

Introduction
Although it receives less attention than postnatal depression, postnatal anxiety may be a more prevalent presentation (Matthey et al., Reference Matthey, Barnett, Howie and Kavanagh2003; Wenzel et al., Reference Wenzel, Haugenn, Jackson and Brendle2005), with considerable negative impacts on children (Glasheen et al., Reference Glasheen, Richardson and Fabio2010; Rees et al., Reference Rees, Channon and Waters2019) and breastfeeding rates (Field, Reference Field2018; Fallon et al., Reference Fallon, Groves, Grovenor Halford, Bennett and Harrold2016b). Prevalence estimates of postnatal anxiety vary widely, possibly attributed to challenges in identification and measurement. Rates span from 13% to 40% (Field, Reference Field2018), with pandemic rates in the UK as high as 61% (Fallon et al., Reference Fallon, Davies, Silverio, Jackson, De Pascalis and Harrold2021). The Irish prevalence of moderate to severe anxiety is estimated at 9.5% (Hannon et al., Reference Hannon, Gartland, Higgins, Brown, Carroll, Begley and Daly2022). Global prevalence of any anxiety disorder is 3.6% (WHO, 2017). Pooled prevalence rates of any anxiety disorder in the postpartum period are at 8.56%, with generalised anxiety disorder (GAD) prevalence at 3.59% and obsessive-compulsive disorder (OCD) at 2.49% (Goodman et al., Reference Goodman, Watson and Stubbs2016). However, Fairbrother et al. (Reference Fairbrother, Collardeau and Albert2021) estimate a higher cumulative incidence of new OCD (≤9%) at 6 months postpartum. Despite this, the concept specificity of postnatal anxiety remains unclear. While a certain amount of anxiety is relatively normal in the postnatal period and even adaptive to a point, there is a call to assess for sustained anxiety (Dennis et al., Reference Dennis, Coghlan and Vigod2013). The issue is further complicated by challenges in determining if prenatal anxiety precedes postnatal anxiety (Field, Reference Field2018). Thereby, it remains unclear if childbirth is a trigger for the development of an anxiety disorder or an exacerbation of a pre-existing anxiety disorder (Furtado et al., Reference Furtado, Van Lieshout, Van Ameringen, Green and Frey2019) or a unique subtype of anxiety. However, rates of anxiety during the postnatal period consistently exceed those found in the general population (Goodman et al., Reference Goodman, Watson and Stubbs2016; Dennis et al., Reference Dennis, Falah-Hassani and Shiri2017) and as such warrant understanding. Much of the research on postnatal anxiety has centred on prevalence, assessment, and identification of postnatal anxiety, with less attention given to more amenable psychological factors associated with postnatal anxiety, which would more usefully inform intervention. Such factors may include intolerance of uncertainty (IU; Freeston et al., Reference Freeston, Rheaume, Letarte, Dugas and Ladouceur1994) and inflated responsibility (IR; Salkovskis et al., Reference Salkovskis, Wroe, Gledhill, Morrison, Forrester, Richards, Reynolds and Thorpe2000).
Intolerance of uncertainty
IU is ‘a dispositional characteristic that results from a set of negative beliefs about uncertainty and its implications’ (Robichaud et al., Reference Robichaud, Koerner and Dugas2019; p. 19). It is strongly linked to worry and anxiety, and may be a transdiagnostic vulnerability for various emotional issues (Rosser, Reference Rosser2019). IU can be prospective, which refers to active information seeking as a way to decrease uncertainty; or inhibitory, which describes avoidance-oriented responses to uncertainty (Carleton et al., Reference Carleton, Norton and Asmundson2007). Wenzel et al. (Reference Wenzel, Eisenlohr-Moul, Nagelli, Peñalver Bernabé and Nagelli2021) examined IU and its association with anxiety, as either a trait- or state-like characteristic in a perinatal black and Latin sample. They found an association between trait-like, not state-like IU and anxiety. However, when IU was separated into inhibitory and prospective forms, a significant, although weak association was observed between state-like prospective IU, not state-like inhibitory IU and anxiety. Wenzel et al. (Reference Wenzel, Eisenlohr-Moul, Nagelli, Peñalver Bernabé and Nagelli2021) concluded that inhibitory IU’s influence on anxiety may be trait-like, with its prospective form having a state-like influence perinatally. In postnatal populations, IU has been significantly associated with exacerbating pre-existing anxiety during the postpartum period (Furtado et al., Reference Furtado, Van Lieshout, Van Ameringen, Green and Frey2019). However, IU alone may not be a sufficient predictor of anxiety. Rosser (Reference Rosser2019) suggests that the impact of IU on psychological challenges may be interactive, contingent not only on IU itself but also on the existence of one or more additional variables. One of these variables could be inflated responsibility (IR) beliefs.
Inflated responsibility
IR is ‘the belief that one has power which is pivotal to bring about or prevent subjectively crucial negative outcomes’ (Salkovskis, Reference Salkovskis1999; p. 32). Targeting IR beliefs is core to the treatment of OCD (Salkovskis, Reference Salkovskis1999) and perinatal OCD (Abramowitz et al., Reference Abramowitz, Schwartz, Moore and Luenzmann2003; Barrett et al., Reference Barrett, Wroe and Challacombe2016). IR may be a predictive factor in anxiety disorders other than OCD (Tolin et al., Reference Tolin, Worhunsky and Maltby2006; Gústavsson et al., Reference Gústavsson, Salkovskis and Sigurosson2021), perhaps, including postnatal anxiety. IR may be a stable trait, which has been shown not to differ significantly between non-childbearing, antenatal and postnatal samples (Barrett et al., Reference Barrett, Wroe and Challacombe2016). Small studies have found an association between maternal responsibility beliefs and postnatal anxiety (Fonseca et al., Reference Fonseca, Monteiro and Canavarro2018; Sockel et al., Reference Sockel, Neill Epperson and Barber2014). Furthermore, increased alcohol use has been associated with reduced postnatal anxiety (van der Zee-van den Berg et al., Reference van der Zee-van den Berg, Boere-Boonekamp, Groothuis-Oudshoorn and Reijneveld2021), perhaps indicating reduced conscientiousness or lower IR.
