


Introduction
Raghib reported the complex cardiac presentation of a persistent left superior vena cava (SVC) draining to the left atrium (LA), coronary sinus (CS) atresia, and a posterior-inferior atrial septal defect (ASD). Reference Raghib, Ruttenberg, Anderson, Amplatz, Adams and Edwards1 Since then, multiple case reports have been published. There are, however, few case reports when this syndrome presents with additional congenital heart disease like ventricular septal defect (VSD), tetralogy of Fallot, Reference Selcuk, Korun and Sasmazel2 or cor-triaatriatum.
In the first Raghib et al. report of eight patients, two patients had associated VSD. However, neither of the two cases reported by Lee et al., in which a VSD was present, had undergone surgical correction of the Raghib complex. Reference Raghib, Ruttenberg, Anderson, Amplatz, Adams and Edwards1 Additionally, in a publication by Lee et al., where VSD was associated with Raghib syndrome, the left superior vena cava was occluded. Reference Lee and Sade3
The experience and outcome of intracardiac rerouting of the left SVC in Raghib syndrome associated with VSD closure is exceedingly rare.
Case Summary
A five-year-old boy, weighing 12 kg and measuring 60 cm high, was diagnosed with ASD and VSD at the age of one year. The boy was unable to walk and talk up to the age of four years.
During physical examination, the oxygen-saturation range was from 82 to 85%. There was a grade IV hollow systolic murmur at the right lower parasternal area. The echocardiography diagnosis was a large ASD & VSD both shunting left to right, an enlarged left ventricle with severe pulmonary hypertension, and a persistent left SVC with unspecified drainage.
