


Introduction
Ethnicity comprises a complex collection of genetic, social, and cultural traits that may influence health and disease. Ethnicity has been linked to health and well-being in childhood, including premature birth, increased paediatric intensive care admissions, and infant mortality. Reference Parslow, Tasker and Draper1,Reference Opondo, Jayaweera, Hollowell, Li, Kurinczuk and Quigley2 There is evidence to suggest that ethnicity is associated with the incidence and severity of CHD. Reference Tjoeng, Jenkins, Deen and Chan3–Reference Knowles, Ridout and Crowe6 United Kingdom (UK) national audit data have demonstrated consistent improvements in 30-day survival after paediatric cardiac surgery in the UK; however, outcomes by ethnicity or socio-economic status are not routinely reported. 7 There are recent suggestions concerning disparities in outcomes between children of different ethnicities, including lower rates of Fontan completion and lower post-operative survival. Reference Knowles, Ridout and Crowe8–Reference Rogers, Pagel and Sullivan10 The reasons for this are poorly understood, given the complex interaction of confounding and mediating factors.
Recent UK studies have examined the impact of ethnicity in children undergoing cardiac surgery. One study of 1557 children with functionally single-ventricle heart disease showed White children did not have a significantly lower adjusted risk of death compared to “non-White children.” Reference Knowles, Ridout and Huang9,Reference Hadjicosta, Franklin and Seale11 On the other hand, Asian and Black children were less likely to complete the Fontan pathway. Reference Hadjicosta, Franklin and Seale11 These children are also at higher risk of complications following cardiac surgery. Reference Mustafa, Leahy, Ridout and Brown12 Knowles et al. subsequently reported that infants of British Asian and “other non-White” ethnicities undergoing any congenital heart surgery were less likely to survive to 1 year, but this did not extend to Black British infants. Reference Knowles, Ridout and Crowe8 This national registry study of infants with CHD found the increased mortality occurred before hospital discharge for British Asian infants, but the effect was mainly restricted to being seen out of hospital for the ‘“other non-White” group. This effect was not explained by socioeconomic status, and no underlying cause for the association was reported. Reference Knowles, Ridout and Crowe8
Similar patterns have been described in the United States (US), with Black and Hispanic children shown to have the highest risk for poor outcomes. Reference Oster, Strickland and Mahle13–Reference Nembhard, Xu, Ethen, Fixler, Salemi and Canfield15 Non-white children with functionally single-ventricle in the US were more likely to have a late Fontan operation and subsequently higher mortality. Reference Sainathan, Agala, Said, Mulinari and Sharma16 Another study showed heterotaxy syndromes were more common in infants of Black or Hispanic mothers. Reference Lopez, Marengo, Canfield, Belmont and Dickerson5 A large registry study of over 44,000 children with CHD observed that Black and Hispanic ethnicity was associated with around 30% and 35% higher in-hospital post-operative mortality compared to White children. Reference Oster, Strickland and Mahle13 This effect size remained similar after adjustment for age, sex, genetic syndrome, surgery risk category and access to healthcare, assessed by health insurance status. Reference Oster, Strickland and Mahle13 One study identified socio-economic status as the primary factor determining mortality, Reference Anderson, Fieldston, Newburger, Bacha and Glied17 whereas another demonstrated that increased severity of illness was the cause. Reference Tjoeng, Jenkins, Deen and Chan3 The latter study reported higher mortality for African-American patients, and concluded that adjusting for the severity of illness removed this association. However, this was predominantly based on statistical significance, as the overall effect size remained similar before and after adjustment (odds ratio 1.40 to 1.30). Reference Tjoeng, Jenkins, Deen and Chan3 A large systematic review found that ethnicity, as well as socioeconomic status, influenced the risk of unexpected death following hospital discharge. Reference Tregay, Wray and Bull18