An inflated sense of responsibility for harm or its prevention could impact interpretations of the experience of childbirth and parenting. A mother’s over-estimation of parental responsibility for negative outcomes would potentially heighten her perception of threat. Gústavsson et al. (Reference Gústavsson, Salkovskis and Sigurosson2021) have hypothesised that IR may play a significant role in GAD, interacting with core beliefs about oneself and the world. As such, it may be the drive towards eliminating uncertainty, rather than beliefs about uncertainty, that causes worry and anxiety. Purdon’s (Reference Purdon2018) work on OCD compulsions hypothesises that specific IU and the need to be certain one is fulfilling their perceived responsibility may drive compulsions. Indeed, although their sample size was small, Lind and Boschen (Reference Lind and Boschen2009) reported that IU may moderate the link between IR and checking behaviours in OCD. Given the high incidence of GAD and OCD in postnatal populations along with high incidence of anxiety, IR and its interaction effects with IU may be important targets of investigation in postnatal anxiety populations.
Postnatal anxiety and mother and infant outcomes
Postnatal anxiety has many negative effects on mother and infant outcomes (Glasheen et al., Reference Glasheen, Richardson and Fabio2010). One of these effects may be breastfeeding outcomes. In the Irish context, Ireland has low breastfeeding rates, with 56% initiation and 2.4% exclusive at 6–7 months (Gallagher et al., Reference Gallagher, Begley and Clarke2016). Postnatal anxiety is associated with reduced likelihood of exclusive breastfeeding (Field, Reference Field2018; Fallon et al., Reference Fallon, Groves, Grovenor Halford, Bennett and Harrold2016b). Higher ratings of postnatal anxiety, as measured by the Postpartum Specific Anxiety Scale (Fallon et al., Reference Fallon, Halford, Bennett and Harrold2016a), correlate with lowered odds of exclusive breastfeeding (Fallon et al., Reference Fallon, Halford, Bennett and Harrold2018). In a large Norwegian sample (n=42,225), Ystrom (Reference Ystrom2012) found that prenatal anxiety and depression were associated with breastfeeding cessation, but in turn potentially triggering postnatal anxiety and depression. Interestingly, in Irish samples, continued breastfeeding has been associated with greater distress and anxiety at various points (Bennett and Kearney, Reference Bennett and Kearney2018; Hennessy et al., Reference Hennessy, Phelan and Kiely2022). Besides causing anxiety about breastfeeding, IU and IR beliefs may also impact both breastfeeding initiation and continuation. As such, the influences of IU and IR on infant feeding warrant further exploration.
Despite cognitive behavioural psychotherapy (CBT) reducing anxiety in the treatment of postnatal depression (Milgrom et al., Reference Milgrom, Negri, Gemmill, McNeil and Martin2005; Misri et al., Reference Misri, Reebye, Corral and Mills2004), and being recommended in the treatment for postnatal anxiety (National Institute for Health and Care Excellence, 2014), research evidence is limited. Our search identified only one CBT-related postnatal anxiety intervention study (Green et al., Reference Green, Haber, Frey and McCabe2015) and one OCD-specific study (Challacombe et al., Reference Challacombe, Salkovskis, Woodgar and Wilkinson2017). A better understanding of the potential roles of IR and IU in postnatal anxiety could help inform postnatal-specific anxiety CBT treatment. Beck’s theory (Beck et al., Reference Beck, Emery and Greenberg1985) of the development of anxiety disorders has developmental factors at its core. It proposes that pregnancy and childbirth can be significant stressors, leading to the activation of underlying core beliefs and other cognitive structures (e.g. IR and IU). Such cognitive structures and processes may mediate the link between life events and distress, with stressful events predicting postnatal anxiety (Clout and Brown, Reference Clout and Brown2015; Wenzel et al., Reference Wenzel, Haugenn, Jackson and Brendle2005; Yelland et al., Reference Yelland, Sutherland and Brown2010). Understanding the potential role of IU and IR in postnatal anxiety could help improve its recognition and treatment. To this end, the present study investigated if IU and IR and their interaction, predicted postnatal specific anxiety in a postnatal population, and also tested for the impact of factors on infant-feeding outcomes. We hypothesised that IU, IR and their interaction would be associated with higher postnatal specific anxiety and in turn, that IR, IU and postnatal anxiety would be associated with reduced likelihood to breastfeed.
Method
Participants and procedure
A group of mothers (n=208; age range 18–50 years) of Republic of Ireland-born infants (≤12 months), were invited to participate in an online survey using Qualtrics. They were recruited via advertisement with a link and QR code posted on the Facebook social media platform, using a snowball sampling methodology. The link took participants to an information leaflet and consent form, to be read and completed before accessing the survey measures, along with websites and directions for seeking further help if needed.
A total of 77 respondents had incomplete and unusable questionnaires, likely attributed to a survey platform error. Five participants were excluded as their infants were aged over 13 months. As such, 126 participants completed the survey, of whom three had infants slightly older than 12 months, which was deemed acceptable and were included in the final sample for analysis. Two of these 126 participants had no data for highest educational level and were hence excluded in analyses that controlled for this variable. No participation incentives were offered.
Measures
Postnatal demographic questions
Information was gathered pertaining to participants’ age, infant age, ethnicity, education, relationship status, number of children, birth induction, type of birth, multiple births, infant health and history of previous mental health treatment/intervention.
