
Case history of a killer disease: Reye’s syndrome: a medical mystery
This year in the wake of an outbreak of influenza B virus 250 cases of Reye’s syndrome have been reported in the United States, with 90 deaths …
Peter arrived as a new assistant professor of pediatric neurology at Yale University in 1966. This was in the midst of the Reye’s syndrome peak of the late 1960s. Reye’s syndrome is a life-threatening pediatric disease characterized by progressive brain and liver damage in children, often after a viral illness. It became a rare condition after epidemiological studies suggested a link between aspirin use in children and the onset of Reye’s syndrome after a viral illness. The reduced rates of Reye’s syndrome are largely attributable to public health messaging to limit aspirin use in children, but until that change, it often fell to pediatric neurologists to keep Reye’s syndrome patients alive.
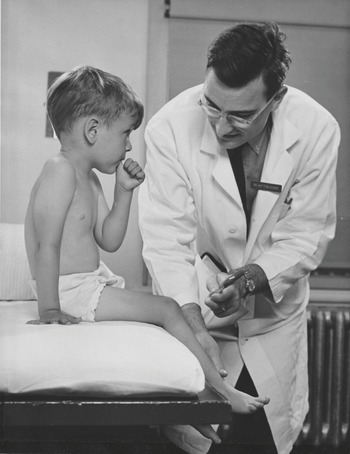
Based on clinical demand, Peter allowed clinical pediatric neurology to consume the largest share of his professional time and attention (Figure 11.1). One of Peter’s medical colleagues, Gabe Mirkin, noted in his online newsletter (DrMirkin.com) in September 2013: “In 1962, when I was a resident at the Massachusetts General Hospital, Peter often consulted on my neurology patients. He would write 30 page-long hand-written histories and physicals on my patients, the result of hour-long interviews (other consultants rarely wrote more than a couple pages or spent more than a few minutes with the patients).” One can ponder whether modern care-tracking medical systems would now tolerate such clinical inefficiency. Peter showed similar commitment to patients with Reye’s syndrome. In the 1960s and 1970s the treatment of these patients could be all-consuming. As neurologist Carter Snead put it, during an interview in May 2022, “The kids died left and right.” Peter would guide their treatment directly in the intensive care unit at all hours of the day and night. Inevitably, this left Peter with less time and less mental space for his scientific research. However, he became a spokesperson for the care and management of patients with Reye’s syndrome and developed a national reputation in the area (Figure 11.2).

Yale University image of Peter talking to the media about Reye’s syndrome in New Haven, Connecticut, in the early 1970s.

The scientist portions of Peter’s activities, while given less time, were never fully set aside. Carter Snead was Peter’s first clinical fellow as a faculty member at Yale University. He later became head of the Department of Neurology at the Hospital for Sick Children at University of Toronto, and a lead researcher in the basic science of epilepsy. Snead remembered that Peter:
had an unbelievable wide range of intellect. An amazing clinician – watching him do an exam provided a wonderful synthesis of clinical findings. He was a true physician scientist before it was even a term … He taught me to do research – I did not even know which end of a test tube was up … He knew I was interested in epilepsy – and suggested an experiment. The experiment worked and launched my entire research career on the basic science of epilepsy.
Snead was only warming up, as he went on to say: “[Peter] did ground breaking work that opened new fields – and then let someone else fill in the details.” He was “visionary.” He was a “Golly gee whiz kind of guy – nothing fake about it – this is how he was – wide eyed with curiosity about everything – and this masked an unbelievable intellect.”
One of the highest-impact outcomes from Peter’s time at Yale was that he pioneered the ketogenic diet for epilepsy. He devised a very - low - carbohydrate, high - saturated - fat diet that was palatable and showed that it worked for epilepsy. Snead noted, “it is still a second-line therapy for the treatment of children with epilepsy.” A ketogenic diet was first tried in the 1920s, but it never caught on because the children refused to eat it. Peter showed that medium-chain triglyceride (MCT) oil worked and made it palatable. He made an “MCT ice cream” and also went on to show it was effective. Published in Pediatric Research in 1976, he reported improved epilepsy control in children with intractable seizures [Reference Huttenlocher1]. The “MCT” diet, comprised of 60% MCT oil and a more palatable combination of protein and carbohydrates, replaced the classic ketogenic diet for use in children with epilepsy.
Snead said that Peter told him, “If you are a clinician scientist – when you are in the lab putzing around – PhD colleagues think you are a dabbler since you are not there full - time.” He went on to say that clinician scientists have a “huge disadvantage in the grant game. However, the advantages are huge – you can see clinical ramifications – Peter taught me this. He had the vision and saw the importance of synaptogenesis – and what it meant for the developing brain – he used to talk to me about it” (this was well before Peter’s discoveries about synaptic pruning). As Eric Kandel later said about this discovery, in his message for Peter’s memorial service, “He saw implications of his findings that many people who had only had a basic science background might have overlooked.”