Because of the limitation of cardiac surgery service in our setup, the patient was operated on at the age of five years. The intraoperative findings were absent CS, a left SVC opening below the left upper pulmonary vein and at the upper end of the posterior type of ASD, and a large perimembranous VSD. A fresh autologous pericardial patch was sutured starting from the opening of the left SVC into the left LA using 5:0 prolene. The patch drained all the small veins en route below the posterior mitral valve annulus until it opened into the right atrium (RA) near the septal leaflet of the tricuspid valve.
The baffling patch at its RA opening makes the lower border during ASD closure using a Sauvage patch. The VSD was closed using glutaraldehyde-treated autologous pericardium. The total cross-clamp and bypass times were 132 and 183 minutes, respectively, and the heart was restored to normal sinus rhythm.
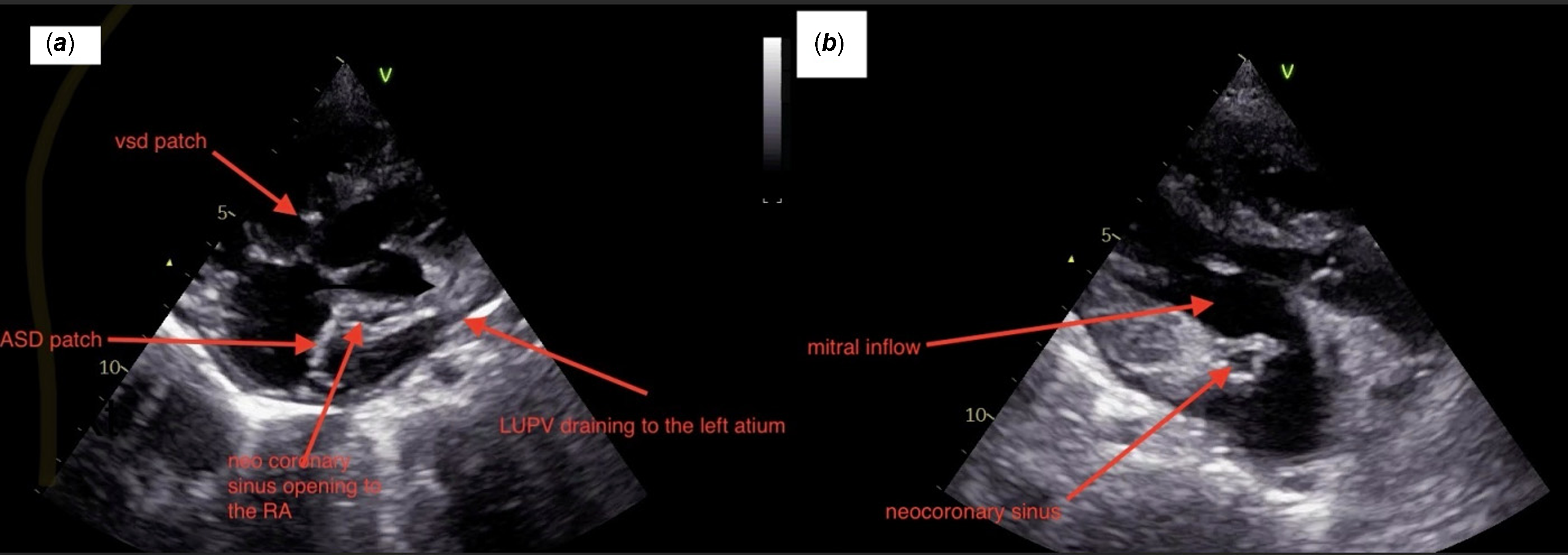
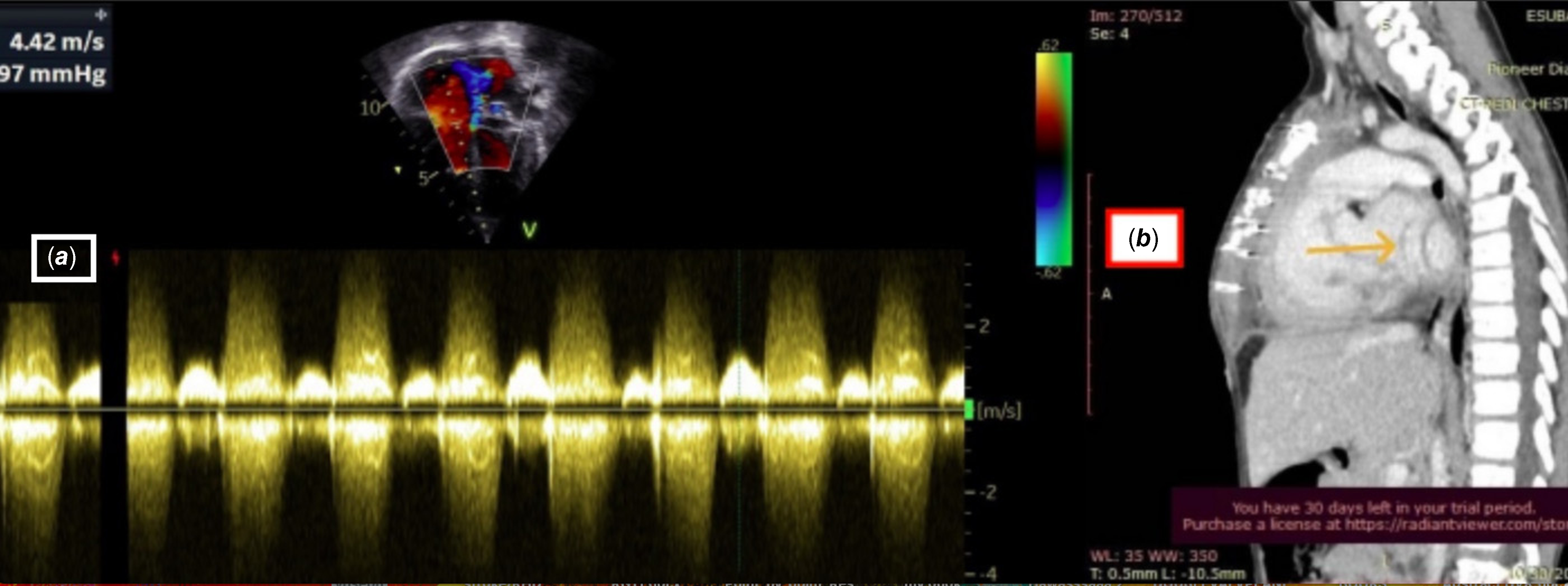
Postoperative echocardiography and cardiac CT scans showed drainage of the neo-CS and left SVC to the RA and unobstructed mitral valve inflow and pulmonary vein drainage. (Supplemental video) There was a tiny residual VSD, reduced systolic left ventricle function, and severe pulmonary artery pressure of 89 mmHg. By echocardiography measurement of tricuspid regurgitation after adding RA pressure (Figures 1, 2, and 3). Six months from the day of surgery, the pulmonary artery pressure dropped to 30 mmHg, and the saturation rose to 98% with atmospheric air.
A postoperative echocardiography showing, ( a) , the intra cardiac baffling of PLSVC into the RA, in situ ASD & VSD patches, and the unobstructed LUPV opening into the LA. ( b ), the echocardiography cross-sectional view of the neo-CS and the unobstructed mitral inflow. VSD = ventricular septal defect; ASD = atrial septal defect; PLSVC = persistent left superior vena cava; RA = right atrium; LA = left atrium; LUPV = left upper pulmonary vein.

