


Introduction
Food insecurity (FI), defined as unreliable access to sufficient, safe, and nutritious food (WHO and FAO, 2002), is a critical global health concern, affecting an estimated 343 million people across 74 countries (WFP, 2025). The consequences are wide-ranging, encompassing compromised diet quality, increased susceptibility to diet-related diseases, and adverse impacts on mental health and overall well-being (Pollard et al., Reference Pollard, Booth and Jancey2002). Beyond immediate hunger, FI represents a fundamental threat to health equity, social participation, and human dignity, positioning it not only as a welfare issue but as a pressing public health and social justice concern.
In the UK, FI disproportionately affects low-income and marginalised populations and is worsening through rising costs and reducing welfare support (Lambie-Mumford, Reference Lambie-Mumford2018). Marginalised groups in this context include low-income households, lone parents, people with disabilities, migrants and people with insecure immigration status, and individuals in precarious or unstable employment, who may face compounded structural and social barriers to accessing adequate food. In 2022/23, approximately 7.2 million people in the UK experienced FI, including 17% who were children; by mid-2024, this rose to nearly 10 million (The Food Foundation, 2024). FI likely increased over this period because the cost-of-living crisis and wider supply shocks (including the Ukraine war) raised household bills and food costs, while ongoing post-Brexit trade frictions also contributed to higher UK food prices, tightening budgets and increasing reliance on food aid (Bakker et al., Reference Bakker, Datta, De Lyon, Opitz and Yang2022; The Food Foundation, 2024). These intersecting economic pressures have intensified household precarity, pushing increasing numbers of individuals towards charitable food provision as a coping mechanism.
This study examines experiences across both formal and informal food aid settings, focusing on under-represented, non-referral-based, volunteer-led services. In the UK, formal food aid includes referral-based services run by charities or authorities, targeting short-term crises (Garthwaite et al., Reference Garthwaite, Collins and Bambra2015), which typically require individuals to obtain a voucher from a recognised professional (e.g., a GP, social worker, or welfare adviser) confirming crisis need before accessing emergency food parcels (Garthwaite et al., Reference Garthwaite, Collins and Bambra2015; Loopstra et al., Reference Loopstra, Reeves and Tarasuk2019). In contrast, non-referral-based or informal food support services, including community pantries, food clubs, social supermarkets, and volunteer-led initiatives, allow individuals to self-refer and access support without professional gatekeeping, often operating through flexible membership or low-cost subscription models, offering flexible, community-led support (Power et al., Reference Power, Doherty, Small, Teasdale and Pickett2018; Caraher and Davison, Reference Caraher and Davison2019). Despite the scale of the crisis, official statistics underestimate FI, as many who rely on informal or non-referral-based food support remain uncounted (Stone and Papadaki, Reference Stone and Papadaki2025). Hence, they overlook individuals who avoid referral pathways due to stigma, mental health challenges, or distrust of institutions, as well as those who rely primarily on informal community provision. Consequently, their lived experiences are often absent from research and policy.
Across both settings, food banks play a vital role in alleviating immediate hunger; however, they often provide shelf-stable, ultra-processed foods (UPFs) with limited nutritional value (Hardcastle and Caraher, Reference Hardcastle and Caraher2021). Reliance on these foods contributes to diets high in calories but low in nutrients, increasing risk of obesity, hypertension, diabetes, and other non-communicable diseases (Morales and Berkowitz, Reference Morales and Berkowitz2016; Caraher and Davison, Reference Caraher and Davison2019; Chávez-Ugalde et al., Reference Chávez-Ugalde, Contreras-Manzano and Moreno Altamirano2024).
With UPFs now comprising 58% of the average UK diet, the public health implications are substantial (Mutebi, Reference Mutebi2024), particularly as every 10% increase in UPF intake is associated with a 6% rise in overall cancer mortality and significantly higher risks of ovarian and breast cancer deaths (Chang et al., Reference Chang, Gunter, Rauber, Levy, Huybrechts, Kliemann, Millett and Vamos2023). Thus, food insecurity is not only about insufficient calories but also about compromised nutritional quality with long-term health consequences, reinforcing the need to examine how food aid structures shape dietary behaviours.
