


Introduction
Hospital onset bacteremia (HOB) is a leading cause of morbidity and mortality in hospitalized patients.1
The acquisition of nosocomial infections is contingent upon an interplay of patient-specific factors (intrinsic factors), such as the degree of immuno-compromised and comorbidities, and extrinsic factors including medical interventions and devices.1–Reference Schrank, Sick-Samuels and Bleasdale4 The nosocomial infection rate serves as a pivotal indicator of the quality and safety of healthcare, with the ultimate objective being the reduction of nosocomial infections.1,Reference Dantes, Rock and Milstone3
Surveillance of HOB is conducted mostly in intensive care units.5,6 There is limited data regarding the rates and sources of hospital wide HOB. Additionally, there is no standardized and uniform protocol for infection prevention measures aimed at reducing HOB acquisition, or standardized methodology for evaluating the prevention potential of various sources of HOB.Reference Dantes, Abbo and Anderson2–Reference Schrank, Sick-Samuels and Bleasdale4
Structured frameworks developed by Dantes et al. and Schrank et al.Reference Dantes, Rock and Milstone3,Reference Schrank, Sick-Samuels and Bleasdale4 enable standardized assessment of HOB preventability by integrating intrinsic and extrinsic risk profiles. Based on their model, we aimed to quantify the prevention potential of hospital wide HOB that were investigated at our hospital as a quality program,Reference Mudrik-Zohar, Chowers, Temkin and Shitrit7 and compare the calculated quantitative prevention potential to the qualitative assessment conducted by both the treating departments and infection control unit.
Methods
We conducted a retrospective study at Meir Medical Center, a secondary 797 beds academic hospital in Israel, 37% internal medicine, 5% intensive care, and 7% geriatric.
We analyzed all nosocomial bacteremia cases from January 2022 to March 2023.
Each case was assessed using
Qualitative assessment: As part of the infection control surveillance, daily reviews of positive blood cultures conducted by the infection control unit. Cultures taken after day 3 of admission with no prior infection, within 7 days postdischarge, or post procedure (7 days) or surgery (30 days), excluding common commensals, were suspected nosocomial and sent to the departments for investigation. Residents or senior physicians in treating departments filled structured electronic form in which they determined whether the bacteremia was nosocomial and preventable. Acquisition status and preventability was reassessed by senior infection control physicians (See investigation form in supplementary material).
Quantitative assessment
A separate quantitative assessment was made by infection control unit, based on Dantes and Scharnk’s et al. works.Reference Dantes, Rock and Milstone3,Reference Schrank, Sick-Samuels and Bleasdale4
Intrinsic and extrinsic factors (Supplementary Table 1) were scored on a one to six (1–6) scale, resulting in a preventability score (1–6) (Supplementary Figure 1), with 5–6 indicating high prevention potential, and 1–2 low prevention potential.
To allow comparison of the quantitative assessment of preventability as determined using the framework developed by Dantes et al.Reference Dantes, Rock and Milstone3 with the qualitative assessments of preventability, nosocomial bacteremia with a preventability score of 4–6 considered preventable, score of 1 considered not preventable, and preventability score of 2–3 considered undetermined.
Qualitative preventability determination of the department and infection control team were compared to the quantitative assessment.
HOB sources were clinically defined. A case was considered primary when appropriate diagnostic evaluation (e.g., sputum or urine cultures, imaging) was performed, no source was identified, and no peripheral line was present. Peripheral line-associated bloodstream (PLABSI) was defined as the source in the presence of a peripheral line, on the day of line removal and the day following it, and in the absence of another source of bacteremia. Unknown source was defined when no source was identified, and evaluation was incomplete.
Statistical analysis
Statistical analysis included descriptive statistics and standard tests (Chi-square, Fisher, t-test, Mann–Whitney). Significance was set at p < 0.05. Agreement between assessments was measured using percent of agreement.
