


Introduction
Preoperative urine culturing in asymptomatic patients undergoing non-urologic surgery is a low-value intervention that increases costs, antimicrobial exposure, and healthcare utilization without improving patient outcomes. Reference O’Brien, Schweizer and Strymish1–Reference Gupta, Wagenlehner and Wilcox3 This holds true across neurological, orthopedic, and vascular surgeries. Reference O’Brien, Schweizer and Strymish1,Reference Gallegos Salazar, O’Brien, Strymish, Itani, Branch-Elliman and Gupta2 Multiple professional organizations recommend against routine preoperative urine cultures. The Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA) advise against testing for and treating asymptomatic bacteriuria (ASB) in non-urological surgery patients. Reference Nicolle, Gupta and Bradley4 The American College of Surgeons’ (ACS) best practice statement for preoperative assessment of geriatric patients says routine urinalysis is not indicated, Reference Chow, Rosenthal, Merkow, Ko and Esnaola5 and the ACS National Surgical Quality Improvement Program guideline for catheter-associated urinary tract infection (UTI) prevention recommends not screening for or treating ASB in catheterized patients. 6 Despite these recommendations, unnecessary preoperative urine cultures remain prevalent.
Diagnostic stewardship optimizes diagnostic test use to prevent diagnostic error and reduce unnecessary downstream treatment including antibiotic overuse. Reference Morgan, Malani and Diekema8 Education combined with audit and evaluative feedback Reference Whittington, Ho and Helfrich9 has demonstrated effectiveness in modifying clinical behavior and represents an evidence-based strategy for reducing low-value care, especially when paired with co-interventions such as interactive feedback and an actionable improvement plan. Reference Ivers, Yogasingam and Lacroix10
Methods
We conducted a prospective pre/post quasi-experimental pilot study across four VAMCs randomly selected from a 15-site research consortium over the following periods: (1) preintervention, January 1 – December 31, 2022, (2) postintervention, January 1 – October 31, 2023. The intervention targeted patients in neurosurgery, orthopedic, and vascular surgery specialties. Reference Gallegos Salazar, O’Brien, Strymish, Itani, Branch-Elliman and Gupta2 The multi-modal intervention comprised site-specific data feedback forms (intervention tool, Supplements A–C) and implementation activities (audit with interactive and evaluative feedback, and education). Our implementation approach was based on interviews with VA surgeons and other healthcare workers that identified audit and feedback combined with education as the most acceptable methods to reduce preoperative urine cultures. Reference Dukes, Gupta and Walhof11 Feedback forms were developed by the central research team and delivered by local facility teams. They provided benchmarking data comparing urine culture rates by unit and specialty against consortium averages and summarized current evidence against preoperative urine cultures, with advice on additional infection prevention steps.
The intervention was implemented at each site by multidisciplinary local facility teams. Each local team included a site-based study co-investigator as study champion (e.g., hospital epidemiologist). Local teams used facility-level knowledge for targeted audit, feedback and education communication with surgical practice leaders and some individual high utilizers. The implementation activities ranged from targeted data review with surgical specialty leadership to general education for surgical services (e.g., in surgical meetings) using the feedback forms.
We collected data on all urine cultures obtained within 30 days before scheduled surgery on asymptomatic patients, excluding cultures performed for acute infectious symptoms (e.g., cultures collected in emergency departments or from febrile patients (temperature > 38°C) or from patients with urinary symptoms identified via manual chart review). Reference O’Brien, Schweizer and Strymish1
The outcome was the proportion of surgeries with preoperative urine cultures. We compared rates between preintervention and postintervention periods, calculating preoperative urine culture rates by facility and surgical specialty. Statistical significance was assessed using χ2 tests. Analysis was performed using R, version 4.0.5 (R Core Team) and Microsoft Excel.
Of note, two intervention VAMCs (VAMC 2 and 4) already had diagnostic stewardship strategies in place to reduce unnecessary urine cultures and were involved in a study piloting additional strategies to reduce inpatient antibiotic use for UTI during our intervention period. Reference Claeys, Brown and Pineles12 The additional strategies piloted did not specifically target preoperative urine culturing, did not measure outpatient urine cultures, and were not uniformly effective in reducing urine cultures. Reference Claeys, Brown and Pineles12 This research was approved by the VA Central IRB and each VAMC’s research and development committee.
