


Introduction
The problem
Approximately 4.4% of the population has needs that are consistent with the diagnostic criteria for personality disorder (Coid et al., Reference Coid, Yang, Tyrer, Roberts and Ulrich2006), including difficulties in maintaining close and mutually satisfying relationships, problems in regulating emotions, and negative or inconsistent self-identity and self-worth (World Health Organization, 2022). The diagnosis of personality disorder is associated with difficulties in occupational, family, and social functioning (Chapman et al., Reference Chapman, Jamil, Fleisher and Torrico2023), high mortality rates (Fok et al., Reference Fok, Stewart, Hayes and Moran2014) and the frequent use of mental health services (Meuldijk et al., Reference Meuldijk, McCarthy, Bourke and Grenyer2017).
Diagnosis and terminology
The diagnosis of ‘personality disorder’ is controversial and has attracted a range of views for and against its use over decades (Centre for Mental Health, 2019). People can feel invalidated or untreatable after receiving the diagnosis and there are examples of it being used in a pejorative or judgemental manner (Sheridan Rains et al., Reference Sheridan Rains, Echave, Rees, Scott, Lever Taylor, Broeckelmann, Steare, Barnett, Cooper, Jeynes, Russell and Johnson2021). Whilst diagnosis is often needed for funding and access to evidence-based treatment, there is recognition that the label of personality disorder needs to change but little consensus on an agreed alternative (Lamb et al., Reference Lamb, Sibbald and Stirzacker2018). With reference to the above discussion, this paper will use the term complex emotional needs (CEN) to refer to people who present with symptoms of personality disorder, with or without a diagnosis.
Treatment (therapies, access and acceptability)
Psychological therapies have been developed for CEN (specifically for people with a diagnosis of borderline personality disorder) and are recommended as evidence-based treatments (National Institute for Health and Care Excellence, 2015). People with CEN present with a variety of symptoms and needs, and therefore flexible approaches that are responsive to the needs of each person are important (National Institute for Health and Care Excellence, 2015). There is encouraging evidence for therapies that involve talking one-to-one with a professional, such as cognitive behaviour therapy (CBT) and psychodynamic therapies, as well as therapies that involve individual and group sessions, including mentalisation based therapy (MBT) and dialectical behaviour therapy (DBT; Katakis et al., Reference Katakis, Schlief, Barnett, Sherdan Rains, Rowe, Pilling and Johnson2003). A Cochrane review highlighted that DBT appears to lead to a decrease in inappropriate anger, a reduction in self-harm and an improvement in general functioning. Whilst the review identified encouraging findings from single studies on other therapies, there were too few studies to establish firm conclusions on treatments other than DBT (Storebø et al., Reference Storebø, Stoffers-Winterling, Völlm, Kongerslev, Mattivi, Jørgensen, Faltinsen, Todorovac, Sales, Callesen, Lieba and Simonsen2020).
DBT was originally developed to treat individuals who present with a high risk of suicide or self-harm. In its standard form it includes weekly skills groups, individual therapy and DBT consultation (supervision groups for the practitioners), as well as telephone coaching which can be accessed between sessions as needed. Four modules are taught which include mindfulness, emotion regulation, interpersonal effectiveness and distress tolerance. The skills aim to help individuals increase their self-awareness, understand and manage intense emotions, maintain healthy relationships and survive crises. The skills are taught over 6 months and are then repeated, making the full course of therapy 12 months in total. Repeating the skills provides participants, who may be in crisis or feeling overwhelmed, the best opportunity to learn and apply them effectively.
DBT has been shown to be effective in a variety of different settings (Hernandez-Bustamante et al., Reference Hernandez-Bustamante, Cjuno, Hernandez and Ponce-Meza2024). However, DBT is resource intensive and therefore not readily available. It is often prioritised for people in secondary mental health care settings who present with the most severe symptoms and associated risks. Moreover, many healthcare professionals have little training or specialism in CEN, resulting in people often struggling to access effective treatments and being misunderstood or stigmatised by the professionals they are working with (Lamb et al., Reference Lamb, Sibbald and Stirzacker2018; Richter et al., Reference Richter, Bruno, Zum Eschenhoff and Bermpohl2016). Services can be set up in a manner that causes unintentional re-traumatisation or iatrogenic harm (Bolton et al., Reference Bolton, Lovell, Morgan and Wood2014). In summary, most individuals with CEN cannot access DBT unless they are in specialist services, and the support they do receive may be ineffective or stigmatising. There is a large disparity between the evidence base and the clinical practice people can expect to receive (Dale et al., Reference Dale, Sethi, Stanton, Evans, Barnicot, Sedgwick, Goldsack, Doran, Shoolbred, Samele, Urquia, Haigh and Moran2017).
National commitment
As part of the Mental Health Community Transformation Programme developed by National Health Service England, within the NHS Long Term Plan published in 2019 (NHS England, 2019), there is a renewed emphasis on providing people with CEN with better access to psychological therapies and personalised trauma-informed care. The transformation has aimed to promote partnership working between agencies to plug gaps in provision and thus more adequately meet a community’s needs, through a focus on early intervention in primary care and an added emphasis on lived experience.
Introduction to paper
Funding from NHS England led to the initial development of 12 pilot sites, each designed in response to local need, with the shared aim of ensuring people with CEN could receive timely evidence-based treatment without accessing secondary or tertiary services. The Relational and Emotional Difficulties Service (REDS) in Cambridgeshire was one of the early pilot sites and opened in early 2020. Subsequently, further teams were established across the UK, including the Help to Overcome Personal and Emotional problems (H.O.P.E) team in Northumberland which began in 2022.
The H.O.P.E team and REDS offer DBT that is adapted from the standard model; consultation, training and scaffolding to primary care, voluntary and community services; support to the local NHS 111 (mental health option) response service; and support to primary care services with assessments and referrals. The services’ offer of adapted DBT aims to provide individuals with skills to regulate their emotions and maintain healthy relationships, supporting them to function better in their work, family and social lives. Consequently, individuals’ mental health and quality of life may improve before their difficulties become more entrenched and require more intensive and costly treatment. Whilst there is research on psychological therapies, there is very little evidence on how to design services and systems of care (Foye et al., Reference Foye, Stuart, Trevillion, Oram, Allen, Broeckelmann, Jeffreys, Jeynes, Crawford, Moran, McNicholas, Billings, Dale, Simpson and Johnson2022). To the authors’ knowledge there has not been any published research evaluating the acceptability and feasibility of these services.
The aim of this paper is to describe and analyse the models offered by two services. We hope it will be interesting for the reader to note the different service designs and therapies offered. Both services provide DBT that is adapted from the standard model. First, we describe and analyse the H.O.P.E service, which is a newer, smaller service; then we describe the REDS service, which has been running long enough to have evolved a more varied offer. Finally, we offer a discussion of our shared learning points. We do not conclude that one service model offers a better service, but leave it to the reader to consider how acceptable and feasible the models might be in their geographical patches with their service users.
Characteristics of individuals referred to each service
Table 1 details the demographics of individuals who engaged with each service.
Development, results and analysis of the H.O.P.E service
Development
The Help to Overcome Personal and Emotional Difficulties (H.O.P.E) team was set up in 2022 through consultation with people with CEN, commissioners and other experts in the field. The initial service was piloted for a 3-month period before feedback was used to inform the team’s final offer.
