


Introduction
Radiotherapy, a cornerstone in the treatment of many cancers, is received by nearly 50% of all cancer patients at some point in their care. It is a high-precision treatment modality that requires meticulous attention to quality and safety. Despite technological advancements, radiotherapy errors ranging from minor deviations to serious adverse events continue to pose risks to patient outcomes. Reference Hendee and Herman1,Reference Das, Johnson, Hayden, Riley, Harrelson and Gillin2 Governance in this context encompasses the policies, procedures and organisational culture that enable safe practice and continuous improvement.
A need to increase patient safety was recognised within the healthcare community. The Institute of Medicine’s Reference Kohn, Corrigan and Donaldson3 seminal report To Err is Human reframed patient safety as a systems issue rather than one of individual failure, catalysing international efforts to develop governance structures that promote transparency, learning and resilience. This foundational work has informed many subsequent initiatives in radiotherapy, where complex technology and multidisciplinary care require coordinated safety oversight. ASTRO’s Safety is No Accident further promoted safety through structured governance and checklists. 4 This was followed by European guidance on risk management, providing a framework for embedding governance into routine radiotherapy practice. 5 The AAPM Task Group 100 methodology advocated for a proactive risk assessment to underpin safety in treatment planning and delivery. Reference Huq, Fraass, Dunscombe, Gibbons, Ibbott and Mundt6
The radiotherapy community has a long history and a solid reputation for safety, as highlighted by Vijayakumar et al and Leonard & O’Donovan. Reference Vijayakumar, Duggar, Packianathan, Morris and Yang7,Reference Leonard and O’Donovan8 Influence has been taken from safety-critical industries and automation to manage complex systems with multiple professionals involved. Reference Hollnagel9,Reference Verhagen, S de Vos and Sujan10 Internationally, the push towards zero harm in radiation oncology has prompted a re-evaluation of how safety is understood and managed. Reference Hollnagel9 Traditional Safety I models, which focus on identifying and preventing failures, are increasingly supplemented by Safety II approaches that emphasise learning from what goes right. Reference Verhagen, S de Vos and Sujan10–Reference Tarkiainen and Haapea12 However, embedding these principles into governance structures remains inconsistent. Reference Verhagen, S de Vos and Sujan10
Context within existing literature
Incident learning systems (ILS) have become a central mechanism for advancing safety governance in radiotherapy, evolving from early international reviews of major incidents to structured national programmes. Shafiq et al. Reference Shafiq, Barton and Noble13 identified over 7,000 radiotherapy-related events across three decades, establishing the foundation for the World Health Organization Radiotherapy Risk Profile and reinforcing the need for global learning structures. Building on this, Arnold et al Reference Arnold, Ward and Gandhidasan14 and Ford et al Reference Ford and Evans15 described the development of ILS as a mature safety science process, emphasising system-based thinking, a just culture and shared learning across institutional and national levels. National programmes demonstrate how coordinated governance frameworks can enhance both safety culture and standardisation. Early European initiatives, such as the Radiotherapy Safety Information System survey, Reference Cunningham, Coffey and Knoos16 demonstrated the value of voluntary international collaboration, setting the groundwork for later programmes such as Safety in Radiation Oncology (SAFRON) and National System for Incident Reporting in Radiation Treatment (NSIR-RT).
In the United States, the Radiation Oncology Incident Learning System (RO-ILS) integrates legal protections under the Patient Safety and Quality Improvement Act, enabling secure nationwide reporting. Reference Hoopes, Dicker and Eads17 Similarly, Canada’s NSIR-RT was developed through consensus to align with international taxonomies, illustrating how stakeholder engagement strengthens adoption and comparability. Reference Milosevic, Angers and Liszewski18 At a global level, the IAEA’s SAFRON database provides valuable insight into error causation, highlighting persistent communication failures and the pivotal role of radiographers in event detection. Reference Zarei, Gershan and Holmberg19
Local experience further underscores the importance of leadership and cultural readiness. Implementation studies, such as Radicchi et al, Reference Radicchi, de Toledo and Alliprandini20 demonstrate that incident learning succeeds when supported by feedback loops and leadership commitment. Broader analyses by Pawlicki et al Reference Pawlicki, Coffey and Milosevic21 confirm that linking local, national and international systems amplifies learning opportunities and aligns governance structures across contexts. Together, these models illustrate a maturing international framework where learning systems act as the operational backbone of radiotherapy safety governance.
