

Introduction
Following the birth of my first child and the prospect of a changed career trajectory, I became involved with women doctors’ organisations both nationally and internationally. I was President of the UK Medical Women’s Federation from 2010–2012, and in 2012 became the Medical Women’s International Association (MWIA) representative to the World Health Organization. The latter made me realise the importance of violence against women and girls (VAWG) and that doctors should become involved, especially with prevention. Essential elements in prevention include the education of boys and girls in schools to develop healthier relationships, the education of health professionals to recognise the problem, and establishing how best to deal with perpetrators.
When I was MWIA President-elect (2016–19), MWIA carried out a survey of its members on Sexual Harassment which showed the extent of the problem among health professionals. In 2017 I organised another survey of MWIA members on Priorities for Medical Women, and sexual harassment was one of the five top priorities for women doctors. I spoke extensively on these subjects at the UN, at the WHO and in various countries around the world.
In 2021, as one of two health representatives on the Policy Committee of the UK Women’s Equality Party, sex and gender in relation to health, as well as VAWG and sexual harassment, were extensively discussed.
Overview
In the UK, the definition of sexual harassment was clarified by the 2010 Equality Act. It centres on behaviour that makes an individual ‘feel humiliated, offended or degraded’ and on ‘unwanted behaviour of a sexual nature’, which encompasses sexual jokes, touching, and sending emails of a sexual nature or putting up pornographic pictures; a claim that a comment was made in jest or as a compliment is not a defence.
The essence of sexual harassment is that:
a) the conduct is of a sexual nature
b) the conduct is unwanted.
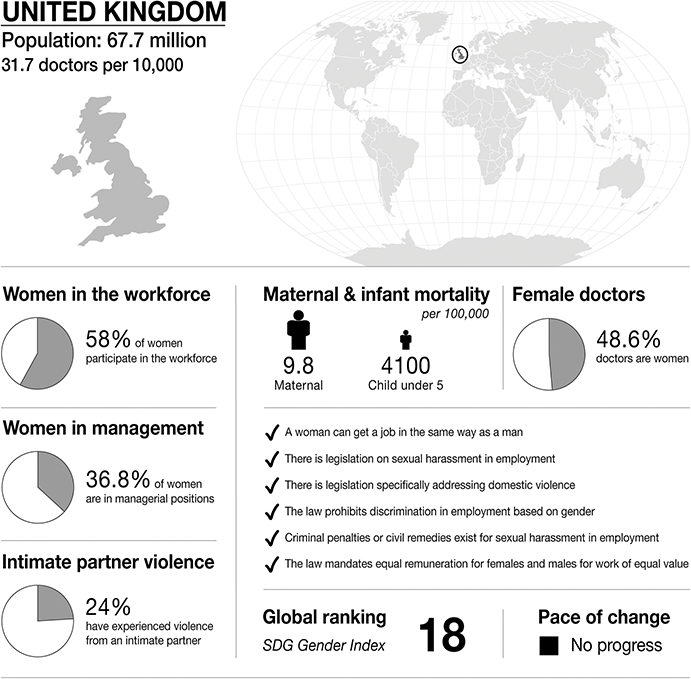
Infographic United Kingdom. Infographics were provided by CartoGIS Services, The Australian National University. Population: from World Bank https://databank.worldbank.org/source/population-estimates-and-projections. Sustainable Development Progress, global ranking and statistics on women in the workplace, women in management and intimate partner violence: from United Nations SDGs Data Portal https://unstats.un.org/sdgs/dataportal. Female doctor percentage: from Global health workforce statistics www.who.int/data/gho/data/themes/topics/health-workforce. Legislation and law statements: from the World Bank gender data portal 2023 https://genderdata.worldbank.org/en/indicators. Maternal mortality statistics: from the Global Health Observatory 2020 https://mmr2020.srhr.org. Infant mortality statistics: from United Nations International Children’s Fund (UNICEF) https://data.unicef.org/topic/child-survival/under-five-mortality.