Structural drivers of FI in the UK are well-documented. Socioeconomic status, education instability, and welfare reliance are all associated with reduced food access (Tingay et al., Reference Tingay, Tan, Tan, Tang, Teoh, Wong and Gulliford2003; Pilgrim et al., Reference Pilgrim, Barker and Jackson2012; Power et al., Reference Power, Doherty, Small, Teasdale and Pickett2018; Loopstra et al., Reference Loopstra, Reeves and Tarasuk2019). However, much of this evidence comes from large-scale surveys or administrative datasets, which lack depth and overlook lived experiences (Garthwaite et al., Reference Garthwaite, Collins and Bambra2015). While these approaches are valuable for estimating prevalence and trends, they often fail to capture the emotional, relational, and practical consequences of food insecurity, including stigma, anxiety, coping strategies, and compromised dietary quality. Marginalised groups are often under-represented, as they may avoid formal data collection due to stigma, language barriers, and mistrust of institutions (Purdam et al., Reference Purdam, Garratt and Esmail2016). This under-representation risks producing an incomplete picture of FI, obscuring the experiences of those most affected, and may contribute to policy responses that prioritise short-term crisis management over structural solutions that address dignity, access, and long-term nutritional adequacy. Consequently, understanding how individuals experience and navigate FI within their everyday social and community contexts is essential for designing meaningful public health and policy interventions.
UK research tends to focus heavily on users of Trussell Trust food banks, referral-based models that prioritise crisis intervention. While valuable, this creates a narrow understanding of FI (Garthwaite et al., Reference Garthwaite, Collins and Bambra2015; Purdam et al., Reference Purdam, Garratt and Esmail2016 and Thompson et al., Reference Thompson, Smith and Cummins2016, Reference Thompson, Smith and Cummins2018), as informal food aid remains understudied despite being more flexible and accessible. As a result, individuals relying on informal or non-referral-based food support may remain uncounted despite advances in national monitoring and their experiences excluded from research and policy (Caraher and Davison, Reference Caraher and Davison2019; Pool and Dooris, Reference Pool and Dooris2022).
While food insecurity is now measured in the UK through the Family Resources Survey, using the USDA Household Food Security Survey Module (HFSSM), which is validated for use in high-income countries, this approach still has important limitations. In particular, its reliance on self-reported data may lead to underestimation of food insecurity due to stigma, shame, and reluctance to disclose need.
Measurement inconsistencies further complicate the FI evidence base. Although widely defined as unreliable access to sufficient, safe, and nutritious food, FI lacks a single internationally agreed operational definition or standardised measurement framework, and the UK has historically lacked a government-endorsed metric, limiting effective monitoring and intervention (Lambie-Mumford and Dowler, Reference Lambie-Mumford and Dowler2015). Despite calls for wider adoption of the Food Insecurity Experience Scale (FIES), a proposed global standard for monitoring hunger, to support data harmonisation (Food Foundation, Sustain and Oxford University, 2016), uptake remains limited. Such that inconsistent methodologies in sampling, timing, and terminology hamper comparison across studies and slow development of a cohesive national evidence base (Pool and Dooris, Reference Pool and Dooris2022).
The psychological toll of food insecurity, including anxiety, shame, and loss of autonomy, has been well documented in UK qualitative research (Garthwaite et al., Reference Garthwaite, Collins and Bambra2015; Purdam et al., Reference Purdam, Garratt and Esmail2016; Power et al., Reference Power, Doherty, Small, Teasdale and Pickett2018; May, Reference May2020; Loh et al., Reference Loh, Knight and Loopstra2021). However, despite this substantial evidence base, limited structural progress has been made in addressing these harms, with policy responses continuing to prioritise short-term crisis relief over upstream prevention (Lambie Mumford and Dowler, Reference Lambie-Mumford and Dowler2015; Loopstra et al., Reference Loopstra, Reeves and Tarasuk2019). The highly context-specific and relational nature of food insecurity may partly explain why qualitative insights have not consistently translated into systemic reform. In addition, whilst qualitative work has explored foodbank user experience (Garthwaite et al., Reference Garthwaite, Collins and Bambra2015; Stone and Papadaki, Reference Stone and Papadaki2025), the perspectives of those who volunteer at food banks are rarely included. As frontline observers of both emotional and material hardship, they could offer essential insight into how FI is navigated in community contexts.
This study explored how structural FI affects dietary behaviours and lived experience among users and volunteers in UK community food support services.
Methods
The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist was used to guide the reporting of this study, to ensure transparency and rigour in the design, conduct, and analysis of qualitative data (Tong et al., Reference Tong, Sainsbury and Craig2007).
Study design
A hermeneutic phenomenological approach was adopted to explore the lived experiences of individuals who use or have used food banks and volunteers working within formal and informal food aid settings in the UK. Phenomenology, grounded in Husserl (Reference Husserl1997) philosophical traditions, seeks to understand human experience as perceived, free from theoretical assumptions. Van Manen (Reference van Manen2016) hermeneutic strand emphasises interpretation, embodiment, and context-specific meaning. This approach addresses gaps in existing literature, where FI is often examined through national surveys of secondary data that overlook lived experiences (Purdam et al., Reference Purdam, Garratt and Esmail2016; Power et al., Reference Power, Doherty, Small, Teasdale and Pickett2018). A hermeneutic phenomenological approach enables a rich, interpretive exploration of how users and volunteers perceive and embody FI, including stress, stigma, and health challenges associated with constrained food access. It supports a holistic understanding of how food-related behaviours are shaped by broader economic, social, and emotional conditions (Daland and Hidle, Reference Daland and Hidle2016).