The reasons for these inequities are unclear. Difficulties with missing data and ethnicity coding in multi-centre datasets have made exploring the underlying effects of ethnicity challenging. Reference Tjoeng, Jenkins, Deen and Chan3,Reference Rogers, Pagel and Sullivan10,Reference Sainathan, Agala, Said, Mulinari and Sharma16 Many studies report outcomes for “White” and “non-White” groups, despite the significant variation in social, cultural, and genetic factors within and between these ethnic groups. Reference Rogers, Pagel and Sullivan10,Reference Hadjicosta, Franklin and Seale11,Reference Gonzalez, Gauvreau, DeMone, Piercey and Jenkins14,Reference Sainathan, Agala, Said, Mulinari and Sharma16,Reference Hudson, Brown and Pagel19 Ethnicity is closely linked to socioeconomic status and other social factors that may contribute to disease onset. The impact of socioeconomic status on children diagnosed with CHD is unclear, with some studies reporting complex or no association with outcomes, Reference Rogers, Pagel and Sullivan10,Reference Best, Tennant and Rankin20 representing the myriad of related contributing factors. Others found strong relationships between socioeconomic status and death. Reference Anderson, Fieldston, Newburger, Bacha and Glied17,Reference DeMone, Gonzalez, Gauvreau, Piercey and Jenkins21 Inequities may also vary by country, depending on the healthcare system and public health policy. Reference Gonzalez, Gauvreau, DeMone, Piercey and Jenkins14,Reference Anderson, Fieldston, Newburger, Bacha and Glied17,Reference DeMone, Gonzalez, Gauvreau, Piercey and Jenkins21
The objective of this study was to examine the effect of ethnicity on survival outcomes following all forms of paediatric cardiac surgery and identify whether this has changed over time in the modern surgical era. We used prospectively collected clinical audit data from a large and diverse population of patients in Yorkshire, UK, to maximise information on sociodemographic and clinical factors contributing to survival. We studied the change in inequities over a prolonged period of the modern surgical era to help further understand the underlying mechanisms behind them. By describing the contribution of modifiable influences to outcome after CHD surgery, we aimed to identify strategies to reduce potential inequities and maximise outcomes for all children with CHD.
Materials and methods
Design and subjects
This retrospective study used clinical audit data ascertained from a large tertiary paediatric cardiac surgical centre in Yorkshire, UK. The centre covers a large and diverse population of over 5.5 million people and performs around 500 surgical procedures every year. The study population comprised children aged 0 to 15 years undergoing a cardiac surgical procedure between the 1st January 2005 and 31st December 2021. Data on all children undergoing cardiac surgery is routinely collected for mandatory national audit purposes, including demographic data, comorbidities and mortality. Where children had multiple surgical procedures, we included only children undergoing a first surgical procedure within the study period. Cardiac catheterisation procedures were not included.
Definition of exposures
Ethnicity was reported by parents and classified into 16 categories according to the 2021 Office for National Statistics Census categories. 22 These were combined into four major ethnic groups, which were then used for analysis: White, South Asian (Indian, Pakistani, or Bangladeshi origin), Black (African or Caribbean origin), and Other (Chinese, Mixed, or other origin). If the ethnicity was not recorded (n = 170, 5%), we cross-referenced patients with the PICANet database. This is a prospectively collected audit of all PICU admissions in the UK and the Republic of Ireland and was established in 2001. 23 Ethnicity could not be determined in a small minority of patients, and these were excluded from the primary analysis (n = 81, 2%). Comorbidities were defined at the time of surgery according to the UK National Congenital Heart Disease Audit list of recognised comorbidities. These include acquired and congenital comorbidities.
Area-based socioeconomic status was assigned using the English Indices of Deprivation 2019 income score. 24 The income index of deprivation is a measure of the proportion of the population experiencing deprivation related to low income. This is assessed using the parental home postcode, and each region is ranked relative to 32,844 neighbourhoods in England. For analytical purposes, children were classified into area-based deprivation fifths according to the income score, with fifth 1 being the most deprived and fifth 5 being the least deprived. Postcode was also used to calculate the Euclidean distance from the home address to the tertiary cardiac centre.
Outcomes
The primary outcome was survival after the first cardiac surgical procedure during the study period. Life status is confirmed for all patients in the database multiple times per year, and the date of death is recorded if the patient has died. The secondary outcomes were survival to hospital discharge and out-of-hospital survival (including deaths occurring in the community or after unplanned readmission). We report Kaplan–Meier crude survival estimates for 30-day, 90-day, 1-year, and 5-year survival. Trends in survival over time were examined for each ethnic group and area-based deprivation fifths using 1-year survival over 4 discrete time periods: 2005–2008, 2009–2012, 2013–2016, and 2017–2021.
