


In the fight against the two-headed dragon that surfaced from musings of the mind, the one champion that has reigned supreme for more than half a century is lithium. Surviving precariously from one decade to the next, this humble, silvery white element continues to demonstrate its silverback status amongst the burgeoning pharmacological armamentarium that is presently used to ‘treat’ bipolar disorder. Numerous combatants belonging to the armies of antidepressants and anticonvulsants, flanked by their armigers brandishing pharmaceutical coats of arms, have successively thrown down the gauntlet to lithium, resulting in interregna marked by its displacement from prescription use. However, on each occasion, the shining knight, true to its mettle, has risen to the challenge and managed to reclaim its succession to the throne.
– The king is dead, long live the king!
– Malhi, 2010 Reference Malhi1
Although lithium dutifully stands tall in international practice guidelines, its real-world clinical utility – not to mention its once-lauded standing in academic circles – seems to be increasingly dismissed. As caring and compassionate clinicians and astute researchers committed to helping those with severe mental illness (SMI) such as bipolar disorder, readers of this journal would accept lithium’s shrinking popularity if, and only if, newer insights and novel interventions were proven to exceed the benefits that lithium therapy presently provides. Indeed, novel interventions that convincingly improve upon both lithium’s efficacy and tolerability in patients with bipolar disorder would likely receive a ‘royal reception’ and perhaps supplant lithium in future practice guidelines. Alas, to date, no such advance is on the horizon or even seems likely given the paucity of evidence from contemporary research.
The use of lithium is diminishing and under threat and its under-utilisation is puzzling given that decades of study demonstrate that lithium therapy provides enormous benefits when utilised with sound judgement. Few would question the effects of lithium in active mania, which it quells in a matter of days, and thereafter maintains mood stability in the long-term. This latter distinction – of being able to offer a lifetime of prophylactic protection from the ravages of bipolar illness, and thereby dramatically improving the prognosis of ‘lithium responders’ – constitutes lithium as offering more than temporary and symptomatic relief, and rather being a true disease-modifying agent. Reference Post, Li, Berk and Yatham2
Years after John Cade’s work, Mogens Schou found it ‘rather astonishing that (lithium’s therapeutic effect) has failed to arouse greater general interest among psychiatrists’. Reference Schou, Juel-Nielsen, Stromgren and Voldby3 We are equally astounded, and hence we feel compelled to ask why lithium therapy lacks currency. After all, it has been over 75 years since John Cade re-introduced lithium.
The current reluctance to make use of lithium is all the more disconcerting given it is readily available, cost-effective and can even lay claim to being naturally-occurring – a label that has additional appeal nowadays. However, its affordability perhaps means it is not an attractive molecule for the pharmaceutical industry because of limited profitability. Consequently, lithium’s elemental status and therefore lack of commercial backing is perhaps to be expected, and to this end, one of the reasons why lithium’s comparative efficacy and safety is unclear in the minds of physicians. Add to this, lithium’s lack of 21st-century sheen, and ongoing mystery as to its mechanism of action, and these factors perhaps explain why its critical role in the treatment of those with SMI is often not acknowledged. Hence, its regal status as the ‘gold-standard mood stabiliser’ is once again at risk of being mischaracterised as archaic, based on a reputation that is a vestige of the past. A revival of lithium is warranted, and, to fuel this, we offer a distillation of its empirical properties.
Is lithium’s efficacy merely historical?
Following Baastrup and Schou’s landmark double-blind discontinuation trial in 1970, lithium’s therapeutic and prophylactic efficacy in comparison with placebo was assured, and the element was heralded as the first psychotropic agent which could demonstrate clear and long-term benefits for patients with mood disorders. However, later in the 20th century, and during the heyday of pharmaceutical company influence, lithium faced competition from multiple classes of agents with a diversity of actions, ranging from chlorpromazine to imipramine and the repurposed antiepileptic drugs (AEDs) such as valproate. Since the introduction of these agents, sold with the promise of being easier to prescribe without requiring regular monitoring, seismic shifts in prescription numbers over decades and across the globe have favoured valproate over lithium, 4 with only recent (and localised) regulatory action going some way to curbing valproate use. Nevertheless, popularity trends must confront the reality of efficacy: the BALANCE trial demonstrated clearly that in maintenance treatment, relative to valproate, it is lithium that provides the lion’s share of prophylaxis either alone or in combination. 4 Further, this is not only a statistically significant difference but one that is clinically meaningful in arguably the most important arena – the prevention of relapse – where patients must defend against the incursions of the illness on a daily basis.