Approach
Assessment, language and venues
The H.O.P.E team service aimed to support individuals with mild to moderate presentations of CEN in primary care settings before their problems became more entrenched and complex. In line with trauma-informed care (Matthew et al., Reference Matthew, Moffitt, Huth-Bocks, Ronis, Gabriel and Burkhart2022) the team’s name, letters and leaflets were co-created to avoid using overly medicalised or pejorative language. To promote accessibility, referral criteria were based on symptoms of mild to moderate personality disorder (World Health Organization, 2022), but formal diagnosis was not required (Table 2). The team aimed to work towards the principles of trusted assessment to minimise the need for people to repeat their story. Referrers were provided with training in assessing CEN and regular interface meetings to discuss referrals were established. Practitioners in the H.O.P.E team co-ordinated individual’s care once they were accepted into the service. The team located community venues across Northumberland to deliver therapy (e.g. community halls), linked to the finding that traditional mental health services and buildings can cause unintentional re-traumatisation (Bolton et al., Reference Bolton, Lovell, Morgan and Wood2014). Group sizes were set at 8–12 people to allow the best opportunity for discussion. Northumberland is largely rural (Northumberland County Council, 2021) and the option of online groups was provided for people that wanted to minimise their travel.
Referral criteria for the H.O.P.E team

Structured psychological intervention content
The team agreed to provide DBT without individual therapy (Kells et al., Reference Kells, Joyce, Flynn, Spillane and Hayes2020) to ensure there was capacity to deliver treatment across Northumberland. Individuals who engage in severe self-harm should be routinely offered one-to-one follow-ups (National Institute for Health and Care Excellence, 2022) and may present with severe, rather than mild to moderate symptoms of CEN. Therefore, the team agreed to focus its resource on supporting the large group of people with CEN that were not currently engaging in serious self-injurious behaviour. Skills to increase their self-awareness (mindfulness), understand and manage their emotions (emotion regulation) and maintain health relationships (interpersonal effectiveness) were included. Distress tolerance skills, focused on managing crises, were considered less relevant for this population and excluded. The ABC skills in the emotion regulation module are focused on helping individuals take care of themselves and work towards meaningful goals and values. Due to the target population having some capacity for self-direction and self-care it was agreed that the ABC skills could be condensed. The content took 3 months to deliver and was then repeated over a total of 6 months to give people the best opportunity to learn and practise the skills (see Table 3 below).
Content of the H.O.P.E adapted dialectical behaviour therapy programme

Additional interventions
The H.O.P.E team also provided interventions offered by peer supporters and a family therapist, which are not evaluated in the paper. The peer support pathway included individual sessions that aimed to be non-clinical and focus on emotional support, sharing personal experiences to inspire hope, and/or practical support where appropriate, and a 6-week psycho-education group on emotions. The family and carers pathway focused on providing family or couples therapy to individuals open to the team.
Method
For the purposes of this paper the analysis focuses on the DBT without individual therapy intervention.
Participants
Two hundred and three adults were referred to the team from January to December 2023. The demographics of individuals that engaged with the service and were included in the study can be found in Table 1. Inclusion criteria included: adults with CEN indicated by symptoms of mild to moderate personality disorder (World Health Organization, 2022). Exclusion criteria included: cognitive impairment resulting in problems retaining information; recent severe self-harm (less than 3 months); and presentations better explained by alternative diagnoses. Twenty-four people did not attend their assessment, 27 did not meet inclusion criteria and 34 did not want to pursue therapy. Out of the remaining 118, 46 (39%) attended an initial group session before discontinuing, 27(23%) engaged but discontinued before the end, while 45 (38%) engaged and completed 6 months of therapy.
Demographics and characteristics of individuals referred to each service

Intervention
The intervention delivered was a 28-week group DBT without individual therapy programme (Table 3). Sessions were 2 hours in duration and delivered in adherence to the DBT teaching manual (Linehan, Reference Linehan2015). The intervention was delivered once a week by DBT therapists with intensive training from a licensed provider who led on presenting the skills and facilitating group discussions, and a co-facilitator with lived experienced of mental health difficulties who focused on helping individuals to attend and stay in the group. The co-facilitators did not have formal training in DBT, which enabled them to focus on their lived experience perspective rather than drawing on professional or taught content. Five groups were delivered online, whilst five groups were delivered face-to-face. Group membership was between four and 12 people. The group was rolling with new members joining at the start of each module. Telephone coaching was provided as needed by the DBT therapists within office hours, Monday to Friday. In line with standard DBT, individuals were encouraged to use the telephone coaching to consolidate their learning, apply skills to everyday situations and manage crises if they arose (although this was uncommon due to the population working with the team). The team engaged in weekly 1-hour DBT consultation (supervision for the practitioners).
Measures
The following measures were completed pre and post treatment.
The Difficulties in Emotion Regulation Scale-16 item version (DERS-16) is a self-report measure which assesses emotion regulation across five subscales (Bjureberg et al., Reference Bjureberg, Ljótsson, Tull, Hedman, Sahlin, Lundh, Bjärehed, DiLillo, Messman-Moore, Gumpert and Gratz2016). It has been found to have high internal consistency (α = 0.92) and good test–retest reliability (Bjureberg et al., Reference Bjureberg, Ljótsson, Tull, Hedman, Sahlin, Lundh, Bjärehed, DiLillo, Messman-Moore, Gumpert and Gratz2016). Using ‘criterion b’ proposed by Jacobson and Traux (Reference Jacobson and Truax1991), data collected from a normative sample can be used to suggest that a score of 49.41 or above (two standard deviations above the mean) may represent a level of functioning that falls outside of the normal population (Burton et al., Reference Burton, Brown and Abbott2022).
The Level of Personality Functioning Scale-Brief Form 2.0 (LPFS-BF 2.0) is a self-report measure which assesses the severity of personality pathology. It has been found to have high internal consistency (α = 0.82) and high test–retest reliability (Weekers et al., Reference Weekers, Hutsebaut and Kamphuis2018). Data from a normative sample suggests using 36 as a cut-off point for symptoms that may represent severe dysfunction (Weekers et al., Reference Weekers, Sellbom, Hutsebaut, Simonsen and Bäck2022). This methodology is consistent with ‘criterion b’ proposed by Jacobson and Traux (Reference Jacobson and Truax1991) for establishing thresholds for clinically significant change.
A goal attainment measure: people identified an important goal in their life and rated how close they were to achieving it from 0 (not close at all) to 10 (achieved).
Procedure
Participants completed pre- and post-treatment measures as part of their standard care. Approval was given by the hosting NHS trust and individual consent was obtained. Participants were provided with the opportunity to engage in one-to-one interviews to provide feedback.
Analysis
Quantitative analysis
A Shapiro-Wilk and a Levene’s test confirmed that the data had a normal distribution and there was homogeneity of variances across groups. It was therefore appropriate to use parametric statistics.
An independent t-test was used to establish differences between participants that completed the 6-month intervention vs those that dropped out. Two-way repeated measures ANOVA analyses were used to analyse completers’ pre- and post-scores, and differences between online vs face-to-face groups. Data were analysed using JASP version 0.18.1.0 for Windows.