While previous reviews Reference Ford and Evans15,Reference Pawlicki, Coffey and Milosevic21 have examined incident learning systems and safety culture in radiation oncology, this review uniquely synthesises governance mechanisms and international policy structures shaping error reporting, offering a radiographer-focused perspective on safety leadership.
Methodology
A comprehensive search was carried out on the topic of interest by a single reviewer using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Figure 1). Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow22 The reviewer identified studies examining governance and error reporting in radiotherapy. A structured literature review was conducted using electronic databases, including Elsevier, ProQuest, Cinahl and Medline. The search commenced in April 2025. When relevant articles were retrieved using the inclusion criteria (Table 1) and thoroughly reviewed, the associated reference lists from those articles were also scanned by a single reviewer. This allowed the identification of further studies of interest that the search terms (Table 2) did not capture and to broaden the scope of the search. Data were extracted into a structured summary table (Table 3) and grouped thematically according to recurring domains of governance, safety culture and technological innovation. Any discrepancies or borderline cases were resolved by decision based on relevance to radiotherapy governance.

Figure 1. PRISMA flow chart. Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow22
Table 1. Inclusion/exclusion criteria

Table 2. Search terms

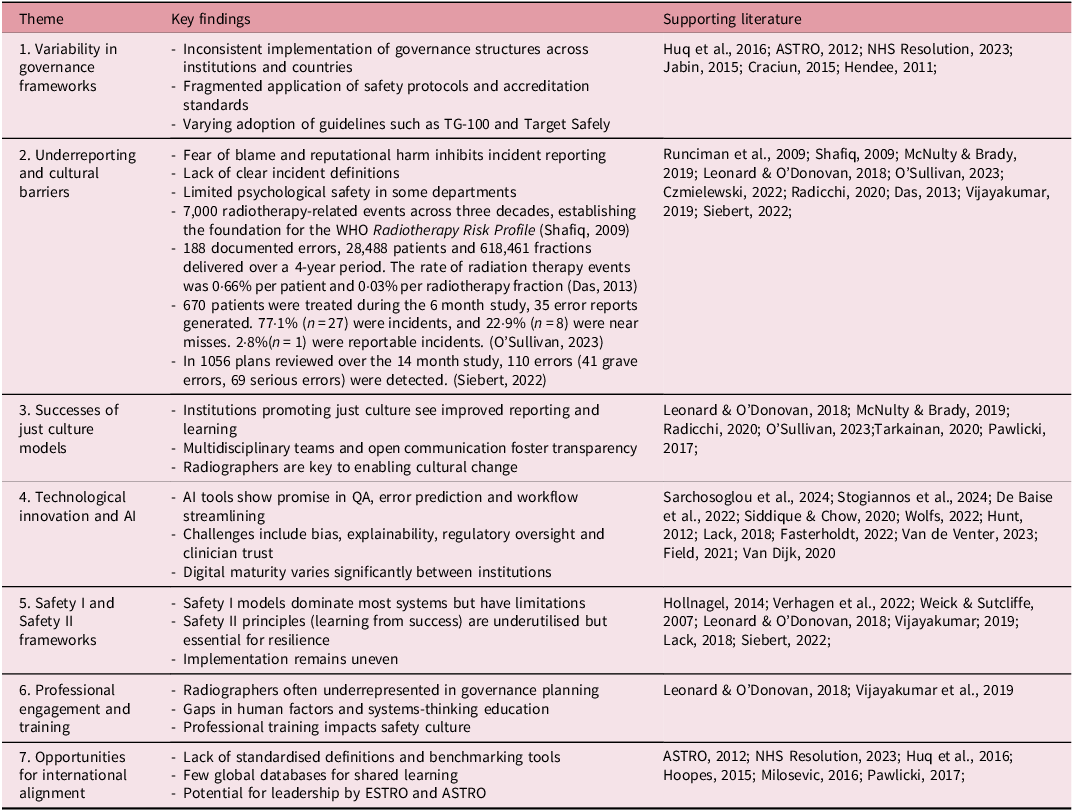
Table 3. Key findings from studies reviewed

Last search performed 24/4/2025
Results
Three primary themes emerged from the literature:
-
1. Variability in Governance Frameworks
Many radiotherapy departments adopt localised governance procedures shaped by national policy or accreditation bodies. Reference Huq, Fraass, Dunscombe, Gibbons, Ibbott and Mundt6,Reference Jabin, Schultz and Hibbert23 While some institutions implement comprehensive risk assessment protocols like those outlined in AAPM Task Group 100, Reference Huq, Fraass, Dunscombe, Gibbons, Ibbott and Mundt6 others lack structured systems. Fragmentation of governance results in unequal levels of oversight, with variability even within the same country or region. In their global study of radiotherapy departments, Leonard and O’Donovan Reference Leonard and O’Donovan8 identified marked variation in how safety culture is perceived and enacted across clinical teams. Their work emphasises the role of governance in fostering a shared understanding of safety, promoting openness and supporting multidisciplinary engagement in incident reporting and learning.
Several national bodies have attempted to classify best practices. The UK’s Ionising Radiation (Medical Exposure) Regulations (IR(ME)R) provide statutory requirements for error reporting and learning, while ASTRO’s Target Safely initiative promotes the use of checklists and prospective risk analyses. Reference Jabin, Schultz and Hibbert23 Despite these efforts, the implementation of such frameworks varies widely. Furthermore, inconsistent application of recommendations often stems from resource limitations, staff shortages and differing levels of commitment to safety improvement initiatives. Reference Tarkiainen and Haapea12 Systematic reviews have demonstrated that structured quality improvement interventions can significantly impact patient safety outcomes. Reference Jabin, Schultz and Hibbert23