It was for all of these reasons that Doris Trauner, currently a pediatric neurologist and professor at the University of California – San Diego, decided to do her pediatric neurology training with Peter at Yale. Shortly after Doris signed on to train at Yale, Peter called to let her know that he would be looking for a job in Chicago. She was stunned that this “famous” talented pediatric neurologist was following his wife to Chicago and had yet to find a job. The move was triggered because Janellen, a rising talent on the Teachers College (Graduate School of Education) faculty at Columbia University, was unable to procure a job at the Yale University Department of Psychology. As Janellen said: “they were explicitly not interested in hiring female faculty” at the time. Professor positions at research universities were rarely offered to women in the 1960s and 1970s. When the University of Chicago recruited Janellen to a prestigious chaired professorship, Peter and Janellen decided it was time to make a move. a move was also motivated by the long commutes to New Haven and New York, which were taxing for a family that now included three children.
Peter started a faculty position at the University of Chicago School of Medicine in 1974. Doris Trauner decided to make the move to the University of Chicago with Peter. She said that, at the time, few people were interested in taking female trainees and he was very supportive. Trauner already had a publication in the Reye’s syndrome field, and he supported her independent pursuit of this project during her training. In an interview in February 2022, she said: “I had the freedom to do what I wanted” and was assisted by Peter’s technician Fran at the University of Chicago. While Trauner worked on Reye’s syndrome she watched with wonder as Peter spent hours at the electron microscope, imaging synapses. He did not have a team. He did this work alone and let Trauner pursue her independent interests. She said: “It was amazing; he did it himself, and his work is still quoted all of the time in pediatric neurology and developmental neuroscience.” Peter was a “thought leader” in human developmental neuroscience.
Doris Trauner recalled sitting for hours in Peter’s office stacked high with journals and papers in seeming chaos, discussing patients and science. Hours of one-on-one mentoring. He enjoyed what he did and was enthusiastic about both the clinic and research. He was a
creative thinker – he would talk about something outside of his field and he would have creative ideas – he was fun to talk to – a superb clinician and diagnostician … you do not come across people like that often. He instilled this into the people he trained – you spend time thinking about what is going on with the patient – what is causing this? Do not take anything for granted. He was thorough and precise, and modeled critical thinking.
Trauner did, however, note that Peter was not a very good administrator. He was “kind and modest and never wanted to do anything to get recognition – he did it because he thought it was the right thing to do.” However, if someone was hired and failed to do a good job, he did not deal with the problem. He avoided conflict and did not handle administration – above or below him – well. He never fired anyone. As Snead said, “Peter had a kind of naivete and innocence” – and was not good for administration “because he was too trusting of everyone.”
The Child Neurology Residency Training Program at the University of Chicago was begun in 1976 by Peter. The program has trained a cohort of pediatric neurology fellows who are now professors at universities across the United States. The former fellows gather yearly at the pediatric neurology meetings to dine – in years past with Peter present – and they still continue this tradition in his absence. When Peter started at the University of Chicago, neurology was in chaos. Adult neurology had been decimated and the entire team had relocated to another university. Pediatric neurology was under the control of the chair of the Department of Pediatrics, who seemingly did not have interest in neurology and was not supportive of the pediatric neurology program, financially or otherwise. Peter was a kind of “spousal hire” and had limited negotiating power (or skill) to advocate for the team. After Peter’s arrival, Barry Arnason became the new director of adult neurology, and recruited a team of neurologists that enlivened the adult team and interfaced well with pediatric neurology (Figure 11.3). However, they did not have the power to make the work conditions better for Peter in the Department of Pediatrics.

Peter also started a learning disabilities clinic at the University of Chicago. This clinic was the first of its kind in the nation. In clinic, Peter worked with faculty member Susan Levine, a developmental psychologist who also worked with Janellen. Levine said, in an interview in February 2022: “the kids loved him. … He saw complicated patients with difficult diseases and the families were struggling. Peter gave them hope – not false hope – but he believed in the plasticity of the brain and the capacity for the children to improve. He also gave the families strategies to cope and how to work with their child.”