Qualitative analysis
The researchers working in the H.O.P.E team conducted online interviews and agreed on questions to use which included ‘What was your experience like with the H.O.P.E team?’, ‘Was there anything we could improve on?’, ‘How did your treatment compare with previous experiences of mental health care?’ and ‘Would you recommend the team to other people?’. Follow-up questions were used to explore initial answers and gain an in-depth understanding of a participant’s experiences. The interviews were not part of usual care and were specifically for the purposes of the service evaluation. Six individuals consented to be interviewed. The data were analysed using reflexive thematic analysis (Braun and Clarke, Reference Braun and Clarke2006; Braun and Clarke, Reference Braun and Clarke2019), which emphasises the importance of the researcher’s role in generating themes and narratives from the data. Whilst reflexive thematic analysis can include looking at the surface meaning of quotes (semantic analysis), it acknowledges that themes are constructed and guided by the researcher’s own experiences and subjectivities rather than existing within the data. Reflective thematic analysis has been widely used in health care (e.g. Aaron and Jones, Reference Aaron and Jones2025; Bekele and Martínez-Hernáez, Reference Bekele and Martínez-Hernáez2025).
The two authors attached to H.O.P.E were involved in each step of the analysis. Reflexive thematic analysis is subjective (Braun and Clarke, Reference Braun and Clarke2023), and whilst it is beyond the scope of the evaluation to provide an in-depth account of the researchers’ personal positions, is it worthwhile mentioning that they had personal and professional experiences of people with CEN often struggling to receive the right help and being stigmatised or rejected from services. Their experiences had motivated them to work for the H.O.P.E team and conduct the present evaluation.
The first step of the analysis involved the interviews being transcribed and reviewed several times to ensure the researchers were immersed in the data. The researchers then independently applied codes (labels) to describe what they had interpreted in the transcripts. To explore richer description of participants’ experiences, the researchers aimed to code inductively rather than using a pre-identified theory or model. The researchers collectively generated themes from the codes, which they organised into tables to construct relationships between themes, including over-arching and subthemes. Finally, the researchers defined and refined the themes and presented these with accompanying narrative.
Results
Drop-out
An independent samples t-test showed no significant difference in intake scores on the DERS-16 between discontinuers (M = 64.08, SD = 9.06) and completers (M = 62.28, SD = 10.26), t 76 = 0.74, p = .46. There were also no significant differences in intake scores on the LPFS-BF between discontinuers (M = 37.92, SD = 5.36) and completers (M = 38.00, SD = 6.25), t 76 = –0.057, p = .96.
DERS-16
A repeated measures ANOVA indicated that there was a significant time effect (F = 90.817, d.f. = 1, p < .001). Descriptive statistics indicated that pre-treatment scores (M = 61.96, SD = 10.33) were higher than post-treatment scores (M = 41.05, SD = 11.11). There was no significant interaction between time and method of delivery (F = 0.004, d.f. = 1, p = .95) and no significant effect of method of group delivery (F = 0.746, d.f. = 1, p = .393). The effect size, as measured by Cohen’s d, was 1.56, indicating a large effect.
LPFS-BF 2.0
A repeated measures ANOVA indicated that there was a significant time effect (F = 45.52, d.f. = 1, p < .001). Descriptive statistics indicated that pre-treatment scores (M = 37.89, SD = 6.29) were higher than post-treatment scores (M = 29.27, SD = 6.38). There was no significant interaction between time and method of delivery (F = 0.238, d.f. = 1, p = .63) and no significant effect of method of group delivery (F = 0.112, d.f. = 1, p = .74).
Goal-attainment scale
A repeated measures ANOVA indicated that there was a significant time effect (F = 181.07, d.f. = 1, p<.001). Descriptive statistics indicated that pre-treatment scores (M = 1.59, SD = 1.91) were lower than post-treatment scores (M = 6.54, SD = 1.35). There was no significant interaction between time and method of delivery (F = 1.42, d.f. = 1, p = .24). There was a significant effect of method of group delivery (F = 4.83, d.f. = 1, p = .03); higher post-therapy scores were reported in online (M = 7.10, SD = 1.14) vs face-to-face groups (M = 5.88, SD = 1.36).
Patient experience
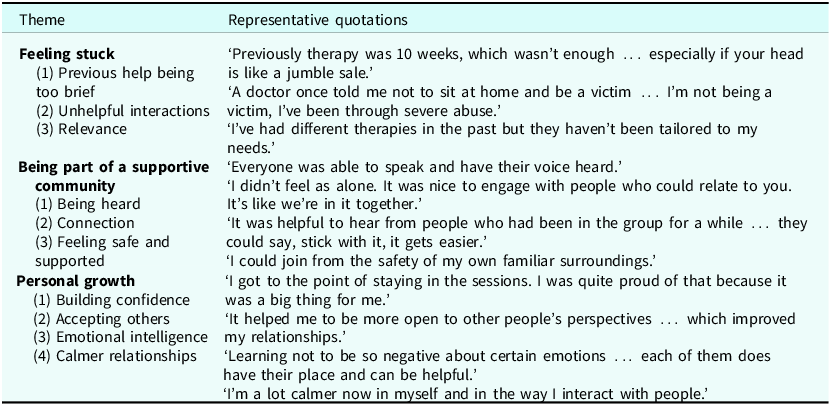
Reflexive thematic analysis of interviews generated three main themes (see Table 4).
Themes and representative quotations

Feeling stuck
The first theme generated from the interviews was ‘feeling stuck’, which related to some of the participants experiencing unhelpful or ineffective care prior to working with the H.O.P.E team. Participants spoke about therapy being too brief to help them understand their difficulties and worrying about therapy ending before they had made meaningful changes in their lives. Others commented that talking therapies had not been tailored towards their needs or relevant to CEN. Moreover, there were examples of unhelpful interactions with professionals who appeared to have a lack of knowledge regarding CEN and could use dismissive or pejorative language.
Being part of a supportive community
The second theme generated from the interviews related to participants feeling like they were part of a supportive community whilst working with the team. Participants spoke about everyone contributing to group sessions and their voice being heard. Several individuals commented on the importance of connecting with others who were experiencing similar difficulties, helping them to feel less isolated. Participants reflected that they received support from peers and valued how the effort the facilitators made to support everyone to attend. Whilst a group of participants preferred joining remotely online, others commented on the value of seeing people face-to-face.
Personal growth
The final theme generated from the interviews related to participants’ personal growth through engaging with the team. Participants commented that being in a group helped them to feel more confident talking in front of other people, gave them a better appreciation of other people’s perspectives and increased their confidence in managing differences of opinion. Participants reflected that therapy gave them more insight into their problems which allowed them to be reflective in their relationships or daily lives. Individuals felt calmer and able to respond to challenges less impulsively. Interestingly, several participants commented that the skills they learnt in therapy helped them to make positive changes in their lives, whilst others commented that the experience of being around others in the group was the most helpful aspect of therapy.
Development, results and analysis of the Relational, Emotional Difficulties Service (REDS)
Development
The Relational and Emotional Difficulties Service (REDS) was set up through a partnership between the Cambridge and Peterborough Foundation Trust (CPFT) Personality Disorder Community Service (PDCS) and the Cambridgeshire Peterborough and South Lincolnshire (CPSL) MIND service. REDS aimed to empower individuals by including them in decisions about their treatment (D’Souza and George, Reference D’Souza and George2019; Hashworth et al., Reference Hashworth, Reis, Townsend, O’Garr and Grenyer2022), and by following the principles of risk-need-responsivity, which involves individuals being offered the correct interventions at the right time (Andrews and Bonta, Reference Andrews and Bonta2010).