-
2. Cultural Barriers to Incident Reporting
Underreporting of incidents remains a persistent barrier to safety improvement. Fear of blame, professional reputation concerns and unclear definitions of error types contribute to low reporting rates. Reference Jabin, Schultz and Hibbert23–Reference Wolfs and Verhaegen25 Additionally, hierarchical dynamics and departmental silos may hinder communication across professional groups, exacerbating the reluctance to disclose mistakes. Reference Wolfs and Verhaegen25–Reference O’Sullivan and Lyons27
Conversely, institutions that foster a “just culture” where staff feel empowered to report and learn from errors without fear of retribution demonstrate improved incident analysis and safety outcomes. Reference Leonard and O’Donovan8,Reference O’Sullivan and Lyons27 Radiographers, as frontline practitioners, play a key role in establishing such cultures by modelling transparency and advocating for system changes. Investment in team training, open communication workshops and interprofessional education can further strengthen this cultural shift.
-
3. Technological Opportunities and Gaps
Emerging technologies offer opportunities for enhanced governance, particularly in the form of artificial intelligence (AI) and automated safety systems. Trends show that advances in computerised systems have been associated with declining rates of radiotherapy errors. Reference Hunt, Pastrana, Amols, Killen and Alektiar28 Innovative detection tools embedded in treatment planning workflows have shown success in capturing errors early. Lack et al. Reference Lack, Liang, Benedetti, Knill and Yan29 demonstrated the effectiveness of automated detection tools in identifying errors during radiotherapy treatment planning. Their study showed a clear reduction in errors over two years when advanced planning review systems were used. This supports calls for governance systems that integrate technology not only as an operational aid but as an embedded safety barrier with real-time oversight capabilities. AI-based quality assurance tools are being developed to detect planning inconsistencies, automate data checks and prioritise high-risk cases. Reference Sarchosoglou, Cividjianm and Zhou30
Despite these benefits, significant challenges remain. Many systems are in early developmental stages and require validation before clinical implementation. Additionally, issues related to algorithmic bias and data governance must be addressed to ensure safe and ethical use. Reference Stogiannos, Litosseliti and O’Regan31,Reference De Baise, Sourlos and Van Ooijen32 Moreover, a lack of digital infrastructure and insufficient clinician training can impede the effective use of such technologies. Stakeholder engagement, including patients, will be critical to ensure that AI adoption enhances, rather than undermines, trust and care quality.