Results
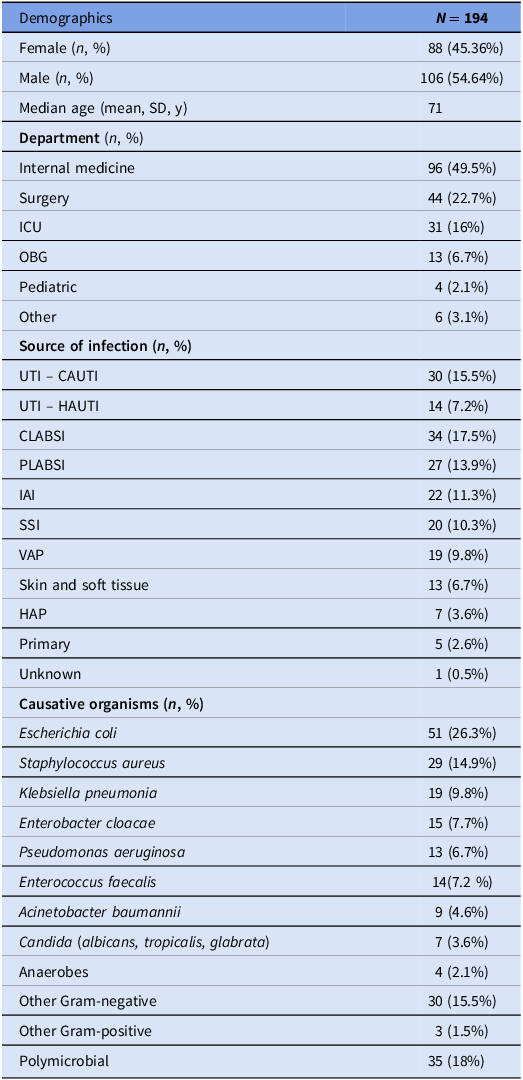
A total of 194 HOB cases were analyzed. According to the department reports, only 88 (45.4%) were classified as nosocomial. Internal medicine departments accounted for 49.5%of cases, followed by surgical departments (22.7%), and intensive care unit (ICU) (16%) (Table 1).
Bacteremia cases characteristics—according to medical charts and infection control unit investigation

Note. ICU, intensive care unit; OBG, obstetrics and gynecology; UTI, urinary tract infections; CAUTI, catheter associated UTI; HAUTI, hospital acquired UTI; CLABSI, Central Line-associated Bloodstream Infection; PLABSI, peripheral line-associated bloodstream infection; IAI, intra-abdominal infection; SSI, surgical site infection; HAP, hospital acquired pneumonia; VAP, ventilator-associated pneumonia.
The predominant origin of infection was urinary tract infection (22.7%), of which 68% were catheter associated. Other sources included central line-associated blood stream infection (17.5%), PLABSI (13.9%), intra-abdominal (11.3%), and surgical site infection (10.3%) (Table 1).
The most frequently isolated organisms were Escherichia coli (26.3%), Staphylococcus aureus (14.9%), and Klebsiella pneumonia (9.8%) (Table 1).
Intrinsic risk scores were low in 57 (29.4%) of HOB investigated, moderate in 85 (43.8%), and high in 52 (26.8%). Extrinsic risk scores were low in 26 (13.4%), moderate in 44 (22.7 %), and high in 124 (63.9%).
Quantitative prevention potential score, based on Dantes et al. toolReference Dantes, Rock and Milstone3 was high in 51.6%, moderate in 36.6%, and low in 11.8% (Supplementary Table 2). Qualitative assessment of the infection control unit classified 66% of cases as preventable and only 4.1% as unpreventable. The departments qualitative assessment classified only 20.1% as preventable, and 40.2% as having undetermined preventability potential.
Percent agreement between the low/medium/high calculated preventability score to the department’s determination was 0.3, and 0.5 to the infection control unit determination.