Statistical analyses
Baseline demographic data were summarised by ethnic group using mean and standard deviation or median and interquartile range as appropriate. Cox proportional hazards models were performed to explore the effect of ethnicity on the primary and secondary outcomes, respectively. Survival time was defined as the time from the first cardiac surgical procedure to either death or the censoring date of 12th August 2022, whichever occurred first. Pre-operative risk of death was estimated using the PRAiS2 model and expressed as a percentage. Reference Rogers, Brown and Franklin25 The PRAiS2 model was not used for any statistical adjustment but has been presented to illustrate differences in pre-operative risk between ethnic groups. Potential confounding for the primary outcome was addressed using causal inference methods. Reference Tennant, Murray and Arnold26 A directed acyclic graph was used to inform the minimal sufficient adjustment set for modelling the total effect of ethnicity on survival, using the DAGitty web application (Supplementary Figure 1). Reference Textor, van der Zander, Gilthorpe, Liśkiewicz and Ellison27 As a result, covariate adjustment for parental socioeconomic status was required to estimate the effect of child ethnicity on survival. The raw income score was used as a surrogate for socioeconomic status in the adjusted Cox models, and the Bayesian Information Criterion was used to confirm that the raw index of deprivation score was superior to the deprivation deciles or fifths. The proportional hazards assumption was tested for each variable in the model. Adjusted Hazard Ratios are displayed with crude survival estimates, expressed as percentages with 95% confidence intervals (CI).
Ethical approval
Patients and parents of children undergoing cardiac surgery are consented at the time of surgery for the use of their data for research and audit purposes, as part of the National Congenital Heart Disease Audit. 7 This project was approved by Leeds Teaching Hospitals NHS Trust Research Governance and Information Governance committees. A letter of approval from the regional Caldicott Guardian was obtained on 12th May 2022 for the use of identifiable patient data.
Results