Discussion
The experiences of international incident learning systems offer valuable parallels for the UK radiotherapy context, particularly as services transition towards the Patient Safety Incident Response Framework (PSIRF). 33 The success of national models such as RO-ILS and NSIR-RT highlights the benefits of structured taxonomies, protected reporting environments and consistent feedback mechanisms. Reference Hoopes, Dicker and Eads17,Reference Milosevic, Angers and Liszewski18 These features align closely with PSIRF principles of system learning and proportionate response, suggesting that radiotherapy governance in the UK could further mature through enhanced data harmonisation and shared learning across centres.
Evidence from SAFRON and departmental ILS implementations also underscores that the effectiveness of governance depends as much on cultural factors as on structural design. Communication failures, limited feedback and variable adherence to procedures remain leading contributors to incidents internationally. Reference Radicchi, de Toledo and Alliprandini20,Reference Pawlicki, Coffey and Milosevic21 These findings mirror challenges identified in UK reporting pathways, where local learning can be isolated from national oversight. Strengthening two-way information flow between radiotherapy departments and national databases could therefore enhance the practical value of learning outcomes, supporting the shift from a reactive Safety I model to a more anticipatory Safety II approach.
Embedding leadership visibility and multidisciplinary engagement, as seen in successful international programmes, may further reinforce local safety governance. In this sense, PSIRF implementation provides an opportunity to operationalise these global insights—moving from compliance-based reporting to a genuinely learning-oriented governance culture.
This review reveals that while advancements in radiotherapy technology and risk management tools have improved safety, these gains are undermined by inconsistent governance structures and persistent underreporting of incidents.
Governance Frameworks: The disparity in governance frameworks across institutions and countries highlights the need for synchronisation. Implementation of Safety II principles and frameworks, such as the High Reliability Organisation model, could foster more resilient systems. Reference Weick and Sutcliffe34,Reference Siebert, Hirt and Delaperriere35 Safety II encourages a proactive approach that examines why things usually go right, thereby strengthening preventive strategies. Embedding such models requires leadership commitment, a shared vision for safety and the allocation of dedicated resources to quality improvement initiatives.
International collaboration could facilitate shared learning and benchmarking, enabling organisations to measure progress against best practice standards. Establishing centralised databases for anonymised incident reporting and analysis would help identify trends and inform policy. Global professional bodies, such as ESTRO and ASTRO, could play a leadership role in standardising expectations and fostering mutual accountability.
Safety Culture: Safety culture is a foundational component of governance. Training in communication, leadership and human factors should be embedded into professional development for radiographers. Studies show that the establishment of multidisciplinary incident review boards can facilitate learning from complex errors and near misses. In their systematic review, Jabin et al. Reference Jabin, Schultz and Hibbert23 evaluated the effectiveness of quality improvement interventions aimed at improving patient safety in radiology. Their findings supported the introduction of evidence-based, system-level changes such as service evaluations, regular staff education and embedded performance monitoring, which are equally applicable in radiotherapy and align closely with governance reform initiatives seeking to strengthen safety and quality.
The frequency of adverse events due to unnecessary radiation exposure across Europe illustrates the continuing need for digital safeguards. Tarkiainen et al. Reference Tarkiainen and Haapea12 analysed data from national incident reports in Finland, identifying multiple cases of unnecessary radiation exposure due to lapses in governance and system checks. Their research underlines the critical importance of routine safety audits, integrated digital controls and adherence to national safety standards, all of which should be central to radiotherapy error governance strategies.