Research Short-Form Postpartum Specific Anxiety Scale (PSAS-RSF; Davies et al., Reference Davies, Christiansen, Harrold, Silverio and Fallon2021)
The PSAS-RSF is a short-form research version of the Postpartum Specific Anxiety Scale (PSAS; Fallon et al., Reference Fallon, Halford, Bennett and Harrold2016a), which is a 4-construct measure (Competence and attachment anxieties; Safety and welfare anxieties; Practical baby care anxieties; and Psychosocial adjustment to motherhood). It has good validity and excellent reliability (Fallon et al., Reference Fallon, Halford, Bennett and Harrold2016a). We employed the 16-item PSAS-RSF which maintains the PSAS’s four factors and exhibited statistical validity and reliability (McDonald’s ω=.88) (Davies et al., Reference Davies, Christiansen, Harrold, Silverio and Fallon2021). This shorter version, suitable for online surveys, has four answer options per item, scoring from 16 to 64. No cut-offs for clinical significance have been established yet.
10-item State-Trait Anxiety Inventory (STAI; Zsido et al., Reference Zsido, Teleki, Csokasi, Rozsa and Bandi2020)
General anxiety levels were assessed using the shortened, 10-item Spielberger State-Trait Anxiety Inventory (STAIS-5 and STAIT-5). It is a measure of state and trait anxiety. The 10-item STAI has sound psychometric properties comparable to Spielberger et al.’s (Reference Spielberger, Gorsuch and Lushene1970) original version (Zsido et al., Reference Zsido, Teleki, Csokasi, Rozsa and Bandi2020). The STAI is the most frequently used measure for non-disorder specific anxiety (Littleton et al., Reference Littleton, Breitkopf and Berenson2007). Cut-off scores suggested for anxiety are STAIS, 9.5 and STAIT, 13.5 (Zsido et al., Reference Zsido, Teleki, Csokasi, Rozsa and Bandi2020).
Breastfeeding outcomes
Following Fallon et al. (Reference Fallon, Groves, Grovenor Halford, Bennett and Harrold2016b), breastfeeding within the first 6 months was assessed using the seven response options below. Intention to breastfeed was also assessed using the same questions:
-
(1) Exclusive breastfeeding (EBF) in first 6 months,
-
(2) Predominantly breastfeeding (80% breastmilk; 20% formula),
-
(3) Mainly breastfeeding (50–80% with some formula),
-
(4) Combination feeding (50:50),
-
(5) Mainly formula feeding (50–80%) with some breastmilk,
-
(6) Predominantly formula feeding (over 80%) with some breastmilk,
-
(7) Entirely formula feeding.
12-item Intolerance of Uncertainty Scale (IUS-12; Carleton et al., Reference Carleton, Norton and Asmundson2007)
The IUS-12 is a 12-item, 2-factor shortened version of the 26-item IUS (Freeston et al., Reference Freeston, Rheaume, Letarte, Dugas and Ladouceur1994), with the English version validated by Buhr and Dugas (Reference Buhr and Dugas2002). It has excellent internal consistency, with good correlation with the original version (Carleton et al., Reference Carleton, Norton and Asmundson2007). We used the readable IUS-R, which is recommended for use in research (Walker et al., Reference Walker, Birrell, Rogers, Leekam and Freeston2010). An overall score of 35 or more indicates vulnerability to anxiety (Carleton et al., Reference Carleton, Norton and Asmundson2007). There are two subtypes of uncertainty assessed in this scale: prospective uncertainty and inhibitory uncertainty. Prospective IU refers to active information seeking as a way to decrease uncertainty, while inhibitory IU assesses avoidance-oriented responses to uncertainty (Carleton et al., Reference Carleton, Norton and Asmundson2007). Furtado et al. (Reference Furtado, Frey and Green2021) reported that the IUS exhibited excellent internal consistency in perinatal populations, making it a reliable tool for assessing vulnerability to perinatal anxiety. A higher score on this scale indicates a greater level of intolerance of uncertainty (IU).
Responsibility Attitudes Scale (RAS; Salkovskis et al., Reference Salkovskis, Wroe, Gledhill, Morrison, Forrester, Richards, Reynolds and Thorpe2000)
The RAS is a 26-item measure of inflated responsibility beliefs. Each item is rated on a 7-point Likert-style scale, with response options running from ‘totally agree’ to ‘totally disagree’. It has demonstrated good psychometric properties (Salkovskis et al., Reference Salkovskis, Wroe, Gledhill, Morrison, Forrester, Richards, Reynolds and Thorpe2000). A lower score on this scale indicates a greater sense of inflated responsibility (IR).
Sample size calculation
Meta-analyses have previously reported associations between IU and anxiety of large effect size (e.g. r=0.60, Osmanağaoğlu et al., Reference Osmanağaoğlu, Creswell and Dodd2018; r=0.50, Carleton et al., Reference Carleton, Collimore and Asmundson2010). The current study was designed to be powered (at α=.05, β=.80) to detect a medium effect size (f 2=.15) of a regression model with nine predictor variables (four demographic measures, STAIT, STAIS, IR, IU and the interaction between IR and IU) on PSAS. HHU G*Power software website (HHU, 2022; linear multiple regression: fixed model R 2 deviation from zero) indicated this required a minimum sample of 114 participants. This sample size was exceeded by our snowball sampling.
Data analysis
Data were to be analysed using IBM SPSS Statistics 27 (IBM Corporation, 2020). Data analysis would first test for bivariate correlations between PSAS, IU, IR and any continuous demographic variables, using Pearson’s correlation coefficient. Next, we aimed to test for unique predictors of PSAS. For this purpose, hierarchical multiple linear regressions were in two steps, first with demographic factors and anxiety (STAIT and STAIS) as predictor variables and PSAS as the dependent variable. IU-total score, IR and their mean-centred interaction were entered as predictor variables in Step 2. The regression was repeated using the factors of the IU (i.e. IU-prospective (IU-p) and IU-inhibitory (IU-i)) as predictors, in combination with IR.