REDS agreed to offer service users the option of multiple interventions, which included a structured psychological treatment, a peer-led approach, or a combination of the two. In addition, service users could be signposted to community support or to a bespoke virtual learning environment which offered self-help and support for family and carers. It was agreed that peer support workers with lived experience would support the delivery of the interventions.
Financial resources were shared between CPFT (NHS) and CPSL MIND, who recruited and managed their own teams although they worked closely together. REDS aimed to cover a large geographical area with a population of 1 million.
Inclusion criteria
Inclusion criteria included being aged 17 or over and presenting with CEN indicated by symptoms associated with mild to moderate personality disorder (Table 5). Exclusion criteria included cognitive difficulties that would prevent the retention of information, and a forensic history assessed as a current risk to other group members (a separate pathway exists for those requiring reasonable adjustments).
Referral criteria for REDS

Structured psychological intervention content
Dialectical behaviour therapy (Linehan et al., Reference Linehan, Korslund, Harned, Gallop, Lungu, Neacsiu, McDavid, Comtois and Murray-Gregory2015) was chosen as the service’s psychological treatment model. DBT, delivered without individual therapy, has been widely recognised for its effectiveness in treating individuals with personality disorders and transdiagnostic difficulties with emotional dysregulation (Dobbs-March & Williams, Reference Dobbs-March and Williams2018; Delaquis et al., Reference Delaquis, Joyce, Zalewski, Katz, Sulymka, Agostinho and Roos2022; Heerebrand et al., Reference Heerebrand, Bray, Ulbrich, Roberts and Edwards2021; Lee et al., Reference Lee, Smith and Johnson2022).
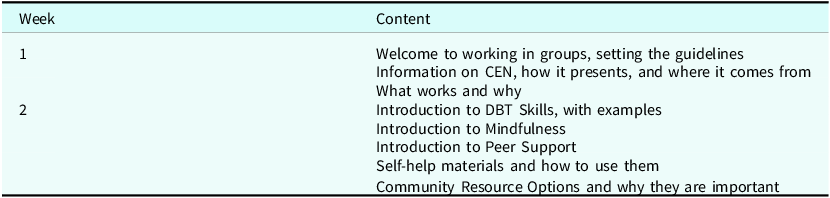
Individuals were initially offered two online sessions in a group called ‘Is This for Me’ (ITFM), which provided them with psychoeducation and an opportunity to experience group treatment (see Table 6). If they wished to proceed with psychological treatment, they were then required to telephone the service to opt-in to the interventions outlined below.
Content of the ‘Is This for Me’ programme

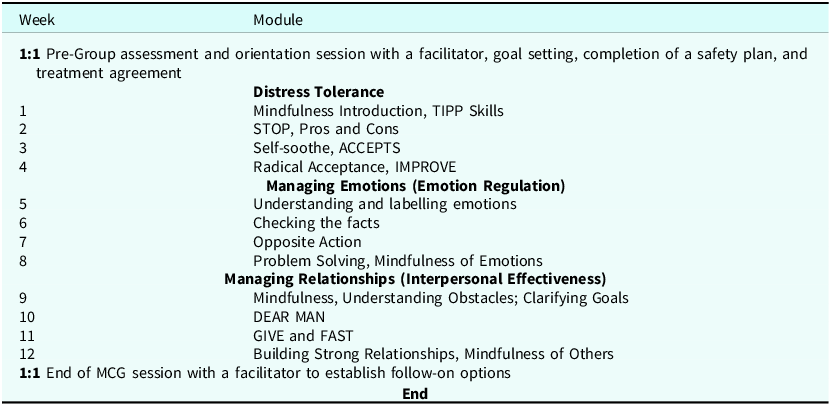
The REDS’ DBT programme – called Making Connections – was designed to meet the needs of a large and clinically diverse population, including individuals presenting with varying levels of severity and risk. Approximately 50% of participants reported engaging in deliberate self-harm at least once per month, although they did not meet the threshold for secondary mental health care services. In REDS, GPs continued to coordinate individuals’ care. Given the prevalence of self-harm, REDS retained all core DBT modules, including distress tolerance (Linehan, Reference Linehan2015). These skills were included to help individuals manage acute emotional distress and crises without resorting to self-harm (see Table 7). Facilitators cautioned against over-reliance on distress tolerance techniques and encouraged their use alongside longer-term strategies taught in other modules.
Module content of the REDS Making Connections programme

To accommodate diverse learning styles, the programme employed a variety of teaching methods, including didactic instruction, video materials, storytelling, metaphor, and peer sharing. Supplementary resources were provided to support skill consolidation, including access to online recordings of all taught skills, comprehensive workbooks, personalised planning tools (e.g. goal-based charts for preferred skills), and optional weekly coaching calls.
Additional interventions
Additional interventions were provided by REDS, which are not evaluated in this paper, but included a Peer Support Pathway, including a 12-week online group facilitated by CPSL MIND peer workers, which aimed to foster hope and connection through shared lived experience (Davidson et al., Reference Davidson, Chinman, Sells and Rowe2006; Repper and Carter, Reference Repper and Carter2011; Pfeiffer et al., Reference Pfeiffer, Heisler, Piette, Rogers and Valenstein2011), and a self-help platform developed to provide psychoeducational materials and a self-guided video programme, currently in pilot evaluation. For individuals that were not ready to engage in treatment, community engagement signposting was offered, promoting lifestyle and social wellbeing through resources such as the How Are You project and Recovery College Hub (Noordsy et al., Reference Noordsy, Abbott-Frey and Chawla2024; Richardson et al., Reference Richardson, Petukhova, Hughes and Pitt2024). Finally, family and carers were offered the chance to engage in the Family Connections Programme, which was a 12-week evidence-based course, shown to reduce caregiver burden and enhance empowerment (Hoffman et al., Reference Hoffman, Fruzzetti, Buteau, Neiditch, Penney, Bruce, Hellman and Struening2005).
Method
Participants
Two thousand four hundred adults were referred to the team between January and December 2024. Referrals to the team were predominantly from the Primary Care Mental Health Service. Additional referrals were accepted from secondary care mental health services for patients transferring, stepping down, or engaging with the REDS team alongside their treatment as usual. The demographics of individuals that engaged with the service and were included in the analysis can be found in Table 1.
Nine hundred and forty-eight people joined the introductory Is This for Me workshops. Three hundred and fifty people started the Making Connections groups, and 201 people completed the programme. This reflects a 57% completion rate, calculated from participants who attended the first session of the Making Connections group and maintained at least 75% attendance across the programme. One hundred and forty-one participants completed their outcome measures and were included in the analysis.
Intervention
The intervention delivered was a 12-session DBT without individual therapy programme (see Table 7).
The DBT skills programme was delivered in accordance with the core principles and recommendations outlined by Linehan (Reference Linehan2015). Groups were conducted online, with up to 20 participants per session. Groups were 2 hours in length, including a short break. Twelve sessions were provided over a 16-week period, in three modules, each four sessions long. New participants joined at the start of each module. Sessions were facilitated by three DBT trained staff, including one peer support worker from CPSL MIND. The facilitators led on presenting skills, whilst the peer support workers facilitated group feedback and shared personal experience to engage and motivate the group. All staff attended a weekly 1-hour supervision session and a 1-hour weekly team meeting.