To further this understanding, the socio-ecological model (SEM) (Bronfenbrenner, Reference Bronfenbrenner1977) was applied during analysis. SEM’s multi-level framework, spanning individual, interpersonal, institutional, community, and policy domains (Sallis et al., Reference Sallis, Owen, Fisher, Glanz, Rimer and Viswanath2008; Kilanowski, Reference Kilanowski2017), enables deeper exploration of how personal experiences reflect structural conditions and systemic injustice (Townsend and Foster, Reference Townsend and Foster2011).
Participant recruitment and sampling
Purposive sampling included users and volunteers from both formal and informal food aid settings, with a focus on non-referral, community-led services to capture under-documented experiences (Sedgwick, Reference Sedgwick2013).
Nineteen participants were recruited: nine food bank users and ten volunteers. The final sample size was guided by principles of data saturation and information power rather than a predetermined numerical target. Recruitment continued until no substantially new themes or insights were emerging across interviews and sufficient depth had been achieved to address the study aims. The focused research question, inclusion of two analytically relevant participant groups, and use of in-depth semi-structured interviews contributed to high information power, supporting the adequacy of the sample size.
Recruitment occurred via personal and professional networks, including associates of the researcher and individuals identified through LinkedIn profiles that indicated volunteer or professional roles in food banks. Additional participants were approached in person at food banks with support from on-site volunteers. Food banks also distributed study information sheets detailing the research purpose, key topics, and ethical considerations.
Three users declined to participate, without providing reasons. The researcher had prior relationships with four participants (one volunteer and three users), while other participants were previously unknown.
Inclusion criteria were established to ensure relevance to the study’s aims and consistency across participants. Individuals were eligible to take part if they met the following inclusion criteria:
-
• Aged 18 or over
-
• Proficient in English to ensure effective participation in interviews
-
• Experience of using food banks (primary or supplementary food source) or past/current volunteer experience at food banks
Participation was voluntary and unpaid. Participants were informed of their right to withdraw at any time.
Data collection
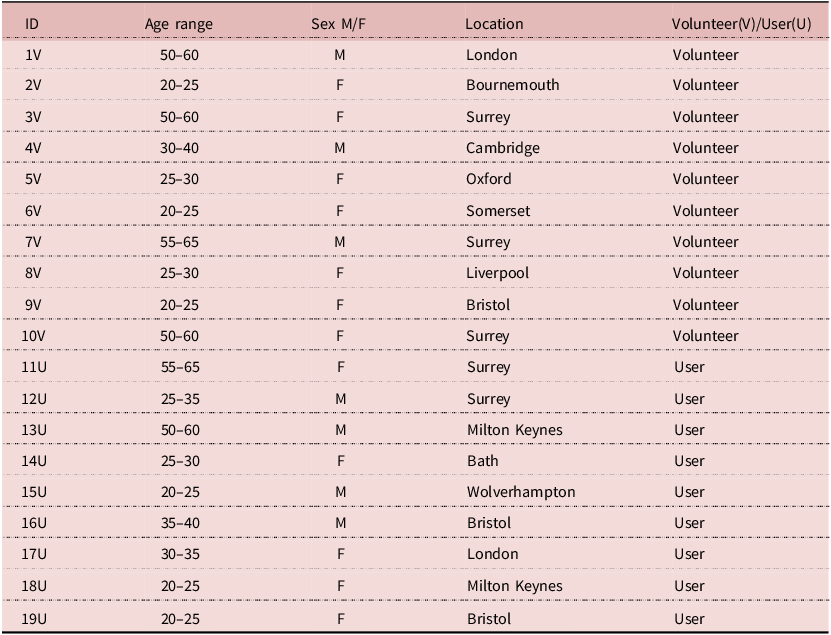
Demographic information was collected by the interviewer after obtaining consent but before the interview began. Participants indicated their age by selecting from provided ranges and self-identified their sex. Location refers to the food bank where the volunteer worked or the user accessed services.
Semi-structured one-to-one interviews were conducted in person at food banks or via WhatsApp video call, depending on participant preference. Interviews lasted 20–55 minutes. Video calls were held in private settings; in-person interviews took place in quiet or semi-quiet food bank areas. Care was taken to ensure privacy and minimise disruptions. Whilst users were being interviewed, volunteers were nearby for safeguarding but not within earshot.