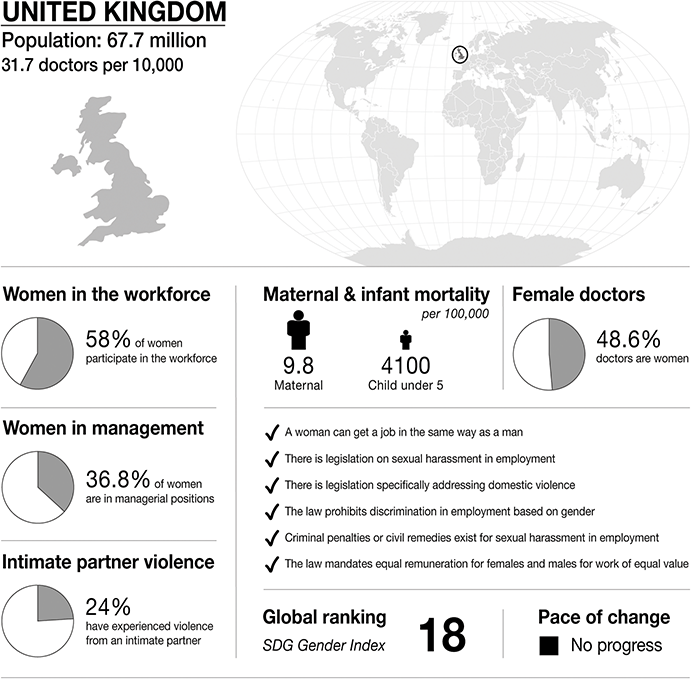
Figure 28.1 Long description
The infographic provides information about the United Kingdom, with a population of 67.7 million and 31.7 doctors per 10,000 people. It highlights several gender-related statistics. 58 per cent of women participate in the workforce. 36.8 per cent of women are in managerial positions. 24 per cent of women have experienced intimate partner violence. Maternal mortality is 9.8 per 100,000. Infant mortality under 5 is 4100 per 100,000. 48.6 per cent of doctors are women.
The infographic lists the presence or absence of law and policy on gender equality. In the United Kingdom:
– a woman can get a job in the same way as a man.
– there is legislation on sexual harassment in employment.
– there is legislation specifically addressing domestic violence.
– the law prohibits discrimination in employment based on gender.
– criminal penalties or civil remedies exist for sexual harassment in employment.
– the law mandates equal remuneration for females and males for work of equal value.
The S D G Gender Index global ranking is 18, and is stable
Certain hallmarks repeat themselves over and over again in cases of sexual harassment, sexual assault, rape and domestic violence – women and children are made to feel complicit by their abuser; the entirely rational fear of not being believed; the humiliation of coming forwards with an account of what happened; the knowledge that reporting an abuser in a position of authority – given the power he wields not just over the victim but those around them – may only make things worse.
Quoting American author Ursula Le Guin, ‘The power of the harasser, the abuser, the rapist depends above all on the silence of women.’
In 2016, the Trades Union Congress (TUC) in the UK issued its report ‘Still a bit of banter?’, which concluded that 52% of women at work suffered sexual harassment and that 80% of them did not report it. (1)
In June 2019, Unison published its NHS survey ‘It’s never OK’, which disclosed that the vast majority of those targeted were women (81%) and the incidents mainly involved perpetrators older than their target (61%), who were often in more powerful roles (37%). Nearly a third (31%) of those who had been sexually harassed said it occurred on a regular basis, and more than one in ten (12%) said it occurred weekly or daily. (2)
At the start of the #MeToo movement in 2018, many men expressed surprise at the number of women who had been the victims of sexual harassment. In 2017/18 a survey done by the Medical Women’s International Association revealed that 34% of women doctors suffered sexual harassment at work. For 22% of these, their job or future job depended on performing unwanted sexual behaviours. Fifty-two per cent said that someone was coming unnecessarily close in a physical or sexual way, and 62% received comments on appearance in an unwanted or sexual way. In 15% of cases, the women doctors were coerced to have physical contact that was unwanted or sexual, and 5% were coerced to have more serious sexual encounters, including rape.
