

Key messages
Chapter 1.1 discusses the use of taxes and social health insurance (SHI) contributions. A key objective of health financing is to redistribute financial resources from the healthy to the sick and from the well-off to the poor. This can be best achieved through compulsory prepayment mechanisms like general taxes and social contributions. Key learning includes that:
A high reliance on public revenue-raising instruments (general taxes and/or SHI) is essential to progress towards universal health coverage (UHC).
Large informal economies and poor governance can make collecting public revenues difficult in low- and middle-income countries.
Health financing systems have to be able to adapt to:
○ offset challenges to the revenue base such as economic decline, low levels of economic development or a preponderance of informal employment or economic activity; and
○ meet increasing health care demands which grow with rising expectations and population ageing.
The traditional distinction between health systems that rely on general taxation (Beveridge or National Health Service (NHS) systems) and social insurance contributions (Bismarck or SHI systems) has blurred with time.
Health systems increasingly rely on a diverse mix of revenue-raising instruments to finance health care.
There is a growing focus on delinking employment from entitlement to services in historically SHI-based systems and on emphasizing general taxation as a complementary source of revenues.
Introduction
The objectives of this chapter are to describe global trends in countries’ use of general taxation and SHI to finance health care and, by taking relevant country examples, to highlight some of the key challenges that governments face in raising public revenues for health as well as some of the solutions.
General taxation and SHI
Public funding of health systems is crucial to promote financial protection and improve access to services. The two dominant styles of publicly financing health care are general taxation and SHI – collectively referred to as public revenue-raising modalities – which enable health systems to move away from reliance on private out-of-pocket (OOP) spending at the time and place of seeking care. Financing health systems from OOP spending is both inefficient and inequitable, exposing individuals and households to financial risk when seeking care, including the risk of deeper impoverishment, as well as contributing to foregone care. Under general taxation, revenue comes from the share of overall government resources apportioned to the provision of health care. Under SHI, on the other hand, revenues are raised in the form of contributions from mandatory earmarked payroll taxes. The nature of health services – the presence of externalities, information asymmetries between providers and patients, the need for protection from the financial burden of unanticipated health spending, common public good elements, lack of competition in the hospital sector, information failures, etc. – is such that overdependence on unregulated private financing inevitably leads to suboptimal outcomes, including from the perspective of equity (Arrow, Reference Arrow1963).
Compulsion and redistribution
Well-designed health financing systems ensure that there is some form of mandatory prepayment combined with redistribution for funding health. Compulsion and redistribution are key elements of public financing for countries to make progress towards UHC, i.e. where everyone can access the essential health services they need without facing undue financial hardship in the process of doing so (Fuchs, Reference Fuchs1996; WHO, 2010; Kutzin, Yip & Cashin, Reference Kutzin, Yip, Cashin and Scheffler2016; Tandon & Reddy, Reference Tandon and Reddy2021). Critically, this involves risk pooling from the healthy to the sick as well as from the well-off to the poor via progressivity in prepayments. Although some countries implement this by mandating the purchase of private health insurance with targeted subsidies for those who cannot afford premiums, most countries have made progress towards UHC using public financing, i.e. via general taxation and SHI (Kutzin, Reference Kutzin2012). Voluntary health insurance (VHI) plays a complementary or supplementary role but is not the primary mechanism for financing UHC globally, while funding from external sources including development assistance plays a role, particularly in lower-income settings (see chapters 1.3 and 1.4).
The health financing transition
In general, as countries grow and develop, overall levels of funding for health increase along with the share that comes from public sources, thus decreasing reliance on OOP and external financing. Across low- and middle-income countries (LMICs), this empirical trend – dubbed “the health financing transition” – brings with it the challenges of raising obligatory contributions for health care, whether as general taxes or mandatory SHI contributions (Fan & Savedoff, Reference Fan and Savedoff2014). These challenges include low levels of economic development, high levels of poverty and informal economic activity, difficulties in collection of taxes, institutional and governance-related weaknesses and a low priority ascribed to, and poor absorption of, allocations for health in government budgets (World Bank, 2016). In high-income countries (HICs), on the other hand, governments are contending with the problems of an ageing population: rates of participation in the labour force are declining, so necessitating general tax infusions for SHI systems as contribution bases shrink, while at the same time the demand for and costs of health care are rising, thus raising issues of the existing systems’ long-term sustainability (Stadhouders et al., Reference Stadhouders2019; OECD, 2015).
The rest of the chapter is laid out as follows. First, we elaborate on the definitions of public financing for health, general taxation and SHI in particular, and examine how each relates to principles of equity and efficiency and where their boundaries have blurred. Next, we summarize the global landscape and trends in public financing for health across countries. Then, we outline key challenges facing public financing for health across the different income groupings of countries and some of the solutions.
General taxation and SHI: how countries use them to raise revenues
High-performing health financing models for UHC can be characterized as those where financing levels are adequate, prepaid funds are pooled in order to spread the financial risks of ill health and spending is efficient and equitable. These characteristics ensure the desired levels of effective service coverage and financial risk protection for all people, and provide a system that is both resilient and sustainable (World Bank, 2019a). In general, the overall objectives of public financing are considered to be the provision of public goods as well as to address market failure, redistribute resources and stabilize the impact of business cycles. In the case of the health sector, expansion of public financing constitutes the means by which most countries have made progress towards UHC, including the elements of compulsion and redistribution that are inherent in such a financing modality, though – in a few cases – countries have instead implemented mandates and subsidies for purchasing private health insurance.
General taxation: definition
Under general taxation, revenues for health come from apportioning a share of overall government resources to the provision of health care, either for the entire population or for specific population subgroups such as the poor and vulnerable (Gottret & Schieber, Reference Gottret and Schieber2006). This type of general tax-financed public delivery system is often referred to as the Beveridge model, named after William Beveridge, the economist whose ideas underpinned the introduction of the United Kingdom’s NHS in 1948. Even earlier than this, in the 1920s, a similar, though more centralized and hospital-focused system of universal coverage had been introduced in the Soviet Union, known as the Semashko model, after health care commissar, Nikolai Semashko.
The term general taxation is often used interchangeably with general government revenue financing, although in fact the latter is more accurate since government funding typically comprises both tax and non-tax sources. For example, general taxation financing also includes both general and sector-specific borrowing by the government. Tax revenues are defined as “compulsory, unrequited” payments to the government; unrequited because the benefits received from government spending are usually not proportional to the amount paid in taxes (OECD, 2021). Tax revenues are further classified into two broad categories, direct and indirect. Direct taxes – for example, taxes on income, profit, wealth and property – can be adjusted based on the characteristics of the payer, but cannot be shifted to another taxpayer. Indirect taxes, in contrast, are paid on transactions that are independent of the characteristics of the payer – for example, taxes on consumption, including sales taxes, value-added tax (VAT), excise taxes and import tariffs; these can, at least in part, be shifted to other taxpayers. Non-tax revenues typically comprise sources of funds other than from taxation: for example, from external grants, rents or royalties from natural resources such as oil, gas and other commodities, as well as profits from state-owned enterprises.
SHI: definition
Under SHI, revenues for health are raised in the form of contributions from a mandatory earmarked payroll tax (Wagstaff, Reference Wagstaff2010; Yazbeck et al., Reference Yazbeck2020). Payment of this mandatory contribution secures entitlement to health care, and it is this quid pro quo payment-for-entitlement that is one of the key differences between SHI and general taxation modalities for raising revenues for health. SHI contributions are generally imposed on wages and are paid by both employers and employees of firms as well as by those who are self-employed. Hence, due to the way revenues are collected, there is typically a link between employment status and entitlement. Under SHI financing, funds are pooled, and service providers are paid prospectively or retroactively on behalf of contributors for utilization of health care services; in some countries; for example, in Costa Rica, the SHI agency that collects and pools contributions also owns and manages service delivery via its own network of providers (OECD, 2017a). Contribution rates are usually set based on actuarial analysis of estimated costs and projected utilization rates. An SHI system is also sometimes referred to as the Bismarck model, named after Otto von Bismarck, Chancellor of Germany, who introduced it there in 1883.
Overlapping approaches to public financing in health
General taxation and SHI contributions are often collectively referred to as public sources of health financing given that they both constitute mandatory prepayments for health care and the fact that management and administration of these funds is usually undertaken by government or quasi-public agencies. Some countries – including the Netherlands (Kingdom of the)Footnote 1 and Switzerland – mandate that citizens purchase private health insurance; despite the presence of this mandate, revenues raised thus are managed and administered by private entities and, hence, are not considered to be public sources of financing. The latest System of Health Accounts (jointly produced by the Organisation for Economic Co-operation and Development (OECD), Eurostat and the World Health Organization (WHO)) eschews categorizing revenue-raising modalities for health in terms of public versus private; instead, the distinctions are based on whether revenues are: (i) compulsory or voluntary; (ii) domestic or external; and (iii) prepaid or OOP (Jowett & Kutzin, Reference Jowett and Kutzin2015; OECD, 2017b). For the remainder of this chapter, we follow others in the literature and take health’s share of general government expenditure – financed by domestic revenues, borrowing, external grants and mandatory SHI contributions, but excluding resources raised via compulsory private insurance prepayments – to represent the overall public financing envelope for health (WHO, 2020).
General taxation and SHI versus principles of equity and efficiency
A key issue is who contributes to and who benefits from a publicly financed health system. One policy objective for such a system is that it should be equitable, with those most able to pay shouldering the heaviest burden of the costs (so in effect redistributing resources from the well-off to the poor). However, obligatory contributions to public funds such as general taxes and SHI can be either progressive or regressive. While progressive payments are defined as those where the well-off pay a generally higher share of their income, a regressive payment is one where the poor pay a higher share of their income relative to the well-off. Generally, direct taxes – on income, property, wealth – are progressive. Indirect taxes – for example, taxes on consumption – are generally regressive. However, governments need to consider not just equity in payments linked to any instrument, but also the possible yield in terms of revenue generation, as well as the cost of collection. They also have the option to compensate for regressivity in any given instrument in two ways: making another instrument more progressive or compensating the poor using transfers in cash or kind from the revenue that is raised. In that sense, progressivity in terms of revenue generation of any particular instrument is not greatly relevant: the equity of the financing system needs to be assessed in terms of the distribution across individuals of net benefits, i.e. the payments into the system overall, including for health, net of what they receive as benefits in cash or kind (and not just health benefits) (Kaiser, Bredenkamp & Iglesias, Reference Kaiser, Bredenkamp and Iglesias2016; Jellema, Wai-Poi & Afkar, Reference Jellema, Wai-Poi and Afkar2017; World Bank, 2018).
Efficiency in how government revenues are raised is another key consideration in public finance, including for health. All taxes introduce distortions to economic activity by creating a gap between what a buyer pays and what a seller receives. Not only does this cause welfare losses, if not offset or balanced by externalities, but it can also adversely impact resource allocation decisions. In addition, some forms of tax collection themselves can be costlier to administer than others. Well-designed tax systems typically aim to reduce the economic inefficiencies that are inherent in any form of taxation, be progressive and broad-based in their incidence (ideally with minimal exemptions and loopholes) – and be relatively easy and cost-effective to administer.Footnote 2
Several countries, mostly high income, that originally financed their health provision by means of SHI systems subsequently abolished them – usually out of concerns for equity or as part of more general political reforms – and replaced them with tax-financed systems (Saltman & Dubois, Reference Saltman, Dubois, Saltman, Busse and Figueras2004). For instance, the United Kingdom absorbed its existing system of SHI when it transitioned to general tax financing in 1948. Norway abandoned its SHI system in 1967, followed by Denmark in 1973. Political transitions furthermore resulted in the removal of SHI and replacement by tax financing for health in Greece, Italy, Portugal and Spain. Conversely, many countries that started out with solely tax-financed health systems later introduced SHI, sometimes as a way to reduce financial pressure on existing tax-financed public delivery systems, but without dismantling them – in particular, in eastern and central Europe. In many countries – for example, in India (see Box 1.1.1), Nigeria, Myanmar and others – both general taxation and SHI financing systems coexist in parallel, but covering different population subgroups.
India’s tax-financed public delivery health system is universal, accessible to all and loosely modelled on the United Kingdom’s NHS. It also has several supplementary noncontributory and contributory SHI schemes.
Pradhan Mantri Jan Arogya Yojana (PM-JAY): Noncontributory tax-financed hospitalization coverage scheme for the poor and near-poor which was introduced in 2018 and targets the bottom 500 million of India’s population.
Central Government Health Scheme: This covers current and retired central government employees and their dependants, giving them access to public and designated private facilities.
Employees’ State Insurance Scheme: For lower-income workers of private firms with 10 or more employees.
One advantage of general taxation over SHI is that the former is more broad-based and, hence, assumed to be more resilient and less volatile as a source of public financing. However, this is not always the case. This purported advantage of general taxation as a source of financing can be lost during economic downturns when public revenues decline significantly, especially in the absence of automatic stabilizers and countercyclical policy responses (Maresso et al., Reference Maresso2015). General taxation financing is also subject to political vicissitudes and competition for resources from other sectors, which can add to elements of unpredictability (Wagstaff, Reference Wagstaff2010). Although SHI revenues are also not immune to economic crises, in some countries – for example, Estonia during the 2008/2009 economic downturn – SHI reserves can help stabilize volatility and other challenges to short-term revenue-raising pressures. In general, a move towards a diversified revenue base appears to offer the best prospects for mitigating some of these challenges.
Over time, distinctions between the SHI versus the general taxation public financing models have blurred, so much so that they have lost several core characteristics that initially differentiated them (Yazbeck et al., Reference Yazbeck2020; Mathauer, Saksena & Kutzin, Reference Mathauer, Saksena and Kutzin2019). Included under the umbrella of general taxation financing modalities are situations in which governments impose additional taxes on income or consumption specifically for health, whether or not these are earmarked at source or for use (or both), although payment of these earmarked taxes is usually not a prerequisite for entitlement to health care. At the same time, SHI systems are increasingly dependent on cofinancing via general taxation, either due to prevalence of informal economic activity or the impact of an ageing population. Where governments subsidize contributions – for example, if SHI contributions are fully or partially subsidized for the unemployed, the poor and pensioners – these are classified and analysed as cofinancing via general taxation even if they are paid out by SHI schemes. Several general tax-financed health funding models now include elements that were previously considered to be hallmarks of SHI-financed systems, such as having a clear separation between purchasers and providers, explicit and well-defined benefits packages, use of non-traditional provider payment mechanisms, as well as the purchasing of services from both public and private providers.
It is important to note that the way revenues are raised in health systems can have significant implications for the pooling function of health financing; for example, if resources are raised and pooled separately by geographical areas or – as is sometimes the case under SHI – by industrial affiliation. This is addressed elsewhere in the book (see Chapter 2.1); for the remainder of the chapter, we focus primarily on issues and challenges related to revenue generation via public financing.
Amount and modality of health funding versus country income level
Globally in 2019, the latest year for which data from WHO’s Global Health Expenditure database were available at the time of writing, levels of per capita health spending – from all sources of financing, not just public – ranged from lows of <US$ 25 in Burundi, the Democratic Republic of the Congo, Madagascar and South Sudan to highs of >US$ 8000 in Norway, Switzerland and the USA. Although these differences are not adjusted for variations in purchasing power of currencies across countries – for example, US$ 1 buys more in low-income countries (LICs) than it does in HICs due to cheaper labour and other costs – the contrast in absolute levels of health spending across countries is nevertheless staggering. Differences are less stark when comparing health spending as share of gross domestic product (GDP). In 2019, health spending among LICs averaged 5.2% of GDP (US$ 35 in per capita terms), compared with 11.4% (US$ 5644 per capita) among HICs (Table 1.1.1).Footnote 3 Average levels of health spending vary significantly across income classifications, but the way health is financed also differs significantly. Public financing for health predominates among upper-middle-income countries (UMICs) and HICs. Among HICs, 67% of spending on health in 2019 came from public funding (34% of the latter, on average, from SHI contributions). Among LICs, on the other hand, only 37% (US$ 12) of funding for health came from public sources (with only 2% of the latter from SHI contributions); this number reduces to 22% if external financing that is channelled via government budgets is excluded (see Chapter 1.4). Private OOP spending is the largest source of funding for health among LICs and LMICs, accounting for 40–52% of health spending. Globally, VHI is not a significant source of financing, contributing only 6% of resources for health. Other private sources – for example, from faith-based organizations, other nongovernmental organizations (NGOs), external financing not channelled via government – are included in the “Other” category inTable 1.1.1.
| Indicators | Low-income countries | Lower-middle-income countries | Upper-middle-income countries | High-income countries | All countries |
|---|---|---|---|---|---|
| Current health spending per capita (US$) | 35 | 97 | 555 | 5 644 | 1 138 |
| Share of GDP (%) | 5.2 | 3.6 | 5.9 | 11.4 | 5.8 |
| Public share of current health spending (%) | 37 | 36 | 55 | 67 | 47 |
| Per capita (US$) | 12 | 39 | 304 | 3 487 | 681 |
| Share from general taxation (%) | 64 | 83 | 60 | 66 | 72 |
| Share from SHI contributions (%) | 2 | 11 | 40 | 34 | 24 |
| Share from external sources (%) | 33 | 5 | 0 | 0 | 5 |
| OOP share of current health spending (%) | 40 | 52 | 33 | 16 | 39 |
| VHI share of current health spending (%) | 2 | 5 | 9 | 3 | 6 |
| Other (NGOs, etc.) (%) | 21 | 7 | 3 | 14 | 8 |
GDP: gross domestic product; OOP: out-of-pocket; NGO: nongovernmental organization; SHI: social health insurance; VHI: voluntary health insurance.
Note: Averages are population weighted.
General taxation is the main source of financing for health in several countries including Australia, Canada, Denmark, Italy, Norway and the United Kingdom (Fig. 1.1.1). SHI contributions, on the other hand, are predominant in Costa Rica, Croatia, France, Germany and Japan, among others. Blended public financing – a combination of financing via general taxation and SHI – is the largest source of health care funding in countries such as Belgium, China, the Republic of Korea and the Russian Federation. General taxation and SHI contributions account for less than half of current health expenditures in most LMICs including; for example, in Bangladesh, Brazil, Egypt, Ethiopia, India, Pakistan, the Philippines and Nigeria.
Public financing is a much bigger share of health spending in richer countries
SHI: social health insurance; UK: United Kingdom; USA: United States of America.