5,422 cardiac surgical procedures were carried out between 1st January 2005 and 31 December 2021. In this period, 3,508 children underwent their first procedure and were included in the study. The process of refining the study cohort is described in Figure 1. Ethnicity was categorised as White (2,578 children, 73%) and South Asian (634 children, 18%), with 95 (3%) Black children and 201 (6%) children of other ethnic origin. 1,404 children (40%) were resident in the most deprived fifth of the index of deprivation, with South Asian and Black children more often having higher levels of deprivation compared to the White and Other groups. South Asian children were more likely to live closer to the tertiary cardiac centre compared to White children (median 15.3 km (interquartile range 12.3–24.6 km) vs. 36.2 km (17.9–60.7 km), respectively).
Flowchart for the included patient population.

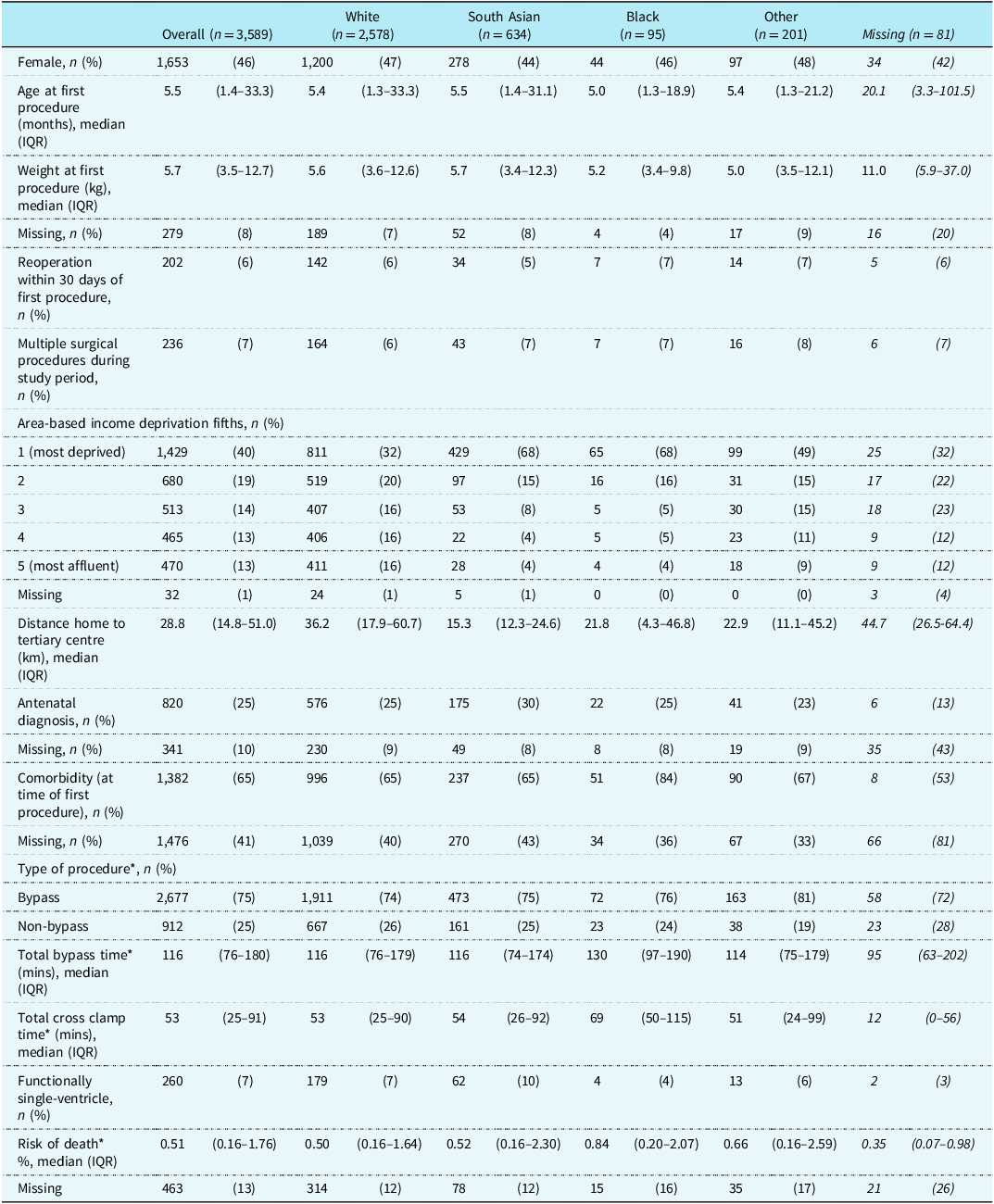
The baseline characteristics of the 3,508 children included in the study, along with those excluded for missing ethnicity, are described in Table 1.
Baseline characteristics of included children by ethnic group. Where categories contain missing data, the proportions are presented by ethnic group

IQR = interquartile range; SD = standard deviation.
*Risk of death was calculated according to the PRAiS2 model.
A greater proportion of South Asian children had a functionally single ventricle circulation compared to White children (62 (10%) vs. 179 (7%), relative risk (RR) 1.41, 95% CI 1.07–1.86). Black children were more likely to have a comorbidity at the time of first procedure (51 (84%) vs. 996 (65%) White, RR 1.39, 95% CI 1.15–1.69) and had a higher overall risk of death as assessed by the PRAiS2 model (median 0.84% (0.20–2.07%) vs. 0.50% (0.16–1.64%) White). Reference Rogers, Brown and Franklin25 Black children had longer bypass time (130 (97–190) mins vs. 116 (76–179) mins White) and cross clamp time (69 (50–115) mins vs. 53 (25–90) mins White). Supplementary Table 1 displays the diagnoses by ethnic group. Diagnoses were similar among all ethnic groups, aside from a higher proportion of atrioventricular septal defects in Black children (17 (18%) vs. 248 (10%) White; RR 1.86, 95% CI 1.19–2.91).
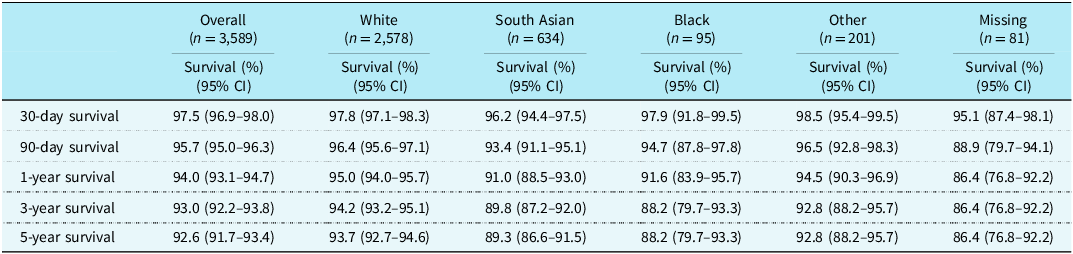
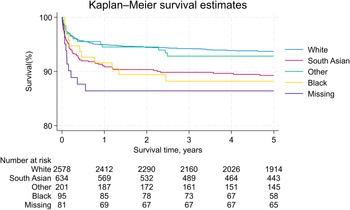
During a total follow-up time of 31,826 patient-years, there were 277 deaths following cardiac surgery. Overall, unadjusted 5-year survival after the first cardiac surgical procedure was 92.6% (95% CI: 91.7–93.4%). Survival rates varied considerably by ethnic group, with White children having the highest survival (93.7%, 92.7–94.6%), followed by Other (92.8%, 88.2–95.7%), South Asian (89.3%, 86.6–91.5%) and Black children (88.2%, 79.7–93.3%). This survival difference was not evident at 30 days post-procedure, but widened progressively at 90 days, 1 year, 3 years and 5 years, as displayed in Table 2.
