

The Malaysian Context
Gender in Society
Malaysia is in South-East Asia with a population of 32.5 million in 2020. Malaysia’s population is mainly divided into three categories: Bumiputera which has 69.3% of the population (Malay and Indigenous people); non-Bumiputera (non-native), which has mostly Chinese (22.8%) and Indian (6.9%) people; and others (1%). The current sex ratio is 106 males per 100 females for citizens and 156 males per 100 females for non-citizens. (1)
Gender equality has improved slightly in Malaysia, with the Malaysia Gender Gap Index (MGGI) increasing from 0.709 in 2019 to 0.714 in 2020. (1) MGGI measures the differences between men and women in fours sub-indices: political empowerment, health and survival, educational attainment, and economic participation and opportunity. A score of 1.0 (100%) indicates that the equality of women and men has been achieved. Women have surpassed men in the educational attainment sub-index with a score of 1.059 but not for the health and survival sub-index recorded (score of 0.956) nor for economic participation and opportunity (score of 0.738). A women’s labour force participation rate (LFPR) of 55.3% in 2020 was far behind neighbouring countries such as Singapore (69.7%) and Thailand (66.8%). There is no barrier for females to enter any industry or occupation in Malaysia. However, there are differences between the number of males and females in different sectors, reflecting the choices and aspirations of Malaysian females. (Reference Lim2) In 2015, 8.6% of females were involved in ‘human health and social work activities’, compared to 1.3% among males. In addition, females contributed to 48.5% of the medical doctors, 38.4% of the obstetrics and gynaecology specialists and 42.4% of psychiatrists. (Reference Arrizabalaga, Abellana, Vinas, Merino and Ascaso3)
Based on the Institut Public de Sondage d’Opinion Secteur (IPSOS) 2018 survey on gender equality, the top three issues facing Malaysian women were sexual harassment, sexual violence and sexualization of women in the media. (4) These findings are similar to women globally, except that the third issue worldwide has been physical violence. Gender equality is still challenged by negative cultural values and misconstrued religious beliefs around power, privilege and control held by men. These differences significantly drive sexual discrimination, gender-based violence and sexual harassment. Despite the government’s commitment to the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW) and SDG5, and while in-roads have been made into education, health and labour, relatively few women hold positions in decision-making roles.
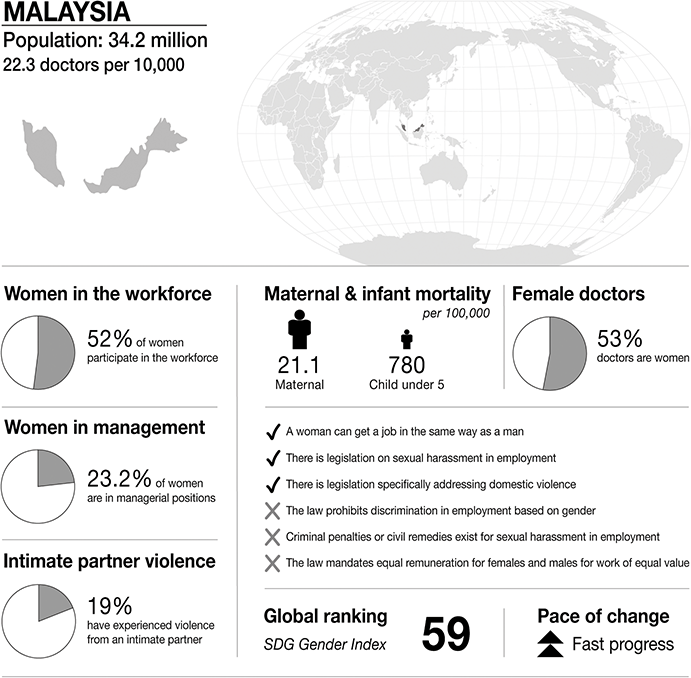
Infographic Malaysia. Infographics were provided by CartoGIS Services, The Australian National University. Population: from World Bank https://databank.worldbank.org/source/population-estimates-and-projections. Sustainable Development Progress, global ranking and statistics on women in the workplace, women in management and intimate partner violence: from United Nations SDGs Data Portal https://unstats.un.org/sdgs/dataportal. Female doctor percentage: from Global health workforce statistics www.who.int/data/gho/data/themes/topics/health-workforce. Legislation and law statements: from the World Bank gender data portal 2023 https://genderdata.worldbank.org/en/indicators. Maternal mortality statistics: from the Global Health Observatory 2020 https://mmr2020.srhr.org. Infant mortality statistics: from United Nations International Children’s Fund (UNICEF) https://data.unicef.org/topic/child-survival/under-five-mortality.