Figure 1.1.1 Long description
The x-axis notes General taxation share of current health spending in percentage from 0 to 100, while the y-axis notes S H I contributions share of current health spending in percentage from 0 to 100. A solid straight line moves from (0, 100) to (100, 0), and all countries below this have Public financing of more than 50 percent of current health spending. These countries, from low to high general taxation, include Croatia, France, Japan, Germany, Costa Rica, Belgium, Korea, China, Russia, Mexico, U S A, Canada, Australia, U K, Italy, Denmark, and Norway. Another dashed line moves straight from (0, 50), to (50, 0), and all countries below this have Public financing of less than 50 percent of current health spending. These countries, from low to high general taxation, include Nigeria, Indonesia, Egypt, Bangladesh, the Philippines, India, Pakistan, Brazil, and Ethiopia.
There is an inverse correlation between public spending on health as share of GDP and the OOP spending share in current health expenditures across countries (Fig. 1.1.2). Low public spending on health often manifests as poor supply-side readiness and responsiveness at public facilities, resulting in the population having to supplement public financing with private OOP payments for medicines and diagnostics or to seek self-financed care at private facilities. Countries that have made the most progress towards UHC generally have OOP spending levels that are less than 15–20% of current health spending, a threshold benchmark recommended by WHO and met or exceeded in HICs within the Organisation for Economic Co-operation and Development (OECD). In the case of countries that have made progress towards UHC despite their OOP spending being higher than the 15–20% threshold, their OOP outlay largely occurs among well-off segments of the population and therefore is no longer a significant risk factor for impoverishment; for example, in Malaysia and Sri Lanka (WHO, 2010). OOP spending shares are particularly high – exceeding two thirds of all spending on health – in sub-Saharan African countries such as in Cameroon, Nigeria and Sudan, as well as in several central Asian and south Asian countries such as Armenia, Azerbaijan, Bangladesh, Tajikistan and Turkmenistan.
OOP falls as public spending grows: the inverse relationship between public versus OOP spending on health, 2019
GDP: gross domestic product; USA: United States of America.

Figure 1.1.2 Long description
The x-axis notes Public expenditure on health as share of G D P in percentage from 0 to 10, while the y-axis notes Out-of-pocket spending as a share of total health expenditures in percentage from 0 to 100. The best-fit line gently curves from about (0.5, 60) to (9, 10). Countries on the low end of public expenditure include Armenia, Bangladesh, Turkmenistan, Cameroon, Azerbaijan, Sudan, India, Pakistan, Ethiopia, Indonesia, and Brazil. Countries on the upper end include South Africa, U S A, and Japan.
Over time, health expenditures have typically risen faster than rates of economic growth, i.e. the unconditional income elasticity of health spending has exceeded unity. Between 2000 and 2019, for instance, there was a secular (long-term) increase in spending on health, both in levels and as share of GDP: for example, per capita spending levels on health increased globally from US$ 713 (5.1% of GDP) in 2000 to US$ 1138 in 2018 (5.8% of GDP). Higher levels of current health spending – and a changing composition of financing away from OOP and external sources towards a greater share coming from public sources – is also notable over time (Fig. 1.1.3). These empirical trends – dubbed the health financing transition – are driven by a range of factors (Fan & Savedoff, Reference Fan and Savedoff2014). Some influence the overall quantum of health spending, while others impact the way in which health systems are financed. The faster growth in health expenditure is partly because people demand more and better services as they get richer. Other influences are population ageing and the associated changes in disease patterns to costlier chronic conditions; the continuous availability of new and often more expensive medicines and health technologies; and a range of public or private choices made around revenue generation, pooling and purchasing of health care.Footnote 4
Spending has increased across the board but patterns of spending have evolved differently in low-, middle- and high-income countries
OOP: out-of-pocket; SHI: social health insurance; VHI: voluntary health insurance.

Figure 1.1.3 Long description
Each chart has an x-axis marking the Year from 2000 to 2018, while the y-axis notes the Constant 2019 U S dollar from 0 to 50. The 4 charts, representing the 4 income groups, are Low income, Lower-middle, Upper-middle, and High income. The expense areas are: general taxation, S H I, external (via government), external (non-governmental), O O P, V H I, and others. General taxation and O O P take up most of the expenses cross all categories, which also notes higher spending trends over the years. The lower-middle and high-income groups show the highest total spending.
The health financing transition reflects what happens on average as countries move up the income ladder. There are important differences, though, across countries and many factors can shape the timing and magnitude of the transition and the extent to which it poses a policy challenge, especially in LMICs. For example, despite rapid economic growth and its transition from LIC to LMIC status in 2015, external financing in Myanmar subsequently increased (not decreased, as might be expected) as a share of health spending (Teo & Cain, Reference Teo and Cain2018). Several countries in the Pacific – including the Solomon Islands, Kiribati and Vanuatu – have relatively low OOP shares in health spending, in contrast to other countries at similar levels of income. In UMICs such as Armenia, the OOP spending share has remained stubbornly high and has been increasing over time despite economic growth (Dudu et al., Reference Dudu2021).
General taxation and SHI: key challenges and country responses
In this section, we examine the challenges posed to the public financing of health, in particular: countries’ levels of growth and poverty; countries’ often weak overall generation of revenue; high rates of informal economic activity; popular resistance to making SHI contributions; conflicting budgetary priorities; and ageing populations. We also include current responses to these challenges: reform of the tax system, blurring and diversifying revenue bases, earmarking new revenues and raising the pension age.
Challenge: Levels of economic growth and poverty
In most countries the overall size of the economy in per capita terms is a key constraint in terms of public financing, including for health. Economic activity is the basis of most forms of taxation, whether taxes are imposed with or without a quid pro quo intent. Countries that have experienced high levels of economic growth generally see levels of public financing for health also increasing at faster rates. India is a case in point: although levels of public financing for health remain far below those expected for its income level, relatively high economic growth rates have resulted in almost a tripling in real public financing for health in India in per capita terms since 2000 (Tandon et al., Reference Tandon2020). Conversely, countries on a lower growth trajectory – for example, Brazil, Mexico, Nigeria, and the Russian Federation – have faced a more constrained environment for public financing for health. Beyond the effects of economic growth, public spending for health is also a function of government revenues as well as the share of government budgets that flow to health (Tandon & Cashin, Reference Tandon and Cashin2010). Lower levels of economic development are also associated with high rates of absolute poverty; hence, even if institutional mechanisms for collecting taxes exist (which often they do not), the ability of the poor to pay such taxes remains a constraint. In addition, ageing not only causes an increase in demand for health but also lowers the tax base as people retire. (We discuss both ageing and the tax system in more detail in the Challenge: Governments’ conflicting budget priorities and the Challenge: Ageing populations sections).
Weak revenue generation
Weaknesses in revenue generation overall are a key challenge facing public financing of health, especially in LMICs. Lower-income countries tend to have lower levels of government revenue as a share of their economies. In 2019, whereas in HICs average general government revenues, both from taxes and non-tax sources, were 38% of GDP, in LICs this number was only 19%, even when external grants are included (Fig. 1.1.4).Footnote 5 Although countries can to some extent borrow to increase spending beyond the revenues received, repayment of debt can constrain future expenditure, especially if nominal economic growth rates are lower than the cost of borrowing (Blanchard, Reference Blanchard2019). Even within country income groups, there are some countries that lag behind in terms of government revenue collection: for example, in 2019, the general government revenue share of GDP was <10% of GDP in countries such as Bangladesh and Nigeria and only between 10 and 15% of GDP in Democratic Republic of the Congo, Ethiopia, Indonesia and Pakistan, therefore constraining the ability of their governments to publicly finance spending across all sectors, including health.
General government revenues are a small proportion of GDP in lower-income countries
GDP: gross domestic product.

Figure 1.1.4 Long description
The y-axis notes the Share of G D P (percentage), from 0 to 50, while the x-axis notes the 4 income groups. Each bar has 3 stacks, representing Tax revenues, Non-tax and other revenues, and Deficit, with tax revenues being the largest share across each. The approximate net revenues across the categories are: Low income: 21 percent. Lower middle: 30 percent. Upper middle: 32 percent. High income: 40 percent.
Response: reform of the tax system
International Monetary Fund (IMF) research has recently suggested a benchmark of at least 15% for the tax revenue share of GDP if countries are to make sustained and inclusive progress on development outcomes (Gaspar, Jaramillo & Wingender, Reference Gaspar, Jaramillo and Wingender2016). But how can countries that have low rates improve tax revenues? A systematic assessment across LMICs found 55 episodes of tax revenue increases during the period 2000–2015 that resulted in an annual increase of at least 0.5% of GDP and that lasted a minimum of three years. In most cases, a combination of tax policy and revenue administration reforms were employed. Increases in rates of indirect taxes and broadening the base for both direct and indirect taxes – in addition to simplification, increasing compliance and elimination of tax exemptions – were found to be key in most cases (see Box 1.1.2) (Akitoby et al., Reference Akitoby2020).
At the time of its so-called Rose Revolution in 2003, Georgia’s tax revenues as a share of GDP were only 12% due to evasion and corruption. Tax reforms – including simplification of the system, curbing exemptions, introduction of flat income taxes for individuals and corporations, a small reduction in the VAT rate and electronic reforms that made it easier to pay taxes – resulted in a sustained increase in tax revenues. In 2008, within just five years of implementing its reforms, Georgia’s tax revenue share of GDP had doubled to 24% (Akitoby, Reference Akitoby2018). As a result, public spending on health expanded from 1.2% to 1.6% of GDP during the period 2003–2008, despite a decline in health’s share of overall government spending over the same period.
Similar reforms led to an increase in tax revenue collection and public spending on health in several other countries including Cambodia, Guyana, Liberia and Ukraine.
Challenge: Informal economic activity
In LICs and LMICs, large and persistent levels of informality in the labour market and in the economy more generally makes collection of taxes – especially direct taxes on income, wealth and property – particularly challenging (e.g. tax revenues as a share of GDP are only 8% in the Democratic Republic of the Congo and 10% in Ethiopia). Recent estimates indicate that whereas one third of GDP on average across LMICs is informal activity output – i.e. market based and legal but unobserved or hidden from public authorities for monetary, regulatory or institutional reasons – more than two thirds of all employment tends to be informal (Ohnsorge & Yu, Reference Ohnsorge and Yu2022; Schneider, Buehn & Montenegro, Reference Schneider, Buehn and Montenegro2010). Informality is often a consequence of poor government enforcement capacity as well as evasive strategies by firms and labourers to avoid (possibly burdensome) taxation and regulation.Footnote 6 There are wide variations underlying these averages: in some lower-income countries with large agricultural sectors and widespread subsistence farming, estimated informal employment exceeds 80%. In addition to its association with agriculture and farming, informal employment is also prevalent among the self-employed or those employed in small firms with relatively few employees. By definition, informal employment occurs without contracts and without formal payroll arrangements.
The challenge of pervasive informality also makes SHI an impractical and ineffective revenue-raising modality for LMICs aiming to make rapid progress towards UHC (Yazbeck et al., Reference Yazbeck2020). When workers lack formal contracts, labour income cannot be taxed directly. This helps explain the relatively tiny share of SHI contributions in financing health in LICs and LMICs (see Table 1.1.1).
Challenge: Resistance to SHI contributions
Many LICs and LMICs have SHI schemes but they tend to cover a small proportion of the labour force: usually civil servants and those employed in the formal private sector. Even for the latter, imposing the mandate for payment of SHI contributions has often been difficult. For example, Nigeria’s SHI programme for the formal sector covers approximately 1.5% of the population, the majority of whom are civil servants. The almost exclusive source of revenue is the employer contribution from the federal government for the civil servants (3.25% of the consolidated salary), while the collection of employee contributions has proven to be politically impossible (World Bank, 2019b). HICs have also faced challenges in maintaining their SHI systems when stakeholders are opposed to contributing because of concerns about rising labour costs and implications for competitiveness.
Response: blurring and diversifying revenue bases
Reluctance on the part of stakeholders to contribute to SHI schemes has led many countries to subsidize and co-finance SHI programmes with revenues from general taxation, notably Belgium and France. In the context of high levels of informality, concerns about competitiveness and an ageing population, many countries are moving towards delinking income-related contributions from entitlements and diversifying sources of earmarked taxation away from income (Kutzin, Yip & Cashin, Reference Kutzin, Yip, Cashin and Scheffler2016).
France and Hungary have diversified revenue bases for their SHI systems, for example. The United Kingdom collects earmarked National Insurance contributions on income from employers, employees and self-employed individuals and part of these revenues are used to provide about one fifth of NHS’s financing; the remainder comes from general taxation (Cylus et al., Reference Cylus2015). Given its significant levels of informal economic activity, Ghana co-finances its SHI fund using earmarked revenues that are levied on consumption – as part of its VAT – in addition to SHI contributions levied on formal sector income (Government of Ghana, 2015). The introduction of India’s tax-financed noncontributory health insurance programme for the poor and near-poor in 2018 that covers almost 500 million individuals was used as a means for the central government to raise a cess – basically, an additional 1% tax on all income taxes paid – although the funds are not strictly earmarked for the programme and most of the beneficiaries of the scheme are not the ones that pay income taxes since almost all of them are poor and in the informal sector (Government of India, 2018).
In some countries, the health sector has been actively involved in lobbying for taxes on “harmful” products such as tobacco, alcohol and products with added sugar, in order to deter their consumption and reduce the subsequent burden of disease on the sector, while also expanding the overall public resource envelope (even if the revenues thus raised are not earmarked for health). Given the growing ill health burden resulting from air pollution, carbon taxes are another possible area where the health sector can seek to raise revenues and reduce the risk of disease, as demonstrated by the experiences of some HICs (World Bank, 2019a). The challenge from a fiscal-space-for-health perspective – as opposed to a fiscal-policy-for-health perspective – is the amount of resources generated by adopting such a strategy and whether they can be earmarked and, if so, whether over time such resources are truly additional. As discussed further below, the Philippines is a recent example of a country that has used earmarked tobacco and alcohol taxes to finance health care contributions on behalf of the indigent and thus create a fiscal space for health (Kaiser, Bredenkamp & Iglesias, Reference Kaiser, Bredenkamp and Iglesias2016).
Challenge: Governments’ conflicting budget priorities
A key challenge – especially in LMICs – is that health is accorded a relatively low priority in government budgets, for a variety of reasons: other sectors’ demands for financing, perceptions that the health sector is inefficient or is unable to absorb allocated funds, or ideologically driven political narratives that favour private over public versus private financing for health. Globally, health’s share in overall public spending stands at about 9% (WHO, 2022). However, there are very large variations across countries: on the one end, health accounts for less than 3% of public expenditure in countries such as Cameroon and South Sudan; on the other hand, health exceeds 20% of public expenditures in other countries such as Costa Rica, Japan, Panama, Uruguay and the USA. Despite large country-specific variations, health’s share of government budgets is, on average, higher in HICs (Table 1.1.2). Health care costs tend to be higher in richer countries, driven by relative price differences as well as the availability of higher-technology care. Richer countries also tend to have more educated and ageing populations with preference structures that expect higher levels of public financing for health. Education tends to receive a higher share of government budgets across LICs, LMICs and UMICs; only in HICs does health’s share end up being higher than education’s, on average. Although both interest payments on debt and military spending represent the same or lower share than health on average, there are notable country-specific exceptions such as Armenia, Bangladesh, India, Morocco, Pakistan, Sri Lanka and Uganda where health receives a lower share vis-à-vis both interest payments and military spending.