Overall crude survival estimates (%) by ethnic group
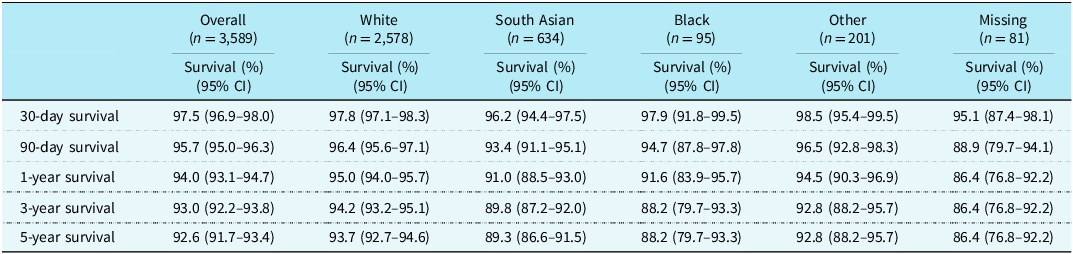
CI = confidence interval.
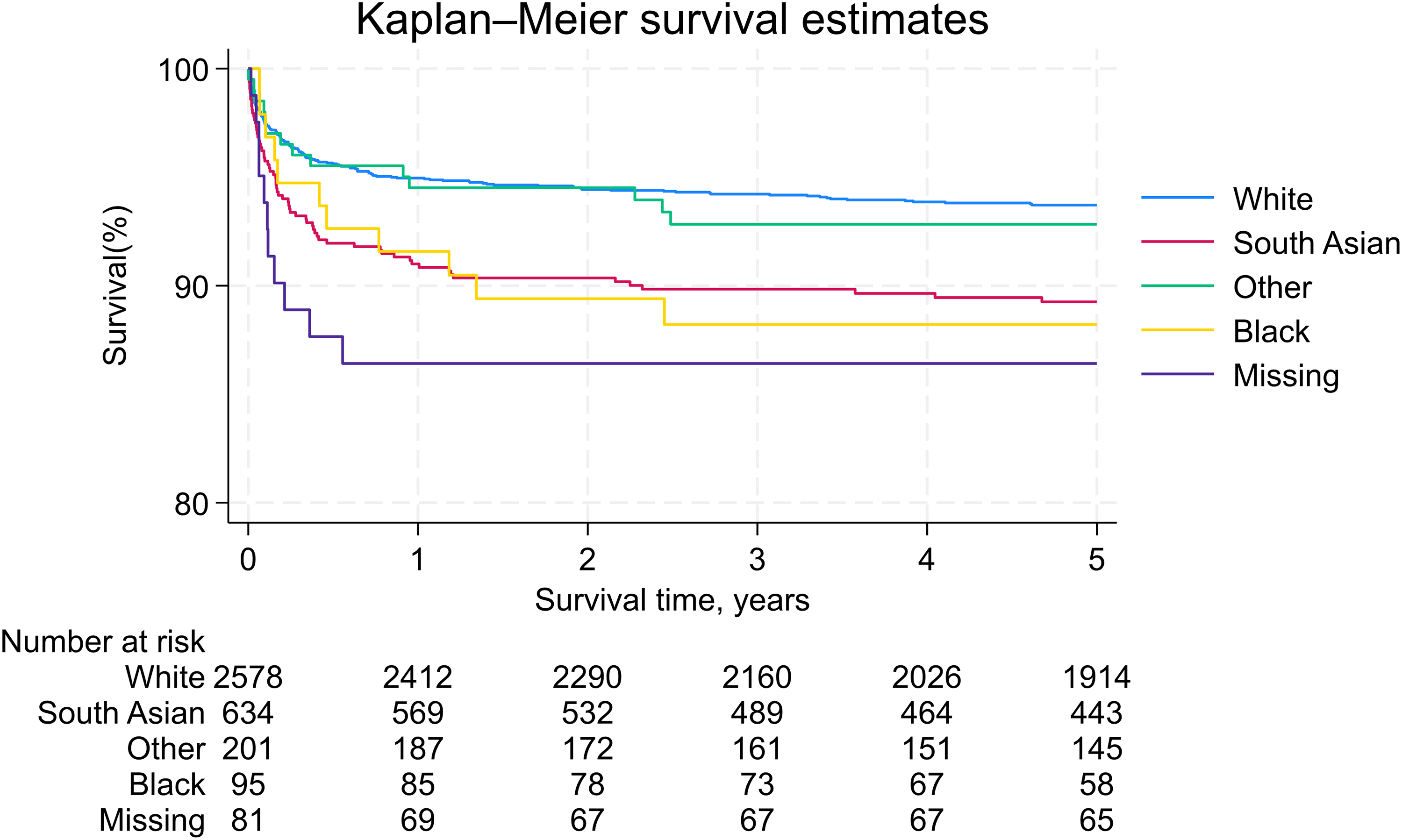
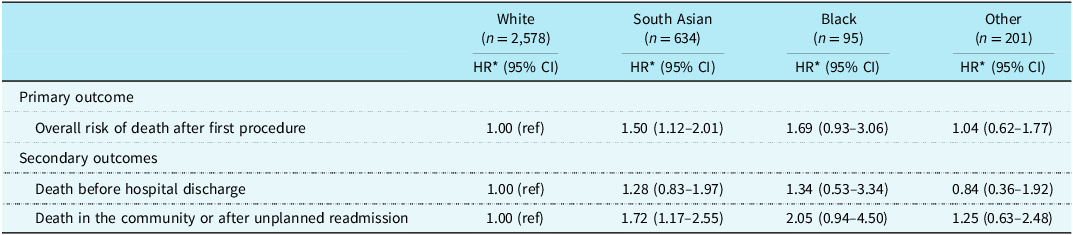
After adjustment for area-based deprivation, South Asian children (Hazard Ratio (HR) 1.50, 1.12–2.01) and Black children (HR 1.69, 0.93–3.06) had a higher risk of death compared to White children during the study period (Figure 2). We observed a higher rate of death in the community or after unplanned readmission (South Asian: HR 1.72, 1.17–2.55; Black: HR 2.05, 0.94–4.50), but death before hospital discharge did not differ between ethnic groups (Table 3). Separate models were run with additional adjustment for diagnosis and pre-operative risk of death. The overall effect size remained similar; therefore, these factors did not appear to mediate the survival differences between ethnic groups.
Kaplan–Meier 5-year survival following the first cardiac surgical procedure by ethnic group.