( a ), The echocardiography measurement of the postoperative pulmonary artery pressure by the tricuspid regurgitation Vmax. ( b) , The sagittal reconstruction CT-angiography of the chest with contrast marked with yellow colour shows a dilated CS draining into the right atrium.

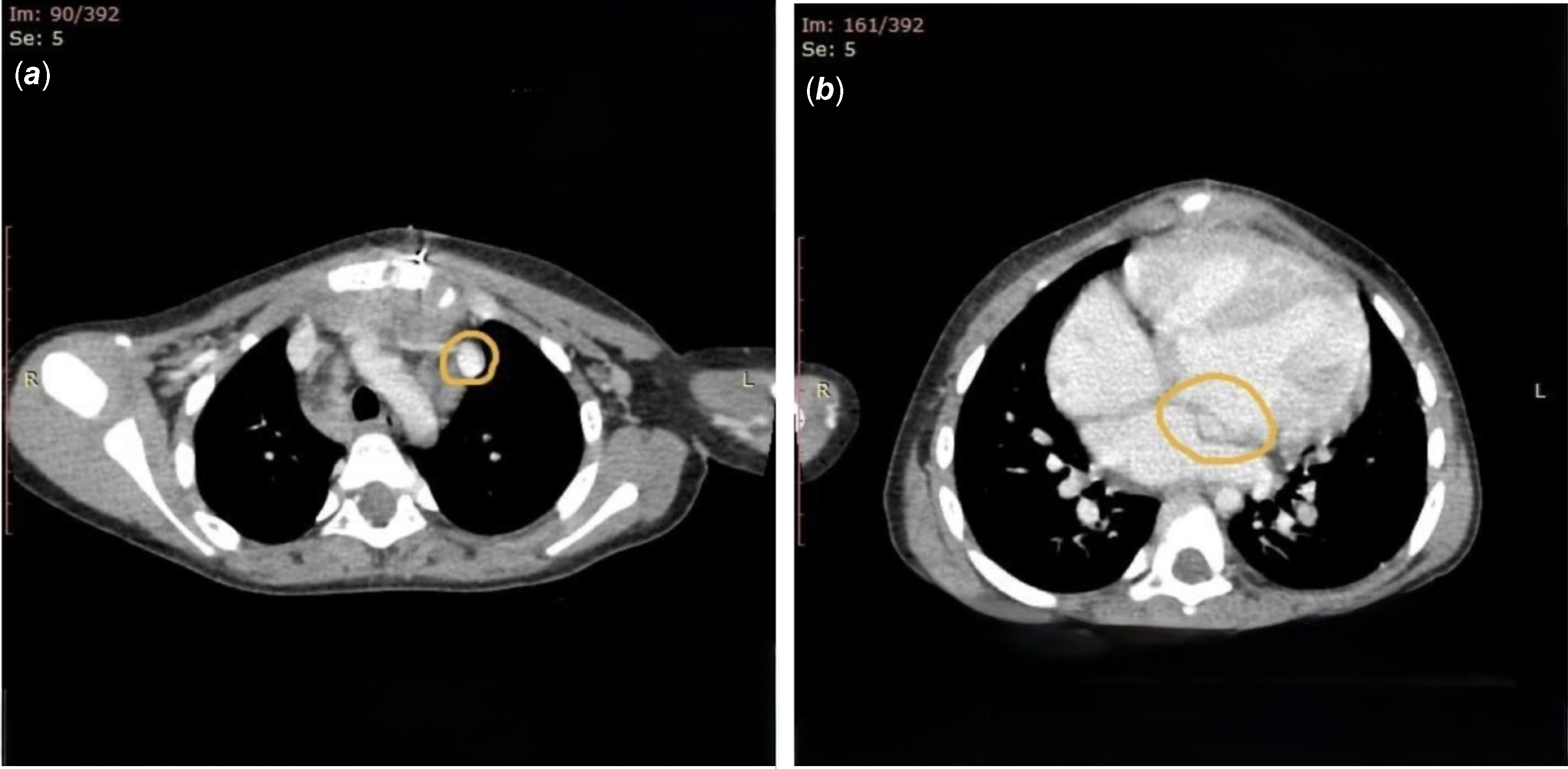
( a) . The axial view of CT-angiography of the chest with contrast showing a persistent left SVC. ( b ). The axial view of CT-angiography of the chest with contrast showing a dilated CS draining to the RA.

Discussion
This is a case report of a successful intracardiac rerouting of the left SVC in a Raghib syndrome patient associated with VSD.
Raghib syndrome and VSD have distinct embryologic development pathways, and their coexisting presentation might be a simple association by chance. But a shared developmental pathway from disruption of neural crest cell migration during the early weeks of gestation may give rise to the two conditions. Reference Raghib, Ruttenberg, Anderson, Amplatz, Adams and Edwards1
Selcuk et al. used extra-cardiac rerouting of the left SVC in their case report of Raghib complex associated with Tetralogy of Fallot. Reference Selcuk, Korun and Sasmazel2 We avoided the extra-cardiac approach for the attending complication of SVC obstruction syndrome. Our case report of intracardiac rerouting of left SVC to RA wasn”t complicated by arrhythmia or mitral inflow and pulmonary vein obstruction. In order to avoid mitral valve or pulmonary vein obstruction from patch redundancy, the width of the patch was adjusted to the circumference of the left SVC. To decrease the chance of arrhythmia, we followed the normal anatomy of the CS path from the opening of the left SVC in the LA up to its RA opening. By considering the anatomy of the triangle of Koch, our suture in the RA was superficial.
Conclusion
This is a case report of a five-year-old boy who underwent a successful intracardiac rerouting of left SVC drainage from LA to RA along with ASD and VSD closure during the same cross-clamp surgery.
Funding statement
None.
Competing interests
None.
Consent for publication
Written informed consent was obtained from the patient’s parent.

 Open access
Open access