Peter also enjoyed training medical students. He was a popular medical school professor, both in the lecture hall and at the patient’s bedside. A former medical student and joint recipient of the 2011 Nobel Prize in Physiology or Medicine, Bruce Beutler, was quoted in the University of Chicago magazine as recalling that Peter Huttenlocher’s mode of instruction was “teaching by example.” “From him I first learned that children, and in particular infants are almost like a different species. They must be examined for neurological function using entirely different tests and evaluation criteria than adults.” Beutler also noted that Reye’s syndrome was alarmingly common in those years: “I remember such a patient, a boy who was treated with aspirin when he had chicken pox and had a severe encephalopathy. Peter seemed deeply moved … I remember him calling out to the comatose child by name, hoping for a response.”
After Peter’s passing, one of his former Reye’s syndrome patients, now a tenured professor, emailed me with the subject: Thanks to your dad for saving my life.
Dear Anna,
Pardon me for contacting you unsolicited and out of the blue, but my mother sent me Peter Huttenlocher’s obituary, and through some googling, I found that you’re his daughter and you’re at UW–Madison [University of Wisconsin–Madison], which is where I got my PhD, and your father saved my life, so the confluence of all those facts made me really want to reach out to you. The life-saving part involves me at age 8 contracting Reye’s syndrome following my receiving aspirin for a fever. I have almost no recollection of the events, but my parents told me that after getting chicken pox, I started acting weird. My pediatrician didn’t think much of it and sent me home with a pat on the head, but my grandma was visiting us then, and I apparently hit her and told her I hated her, and from this she recognized instantly that I was not right. So my parents brought me back to the doctor, and I subsequently ended up under the treatment of your father. While in the hospital, I slipped into a coma for two days, and my mom tells me your father stayed at the hospital for the whole time. She said when I finally emerged from the coma, he reacted like “a proud papa.” Again, I don’t remember any of this, but I can now obviously recognize what this meant, and my mom sent me a long letter detailing the whole experience after seeing your father’s obituary. Long part of the story short, after being saved by your father, I got through middle & high school, went to college at University of Illinois, then went to grad school at UW-Madison, where I got my PhD in film studies. I then got a job teaching film studies, published a book, got tenure, got married, and all along have had an extremely happy life. So … it feels weird to email someone to say, “Thanks to your dad for saving my life!” but I did want to share this thought nonetheless. Though I don’t remember much of what I went through, your dad’s name and his dogged pursuit of medical knowledge will forever mean the world to me and my family. I am so sorry for your loss (and humanity’s loss), but I hope that hearing of his impact on one life will serve some value.
Thanks, and bless you and your family
In another former-patient encounter, this time unrelated to Reye’s syndrome, I was approached after teaching Immunology to undergraduates at the UW–Madison. A student, Andrew, came up to me after class and said: “Your father was my doctor.” Andrew’s mother subsequently described his condition in an email:
It was late summer in 1995, when we went to our family doctor and he had no idea what was wrong with Andrew. He told us to make an appointment with Dr. Huttenlocher because he said if anyone can make a diagnosis it would be him. At the appointment, Dr. Huttenlocher asked about Andrew’s symptoms. I was surprised that he did not physically examine Andrew, but he asked him to go to the long hallway outside his office and walk back and forth. As Andrew was walking back towards us, Dr. Huttenlocher said that Andrew has strep and needs to be tested, that he has rheumatic chorea that would get better in about 8 weeks and that he needed to see a pediatric cardiologist for any possible heart damage. I was amazed that he could tell all this by Andrew just walking in the hallway. What struck me was his calm demeanor and his assurance that this was all manageable. It was a relief. He also told us that there used to be hospital wards with children with rheumatic chorea and that he had not seen any case in about 20 years. We are looking forward to reading the book when it is published and sharing it with our family.
Andrew said:
When I was a child of ~10 years I remember having a very bad cold/flu and feeling the worst I had ever felt, I also had hives all over, and later a type of palsy on one side of my body. My pediatrician was flummoxed, and referred me to a specialist and children’s hospital by the University of Chicago, Dr. Huttenlocher. I remember he was a kind older man with a European accent who reminded me of my Grandpa. He quickly diagnosed me with rheumatic chorea, and referred me to a pediatric cardiologist as my heart may have been damaged. I then was put on a prophylaxis treatment of penicillin to prevent me from getting strep throat again and causing another reaction. I had some heart damage due to my illness that if Dr. Huttenlocher had not treated early enough I may have died or had permanent heart problems. Thankfully, my heart healed during my teenage years, and I no longer have a heart murmur. I remember how Dr. Huttenlocher had a great bedside manner as he addressed me, a precocious child at the time, with respect, like an adult.
Peter habitually talked to children like they were adults. Trauner also noted “he treated everyone equally” – women, men, his patients – “he treated everyone with the same amount of respect and consideration – patients from all backgrounds.” The boy from Germany may have found his greatest calling as a physician, taking care of patients.