Interviews followed Manen’s (Reference van Manen2016) hermeneutic phenomenological method, using a conversational open-ended style. The core guide was adapted from Puddephatt et al. (Reference Puddephatt, Keenan, Fielden and Reaves2020) in order to explore broader contexts such as hardship, coping strategies, health, and the meaning of food bank support. Prompts and targeted questions were used as needed. Printed question guides supported communication during in-person interviews (Phellas et al., Reference Phellas, Bloch, Seale and Seale2011) (Supplementary File 1).
All interviews were audio-recorded and transcribed verbatim by the researcher. The researcher had prior relationships with a small number of participants, which may have shaped interview dynamics and interpretation. The researcher had academic and voluntary experience related to community food access but was not a food bank user and acknowledged their relative privilege and its potential influence on rapport and meaning-making. Reflexive journalling was maintained throughout data collection and analysis, and regular supervision supported critical reflection on positionality, assumptions, and power dynamics.
Data analysis
Data were analysed using reflexive thematic analysis (TA), following Braun and Clarke’s (Reference Braun and Clarke2006, Reference Braun and Clarke2020) six-step framework. This approach aligned with hermeneutic inquiry, emphasising meaning-making, reflectivity, and depth (Smith et al., Reference Smith, Flowers and Larkin2009). NVivo 12 supported data management and coding (Woods et al., Reference Woods, Paulus, Atkins and Macklin2015).
An inductive approach guided initial analysis. The lead researcher read each transcript and recorded reflexive notes. Reflexive engagement with the data was maintained throughout coding and theme development, recognising the researcher’s active role in interpretation. Based on initial observations, a codebook was developed and refined through interactive reading (‘hermeneutic circle’) (Crist and Tanner, Reference Crist and Tanner2003). Codes were compared across interviews for convergency and divergency.
Following this, codes were consolidated into conceptual themes. A deductive phase followed, mapping content into SEM’s levels to highlight influences on FI. This included integration of key theoretical concepts such as food literacy, financial precarity, and stigma (Schreier, Reference Schreier2012; Adeoye-Olatunde and Olenik, Reference Adeoye-Olatunde and Olenik2021). To enhance validity, a second researcher reviewed the final coding framework, supporting interpretive credibility through peer scrutiny (Crist and Tanner, Reference Crist and Tanner2003). Transcription validation was considered, but member checking was unfeasible due to population mobility (Davies, Reference Davies2021).
Ethical approval was obtained by the School for Policy Studies Research Ethics Committee (approval code 24487), and all participants provided written informed consent.
Results
Sample demographics
The study included 19 participants from 11 locations across England, comprising 9 food bank users and 10 volunteers (Table 1). Participants were diverse in age, ranging from early 20s to mid-60s, and included 11 women and 8 men. Most participants were from non-referral, community-led food aid, reflecting the study’s focus on informal support settings, although data were also collected from formal food bank settings.
Participant information
Five key themes were identified and mapped onto the SEM (Bronfenbrenner, Reference Bronfenbrenner1977) (Figure 1), illustrating the complex, multi-level drivers of FI (Sallis et al., Reference Sallis, Owen, Fisher, Glanz, Rimer and Viswanath2008). At the individual level, poor mental health, stigma, and shame shaped food-related behaviours. At the interpersonal level, caregiving roles and emotional responsibilities often led individuals to make personal sacrifices. At the institutional level, participants described long-term reliance on food aid, limited nutritional quality, and barriers to cooking due to inadequate kitchen facilities. At the community level, informal networks offered nutritional foods absent in most formal services. At the public policy level, inadequate welfare and political neglect were cited as root drivers of FI. These findings reinforce the SEM’s utility in addressing FI through integrated, multi-level responses (Kilanowski, Reference Kilanowski2017).
Key themes of food insecurity in the UK mapped onto the socioecological model.

Theme 1: individual
The interconnection between mental health and FI
Poor mental health associated with FI was highlighted by 17 participants who described FI as both a cause and a consequence of mental health challenges. Anxiety, depression, trauma, and shame were central to their experiences, frequently exacerbated by unemployment, isolation, and the stigma of seeking help.
Poor mental health was linked to an impaired ability to work, deepening financial instability, and reliance on aid.
‘For the single adults who might have real mental health issues… that’s having a knock-on impact on their ability to get a job and work, which then obviously impacts their ability to have an income.’ – 5V
Volunteers (n = 6) repeatedly identified emotional distress as a core driver of food bank use, often preceding financial hardship:
‘Mental health is a massive one… and then with that comes a spiral of involvement in drugs and crime.’ – 3V
Social anxiety and stigma further limited access to support, as described by 12 participants. For some, the anticipation of judgement and the emotional burden of being ‘seen’ in need shaped everyday decision-making, leading to self-exclusion from both formal and informal support and intensifying isolation. With participants reporting that they avoided public spaces and delayed help-seeking due to fear of judgement or being recognised.