Finally, we tested for predictors of infant feeding. Due to small proportions of the sample in the different breastfeeding groups, the infant feeding outcome was dichotomised as ‘Any breastfeeding (ABF)’ and ‘No breastfeeding’. The same was done for ‘Exclusive breastfeeding (EBF), yes/no’ and ‘Intention to ABF’ and ‘Intention to EBF’. A MANOVA was then to be performed, testing for associations between five dependent variables (IU, IR, STAIT, STAIS and PSAS) and the dichotomised breastfeeding (yes/no) independent variables.
Results
Descriptive statistics
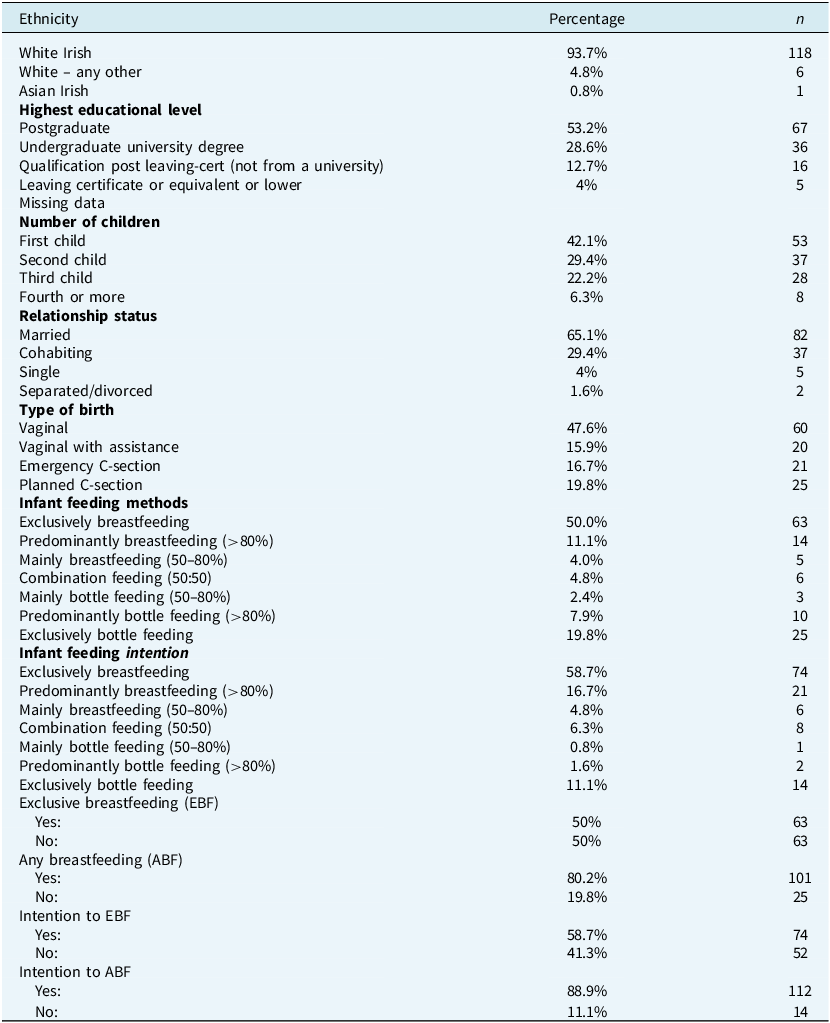
The 126 participants’ ages at the time of the birth of their last child ranged from 20 to 44 years (M=33.75, SD=4.81), with their infants’ ages ranging from 1 to 12 months (M=6.35, SD=3.57). Participants were predominantly white Irish, highly educated, and in relationships. A previous history of mental health problems/intervention was reported by 39 participants (31%). There was only one multiple birth reported, 20 participants (15.9%) reported having an ill child after birth, and 44 (34.9%) participants were induced with syntocinon. Table 1 presents the characteristics of the sample.
Description of sample

Measure reliability and level of distress within the study
Reliability scores were calculated for all measures, along with means and standard deviations (Table 2). Cronbach’s alpha (α) scores showed good reliability (α>0.7) for all measures.
Scales means, standard deviations, and Cronbach scores and cut-offs

PSAS, Postpartum Specific Anxiety Scale; STAIS, State Anxiety; STAIT, Trait Anxiety; IU, intolerance of uncertainty; IR, inflated responsibility.