In a parallel mêlée, recent decades have seen second-generation antipsychotics (SGAs) such as quetiapine, risperidone, and olanzapine overtake lithium in the minds of clinicians, no doubt enhanced by the promotion of multinational pharmaceutical corporations. These compounds are commonly offered both as treatment for acute mania and continued for ‘maintenance’ treatment of bipolar disorder; notably, not mood stabilisation. Unfortunately, patients who suffer from these conditions are at a significantly greater risk of relapse than those on lithium monotherapy. Reference Wingård, Brandt, Bodén, Kieler, Andersen and Reutfors5 Any significant increase in a patient’s likelihood of achieving and maintaining an illness-free period ought to be considered analogous to achieving remission from bipolar disorder – a goal that lithium achieves more consistently and with greater efficacy than any other single agent.
However, lithium’s commanding advantages may already be lost to the march of time, as psychiatric practice continues to prioritise novelty over nuance. Prescriber comfort with newer alternative agents, despite significant limitations in the efficacy of these agents in the various phases of bipolar illness, and their detrimental impact upon patient morbidity and mortality, is difficult to reverse with papers and books alone. The clinical wisdom shared during psychiatry training, and residency programmes, is declining in line with lithium’s prescription rates and prescriber confidence. The novelty and intense marketing of patented agents continues to divert clinician interest towards these newer and more profitable drugs, seen by some as more effective, easier to prescribe, less cumbersome to manage and more acceptable to patients. Following the Golden Age of psychopharmacology, efforts in the latter decades of the 20th century to improve upon the efficacy of older agents, including lithium, have clearly been unsuccessful, and a broad focus on tolerability continues to undermine the stringent evidence of lithium’s effectiveness.
Moreover, the broadening of diagnostic criteria in psychiatry, and the lack of diagnostic (and therefore treatment) specificity inherent to intervention trials, does not favour lithium. Lithium has profound effects upon those with ‘classic’ bipolar disorder (or Cade’s disease) – namely, those tending to present with clearly recognised (and recurrent) episodes of illness and equally clear episodes of remission, and with a positive family history of both bipolar disorder and lithium response. This group of lithium responders may make up one-third of patients with bipolar disorder. In the absence of a clear biomarker to aid in the designation of lithium responder status a priori, clinical recognition of this profile, and the astute promotion of lithium treatment in the prioritisation of management of these patients, would likely have significant ramifications upon the recovery of this cohort, some to the degree of living in bipolar remission, potentially for decades. This degree of sustained recovery from severe illness is unfortunately rare in psychiatry; however, comparator trials, and increasingly clinicians, utilise broad diagnostic categories to group patient populations and measure intervention effects, with the end result being that lithium’s most impressive effects are diluted in comparison to the broad spectrum actions of competing agents such as SGAs.
Safety concerns – passé and passed over?
Some 75 years since Noack and Trautner established methods and parameters for the safe and therapeutic use of lithium, clinician and patient anxiety alike remain at least partly responsible for the low levels of lithium initiation over much of the last century, even prior to the arrival of newer dopaminergic agents and valproate. Here, the rationale for choosing these alternative agents is likely related to concerns about safety. Critically, the adverse effect profile of valproate and SGAs, including the propensity of both types of treatments to significantly increase the incidence and burden of cardiovascular risk factors, not to mention valproate’s clear and significant risks for major congenital and neurodevelopmental anomalies, must be considered in balance with their substantial inferiority to lithium.
Since the turn of this century, scores of researchers have attempted to counter this pervasive misapprehension with new data, and, as such, after decades of investigation and monitoring, lithium’s therapeutic (and adverse) effects should be seen as predictable, with millions of cumulative treatment-years across thousands of patients which, in sum, provide us with reliable data and guidance for prevention. Given the clear advantage that serum monitoring affords, and the relationship of circulating lithium to both therapeutic and adverse effects, there is a clear predictability to commencing and maintaining lithium for the long-term. Thus, in contrast to alternative agents, many of which have neither a practicable measure of monitoring safety, adherence, nor relationship to expected therapeutic doses, lithium’s propensity to be measured easily ought to be seen as a boon. Such monitoring need not be as onerous as often perceived; once stabilised, most patients need only to attend to serum blood draws and urine collection twice a yearFootnote a (if that) – a process that is likely to become more accessible as point-of-care-testing (POCT) becomes available for such purposes.