Adjusted hazard ratios (HR) and corresponding 95% confidence intervals (95% CI) from cox regression models presenting the effect of ethnic group on risk of death in children following first cardiac surgical procedure
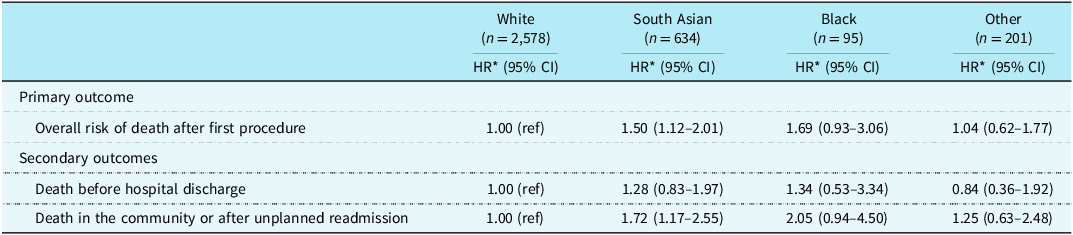
*Adjusted for area-based income deprivation score.
HR = Hazard Ratio; CI = confidence interval.
Unadjusted 1-year survival increased across the study period, from 92.2% (90.1–93.8%) in 2005–2008 to 95.6% (93.9–96.8%) in 2017–2021 (Supplementary Table 2, Supplementary Figure 2). Ethnicity-related 1-year survival inequities between South Asian and White children were highest in 2005–2008 (White 93.5 %, South Asian 86.6%) and gradually reduced over time (2009–2012: 94.1% vs. 91.0%; 2013–2016: 95.7% vs. 91.6%; 2017–2021: 96.8% vs. 94.7%). A similar pattern of improving survival was seen for Black and Other ethnic groups from 2005 to 2016. However, hazard ratios increased in all ethnic groups in the 2017–2021 period, with a fall in overall survival for Black and Other children.