Optional weekly telephone coaching (15 minutes per week) was provided within office hours with participants encouraged to book as needed. While in standard DBT telephone coaching is used to manage crises, the REDS programme primarily focused on using coaching to support participants to apply skills to everyday situations and consolidate their learning. Participants with urgent needs were signposted to the local First Response Service (FRS) who had received training in DBT skills.
Measures
The following measures were completed pre- and post-treatment.
The Difficulties in Emotion Regulation Scale-18 item version (DERS-18) is a self-report measure which assesses difficulties in emotion regulation across five subscales (Victor and Klonsky, Reference Victor and Klonsky2016). The internal consistency of the DERS in this study was excellent, with a Cronbach’s alpha of 0.91. Using ‘criterion b’ proposed by Jacobson and Traux (Reference Jacobson and Truax1991), data collected from a normative sample can be used to suggest that a score of 53.26 or above (two standard deviations above the mean) may represent a level of functioning that falls outside of the normal population (Burton et al., Reference Burton, Brown and Abbott2022).
Two risk-related questions asked for the frequency of deliberate self-harm and attempted suicide in the previous month.
Two open-text questions related to the experience of treatment: ‘What do you think were the best or most useful parts of the treatment group?’ and ‘Is there any feedback you would like to give us that may help us improve the group programme?’.
Procedure
Participants completed their outcome measures as part of their standard care – pre- and post-treatment, alongside basic demographic information.
Analysis
Quantitative analysis
A Shapiro-Wilk and a Levene’s test were conducted, confirming that the data had a normal distribution and there was homogeneity of variances across groups. Independent t-tests were used to establish differences between participants who completed treatment and those that discontinued, and to compare completers that filled in both pre- and post-treatment measures, against completers that only filled in their pre-treatment measures.
To understand more about which participants benefited the most from treatment, participants were separated into two groups. The self-harm group included participants that had engaged in any form of self-harm or suicidal behaviour a month prior to treatment and included 36 individuals. The no self-harm group had not engaged in any self-injurious behaviour a month prior to treatment and included 105 individuals. Two-way repeated measures ANOVA analyses were used to analyse completers’ pre- and post-scores, and differences between the self-harm vs the no self-harm group.
The data collected for risk was measured on an ordinal scale, which does not require the assumption of normal distribution. Therefore, a non-parametric test was deemed more appropriate. A Wilcoxon signed-rank test was conducted to compare frequency of incidents of self-harm prior to receiving treatment and after treatment.
Data were analysed using SPSS version 29.0 for Windows.
Qualitative analysis
REDS routinely asked participants an open-ended question administered with their outcome measures, ‘What do you think were the best or most useful parts of Making Connections (DBT skills group)?’. Due to the time constraints of routine clinical practice, no follow-up questions were used. A total of 141 responses were received and included in the analysis. To align with the H.O.P.E. approach, the team adopted the same reflexive thematic analysis methodology (Braun and Clarke, Reference Braun and Clarke2006; Braun and Clarke, Reference Braun and Clarke2019).
Two authors affiliated with REDS were involved in all stages of the analysis. These researchers are professionals who chose to work in the service to improve the support and treatment for a group of people who are often stigmatised and overlooked.
The first step of the analysis involved collating and repeatedly reviewing the written feedback to ensure immersion in the data. The researchers then independently applied codes to capture the meaning and key features of the responses. Next, the researchers collaboratively generated inductive themes from the codes, organising them into tables to illustrate relationships between over-arching themes and subthemes. Finally, the themes were defined and refined and presented alongside a narrative summary to convey participants’ experiences.
Results
Drop-out
An independent samples t-test showed no significant difference in intake scores on the DERS-18 between discontinuers (M = 65.34, SD = 12.42) and completers (M = 64.74, SD = 12.73), t 443 = 0.497, p = .62. There was also no difference in the intake scores of completers that filled in pre- and post-measures (M = 65.01 SD = 12.47), against completers that only completed their pre-treatment measures (M = 64.42, SD = 13.07), t 259 = 0.38, p = .71.
DERS-18
A repeated measures ANOVA indicated that there was a significant time effect (F = 86.386, d.f. = 1, p < .001). There was no significant interaction between time and self-harm status (F = 1.815, d.f. = 1, p = .180). There was a main effect of self-harm status (F = 6.680, d.f. = 1, p < .05). Descriptive statistics indicated that the self-harm group had higher pre (M = 70.53, SD = 11.51) and post (M = 56.50, SD = 14.14) intervention scores, compared with the no self-harm group’s pre (M = 63.12, SD = 12.27) and post (M = 52.65, SD = 14.21) intervention scores. The effect size, as measured by Cohen’s d, was 0.83, indicating a large effect. These findings suggest that Making Connections groups had a meaningful impact on individuals’ ability to regulate their emotions.
Self-harm
A Wilcoxon signed-rank test was conducted to compare frequency of self-harm at two time points. The results indicated a statistically significant difference between frequency of self-harming behaviour at pre-treatment (Mdn = 2) compared with post-treatment (Mdn = 1), U = 99.5, z = –1.97, p = .05, r = –0.25, indicating a small to medium effect size. This suggests that risk scores significantly reduced following completion of Making Connections.
Qualitative patient experience
Analysis of participant feedback from the Making Connections Group revealed four over-arching themes (Table 8).
Themes and representative quotations

Developing skills and gaining control
Participants consistently highlighted the value of learning DBT skills such as STOP, TIPP, mindfulness, Radical Acceptance, and Check the Facts. Applying these tools allowed them to regulate emotions, respond more thoughtfully to challenging situations, and experience increased confidence and control over their behaviours.
Connection and shared understanding
The group format provided a strong sense of community. Participants valued hearing others’ experiences, realising they were not alone and feeling understood. Peer discussion and feedback normalised struggles, enhanced motivation to practise skills, and reduced feelings of isolation and shame.
Supportive and accessible learning environment
Facilitators were praised for their clarity, warmth, and professionalism. Structured materials, visual aids, opportunities for reflection, and the balance between presentation and discussion supported engagement and skill retention. While some participants found the online format challenging, most appreciated its accessibility and flexibility.
Personal growth and hope
Many participants described meaningful personal transformation, including improved emotional awareness, better relationships, and a greater sense of optimism. The group fostered motivation to continue using DBT skills and helped participants feel more capable of managing distressing situations independently.
Overall, Making Connections was perceived as a practical, supportive, and transformative programme, combining skill development with relational support to enhance participants’ emotional wellbeing and self-efficacy.
Discussion
Learning point 1: The H.O.P.E team and REDS provide acceptable service models
The present study aimed to present and compare two services that support people with CEN in primary care. The results of this study suggest that both the H.O.P.E team and REDS provide evidence-based therapy in primary care that is acceptable for people with CEN in Northumberland and Cambridgeshire. Before receiving treatment, participants’ average scores in both services were in the clinical range for emotion dysregulation. In the H.O.P.E team, average scores on an additional outcome measure for symptoms of personality disorder were also in the clinical range. People who completed therapy with both teams reported a statistically significant improvement in their ability to regulate their emotions. In the H.O.P.E team, average post-treatment scores fell within the non-clinical range, while in REDS average scores reduced but were still within the clinical range. However, it should be noted that REDS had broader inclusion criteria and likely worked with a population that had a higher severity of difficulties. In the H.O.P.E team, after receiving treatment, average scores for symptoms of personality disorder were within the non-clinical range, whilst people felt closer to achieving meaningful goals in their lives.