Using lithium with confidence today
It is not the aim of this piece to minimise and dismiss the potential impact of lithium upon end-organ function, but merely to place such outcomes in perspective in light of today’s knowledge. Modern prescribing practices, such as once-daily (ideally nightly) dosing, regular (but not necessarily frequent) monitoring of renal function (eGFR), treating early concerns of polyuria with amiloride, avoiding lithium serum peaks into the toxic range and the assertive management of common comorbid risk factors for chronic kidney disease (diabetes mellitus, hypertension) can minimise the oft-feared outcomes of end-stage renal failure. When considered as an independent risk factor for renal insufficiency, lithium treatment has been grossly over-estimated; recent analyses estimate lithium’s independent contribution to monthly eGFR decline as 0.02 mL/min, Reference Clos, Rauchhaus, Severn, Cochrane and Donnan6 while cross-sectional studies find that there is no significant difference in eGFR between those treated with lithium for a mean of 7 years, and a matched non-lithium-treated cohort of patients with bipolar illness Reference Dastych, Synek and Gottwaldová7 – though notably, urine concentrating ability was reduced in the lithium cohort. Therefore, as with every medical intervention, the potential-yet-predictable risks of lithium treatment must be considered alongside its unmatched efficacy in preventing relapse and admission, preventing suicide and allowing patients to maintain recovery and hope in the long term (see Table 1).
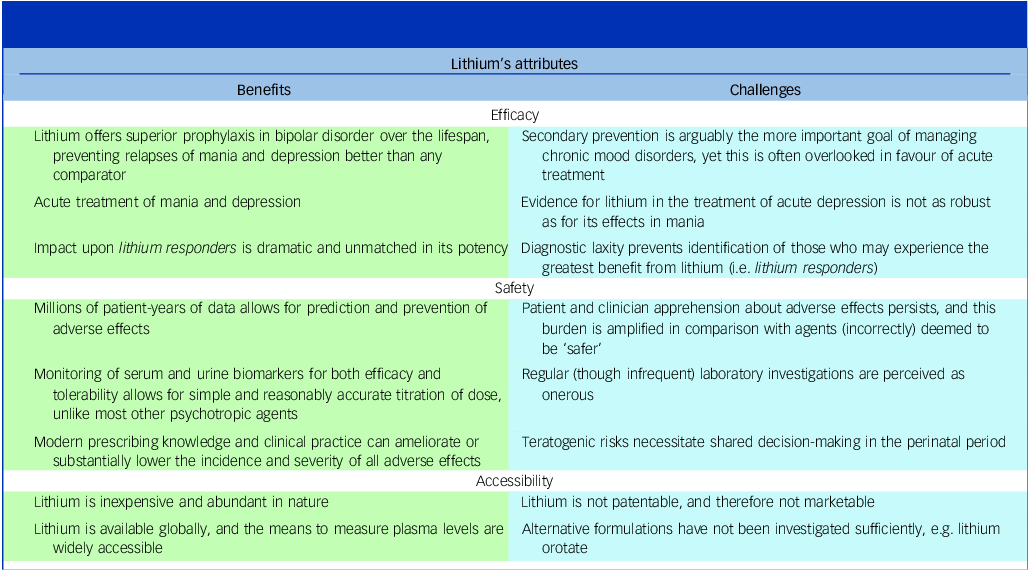
An overview of lithium’s attributes, and the challenges that prevent its renewed interest and ascendancy to the peak of management of bipolar disorder

What (else) makes lithium ‘special’?
Some of the key attributes of lithium therapy are shown in Table 1; however, if its merits over competitors remains unconvincing, then consider lithium’s neuroprotective abilities. First, people with bipolar disorder have a threefold higher risk for dementia, and longer-term lithium treatment decreases this risk by about half. Reference Velosa, Delgado, Finger, Berk, Kapczinski and de Azevedo Cardoso8 Second, alongside emerging evidence of ‘microdosed’ lithium having anti-aging properties, given that its comparators lack any such effects, this should bolster lithium’s primacy of use both in first-episode presentations of bipolar disorder, and over the course of the illness.