‘I’ve met numerous people… they’ve got into such a state of despair, that for them, leaving their house to go to the local corner shop… is hell on earth.’ – 1V
Ongoing stress was cited by 7 users, who associated this with uncertainty around food access, financial instability, and the emotional toll of repeatedly navigating food shortages.
‘I feel stressed with food a lot of the time because it’s never certain we will have enough’ – 14U
Shame and stigma as psychological barriers to accessing food
Shame was described as a persistent emotional burden associated with food bank use, as reflected in accounts from 18 participants (11 users and 7 volunteers). Many conveyed feelings of personal failure and a loss of dignity, which often endured with continued reliance on support.
‘There’s a constant weight of shame… it felt like I’d lost a part of myself’ – 16U
Stigma particularly affected caregivers, with several users questioning their entitlement to support and expressing feelings of guilt, perceived failure, or concern about being judged.
‘There’s a big stigma around it… everyone thinks we are greedy’ – 19U
Concerns about stigma discouraging attendance, particularly among older and socially isolated individuals, were echoed by five volunteers. Several noted users’ tendency to justify their presence.
‘People feel the need to explain themselves as to why they’re there’ – 2V
One volunteer also highlighted the direct consequences of this stigma, noting how individuals avoid seeking help due to feelings of shame.
‘I know a lot of people who actually go hungry as a direct result… of them just feeling too shy and embarrassed to go out’ – 1V
Although one food bank user pointed to the welcoming atmosphere of the food bank as mitigating shame.
‘You can tell they [Volunteers] just want to help’ – 13U
Theme 2: interpersonal
Caregiving responsibilities and the emotional burden of providing food
Caregiving emerged as a deeply gendered and emotionally charged experience, with at least 8 women (5 users, 3 volunteers) and 3 men (2 users, 1 volunteer) describing food provision for dependents as a core moral responsibility. These accounts spanned biological parents, adoptive carers, grandparents, and couples acting as joint providers.
Feeding others was described by 11 participants (7 users, 4 volunteers) as a moral and emotional duty, particularly within maternal and grandparent roles. Sacrificing food for dependents, especially children, was seen as routine.
‘Single mothers… get into a bad habit of skipping breakfast and skipping lunch and then like, before you know it, they’ve not eaten for three days just so that their kids can have food’ – 8V
Shielding children from financial stress or hunger was a common concern raised by 7 participants (5 users and 2 volunteers).
‘We try not to let the kids know we are struggling’ – 13U
‘My dad would… say he’d eaten dinner later but… he probably didn’t eat some nights’ – 18U
Grandparents also played central caregiving roles. One food bank user described giving up employment to care for grandchildren.
‘I had to give my job up because I’ve got custody of my three grandchildren’ – 11U
Food choices noted by 7 participants prioritised affordability and children’s comfort over nutritional value.
‘Nutrition comes second to bulk and price’ – 16U
Theme 3: institutional
The shift from emergency relief to sustained dependency on food aid
For many participants, food bank use had transitioned from an emergency response to an ongoing necessity (12 participants; 6 users and 6 volunteers).
‘Now it’s part of our weekly routine’ – 16U
Volunteers observed this shift too, likening food banks to A&E departments, appropriate for crises, not ongoing needs.
‘Emergency need has transformed into an ongoing chronic need… people come in month on month, if not week on week.’ - 4V
Participants (5 volunteers, 1 user) linked this trend to inflation and the aftermath of COVID-19.
‘Most people came out of work post-COVID… now realise they need it’ – 3V
Concerns about the sustainability of the food bank role were also voiced, particularly regarding their capacity to meet long-term needs rather than short-term crises. Participants questioned whether food banks, originally intended as emergency interventions, were becoming normalised as a substitute for adequate welfare provision.
‘Food banks are a sticking plaster, not a fix.’ – 16U
This framing reflected a broader unease about the institutionalisation of charitable food aid and its potential to displace state responsibility, reinforcing dependency rather than addressing structural drivers of food insecurity.
Nutritional limitations and quality concerns in food parcel provision
Concerns about the nutritional adequacy and quality of food aid were raised by 17 participants (11 users, 6 volunteers). Parcels typically comprised ambient, long-life items such as tinned goods and pasta, with limited fresh produce. Users felt their diets were nutritionally poor not by choice but necessity.
‘When your money’s run out, nutrition takes a back seat’ – 16U
Volunteers confirmed that ultra-processed foods (UPFs) were often more accessible than nutritionally balanced alternatives, both within food parcels and in wider retail environments. This was linked to affordability, longer shelf life, and donation patterns that prioritised non-perishable goods. As a result, participants described constrained dietary choices shaped not solely by preference but by structural limitations embedded within both charitable provision and the broader food system.