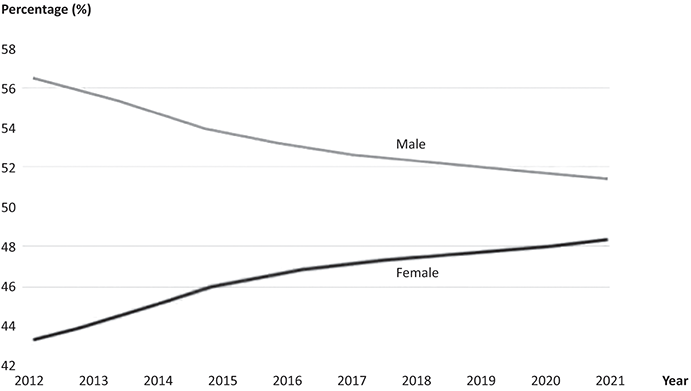
In the UK, the gradual increase in the proportion of licensed doctors who are female has continued towards parity with male doctors but has slowed in recent years (figure 28.2). (3)
Women in medicine in the UK.
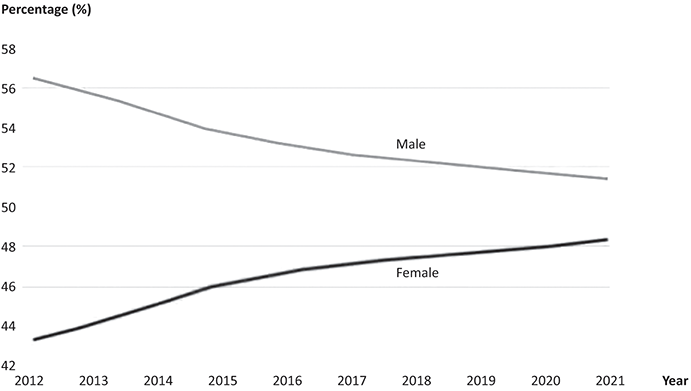
Figure 28.2 Long description
'The graph shows Percentage from 42 to 58 on the y-axis, and years from 2012 to 2021 on the x-axis. Line 1, Male: Starting at approximately 56.5 percent in 2012, the male percentage shows a steady decline over the years. The line decreases gradually, reaching about 51.5 percent by 2021. Line 2, Female: Beginning at around 43.5 percent in 2012, the female percentage demonstrates a consistent increase throughout the period. The line rises steadily, approaching 48.5 percent by 2021.
There is currently in the UK an almost equal balance of men and women joining the workforce each year. More women are entering medical school (64% of the medical student intake was female in 2021). This is largely counterbalanced by the increase in the number of international medical graduates (IMGs) whose primary medical qualification is from outside the UK and European Economic Area, who are mostly male. All specialties had an increasingly female composition between 2012 and 2021. The highest proportion of female doctors is seen in obstetrics and gynaecology (60%), followed by paediatrics (58%), general practice (57%), and public health (55%). The lowest proportion of female doctors is seen in surgery, which was 15% female in 2021, up from 9% in 2012. (3)
The number of IMGs in the UK has increased by 40% in the last five years (from 58,222 in 2017 to 81,457 in 2021) at a time when the number of UK graduates in the workforce has increased by 10% (from 162,634 to 178,173). The number of associate specialist doctors has grown at almost six times the rate of general practitioners in the last five years and four times the rate of consultants.