Figure 24.1 Long description
The infographic provides information about Malaysia, with a population of 34.2 million and 22.3 doctors per 10,000 people. It highlights several gender-related statistics. 52 per cent of women participate in the workforce. 23.2 per cent of women are in managerial positions. 19 per cent of women have experienced intimate partner violence. Maternal mortality is 21.1 per 100,000. Infant mortality under 5 is 780 per 100,000. 53 per cent of doctors are women.
The infographic lists the presence or absence of law and policy on gender equality. In Malaysia:
– a woman can get a job in the same way as a man.
– there is legislation on sexual harassment in employment.
– there is legislation specifically addressing domestic violence.
– the law does not prohibit discrimination in employment based on gender.
– there are no criminal penalties or civil remedies for sexual harassment in employment.
– there is no law that mandates equal remuneration for females and males for work of equal value.
The S D G Gender Index global ranking is 59, and there has been fast progress
Gender in Medicine
Gender disparities can occur in medical specialities, although these disparities may vary by country. Generally, females make up the majority in fields such as general practice, obstetrics and gynaecology, and palliative medicine, while men dominate in specialities such as cardiology and most surgical areas. (Reference Moberly5; 6) The reasons for this are unknown, but it could reflect women’s role in society, where they are seen as warm caregivers. Proportion-wise, a study conducted in 2014 found that far fewer female doctors attained consultant status compared to their male counterparts within a similar timeframe. (Reference Arrizabalaga, Abellana, Vinas, Merino and Ascaso3) There is limited up-to-date statistical data on gender distribution in the Malaysian health care workforce, but available figures suggest that the number of female doctors is rising in Malaysia. While 63.6 per cent of medical specialists were male in 2010, analysis within age groups revealed that Malaysian doctors were gradually shifting from a male-majority workforce towards a female-majority workforce. (6) The data showed that while medical specialists over sixty had an 85:15 male-to-female ratio, this ratio gradually progressed in the opposite direction with younger age groups. For medical specialists under thirty, the gender distribution was 39:61, favouring females. The trend was reversed with more senior specialists. The Ministry of Education of Malaysia reported that the proportion of female medical students enrolled in public universities was 63.3% in 2014. However, a lack of more recent data suggests that it remains uncertain whether these higher numbers of female medical students were translated into higher numbers of female clinical specialists and consultants. (Reference Arrizabalaga, Abellana, Vinas, Merino and Ascaso3; Reference Wan7)
Medical Education
Medicine is a very challenging field, and selection into medical school was only available for a select privileged few before the mushrooming of private medical schools. Medicine is a very desirable career among Malaysians. Many Malaysian parents aspire for their children to study medicine, which is perceived as a noble, honourable, and well-paid profession. The entry points into medical school are generally very competitive. Surviving medical school for five to six years can be gruelling. Furthermore, things do not get easier upon graduating as house officers. House officers have to wait a long time for a posting, which can be competitive, as permanent posts are limited. The remaining doctors may be offered positions working with the government under contract, which comes with significantly fewer benefits, such as access to speciality training.
There are a few pathways of study to become a doctor. Students can opt to train after completing a pre-university programme such as Form 6 (government schools), matriculation (in local colleges/universities) or other internationally recognized programmes such as A-Levels. (8) After a recognized pre-university programme is completed, a student can opt to study medicine at a public or private university. Currently, there are eleven public universities and twenty-two private universities offering medicine as a course that the Malaysian government recognises. (9) The curriculum in medical schools may not include modules on gender-based violence. Similarly, post-qualification training may not provide training on this topic.