Discussion
This study provides the first analysis of trends in survival following cardiac surgery for children of different ethnic groups in the UK. South Asian and Black children had reduced survival following cardiac surgery compared to White children. We studied the trends in 1-year survival from 2005 to 2021 and found that survival inequities reduced throughout the study period until 2016, followed by a marked increase in survival differences in the most recent period. The excess deaths predominantly occurred after hospital discharge, in the community or after unplanned readmission. We observed a higher proportion of Asian children with functionally single-ventricle heart disease, and Black children had more comorbidities and a higher pre-operative risk of death; however, these factors did not fully explain the lower survival.
Our analysis features children in a single tertiary cardiac centre; however, our results are consistent with several previous studies reporting ethnic disparities in survival for UK children. Knowles et al. studied the survival to 1 year of age for 5350 infants undergoing cardiac surgery for CHD. Reference Knowles, Ridout and Crowe8 Across all centres in England and Wales, British Asian (Indian, Pakistani and Bangladeshi) infants had higher mortality compared to White infants (relative risk 1.52; 95% CI 1.19–1.95). There was also a trend towards higher mortality in Black infants. Reference Knowles, Ridout and Crowe8 We have reported similar differences for overall survival of South Asian children compared with White children (HR 1.50; 95% CI 1.12–2.01). This confirms the major ethnic disparities that are present in the UK, across children of all ages undergoing cardiac surgery. Contrary to our results, Knowles et al. reported higher in-hospital mortality for South Asian infants and no difference in “unexpected” deaths in the community. Reference Knowles, Ridout and Crowe8 This may be related to our extended follow-up period and ability to capture a greater number of late deaths. Differences may still exist between cardiac centres, and this should be an ongoing focus for national audit data.
Our results demonstrate a higher rate of deaths in the community or after unplanned readmission for South Asian and Black children, although the explanation for this is unclear. An analysis of childhood cancer outcomes in Yorkshire also observed that South Asian children with lymphoma had 15% reduced survival compared to White children. Reference Cromie, Hughes and Milner28 One hypothesis is that differences in access to healthcare may be present across ethnic groups. We investigated possible geographical differences, and we found that children of South Asian and Black origin lived closer to the tertiary surgical centre on average compared to White children. This is consistent with one previous study, where children living 90–300 minutes from the nearest cardiac centre had a lower risk of unplanned readmission, but not higher mortality. Reference Pinto, Lasa, Dominguez, Wernovsky, Tabbutt and Cohen29 We adjusted our results for area-based deprivation by household income. We were not able to measure other factors, such as parents’ first language or car ownership, that may influence access to healthcare; therefore, challenges in accessing services may exist. Despite free healthcare in the UK, a diagnosis of CHD still places a significant financial burden on the family that may influence access to healthcare.
We have shown that congenital heart diagnoses vary by ethnicity. There was a greater proportion of septal defects, including AVSD, in Black children compared to other ethnicities, making up 46% of all children within this group. This has been observed in multiple previous studies. Reference Knowles, Ridout and Crowe8 The RACHS-2 risk stratification places VSD closure at the lowest risk category, and a complete AVSD repair is in the second-lowest risk category. Reference Allen, Zafar and Mi30 However, Black children had a higher pre-operative risk of death compared to White children according to the PRAiS2 model. This model encompasses procedural and diagnostic information, in addition to comorbidity burden, age and weight. Reference Rogers, Brown and Franklin25 In our study, black children had a greater number of comorbidities, and slightly lower age and weight at their initial surgery. This is consistent with one US study where African-American children undergoing cardiac surgery had higher severity of illness scores and increased odds of postoperative mortality. The authors described that adjusting for the severity of illness removed the survival difference. Reference Tjoeng, Jenkins, Deen and Chan3 However, when we conducted a similar analysis, the hazard ratio was not substantially altered by adjusting for pre-operative risk of death. This may be due to other factors we could not capture, or differences in social, cultural or healthcare differences between the US and UK.