Women in Surgery
There remains in the UK a large gap between the numbers of women who go into training and those that become consultants, especially in surgery where there is a high drop-out rate. In 2018, 54% of foundation trainees in surgery were women, dropping down to 12% of consultant surgeons. (Reference Moberly4) The surgical specialties with the highest representation of female registrars are ophthalmology (50%), otolaryngology (48%), and paediatric surgery (45.5%), while the lowest are trauma and orthopaedics (21%), cardiothoracic surgery (21%), vascular surgery (25%), and neurosurgery (25%). (5)
It has long been an ‘open secret’ that surgery and surgical training have a problem with sexism, ranging from ‘bad jokes’ to sexual assault and even rape. (Reference Fleming and Fisher6)
Women in Universities and Academia
A poll of 56,499 university students in 2019 (7) showed that more than half said they had experienced unwanted advances and assault, including rape, with only 8% reporting the incident to the police or their university. Nearly two-thirds of the women surveyed said they did not feel confident in saying no to sex for fear doing so might lead to violence.
‘Unsafe spaces: ending sexual abuse in universities’ (Reference Tutchell and Edmonds8) highlights the role of the ‘lad culture’ in students’ sports clubs – especially rugby clubs – in creating a toxic atmosphere leading to sexual abuse and harassment, with abusers adopting a ‘pack mentality’. It also shines a light on sexual harassment and abuse by staff, including distinguished academics, where universities can be reluctant to take action because they want to keep their star performers.
In the wake of the Harvey Weinstein scandal in 2017, Dr Karen Kelsky, the originator of the #MeTooPhD hashtag, looked at the extent of the problem of sexual harassment across academia. (Reference Kelsky9) She set up a spreadsheet, allowing individuals to share their experiences. There was an overwhelming response with reports of violence, manipulative behaviour and sexual harassment.
The biggest surprise, the biggest insight that I gained from doing this spreadsheet is that it is really a false dichotomy to claim that there are serious incidents such as sexual assault and less serious incidents … .What I am interested in are the 40 women or the 100 women or the 1000 women – and we don’t know how many – that one man may have victimised and what they did not achieve because of him.
In 2018 in the UK, the Wellcome Trust announced that universities must now report findings of sexual misconduct investigations, and that the Trust will consider withholding funding from academics who have been found guilty of bullying or harassment. However, there are concerns that universities could settle complaints informally to hide problems, or that false claims could penalise innocent researchers. The effectiveness of the policy will rely on institutions being transparent. Researchers are under extreme pressure to bring in grants and publish research papers, providing a fertile breeding ground for bullying and harassment. ‘If an institution has someone bringing in huge amounts of overhead and publishing in prestigious journals, are they really going to take action against them if they are a bully? I think not’, said an Oxford academic. (Reference Else10)
Sexism in Medicine
Nine in ten female doctors have experienced sexism at work in the UK, including unwanted physical contact (31%), denial of opportunities and being asked to massage male colleagues in meetings. These findings emerged from a survey of doctors, which was a collaborative effort between the British Medical Association and Dr Chelcie Jewitt, a trainee hospital doctor and founder of the Sexism in Medicine campaign. (Reference Politis11) Over 70% of female respondents felt their clinical ability had been doubted or undervalued because of their gender. Fifty-six per cent of women had received unwanted verbal comments related to their gender. Forty-two per cent of doctors who had witnessed or experienced sexism felt they could not report it.
Hewitt and a GP colleague have launched a website where doctors can feel safe to talk about their experiences. Raising awareness is the first step, followed by campaigning for change.
Medical Regulation
Data obtained by the Independent newspaper in 2022 showed that between 2016 and 2020 an average of twenty-eight doctors have been sanctioned each year by the General Medical Council (GMC), which regulates more than 350,000 doctors in the UK, after allegations of sexual misconduct were proven against them. These figures probably reveal ‘the very tip of the iceberg’ in terms of the actual levels of sexual assault within health care (12; 13).
The majority of these doctors were erased from the register, meaning they lost their licence to practise. Of the proven allegations, forty-one were made by another health care professional, forty-two by a patient, and the remainder were unknown.
A doctor who has been erased cannot apply to be restored to the medical register for five years. At that stage, a tribunal will have to decide whether the doctor is fit to resume unrestricted medical practice.