An undergraduate medical course typically takes five years to complete before graduation. (8) After graduation, a medical graduate must complete two years of compulsory service as a house officer or intern at a designated tertiary-level public hospital anywhere in the country. Training includes postings in six compulsory departments, and each department has an appointed supervisor for house officers. Any medical graduate must be employed in a government hospital for house officer training and a further two years as a medical officer. At present, private hospitals in Malaysia do not offer house officer training. A medical officer can opt to pursue postgraduate training after serving another two years of compulsory service in a government hospital. (Reference Yong10). Postgraduate training typically takes four years, and fellowship training can range from three to four years. This can also be done at a government hospital or overseas. (Reference Yong10)
Legal Framework
Malaysia has different legislative instruments which can be used to address sexual harassment cases, but a standalone comprehensive sexual harassment law does not exist. The Penal Code requires proof beyond a reasonable doubt and is therefore rarely enforced in the case of sexual harassment. The following key legislations are referred to or used for sexual harassment cases. They include the Code on Prevention and Eradication of Sexual Harassment in the Workplace (1999); the Employment Act 1955 (amended 2012), Part XVA on sexual harassment, which provides guidelines on prevention in workplaces; and Tort of Sexual Harassment for civil action since 2016. (11) The draft of specific sexual harassment legislation was by the joint action group against violence against women (JAG-VAW). Currently, it is known as Joint Action Group on Gender Equality (JAG-GE) and has fourteen active women’s groups.
Women’s groups first proposed a draft sexual harassment bill in 2001. It was further developed by a Special Project Team on the Sexual Harassment bill and first presented to Parliament in 2021. Several provisions from the original Bill were dropped, including that of organizational duties, which would have provided provisions for organizations to have a duty to prevent and address sexual harassment. A Coalition on Advocacy of Sexual Harassment Bill 2021, comprising the JAG-GE, Engender Consultancy and Young Women Making Change, advocated for an initial comprehensive Sexual Harassment Bill. However, when the Sexual Harassment Bill 2021 was passed in 2022, it only defined sexual harassment, the setting up of a Tribunal to address sexual harassment cases and a committee to work on the guidelines and implementation of the new Act. Moving forward, women’s groups are intending to continue to work with the Ministry of Women, especially on guidelines for the new Sexual Harassment Act, including positive organisational duties. The Ministry of Women, Family and Community Development has announced that the Act will be implemented in stages, including the setting up of the Tribunal. We hope that this new Sexual Harassment Act will provide protection for all and prevent sexual harassment in the country.
Medical Regulation
All medical practitioners in Malaysia, regardless of whether they are in the public or private sectors, are regulated by one body, the Malaysian Medical Council (MMC). (12) All medical practitioners are required to abide by and comply with the Code of Professional Conduct of the MMC, and this is mainly to ensure propriety in professional practice by medical practitioners and to prevent abuse of professional privileges. The Code of Professional Conduct emphasises the health and welfare of the individual and family under the care of a practitioner as of the highest importance.
The council is comprised of medical professionals and was established under the Medical Act 1971 (amended 2012). The Medical Act is legislation related to the registration of medical practitioners and the practice of medicine. Together with the Medical Regulations 2017, the Medical Act deals with all disciplinary matters involving registered medical practitioners. If there are transgressions made of the expected norms of practice, it can result in punishment after a due process of inquiry.
The MMC has disciplinary jurisdiction over registered medical practitioners and will exercise it over anyone who has, for example, committed serious professional misconduct as outlined in the Code of Professional Misconduct or any other guidelines issued by the Council. Serious professional misconduct here refers to ‘a failure to meet the minimum standards of professional medical practice’ and ‘sufficiently immoral or outrageous or disgraceful character’. When a complaint is made in accordance with the Act, it is forwarded to the Complaint Management Committee (CMC), which comprises five council members who usually hold office for one year at a time. The CMC scrutinises each complaint, and if it meets their requirements, it is forwarded to a Preliminary Investigations Committee (PIC) and/or Disciplinary Board (DB). The PIC and DB members are selected from the Disciplinary Panel, which comprises council members and/or fully registered medical practitioners with at least ten years of registration under the Council. The Council then reviews the investigation of the mentioned panels and determines the next course of action. Depending on the offence, medical practitioners can be reprimanded, suspended, or struck off the registry. (13)
Case Studies
The pervasiveness of sexual harassment means that everyone and anyone is at risk, regardless of their background. We want to outline two scenarios on different ends of the spectrum of sexual harassment experience in Malaysia, which can help readers understand what survivors have endured. The cases below are based on true stories.