Results
Overall, 5,508 surgeries eligible for inclusion were performed at the four intervention VAMCs across the study period, with 952 preoperative urine cultures eligible for inclusion. There was substantial variation in preoperative urine culturing by VAMC and surgical specialty (Table 1). Preintervention, rates ranged from 1% to 79% for neurosurgery, 1% to 52% for orthopedic surgery, and 4% to 19% for vascular surgery.
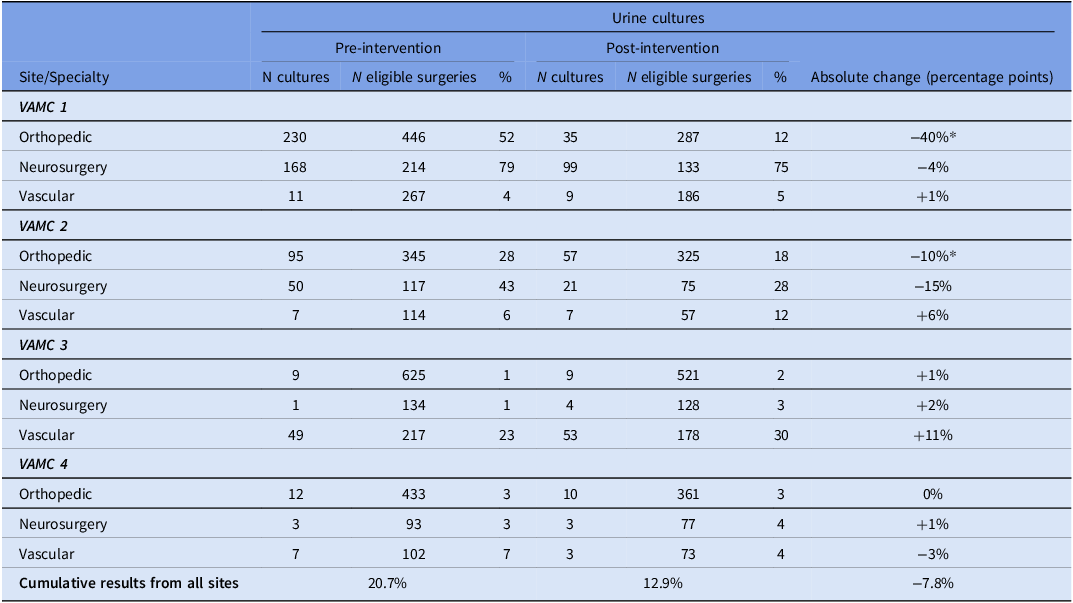
Preoperative urine culture rates by facility and surgical specialty

Table 1. Long description
The table presents data on preoperative urine culture rates by facility and surgical specialty across four Veterans Affairs Medical Centers (VAMCs) before and after an intervention. It includes columns for the number of urine cultures, eligible surgeries, and the percentage of cultures pre- and post-intervention, along with the absolute change in percentage points. The table is divided into sections for each VAMC, with rows for orthopedic, neurosurgery, and vascular specialties. Notable trends include a significant reduction in urine culture rates for orthopedic surgery at VAMC 1 and VAMC 2, while neurosurgery and vascular surgery show varied changes across different VAMCs. The cumulative results from all sites indicate an overall decrease in urine culture rates post-intervention.
* Statistically significant differences (P < .05).
In total, preoperative urine culture rates decreased from 20.7% in the preintervention period to 12.9% in the postintervention period, representing a 37.5% relative reduction (95% confidence interval [95%CI: 29.2%–44.8%]; P < .01). Two VAMCs demonstrated statistically significant declines in urine culturing (Figure 1).
Change in percentage urine culture postintervention at each site. * Statistically significant change in percentage (P < .05).