Table 1.1.2 Long description
The table has 2 main columns (and further subcolumns): Classification and Share of government expenditure (Health, Education, Military, and Interest payments, all in percentage). It reads as follows. Low-income country: 9; 16; 7; 5. Lower-middle-income country: 6; 15; 8; 15. Upper-middle-income country: 10; 13; 5; 5. High-income country: 18; 13; 6; 4. All countries: 9; 14; 7; 9.
Response: earmarking new revenues
Earmarking of new revenues is often implemented to increase health’s share of the overall public financing envelope. Earmarking is when revenues are assigned through constitutional or statutory law from certain sources to specific expenditures (McCleary, Reference McCleary1991; Bird & Jun, Reference Bird and Jun2005). Apart from the standard case of SHI, different types of earmarks for health have emerged or gained popularity over the past two decades. Earmarks take different forms, with various attempts to categorize them based on the rationale, source of revenue, expenditure category and the revenue–expenditure link. The revenue–expenditure link may be tight, i.e. the amount spent is restricted to the amount raised through the earmark, or soft, i.e. the amount spent is loosely related, if at all, to the amount raised. In practice, many earmarks fall between these two extremes of strength of link. From a sector perspective, two classes of earmarks are of special interest as in both the earmarked revenues are substantial, i.e. they are a prominent source of funding.
Increased rates or new indirect taxes
The first class comprises cases of increased rates or the introduction of entirely new indirect taxes to finance the expansion of health care coverage beyond formal workers and their dependants. The most notable examples include Ghana (a 2.5% increase in VAT in 2004) and the Philippines (additional revenue generated from a comprehensive reform of tobacco and alcohol taxes in 2012). Other countries are emulating the approach. For example, Egypt, as part of a comprehensive overhaul of its SHI system, introduced earmarks on additional revenue from tobacco tax reforms and new levies on toll roads, drivers and car licenses to complement compulsory, individual contributions (Government of Egypt, 2018). Lessons from Ghana and the Philippines highlight the potential advantages of a soft revenue–expenditure link (Cashin, Sparkes & Bloom, Reference Cashin, Sparkes and Bloom2017). In both instances, tax reforms generated substantial amounts of funding for the extension of SHI: more than 0.5% of GDP. However, in the Philippines, even in the medium term, additional revenues exceeded the funds that the SHI agency managed to absorb (Ulep, Pargas & Alcantara, Reference Ulep, Pargas and Alcantara2021). In contrast, in Ghana, from year three onwards, additional revenues fell far short of operational expenditures (Kurowski & Iglesias, Reference Kurowski and Iglesiasin press).
Designated fixed shares for health in budget allocation
The second class of earmarked revenues comprises fixed shares for health in the allocation of general funds. Such fixed shares have been reported by more than a dozen countries. In decentralized systems, fixed shares for health have not only been established at the central level, but also in transfers from central to subnational governments, as well as for lower levels of government, to ensure the overall level of expenditure is adequate but also to reduce spending inequalities. Some countries use this type of earmark for specific expenditure categories – for example, Nigeria does so for its basic health care provision fund and South Africa for its HIV/AIDS programme. The fixed shares typically reflect only a minimum level of spending. As they fall short of actual spending needs, countries have combined them with other types of earmark.
But do these substantial earmarks affect spending levels in the targeted expenditure categories and ultimately in the health sector? In the absence of a counterfactual, this question is difficult to resolve. Country experiences suggest that there may be a short-term effect on government expenditures. For example, in Ghana, the size of the earmark correlated in the early years after its introduction with increases in the level of government spending on health (Kurowski & Iglesias, Reference Kurowski and Iglesiasin press). With time, however, the likelihood increases that allocations from general taxes are reduced. These cuts may lead to a shift in expenditure priorities with potential consequences for the efficiency of spending. In Ghana, for example, concerns have been raised that priority services outside SHI benefits – for example, immunization services – took a hit.
More generally, empirical work on prioritization has been sparse: the limited cross-country econometric analyses that exist suggest that factors such as democratization, lower levels of corruption, ethnolinguistic homogeneity and more women in public office are correlated with higher shares of public spending on health; however, these findings are not robust and are sensitive to model specification (Lebovic, Reference Lebovic2001; Meltzer & Richard, Reference Meltzer and Richard1981; Keefer & Khemani, Reference Keefer and Khemani2005; Tandon et al., Reference Tandon2014). A range of factors – political changes, disease outbreaks/pandemics, macroeconomic shocks – are common triggers that can sometimes lead to a sustained increase in health’s share of a government’s budget. The use of budgetary or numeric financing targets (e.g. the Abuja Declaration target that health’s share of the government budget be at least 15%) generally has not resulted in a higher priority for health. Evidence to date suggests that country-specific political economy considerations are key and that results-focused reform efforts – in particular efforts to explicitly expand the breadth and depth of health coverage as opposed to efforts focused only on government budgetary and numerical targets – are more likely to result in a sustained and politically feasible prioritization of health.
Challenge: Ageing populations
Another key policy challenge – particularly among UMICs and HICs – is that of an ageing population. With higher life expectancies and declining fertility has come a growing proportion of the population that is elderly with greater needs for health spending and long-term care. Some UMICs are seeing higher median ages resulting from declining fertility alone, even without registering significant improvements in life expectancy. United Nations estimates place the total number of people aged 65 years and above at 727 million in 2020, about 9% of the global population; this number is expected to more than double – to 1.5 billion, 16% of the global population – by 2050. In 2020, several countries such as Brazil, China and Mexico were already classified as “ageing”, i.e. with a population share of people aged more than 65 years over 7%; the Russian Federation and the USA counted among “aged” countries – with a population share of people aged more than 65 years exceeding 14% – and Japan was already “super-aged” with a share of the population aged more than 65 years of more than 21% of its total population (United Nations, 2020).
From a revenue generation perspective, the immediate risks from ageing are rising old-age dependency ratios – i.e. increasing numbers of those aged over 65 years relative to those in the working age population group aged 15–64 years – such that even if the size of the working age population is growing, it is having to provide a resource base for public financing for health and other services for a dependent population of people aged more than 65 years that is growing at an even faster rate. Elderly populations tend to have greater rates of multimorbidity from noncommunicable diseases (NCDs) than younger, working populations and need integrated care, which currently is provided in a fragmented manner across most countries. This rise in old-age dependency is already occurring in nearly all countries – albeit at different rates – and the trend is expected to accelerate in coming decades, especially in HIC. According to the United Nations’ projections, by 2050, the proportion of those people aged more than 65 years will be almost three quarters the proportion of those in the working age population group in Japan; this same old-age dependency ratio will exceed 35% in China, Brazil, the Russian Federation and the USA.
Although rising over time, the old-age dependency ratio in 2050 is expected to remain 10% or below in lower-income countries such as Ethiopia and Nigeria (Fig. 1.1.5). In some countries such as China, Japan and the Russian Federation, the rise in old-age dependency is occurring on top of an ongoing decline in the working age population of 15–64 years old. With ageing comes the potential for declining labour productivity and, when combined with a shrinking labour force, the possibility of reductions in investments and economic output. These trends can have adverse knock-on effects on public financing including for health, increasing the need for additional public spending while at the same time reducing the ability of governments to raise revenues as (generally lower) pension incomes replace (generally higher) labour incomes. Tax revenues tend to be highly correlated with the size of the employed population rather than with the size of the total population (Rouzet et al., Reference Rouzet2019). For lower-income countries, the challenge of ageing is that it is likely to occur at a rate that is faster than underlying rates of economic development, i.e. many of these countries will become old before they become rich.
Old-age dependency ratios are projected to increase in many (middle- to higher-income) countries
USA: United States of America.