‘Ultra-processed food is cheaper per calorie’ – 8V
‘If someone’s on a low income… they would have to spend a huge portion of that to eat a nutritious diet.’ – 4V
Several participants (6 users and 1 volunteer) also noted the poor condition of some donations, describing them as expired, damaged, or low quality.
‘I’ve thrown food away because it was expired or damaged’ –16U
Practical constraints in food preparation and meal planning
Barriers to effectively using food parcels, including inadequate cooking facilities and rising energy costs, were mentioned by 16 participants (9 users and 7 volunteers).
‘I have nothing in my kitchen, so I can’t cook anything.’ – 13U
‘Not having an oven or a hob… how can we accommodate that?’ – 5V
Unpredictable donations further complicated meal planning.
‘You can’t plan proper meals when you don’t know what you’re going to get’ – 16U
Many users reported relying on cheap, filling food rather than meals that reflected nutritional or cultural preferences.
‘It’s about survival, not choice or preferences’ – 15U
Theme 4: community
The role of informal networks in enhancing food access
The importance of local networks, social supermarkets, school meal initiatives, and community food hubs was emphasised by 18 participants (10 volunteers and 8 users).
‘It’s a lifeline. I still get parcels now and again but now we’re doing okay… now it is somewhere to come for a cup of tea and a chat.’ –19U
Participants emphasised that much of the higher-quality or fresh food accessed by food bank users came through informal networks, including local farms, bakeries, surplus redistribution schemes, and community members sharing resources via social media or word of mouth. Unlike traditional referral-based food banks, which distribute pre-packed emergency parcels composed largely of non-perishable goods, these informal channels often operated outside formal voucher systems and provided more flexible, relationship-based access to food. In some cases, they supplemented formal food parcels by adding fresh produce or culturally preferred items; in others, they functioned independently as community-led alternatives to the conventional emergency food bank model.
‘to get good stuff to your food banks close contacts and networking goes a long way to bring fresh things in’ – 10V
Theme 5: public policy
Socioeconomic and political drivers of FI
Structural issues such as precarious employment, low wages, and inadequate welfare were identified as main drivers of FI by 19 participants (9 users and 10 volunteers). In addition, rising food prices were repeatedly described as exacerbating household financial strain, with participants highlighting the increasing cost of staple and budget foods as a key contributor to food insecurity.
‘I think they [government] should put a cap on the prices… it’s horrendous… Spam used to cost 90p, now it’s like four quid.’ – 11U.
Unstable work was described as a barrier to long-term planning by 9 users.
‘I’ve got to wait another month to get paid… I come here once a month when things get tight’- 12U
Welfare support was criticised as insufficient, particularly for disabled people and carers by 13 participants.
‘I’m on disability benefits now, but it’s barely enough to cover rent, bills, and essentials.’ – 17U
Trade-offs between food, heating, rent, and debt were reported by 11 participants.
‘Do people eat or do they heat their homes?’ – 1V
Political neglect and the limits of charity
Concern that food banks mask systemic failure by successive UK governments and the broader welfare system was expressed by 14 participants (9 volunteers and 5 users). While valued, they were seen as a stopgap, filling the void left by a retreating welfare state.
‘The government moan about food insecurity, but they’re not doing anything.’ – 2V
Users reported feeling excluded from policymaking, describing a lack of meaningful engagement with people experiencing food insecurity and a perception that their lived realities were not reflected in political decision-making. Several participants expressed frustration that policies affecting welfare and food access were developed without consultation with those directly impacted.
‘Politicians just don’t want to know… it’s up to charities to help us.’ – 13U
Volunteers frequently criticised the government’s reliance on charities, advocating for a legal right to food and stronger welfare support.
‘We’re campaigning for policy change so benefits cover essentials.’ – 4V
Discussion
This study examines how structural factors shape food choices among individuals experiencing FI, focusing on users and volunteers in both formal and informal food aid settings in the UK, particularly non-referral community-led services. Thematic analysis showed that food-related behaviours are influenced not only by material deprivation but also by psychological, social, and policy-related forces. These findings align with Bronfenbrenner’s (Reference Bronfenbrenner1977) SEM, affirming FI as a multidimensional issue best understood through a multilevel lens (Sallis et al., Reference Sallis, Owen, Fisher, Glanz, Rimer and Viswanath2008; Kilanowski, Reference Kilanowski2017).
However, beyond this alignment, this study makes a methodological contribution through the deductive application of the SEM to lived experience data. While the SEM is frequently cited in public health research, it is less commonly operationalised to structure qualitative findings on food insecurity across user and volunteer perspectives simultaneously. By mapping themes across individual, interpersonal, institutional, community, and policy domains, this study demonstrates how qualitative insights can be systematically translated into multi-level intervention targets.
