 However, based on these findings, the influence of ACEs before the GEJE would be weaker than that of ACEs experienced after the GEJE. Despite these studies, our results showed that higher levels of pre-disaster ACEs continued to have a significant impact on DD, suggesting the importance of considering a sensitive period in childhood. Fourth, although we examined the relationship between the total number of ACEs or GEJE-related trauma and DD in order to observe the cumulative effects, we did not assess the severity of ACEs or trauma experiences. Future studies should consider trauma severity to provide a more nuanced understanding of its impact on DD. Fifth, the participants’ municipalities were not randomly selected from disaster-affected areas. Children who experienced severe trauma related to the GEJE (e.g., children in areas that suffered particularly severe damage from the tsunami) might not have participated in the survey, possibly leading to an underestimation of traumatic experiences. Also, some children might not have accurately reported their traumatic experiences during interviews or might have erased their memories as a form of psychological adjustment. Finally, the small sample size warrants cautious interpretation of our findings. Although the study suggests that different ACE experiences may influence DD in distinct ways, we cannot draw definitive conclusions about the specific impact of different types of ACEs in the present study.
In conclusion, this study demonstrated the contribution of LBW and ACEs before the GEJE in early childhood in lowering DD in later childhood. This effect surpassed the impact of trauma related to the GEJE and ACEs following the GEJE on DD. Children with LBW might display the thrifty phenotype described in the DOHaD hypothesis and therefore tend to seek more resources. Early childhood ACEs may also lead to the thrifty phenotype, with a sensitive period up to age five. Finally, children with LBW or multiple ACEs in early childhood did not always show high DD. Future research is needed to develop interventions that utilize the thrifty phenotype to help children with LBW or multiple ACEs in early childhood acquire improved self-control.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S2040174425100160.
Acknowledgments
None.
Financial support
This work was supported by a grant from the Ministry of Health, Labour and Welfare (H24-jisedai-shitei-007, H25-seiiku-shitei-00x, H28-sukoyaka-shitei-003, H28-kodomokosodate); Japan Society for the Promotion of Science (19H04879); and Meiji Yasuda Mental Health Foundation (H28). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests
Dr Surkan maintains a paid academic appointment at the Institute of Science Tokyo. This arrangement has been reviewed and approved by Johns Hopkins University in accordance with its conflict of interest policies.
Ethical standards statement
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation (Ethical Guidelines for Medical and Biological Research Involving Human Subjects) and with the Helsinki Declaration of 1975, as revised in 2008, and has been approved by the institutional committees (The Research Ethics Committee at the National Center for Child Health and the Development and Tokyo Medical and Dental University).





 Open access
Open access