In addition to the erasures, several doctors were suspended from the register after hearings for alleged sexual assault. The maximum suspension is twelve months. In deciding the length of the suspension, the GMC considers the seriousness of the findings of the investigation. A warning is issued if a doctor’s behaviour departs significantly from the GMC’s Good Medical Practice but restriction on registration is not necessary.
How Easy Is it to Bring a Case of Sexual Harassment to an Employment Tribunal in the UK?
Leaving aside sexual assault, which would be dealt with in a criminal court, harassment cases are brought under the Equality Act. Unfortunately, that tends to be one person’s word against another. It is then a case of looking at corroborative evidence, for example email correspondence or diaries, and asking whether the victim contacted human resources and raised a grievance. A lot of cases settle before they get to court, a level of compensation might be paid, other measures might be put in place. There is a great deal to be gained by resolving it as soon as possible. It is now the job of institutions to take responsibility for this.
Case Study
Instead of an individual case study of sexual harassment or abuse, I am going to discuss what happened in 2019 at the British Medical Association (BMA), the body which represents and stands up for doctors in the UK.
October 2019 was not a good month for the BMA. Headlines in the national and medical press with comments like ‘dark dinosaur infested depths of the world of GP politics’ and ‘Female doctors groped, propositioned and harassed by senior male colleagues in BMA’ shook the medical establishment.
An article written by two prominent women general practitioners (GPs) on the BMA General Practitioners’ Committee (GPC) had been published in GP online. (Reference Bostock14) GPC meetings take place once a month, with an overnight stay before the meeting for those who live far from London, and a dinner that evening. There seemed to be a lingering feeling of entitlement among some doctors, particularly towards younger women doctors and members of staff, which tended to emerge during drunken events such as conferences and dinners. Incidents included being touched inappropriately, lewd and inappropriate sexual remarks directed to or made about women, invitations or even instructions to accompany a male doctor to his hotel room, staring at a woman’s breasts, and inappropriate comments about a woman’s appearance. One senior woman on the GPC said that she felt unable to attend evenings of drinking and fine dining away from home without a family member to accompany her, after being propositioned by a male colleague.
It became clear that, as in many other spheres, there is a major problem with sexual harassment at the BMA, and a culture insensitive to gender equality.
The BMA commissioned a leading Queen’s Counsel (senior lawyer), Daphne Romney to investigate and to write a report on sex discrimination, sexual harassment and bullying within the BMA. (15) For many doctors it was very welcome.
The review revealed a culture in which women (doctors and staff) were bullied, undermined, and in some cases sexually harassed. It criticised the discriminatory culture at the BMA and the leadership for failing to call out bad behaviour. The allegations prompted other doctors to speak out. Since they spoke out, some of the women have been subjected to deeply unpleasant behaviour and allegations. One of the women doctors called for those responsible for the behaviour or for perpetuating it to consider leaving their posts to allow a culture change at the Association. The alleged perpetrators were not named in the report.
This is not just a GP committee problem. On GPC England, men outnumber women by two to one, although 54% of GPs are now women. On the Consultants’ Committee, women make up 25% of the committee although 37% of consultants are women. On the Staff and Associate Specialists’ Committee, men outnumber women by ten to one, although that branch of practice has roughly equal numbers of men and women.
As Romney says in her Report:
The majority of men in the BMA are not sexist or sexual harassers, and every committee is not riddled with discrimination, but problems with culture remain. There are now equal numbers of men and women in medicine, and we need to reflect that change by leaving that ‘old boys’ club’ culture behind, and embracing a forward looking, modern and equal world.
Living Our Values (LOV) and the Resolution Process
‘Living Our Values’ was incorporated in a Code of Conduct and a disciplinary procedure, now known as the Resolution Process, at the BMA in 2017. The Code was introduced to deter and also to deal with bad behaviours. It was rolled out to BMA committees to raise awareness of the union’s core values and expectations of staff in terms of behaviour.
The Code of Conduct should have dealt with the issues raised by the women GPs. However, it was abused and weaponised and not used as it should have been. Had it worked properly we would not have needed the Daphne Romney Report.