Furthermore, organisational leadership must prioritise psychological safety, enabling open dialogue and feedback without fear of repercussion. Regular staff surveys, focus groups and anonymous suggestion schemes can provide valuable insight into cultural barriers and perceptions. Radiographers should be encouraged to participate in policy development and quality assurance committees, reinforcing their ownership of safety processes. Reference Tarkiainen and Haapea12 Effective governance requires integration of risk management principles recognised in other imaging specialities, as highlighted by Craciun et al., Reference Craciun, Mankad and Lynch36 who described how well-established risk management structures in diagnostic radiology departments, such as standardised error classification systems, proactive audits and training in human factors, have contributed to a culture of safety. These strategies are directly translatable to radiotherapy settings and can enhance governance by creating structured, preventative frameworks to mitigate patient risk before errors occur.
Digital Transformation and Risk Mitigation: Fluctuations in error reporting during system stressors, such as the COVID-19 pandemic, further highlight the importance of resilient digital governance frameworks. Czmielewski et al. Reference Czmielewski, Gallina and Tripoli37 demonstrated that the COVID-19 pandemic caused significant disruption to routine reporting of radiotherapy errors, particularly in treatment planning. The shift in reporting patterns during this period was attributed to increased clinical workload, rapid protocol changes and stress across teams. Their findings reinforce the importance of embedding governance frameworks that are flexible and resilient during crisis scenarios, capable of sustaining safety surveillance even under pressure.
AI presents a transformative opportunity for radiotherapy governance. However, to realise its potential, integration must be carried out with clinician involvement and robust regulatory oversight. Trust in AI systems can be enhanced by co-design approaches, clear accountability structures and outcome evaluation. Reference Fasterholdt, Kjølhede and Naghavi-Behzad38–Reference van de Venter, Skelton and Matthew40
Further research is needed to evaluate the real-world impact of AI-driven interventions on safety outcomes. Partnerships between academic institutions, industry and clinical departments can support its development. Education programmes should prepare future radiographers and oncologists to interpret AI outputs, understand their limitations and use them judiciously. Reference Field, Hardcastle and Jameson41,Reference van Dijk, Van den Bosch, Aljabar, Peressutti, Both and Steenbakkers42
Limitations of the Review: The review is limited by its focus on English-language studies and may not capture governance practices in non-English-speaking countries. Furthermore, much of the literature relies on self-reported data, which may underestimate error frequency. Another limitation is the heterogeneity of study designs and methodologies, which makes direct comparison challenging. Future reviews could benefit from including patient advocacy perspectives to gain a more comprehensive understanding. While few studies directly examined patient involvement in error governance, emerging NHS frameworks advocate for transparency and co-production. Incorporating patient perspectives into safety discussions could enhance accountability and trust.
Recommendations
-
Develop international consensus on error definitions and reporting frameworks
-
Embed just culture training within radiotherapy departments
-
Facilitate multidisciplinary review and learning from near misses
-
Involve radiographers in governance design and AI development
-
Support national-level benchmarking and incident sharing initiatives
-
Allocate resources for leadership development in safety and quality
Key implication for practice
Establishing a radiographer-led governance initiative that integrates just culture principles and AI-supported incident analysis could significantly enhance patient safety, promote learning from near misses and standardise practice across radiotherapy departments.
Conclusion
Radiotherapy governance must evolve to meet the demands of increasingly complex treatment delivery and rapid technological change. A comprehensive approach incorporating standardised policy, a robust safety culture and responsible use of AI can improve patient safety and system learning. Radiographers, as integral members of the oncology team, must be central to these efforts. By promoting transparency, collaboration and innovation, radiotherapy services can foster a culture of continuous quality improvement. Importantly, sustained improvements in governance will require long-term commitment, cross-sector collaboration and a willingness to challenge the status quo. The future of safe radiotherapy lies not only in technology but also in the systems and cultures that support its responsible use.
Financial support
None.
Competing interests
None to declare.




 Open access
Open access