Figure 1. Long description
The horizontal bar graph compares the percentage change in urine culture post-intervention at four sites. The x-axis ranges from negative fifty percent to positive twenty percent, with increments of ten percentage points. The y-axis lists four sites labeled VAMC 1, VAMC 2, VAMC 3, and VAMC 4. VAMC 1 shows a significant decrease of forty-three percent, marked with an asterisk indicating statistical significance. VAMC 2 shows a decrease of nineteen percent, also marked with an asterisk. VAMC 3 shows an increase of fourteen percent, and VAMC 4 shows a slight decrease of two percent. The bars are colored in dark blue, and the values are clearly labeled on each bar. All values are approximated.
Orthopedic surgery demonstrated the largest overall reductions, though results varied considerably between facilities. VAMC 1 showed the most dramatic reduction in orthopedic surgery urine cultures (52% to 12%, 76.3% relative reduction, [95%CI: 67.4%–82.9%]; P < .01]). VAMC 2 showed a reduction in neurosurgery (43% to 28%, 34.5% relative reduction, [95% CI: .36%–56.9%]; P = .05]) and a significant reduction in orthopedic surgery (28% to 18%, 36.3% relative reduction, [95%CI: 14.8%–52.4%]; P < .01). Some surgical specialties experienced small, non-statistically significant increases in urine testing. VAMCs 3 and 4 had relatively low baseline rates and showed minimal changes.
Discussion
Our multi-center study demonstrates that education combined with audit and feedback may reduce unnecessary preoperative urine culture testing. The 37.5% overall relative reduction represents progress toward evidence-based preoperative care and supports the potential for similar diagnostic stewardship strategies.
The substantial variation in preintervention urine culture utilization among facilities and surgical specialties suggests that usage is driven primarily by individual providers and local contextual factors, rather than specialty-specific or nationwide policies. Differences among sites may also reflect independent VAMC efforts to decrease utilization. VAMC 2 and 4 each had additional strategies implemented as part of quality improvement or research and these had variable results in terms of urine culture rates and antibiotic use rates. These additional strategies did not lead to uniform reductions across specialties. This underscores our findings that interventions need to be tailored to the specific site/unit/specialty to have the most efficient effect. Reference Claeys, Brown and Pineles12 These concurrent activities and the heterogeneity associated with a tailored intervention are limitations of our work, but reflect the real-world conditions of complex academically-affiliated medical centers.
Our results also demonstrate ceiling effects of low baseline usage: at VAMCs 3 and 4, preintervention rates were low, such that further intervention produced no statistically significant changes. Urine culture persistence at the lowest-utilization site postintervention suggests that some cultures remain clinically indicated (e.g., symptoms of UTI). Another limitation is that our research focused solely on process rather than clinical outcomes. Yet, prior studies have consistently shown that preoperative ASB is not associated with postoperative surgical site infections or UTI. Reference O’Brien, Schweizer and Strymish1
Orthopedic surgery showed the greatest response to intervention, potentially reflecting education on recent evidence against routine preoperative urine cultures in joint replacement surgery, and opportunities for focused educational messaging around prosthetic joint infection prevention. Variation in neurosurgery and vascular surgery likely reflects differences in baseline knowledge, guideline interpretation, and local surgical culture, underscoring the importance of targeted strategies.
These findings support the effectiveness of targeted strategies for reducing low-value preoperative testing, when delivered via local clinical champion engagement. Observed variation between facilities highlights the need for flexible implementation approaches adaptable to local contexts and practice patterns. Advantages include adaptability to specialty, and the potential to spread knowledge to trainees and colleagues (train the trainer effect).
Conclusion
This pilot intervention of education combined with interactive audit and evaluative feedback may have reduced unnecessary preoperative urine culture testing across multiple VAMCs. Substantial variation in intervention effectiveness between facilities and surgical specialties emphasizes the importance of tailored diagnostic stewardship strategies.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ice.2026.10470
Acknowledgments
The authors thank the local champions at participating VAMCs for their dedication to improving perioperative care quality. The authors also acknowledge the support of the VA/CDC Partnered Infection Control Practice-Based Research Network and the healthcare teams who participated in this quality improvement initiative.
Financial support
This work was funded by the US Department of Veterans Affairs Health Services Research And Development (grant no. IIR 18-057; PIs KG and MLS).
Competing interests
The authors declare no conflicts of interest.




 Open access
Open access