Other critical outcomes of bipolar illness often include admission and suicide, and here lithium asserts its dominance yet again; a 2024 review by Tondo and Baldessarini found a consistent association of long-term lithium treatment with reduced suicidal risk. Reference Tondo and Baldessarini9 This effect, though obviously important in patients with bipolar disorder who are the most likely to die by suicide, Reference Tondo and Baldessarini9 is also found in those with other mood disorders, such as unipolar recurrent major depression. Critically, the risk of suicidal behaviour increases 20-fold in the months following lithium discontinuation, and reduces again when lithium is restarted, Reference Tondo and Baldessarini9 supporting a likely specific drug effect. Thus, lithium’s status as perhaps psychiatry’s only disease modifying drug – one which alters the course of an illness and its prognosis, rather than merely providing symptomatic relief – is well-supported by the data, Reference Post, Li, Berk and Yatham2 and is reason enough to offer lithium to those that may benefit. Curiously, the longitudinal nature of these findings is consistent with some epidemiological studies, which found a link between higher concentrations of lithium in drinking water with lower rates of suicide. Reference Tondo and Baldessarini9 While certainly a novel approach to reduce suicide at a population level, such attributes are unique and ought to invite further speculation and interest. We summarise more of lithium’s unique capabilities in Box 1.
Additional attributes unique to lithium.
-
(a) Neuroprotective evidence, including decreasing the risk of Alzheimer’s dementia in those with bipolar illness, is unique among psychotropic agents
-
(b) Anti-suicide effects are consistent across diagnostic cohorts, and unmatched by other agents
-
(c) Emerging evidence that lithium may play a role in extending healthy lifespan and reducing all-cause mortality
-
(d) Positive haematological effects on neutrophilia and stimulating the immune response and possible antiviral effects
-
(e) A true disease-modifying agent for psychiatry that improves the course of mood disorders and enhances patient recovery substantially
The scarcity of similarly multi-faceted agents within psychiatry ought to magnify lithium’s popularity; yet, prescriptions for lithium in bipolar disorder have halved in recent decades while those for AEDs and SGAs have risen. 4 While this and other inconsistencies between evidence, clinical guidance and clinical utility reflect a complex interplay of factors, lithium’s intrinsic capabilities are not among the shortcomings. Any endeavours to enhance lithium’s uptake must therefore overcome the biases present within both clinicians and institutions that have thus far allowed other agents to overtake lithium in frequency of use, but not in primacy, ability or accessibility.
In conclusion, ever since its discovery, lithium continues to command authority having repeatedly reclaimed its throne. It has achieved this somewhat uniquely, not by assertion, but by fulfilling the treatment needs of those suffering from a severe mental illness such as bipolar disorder.
As a cornerstone of maintenance therapy for mood disorders, lithium serves as a cost-effective, globally accessible treatment that significantly reduces both morbidity and mortality. Indeed, nearly a century and half after Carl Lange’s prescient description of lithium’s effects on mood, and more than three-quarters of a century since John Cade’s (re)discovery of its benefits, lithium has once again demonstrated its supremacy in prophylaxis 4 – a decade and a half after the BALANCE trial. As the prototypical mood stabiliser, lithium excels beyond all, and reigns supreme.
Acknowledgements
The authors would like to acknowledge ongoing support from the Greek Young Matrons’ Association (GYMA) and from the Wellcome Trust. Gurubhaskar Shivakumar is currently enrolled as a Doctor of Philosophy student.
Author contributions
G.S. drafted the manuscript with input from all authors. All authors read and approved the manuscript.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
G.S. and K.S. have received grant funding from the GYMA. E.B. has received joint grant funding from the University of Sydney and National Taiwan University (Ignition Grant), grant funding from The North Foundation, and grant funding from the GYMA. R.P. has been provided with computer software (from SBT-pro) at no cost for research purposes. P.B. has received research funding through the NHMRC and has been on an advisory board for Servier and has received speaker fees from Lundbeck. G.S.M. has received grant or research support from the National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier; and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. He is the recipient of an investigator-initiated grant from Janssen-Cilag (PoET Study), joint grant funding from the University of Sydney and National Taiwan University (Ignition Grant) and grant funding from The North Foundation. G.S.M. is Editor-in-Chief of the British Journal of Psychiatry; he did not take part in the review or decision-making process of this paper.

eLetters
No eLetters have been published for this article.