The Resolution Process has been used successfully to resolve many informal complaints, and to resolve some substantial complaints through the formal route, with adjudication by a panel of three doctors. However, the process has been undermined; there is a perception that the process is not effective (because its operation is shrouded in secrecy), and many perceive its application to be partial, which has deterred them from using it. Others have chosen not to use it because they are frightened of repercussions, and in the case of some staff, of losing their job.
Daphne Romney made thirty-one recommendations. The recommendations include education on equality, diversity and inclusion, a helpline for staff facing sexism or discrimination, an external independent complaints service, bespoke face-to-face training for all committee members, and mandatory training for committee chairs.
There must be a policy of zero tolerance, and there must be consequences for the perpetrators, once proven ‘guilty’. The BMA must have proper sympathetic reporting structures, and good collection of data. The current systems in place, including Codes of Conduct and the inappropriate acronym ‘LOV’ (‘Living our Values’), are inadequate. They are felt to be intimidating and unsupportive. Institutions should convey that reporting sexual harassment is important and courageous.
BMA committees should introduce quotas or minimum numbers of women in order to better reflect the percentages of men and women in each branch of practice. Daphne Romney accepted that quotas are very unpopular with some, but years of diversity reports and recruitment attempts have not managed to even out the gender balance on the major committees, particularly on the Staff and Associate Specialist Committee. She regarded this as a temporary measure to change the culture, perhaps for ten years, when hopefully the balance will change.
Members of committees should be prevented from standing for re-election for that committee after twelve years unless they hold an executive position. This will allow new members onto the committee. Members may seek re-election to that committee after three years. When I was on the GPC, some committee members had been in post for twenty-five years!
BMA members should be restricted in the number of committees they can sit on.
The BMA must ensure that there is adequate support, counselling and protection for the complainant and ensure that he or she is not victimised for having made a complaint. I have personally tried to speak with the GPs involved in the initial revelations, but most are reluctant to discuss the matter at all.
Existing strategies to tackle bullying, undermining behaviour and harassment focus on changing behaviour in the victim. It is more useful to focus on prevention, rather than mitigating strategies.
In spite of all the initiatives that have been introduced, the current methods for tackling mistreatment are perceived as ineffective and potentially damaging to victims.
The BMA Network of Elected Women (NEW) was set up in 2019. It is a group of BMA-elected medical women who aim to champion and strengthen female leadership and advance diversity for the benefit of the Association. The collaboration of different voices at all levels and from all backgrounds is key to unlocking women’s collective potential. There is now an informal WhatsApp group, a formal list server, a book club, and an after-school club, and webinars are planned.
A parallel and informal group of male allies (Active Allyship) has been established, which is separate but complementary. They advocate for greater gender equality at the BMA. Bystander training (see later) is planned as one of their activities, with a national programme carried out at a regional level.
What Has Been the Effect of the Daphne Romney Report?
Some senior members of the BMA said ‘How dare you raise this?’ when the women GPs went to the press. It was said that the BMA Code of Conduct should have been used, but the women doctors involved had no faith in the current processes.
It is now easier to acknowledge that sexual harassment is an issue. The Report has given women the support to speak up. It is interesting that there was resistance to setting up the Report in the first instance.
The current mandatory online training models are seen as ineffectual – people look up ‘correct’ answers and unthinkingly comply. Existing training sessions in diversity and equality are not taken seriously, especially by those who need them. I remember well when I was on the GPC from 2007 to 2012 the ‘nudging’ and jokes made during the equality and diversity sessions that we were required to attend. During a discussion on perceived lack of gender balance, there were eye rolls, and uncomfortable grunts in the GPC chamber.
Although doctors agree that some progress has been made since the Romney Report, more needs to be done to improve the situation. (Reference Limb16; 17) Since the publication of the Report, several women doctors have risen to leadership positions on committees, including the first ever female Chair of the GPC, and have had a very difficult time. The problems are far from over.