Case Study 1
Prelude
This is about a specialist who viewed her experiences as trivial, though unacceptable and uncomfortable, and led to the experiences being lost in her memory. Recent discussion on the topic sparked her memory of the incident and made her realise the intensity of her experience.
Assault
The survivor has had a few encounters with sexual harassment. Her first encounter was when she was a house officer (intern) doing her surgery rotation at a tertiary hospital. It was the norm for consultants to shout at surgeons during ward rounds and surgeons to regularly shout at medical officers (MOs) and house officers (HOs). However, stories of sexual harassment were rarely heard of or spoken about. There were, however, frequent rumours of surgeons pairing up with medical officers and house officers or fraternising outside work.
She assisted a surgeon in the operating theatre one day with a scrub nurse present. While the surgery was progressing, the surgeon asked her personal questions that made her uncomfortable. She was startled to be asked whether she had a boyfriend. Despite stating having one, he further asked whether she would go out clubbing and dancing during the weekends. She replied uncomfortably, ‘Not really …’, but was startled to get his statement that he would like to see her dancing and see her moving. ‘I felt very uncomfortable then and did not respond to his remarks. I looked pleadingly to the scrub nurse who was present for a reaction, but she appeared not to have noticed what had happened and was absorbed in her work.’
Her subsequent encounter was as a post-graduate trainee doing hospital rotations. She was assigned to an internal medicine ward and described her working experience as enriching but challenging sometimes. She enjoyed working with most of her colleagues in the department, who were supportive and willing to teach. One physician was exceptionally attentive and helpful. Although he was not the physician in charge of the ward, he occasionally came to the ward to help do rounds when the physician in charge was unavailable. He was professional in his conduct with patients and other staff. Still, the trainee noticed that he paid more attention to her and often asked her how she was coping in the posting and how she was doing her studying sessions outside the hospital premises.
He asked her personal questions, such as whether she was single and how often she travelled back home to her hometown. He even offered to coach her privately over lunch or dinner outside work. On a few occasions, he asked her if he could travel with her back to her hometown whenever she planned to. She felt strange about the inquiries and the offers since they were not close to begin with. She declined all his requests as she felt uncomfortable and suspicious of his intentions. In addition, it was known that he was married with a child, and his family was based in another state. A more unacceptable behaviour occurred a few times during ward rounds where he would put his hand on her shoulder or back while saying, ‘it’s ok, don’t worry’. Not knowing how best to react, she pretended not to notice as these incidents were in front of patients. She was confused about whether he was trying to be friendly, but she did know that his behaviour made her increasingly uncomfortable.
Limbo
The survivor related,
I wondered if I should do anything about it like reporting but did not do so because I felt that I did not have enough evidence to proceed with any report or enough basis. I did feel uncomfortable, confused about what to do next and afraid of the repercussions that I might face making a report against a surgeon. I was worried that my progression through the posting would be jeopardised. So, I brushed it off and continued to work as usual. I worked closely with that surgeon in doing rosters for house officers but kept a cautious distance during that period. I wanted to keep that incident locked away in the past.
In the second incident, as a trainee, she confided in another MO about her situation. She discovered that the perpetrator did have a history of similar behaviour with other MOs who were no longer in the posting. The other MO offered to inform the physician in charge of rosters not to slot her and the physician together in future. She faced no further problems throughout the duration of that posting.
Exposure
The survivor, in this case, did not encounter any issues when disclosing the incidents to others. Not many people knew of the incidents, as she revealed the details to a few close friends who were her colleagues in the concerned departments. She thought of the incidents as trivial, not realising at the time that she experienced sexual harassment. She believed there was insufficient concrete evidence to justify making a report and felt uncomfortable dealing with any scrutiny. Until now, she questioned herself if she had done something to provoke these advances. Her strategy was to go under the radar and continue working without causing fuss or disruption.
Aftermath
The survivor is now a specialist at a local university, and the incidents she experienced did not appear to hamper her career progression. She is, however, more empowered now and intends to work towards creating a safer working environment for other health care workers, such as working with this book chapter.
Case 2
Prelude
Case 2 involved a compilation of events experienced by ten survivors with a history of sexual harassment from a similar perpetrator and received national coverage in 2018. The information was retrieved from newspaper reporting and those handling the case, including officials who investigated the case. None of the survivors agreed to be interviewed when approached by a third person who assisted their case.