At the individual level, participants described mental health struggles, stigma, and shame as both causes and consequences of FI. This echoes studies on the emotional burden of food poverty, especially among marginalised and low-income groups (Booth and Smith, Reference Booth and Smith2001; Garthwaite et al., Reference Garthwaite, Collins and Bambra2015; Spinosa et al., Reference Spinosa, Christianson and Metz2019).
The present study highlights a bidirectional link between FI and mental health, showing how anxiety and fear of judgement can lead to self-exclusion from food aid, a less explored factor in existing literature (Power et al., Reference Power, Doherty, Small, Teasdale and Pickett2018; Stone and Papadaki, Reference Stone and Papadaki2025).
Interpersonally, caregiving roles shaped food choices. Many users prioritised feeding children or grandchildren over their own nutritional needs. This supports findings on the gendered burden of FI (DeMarco and Thorburn, Reference DeMarco and Thorburn2009; Pilgrim et al., Reference Pilgrim, Barker and Jackson2012) and highlights the pressures of kinship carers. Thompson et al. (Reference Thompson, Smith and Cummins2016) also reported that parents shield children from hunger. This study further shows that, although caregiving responsibility was shared, it was described more frequently by women, pointing to a potential gendered imbalance in how emotional and nutritional sacrifices are experienced within households.
At the institutional level, participants criticised the inadequacy and unsustainability of food aid. Echoing Caraher and Davison (Reference Caraher and Davison2019) and Loopstra et al. (Reference Loopstra, Reeves and Tarasuk2019), they noted a shift from short-term help to long-term dependence. Volunteers saw themselves filling welfare gaps, aligning with Garthwaite et al. (Reference Garthwaite, Collins and Bambra2015) framing of food banks as ‘emergency infrastructure’. This study adds that limitations such as poor-quality donations, unpredictable supply, and lack of cooking facilities reduce the nutritional value and usability of aid. These issues support critiques that England’s food aid relies too heavily on UPFs, worsening diet-related health risks (Morales and Berkowitz, Reference Morales and Berkowitz2016; Hardcastle and Caraher, Reference Hardcastle and Caraher2021; Henney et al., Reference Henney, Taylor and Boon2024).
Community-level initiatives such as social supermarkets, local farms, and peer networks were valued for their dignified, consistent quality, and stronger support compared to traditional food banks. While Pool and Dooris (Reference Pool and Dooris2022) call for more research on these spaces, this study uniquely highlights how volunteers shape and navigate these systems through community relationships. This participatory dimension is rarely addressed and has implications for more inclusive policy design.
At the policy level, these findings reinforce critiques that link FI to austerity, wage stagnation, and weak social protection, consistent with the work of Lambie-Mumford and Dowler (Reference Lambie-Mumford and Dowler2015) and Power et al. (Reference Power, Doherty, Small, Teasdale and Pickett2018). Participants cited low income, precarious employment, and inadequate welfare as key drivers of FI. Many voiced a deep sense of abandonment, viewing food aid as a last resort amid government inaction, supporting May’s (Reference May2020) call to frame FI as a symptom of broader precarity, not individual failure.
Overall, the findings align with existing UK literature on FI regarding stigma, structural causes of hunger, and the limitations of food banks. Yet, this study extends that literature in three important ways.
First, while stigma is well documented, few studies examine how it intersects with mental health to drive self-exclusion from food aid. This study shows that anxiety, social withdrawal, and anticipatory shame do not merely accompany FI but actively shape access pathways, potentially contributing to underestimation in prevalence data and reinforcing hidden hunger (Stone and Papadaki, Reference Stone and Papadaki2025).
Second, users’ food choices were shaped not just by cost but by emotional comfort, especially when feeding dependents. The preference for ‘bulk and familiarity’ over nutrition reveals that coping strategies are emotionally and relationally driven. This builds on existing work on parental buffering (Thompson et al., Reference Thompson, Smith and Cummins2016) by demonstrating how emotional labour and moral responsibility operate as mediating mechanisms between structural poverty and dietary compromise.
Third, this study incorporates volunteers’ perspectives as analytical contributors rather than background informants. Their accounts illuminate how charitable systems function relationally, revealing both the emotional labour required to preserve dignity and the structural tensions inherent in operating ‘sticking plaster’ services. This dual perspective strengthens understanding of how food aid systems are sustained, normalised, and contested at the community level.
Taken together, these findings add empirical depth to critiques of the charitable food aid model, which argue that reliance on emergency provision can normalise food insecurity and displace responsibility away from the state (Lambie-Mumford and Dowler, Reference Lambie-Mumford and Dowler2015; Lambie-Mumford, Reference Lambie-Mumford2018; Power et al., Reference Power, Doherty, Small, Teasdale and Pickett2018). Importantly, the deductive application of the SEM also strengthens the intervention relevance of this study by identifying entry points across levels: reducing stigma and mental health barriers to access (individual/interpersonal), improving the nutritional quality and usability of provision through cooking facilities and more consistent donations (institutional), strengthening non-referral community-led models that promote dignity and belonging (community), and advocating welfare adequacy and rights-based policy approaches (policy).