Discussion
It is clear that, in spite of all best efforts, sexual harassment remains a significant problem for women in medicine in the UK and worldwide. Women alone sharing their stories through websites, chat groups, spreadsheets, etc. is not enough. Formal policies have been in effect for years, but sexual harassment has not significantly decreased. Although robust organisational processes are necessary, they are insufficient to change cultures.
Systemwide change is needed, not only reporting and punishing offenders after the event. That approach leads to symbolic compliance with current law and avoiding liability but does not prevent sexual harassment. Institutions should have to report sexual harassment findings. It should be considered a form of scientific misconduct.
Bystander Training
It has been suggested that the profession must also articulate the ethical obligations of individuals who witness harassment and inequitable treatment. (Reference Mello and Jagsi18) In their New England Journal article in 2020 ‘Standing up against gender bias and harassment – a matter of professional ethics’, Mello and Jagsi stated that health professionals have a moral duty to intervene as bystanders (‘upstanding’). (Reference Mello and Jagsi18) This obligation should be described in codes of medical professional ethics and supported with institutional training. Bystander intervention is especially useful for conduct that is not severe or sustained enough to trigger institutional investigations. Witnessed incidents abound in the profession, and upstanding is therefore critical. Bystanders are more likely to intervene if they believe their organisation has effective mechanisms for addressing the problem.
Bystanders often have multiple, idiosyncratic, and conflicting interests, and experience painful dilemmas. How can they be supported to be more effective when faced with unacceptable behaviour? Rowe has some practical advice in ‘Fostering constructive action by peers and bystanders in organisations and communities’. (Reference Rowe19)
Potential responses to observed instances of sexual harassment and gender bias:
1. Document details of behaviours in a diary for possible future use. For example ‘10/3/19, 11.00: JB stated during surgery that female surgeons “are never good under pressure”.’
2. Remove the target from the situation. For example, ‘Mr King, I’m going to have Dr Target assist with another patient.’ ‘So sorry to interrupt – I really need Dr Target’s help in exam room 5.’
3. Provide support privately to the target of the behaviour. For example ‘I thought what he said was unacceptable, and I’m really sorry it happened. How are you doing? What can I do to support you?’ ‘I wanted to check in with you. Has Jim caused any further problems for you?’
4. Ask civil but pointed questions of the perpetrator in the moment. For example, ‘Do you really mean that?’, ‘What do you mean by that?’, ‘It sounded like you were saying … .’
5. Deflect the behaviour using humour.
6. Express disapproval of the behaviour to the perpetrator in a private setting.
7. Engage others to help deal with the behaviour if it recurs.
8. Name the behaviour as unacceptable on the spot.
9. Report the perpetrator to the institutional sexual harassment officer.
10. Remove the perpetrator from duties that might prompt a recurrence of the behaviour.
True culture change will occur more quickly if combating harassment is recognised not just as an institutional responsibility, but also as a personal ethical obligation of every health professional.
Prevention
Unfortunately, it is difficult to demonstrate that preventive measures are effective. Schemes therefore receive little or no investment.
The key is to start in schools.
Girls and young women aged between ten and twenty-four are more likely to be victims of sexual offences recorded by the police than older women. (Reference Jones, Farrelly and Barter20) According to a 2020 Government report, one-third of all female victims recorded by police were under fifteen years old.
Sexual harassment of girls is rife in schools but largely goes unreported and unaddressed. A 2017 report revealed that 37% of female students in mixed sex schools have personally experienced some form of sexual harassment, 24% have experienced unwanted touching of a sexual nature compared to 4% of boys, 58% of female students have experienced or witnessed sexual harassment at school, 66% have experienced sexist language. (21; 22) Many teachers feel ill-equipped to tackle the issue. Female teachers also experience harassment by pupils.
In 2020 the government introduced compulsory age-appropriate Relationship and Sex Education in all primary and secondary schools. (23) This is definitely a step in the right direction, but much remains to be done to improve it.