Assault
This case was a high-profile case involving a senior orthopaedic consultant who was also the head of the department (HOD) at a tertiary-level hospital. The perpetrator had a long-standing reputation for sexually harassing new house officers in his department, but complaints were either not made or did not make it to investigations by higher authorities. (Reference Zainal and Chung14) The perpetrator was a very senior consultant and a very influential and well-connected person in his discipline. House officers (HOs) who were exposed to his misconduct were terrified of making any official complaint for fear of being penalized. They are concerned that the heads of departments, who are responsible for deciding whether the HOs have completed a posting successfully, may discriminate against them. Failure to successfully complete any postings would then disrupt their career progression.
A survivor’s account was reported in the Star newspaper, where she was summoned to meet the HOD in his office. She said,
He then grabbed me and started to unbutton my shirt and kiss my lips. He said he was going to give me his ‘blessings’. I pushed him away and ran out of the room. I was shocked and depressed; I was disgusted.
Another HO detailed her account where she received advances during work and spotted a dark vehicle parked outside her apartment for an extended period. The HOD had texted her, saying he had found out where she lived and was waiting for her outside. (Reference Zainal and Chung14)
Limbo
The sexual harassment incidents had spanned many years, but many HOs who were affected did not come forward to complain. This changed when one of those affected did come forward to make an official complaint at the institution. The discussion spiralled into the national agenda when it came to the attention of the Ministry of Women, Family and Community. This Ministry then alerted the Ministry of Health and the then Minister of Health ordered an immediate investigation into the case. This resulted in several other HOs coming forward to make official complaints.
Exposure
Those affected grappled with all the possible outcomes of making a complaint, such as the HOD not signing them off to the next posting or receiving an unsatisfactory report resulting in a permanent blemish in their personnel files. In this case, no police reports were initially made. Some who did lodge reports within the organisation were left disappointed by the inaction. When news of the reports had broken, the perpetrator was told to go on leave and more survivors stepped forward with reports of his transgressions. (Reference Radhi15; 16)
An independent inquiry body was formed to investigate the matter. As the HOD was put on leave, he drafted a letter of support addressed to the inquiry body vouching for his good character and noting that under his leadership, his department achieved an excellent track record and that he was respected by many. He then pressured specialists, medical officers (MOs) and nurses in his department to sign it, going to the extent of identifying who had not done so and personally contacting them to request their signatures. (Reference Zainal and Chung14)
Aftermath
Based on the interviews with investigators, many of those who came forward had left the medical fraternity. They considered the challenges they faced, and decided they couldn’t focus on their job after such an ordeal. We were informed that at least one of the doctors has not recovered from the impact of the experience and is still receiving ongoing psychological support. The fate of those who went through similar experiences but did not lodge complaints is unknown.
There was also collateral damage in this case. After one month of investigations by the independent inquiry, the body recommended that the HOD be suspended from his duties. When investigations were completed months later, the HOD was terminated in all services upon the consent of the King of Malaysia. At around the same time, specialists from the same department were informed that the entire department (including fourteen specialists, twenty-five MOs and fifteen paramedics) would be getting transfer letters to different hospitals. Questions to top officials for reasons of the en-masse transfer were met with responses like, ‘It was to dismantle the toxic environment’, ‘the department was guilty by association and inaction’ and ‘it was collateral damage’. The transfer plan was eventually shelved after much opposition. (Reference Foon Fong17)
Discussion
Sexual harassment is everywhere. Even health care workers are not protected against it; worse still, in Malaysia, it remains hidden. The two cases discussed earlier highlighted the diversity of sexual harassment experiences and the different ways of responding to the situation. We believe that many more doctors are affected by sexual harassment but have decided to keep silent about it given the challenges towards help-seeking and disclosure. Unfortunately, good quality data on the prevalence of sexual harassment in Malaysia is scanty and practically non-existent for medical professionals.