The findings highlight the need for a shift in both policy and practice to address the structural causes of FI and reduce reliance on charitable food aid. Echoing Lambie-Mumford (Reference Lambie-Mumford2018) and The Food Foundation (2024), several participants advocated a legal framework ensuring food access as a human right. While charitable food aid offers vital short-term relief, growing reliance on it raises concerns about the adequacy of state welfare. Alongside strengthened state support, a move towards sustainable, dignity-based models is essential. Government investment in not-for-profit initiatives, such as social supermarkets, food hubs, and community kitchens, can enhance both nutritional value and relational support. Improving the quality of food parcels requires better coordination between producers, donors and distributors. Local partnerships with farms, bakeries, and surplus platforms could increase freshness and variety. Volunteers are central to informal food aid yet often lack support. Providing training, supervision, and recognition could improve both service quality and volunteer wellbeing.
This study’s primary strength lies in its rich, interpretive approach, underpinned by hermeneutic phenomenology and the application of the SEM (Bronfenbrenner, Reference Bronfenbrenner1977). It provides deep insights into the lived experiences of individuals often excluded from survey-based research and triangulates findings across users and volunteers. Reflexive TA further supports the credibility of the interpretations presented.
However, limitations must be acknowledged. Although the sample was diverse in age and geography, it under-represents some ethnic groups and may not reflect the experiences of non-English speakers or those in rural or remote areas. Excluding individuals who were not proficient in English may also have introduced selection bias, as language barriers can deter participation in research and reduce engagement with formal services, contributing to the under-representation of some migrant and minority ethnic groups (Purdam et al., Reference Purdam, Garratt and Esmail2016). This criterion may therefore have skewed the sample towards people who are more able to navigate UK institutions and referral pathways, potentially overstating reliance on food banks and understating the role of informal support. Evidence from multiethnic settings suggests that experiences of food insecurity and help-seeking can be culturally mediated, with some communities drawing more heavily on family or community food sharing and reciprocal support, which may reduce visibility within food bank-based samples (Power et al., Reference Power, Doherty, Small, Teasdale and Pickett2018). Future research should consider using interpreters or multilingual recruitment to better capture these experiences and assess how linguistic and cultural factors shape pathways into formal and informal food aid (Purdam et al., Reference Purdam, Garratt and Esmail2016; Power et al., Reference Power, Doherty, Small, Teasdale and Pickett2018).
Participation was voluntary, so individuals facing acute stigma, poor mental health, or social isolation may have not participated, potentially leading to underestimation of these issues. Member checking was unfeasible due to population mobility. Although the sample of nineteen participants may appear modest when divided into users (n = 9) and volunteers (n = 10), the study was grounded in hermeneutic phenomenology, which prioritises depth of lived experience over numerical breadth. In phenomenological research, sample adequacy is determined by interpretive depth and information power rather than participant numbers. The focused research question, inclusion of two analytically distinct groups, and use of in-depth, conversational interviews generated high information power, supporting the adequacy of the sample. The recurrence of key themes across users and volunteers further strengthens interpretive credibility. Volunteers offered valuable insights and helped build a broader understanding of food aid dynamics. Although some of their accounts reflected second-hand perceptions rather than direct foodbank user experience, which may have introduced bias, these were not treated as proxies for user experience but as complementary perspectives that illuminated the relational and institutional mediation of food insecurity. Finally, prior relationships between the main researcher and a few participants may have influenced responses; however, reflexivity and peer review were maintained throughout the study to help mitigate bias.
Conclusion
Findings from this study reaffirm that charity-based food aid, while essential in the short term, is not a sufficient or sustainable solution to FI. They highlight the need for systemic policy change, including a legal right to food, more inclusive welfare provision, and investment in dignity-based, community-responsive food systems. Future research should include more diverse linguistic and cultural communities, examine rural FI, and evaluate scalable models that preserve autonomy and nutritional adequacy.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0021932026100583.
Funding statement
No funding was received for this research.
Competing interests
The authors declare no conflicts of interest.
Ethical standard
This study was conducted in full accordance with the ethical principles set out in the World Medical Association Declaration of Helsinki (1975, revised 2008) and complied with all additional requirements of the United Kingdom, where the research was carried out. Ethical approval for the research was obtained from the University of Bristol School for Policy Studies Research Ethics Committee (reference number: 24487). All participants provided free and informed consent prior to participation.





 Open access
Open access