Sexism and Misogyny
Laura Bates founded the Everyday Sexism project in 2012, (Reference Bates24) inviting women on social media to detail sexist encounters they had had. In 2014 she published the book Everyday sexism: the project that inspired a worldwide movement. Bates was surprised at how many of the accounts came from girls in their mid-teens. She herself received torrents of abuse, including graphic rape and death threats.
Over the last five years she has concentrated her efforts on her work in schools. In 2018 ‘something changed’.
I started hearing boys coming out with some quite extreme things: feminism is a cancer, all women lie about rape, white men are the real victims of society … But the moment it really clicked for me was when they started repeating, at schools from rural Scotland to inner city London, the same wrong statistics.
This began her journey into the manosphere, posing as ‘Alex’, a confused young man looking on Reddit, and elsewhere, for answers. This took her from the Incels (Involuntary Celibates) to the MGTOW (Men Who Go Their Own Way). She went undercover to an MRA Conference (Men’s Rights Activists). It was a chilling experience. ‘The reality was that these are men you might walk past in the street’. The list of MRA grievances is long. They include the low attainment of some boys in schools; male suicide as a leading killer of men under fifty in the UK; higher levels of women entering higher education in some countries; male circumcision, or MGM; and the lack of provision for male victims of domestic violence. Other big issues are child custody, and false accusations of rape and sexual assault. Bates writes that these grievances are interpreted as attempts by feminists to control men’s lives. ‘At its simplest, the argument goes like this: if women’s sexual autonomy has given them wicked and tyrannical control over men’s lives, then women’s liberation is at the root of all male suffering. Therefore, the obvious remedy is to remove women’s freedom and independence and to use specifically sexual means … to do so.’ (Reference Bates25)
What came out very clearly in her research was that we were looking at hundreds of thousands of people, millions of views, so many different websites and forums. We are talking about a massive network.
The point Bates makes is both stark and subtle: there is a live community of violent extremists, operating online without censure, with a guiding ideology of misogyny, and with an aim of radicalising young boys. Her book, Men who hate women was published in 2020.
Existing stereotypes encourage boys to join misogynistic groups. Boys do not cry. Men do not talk about their feelings. There is a harking back to women staying at home. Feminism is the great evil and the root of all their problems. The men are often victims of sexual violence. They spout extreme rhetoric online. They have tried to de-fund women’s refuges.
Around 70% of boys in schools have come in contact with these groups. Almost none of the parents have heard of them.
We need to start taking extreme misogyny seriously rather than writing it off as a community of oddballs: not to do so is to utterly fail to keep this generation of boys and girls safe. We need to develop our understanding of how to help those boys at risk of going down this path and prevent it happening in the first place. As Bates says, ‘failing to act is the mark of a society that devalues not just women, but men.’ (Reference Bates25)
How Can Men Help in Prevention of Sexual Harassment?
There are many men who are supportive. We need men to call other men out. There must be disciplinary procedures for people who ‘cross the line’. The temptation to keep the matter private, as happens at present, is very great.
The Good Lads project is active in many universities and further education colleges. It includes mandatory sexual consent workshops for all freshers. (26) Active solidarity from groups of men such as football or rugby clubs is helpful. The White Ribbon Alliance (27) has a youth programme for schools, and the BMA’s Active Allyship is a definite step in the right direction.
We have to teach everyone the importance of consent and we have to start as early as possible.
Conclusion
It is clear that, in spite of all best efforts, sexual harassment remains a significant problem for women in medicine in the UK and worldwide. Women alone sharing their stories through websites, chat groups, spreadsheets, etc. is not enough. Formal policies have been in effect for years, but sexual harassment has not significantly decreased. Although robust organisational processes are necessary, they are insufficient to change cultures.
Systemwide change is needed and there must be adequate repercussions for the perpetrators. What really needs to change is men’s behaviour, starting in schools. Bystander Intervention and training are encouraging initiatives. Intervention is especially useful for conduct that is not severe or sustained enough to trigger investigations. And that is the majority of incidents.

 Open access
Open access