

Introduction
In an era where the flow of information is both boundless and instantaneous, institutional health communication faces an extraordinary challenge. The overwhelming circulation of health content, ranging from rigorous scientific insights to false, misleading, and overall poor-quality information, has thrust health institutions into a pivotal role. They are tasked not only with disseminating credible, evidence-based messages but also with safeguarding public trust and fostering resilience. This Element addresses these pressing demands and provides a roadmap for empowering institutions to craft communication practices that are as scientifically robust as they are socially transformative.
The term institutional in this context encompasses the spectrum of public communication efforts by traditional healthcare settings – such as hospitals, clinics, rehabilitation centers, and nursing homes – as well as broader health organizations, including government agencies, nonprofit groups, research institutions, and international bodies. While health institutions focus on direct medical care and patient support, health organizations engage in activities such as policymaking, health promotion, disease prevention, and research. These entities often collaborate to address health challenges at local, national, and global levels. For clarity and brevity, the term health institutions will be used throughout this Element to represent both, while recognizing their distinct yet complementary roles.
The rationale for this work stems from the critical need to navigate the complexities of contemporary communication landscapes while preserving the integrity, relevance, and trustworthiness of health messaging. It integrates perspectives from multiple disciplines, including health communication, behavioral sciences, social marketing, political science, media studies, and rhetorical theory. Central to its framework is the promotion of participatory communication models that actively engage individuals and communities. These models emphasize collaboration, enhance public health and scientific literacy, and empower autonomous, informed decision-making.
This Element is structured around seven interconnected sections, each addressing a critical aspect of institutional health communication. It opens with a discussion on the role of health institutions in confronting the rise of poor-quality health information and in balancing transparency, accuracy, and public trust while shifting from top-down messaging to participatory approaches (Section 1). Section 2 explores how institutions can translate complex scientific knowledge into accessible and actionable messages, overcoming barriers such as uncertainty, cognitive bias, and fragmented attention. The intersection of politics and public health is addressed in Section 3, which unpacks the tensions between scientific priorities and political agendas, and the impact of distorted or strategically framed health narratives. Section 4 centers on trust, examining how institutions can build and sustain credibility through transparency, consistency, and meaningful engagement.
Traditional mass media, which continue to shape public health discourse, are analyzed in Section 5, with a focus on aligning institutional communication priorities with media dynamics while safeguarding message integrity. Section 6 turns to the digital world, examining the influence of online creators and the dual potential they hold to amplify evidence-based content or, conversely, spread misleading or manipulative messages. The final section, Section 7, synthesizes classical rhetorical principles with insights from behavioral science and social marketing, offering a strategic framework for designing compelling and effective health messages for diverse audiences and media environments.
Each section is enriched with fictionalized examples based on real-world practices. These serve two essential purposes: to avoid singling out or judging specific institutions or individuals, and to illustrate the diverse and often complex origins of poor-quality information, which may emerge from political agendas, digital influencers, or even within the professional health community. Each section concludes with a practical table that summarizes key strategies and offers guidance for real-world implementation.
Overall, this Element contributes to bridging the gap between academic inquiry and practical application by addressing the nuanced challenges of institutional health communication. The hope, and indeed the dream, is that it may serve not only as a guide but also as an inspiration for building informed, discerning, and resilient communities capable of engaging critically with modern health discourse and making sound decisions in an age of information excess.
1 The Bases of Institutional Communication and the Challenges of Poor-Quality Information
1.1 Overview
In contexts of uncertainty and poor-quality information, the path to effective institutional health communication lies in transparency, participation, and the respectful exchange of knowledge. It’s a dialogue, not a monologue, that empowers individuals and communities alike.
This section examines the fundamental principles of institutional health communication and the challenges it faces in the modern era, particularly in the flood of both accurate and misleading health information that is overwhelming people today.
1.2 Goals of Institutional Health Communication
Health institutions undertake health communication for multiple purposes, each serving a distinct role in improving public health outcomes. These can be grouped into four broad categories.