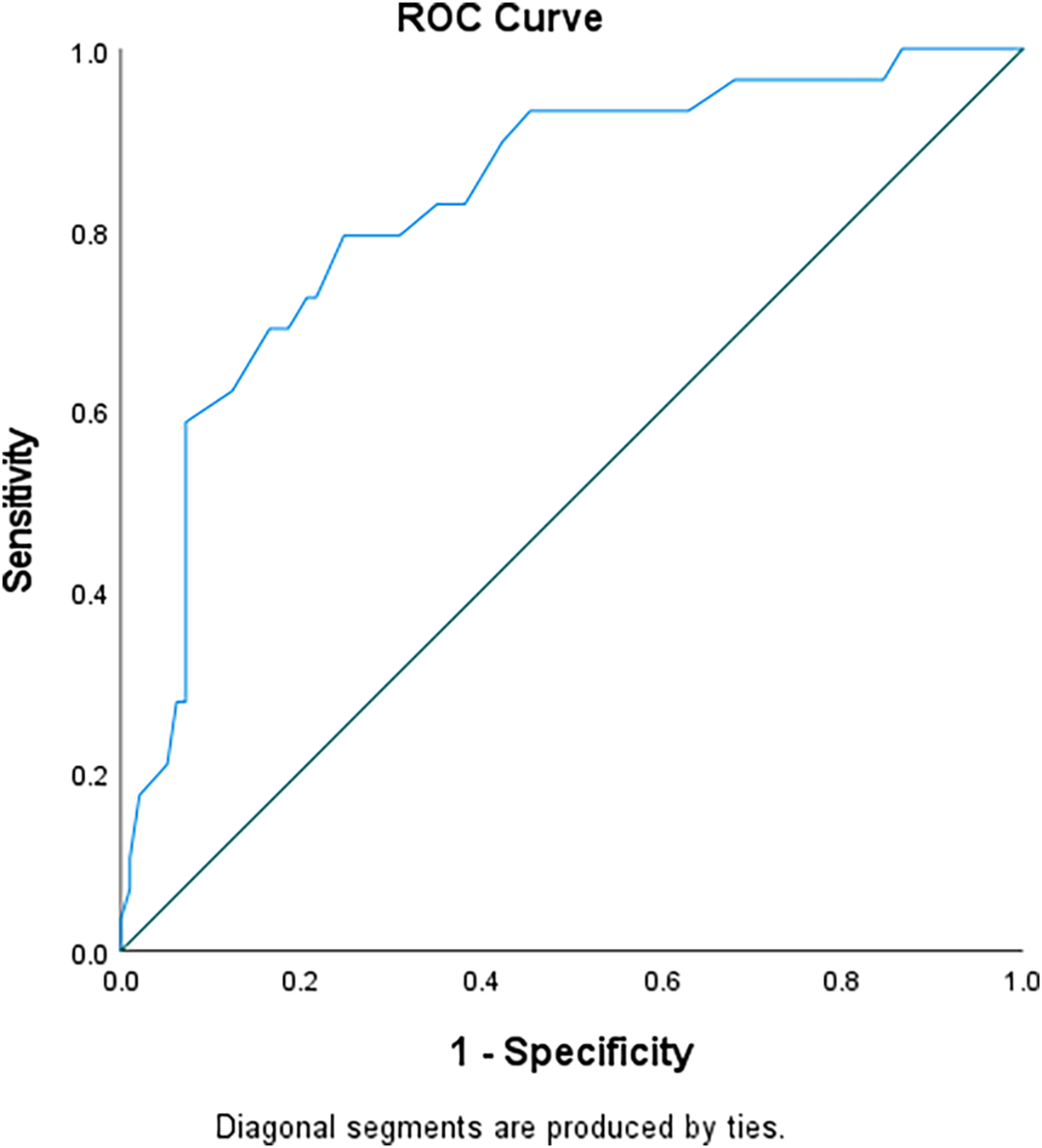
As the sample was non-clinical, we quantified levels of distress using published clinical cut-offs (see Table 2). As there are no published cut-off scores for the PSAS-RSF, a receiver operating characteristic (ROC) analysis was carried out on it with STAIS anxiety (Fig. 1). The Area under the curve was .83 (SD=.04), p<.001. A suggested cut-off score of 36.5 on the PSAS would correctly detect 79% of women with a diagnosis of state anxiety. This aligns with the sensitivity reported on the original PSAS-51-item, which had a cut-off of 112 out of 164 with sensitivity of 75% (Fallon et al., Reference Fallon, Halford, Bennett and Harrold2016a). The mean on the PSAS-RSF of the anxious group was 43 (SD=7.5), versus a mean of 32.73 (SD=8) for the non-anxious group; 42.1% of the sample scored over this cut-off of 36.5 on the PSAS-RSF.
ROC curve for PSAS (Postnatal Specific Anxiety Scale) and STAIS (State Anxiety).

Despite the sample being non-clinical, many participants scored within clinical ranges on variables (Table 2).
Relationships between study variables
Bivariate correlations between continuous study variables are reported in Table 3. Maternal age showed a significant negative correlation with many of the study variables. The relationships between the presence of previous mental health difficulties and study variables were tested for using t-tests. These showed that a history of mental health difficulties was associated with significantly higher IU scores (t=–4.77, d.f.=124, p<.001), STAIS scores (t=–3.74, d.f.=124, p<.001), STAIT scores (t=–4.82, d.f.=124, p<.001), and PSAS scores (t=–2.88, d.f.=124, p=.002), and significantly lower RAS scores (t=4.42, d.f.=124, p<.001). Finally, ANOVAs revealed an association between highest educational level and two study variables, namely IU, F 3,120=3.63, p=.02, and STAIS, F 3,120=4.46, p=.005. As a result, our regression analyses would control for maternal age, history of mental health difficulties, and highest educational level (dummy coded). Infant age did not correlate with anxiety in the current study and there was no correlation between PSAS and either infant health, parity, birth induction or birth type.
Bivariate correlations

**Correlation is significant at the 0.01 level (2-tailed). *Correlation is significant at the 0.05 level (2-tailed). PSAS, Postpartum Specific Anxiety Scale; STAIS, State Anxiety; STAIT, Trait Anxiety; IU, intolerance of uncertainty; IR, inflated responsibility.
Unique predictors of postnatal anxiety
Multiple linear regression analyses were run to test for unique predictors of postnatal anxiety (i.e. PSAS-RSF score). The variance inflation factor (all VIF <6) did not suggest multi-collinearity. The Durbin–Watson value of 2.38 in the model assured the assumption of independence of residuals. Standardised residuals did not deviate from normality (Kolmogorov–Smirnov test D=0.053, d.f.=126, p>.05). As such, the model met assumptions for linear regression analyses.