Figure 1.1.5 Long description
The y-axis shows the Old-age dependency rate in percentage from 0 to 80, while the x-axis lists the countries. Each country has 4 serially higher dots, representing current and projected ratios from 2020, 2030, 2040, and 2050. They increase as follows. Nigeria and Ethiopia: all projections stay below 10. Pakistan: 6 to 15. Egypt: 8 to 16. Philippines: 9 to 19. India: 9 to 20. Bangladesh: 9 to 22. Indonesia: 9 to 23. Mexico: 10 to 28. Brazil: 12 to 38. U S A: 18 to 28. Russia: 21 to 40. China: 25 to 44. Japan: 49 to 77.
Response: strategies to offset the impacts of ageing on revenues
There is growing empirical evidence that suggests the impact of ageing on health spending might not be as high as expected. Although ageing is associated with higher prevalence of multimorbidities and greater rates of utilization of health care, the impact is not as dramatic as that of other drivers of health spending such as technological innovations (Greer et al., Reference Greer2021). Moreover, countries could cope with some of the challenges of reduced revenue generation due to ageing by implementing corrective policies. Many HICs have raised the mandatory retirement age in line with rising life expectancies to increase the potential labour force while at the same time decreasing old-age dependency ratios. In Portugal, for example, the mandatory retirement age now automatically increases by two thirds of any increase in life expectancy. Similar approaches have been adopted in Denmark, Finland, Italy, the Netherlands and elsewhere. Simply raising the mandatory retirement age, however, may not be sufficient to induce older people to work: such policies would need to be combined with other incentives including flexible working arrangements and designing older people-friendly workplaces. A recent systematic review of the literature did find evidence, though, that raising the mandatory retirement age increased labour force participation rates among older people (Patrick, Groot & Pavlova, Reference Patrick, Groot and Pavlova2021).
As outlined above, other options include diversification of the revenue base by increasing taxes on consumption and wealth rather than relying on wage-based income alone. For example, although France’s SHI system was initially almost entirely funded from wage-based payroll contributions, these now account for only about half of the system’s revenues. The remainder is financed by an earmarked income tax – levied on all sources of income – along with taxes on tobacco and alcohol, the pharmaceutical industry – and VHI (Commonwealth Fund, 2020). The shift to a broader definition of taxable income in France has also decreased inequities in revenue generation as richer individuals not only tend to be older but they also have higher wealth-related income (World Bank, 2019a). Similarly, Hungary’s SHI system is now a hybrid: transfers from general taxation are just as important a revenue source as payroll-based contributions, potentially enhancing the sustainability of health financing in the light of ageing (Szabolcs et al., Reference Szabolcs2019).
Policy relevance and conclusions
This chapter has landscaped revenue raising for health via public financing – both general taxation and SHI – with an understanding that the compulsory and redistributive elements of this source of financing have been key for making sustained progress towards UHC. Public financing for health is predominant among HICs where key challenges faced include those of sustainability, diversification of revenue sources (especially where SHI is prevalent) and cost containment in light of demographic, epidemiological and technological trends. Among lower-income countries, on the other hand, the key challenge is navigating and accelerating the transition from predominantly private OOP financing of health systems towards greater levels and effective use of public resources for health. Lower-income countries that have successfully made the transition to expanding public financing for health have done so by means of expanding general taxation through a combination of economic growth, improving government revenue generation and increasing the share for health in government budgets, and by targeting spending towards the poor (Cotlear et al., Reference Cotlear2015).
We underscore the view that SHI financing for health is, in essence, earmarked taxation of wages and, over time and across countries, we are seeing a blurring of institutional and other differences between systems that were previously separately classified as general tax-financed models of health financing versus SHI-financed. Several general tax-financed health financing systems now include elements – for example, strategic purchasing of health services and a purchaser-provider split – that were previously considered to be hallmarks of SHI-financed systems. And SHI-financed systems are increasingly becoming dependent on complementary general tax-financed sources, especially for subsidizing financing of health care coverage for the poor, unemployed and retired populations. In some HICs, stakeholders oppose raising SHI contributions because of concerns about rising labour costs and implications for competitiveness. Such constraints have led many countries to subsidize and co-finance SHI programmes with revenues from general taxation. In such environments – with high levels of informal economic activity, competitiveness concerns and an ageing population – countries should consider delinking income-related contributions from entitlements and diversifying sources of earmarked taxation away from income (Kutzin, Yip & Cashin, Reference Kutzin, Yip, Cashin and Scheffler2016). The challenge of pervasive informality makes SHI an impractical and ineffective large-scale revenue-raising modality in LMICs (Yazbeck et al., Reference Yazbeck2020).
Globally, it is increasingly evident that expansion in general taxation, more so than SHI, has been central for precipitating health financing transitions as well as for making and sustaining progress towards UHC. Although SHI financing remains part of the revenue-generating arsenal to varying degrees depending on country context, the global policy dialogue is increasingly centred around constraints and opportunities related to diversifying revenue sources, delinking employment from entitlement and moving towards a more central role for general taxation as the core source of public financing for health.Footnote 7
Key messages
Chapter 1.2 assesses community-based health insurance (CBHI). CBHI is a voluntary, self-organized approach to financing health care for groups of individuals in the absence of other forms of health care coverage. CBHI scheme members organize themselves, collect and pool their insurance premiums, and use them to purchase health services for members. Key learning includes that:
CBHI is not a miracle solution to affordable access to health care:
○ the very poor often do not enrol, and when they do, they tend to use fewer health services;
○ out-of-pocket (OOP) payments are not necessarily reduced.
Low uptake, poor delivery of promised benefits and challenges around governance undermine the impact of CBHI.
CBHI does not overcome broader issues, such as a lack of financial resources.
CBHI might serve as a transitionary mechanism towards universal health coverage (UHC) and offer some financial protection for the most vulnerable provided that:
○ policy-makers create a supportive political and economic environment;
○ social capital can be mobilized;
○ schemes are institutionalized within the health sector.
Introduction
CBHI is one of many terms used to describe small-scale schemes which aim to provide financial protection for individuals when they seek medical care.Footnote 1 Community members organize themselves, collect and pool their insurance premiums, and use these to purchase health services for their members. Traditionally associated with settings where health care is not publicly funded or provided universally, CBHI schemes apply the same principles used in formal health insurance – in particular, resource pooling, prepayment and risk sharing – and adapt these to local social contexts.
CBHI’s proponents advocate for its use on two main grounds. Firstly, it can provide an additional or alternative form of revenue-raising in low- and middle-income countries (LMICs) without a robust tax base and the institutional capacity to collect either taxes or insurance premiums effectively. Secondly, in the absence of universal public provision of health care, CBHI has the potential to overcome the financial barriers to accessing health care put up by formal private and social health insurance (SHI) schemes (see chapters 1.1 and 1.3). In particular, these formal schemes tend to exclude rural and informal sector workers and those with an irregular income or none. In many LMICs, those excluded constitute over three quarters of the population and the members of this already vulnerable group – often the most affected by ill health – are left without any form of financial protection from its effects (Donfouet & Mahieu, Reference Donfouet and Mahieu2012).
CBHI schemes are intended to provide financial protection, cushioning households from potential poverty occasioned by catastrophic health care costs (Haddad et al., Reference Haddad2012; Rosner et al., Reference Rosner2012). They reduce members’ vulnerability to health-related financial shocks by eliminating dependence on OOP payments at the point of health service utilization. Pooling risks across members enrolled in the CBHI scheme reduces the financial burden among the members, as they do not have to incur financial costs to receive health services (see Chapter 2.1). The removal or reduction of financial barriers is intended to increase access to health care and prevent absolute poverty among beneficiaries (Donfouet & Mahieu, Reference Donfouet and Mahieu2012).
Some advocates of CBHI go further, suggesting that its implementation is a plausible option for countries seeking to achieve United Nations Sustainable Development Goal 3.8 of UHC, including financial protection (Seventieth United Nations General Assembly, 2015; Qin et al., Reference Qin2019; van Hees et al., Reference van Hees2019). International development agencies are leading the narrative that CBHI holds potential as a transitionary mechanism for UHC and many LMICs now include CBHI in their strategies towards UHC (Mladovsky & Mossialos, 2008).
Countries vary in their definition of CBHI, however. In its purest form, CBHI is defined as a form of micro health insurance (Donfouet & Mahieu, Reference Donfouet and Mahieu2012), which is distinguished from other health financing structures by five key characteristics: (i) voluntary enrolment; (ii) prepayment of premiums; (iii) community ownership and participatory management of the schemes; (iv) solidarity, with membership not tied to risks and an emphasis on inclusivity; and (v) non-profit, with the primary goal being supporting members to assure the community’s health status (Atim et al., Reference Atim1998; Criel et al., Reference Criel, Heggenhougen and Quah2008; Michielsen et al., Reference Michielsen2010; Soors et al., Reference Soors2010). However, in the case of some of the schemes held up as the success stories of CBHI, for example, in Ghana and Rwanda, enrolment is mandatory (among other differences), so their status as exemplars of CBHI is questionable (McIntyre et al., Reference McIntyre2008; Witter & Garshong, Reference Witter and Garshong2009).
In this chapter, we look in more detail at how CBHI works and its impact, the challenges in implementing it, the preconditions required for its success (including a brief case study of CBHI as implemented in Senegal), and assess CBHI’s potential as a transitionary mechanism to UHC. First, however, we examine the nature and origins of the financial barriers that CBHI is intended to overcome.
Financial barriers to accessing health care
Since the 1980s, in response to structural adjustment programmes (SAPs) imposed by the World Bank and the International Monetary Fund, LMICs have introduced a series of health financing reforms to generate revenues for the health sector (Helleiner, Reference Helleiner1983).
Initially, these reforms created a health care market, allowing for the introduction of user charges and the establishment of an insurance market, for both public (i.e. social) and private health insurance. Anyone wishing to access health care was therefore required to pay the user charges either by means of their health insurance or “OOP”, i.e. with their own money. Unfortunately, the quantification of health as an economic good as envisioned by the proponents of such reforms was, and remains, far removed from the realities of many of the countries where SAPs were imposed. Their realities include an economic and financial base which is too low to support individual OOP payments, a fiscal capacity too limited for governments to subsidize much of the population and similarly limited capacity to pool resources from the large informal economy (Helleiner, Reference Helleiner1983).
In practice, targeting mechanisms for both social and private health insurance exclude rural and informal sector workers and those with an irregular or no income at all from coverage (Donfouet & Mahieu, Reference Donfouet and Mahieu2012). Excluded households must instead pay user charges for their health care via OOP payments, which have been described by some as “the worst form of health care financing conceivable” (Rosner et al., Reference Rosner2012; Qin et al., Reference Qin2019) (see Chapter 2.4). Many are unable to pay and, unprotected by health insurance, therefore are faced with an insurmountable financial barrier to accessing health care.
An overwhelming body of evidence confirms the negative effects of this form of financing on the utilization of health services and population health outcomes (Ridde, Reference Ridde2015; Leone et al., Reference Leone2016; Ponsar et al., Reference Ponsar2011; Qin et al., Reference Qin2019; Tahsina et al., Reference Tahsina2018; Watson et al., Reference Watson, Wroe and Dunbar2016). Further, it is now widely acknowledged that health service user fees are incompatible with UHC. Faced with health care costs, uninsured households either opt to forgo or postpone access to medical care, or resort to borrowing funds or selling household assets to meet the costs (Leive & Xu, Reference Leive and Xu2008; McIntyre et al., Reference McIntyre2006; Nguyen et al., Reference Nguyen2012; Rosner et al., Reference Rosner2012; Sangar, Dutt & Thakur, Reference Sangar, Dutt and Thakur2019; Tahsina et al., Reference Tahsina2018).
It is unsurprising that attempts to institutionalize reforms such as user fees at a national level have not yielded the desired impact – i.e. increased health revenues, greater access to health care and improved health outcomes (Ridde, Reference Ridde2015). Since the 1990s, then, many LMICs have looked to CBHI schemes as a way of overcoming the financial barrier faced by so many when in need of health care.
Diop and Ba (Reference Diop and Ba2010) highlight four forms/levels of financial exclusion which characterize population groups likely to be without both public insurance and SHI (Diop & Ba, Reference Diop and Ba2010; Soors et al., Reference Soors2010): (i) total exclusion – those who are unable to pay for health care services due to economic inability to do so; (ii) temporary exclusion – those who are unable to pay for health care services at the time of need and therefore opt to postpone care; (iii) seasonal exclusion – those who may be seasonally excluded owing to cash flow constraints resulting from the nature of their work, such as farmers dependent on harvests; and (iv) partial exclusion – individuals who may not be able to cover part of their treatments. Therefore, theoretically CBHI mechanisms can fill a gap and offer health services and financial protection to individuals and households thus excluded, in particular those totally excluded (group i) and those seasonally excluded (group iv).
How CBHI works
The simplicity of CBHI designs, affordability by group members with flexible premiums and payment options and the community-based nature make CBHI schemes attractive. Their flexibility in design allows for different types of health insurance dependent on a community’s specific set-up and needs. The schemes are often linked to a social, family, ethnic or community group or health care provider (Alkenbrack, Jacobs & Lindelow, Reference Alkenbrack, Jacobs and Lindelow2013; Fadlallah et al., Reference Fadlallah2018; Musau, Reference Musau1999; Nshakira-Rukundo, Mussa & Cho, Reference Nshakira-Rukundo, Mussa and Cho2021). Members often share residence; for example, a village or groups of villages in the same locality or neighbourhoods or other geographical and administrative boundaries. Some are user-initiated or local health care provider-initiated schemes, as is the case in Uganda (Basaza, Criel & van der Stuyft, Reference Basaza, Criel and Van der2010) and India (Devadasan et al., Reference Devadasan2006), or schemes initiated by microfinance institutions, as in Kenya and India (Devadasan et al., Reference Devadasan2006; Musau, Reference Musau1999), cooperative movements and nongovernmental organization (NGO)-led schemes (Aggarwal, Reference Aggarwal2010; Devadasan et al., Reference Devadasan2010; ILO, 2008; Kamau & Njiru, 2014; Yap, 2003).
The groups organize themselves in a voluntary capacity to pool resources, allocate these and purchase needed health services for their members. The community agrees the premiums and the range of benefits covered, which may be linked to the level of contribution. Premiums are paid in cash or kind, with some schemes designing payment to coincide with the availability of the means to do so; for example, following a harvest (Preker et al., Reference Preker2001). By pooling both risks and resources from involved communities, members are responsible for ensuring the viability of the scheme (Criel et al., Reference Criel, Heggenhougen and Quah2008; Soors et al., Reference Soors2010).
Externally sponsored CBHI schemes
Since the 1990s, CBHI has been seen as the way to extend social health protection, with multiple experiences in LMICs. Interest in CBHI (re)intensified after 2015 when United Nations’ Member States adopted UHC, including financial risk protection, as part of Sustainable Development Goal 3.8.
Most CBHI schemes in Africa and Asia were introduced and supported by external actors; for example, Belgians and the French for CBHIs in west and central Africa. Many started as research projects or pilots, such as in Guinea (Sylla et al., Reference Sylla, Criel and Barry2002), Lao People’s Democratic Republic (Bodhisane & Pongpanich, Reference Bodhisane and Pongpanich2017), government trials, such as in China (Hsiao, Reference Hsiao2001; Wang et al., Reference Wang2005; Yip & Hsiao, Reference Yip and Hsiao2008), the Philippines (ILO, 2004) and Ghana (McIntyre et al., Reference McIntyre2008).
Some were initiated by NGOs, both locally and internationally; for example, the ORT Health Plus scheme in the Philippines (Aviva & Kupferman, Reference Aviva and Kupferman1996) and faith-based institutions, such as the Presbyterian Church of East Africa’s CBHI scheme at Chogoria mission hospital in Kenya (Musau, Reference Musau1999). In Mali, early CBHI schemes targeted specific members of the population; for example, pregnant women (Ndiaye et al., Reference Ndiaye, Richard, Witter and Brouwere2008) while the Bwamanda district hospital scheme in the Democratic Republic of the Congo started in 1986 with funding from the Belgian government which was targeted to health providers (Moens, Reference Moens1990).
In Africa, CBHIs started in, and were more common in, West Africa than the rest of the continent. In Senegal, the first CBHI schemes were trialled during the colonial period from 1910 onwards, but they did not remain in place for long and covered very few people (mostly colonists) (Ridde, Diaw & Béland (2025). The Mutuelle Pharmaceutique de la Sainte Famille Tounouma in Burkina Faso was one of the first, initiated in 1986 (Soors et al., Reference Soors2010). Senegal and Benin followed closely, with other countries in the continent establishing similar schemes albeit with variations in the designs (Atim et al., Reference Atim1998; Criel et al., Reference Criel, Heggenhougen and Quah2008; Musau, Reference Musau1999).
In Asia, CBHIs were piloted primarily in Afghanistan, Bangladesh, India and Nepal (Bhageerathy, Nair & Bhaskaran, Reference Bhageerathy, Nair and Bhaskaran2017; Criel et al., Reference Criel, Heggenhougen and Quah2008; Devadasan et al., Reference Devadasan2010; Soors et al., Reference Soors2010). While CBHIs were mainly designed for and available in rural populations, schemes were also established in Tanzania and Ivory Coast targeting urban populations (Soors et al., Reference Soors2010).
Subsequently, such schemes have been considerably expanded, in particular by government initiatives to subsidize contributions for people who wish to join CBHIs voluntarily, and thus to increase coverage. For example, in Mali and Senegal, the state subsidizes 50% of the annual premiums for the general population. In Senegal, the state subsidizes 100% of premiums for indigent people with varied provisions for other population groups while in Burkina Faso the poorest pay 50% of the premiums (Ridde et al., Reference Ridde2018; Parmar et al., Reference Parmar2014). In 2019, the Senegalese government provided CFA franc 19 billion to cover 50% of the premium costs for 2.84 million general population CBHI members and 100% of coverage for 1.27 million indigent people (Ridde et al., Reference Ridde2018; Daff et al., 2020).
CBHI’s impact: mixed evidence
Evidence on the impact of CBHI is mixed. Some is positive: for example, evidence from the first CBHI scheme in Mali suggested increased coverage across all dimensions, higher hospital utilization rates and a reduction in OOP payments for members compared to non-members (Soors et al., Reference Soors2010). We present here some of the evidence of CBHI’s impact on the level of utilization of health services, equity in using them (i.e. do the poor use them as much as the non-poor?), financial protection and population coverage.
Utilization
On the positive side, affiliation to a CBHI scheme has been associated with increased use of hospital-based health services in countries such as Ethiopia and Senegal (Mebratie et al., Reference Mebratie2019; Joshi et al., Reference Joshi2020; Artignan & Bellanger, Reference Artignan and Bellanger2021), and greater use of preventive services, including insecticide-treated mosquito nets and deworming services in Uganda (Nshakira-Rukundo, Mussa & Cho, Reference Nshakira-Rukundo, Mussa and Cho2021).
Equity
There is positive evidence on equity in Rwanda (Collins, Saya & Kunda, Reference Collins, Saya and Kunda2016) – but questions surround whether Rwanda’s health insurance scheme is CBHI in anything but name; and some evidence of success in Armenia (Polonsky et al., Reference Polonsky2009) and Burkina Faso (Parmar et al., Reference Parmar2014). In most settings, the very poor are still less likely to enrol or to use health services even when enrolled in a CBHI scheme (Parmar et al., Reference Parmar2014). An evaluation of CBHI schemes in Senegal established that while membership increased utilization of services by the non-poor, the schemes had no impact on poor people’s health care utilization and did not protect them against impoverishing catastrophic expenditures (Ly, Faye & Ba, Reference Ly, Faye and Ba2022).
Financial protection
Overall, the evidence on the impact of CBHI schemes on financial protection has been either limited or very modest. A 2015 review of the role of CBHI in 14 Asian and nine African countries established that by reducing OOP payments, current health expenditure, total health expenditure, household borrowings and poverty in the majority of cases, targeted schemes contributed to the financial protection of members (Habib, Perveen &Khuwaja, Reference Habib, Perveen and Khuwaja2016).
Evidence also suggests a reduction in OOP payments for enrolled households in some of the CBHI schemes in Senegal (Jutting, Reference Jütting2003), Burkina Faso (Parmar et al., Reference Parmar2014), Benin (Haddad et al., Reference Haddad2012), Tanzania (Msuya, Jutting & Asfaw, Reference Msuya and Asfaw2007), Rwanda (Lu et al., Reference Lu2012; Saksena et al., Reference Saksena2011) and India (Aggarwal, Reference Aggarwal2010; Devadasan et al., Reference Devadasan2007).
However, CBHI affiliation in China was associated with increased OOP payments and the risk of catastrophic health spending during the period 1991–2003 (Wagstaff et al., Reference Wagstaff2009).
With less than 1.5% of the Guinea population enrolled in a CBHI scheme as of 2006, there was no impact on financial protection and population coverage (Ndiaye, Soors & Criel, Reference 87Ndiaye, Soors and Criel2007).
Population coverage
In 2011, Ethiopia set a target of 80% CBHI coverage by 2020. However, more than a decade later, the national coverage is estimated as 50% with significant variations across the regions (Tahir, Abdilahi & Farah, Reference Tahir, Abdilahi and Farah2022).
Higher rates are reported in Ghana and Rwanda, where management by government officials and mandatory enrolment have transformed community-based schemes into SHI. A strict enforcement of enrolment in Rwanda has led to near-universal population coverage (Chemouni, Reference Chemouni2018). However, with minimal enforcement in Ghana, the expected coverage has not been attained (Kwarteng et al., Reference Kwarteng2019) and remains at under 40% (Salari et al., Reference Salari2019).
Next we turn to the challenges in implementing CBHI schemes that help to explain why their overall impact so far is disappointing.
Challenges to implementing CBHI
Many CBHI schemes have collapsed after initial pilot phases or are struggling due to an array of factors, ranging from discontinuity of funds, heavy dependence on external funding for survival, limited government involvement, lack of trust and non-affordability of premiums, to broader health system issues such as the inaccessibility of health facilities (Bennett, Reference Bennett2004; Criel & van Dormael, 1999; Kigume & Maluka, Reference Kigume and Maluka2021; Muchabaiwa et al., Reference Muchabaiwa2017; Fadlallah et al., Reference Fadlallah2018; Waelkens et al., Reference Waelkens2017; Umeh, Reference Umeh2018; Atinga, Abiiro & Kuganab-Lem, 2015). As already mentioned, Francophone west African countries have witnessed decades of trials and large-scale deployments of CBHI – yet they still fail to cover and protect many people in the informal sector, especially in rural areas (Ridde et al., Reference Ridde2018). Indeed, while seeking to provide a solution to the problems of exclusion from health care and financial protection, CBHI brings with it its own set of challenges – in particular, low uptake, inadequate benefits packages and issues of governance – as well as having to contend with broader health system issues. We explore each of these challenges briefly below.
Challenge 1: Low uptake
The uptake of CBHI schemes remains limited in many settings. A core barrier to increasing uptake of CBHI is the limited ability of people in the informal sector to pay for premiums (Adebayo et al., Reference Adebayo2015). High poverty levels, lower education and the resultant limited purchasing power among households preclude the sustainability of CBHIs (Fadlallah et al., Reference Fadlallah2018; Shewamene et al., Reference Shewamene2021; Umeh & Feeley, Reference Umeh and Feeley2017; Adebayo et al., Reference Adebayo2015). Evidence also points to a lack of awareness or limited understanding about health insurance generally, and CBHI specifically, which leads to poor uptake among communities (Alkenbrack, Jacobs & Lindlelow, Reference Alkenbrack, Jacobs and Lindelow2013; Cofie et al., Reference Cofie2013; Kigume & Maluka, Reference Kigume and Maluka2021; Noubiap et al., Reference Noubiap2013; Shewamene et al., Reference Shewamene2021). The limited uptake of CBHI schemes is also considered to be a function of the lack of supportive regulatory frameworks, and interpersonal, community- and system-level conflicts in horizontal and vertical relationships (Atim et al., Reference Atim1998; Alkenbrack, Jacobs & Lindlelow, Reference Alkenbrack, Jacobs and Lindelow2013; Bennett, Reference Bennett2004; Carrin, Waelkens & Criel, Reference Carrin, Waelkens and Criel2005; Purohit, Reference Purohit2014) (see the Challenge 3: Issues with governance section).
Challenge 2: Inadequate benefits poor delivery
The benefits expected with CBHI membership are not always delivered. For example, in one scheme in the Democratic Republic of the Congo, while all costs were covered in theory, hospitals did not recognize CBHI cards (Soors et al., Reference Soors2010). As a result, patients incurred significant OOP costs while accessing care, defeating the purpose of their CBHI membership. Similarly, in Bangladesh, the level of financial protection offered by the CBHI schemes often did not sufficiently protect households from incurring catastrophic health expenditures (Werner, Reference Werner2009). Perceived poor quality of health services and frequent medication stockouts have also been documented (Criel et al., Reference Criel2020; Kigume & Maluka, Reference Kigume and Maluka2021). In part, CBHI’s failure to deliver is a function of its low uptake: small-scale CBHI pools with very limited risk sharing present a serious organizational challenge (see Chapter 2.1), and the poor delivery of services then further discourages uptake.
Challenge 3: Issues with governance
CBHI issues with governance are both internal, related to the schemes’ community base, and external, related to the quality and level of support they receive from outside agencies, including other parts of the health system, local and national government and NGOs (i.e. both horizontal and vertical linkages).
Internally, the weak managerial capacity in many CBHI schemes is attributed to the community ownership and management of the structures (Atim et al., Reference Atim2001; Basaza, Criel & van der Stuyft, Reference Basaza, Criel and Van der2007; Kigume & Maluka, Reference Kigume and Maluka2021; Mladovsky, Reference Mladovsky2014). By excluding non-members from their management and decision-making, CBHI schemes can lack necessary input from management experts, as well as health professionals (Soors et al., Reference Soors2010). Lack of trust in CBHI leadership and among fellow members has also been associated with low enrolments and dropouts of previously enrolled members (Alkenbrack, Jacobs & Lindelow, Reference Alkenbrack, Jacobs and Lindelow2013; Fadlallah et al., Reference Fadlallah2018; Muchabaiwa et al., Reference Muchabaiwa2017; Ozawa & Walker, Reference Ozawa and Walker2009; Rao et al., Reference Rao2009; Shewamene et al., Reference Shewamene2021). The communal membership, which would otherwise be a strength, instead becomes a risk.