Higher overall childhood mortality has been reported for South Asian and Black children across the entire population in England and Wales 31 We were not able to obtain cause of death for children in this study; therefore, non-cardiac causes may have contributed to the ethnic disparities in survival. However, the leading cause of death in children nationally is congenital anomalies, and this is responsible for the majority of the variation in mortality amongst children across different ethnic groups. 31,Reference Firth, Petherick and Oddie32
A third contributor to the reported inequities may be due to antenatal diagnosis. Termination of pregnancy in England is offered at any gestation for serious fetal abnormalities. 33 A lower termination rate for South Asian mothers after fetal diagnosis of CHD has been reported previously. Reference Lillitos, Nolan and Cave34 This may result in a population of South Asian children with a more severe phenotype of CHD relative to White children born with CHD, and subsequently worse outcomes. Lillitos et al. also observed that single-ventricle infants of South Asian mothers had reduced survival to the first postnatal procedure. Reference Lillitos, Nolan and Cave34 We were not able to assess survival from fetal diagnosis; however, we did observe a higher rate of functionally single-ventricle heart disease in the South Asian group. We hypothesise this is due to choices around termination, in addition to genetic factors. However, with the advancements in fetal diagnosis over this time period, we would have expected inequities to grow rather than reduce, as we have shown. Therefore, this may be a contributing factor, but not the primary explanation for the inequities we have described.
This study describes the changes in ethnicity-specific 1-year survival for children following cardiac surgery in the UK in the modern era. Survival inequities between South Asian and White children were greatest in 2005–2008 (86.6% vs 93.5%, respectively). Overall, 1-year survival improved over the study period, with a difference of only 2.1% between White and South Asian children in 2017–2021. However, we observed an unexpected reduction in 1-year survival for Black and Other groups in 2017–2021. Whilst we were not able to explore this in further detail, it is important to consider the role the COVID-19 pandemic may have had on survival inequities for those undergoing surgery between 2020 and 2021. These may result from delayed surgery, fewer face-to-face clinics, reduced screening, late presentation to the hospital or vaccine uptake. Reference Protopapas, Lo and Vida35 Acknowledging that small group sizes may have contributed to this observation, this effect requires further study to ensure that survival continues to improve for all children.
Limitations
A minority of children had to be excluded from the multivariable regression analyses due to missing ethnicity data (2%). However, all data were collected for national audit purposes prospectively and therefore had high quality and complete patient information. We made every attempt to minimise missing data, including cross-referencing with the PICANet database. Regular life status checks were made, ensuring the validity of our primary outcome measure. In addition, our novel approach measuring temporal changes in inequities over the last 17 years has revealed important trends in survival inequities.
To assess the socioeconomic status of children undergoing cardiac surgery, we used the income domain of the index of deprivation according to parental postcode. 24 Whilst this is a well-established and widely-used metric, it may be limited in predicting an individual’s level of income or employment deprivation. Reference McCartney, Hoggett, Walsh and Lee36 Therefore, whilst we have not shown significant variation in outcome by index of deprivation, socioeconomic status may still play an important role in influencing outcomes. This is notable given the high degree of association between ethnicity and socioeconomic status.
Data on parents’ first language, genetic information and cause of death were not available in the current study. This limited the extent to which some factors underpinning ethnic variation in survival outcomes could be explored. We did not have data on maternal smoking, alcohol use or mental health, and these are also potential confounding factors related to ethnicity and survival. Data for comorbidities were also incomplete, particularly in the oldest cohort of patients. This was because comorbidities were not previously required for national audit data. As the proportion of missing comorbidities data was high (41%), we did not feel this could be addressed using statistical imputation. When assessing unplanned readmissions following surgery, we could only capture admissions that occurred with a cardiac surgical procedure; therefore, some out-of-hospital deaths may in fact have been after readmission for a non-cardiac illness. However, we expect this number to be small, and is unlikely to influence the inequities seen.
Impact on current practice
Our study highlights the ongoing challenge of healthcare inequities facing children with CHD. This affects children at all stages of treatment, especially during long-term follow-up after cardiac surgery. Whilst the focus of this study has been on survival after cardiac surgery, it is likely that inequities may also exist for morbidity, but may be less apparent. Whilst survival inequities generally improved from 2005 to 2016, the challenge of ensuring equality in outcomes for all children still exists. Clinicians should make every effort to reduce modifiable inequities, including maximising access to services.
Conclusion
Black and South Asian children have reduced survival after cardiac surgery compared to White children, independent of socioeconomic status, diagnosis and other pre-operative risk factors. The majority of excess deaths occurred after hospital discharge or unplanned readmission. Whilst survival differences between have gradually reduced over the last two decades, South Asian and Black children still show poorer 1-year survival, and the explanation for this effect remains unclear.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951126112876.
Acknowledgements
We would like to thank Stacey Boardman for her assistance with data collection.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors. D.C. received funding from the National Institute for Health Research as part of an Academic Clinical Fellowship.
Competing interests
None.




 Open access
Open access