Medical Fraternity
Sexual harassment seems to be a commonplace occurrence in the medical fraternity but is not usually reported. This was until a high-profile case came into light involving an eminent and senior orthopaedic surgeon who was also the head of his department at a leading tertiary-level hospital in the country. A house officer had lodged a formal complaint against him for sexual harassment, and the Ministry of Women’s Affairs raised the alarm and called for an investigation. It was then that the Ministry of Health opened investigations into the wrongdoings of the surgeon. This triggered a domino effect which saw several other junior doctors coming forward with complaints of harassment by the surgeon dating back several years.
While it was good that investigations into this surgeon had finally begun, it begged the question of why it took the intervention by not one but two ministries to initiate investigations. A system already exists for incidences such as this, but it was not utilised in this case(s). Another question raised is what the role of the surgeon’s hospital is in dealing with harassment. Were no complaints made at all to the hospital authorities? There appear to have been weaknesses in a system that should have functioned to provide a safe space for employees. There is also an apparent lack of deterrents in an existing system, which ideally should be built into the reporting system, the investigation processes, the provision of support for the survivor/perpetrator, and the actual redress or inquiry.
Several factors involving the health care environment may explain the reluctance of victims of sexual harassment to come forward. What was noted in the cases reported is that perpetrators of harassment are usually in a more senior post than the victim. Junior doctors are typically reliant on the assessment of senior doctors to progress within a posting and on to other postings. Hence, when harassment happens, junior doctors may be reluctant to lodge a formal complaint in writing for fear of jeopardising their careers. Compromises in a junior doctor’s career can range from minor actions such as not being included in the operating theatre for critical surgeries, to more major ones, like receiving a failing grade in an end-of-posting exam. It is this hierarchical nature of the medical community, the existence of ‘senior’ and ‘junior’ doctor labels, and fear of consequences to their careers that causes its members to enable predatory behaviour in a way to ‘save their necks’. To further aggravate this is the issue of power dynamics in the workplace, which is prevalent in the Malaysian working culture. Hofstede’s Power Distance Index was developed to measure power distribution between individuals in a business, culture, or nation. Malaysia scored the highest in this among countries all over the world, which means that Malaysia has the most significant power distance between employers and employees. (Reference Hofstede18) Hence, it is not surprising that junior doctors would be hesitant to call out harassing behaviour by their seniors.
The medical fraternity exists within a relatively small circle. This means that even when transfers occur due to disciplinary problems, there is still the tendency for a victim to run into a perpetrator later, as the circle is a small one. Another question that has arisen is whether the workplace is a safe space considering the potentially many (unreported) cases of harassment or bullying. Is there any safeguarding in place and is it given priority in the health care system? If there is a written policy in place, it is essential to ensure that the policy gets implemented. Looking back at these cases, awareness about sexual harassment and ways of getting help may need to be addressed. Junior doctors go through an orientation process when they begin their careers, and awareness of sexual harassment may be a useful component to add to their training.
Survivors
We examined how victims from two different perspectives dealt with their situations and how they ultimately carried on with their careers and lives. In the first case, the survivor experienced relatively minor but still significant encounters of sexual harassment. While instinctively knowing that something was off but unsure if what she was experiencing was sexual harassment, she went into survival mode and got out of the situation(s) by saying ‘no’ in a good-natured way by laughing it off rather than stating it assertively. It is not unusual for survivors to face confusion about the types of behaviours that fall into the category of sexual harassment and the perceived severity that warrants legal action. In contrast, the survivors from the second scenario suffered for months or years in fear and shame until one of them took a fateful step to lodge a report. While the public classifies the case as a triumph as the perpetrator was eventually found guilty and punished, with his practising licence revoked, this could not reverse the damage faced by survivors. The perpetrator is still a free man and was not convicted under a court of law for his crime because none of the survivors were keen to make a police report.
Ideally what should have been done in both cases was to immediately document in writing either in a book or electronic device what had transpired and with whom, when and if there were any witnesses present. The next step would be to report their experiences to a higher authority. That higher authority would then be responsible for investigating or appointing someone suitable to do so before appropriate action is taken. The survivor should then take note of the action taken by the investigating authorities, where keeping a timeline of events would be helpful.
In the short term, talking to someone, albeit a friend or counsellor, would help immensely in relieving a huge burden and getting clarity. This is provided when an appropriate response is given. Ignorance of others on sexual harassment matters can cause harm when the listener invalidates the experiences with reactions such as ‘you are being so sensitive’, discouraging the survivors from pursuing further action and speaking up. There is also the issue of normalising certain seniors’ ‘acceptable behaviours’, leading to a workplace culture of sexual harassment.