Externally, researchers have pointed out that some CBHI schemes are disconnected from the local health systems (Alkenbrack, Jacobs & Lindelow, Reference Alkenbrack, Jacobs and Lindelow2013; Bousmah et al., Reference Bousmah2021; Mladovsky, Reference Mladovsky2020). The non-recognition by hospitals of CBHI cards in the Democratic Republic of the Congo, as described above, constitutes a prime example (Soors et al., Reference Soors2010).
Government support for CBHI schemes includes establishing a regulatory framework within which CBHIs can operate, monitor, coordinate and manage the schemes (but stopping short of mandating enrolment and transforming CBHI schemes into SHI). However, overall, the lack of, or often-limited, political buy-in has been highlighted as a major challenge facing CBHIs (Basaza, Criel & van der Stuyft, Reference Basaza, Criel and Van der2010; Purohit, Reference Purohit2014; Uzochukwu et al., Reference Uzochukwu2009). There have been attempts to create and adopt legislative frameworks within which CBHIs can operate in countries such as Mali, Senegal and Togo (Barry, Reference Barry, Waelkens and Criel2007; Diop & Ba, Reference Diop and Ba2010; Letourmy & Ouattara, Reference Letourmy, Ouattara, Dussault, Fournier and Letourmy2006). In India, a policy supporting the development of health insurance programmes encourages the involvement of community-based organizations in pro-poor risk pooling arrangements (National Rural Health Mission, 2005; 2007). Similarly, the SHI master plan in Cambodia, while offering a fragmented approach towards achieving UHC, recognizes the use of CBHI as one of the strategies and has established relevant implementation guidelines (Annear, Reference Annear2009; ILO, 2008). The community health funds and TIKA schemes in Tanzania, and CBHI in Lao People’s Democratic Republic, are backed by legislation (Alkenbrack, Lindelow & Jacobs, Reference Alkenbrack, Lindelow and Jacobs2010; Jutting, Msuya & Afsaw, Reference Jutting, Msuya and Asfaw2004) while in the Democratic Republic of the Congo, development of CBHIs was included in the country’s 2009–2011 specific action plan (Programme National de Promotion des Mutuelles de Santé, 2009). However, the evidence on the impact of such policies aimed at enabling CBHI is limited.
It remains the case that most countries do not have regulatory frameworks supporting the operationalization of CBHI schemes and, where they do exist, for example offering financial support to cushion vulnerable population groups, or re-insurance of schemes and guarantees, they are perceived as weak (Atim et al., Reference Atim1998; Diop & Ba, Reference Diop and Ba2010). Nonetheless, there have been several initiatives to subsidize contributions for people who wish to join CBHIs voluntarily – again including in Mali and Senegal. In both countries, the state subsidizes 50% of the annual premiums for the general population (Ridde et al., Reference Ridde2018). In Senegal and Burkina Faso, the state subsidizes 100% of premiums for indigent people, with varied provisions for other population groups, while in Burkina Faso the poorest pay 50% of the premiums (Ridde et al., Reference Ridde2018; Parmar et al., Reference Parmar2014). However, there is limited evidence on the effectiveness of such subsidies on the utilization of services and financial protection for indigent people.
Challenge 4: Broader health and insurance system issues
Broader health and insurance system issues have also been highlighted as key barriers to enrolment in, and the sustainability of, CBHI schemes.
Moral hazard, adverse selection and supplier-induced demand
By being based in the community, theoretically, the occurrence of some of the challenges faced by private and SHI systems can be minimized, such as moral hazard, adverse selection and supplier-induced demand. This is because, theoretically, these can be accounted for at the design stage. However, CBHI faces these problems too, as well as underinsurance and information asymmetry.
Moral hazard refers to the situation where individuals alter their health-seeking behaviours, accessing or utilizing care simply because they are covered (Powell & Goldman, Reference Powell and Goldman2021). The voluntary nature of the membership of CBHI schemes makes them more prone to adverse selection, a situation where high-risk or sicker individuals are more likely to self-enrol than those who are deemed low risk or healthier (Parmar et al., Reference Parmar2012). Adverse selection has been identified among CBHI enrollees in Zimbabwe (Muchabaiwa et al., Reference Muchabaiwa2017) and elsewhere in sub-Saharan Africa (Wiesmann & Jutting, Reference Wiesmann and Jutting2000); and especially following the introduction of subsidies in Burkina Faso (Parmar et al., Reference Parmar2012). Evidence of moral hazard and supplier-induced demand for services among members of CBHI schemes has also been documented in Ethiopia (Ayana, Reference Ayana2020) and Zimbabwe (Muchabaiwa et al., Reference Muchabaiwa2017). Supplier-induced demand occurs when health providers use their discretionary powers to influence change in demand; for example, by overprescribing services and commodities (Crane, Reference Crane1992). Such malpractices threaten the sustainability of CBHIs.
Overall lack of resources for health care
Sparse distribution of health facilities and limited health benefits have been identified as contributing to low CBHI enrolment and dropout rates (Basaza, Criel & van der Stuyft, Reference Basaza, Criel and Van der2008; Hao et al., Reference Hao2010; Shewamene et al., Reference Shewamene2021). We have already noted the problems of perceived poor health services and frequent stockouts of medications (Criel et al., Reference Criel2020; Kigume & Maluka, Reference Kigume and Maluka2021).
Preconditions for CBHI’s success
Are there, then, any conditions under which CBHI can succeed on its own terms, without giving up its voluntary nature and transmuting into SHI? To answer this, we first present a case study of CBHI as implemented in Senegal, before listing the preconditions identified as enabling CBHI schemes to work.
Evidence in practice: Senegal
In 2014, in Senegal, the communal mutuals of two departments were merged to create a single health insurance department (UDAM – Les Unités Départementales d’Assurance Maladie) managed by professionals (Ridde et al., Reference Ridde2022). Membership remains voluntary, so risk sharing on a large scale is still limited. However, through professional management and the recruitment of specialists, innovative strategies for recruiting members have been implemented. These include a state contribution for entire villages or schools which enables CBHI membership fee reductions for all those living, studying or working in these places and creates collective conduits to channel the state subsidy to the recipients. These UDAMs have a headquarters, general management and qualified support staff for all administrative tasks (Mbow et al., 2020). The scheme’s management by professionals is the main way in which it deviates from the Donfouet & Mahieu (Reference Donfouet and Mahieu2012) definition of CBHI we introduced at the beginning of this chapter. The two UDAMs have been effective and able to cope with overdue subsidies from the state. In addition, all the health facilities in the region have transitioned from unit pricing for each service to a global flat rate, making the price predictable for patients (Mbow et al., 2020). UDAMs also influence the supply of care during the regional health team coordination meetings. In 2021, more than 50% of the population in the two districts were members of the UDAMs, which is an impressive achievement. In addition, between 30% and 60% of the region’s hospital revenue comes from the UDAMs, which gives them undeniable power. The Senegal national UHC agency (ANCMU – Agence Nationale de Couverture Maladie Universelle) is scaling up this reform to other districts. This has been noted by neighbouring countries which have visited for benchmarking. However, the scalability of these reforms has been opposed by the community mutualist movement, which is challenging the management of mutuals by professionals rather than volunteers (Ridde, Kane & Faye, 2025). With the support of the Belgian and French mutualist movements, the Senegal body has engaged in advocacy through the Lomé Platform so as to scale up these reforms.
What preconditions are needed for CBHI to work?
Available evidence suggests that success of a CBHI scheme is heavily dependent on its design and structure, including the affordability of the scheme, managerial capacity, benefits package, level of trust, distance to facilities and the perceived quality of health care covered by these schemes; as well as personal factors, such as individual knowledge and understanding of the scheme, among others (Dror et al., Reference Dror2016). It is argued that barriers to the successful implementation of CBHI schemes are largely operational in nature (De Allegri et al., 2009) and these have been documented widely (Ekman, Reference Ekman2004; De Allegri et al., 2009; Ridde et al., Reference Ridde2010; Fadlallah et al., Reference Fadlallah2018).
Here we outline the underlying preconditions for the successful implementation of CBHIs, as follows: a supportive political and economic environment (from which several of the other preconditions flow); the availability of and ability to mobilize social capital; awareness of CBHI and issues of equity; the formalization/institutionalization of CBHI schemes within the overall health sector; and enhanced vertical and horizontal linkages.
Supportive political and economic environment
Country evidence shows that successful UHC schemes are politically driven or have government support (de Ceukelaire, de Vos & Criel, Reference De Ceukelaire, De Vos and Criel2011). This ensures that the required economic and regulatory frameworks supporting CBHI are established. Such frameworks enable the creation of incentives for expanding access to health care to rural and informal sectors, and for insurers willing to establish a presence in these settings. The government can use its infrastructure to facilitate the pooling of multiple schemes, purchase health care, provide subsidies for the indigent, ensure civic education and harness support from civil society actors (Bennett, Reference Bennett2004; Fadlallah et al., Reference Fadlallah2018; Mladovsky & Mossialos, Reference Mladovsky and Mossialos2008). However, without the correct balance, such government intervention easily changes the scheme from CBHI to a pooling and collection agency for SHI taxes. Therefore, an appropriate balance must be determined.
Availability of and ability to mobilize social capital
The central role of social capital in the success of CBHI schemes has been highlighted in the literature (Donfouet & Mahieu, Reference Donfouet and Mahieu2012; Derose & Varda, Reference Derose and Varda2009). Social capital, in the context of health financing, is generally understood as the “norms and broader social networks that enable individuals to act collectively” (Woolcock & Narayan, Reference Woolcock and Narayan2000). These norms promote trust, build cooperation and move communities to work together towards an agreed objective. The networks thus enhance solidarity which is essential for pooling risks and resources within a community. Addressing individual and community level social capital is associated with willingness to enrol, contribute and stay in a CBHI scheme (Chemouni, Reference Chemouni2018). The evidence from Senegal, for example, suggests that CBHI is more likely to thrive where individuals already possess social capital (Mladovsky, Reference Mladovsky2014).
Awareness of CBHI
An awareness of the possibilities of health insurance and issues of equity among the general population empowers target communities to actively engage in purchasing health care and demand accountability from health providers (de Vos et al., Reference De Vos2009). In addition, an overall awareness is necessary to address inequity, including strategies for dealing with inability to pay, identification of indigent people and targeting mechanisms in rural populations and the informal sector (Mladovsky et al., Reference Mladovsky2014). The government is often best placed to ensure civic education and create such awareness (Fadlallah et al., Reference Fadlallah2018).
Formalization/institutionalization of CBHI schemes within the health sector
Giving a CBHI scheme formal status facilitates linkages with other arms of the health sector and enhances the trust, sustainability and scalability of the schemes, as has been evidenced in Ethiopia (Tahir, Adilahi & Farah, Reference Tahir, Abdilahi and Farah2022). Institutionalization would also facilitate required managerial support. As demonstrated by the UDAMs in Senegal, managerial capacity is critical for the effective functioning of CBHIs (Ridde et al., Reference Ridde2022).
Enhanced vertical and horizontal linkages
Enhancing vertical and horizontal linkages involves creating synergy between the central government, community, local government and other players in the health sector. It requires engaging with other actors such as civil society, the private sector and other relevant bodies who can support civic education or create awareness of health insurance and strengthen the managerial capacity of CBHIs. These linkages would also support the regulation and accountability of CBHI schemes. Relationships should also be developed with other CBHI schemes to facilitate pooling of risks and resources and enable the strategic purchasing of services.
CBHI and UHC
Available evidence to support the narrative that current CBHI schemes can be used as a vehicle to achieve UHC in their different settings is limited and patchy (Carrin, Waelkens & Criel, Reference Carrin, Waelkens and Criel2005; Ekman, Reference Ekman2004; Mladovsky & Mossialos, Reference Mladovsky and Mossialos2008; Soors et al., Reference Soors2010), and thus researchers express cautious optimism about CBHI’s potential.
Arguments against the use of CBHI to advance UHC relate primarily to design issues. The significant heterogeneity in current CBHI scheme designs poses challenges to building large-scale and sustainable financing mechanisms. The huge variation in coverage and the range of benefits offered also hinders measurement of CBHI’s progress in achieving universal coverage. By design, the population group targeted by CBHI schemes (rural populations, informal sector and the indigent) all have irregular and often seasonal incomes. This creates barriers to effective and sustainable collection of CBHI contributions. Challenges related to unaffordability, small pools and limited contributions to the CBHI scheme lead to issues of equity. In the absence of significant support from other sources, the precarious financial state of CBHI schemes threatens their long-term sustainability (Atim et al., Reference Atim1998; Creese & Bennet, 1997; Criel, Reference Criel, Van Lerberghe, Kegels and De Brouwere1998; Ekman, Reference Ekman2004).
Countries such as India, Ethiopia, Ghana and Rwanda have nominally embraced CBHI as one of the potential instruments to achieve UHC (Lavers, Reference Lavers2019; McIntyre et al., Reference McIntyre2008; WHO, 2010; Urban Health Division, 2008). These countries have made pragmatic decisions to institute their own versions of CBHI, developing relevant regulatory frameworks to enable their schemes’ establishment and expansion. However, countries such as Ghana and Rwanda have deviated significantly from the CBHI concept by enforcing mandatory membership.
The enforcement of mandatory CBHI membership is the subject of ongoing debates across west African states. Some countries have suggested enforcing this by requiring proof of membership in a health insurance scheme for the issuance of administrative documents such as a passport, birth certificate or national identity card. However, this proposal has faced objections already. For example, unions in Mali won a legal battle rejecting mandatory contributions, but they finally reached an agreement several years later (Ridde et al., Reference Ridde2018). Time will tell whether these solutions are feasible in sociopolitical contexts very different from Rwanda, which has been able to make membership mandatory (Chemouni, Reference Chemouni2018).
Policy relevance and conclusions
Theoretically, in the absence of state-provided, tax-funded health care or formal health insurance, CBHI has the potential to reach rural and informal sectors, helping to create awareness of the concept of health insurance and providing some access to health care. Ideally, CBHI schemes would help to build trust in the use of health insurance. This would facilitate the entry of insurers into this market (Rosner et al., Reference Rosner2012), including private and SHI schemes, and non-salary-based options. In addition, CBHI schemes could support functions such as the recruitment of community members and identification of indigent people requiring subsidies, as is the case with the Rwanda scheme (Diop & Ba, Reference Diop and Ba2010; Chemouni, Reference Chemouni2018). However, CBHI design attributes – in particular the voluntary nature of enrolment and contribution – often prevent it from being a successful mechanism to raise sufficient revenue in practice. CBHI may therefore be better suited as solely a collection mechanism, given its potential to reach rural and informal sectors. If successful, this would support at least two of the UHC coverage goals: expanding population coverage and enhancing financial protection. With relevant awareness, community members can also demand accountability from the health system which would hopefully enhance responsiveness to their health needs, improved efficiency and quality of care.
Based on the evidence presented in this chapter, current CBHI schemes are still a long way from making a significant contribution to achieving UHC. Those held up as current examples of success can no longer be defined as CBHI schemes. Beyond the small pilots of CBHI schemes, there is very limited and often mixed evidence on the impact of pure CBHI across the different health financing functions and population health coverage. The role of the government is critical for the establishment and sustainability of effective CBHI schemes. Only then can CBHI be included in the suite of financing mechanisms that countries can use to advance the UHC agenda. Wide-scale adoption of CBHI rests on policy-makers’ decisions to create a regulatory space where these systems can operate. This would also facilitate the generation of sufficient evidence to support definitive decision-making on the implementation of CBHI, including appropriate design and scale-up.Footnote 2
Key messages
Chapter 1.3 considers voluntary health insurance (VHI). VHI is paid for privately by or on behalf of individuals and most often provides people with faster access to treatment and greater choice of health care provider. Premiums are not typically based on the policyholder’s income but are likely to vary depending on their risk of ill health. Key learning includes that:
Despite prepayment and risk pooling, VHI has limitations and does not align well with progress towards universal health coverage (UHC) because:
○ risk pools in VHI schemes are typically much smaller than pools established through statutory schemes, which means there are fewer people to share risk;
○ inequities are created because of the cost of premiums, which may not be affordable or accessible to everyone, including those most in need of financial protection.
VHI has wider equity implications because it offers those who can afford to pay faster access to, or greater choice of, services (supplementary insurance) or coverage of excluded services or user charges for statutory care (complementary insurance).
Governments seeking to use VHI to expand coverage typically have to make significant interventions, including through tax subsidies to make premiums more affordable, but this creates market distortions and is inefficient.
Policy-makers can secure better health system performance by improving access to publicly financed health care than by promoting VHI.
Introduction
Economic theory and empirical evidence indicate that it is difficult to get VHI to cover all needed health services for all those who require health care. As a result, countries struggle to make progress towards UHC – ensuring everyone can use quality health care without financial hardship (WHO, 2010) – through VHI alone. Although VHI generally improves financial protection (affordable access to health care) for those who have it, it can undermine the performance of the health system as a whole, particularly where it plays a large role.
It is not always easy to address the challenges posed by VHI; doing so requires political willingness and ability to shape the role VHI plays through careful policy design and implementation, strong regulatory capacity to ensure VHI functions in line with health system goals, and effort to ensure that publicly financed coverage meets the needs of those who are less likely to be covered by VHI, i.e. people with lower incomes or chronic conditions.
This chapter has three sections: understanding the role VHI plays in health system financing; understanding the challenges it brings with it as a policy; and providing advice for any policy-maker contemplating its introduction or, with an existing system of VHI, seeking to make it work better.
In the first section, we explain how VHI works, set out its distinguishing features and compare it with out-of-pocket (OOP) payments and medical savings accounts (MSAs) (see Box 1.3.1), outlining the even-worse-than-VHI failings of the latter. We examine VHI’s relationship with publicly financed health care coverage (supplementary, complementary or substitutive) and look at how much VHI is currently used and where, as well as reasons for changes in its level of use.
Understanding VHI’s role in health system financing
VHI can cover all or some of the risk of a person incurring health care costs. It can be bought by individuals or groups (for example, employers on behalf of their employees) and it can be sold by a wide range of entities – not only by for-profit (commercial) and non-profit-making private organizations, but also by public and quasi-public bodies.
What differentiates VHI from other types of health insurance is that it is taken up voluntarily, i.e. there is no compulsion to buy it, and paid for privately rather than publicly: VHI premiums are typically delinked from a policyholder’s income and often linked to a person’s risk of ill health (Mossialos & Thomson, Reference Mossialos and Thomson2002; Sagan & Thomson, Reference Sagan and Thomson2016a; Thomson, Sagan & Mossialos, Reference Thomson, Sagan and Mossialos2020). VHI therefore tends to be more regressive and less efficient in terms of raising revenue than public spending on health, and those who need it the most may not be able to access it or afford the premiums. The benefits offered by VHI can also be subject to user charges (co-payments) or limited in other ways to protect insurers from incurring losses, which means that some people may not be adequately protected from financial hardship caused by out-of-pocket (OOP) payments, even though they have VHI.
VHI is a form of prepayment, alongside other forms of prepayment such as taxes, mandatory health insurance contributions and MSAs (Box 1.3.1). In contrast to OOP payments, VHI premiums are collected in advance to pay for health care when it is needed, spreading the financial risk of ill health over time. In contrast to OOP payments and MSAs, VHI enables funds to be pooled, spreading financial risk across insured people. Financing health care through prepayment with risk pooling supports progress towards UHC by reducing financial barriers to access and financial hardship caused by OOP payments. However, VHI risk pools are generally much smaller than pools established through publicly financed coverage, which means there is less redistribution of financial risk.
MSAs are another form of prepayment, but, unlike VHI, they do not allow the spread of financial risk across insured people and thus typically do not provide sufficient financial protection.
MSAs allow enrollees to withdraw funds set aside to cover eligible health care costs. They are usually coupled with a high-deductible insurance plan to cover very high costs, allowing those who hold such accounts to manage risks over time but not across the broader population. In terms of overall health system policy, MSAs have very limited ability to achieve goals such as efficiency, equity and financial protection.
Although the accounts are expected to enhance efficiency by reducing the use of low-value treatments and controlling health care costs, evidence shows that they can discourage the use of both low- and high-value treatments, leading to reduced adherence to medication and preventive care. People who switch to MSAs tend to spend less on health care initially, but the long-term impact on costs is unclear.
MSAs allow individuals to spread financial risk over time, but they may not be sufficient to cover some health care costs and are likely to discriminate against people who are less able to save, including unemployed, disabled or chronically ill people. Evidence also shows that enrolment in the accounts can lead to a reduction in beneficial care, potentially undermining the health of people with low incomes or chronic conditions.
Despite the policy challenges related to MSAs, policy-makers in some countries continue to regard them as a desirable health financing mechanism. This may be due to the common use of savings for pensions, leading to the mistaken belief that savings alone can cover health care costs, and due to lobbying by financial service providers who offer the accounts. MSAs play a role in health system financing in China, Singapore, South Africa and the USA.
The role of VHI in health system financing is usually defined in relation to gaps in publicly financed coverage (Table 1.3.1). It typically supplements or complements publicly financed coverage; in a few cases it substitutes publicly financed coverage.
Supplementary coverage
Perceived problems with the quality and timeliness of publicly financed health care can motivate people to buy supplementary VHI. Supplementary VHI plays a role in the majority of countries, but its role is usually small both in terms of contribution to spending on health and share of the population covered. Ireland, Israel and South Africa are key exceptions: in these countries supplementary VHI either covers a large share of the population (Ireland, Israel) or only covers a small share of the population but accounts for an unduly large share of current spending on health (South Africa) (Thomson, Sagan & Mossialos, Reference Thomson, Sagan and Mossialos2020).
Complementary coverage
Gaps in the scope of the publicly financed benefits package or the existence of user charges for publicly financed health care can drive demand for complementary VHI coverage. Complementary VHI covering services excluded or not well covered by publicly financed health care usually plays a small role. It often focuses on dental care and is sold alongside supplementary VHI. The two main outliers are Canada, where outpatient medicines are not routinely publicly financed and many employers offer VHI to their employees, and the Netherlands, where over 80% of the population has VHI covering dental care and physiotherapy (Thomson, Sagan & Mossialos, Reference Thomson, Sagan and Mossialos2020). Complementary VHI covering user charges also usually plays a small role. Globally, Croatia and France are the main countries in which this type of VHI plays a significant role (Thomson, Sagan & Mossialos, Reference Thomson, Sagan and Mossialos2020). Slovenia was another notable case until 2024, when complementary VHI covering co-payments was abolished and replaced with a fixed compulsory contribution within the public health insurance scheme, and co-payments were removed.
Substitutive
People can buy substitutive VHI if they are excluded from publicly financed coverage or allowed to choose between publicly and privately financed coverage. Usually, only a small share of the population – often those with higher incomes – benefits from this type of coverage, but it can represent a more significant share of current spending on health. Substitutive VHI plays a significant role in a few countries only: Bahamas, Botswana, Brazil, Chile and Germany (Mathauer, Saksena & Kutzin, Reference Mathauer, Saksena and Kutzin2019; Thomson, Sagan & Mossialos, Reference Thomson, Sagan and Mossialos2020). It was abolished in the Netherlands in 2006 (Sagan & Thomson, Reference Sagan and Thomson2016b). Over time policy-makers in Chile and Germany have tried to limit the role of substitutive VHI because of its disruptive effect on the wider health system (Thomson, Sagan & Mossialos, Reference Thomson, Sagan and Mossialos2020).
| Role | Nature of coverage | Country examples |
|---|---|---|
| Supplementary | Offers faster access to services, greater choice of health care provider or enhanced amenities | Most countries, with a particularly large role in Ireland, Israel and South Africa |
| Complementary (user charges) | Covers user charges (co-payments) for goods and services in the publicly financed benefits package | Very few countries, but a significant role in Croatia and France |
| Complementary (services) | Covers services excluded from the publicly financed benefits package – typically dental care | Many countries, often sold alongside supplementary VHI but with a significant role in a few countries only, including Canada and the Netherlands |
| Substitutive | Covers people excluded from or allowed to opt out of publicly financed coverage | Very few countries have a significant role for substitutive VHI: Bahamas, Botswana, Brazil, Chile and Germany |
VHI: voluntary health insurance.
How much is VHI currently used and in which countries?
VHI makes a negligible contribution to spending on health in most countries.
In 2021, the VHI share of current spending on health exceeded 10% in only 22 countries globally (Fig. 1.3.1). VHI accounted for between 5% and 10% of current spending on health in a further 39 countries and was negligible everywhere else (WHO, 2023).
In 2021, the number of countries in which VHI accounted for at least 10% of current spending on health was very small
Note: SHA: System of Health Accounts; VHI: voluntary health insurance, USA: United States of America. VHI here is defined as health insurance schemes that are based upon the purchase of a health insurance policy, which is not made compulsory by government using the SHA code HF2.1. The figure excludes previously voluntary forms of private health insurance in France and the USA, which have been reclassified as compulsory health insurance in health accounts.