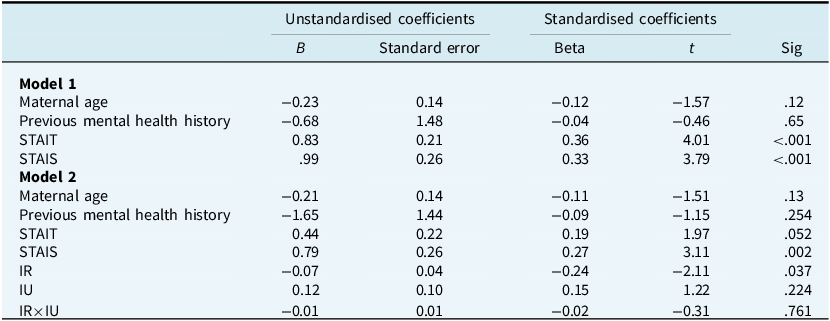
Step 1, with maternal age, highest educational level (dummy coded), previous mental health history, STAIT (trait anxiety) and STAIS (state anxiety) as predictor variables, was a significant predictor of PSAS (R 2=.43, F 7,118=12.94, p<.001). STAIT and STAIS anxiety were the only significant individual predictors (Table 4). In Step 2, with IU-total score and IR being entered along with their mean-centred interaction, both Step 2 (∆R 2=.07, ∆F 3,115=5.08, p=.002) and model 2 (R 2=.50, F 10,115=11.52, p<.001), were significant predictors of PSAS. In model 2, only IR and STAIS were significant individual predictors of postnatal anxiety. As such, greater experiences of IR and state anxiety, not IU, STAIT or the demographic factors, predicted postnatal anxiety.
Multiple regression for Postpartum Specific Anxiety Scale
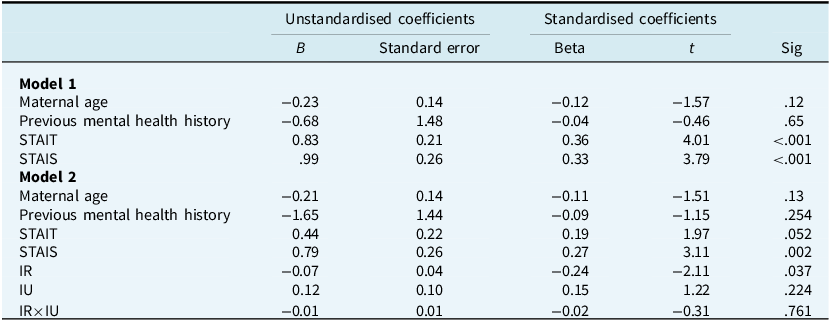
Dummy coded education variable is not reported in the table. IU, intolerance of uncertainty; IR, inflated responsibility; interaction IR×IU is the interaction of IR with IU; STAIS, State Anxiety; STAIT, Trait Anxiety; PSAS, Postpartum Specific Anxiety Scale.
When Step 2 was repeated, but with the factors of IU (i.e. prospective IU (IU-p) and inhibitory IU (IU-i)) as predictors, a similar pattern of results was observed. IR remained a significant predictor, with neither IU-p nor IU-i being significant predictors of PSAS.
What predicts infant feeding outcomes?
A MANOVA was performed with IU, IR, PSAS, STAIS and STAIT as the dependent variables and breastfeeding (dichotomised as ‘Any breastfeeding’ and ‘No breastfeeding’) as the independent variable. The same process was then repeated three times, first using ‘Exclusive breastfeeding’ (yes/no) as the independent variable, then ‘Intention to breastfeed’ (yes/no) and finally ‘Intention to exclusively breastfeed’ (yes/no). Only the ‘Any breastfeeding’ MANOVA was statistically significant.
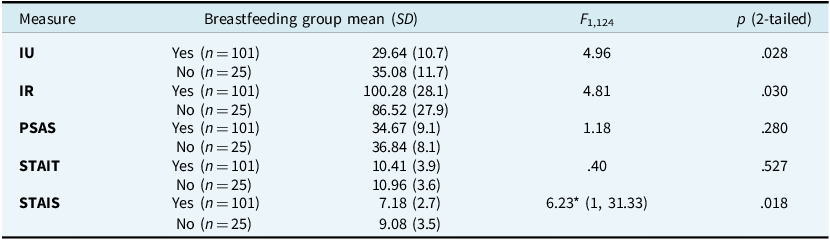
Pillai’s trace (F 5,120= 2.78, p<.05) indicated a significant effect of group and hence t-tests were used to test for differences between the breastfeeding groups on each of the dependent variables. Levene’s test for equality of variances was non-significant (p>.05) for all scales, except the STAIS. Therefore, the significance level in Table 5 for the STAIS analysis comes from the performance of a Welch t-test (which does not assume equality of variance). As Table 5 shows, the non-breastfeeding group had significantly higher STAIS and IU scores than the breastfeeding group, and significantly lower IR scores (indicating higher levels of inflated responsibility).
Impact of IU, IR, PSAS, trait and state anxiety on breastfeeding outcomes
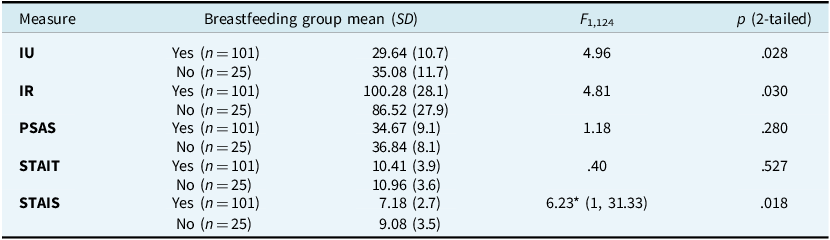
IU, intolerance of uncertainty; IR, inflated responsibility; PSAS, Postpartum Specific Anxiety Scale; STAIT, State Trait Anxiety Inventory (Trait); STAIS, State Trait Anxiety Inventory (State). *This represents the Welch statistic, with this test being performed due to violation of Levene’s test for equality of variances for this variable.
Discussion
Using an online survey with a sample of educated Irish women, this study explored the impact of two potential cognitive vulnerability factors, namely intolerance of uncertainty (IU) and inflated responsibility (IR), on postnatal specific anxiety and feeding outcomes. We found a unique relationship between IR and postnatal anxiety, with greater levels of inflated responsibility being associated with greater levels of postnatal anxiety. However, IU did not predict postnatal anxiety. Furthermore, state anxiety was a significant predictor of postnatal specific anxiety, while trait anxiety was not. In relation to feeding outcomes, non-breastfeeding was associated with greater levels of IR, IU and state anxiety.