REDS found that post-treatment, participants reported a significant reduction in the frequency of self-harm, which is an encouraging finding. Both services manage risk through safety planning, access to skills coaching and frequent liaison with professionals in primary care. However, in the REDS model, GPs remain the primary coordinators of a patient’s overall care, whereas in the H.O.P.E team, this responsibility sits with practitioners in the team. REDS also employs two senior nurse practitioners, who work as non-medical prescribers and can review individuals’ pharmacological treatment further to providing advice to GPs. The H.O.P.E team follows policies and processes designed for secondary mental health care services, which includes practitioners providing individual face-to-face reviews after incidents of self-harm and assertive attempts to engage participants who do not attend appointments. Paradoxically, the processes followed by the H.O.P.E team results in the service having limited capacity to manage individuals that present with higher risks. REDS has the flexibility to follow policies and procedures designed for primary care. The service is generally uninformed of incidents of self-harm, and as a result, there is no formal process for practitioners to follow up with participants. In addition, participants are required to opt in rather than being assertively followed up after missed appointments. The service also has additional support from non-medical prescribers. The REDS model allows clinicians to provide input for individuals who present with higher risks. Other services may wish to consider how these models fit their contexts.
In Northumberland and Cambridgeshire, people with CEN previously struggled to access evidence-based therapy. Therapies such as DBT have a strong evidence base (Hernandez-Bustamante et al., Reference Hernandez-Bustamante, Cjuno, Hernandez and Ponce-Meza2024) but are resource intensive. DBT involves a year of treatment that includes weekly skills group, individual therapy and DBT consultation (supervision groups for the practitioners), further to telephone coaching as needed. As a result, specialist mental health teams often prioritise therapy for people with the highest complexity and risk. People trying to access therapy often do not have the opportunity to receive evidence-based therapies for CEN. When therapies are available there can be significant waiting times, repeated assessments and a requirement for individuals to receive diagnoses that can be stigmatising (Bolton et al., Reference Bolton, Lovell, Morgan and Wood2014). The H.O.P.E and REDS teams were established to ensure that people with CEN in Northumberland and Cambridgeshire received better care. The teams aimed to make therapy accessible by providing shorter adapted versions of DBT that did not include weekly individual sessions and used the principles of trauma-informed approaches, including access being based on need rather than diagnosis. DBT skills groups have previously been found to be effective in reducing symptoms of CEN (Kells et al., Reference Kells, Joyce, Flynn, Spillane and Hayes2020). The findings of the present study suggest that providing an adapted 28- or 16-week model of DBT using the principles of trauma-informed care is an acceptable and cost-effective intervention.
Qualitative feedback highlighted that the services provided people with the opportunity to be part of a supportive community, which helped them to appreciate others’ perspectives, tolerate different personalities and feel less isolated with their difficulties. People also spoke about building confidence in expressing themselves in front of other people and learning specific skills to manage their emotions and relationships, which had improved their quality of life. Individuals commented that their experiences with the services contrasted with previous help which was often not tailored to their problems, too short, or delivered in a stigmatising or pejorative manner. In summary, the H.O.P.E and REDS teams provide a model which is less resource intensive and enables services to deliver cost-effective therapy to many people. We would recommend that other services consider the use of adapted DBT without providing individual therapy.
We believe that the following issues and service developments warrant discussion as they represent our on-going efforts to develop easy-to-access services to meet the needs of a wide range of people, some of whom continue to struggle to access therapy.
Learning point 2: Recommended length of treatment
The two services provide DBT without individual therapy that is adapted from the standard model. The H.O.P.E team’s intervention is 28 weeks long and delivered by qualified DBT therapists. It includes weekly skills groups, DBT consultation (supervision group for practitioners adhering to a strict agenda) and telephone coaching as needed. The REDS team provides a 16-week model, which is delivered by a broader range of practitioners, some of whom are qualified DBT therapists, and some who have completed basic DBT training only. The service includes a weekly skills group, a supervision group for the practitioners and telephone coaching on request (up to 1 × 15-minute call a week). The H.O.P.E model is closer to the gold standard of DBT but is more resource-intensive, whilst the REDS model is further away from the full model but allows more people to be seen with a smaller resource. The findings indicated that people who finished therapy with either team reported significantly lower levels of symptoms.
Qualitative feedback highlighted some advantages of a longer period of therapy. Participants reported that they valued having the time to build trust and make supportive relationships with other people in the group. The longer duration of therapy allowed participants to learn how to manage differences of opinion, gain a better insight into others’ perspectives and build their confidence in expressing themselves. Participants spoke about initially struggling to take in all the information presented but being more able to understand and reflect on the content during the second half of therapy. Participants commented that 6 months of therapy contrasted with previous experiences of individual therapy that had not led to meaningful changes in their life.
The current study’s methodology, however, does not allow the effectiveness of both services’ therapy programmes to be directly compared beyond observing descriptive statistics. It is therefore worthwhile considering the broader literature. Evidence-based approaches for CEN are intensive and normally last between one and two years (Binks et al., Reference Binks, Fenton, McCarthy, Lee, Adams and Duggan2012). Clinicians providing shorter interventions for CEN should carefully consider the length of treatment related to the findings that interventions which are too brief may be ineffective when compared against treatment as usual (McMurran et al., Reference McMurran, Crawford, Reilly, Delport, McCrone, Whitham, Tan, Duggan, Montgomery, Williams, Adams, Jun, Lewis and Day2016), or increase the cost of people’s care (Tyrer et al., Reference Tyrer, Tom, Byford, Schmidt, Jones, Davidson, Knapp, MacLeod and Catalan2004). In relation to DBT without individual therapy, most of the evidence base is for interventions delivered over 6 months (Kells et al., Reference Kells, Joyce, Flynn, Spillane and Hayes2020; Lyng et al., Reference Lyng, Swales, Hastings, Millar, Duffy and Booth2020; McMain et al., Reference McMain, Guimond, Barnhart, Habinski and Streiner2017; McMain et al., Reference McMain, Chapman, Kuo, Dixon-Gordon, Guimond, Labrish, Isaranuwatchai and Streiner2022) or 12 months (Linehan et al., Reference Linehan, Korslund, Harned, Gallop, Lungu, Neacsiu, McDavid, Comtois and Murray-Gregory2015). However, Soler et al. (Reference Soler, Pascual, Tiana, Cebrià, Barrachina, Campins, Gich, Álvarez and Pérez2009) found encouraging outcomes for a 13-week intervention and the current evaluation suggests that the REDS 3-month offer was acceptable.
In summary, no firm conclusions about the optimal length of treatment can be made based on the present study. We would recommend that future researchers and clinicians aim to establish the best treatment duration by directly comparing the effectiveness of 3- vs 6-month interventions.