Figure 1.3.1 Long description
The y-axis notes the voluntary health insurance schemes as a percentage of current health expenditure, while the x-axis notes the countries. The values are as follows. Liberia: 47.0. South Africa: 43.0. Venezuela: 37.9. Namibia: 36.4. Bahamas: 31.6. Brazil: 27.6. Lebanon: 26.0. Thailand: 16.5. Jamaica: 14.3. Andorra: 14.3. Botswana: 13.8. Jordan: 13.6. Antigua and Barbuda: 13.6. Slovenia: 12.4. Canada: 11.4. Argentina: 11.4. Bahrain: 11.1 Uruguay: 10.9. Eswatini: 10.7. Ireland: 10.4. Gabon: 10.4. Israel: 10.1.
Across all countries for which data are available, on average VHI accounts for only 5.3% of current spending on health, ranging from 3.6% in lower-middle-income countries to 7.4% in upper-middle-income countries (UMICs) (Fig. 1.3.2).
In 2021, the VHI share of current spending on health was highest in UMICs
Note: SHA: System of Health Accounts; VHI: voluntary health insurance. Only includes countries for which VHI data were available. VHI here is defined as SHA code HF2.1.

Figure 1.3.2 Long description
The y-axis notes the Voluntary health insurance schemes as a percentage of current health expenditure from 0 to 50, while the x-axis represents the income groups, each with three values: Range, Average, and Median, respectively. The values are as follows. Low (21 countries): 46.0; 4.2, 2.0. Lowe-middle (46 countries): 25.5; 3.6; 2.5. Upper middle (51 countries): 44.0; 7.4; 5.0. High (55 countries): 31.5; 5.1; 4.9. All (173 countries): 46.0; 5.3; 4.0.
In terms of World Health Organization regions, on average the VHI share of current spending on health was highest in the Americas (8.1%) and the lowest in Europe (3.2%) (Fig. 1.3.3).
In 2021 the VHI share of current spending on health was higher in the Americas than in other parts of the world
AFR: WHO African Region; AMR: WHO Region of the Americas; EMR: WHO Eastern Mediterranean Region; EUR: WHO European Region; SEAR; WHO South-East Asian Region; SHA: System of Health Accounts; VHI: voluntary health insurance; WHO: World Health Organization; WPR: WHO Western Pacific Region.
Notes: Only includes countries for which VHI data were available. VHI here is defined as SHA code HF2.1.

Figure 1.3.3 Long description
The y-axis notes the Voluntary health insurance schemes as a percentage of current health expenditure from 0 to 50, while the x-axis represents the regional groups, each with three values: Range, Average, and Median, respectively. The values are as follows. A F R (43 countries): 47.0; 6.1; 3.0. A M R (35 countries): 27.5; 8.1; 5.5. E M R (16 countries): 25.0; 5.5; 3.0. S E A R (9 countries): 15.5; 3.6; 1.5. E U R: 15.0; 3.3; 3.0. W P R (20 countries): 10.0; 4.3; 4.0.
Changes in levels of use of VHI
Only a handful of countries have seen large changes in VHI’s contribution to current spending on health over time, with decreases usually recorded in high-income countries (HICs) and increases in middle-income countries.
VHI’s share of current spending on health did not change much between 2000 and 2021 in most countries. Looking at changes between two points in time can conceal fluctuations, but during this period the VHI share fell by five or more percentage points in only eight countries globally (mostly HICs) and grew by five or more percentage points in 21 mostly lower-middle or UMICs (Fig. 1.3.4).
Not many countries saw substantial changes in the VHI share of current spending on health between 2000 and 2021
Note: CHE: current health expenditure; SHA: System of Health Accounts; VHI: voluntary health insurance, USA: United States of America. VHI here is defined as SHA code HF2.1. In France, Germany and the USA the changes are due to changes in health accounting that resulted in VHI being reclassified as compulsory health insurance.

Figure 1.3.4 Long description
The y-axis lists the percentages from minus 40 to 60, while the x-axis lists the countries. The countries with negative age point change are: United States of America, Uruguay, Morocco, Netherlands, Monaco, France, Germany, and Antigua and Barbuda. Those with positive age point changes are: Croatia, Benin, Kenya, Côte d’Ivoire, Suriname, Poland, Iran, Israel, Haiti, Republic of Korea, Brazil, Zimbabwe, India, China, Bahrain, Ireland, Jordan, Thailand, Lebanon, Venezuela, and Liberia.
The large drop in the VHI share of current spending on health in France, Germany and the USA was due to changes in health accounting. VHI was reclassified as compulsory health insurance in National Health Accounts in response to reforms making private health insurance compulsory for some groups of people (OECD, Eurostat & WHO, 2017). In France, the VHI share fell from 13% in 2012 to 7% in 2016 following the government’s introduction in January 2013 (with effect from 2016) of a mandate on all employers to offer complementary private health insurance covering user charges to their employees (Couffinhal & Franc, 2020; Bricard, Reference Bricard2024). The introduction of a universal mandate in Germany in 2009, making it compulsory for people who choose to opt out of publicly financed coverage to take up substitutive private health insurance (as opposed to remaining without any coverage), resulted in the VHI share falling from 9% in 2008 to 1% in 2009 (Ettelt & Roman-Urrestarazu, Reference Ettelt, Roman-Urrestarazu, Thomson, Sagan and Mossialos2020). In the USA, the implementation of the Affordable Care Act in 2014 made health insurance mandatory for people under the age of 65 years for the first time, leading the VHI share to fall from 33% in 2013 to 1% 2014 (Brown & Glied, Reference Brown, Glied, Thomson, Sagan and Mossialos2020).
In Morocco, the Netherlands and Uruguay, the decline in the VHI share of current spending on health followed reforms to expand access to publicly financed coverage. A sudden fall in the VHI share in Morocco (from 12% in 2005 to 1% in 2006) followed the creation of a mandatory social health insurance (SHI) scheme, which extended publicly financed coverage from 16% to 30% of the population (Mulvihill, Reference Mulvihill2022). In the Netherlands, a national health insurance scheme introduced in 2006 abolished substitutive VHI for richer people, who had previously been excluded from publicly financed coverage, leading to a fall in the VHI share from 20% in 2005 to 6% in 2006 (Maarse, Jeurissen & North, Reference Maarse, Jeurissen, North, Thomson, Sagan and Mossialos2020). In Uruguay the VHI share fell progressively from 32% in 2000 to 12% in 2020, following the establishment and gradual expansion of publicly financed coverage (Arbulo et al., 2015). The speed of decline in the VHI share was slower than expected, however, partly due to employers continuing to be allowed to provide VHI to their employees (Pettigrew & Mathauer, Reference Pettigrew and Mathauer2016).
The decline in VHI’s share of current spending on health in South Africa is linked to a decline in VHI population coverage due to rising premiums (Pettigrew & Mathauer, Reference Pettigrew and Mathauer2016). Despite this, the VHI share in South Africa remains the highest in the world (43% in 2021), despite the fact that VHI only covers around 16% of the population (see Fig. 1.3.1) (McIntyre & McLeod, Reference Mcintyre, Mcleod, Thomson, Sagan and Mossialos2020).
In countries such as Jordan, Thailand and Venezuela, large increases in the VHI share of current spending on health reflect a combination of factors, including the poor performance of publicly financed coverage, growing purchasing power in the middle class and wider economic trends, including trade liberalization and privatization (Pettigrew & Mathauer, Reference Pettigrew and Mathauer2016).
Growth in public spending on health slowed significantly following the global financial crisis of 2007–2008, leading to an increase in the private share of current spending on health in many countries, but this often occurred due to increased reliance on OOP payments rather than growth in VHI (Thomson et al., 2015). In response to COVID-19, many countries sought to increase public spending on health and some expanded publicly financed coverage, at least for services related to COVID-19 (Thomson et al., 2022; WHO Regional Office for Europe, 2021). Access problems, including large backlogs in health services and higher waiting times, have fuelled interest in purchasing VHI in countries like the United Kingdom (Campbell, Reference Campbell2022). Indeed, per capita spending on VHI in the United Kingdom rose from US$ 123 to 140 between 2019 and 2021 (WHO, 2023). Over this period, 26 countries experienced an increase in per capita VHI spending by more than US$ 10, with the most substantial increases observed in Canada, Australia, Ireland and Liberia (exceeding US$ 50 per capita). Conversely, eight countries noted declines in VHI per capita spending of US$ 10 or more, with the largest falls observed in Cyprus, Lebanon, Monaco and United Arab Emirates (WHO, 2023). However, on the whole, per capita VHI spending changed little in most (80%) countries (WHO, 2023).
Key policy challenges for the use of VHI
VHI on its own cannot help countries to progress towards UHC. It can help to fill some gaps in publicly financed coverage, but it is generally difficult to align VHI with the goal of ensuring that everyone can access health care without experiencing financial hardship. We identify four key policy challenges that explain this difficulty: VHI does not stop reliance on OOP payments; it is difficult to ensure affordable access to VHI for those who need it most; VHI undermines equity and efficiency in the use of resources; and history and politics get in the way of an effective VHI policy. We deal with each of these in turn below.
Policy challenge 1: VHI is unlikely to be helpful in making progress towards UHC in countries that rely heavily on OOP payments
Both economic theory and empirical evidence indicate that VHI is unlikely to provide comprehensive coverage for the whole population.
Economic theory
It is extremely difficult for VHI to provide comprehensive coverage for the whole population, even when it is heavily regulated, due to market failures. Market failures in health insurance are well recognized (Barr, 1992). Problems such as moral hazard and monopoly issues afflict both compulsory and voluntary health insurance (Nyman, 2004; Barr, 2004; Einav & Finkelstein, 2018). In addition, VHI is prone to adverse selection and risk selection.
Adverse selection refers to a situation in which people with higher risks of ill health are more likely to take up VHI, which limits risk pooling and pushes up health care costs, leading insurers to increase premiums or reduce benefits. This in turn may make VHI less accessible for people with high risks and less attractive for people with low risks. If low-risk people stop buying VHI, the ensuing “death spiral” can lead to the collapse of an insurance company. Similarly, it is difficult to sustain VHI among people who are already ill or at high risk of becoming ill and when the risks of becoming ill are linked, such as during epidemics (Barr, 2004). Financial regulation of VHI can provide the necessary stability, but adverse selection is best prevented by making health insurance compulsory. In practice, adverse selection may be less of an issue because richer (and healthier) people are often more likely to buy VHI, especially when it is offered alongside publicly financed coverage.
Insurers typically try to prevent adverse selection by selecting people with lower health risks; for example, by excluding from coverage or charging higher premiums for pre-existing conditions. Again, this means that some people may not be able to obtain any or sufficient coverage through VHI, limiting risk pooling. Material regulation involving rules around premiums, benefits and other contractual conditions can help avoid some of these problems (Thomson, Sagan & Mossialos, Reference Thomson, Sagan and Mossialos2020).
Empirical evidence
The empirical evidence supports economic theory. Historically, as the precursor to publicly financed coverage, VHI never succeeded in covering the whole or even most of the population. The goal of universality was only achieved through the introduction of mandates for publicly financed health care.
We can briefly recap VHI’s history, based on the account of Thomson, Sagan & Mossialos (Reference Thomson, Sagan and Mossialos2020). VHI is the earliest form of prepaid health financing. It first emerged in Europe in the Middle Ages, before the rise of modern medicine, and aimed to compensate people for loss of earnings due to illness, which is why it was linked to employment. VHI offered by mutual-aid associations serving industrial workers had become the norm in Europe by the mid-19th century and spread via colonialism to countries outside Europe (e.g. South Africa, where it initially covered white mine workers).
Medical advances led to an increase in the cost of health care, motivating health care providers in the early 20th century to develop VHI, often in league with hospitals run by the charitable sector, so that people could continue to pay for their services. Provider-driven VHI proliferated in Europe and beyond, including Australia, Canada and the USA. Over time, these largely non-profit schemes were joined by commercial schemes.
Few of these early forms of VHI grew to cover more than a small share of the population, not only because health insurance was voluntary and also usually linked to employment, but also because it was unaffordable for many people. Starting with Germany in 1883, national governments began to introduce compulsory publicly financed schemes to extend coverage to more people, filling gaps that VHI could not cover.
Further empirical evidence is provided by data on health spending, which suggest that public spending on health is more likely to reduce OOP payments than VHI. Across countries there is very little association between spending through VHI and spending through OOP payments (Fig. 1.3.5a). Liberia, Namibia and South Africa are the only countries where the VHI share of current spending on health substantially exceeds the OOP payment share. In South Africa, for example, the decline in the OOP payment share (from 14% in 2000 to 5% in 2020) was accompanied by a small decline in the VHI share (from 47% to 42%) and a large increase in the public share (from 37% to 51%) (WHO, 2023). This means that it is unlikely that it was VHI that drove down OOP payments in South Africa. Across countries there is a much stronger correlation between public spending on health and OOP payments (Fig. 1.3.5b).
Public spending on health is more likely to reduce OOPs than VHI

Figure 1.3.5a Long description
The x-axis represents V H I as percentage of current health spending from 0 to 50, while the y-axis represents O O P spending as percentage of current health spending from 0 to 90. Most of the plots are concentrated between x equals 0 and x equals 15, along the full length of the y-axis. The best-fit line moves straight from (0, 30) to (47, 12), where R-squared equals 3 percent.
Domestic general government spending on health as a percentage of GDP versus OOP payments as percentage of current spending on health, 2021
Note: GDP: gross domestic product; OOP: out-of-pocket; SHA: System of Health Accounts; VHI: voluntary health insurance. VHI here is defined as SHA code HF2.1. Domestic general government spending on health here is defined as health expenditure funded from general government domestic sources (government domestic revenues and SHI contributions). In SHA it is calculated as FS.1 (transfers from government domestic revenue allocated to health purposes) plus FS.3 (social insurance contributions).