Our hypothesis that IR would predict postnatal anxiety was supported by the results of regression analyses. Our findings support those of other cross-sectional studies in postnatal populations (Fonseca et al., Reference Fonseca, Monteiro and Canavarro2018; Sockel et al., Reference Sockel, Neill Epperson and Barber2014). We cannot assume this sample’s IR beliefs precede the perinatal period, although Barrett et al. (Reference Barrett, Wroe and Challacombe2016) found IR beliefs (measured using RAS) did not differ significantly between non-childbearing, antenatal and postnatal samples, suggesting stability from pre- to post-childbirth. This study supports Tolin et al.’s (Reference Tolin, Worhunsky and Maltby2006) proposition that IR may be a factor in other anxiety disorders outside of OCD, which perhaps, has greater relevance to postnatal-specific anxiety than does state anxiety or IU. A longitudinal cohort study exploring IR beliefs may help to clarify this hypothesis.
Our hypothesis that IU would predict postnatal anxiety was not supported by the results of regression analyses, even when split into IU-prospective and IU-inhibitory. This was despite significant bivariate correlations between IU and postnatal anxiety. This finding contrasts with the commonly accepted hypothesis that IU predicts anxiety, especially worry (Dugas et al., Reference Dugas, Gosselin and Ladouceur2001). Wenzel et al. (Reference Wenzel, Eisenlohr-Moul, Nagelli, Peñalver Bernabé and Nagelli2021) report that prospective IU may be state-like and associated with perinatal anxiety. However, in the current study, investigating the IU scale factors did not provide any further support for the findings of Wenzel et al. (Reference Wenzel, Eisenlohr-Moul, Nagelli, Peñalver Bernabé and Nagelli2021). This could be due to our use of a postnatal specific anxiety questionnaire rather than the GAD-7 scale used in their study. While a small study implicated IU in postnatal anxiety exacerbation (Furtado et al., Reference Furtado, Van Lieshout, Van Ameringen, Green and Frey2019), the lack of pregnancy-to-postnatal IU score comparison hinders conclusive understanding. Adapting the IUS to the postpartum population might enhance its utility in identifying vulnerabilities during this specific period. There is a need for further investigation into potential differences in anxiety factors during these periods.
In our sample, mean IU scores of 30.72 were higher than Carleton et al.’s (Reference Carleton, Norton and Asmundson2007) seminal study which reported a mean of 25.85. However, our mean IU scores were lower than those reported in perinatal-specific samples by Wenzel et al. (Reference Wenzel, Eisenlohr-Moul, Nagelli, Peñalver Bernabé and Nagelli2021) (M=40.97), and Sbrilli et al. (Reference Sbrilli, Haigler and Laurent2021) (M=33.15), suggesting high IU in perinatal samples. This elevation might imply IU as a context specific state, associated with childbirth and pregnancy in postnatal populations. This challenges the notion of IU as a rigid and global trait and supports its conceptualisation as bi-directional, influencing and being influenced by contexts (Rosser, Reference Rosser2019).
The interaction between inflated responsibility and intolerance of uncertainty did not show a significant association with postnatal anxiety. It remains unclear if these results support the idea that intolerance of uncertainty’s influence may be interactional (Rosser, Reference Rosser2019). There may be several reasons for this, including the possibility that the current study may have been insufficiently powered to detect such an association. Exploring how an inflated sense of responsibility interacts with difficulty tolerating uncertainty postpartum could be a promising avenue for further research, considering the potential increased vulnerability to anxiety. Further studies examining IU as a moderator of IR and postnatal anxiety would also be beneficial. Although the overall regression model was significant, indicating that IR, IU and their interaction predicted postnatal anxiety, only IR showed a significant main effect. Further examination of the constructs of PSAS would be interesting. For example, competence and attachment anxieties may be more related to uncertainty while safety and welfare anxieties and practical baby care anxieties may be more associated with IR.
Although we did not find a significant interaction between IU and IR in our non-clinical sample, the relationship between them appears complex and may vary depending on clinical context and stage of motherhood. Drawing on Freeston and Komes’ (Reference Freeston and Komes2023) proposal that IU may be associated with a sense of unsafety, we hypothesise that this sense may motivate a mother towards taking responsible action. This perspective may partially suggest a link between IU and IR. For example, if IU motivates a mother to take responsibility, appropriate actions may include both mental actions (e.g. worry) and active safety behaviours (e.g. prenatal and breastfeeding classes, etc.). Once such actions are taken, the sense of uncertainty and unsafety may resolve somewhat. This view may partially explain the results of the current study, which found neither a significant interaction between IU and IR nor prediction of postnatal anxiety by IU. Our findings may partially support Gústavsson et al. (Reference Gústavsson, Salkovskis and Sigurosson2021). Our hypothesis of IU and unsafety as motivating towards responsibility potentially imply that IU is the spark that cues IR. By implication, IU may be more significant at an earlier stage of the mothering journey, resolving with increased IR and the taking of perceived responsible actions. IU may then become non-significant as per the current study’s results. It is also possible that IU and IR have different functions in non-clinical samples, such as the one in our study, and clinical ones. Although the levels of anxiety in our sample were high, IU and IR may still have different functions than in clinical samples, where they may lead to psychological illness and dysfunction. It would seem that there is a need for longitudinal studies that compare clinical and non-clinical samples at different stages of motherhood.