All health care workers should familiarise themselves with the available protocols (if any) for sexual harassment. While making a report is the idealistic approach to dealing with an encounter of sexual harassment, it is important to consider several issues that have plagued the minds of our survivors here. Firstly, the time between making a report and eventually taking action can be lengthy. As if the incident of harassment were not traumatising enough, the victim would be subjected to reliving the episode repeatedly while making the report and during the investigation. To top that off, victims often face retaliation in the form of intensified bullying as their perpetrators roam freely and blame victims. Victims often get blamed for the harassment they experience and are accused of provoking the attack in the first place.
On the other hand, when a report is made, action is not always taken. This is mainly the case when the perpetrator is in a position of power and influence. Hence, not only is no action taken to reprimand the perpetrator, but the victim is placed in an even more vulnerable position. The perpetrator, being a HOD, can exert power by not allowing the victim to complete the rotation within the department, jeopardising the completion of housemanship, which is compulsory to be confirmed in service.
The organisations here have an essential role in ensuring the workplace’s safety for all. Its policy in supporting its employees needs to be clear and solid. It also needs to take reports of sexual harassment seriously and take the necessary steps to investigate them and take action. This will ensure that all health care professionals feel safe at the workplace and act as a deterrent to perpetrators of sexual harassment. This would add further value to the organisation in the long run. These organisations (clinics, hospitals, ministries) would not be able to function without good leaders. Leaders need to place appropriate emphasis on sexual harassment, and politicians need the political will to emphasise the implementation of the newly approved Anti-Sexual Harassment Bill. (19)
Legal Issues
An issue with reporting sexual harassment is the high burden of proof that falls on the victims. Sexual harassment is, unfortunately, usually difficult to prove in the absence of physical evidence such as bruises or witnesses. Often the victims look like their complaints were made based on misunderstandings. There are also limitations in the availability of current legal remedies. The definition of sexual harassment itself is not very clear under Section 509 of the Penal Code, where it is stated ‘to insult the modesty of any person’ and ‘intrudes upon the privacy of such person’. (20) There is also no specific coverage of online sexual harassment in the Communications and Multimedia Act of 1998. (21)
There is also limited coverage of situations in the workplace. The Employment Act 1955 only applies to employers and employees in Peninsular Malaysia. (22) The Public Service Department Circular also mentions sexual harassment but is only restricted to the workplace in the public sector. Apart from that, there is an absence of legally mandated obligations by the public and private sectors to establish in-house policies and mechanisms to prevent and address sexual harassment. Presently, the Code of Practice on the Prevention and Eradication of Sexual Harassment only recommends that employers set up policy statements prohibiting sexual harassment in the organisation, protective and remedial measures (including complaint measures), as well as educational programmes (including training) to raise awareness of sexual harassment at all levels within the organisation. (19)
When a case goes to court, hearings are often time-consuming and expensive. The processes deprive survivors of their privacy. There is also a high burden of proof on the victims of sexual harassment as it is complicated to prove, and judges have to ascertain beyond reasonable doubt that the case is indeed one of sexual harassment. It is not surprising that many victims do not come forward due to this and the possible repercussions where the perpetrators do not usually get more than a rap on the wrist. Monetary compensation is only possible if a civil suit is to be pursued under the tort of sexual harassment. While this is not the most effective form of a deterrent for some perpetrators as it can be quickly paid off, it is also not what victims often seek, such as an apology or acknowledgement from the perpetrator that an offence has been committed.
Conclusion
While the topic of sexual harassment is an ongoing discussion, there is still reluctance among victims to come forward for action to be taken against perpetrators. This is despite regulations being in place and being improved over time. The closely linked medical fraternity should provide a safe space for all its members and not be seen as a challenge for disclosure of any forms of abuse. The Ministry of Women, Family and Community Development is the ministry responsible for the implementation of the Anti-Sexual Harassment Act. (Reference Nasri23) They are now doing roadshows to create awareness and provide information on the Anti-Sexual Harassment Act to the public, especially on the roles and responsibilities of individuals and companies. We trust more people will become aware of the issue of sexual harassment and will be able to take appropriate action with the implementation of this new Act.

 Open access
Open access