Figure 1.3.5b Long description
The x-axis represents Domestic general government expenditure on health as percentage of G D P from 0 to 14, while the y-axis represents O O P spending as percentage of current health spending from 0 to 90. Most of the plots are concentrated between x equals 0 and x equals 4, along the full length of the y-axis. The plots move down the y-axis as the x-axis increase. The best-fit line moves straight from (0.5, 42) to (11.5, 0), where R-squared equals 33 percent.
Policy challenge 2: It is difficult to ensure affordable access to VHI for those who need it most
Empirical evidence shows that VHI is more likely to be taken up by richer people, which exacerbates inequality in financial protection (affordable access to health care) (Sagan & Thomson, Reference Sagan and Thomson2016a; Thomson, Sagan & Mossialos, Reference Thomson, Sagan and Mossialos2020). This is sometimes the result of policy design – for example, in countries such as Germany where only richer people are allowed to opt out of publicly financed coverage. More often, it is due to insurer behaviour, perhaps in response to concerns about adverse selection (as described above), which makes VHI less accessible to people with a higher risk of ill health and less affordable for people with lower incomes. As a result, it is generally difficult for VHI to improve financial protection in the health system as a whole – but the degree to which affordability is a problem varies according to whether VHI is playing a supplementary, complementary or substitutive role in the overall health coverage mix.
Where VHI plays a supplementary role
Problems with affordable access to VHI need not be a concern where VHI plays a supplementary role and the policy goal is merely for VHI to offer more choice to a small share of the population – as in the United Kingdom.
Where VHI plays a substitutive or complementary role
Affordability is more of a concern where VHI plays a substitutive role and is the only form of coverage for some groups of people or where VHI plays a complementary role and covers significant gaps in the publicly financed benefits package or user charges. In such cases VHI can be critical to ensuring financial protection and should therefore cover all those who need it, but many countries have struggled to achieve this.
Globally, only three main countries – Croatia, France and Slovenia – have managed to provide complementary VHI covering user charges to almost all those who need it, but this has involved heavy government intervention through regulation and tax subsidies for people with low incomes and, in France, making private health insurance compulsory for employees (WHO Regional Office for Europe, 2019; 2023).
VHI covering co-payments in Croatia, France and – until recently – Slovenia achieves very high rates of population coverage, reaching over 80% of those who have to pay co-payments in Croatia, around 90% of the population in France and around 95% of those with compulsory health insurance in Slovenia. Partly due to high take-up of VHI covering co-payments, the incidence of catastrophic health spending is very low in Slovenia and France and relatively low in Croatia (WHO Regional Office for Europe, 2019; 2023; Voncina & Rubica, 2019; Bricard, Reference Bricard2024; Šarec & Jošar, 2025).
High levels of VHI take-up in these three countries can be attributed to the following factors:
People need VHI covering co-payments because user charges are widely applied in all three countries and are in the form of percentage co-payments for secondary care, meaning that people have to pay 20% of the cost of inpatient care. Although there are caps in place for inpatient care (France) and secondary care (Croatia), these caps are set at a high level; many households would face financial hardship before reaching them.
VHI covering co-payments is accessible to all those who want to buy it due to regulation (open enrolment plus community-rated premiums) in Croatia and until recently in Slovenia and tax subsidies targeting people with low incomes in France (see Box 1.3.2).
VHI covering co-payments is affordable for most people because it is free for people with very low incomes in Croatia and France. In Slovenia, people with very low incomes were exempt from co-payments and did not need VHI. However, for the rest of the population, complementary VHI was financed through flat-rate premiums rather than income-related contributions, raising longstanding equity concerns and making it politically contentious. Premium hikes in early 2023 risked pushing coverage out of reach for some households, prompting the government first to introduce a price cap and ultimately to abolish most co-payments (Šarec & Jošar, 2025).
Using complementary VHI to cover user charges is not a panacea, however. VHI premiums are regressive in comparison to public spending on health, undermining equity in financing health care; VHI does not eliminate inequalities in access to health care; and in spite of regulation and tax subsidies, people with low incomes are still more likely to lack VHI coverage and less likely to have good quality VHI coverage than richer people (e.g. in France) (WHO Regional Office for Europe, 2023; Bricard, Reference Bricard2024).
Government intervention in VHI has generally intensified over time, regardless of VHI’s role, for two reasons: changes in the nature of VHI with the entry of commercial insurers and, in some countries, growth in VHI, which has made its negative effects on health system performance more visible (Thomson, Sagan & Mossialos, Reference Thomson, Sagan and Mossialos2020).
VHI in France is dominated by non-profit mutual associations and predates the establishment of national health insurance in 1945. VHI coverage grew from around 30% of the population in 1950 to 86% in 2000. In 2000, to address concerns about low VHI uptake among poorer households, the government introduced tax subsidies, making VHI free for people with very low incomes and cheaper for people with low incomes. VHI coverage subsequently reached 95% in 2013.
In 2016, the government required all employers to offer VHI to their employees – a measure intended to improve access to group VHI contracts, which are known to be more advantageous than individual contracts. Although this is expected to reduce inequities in VHI access among employees, it may widen disparities between salaried employees and students, pensioners and unemployed or self-employed people. Recent studies suggest that this policy could potentially diminish overall welfare, as employers are likely to pass on the cost of insurance contracts to employees through salary adjustments. The key net beneficiaries of this policy would likely be short-term unemployed individuals (around 7% of the population), who could retain their former complementary health coverage (Benoît & Coron, Reference Benoît and Coron2019). Recent data on population coverage indicates a slight decline from 93% in 2017 to 90% in 2018 (FNIM, 2019).
Policy challenge 3: VHI undermines equity and efficiency in the use of resources
Erosion of equity and efficiency in the use of health system resources is a particular challenge when VHI plays a supplementary or substitutive role.
VHI can undermine equity and efficiency in the use of health system resources in various ways (Box 1.3.3). This is most likely to occur in contexts where, rather than complementing publicly financed coverage, VHI plays a significant supplementary or substitutive role, covering the same services as publicly financed coverage and drawing on the same pool of health care providers. Negative spillover effects are common when the services offered by VHI are more expensive than those offered by publicly financed coverage, creating incentives for providers to prioritize the treatment of people with VHI or to work in the private sector. Spillover effects may be present even where VHI plays a minor role, but they become more visible and more detrimental where VHI plays a more significant role.
Other concerns related to VHI include the inefficiencies that arise from duplication of administrative and other responsibilities for managing different risk pools (Smith & Witter, Reference Smith and Witter2004). Risk-rating requires information and auditing capacity to assess individual health risks, write appropriate contracts and monitor health care use (Smith & Witter, Reference Smith and Witter2004). Available data suggest that administrative costs are almost always higher in VHI than publicly financed coverage (Sagan & Thomson, Reference Sagan and Thomson2016a).
Tax subsidies benefit richer households: Tax subsidies introduced to promote VHI take-up usually benefit richer households. For example, in Brazil and South Africa tax subsidies amount to about 30% of federal government spending on health (Brazil) and all public spending on health (South Africa), despite VHI covering only 24% and 16% of the population respectively (McIntyre & McLeod, Reference Mcintyre, Mcleod, Thomson, Sagan and Mossialos2020; Montoya Diaz et al., 2020). There is no evidence to support the idea that general tax subsidies for VHI are an efficient use of public resources.
Inadequate compensation for VHI’s use of public resources: In some countries, such as Brazil, Chile and Ireland, many people with VHI continue to use public facilities, including as backup cover. While this is permitted by law and private insurers are required to compensate public providers for the use of their facilities, this has been difficult to enforce (Brazil, Chile) or has never reflected the full economic cost (Ireland). Implicit subsidies also arise from public funding of medical education.
Migration of health professionals from public to private facilities: Since services covered by VHI are usually provided in the private sector, where earnings tend to be higher than in the public sector, this may lead to a migration of health professionals from public to private facilities, as in Kenya and South Africa. This can leave public facilities under-staffed, with implications for quality of care.
Increase in waiting times for publicly financed treatment: Failure to align provider incentives leads to increased waiting times for publicly financed treatment because doctors permitted to work in both private and public sectors may face strong financial incentives to prioritize patients with VHI; for example, if they are paid more to treat people with VHI or when waiting times are the main reason for purchasing VHI, as in Ireland.
Loss of financial contributions to publicly financed coverage: In countries where people can choose between publicly financed coverage or substitutive VHI (Chile and Germany), the publicly financed scheme loses contributions from those with higher incomes and better health when they opt for private health insurance. If those who opt for private health insurance are allowed to return to the publicly financed scheme; for example, when they are sicker and their premiums increase, this may put pressure on the publicly financed scheme. On the other hand, if opting out of the publicly financed scheme is irreversible, heavy regulation is required to ensure that private health insurance is accessible and affordable for those who can no longer return to publicly financed coverage.
Policy challenge 4: History and politics are a challenge to effective public policy towards VHI
Once established, VHI markets can be difficult to shape, especially where VHI plays a larger role.
Aligning VHI with the goals of UHC requires effective public policy. A government’s ability to ensure this may be more difficult where VHI plays a large or significant role, which in turn may be the outcome of historical developments (path dependency), political ideology and the relative power and interests of different stakeholders (Thomson, Sagan & Mossialos, Reference Thomson, Sagan and Mossialos2020).
Health care providers and insurers have frequently opposed efforts to expand access to publicly financed coverage or tighten regulation of VHI, sometimes with the support of employers, civil servants and richer people – those most likely to benefit from preserving the status quo. Private interests have blocked or delayed the implementation of universal schemes in a wide range of countries, including Canada, Chile, Germany, Ireland, Kenya, the Netherlands, South Africa, Switzerland and the USA (Thomson, Sagan & Mossialos, Reference Thomson, Sagan and Mossialos2020). In some LMICs, the promotion of VHI by donors and other actors has given it disproportionate political power (Pettigrew & Mathauer, Reference Pettigrew and Mathauer2016).
In many countries, VHI does not fall under the purview of the health ministry but is regulated as a financial service by the finance ministry or other ministries concerned more with economic or industrial policy than social policy (Sagan & Thomson, Reference Sagan and Thomson2016a). This is another obstacle to effective public policy and may explain why oversight of VHI is often weak in countries at all income levels (Thomson, Sagan & Mossialos, Reference Thomson, Sagan and Mossialos2020).
Understanding how policy challenges can be addressed
Policy responses using VHI to fill gaps in publicly financed coverage can vary depending on the nature and size of the role VHI plays. We suggest strategies that policy-makers can implement to address the challenges that come with VHI according to two scenarios: where VHI is newly introduced, or plays only a small role, and another, where VHI is already well established.
If VHI does not yet play a role or only plays a small role in the health system
Decision-makers should anticipate the policy challenges that VHI brings and consider whether there is enough capacity to monitor and regulate VHI and manage interests. Alongside this, they must remember that, once established, VHI may be more difficult to shape.
If thinking about introducing VHI, careful consideration should be given to policy design so that it does not undermine publicly financed coverage. Further, clear boundaries between publicly and privately financed health care should be drawn.
Supplementary VHI (offering people faster access to treatment) is best when it is limited to a small share of the population. Keep it that way. Do encourage growth through tax subsidies or material regulation to make VHI more accessible and affordable.
Complementary VHI can protect against OOP payments where there are significant gaps in the publicly financed benefits package or heavy user charges. Globally, only a handful of countries have managed to achieve the high rates of population coverage needed if this type of VHI is to help meet UHC goals. Achieving high rates of population coverage comes at a cost: to ensure VHI is accessible and affordable for those who need it most requires heavy government intervention, including tax subsidies exclusively for people with low incomes.
Do not allow people to opt out of publicly financed coverage. Substitutive VHI does not enhance health system performance. Some countries have abolished substitutive VHI (Netherlands) and others are trying to limit its role (Chile and Germany).
VHI is not a panacea for high OOP payments. Increases in public spending on health are more likely to reduce OOP payments than VHI, so rather than trying to encourage VHI through tax subsidies or other means, policy should focus on improving affordable access to publicly financed health care. Tax subsidies for VHI are generally inequitable and inefficient and waste public resources.
If VHI already plays a significant role in the health system
Ensure there is sufficient capacity and political will to monitor and regulate VHI, enforce boundaries between publicly and privately financed health care and manage stakeholder interests.
Enforce boundaries between publicly and privately financed health care so that VHI does not undermine equity and efficiency in the use of public resources. In practice this can be difficult to achieve due to entrenched stakeholder interests.
Where VHI plays a significant complementary or substitutive role, careful intervention is needed to ensure affordable access to VHI for those who need it. This can be achieved through material regulation involving a wide range of rules, including open enrolment (guaranteed issue); lifetime cover (guaranteed renewal); community rating (delinking premiums from individual risk of ill health); premium review, approval or caps; mandated (usually minimum) benefits; prohibition of exclusion of pre-existing conditions; caps on user charges for VHI-covered services; and prohibition of benefit ceilings (Sagan & Thomson, Reference Sagan and Thomson2016a).
Country experience shows that it is not easy to ensure affordable access to complementary or substitutive VHI for people with low incomes or chronic conditions. Some countries have resorted to making VHI compulsory, but this has not been unproblematic, in part because it is a regressive way of financing health care, placing a disproportionate financial burden on those with lower incomes. A better solution would be to make sure that people with low incomes or chronic conditions do not need VHI.
Conclusions
VHI plays a very minor role in financing health care in most countries, especially in countries that rely heavily on OOP payments. However, due to a combination of market failures and weaknesses in public policy towards VHI, it can have a disproportionately negative effect on health system performance. Although VHI does fill gaps in publicly financed coverage, it often favours richer people, exacerbating inequity in financial protection. It can also draw financial and human resources away from publicly financed coverage, particularly where it plays a substitutive role or a large supplementary role.
Ensuring that those who most need VHI can buy it – and that VHI does not undermine equity and efficiency in the use of public resources – requires significant capacity to monitor and regulate VHI and enforce boundaries between publicly and privately financed health care. Governments often struggle to shape VHI in the face of opposition from entrenched stakeholder interests. Even when VHI improves access and financial protection for people with low incomes, which is generally rare, it remains a regressive form of financing health care.
Given what we know about VHI from economic theory and empirical evidence, countries should lower their expectations about its ability to meet the goals of UHC and focus instead on improving affordable access to publicly financed health care.Footnote 1
Key messages
Chapter 1.4 looks into official development assistance (ODA). ODA is provided by governments or multilateral development banks (MDBs) to support economic development in other countries. Key learning includes that:
ODA is critical to achieving the Sustainable Development Goals (SDGs) in the world’s poorest countries.
Lower-middle and middle-income countries (MICs) tend to receive more ODA than lower-income countries (LICs) due to a number of factors, including precedence and project continuity, differences in the ability to borrow and attract higher volumes, and extenuating circumstances and differences in capacity to absorb additional funds.
MDB funds are best utilized when they are invested in under resourced areas, such as global or regional public goods, and when they are well-aligned with domestic policies and national goals.
ODA success (i.e. resources having a meaningful impact on development outcomes) depends on:
○ prioritizing the right long-term development challenges;
○ effective domestic governance and an active role for national-level stakeholders;
○ transparency around ODA activities;
○ continuous assessment, evaluation, learning and improvement.
ODA and financing institutions must adjust to new challenges such as climate change – moving away from a sector-by-sector approach, addressing trends and emerging themes and delivering innovative and agile financing mechanisms.
Introduction
In years to come, the early 2020s may prove to be an anomalous period in terms of ODAFootnote 2 in health. In 2020, COVID-19 wreaked havoc and required development partners to rapidly scale up support for fragile health systems. In the years since, we have had the opportunity to carefully reflect on the performance of the initial COVID-19 responses and consider paths towards more resilient and inclusive recovery. However, recognizing that many countries – and particularly low- and lower-middle-income countries with financing constraints – fall in and out of emergency situations frequently, the lessons we can take from COVID-19 will be relevant for many years to come. One trend has been clear from the outset: COVID-19 derailed the SDGs and forced governments to reprioritize their budgets both at home and abroad. Many developing countries – already facing resource-challenges – experienced significant gaps in resources. As such, COVID-19 has provided a strong case for ODA to fill some of these gaps by way of fiscal and technical assistance – not least, to support struggling health systems.
This chapter argues that ODA finance, particularly that provided by MDBs, is – and will remain – central in supporting developing countries to reach their SDGs and achieve poverty reduction in the aftermath of the COVID-19 pandemic. The chapter looks first at what ODA is and how much there is of it. It contrasts the support given by different types of donor – individual governments (bilateral support), international financial institutions and multilateral organizations – and issues raised by the provision of support as loans rather than grants. Next it looks at the recipients of ODA – by sectors and level of development as measured by income level. It outlines the support given during and since the COVID-19 pandemic and why external development financing for health remains crucial. The focus then shifts to the particular role played by the MDBs and a case study of the response by the Asian Development Bank to COVID-19 is presented. Finally, the chapter sets out the implications for policy that flow from the use of ODA as a financing mechanism – how to assess its quality and impact; its continuing role in supporting countries post pandemic and in the context of climate change – and the concluding section summarizes key points and suggests ways forward.
ODA: definition and quantity
What is ODA?
ODA is defined as government aid that promotes and targets the economic development of developing countries. ODA constitutes over 70% of total external finance of the poorest countries in the world, and the Organisation for Economic Co-operation and Development (OECD) Development Assistance Committee (DAC) provides a unique platform for coordination among aid givers. Formed in 1961, the Committee’s mandate is to promote development cooperation in order to help implement ODA and sustainable development. The Committee comprises an international group of some of the largest providers of aid, including 30 bilateral members (who give aid government to government), six observers (those who channel and pool aid, commonly known as international financial institutions) formed of four MDBs, the International Monetary Fund (IMF) and the United Nations Development Programme (UNDP), and other participants, which are countries who are not members of OECD but want to contribute to discussions of the DAC. The current seven participating countries include Bulgaria and United Arab Emirates.Footnote 3 The DAC list of countries eligible to receive ODA, based on per capita income, is updated every three years. The Committee recognizes ODA as the gold standard of foreign aid, having provided billions of dollars in aid and technical support over the years (OECD, 2023).
How much ODA is there?
2009–2019
Total ODA remained robust in the decade prior to COVID-19. Between 2009 and 2019, there was a steady rise in ODA volume across all sectors from US$ 119 billion to over US$ 150 billion (2018 saw a high of US$ 153 billion),Footnote 4 albeit representing only a minor fraction of gross national income (GNI) per capita (OECD, 2023; OECD, 2021). Of this total ODA, support to the health sector consistently comprised about 13% each year (Knox, Reference Knox2020). Multilateral organizations including the IMF, Asian Development Bank and the World Bank accounted for around 35% of health ODA, with DAC members (particularly USA and United Kingdom) disbursing the remainder.
Since COVID-19
During times of crisis, such as COVID-19, ODA is critical in maintaining development progress – or, at the very least, limiting regression. Preliminary analyses of figures give some insights into the scale of overall ODA growth. In 2020, ODA amounted to US$ 161 billion, representing 0.32% of combined GNI of DAC (OECD, 2021). At the time, this amount was the highest level ever recorded and reflects the urgent response to COVID-19, made available by maintaining previously planned ODA commitments, reorienting funds, as well as mobilizing additional funds (Ahmad et al., Reference Ahmad2020). Such records were broken again in 2021, when ODA reached $178.9 billion (of which support for COVID-19 vaccines accounted for $18.7 billion) (OECD, 2022).
ODA donors: bilateral support versus international financial institutions and multilateral organizations
While ODA levels increased overall, COVID-19 had differing impacts on the source of support. For example, as domestic economies were hit in 2020, ODA commitments from bilateral members fell by 26% compared to the same period in 2019. This decrease was somewhat offset by the increase in commitments by the international financial institutions, but trends depend heavily on contributing governments’ priorities as much as – or perhaps more than owing to – the needs of developing countries.
Loans versus grants
Notably, most of the support is increasingly provided through loans as grant resources dwindle, which may have long-term consequences: 22% of gross bilateral ODA in 2020 comprised loans and equity investments, up from 17% in previous years. International financial institutions also increased the volume of commitments significantly between 2019 and 2020 from US$ 21.6 billion to US$ 62.5 billion (Dodd, Knox & Breed, Reference Dodd, Knox and Breed2021). Even though, compared to 2019, US$ 40 billion more in concessional loans have been provided in 2020, overall, grants represent just 1.4% of ODA commitments from the international financial institutions. Even if concessional (i.e. on favourable lending terms), these loans carry significant implications because clients (particularly governments) must eventually pay them back. So while this aid may benefit countries in the short term, it can also result in a heavy debt burden which countries may not be able to manage, especially where unforeseen events occur. There have been many calls for eradicating all debt held by the poorest countries. Even prior to the fallout from COVID-19, the IMF found that 36 of 70 low-income countries (LICs) were at high risk of debt distress, or already in debt distress. Many countries have since turned towards debt restructuring, and the pandemic has forced countries to make the difficult trade-off between investments in health and social welfare, versus addressing debt (IMF, 2021).
ODA recipients: by sector and by country income level
Which sectors benefit?
Support continues to vary significantly by sector. With the onset of COVID-19, the social sector (including health, education, social infrastructure and services) took centre stage. Social infrastructure commitments by the international financial institutions comprised only a small portion of resources compared to physical infrastructure investments prior to COVID-19. This picture changed dramatically in 2020, when the largest increase in commitments was for the social sector, as measured by percentage change in share of total ODA, especially from international financial institutions. These increases have largely come at the expense of investments in transport, storage, energy and industry. Moreover, worryingly, investments in water and sanitation – critical for the COVID-19 response – fell (Dodd, Breed & Coppard, Reference Dodd, Breed and Coppard2020).
Which countries benefit, by income level?
Historically, ODA commitments from international financial institutions tend to be delivered to lower-middle and middle-income countries rather than lower-income countries; and this trend is likely to continue. The reasons behind this are linked to a number of factors: precedence; project continuity (hence once a client, always a client); the ability of larger and typically more developed countries to borrow and attract higher volumes; and extenuating circumstances (for example, natural hazards or political strife) which can delay or defer support to smaller and/or poorer, less developed countries. In 2019, as a proportion of the international financial institutions’ commitment, middle-income countries received 83% while lower-income countries received 11% (Dodd, Breed & Coppard, Reference Dodd, Breed and Coppard2020). Commitments to high-income countries (HICs) and upper-middle-income countries (UMICs) rose between March 2018 and February 2019 before stabilizing or falling only marginally between March 2020 and February 2021, while commitments consistently fell across 2018 to 2021 for LICs (Knox & Jalles d’Orey, Reference Knox and Jalles d’Orey2021). While it is important to carefully consider the product type (for example whether ODA comes through grants or loans), it is clear there are significant differences in commitment volume across-country income groups.
ODA’s role in the first years of the pandemic
Financing for sustainable development, marked by the inability to fulfil the SDGs, was in short supply even prior to COVID-19 (OECD, 2018). COVID-19 has added new development challenges while simultaneously undoing years of progress and forcing the re-evaluation of goals still unmet. In 2020, developing countries were estimated to require US$ 2.5 trillion to respond to the pandemic and associated economic shocks (Georgieva, Reference Georgieva2020; UNCTAD, 2020), yet existing mechanisms will only provide a fraction of this. Governments worldwide have diverted their budgets to address COVID-19, often taking a domestic policy first stance, and external private investments have dropped significantly (OECD, 2020a). Research shows that domestic resource and external private finance including remittances, foreign direct investment and trade, were expected to have fallen by US$ 700 billion in 2020 compared to 2019 (OECD, 2020a). The need for concessional development finance, including from ODA, has never been more acute.
Why ODA remains critical to health financing
In the medium- to longer-term, ODA for sustainable development financing, particularly for health, will remain critical for a few reasons: the magnitude and nature of support required; the need for consistent, reliable funding; and the weakness/failure of other funding mechanisms.
Magnitude and nature of support
Health has typically been underfunded and underinvested in domestically, and thus the foundations upon which COVID-19 responses were built were weak at the outset. In 2019, lower-middle-income country governments spent about US$ 60 per capita on health while upper-middle-income governments spent over US$ 270 (WHO, 2019). This underspend means that additional resources, such as ODA, are required to support the basic functions of health systems and put countries back on track to achieve universal health coverage goals, while also tackling more complex and newer challenges such as COVID-19. The pandemic has also renewed pressure for better preparedness, for which ODA is the most likely funding candidate given its public goods nature and investment returns that will only be seen in the medium- to longer-term.
Consistency and reliability
Governments are scrambling to allocate scarce resources to finance multiple crises, endangering prioritization for health. While economic growth was restored for many parts of the world by the end of 2022, governments will struggle to keep up high spending levels. This trend is even more likely to be mirrored in the health sector with an expected decrease in government health expenditures per capita of 3% in developing countries (Kurowski et al., Reference Kurowski2021). In this sense, ODA, despite forming only a small fraction of all sources of finance, may prove to be the steadiest and most resilient, providing predictability for planning and strategic investments (OECD, 2020b).
Weakness/failure of other funding mechanisms
With increasing levels of poverty and job insecurity, private sources of financing, particularly those made out-of-pocket (OOP) by households, are falling. In almost every country, disruptions in essential health services have been experienced due to both demand- and supply-side factors, with knock-on effects on utilization (WHO, 2020). Worse still, poor households may defer utilizing health care until the sick householder’s health deteriorates irreversibly and to the point of catastrophic expenditure. Other private sources of finance such as remittances can be erratic and sensitive to changes in external circumstances, and subject to statistical inconsistencies between formal and informal channels (Dinarte-Diaz, Jaume & Medina-Cortina, Reference 132Dinarte-Diaz, Jaume and Medina-Cortina2022). Foreign direct investment shows a similar boom and bust pattern – and investments in least developed countries typically see more modest recovery following crises (UNCTAD, 2022). Thus, the public sector will remain a key source of financing, and ODA will become more important in safeguarding the poorest and vulnerable populations in developing countries. This is where MDBs can play an important role.
MDBs: their role in ODA
As introduced above, MDBs are international financial institutions which can play significant roles in channelling and pooling resources, most commonly from developed nations. After the Second World War, they were established in an avowed spirit of collaboration to help finance the development of poorer nations, and to help stabilize and rebuild the global financial system (The Rockefeller Foundation, 2021). The MDB Observers of the DAC are the Asian Development Bank, the African Development Bank, the Inter-American Development Bank, the IMF, the UNDP and the World Bank. Most MDBs declare their vision to end or reduce poverty and inequality, and target investments to strengthen the economy – for example, through public financial management, to support infrastructural development in the transport and energy sectors or funding for the social sectors of education and health, and so on. They have been evaluated as offering a low risk of default for investors because of strong shareholder support from their members, backed by powerful capital structures, high asset quality and strong risk-bearing capacity. MDBs can mobilize capital quickly, making them ideal providers of liquidity and countercyclical support in times of crisis (for example, during the global financial crisis and during COVID-19). In theory, effective MDBs provide loans, which are often concessional (i.e. they have favourable terms, particularly related to interest rates and grace periods); grants, provided free; and technical assistance – all of which can complement core activities and assist governments and other clients in capacity-building activities or implementing policy reforms.
MDB resources have the potential to fill gaps left by governments, and invest in typically underinvested goods, such as global or regional public goods, thus helping to avoid negative externalities and amplify positive externalities. MDBs also act as catalysts for investment because they can use tools such as guarantees to hedge risk in areas that are often underfunded, but which offer significant medium- to longer-term returns and impacts (such as those in health, social protection and education). Further, MDBs can mobilize counterpart funding by governments and cofinancing with other development partners. In countries that are moving from lower to middle-income status, MDBs are thought to be important in filling a transition gap. Research finds that as per capita income rises, ODA in health and social protection declines, but domestic and private spending are not able to fill this gap fast enough and leave a void which can be filled by MDBs (Piemonte et al., Reference Piemonte2019). Further, where domestic governments have started to increase spending, priority is often given to infrastructure, rather than human capital development, leaving this area for MDB assistance. Such countries also exhibit high inequalities that are yet to be addressed, and MDBs are well placed to step in during the transition period.
In the best-case scenario, MDBs adhere to several principles and characteristics to ensure their assistance can be used most effectively and efficiently. For example, they will maintain commitment to the idea of “sovereignty above all else” and ensure that their initiatives align with domestic policies and national goals (see the Assessing ODA quality section for the Quality of Official Development Assistance (QuODA) priority area “ownership”). Such a commitment can help ensure that all projects support – and build on – government strategies. Otherwise, if these are misaligned, ODA can run the risk of shifting financial decision priorities and, in terms of health care for instance, crowd out funding for certain disease areas. Relationships and dialogues between MDBs and governments are, in theory, strengthened through country-based offices that are staffed with both international and national experts whose backgrounds and specialisms are usefully varied.
Second, by having expertise in multiple fields and in multiple countries, MDBs not only have convening and coordination power among sectors, but also across countries, sectors and subregions. This has the potential for several positive knock-on effects. Importantly, it allows for development partners to avoid duplication and attain maximum synergies when thinking through work programmes, which can lead to more efficient use of limited resources. It also allows MDBs to play intermediary roles as poolers of resources, particularly finance, through the provision and management of trust funds. Hence, again, MDBs are seen as providing catalytic financing, including that which leverages private and philanthropic financing. MDBs can actively promote and facilitate the use of instruments such as guarantees, equity investment and blending (private and public funds) to maximize synergies and resources.
Third, MDBs are able to provide the checks and balances in areas that may benefit from additional external support. This includes anticorruption measures, as well as safeguards – for minority ethnic groups, women, children and youth, remote and rural populations, people with disabilities and environmental and resettlement issues. Such checks and balances are reflected in legal agreements and project documents to ensure maximum accountability and transparency in operations.
In summary, MDBs can provide a speedy and powerful mechanism for filling gaps in underinvested areas, providing checks and balances and mobilizing finance and other resources from development institutions and governments.
Evidence in practice: the response of the Asian Development Bank to COVID-19
The Asian Development Bank, one of the largest MDBs, was established in 1966 with goals focused on poverty reduction and improvements in quality of life for all. In more recent years, the bank’s objectives have been closely aligned with the SDGs (ADB, 2018).
When COVID-19 hit, the Asian Development Bank and many other MDBs swiftly committed resources to try to fill gaps in response and recovery efforts.
In mid-March 2020, the bank announced a US$ 6.5 billion COVID-19 response package which was increased to US$ 20 billion by mid-April 2020. As part of the package, the bank expanded resources available for nonsovereign operations and established the COVID-19 Pandemic Response Option (CPRO) under the Countercyclical Support Facility. CPRO resources were used to help governments implement countercyclical expenditure programmes to mitigate the impacts of the pandemic, with a focus on the poor and vulnerable. In December 2020, the bank announced that it would provide an additional US$ 9 billion for the Asia Pacific Vaccine Access Facility (APVAX) to help with COVID-19 vaccine procurement and vaccination programme implementation. In sum, the Asian Development Bank’s commitments in 2020 increased by 33% compared to 2019, with a record US$ 31.6 billion in 2020 (up from US$ 24 billion in 2019), both to governments and to the private sector. Approximately half (US$ 16.1 billion) of this was tagged for COVID-19 response.
Type of support offered
The Asian Development Bank’s range of products is separated into regular ordinary capital resources (comprising loans, equity investment and other debt securities), concessional resources (loans and grants) and other special funds (grants only). Contrary to the general landscape of ODA which saw declines in grant resources, the volume of grants disbursed by the bank increased significantly from US$ 514 million in 2019 to US$ 877 million in 2020. Partly due to this, the net resources transfer (the net amount of disbursements in excess of payments of principal, interest and other charges) to Developing Member Countries more than doubled between 2019 and 2020. The bank also provided a record US$ 41.6 million in technical assistance resources in 2020 for medical equipment, personal protective equipment and advisory services.
Which sectors benefited?
The portfolio of approved projects changed significantly owing to COVID-19. Pre-COVID-19, heavily committed sectors were classed as transport, finance and public sector management, with health ranked as the second smallest standalone sector (with commitments totalling just US$ 644 million in 2019). With COVID-19, health operations increased more than fivefold, becoming the fourth largest by volume of 11 sectors behind public sector management, finance and energy. As a share of the total Asian Development Bank portfolio, the health sector accounted for over 11% of the bank’s commitments in 2020, significantly exceeding its target of 3–5% set in the Midterm Review of Strategy 2020. Such trends follow those found in the general ODA landscape introduced earlier.
Which countries benefited, by income level?
The increase in commitments resulting from the COVID-19 response, especially between 2019 and 2020, is reflected in increases in support to all countries, but lower-middle-income countries have benefited the most. In 2020, 67% of the Asian Development Bank’s portfolio was found to have supported lower-middle-income countries (versus 0.2% to HICs, 28% to UMICs, 4% to LICs and 1.2% to the regional portfolio), reflecting their larger economies and higher absorptive capacities. Such trends are consistent with general ODA trends which showed commitments consistently fell across 2018 to 2021 for LICs, with larger volumes supporting middle and HICs.
Policy relevance and conclusions
Factors to consider when assessing ODA as a financing instrument
The concept of ODA – providing government aid to promote and target economic development in countries which need it – is fairly straightforward; however, measuring how successful ODA is executed in practice, and to the extent to which they contribute to sustainable development, is not simple. Some tools are offered here by way of example only.
Assessing ODA quality
The QuODA index summarizes four dimensions comprising: prioritization; ownership; transparency; and evaluation to consider when analysing aid effectiveness (Mitchell, Calleja & Hughes, Reference Mitchell, Calleja and Hughes2021). Prioritization measures how well allocations are targeted to respond to long-term development challenges. Ownership demonstrates how well providers work with countries to ensure ownership and use of national systems. Transparency considers how timely and comprehensive reporting on ODA activities are; and evaluation assesses quality of learning and evaluation systems.
In its most recent assessment referring to aid distributed in 2019, QuODA placed multilateral organizations at the top of overall rankings, scoring highly on all four dimensions. Nearly all resources provided by multilateral organizations reach their intended recipients, with a focus on the poorest and “under-aided” countries (Mitchell, Calleja & Hughes, Reference Mitchell, Calleja and Hughes2021). Recipient countries promote domestic ownership and use of national systems, while untying their procurement practices from domestic contractors. Authors also find that donors that provide the most, also produce the highest quality of aid (Mitchell, Calleja & Hughes, Reference Mitchell, Calleja and Hughes2021). Such trends are largely driven by Scandinavian and northern European providers, who are known for their strong commitment to development finance and impact (Mitchell, Calleja & Hughes, Reference Mitchell, Calleja and Hughes2021).
Such indices provide a partial response to critics of ODA systems, who argue that to improve efficiency, accountability, performance and equity impacts of ODA, more detailed descriptions of financing are needed (McCoy et al., Reference McCoy2009). Critics argue that the landscape is so complex and involves so many stakeholders who are currently not accounted for (for example, non-OECD donors and funds, private sector, philanthropists, etc.) that the current system does not do a good job of tracking and monitoring aid activities. Indeed, the COVID-19 pandemic has shown that multiple stakeholders, not just public sector actors, are critical to overcome global challenges and their financial contributions should be reflected accordingly.
Impact at the organizational level
For donors, the professed priority is to ensure that their resources positively change the lives of those who need aid the most. Organizations, including MDBs, carry out regular evaluations by both internal project officers and independent, external others. Commonly, a systematic tool is deployed to monitor impact, for example, logframes. The extent to which projects are successful can generally be summed up across four aspects: relevance, sustainability, efficiency and effectiveness.Footnote 5 Relevance measures whether projects align with country and organizational strategic priorities. Sustainability evaluates if outcomes and outputs may last beyond project completion. Efficiency looks at the use of resources to achieve intended outcomes. Effectiveness refers to the extent to which outcomes and outputs were achieved. Achieving balance between these aspects and applying lessons in the pursuit of the SDGs is an ongoing challenge, in the light of financial considerations such as ensuring high disbursement rates.
Effect of COVID-19 on MDB operations and their health sectors
COVID-19 and its after-effects has given rise to new challenges – especially for MDBs working in the health sector – and will have long-lasting effects on how MDBs operate, and their place in the ODA sphere. Since 2020, not only has ODA been required to support developing countries in their urgent COVID-19 response, but it has also been needed to support medium- to longer-term health goals. For some MDBs, this required a recasting of corporate strategies to give a higher priority to health and social sectors since COVID-19 has taken centre stage in many developing countries in the last few years, even as investments have moved from emergency response towards more longer-term, sustainable outcomes.
In the health sector, increased investment to boost capacity to prevent, detect, and treat COVID-19 (including contact tracing, testing, vaccines and vaccinations, and therapeutics) has been critical. Now the focus has turned to mainstreaming COVID-19 as part of communicable disease control with an emphasis on primary care, basic infection prevention control and strengthening laboratory networks. Restoration of health services which were severely curtailed during the height of the pandemic, and clearing the backlog of missed appointments and surgeries is the first priority. At the same time, as the science evolves and longer-term effects of COVID-19 become better known, the health system will need to cope with the virus’s detrimental consequences on physical and mental health.
In addition to disease control, addressing COVID-19 fully requires countries to focus on various newer areas, including medium- to longer-term vaccine supply for boosters and further R&D to provide these; genome sequencing; vaccination logistics; health data management; and digital or e-health including telehealth, among others. Investments in pandemic preparedness (still an underinvested area) are also required to help avert and mitigate future catastrophes. This, in turn, will require reforms to public financial management including the allocation of funding to health, but which go beyond the health sector alone.
COVID-19 has both highlighted and intensified health-related inequities across ethnicities, sexes, ages and within and across countries; addressing these divides will pose one of the most difficult challenges for the health sector, which must work harder to address the causes of health inequities that lie within its control, and the impacts of those root causes which lie beyond its control. Resources are required to increase access to health care for all – which calls for more outreach, better financial protection and increase in quantity and quality of health care in typically underserved areas. Critically, countries will need to increase cooperation to redistribute resources, recognizing that global public bads can only be controlled when everyone gains access to vaccines and treatments.
The development community will need to take a multisectoral and whole-of-government approach to cross-sectoral concerns. Provision of the following, and more, is needed: basic water supply and sanitation; safe and nutritious food; and clean air and safe environments. Investments to improve the quality of health infrastructure, especially green facilities, will require close coordination with environmental experts; a pivot towards patient-centred care and improved quality of health human resources will require more emphasis on health education and training; and addressing zoonoses will require increased research and cooperation with the agricultural sector. Accordingly, ODA must shift from a sector-by-sector approach towards addressing challenges along salient trends and themes.
Conclusions
This chapter has analysed what ODA is, why it is important and its major trends, highlighting health ODA trends. It has focused on MDBs as critical ODA players, using a case study of the Asian Development Bank and its experience in financing COVID-19 response and recovery. ODA remains the main source of international development financing for many developing countries, and has proved its worth by stepping up during the COVID-19 pandemic. The DAC mechanism enables a consensus-led, concerted effort to deliver aid to those who need it the most, while supporting the monitoring of the quality of public spending and investments. However, the true test of ODA is whether resources have had a meaningful impact on development outcomes: while this chapter has touched on ODA volumes, effectiveness and its measurement with regards the health sector, focused research is required to fully comprehend medium- to long-term results and support evidence-based policy-making across multiple sectors and themes. This will become more salient as the world tackles other challenges such as the climate crisis and food insecurity. The Asian Development Bank and other such agencies must continue to build on the successes from the COVID-19 response, and stand ready with increasingly plentiful, innovative and agile financing mechanisms.Footnote 6
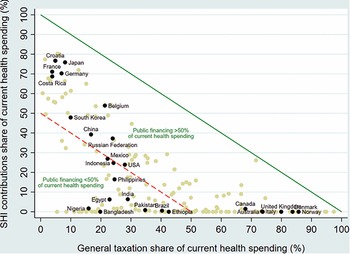
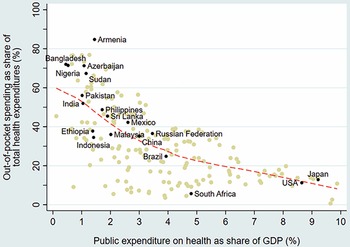
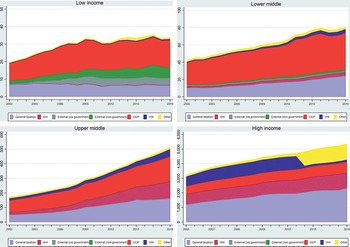
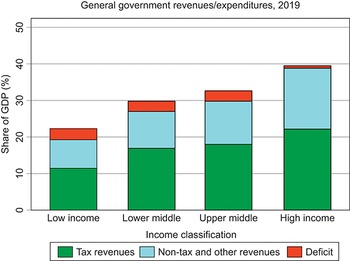