Our study also found a higher prevalence of anxiety in our sample than previous Irish studies (Hannon et al., Reference Hannon, Gartland, Higgins, Brown, Carroll, Begley and Daly2022). This may have been a function of the COVID pandemic context. The link between state anxiety (assessed by the STAIS scale) and postnatal specific anxiety was expected, but it was surprising that trait anxiety (STAIT scale) and having a history of mental health intervention did not predict postnatal specific anxiety. This contradicts established findings that anxiety history predicts postnatal anxiety (Field, Reference Field2018). While trait anxiety was not a predictor in the regression for postnatal anxiety, the STAIT score was trending towards significance. This may be influenced by the higher rates of anxiety in this study due to pandemic effects and it would be expected that if the study was replicated now, trait anxiety and previous mental health history would be a predictor of postnatal anxiety. It remains unclear if postnatal anxiety is a discrete concept, which is distinct from other anxiety disorders or can be a precipitant for the onset of an anxiety disorder in the postnatal period. However, the findings in this study suggest that the vulnerability factors in OCD and GAD, i.e. IU and IR, are also vulnerability factors in postnatal anxiety. This may lend some understanding to the higher incidence of those two disorders in the postnatal population.
The influence of IR, IU and postnatal anxiety on breastfeeding outcomes
In the current study, mothers with higher inflated responsibility (represented by lower RAS scores), higher intolerance of uncertainty and higher state (STAIS) anxiety were less likely to breastfeed, while trait anxiety (STAIT) and postnatal specific anxiety had no association with infant feeding. While these findings mostly fit with our hypotheses, there are interesting points to explore. PSAS not being associated with non-breastfeeding contradicts the study of Fallon et al. (Reference Fallon, Halford, Bennett and Harrold2016a), but perhaps fits with the Irish studies, which showed an inconsistent link between non-breastfeeding and anxiety (Bennett and Kearney Reference Bennett and Kearney2018; Hennessy et al., Reference Hennessy, Phelan and Kiely2022).
Even though IR predicted higher postnatal specific anxiety, IR, IU but not postnatal anxiety was associated with non-breastfeeding. This may potentially point to postnatal specific anxiety being a more nuanced anxiety than simply an anxiety disorder triggered or exacerbated during the postnatal period. It perhaps means that state anxiety, IU and IR influence a mother’s decision to breastfeed but postnatal specific anxiety is impacted by IR regardless of infant feeding decision. The PSAS, which assesses postnatal specific anxiety and as such is potentially a more detailed and nuanced measure that captures a mother’s anxiety in this period, is not associated with infant feeding choices in the current study. However, due to the small and heterogenous numbers in the current study and the fact that it was carried out at the tail-end of the pandemic, these results are difficult to generalise and a larger study, including prenatal intention to breastfeed, would be more informative.
The inherent uncertainty in breastfeeding, such as not knowing exactly how much milk an infant is consuming, might lend itself to the mother becoming more anxious. However, uncertainty-intolerant mothers may be less likely to start breastfeeding in the first place. Expanding Wenzel et al.’s (Reference Wenzel, Eisenlohr-Moul, Nagelli, Peñalver Bernabé and Nagelli2021) concepts of prospective and inhibitory IU may be helpful and explanatory also. For example, prospective ‘approach’ IU could lead to anxiety, but motivate mothers towards breastfeeding. IU, on the other hand, may be an inhibitory concept, leading to coping by avoiding breastfeeding and related tasks, thereby reducing intolerable uncertainty and anxiety. The inhibitory-prospective hypothesis potentially clarifies inconsistencies in the link between breastfeeding and anxiety reported in previous Irish studies (Bennett and Kearney Reference Bennett and Kearney2018; Hennessy et al., Reference Hennessy, Phelan and Kiely2022). However, this is only a hypothesis and requires further exploration. These results highlight the nuanced nature of postnatal anxiety and breastfeeding experiences, warranting further study with larger and more diverse samples, as well as qualitative research. The failure of our results to identify a correlation between IR, IU and anxiety and intention to breastfeed may simply be a function of our study being under-powered to detect such effects combined with the small numbers of non-breastfeeding participants.
Limitations
While the current study contributes valuable insights to the literature on postnatal anxiety and breastfeeding, caution is warranted due to limitations inherent in the study design. Although some have already been mentioned, of note, the sample was predominantly white, partnered, highly educated, and breastfeeding-prevalent, perhaps limiting generalisability to the broader context. The research was also carried out at the tail-end of the COVID pandemic, thus potentially impacting reported distress in the sample. The self-report nature introduces the possibility of recall bias, and inflated/minimised answers remain potential issues. Additionally, the cross-sectional design offers only a snapshot of current experiences, lacking the ability to capture the broader postpartum period. The absence of longitudinal data and a relatively small sample, particularly for breastfeeding data, further influence the study’s scope.
Conclusions
This is an important study, which points to nuanced concepts of IR and IU, with influences on postnatal anxiety that need further exploration. IR is more predictive of postnatal anxiety and may be more trait-like, while IU may be more situational or context driven. These results question accepted understanding and deserve further exploration. We identified that IU and IR may have a specific, negative influence on breastfeeding. The high incidence of anxiety scores within the clinical range in this non-clinical sample was surprising, suggesting a need for research and clinical focus on anxiety in this population. State anxiety predicted postnatal anxiety more than trait anxiety. We failed to find an influence of the interaction of IU and IR, perhaps because the two are distinct concepts with different functions, but again, this deserves further investigation. Postnatal anxiety may be a considerable precipitant for the development of an anxiety disorder, with qualities similar to other anxiety disorders, and may benefit from qualitative and longitudinal investigation to gain an in-depth understanding of its experience. Quantitative studies may be necessary to clarify the directions of causality and the mediating and moderating factors.
Data availability statement
The data that support the findings of this study are available from the corresponding author (C.L.) upon reasonable request.
Acknowledgements
Special thanks to Dr Vicky Fallon for her help and guidance on using the PSAS-RSF.
Author contributions
Catriona Larkin: Investigation (lead); Simon McCarthy-Jones: Supervision (equal); Craig Chigwedere: Supervision (equal).
Financial support
There was no funding for this research.
Competing interests
The authors declare there are no competing interests for this study.
Ethical standards
Ethical approval was obtained from Trinity College Dublin (20211109) and the study conformed to the Declaration of Helsinki. Permission was granted for use of all questionnaires.



 Open access
Open access
Comments
No Comments have been published for this article.