Learning point 3: Making services accessible and reducing discontinuation rates
Both services predominantly received referrals from primary care settings (primary care mental health practitioners or NHS Talking Therapies for Anxiety and Depression), with a smaller proportion referred from secondary mental health care services. In a direct comparison of the services, the H.O.P.E team received a higher proportion from secondary care, which is likely due to REDS accepting individuals who were engaging in self-harm directly from primary care, whilst these individuals may have been referred to secondary mental health care services in Northumberland.
The discontinuation rates in both services were high. After people had contacted the HOPE team, 27% went on to complete therapy (discontinuation rate of 73%), whilst in the REDS team, 25% went on to complete therapy (discontinuation rate of 75%). These findings suggest that even when evidence-based therapies are available, many individuals struggle to engage in them. High discontinuation rates are likely to be an inevitability of such a service. Severity of symptoms, age, risk history, therapeutic relationship quality, specific characteristics of complex emotional needs (e.g. impulsivity, identity confusion), various psychological elements (e.g. motivation, anxiety), and sociodemographic variables all contribute to a higher discontinuation rate (Martino et al., Reference Martino, McDermut and Behrends2012; Panfilis et al., Reference Panfilis, Frater and Roberts2012). Practitioners’ experience, waiting times, and external factors such as childcare costs, work, and health commitments have also been recognised as influencing whether people drop out of therapy (Marshall et al., Reference Marshall, Thompson and Fisher2016). Moreover, regardless of the type of therapy, people with CEN have been found to be more likely to drop out of group-based interventions compared with individual therapies. This finding is likely to be due to groups being less personalised and individuals with CEN struggling to trust or tolerate being with other people in a group treatment (Arntz et al., Reference Arntz, Mensink, Cox, van den Berg, Hafkenscheid, van Dijke and de Jongh2023). However, high discontinuation rates represent a risk to services; service users can interpret their lack of attendance as failure (with long-term negative ramifications), and services waste resources by providing clinicians to run poorly attended groups. To mitigate against these factors, the H.O.P.E and REDS services have considered the pre-treatment process.
Both the H.O.P.E and REDS services use language that focuses on service users ‘opting-into’ therapy, and being able to easily return in the future, normalising that it can be hard to commit to therapy. They offer people the chance to meet someone from the team in a one-to-one appointment (the H.O.P.E team calls these introductory appointments, whilst the REDS team calls these pre-group one-to-one’s) and attend two initial group sessions before opting-in to the full programme. In REDS these sessions are called ‘Is This for Me’ and participants need to formally opt in, while in the H.O.P.E team the two sessions are the two mindfulness sessions at the start of each module; participants are asked to inform the team if they do not want to continue with the group. The one-to-one sessions help people problem-solve barriers to attending therapy and set measurable goals, which have been shown to improve motivation, clarify expectations, and improve client satisfaction (Elliott et al., Reference Elliott, Watson, Goldman and Greenberg2013; Locke and Latham, Reference Locke and Latham2002). People particularly value meeting someone from the team with lived experience, and whenever possible connected to the therapy group they will be joining. The group sessions are aimed at helping people understand what therapy involves and whether they can manage a group setting, before committing to treatment. The H.O.P.E service provides a one-to-one appointment before the chance to trial group sessions, whilst REDS provide the group sessions before the one-to-one appointment. The order appears to make no noticeable difference to longer-term retention.
When people attended both initial group and one-to-one sessions, 63% of people went on to complete therapy with the H.O.P.E team (discontinuation rate of 37%) whilst 57% of people went on to complete therapy with the REDS team (discontinuation rate of 43%). This is comparable to other studies providing DBT without individual therapy (49%, Kells et al., Reference Kells, Joyce, Flynn, Spillane and Hayes2020). It is worth noting that lower drop-out rates have been reported by programmes that offer ongoing individual therapy or case management alongside group attendance (Linehan et al., Reference Linehan, Korslund, Harned, Gallop, Lungu, Neacsiu, McDavid, Comtois and Murray-Gregory2015).
Our findings suggest that services should consider offering people one-to-one appointments and trial sessions in a group setting before starting therapy. People value these appointments and can decide whether they want to proceed with therapy. If they are not ready, services may then offer their place to someone else. Research suggests that services may consider incorporating some form of case management to run alongside group programmes to further improve engagement. It is important that services try to reduce non-engagement, although any offer of individual sessions needs to be balanced against the team’s capacity and resources.
Learning point 4: Matching the right level of therapy to the severity of need
The H.O.P.E team and REDS have attempted to remain inclusive, managing a diverse range of need whilst providing the appropriate level (or dose) of therapy. Both services accept referrals based on need rather than diagnosis and were set up to support people with CEN in primary care settings, bridging gaps between primary and secondary care. Each service was developed to work alongside secondary mental health care services.
The thresholds of the H.O.P.E and REDS services differ. The H.O.P.E service excludes people who present with deliberate self-harm or other high-risk behaviours, referring these cases to secondary care. In contrast, REDS supports individuals who present with ongoing self-harm and suicidal behaviour, if they are motivated to engage in treatment. Only those who are ambivalent towards therapy or present with a high degree of complexity or co-morbidity are referred to the secondary care mental health care services.
In the REDS team, individuals that engaged in any self-harm in the month before treatment, had higher pre- and post-scores on the DERS-18. Post-treatment scores were within the clinical range. Research has shown that individuals with the highest level of risk place the most demand on services and often experience the lowest quality of life (Mizen et al., Reference Mizen, Rost and Cardoso2025). Therefore, to further address the needs of individuals who present with self-harm, the REDS team introduced DBT (FASTER) (McMain et al., Reference McMain, Chapman, Kuo, Dixon-Gordon, Guimond, Labrish, Isaranuwatchai and Streiner2022). This intervention includes 20 wrap-around individual sessions with a DBT therapist, focused on reducing risk behaviours. Participants are expedited into a DBT skills group, reducing the time they wait for therapy.
Initial findings suggest that DBT (FASTER) is operating successfully and a full evaluation is currently taking place. Although this model requires additional staff and resources, it is less intensive than a full DBT programme and enables individuals with higher levels of risk to access therapy in primary care settings.
The team’s findings suggest that consideration should be given to whether groups are too inclusive. It is likely that people who engage in more serious self-harm and risky behaviour may need more intensive interventions including individual sessions. One solution may be to consider different groups for different severities, or shorter vs longer therapy models.
Learning point 5: Online vs face-to-face therapy
Northumberland is a largely rural county (Northumberland County Council, 2021) whilst Cambridgeshire is more densely populated. A large proportion of people accessing help from the H.O.P.E team therefore live in remote locations with poor transport links. The team aims to stay accessible by providing face-to-face groups across the county, alongside online therapy that allows people to receive help without travelling. This evaluation identified that online therapy was an acceptable alternative to face-to-face therapy. Participants in online groups reported that they felt closer to achieving important goals in their lives. However, there were no further significant differences between self-reported outcome measures or drop-out rates. Due to the design of study, it is hard to establish why goal attainment was different across the two groups. However, overall findings are consistent with research suggesting that people can still feel connected and benefit from DBT when it is delivered online (Bock et al., Reference Bock, Graf, Woeber, Kothgassner, Buerger and Plener2022). Qualitative feedback highlighted that people valued the flexibility of being able to join online and avoid long journeys or costly trips on public transport, especially for people with work or childcare commitments. Several people reported that an online evening group outside of normal working hours was particularly accessible. Others preferred face-to-face therapy, commenting that they were uncomfortable using technology and could make better connections with other people in person. The REDS team operates almost entirely online, except for the offer of a choice of online or face-to-face appointments for any pre-group individual sessions.