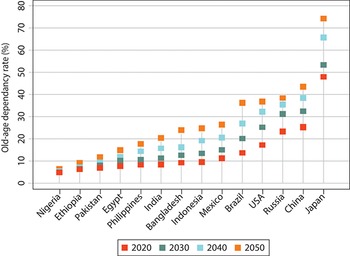
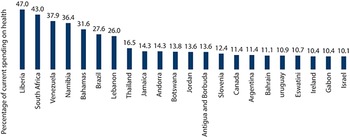
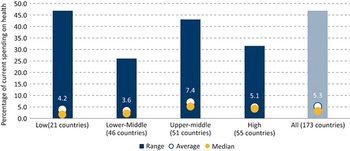
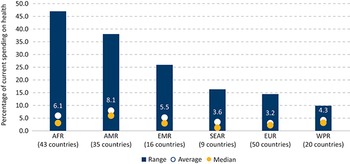
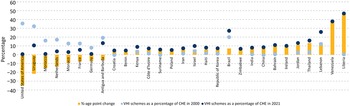
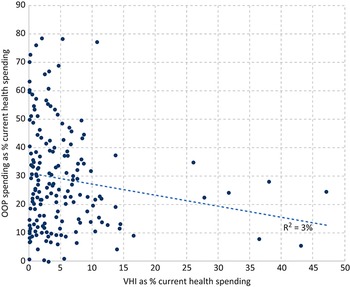
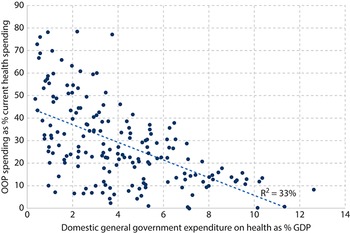

 Open access
Open access