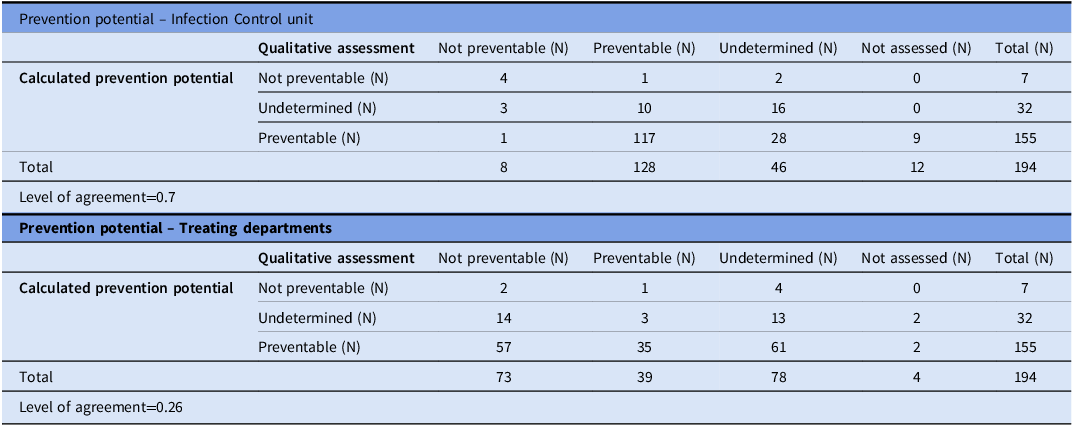
Percent agreement between the quantitative determinations of the bacteremia as preventable/undetermined/not preventable and the qualitative determination by the departments was 0.26, and by the infection control unit was 0.7 (Table 2).
Agreement levels between the quantitative rating score and the qualitative assessment

Discussion
Our study found that the most of HOB cases had a high prevention potential, primarily due to extrinsic factors, similar to prior studies suggesting significant proportion of HOB events are preventable under optimal conditions.Reference Dantes, Abbo and Anderson2,Reference Dantes, Rock and Milstone3
Leekha et al.Reference Leekha, Robinson and Jacob8 evaluated the sources and preventability of HOB events. They categorized cases of bacteremia based on their sources into commensal and non-commensal bacteria. Only 36% of non-commensal HOB events were considered potentially preventable.Reference Leekha, Robinson and Jacob8 These findings were consistent with previous preventability assessments of HOB events, ranging from 19.5% to 44%.Reference Bonnal, Mourvillier and Bronchard9,Reference Stack, Dbeibo, Fadel, Kelley, Sadowski and Beeler10 The fact that we found a higher percentage of preventable events may be explained by differences in data interpretation, particularly the fact that we did not initially classify positive culture events attributed to commensals as HOB events.
The discrepancies between department assessments of nosocomial status and preventability highlight the ongoing need for targeted interventions to refine the understanding of HOB definitions and improve bacteremia prevention strategies. This finding underscored the importance of directing our efforts toward prevention rather than merely focusing only on acquisition.
Since intrinsic factors cannot be modified during hospitalization, prevention efforts should focus on minimizing extrinsic risk factors to improve patient outcomes.
Based on these insights we are planning to incorporate a structured, quantitative assessment into the self-investigation process. Additionally, we aim to strengthen mutual discussions regarding prevention potential, particularly emphasizing interventions targeting extrinsic risk factors that can be actively mitigated.
By integrating quantitative assessment into routine evaluations, we seek to create a shared understanding with clinical teams, ultimately enhancing prevention strategies and reducing nosocomial infections.
Study limitations
This study has several limitations. First, it was a single-center study, which may limit the generalizability of our findings. Second, the study is qualitative in nature, relying on clinical judgment for the assessment of nosocomial acquisition and preventability, which may introduce subjectivity. Third, as the data were extracted from electronic medical records, there is a possibility that not all relevant information was complete or accurately documented.
Despite these limitations, our study provides valuable insights into the preventability of HOB and highlights the importance of structured assessment tools in infection control efforts. Future multi-center studies using standardized methodologies and automated data collection may help further validate these findings.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/ice.2025.10298.
Acknowledgments
There was no financial support or conflict of interest.



 Open access
Open access