The findings of the study suggest that services should consider offering people the choice of online or face-to-face therapy. Online therapy appears to be an acceptable option for people wanting to minimise their travel and accommodate work and family commitments, whilst face-to-face therapy provides the chance to connect with others in person. When working with people in rural and remote locations, often with poor transport links, offering both online and face-to-face options is particularly important.
Learning point 6: Ensuring services are accessible to groups from ethnic minorities, and patients with complex needs
Northumberland has a largely White population (97.7% White, 1.0% Asian, 0.8% Mixed Race; Northumberland County Council, 2021) whilst the population in Cambridgeshire is more diverse (88.6% White, 5.8% Asian, 1.4% Black; JNSA, 2023). A recent REDS service evaluation (K. Peterson, Reference Peterson2023; in-house, unpublished) looked at how proportionately the service is meeting the needs of the population. Results showed that in Cambridge, ethnic groups are proportionally represented. However, in Peterborough, the service was under-represented by minority ethnic groups. This finding is consistent with several published papers exploring representativeness of service users and finding inequality in access for minority ethnic groups (e.g. Beck et al., Reference Beck, Naz, Brooks and Jankowska2019; Mercer et al., Reference Mercer, Evans, Turton and Beck2019; Teager et al., Reference Teager, Dunning, Mirza, Methley and Twigg2023).
In Cambridgeshire, the REDS team are developing their relationship with the Ely Neighbourhood Wellness Hub. This is an initiative bringing together community-based health, social care, and third sector organisations to improve the accessibility of care by providing joined-up, person-centred support in the community. Ely have funded a full-time post in REDS, to support the team to provide a more flexible service to residents and explore barriers that prevent people from accessing the team. REDS have begun to run therapy groups face-to-face in neighbourhood premises (non-NHS settings). Staff employed in third sector agencies are present to support people to attend. This offer appears to be particularly useful for people with social issues who may not be able to access technology or require more assertive support to attend group sessions. Part of the offer has included REDS providing specialist training, which aims to upskill professionals in supporting individuals with CEN across the system. An evaluation of the pilot is underway.
We would recommend that services consider how to engage under-represented groups; this may include thinking about venues used for therapy, partnership working with third sector agencies and raising the awareness of services through training and education with key stakeholders.
Limitations
The current study has several limitations. Firstly, measures were only collected pre- and post-intervention and around 25% of service users did not complete measures in the REDS team. As a result, it was difficult to establish when change occurred and if it was attributable to therapy. Secondly, the study did not include intention to treat analysis, and both services used different outcome measures (apart from variations of the DERS). As a result, direct comparisons could not be made between the effectiveness of the two service models. A measure of skill acquisition (e.g. DBT ways of coping checklist; Neacsiu et al., Reference Neacsiu, Rizvi, Vitaliano, Lynch and Linehan2010) would have enabled the paper to explore which component of therapy appeared to be more important (learning new skills, connecting with other people, clinicians inspiring hope, etc.). Thirdly, the qualitative analysis for the REDS service was based on a single positively framed question. We recognise that this approach likely reduced the breadth of responses and potentially introduced bias, limiting the opportunity to explore the service limitations or participants’ negative experiences. Finally, there was not enough follow-up data collected to be included in the study. As a result, the longer-term impact of the REDS 3-month intervention, compared with the H.O.P.E team’s 6-month intervention could not be explored. We would recommend that future research should consider more frequent data collection, more sensitive outcome measures, follow-up data and the use of intention to treat analysis.
Conclusion
In conclusion, it has been recognised that individuals with CEN in Northumberland and Cambridgeshire have struggled to access evidence-based treatment for their difficulties, often facing long waiting times, repeated assessments and the need to receive a diagnosis before getting the correct help. As part of community transformation, the H.O.P.E team and the REDS team were set up to provide better care for this group of people. Both services aimed to provide adapted versions of DBT that could provide people with evidence-based therapy, whilst remaining accessible by shortening the length of therapy and removing individual therapy sessions. The present study found that both services supported individuals with CEN to access evidence-based therapy. Whilst there were high discontinuation rates, individuals that completed therapy found it to be acceptable, reported significantly lower scores on measures of symptoms and felt closer to achieving important goals in their lives. Several recommendations are provided for similar services including reflections on helping to reduce the number of people who drop out, the length of treatment, online vs face-to-face offers and engaging people from minority groups. The results of the study are encouraging and have implications for future research and clinical recommendations.
Key practice points
-
(1) Adapted DBT without individual therapy appears to be cost-effective and acceptable treatment for people in Northumberland and Cambridgeshire.
-
(2) CEN services should consider ways to help people engage in therapy, including offering pre-treatment one-to-one sessions, taster group therapy sessions and the opportunity to meet peer supporters with lived experience. Online is an effective alternative to face-to-face therapy and where possible people should be offered a choice.
-
(3) We would recommend that services should be led by need, rather than diagnosis. Services should be sensitively designed to provide interventions of varying intensity and duration to meet differing needs in risk and complexity.
-
(4) CEN services should consider how to engage people from minority backgrounds. This may include partnership working with third sector agencies, considering the venues used for therapy, and raising the awareness of services through training and education with key stakeholders.
-
(5) Future researchers should consider regular data collection, follow-up data, sensitive outcome measures, and comparison groups to establish the effectiveness of treatment.
Data availability statement
The data that support the findings of this study are available from the authors J.B.C. and A.B., upon reasonable request.
Acknowledgements
The REDS service would like to thank colleagues at CPFT who wrote the early bids and have supported the development of this new service. The REDS service would like to acknowledge the input from their partners at CPSL MIND, with whom they have a close working relationship and who provided information and data on the Peer Support Groups presented in this article. With particular thanks to Bex Ward-Turner (Service Manager: Emotional Difficulties Support Service) and Hannah Turner (Head of Services: Crisis, Recovery and Safeguarding). The REDS service would like to thank Dr H. Fraser, and Dr K. Peterson who completed their DClinPsyc Service Evaluation Projects for the REDS (in conjunction with the University of East Anglia) and who contributed significantly to our understand of Discontinuation Factors (Dr Fraser), and our Ethnic Minority reach (Dr Peterson). The H.O.P.E team would like to thank colleagues in CNTW who have supported the development of this initiative.
Author contributions
James Bowness Clarke: Conceptualization (equal), Formal analysis (equal), Investigation (equal), Methodology (equal), Validation (equal), Writing - original draft (equal), Writing - review & editing (equal); Amanda Barton: Conceptualization (equal), Formal analysis (equal), Investigation (equal), Methodology (equal), Software (equal), Writing - original draft (equal), Writing - review & editing (equal); Natalia Bojor: Data curation (equal), Project administration (equal); Lauren Green: Data curation (equal), Project administration (equal); Jonathan Tse: Data curation (equal), Project administration (equal).
Financial support
None.
Competing interests
The authors declare none.
Ethical standards
The authors have abided by the Ethical Principles of Psychologists and Code of Conduct as set out by the BABCP and the BPS. Standard local NHS governance arrangements were in place to manage data. Participants consented to their data being used for service evaluation purposes, including publication of findings.






 Open access
Open access
Comments
No Comments have been published for this article.