(1) Informing and educating
Health institutions inform and educate the public. They act as reservoirs of knowledge, providing essential information on diseases, prevention, and treatment. They promote health literacy (Schulz, Reference Schulz, Corrigan, Dillon and Gunstone2012; Parker and Ratzan, Reference Parker and Ratzan2019), address determinants of behavior, and encourage healthier living (Laverack, Reference Laverack2017; Rubinelli and Diviani, Reference Rubinelli and Diviani2020). Extensive literature illustrates how they design and evaluate campaigns and interventions (Naidoo and Wills, Reference Naidoo and Wills2009; Bartholomew Eldredge et al., Reference Bartholomew Eldredge, Markham, Ruiter, Fernández, Kok and Parcel2016).
They disseminate scientific knowledge. Institutions communicate research findings, innovations, and best practices through conferences, publications, websites, media, and social platforms, fostering evidence-based approaches (Funkhouser and Maccoby, Reference Funkhouser and Maccoby1971; Wilson et al., 2017; Turon et al., Reference Turon, Wolfenden and Finch2023).
(2) Managing crises and risks
Health institutions act in crisis communication and risk management. In emergencies, outbreaks, or disasters, institutions function as central information hubs. Risk communication literature, particularly on COVID-19, underscores this role (Glik, Reference Glik2007; Lundgren and McMakin, Reference Lundgren and McMakin2018; Kim and Kreps, Reference Kim and Kreps2020; Loss et al., Reference Loss, Boklage, Jordan, Jenny, Weishaar and El Bcheraoui2021). They clarify preventive measures, outline risks, and guide the public in seeking care and complying with protocols (Kim and Kreps, Reference Kim and Kreps2020; Zhang, Li, and Chen, Reference Zhang, Li and Chen2020; Bolsewicz, 2024).
(3) Shaping policy and practice
Health institutions advocate for policy changes. Drawing on expertise, institutions issue evidence-based recommendations to influence health policy and regulation. Through strategic communication, they aim to bridge research and practice, ensuring decisions are informed by the best evidence (Hubinette et al., Reference Hubinette, Dobson, Scott and Sherbino2017; Townsend et al., Reference Townsend, Tenni, Goldman and Gleeson2023; Bode et al., Reference Bode, Anwar, Best, Patel, Beers, Kaczorowski, Solomon and Chamberlain2024).
They enhance patient–provider interactions. Hospitals and health organizations train professionals in communication to strengthen person-centered care and shared decision-making, ultimately improving healthcare delivery (Spagnoletti et al., Reference Spagnoletti, Bui and Fischer2009; Bylund et al., Reference Bylund, Brown, Bialer, Levin, Ciccone and Kissane2011; Shahnazi et al., Reference Shahnazi, Araban, Karimy, Basiri, Ghazvini and Stein2021; Mahdiabadi et al., Reference Mahdiabadi, Mirzaei, Entezari and Nasiriani2023).
(4) Promoting equity and collaboration
Health institutions address health disparities and promote equity. They reach marginalized and underserved groups to reduce barriers and ensure fair access to health information and services (Freimuth and Quinn, Reference Freimuth and Quinn2004; Schiavo, Reference Schiavo2015; Thornton et al., Reference Thornton, Glover, Cené, Glik, Henderson and Williams2016).
They engage with public communities. By fostering dialogue and seeking input, institutions empower communities to participate in shaping health systems (Scutchfield, Hall, and Ireson, Reference Scutchfield, Hall and Ireson2006; Cyril et al., Reference Cyril, Smith, Possamai-Inesedy and Renzaho2015; Schiavo, Reference Schiavo2015; Adebisi, Rabe, and Lucero-Prisno III, Reference Adebisi, Rabe and Lucero-Prisno2021). Community engagement is a core theme in public health (Cyril et al., Reference Cyril, Smith, Possamai-Inesedy and Renzaho2015; Glanz, Rimer, and Viswanath, Reference Glanz, Rimer and Viswanath2015).
They engage in interdisciplinary and transdisciplinary efforts. Institutions foster collaboration across health disciplines and beyond – medicine, nursing, psychology, economics, sociology, and environmental science – to address chronic diseases and inequities. Communication enables inclusive dialogue and co-created strategies (Flowers, Mertens, and Mulhall, Reference Flowers, Mertens and Mulhall2000; Vyt, Reference Vyt2008; Singh et al., Reference Singh, Küçükdeveci, Grabljevec and Gray2018).
1.3 The Content Basis of Institutional Communication
As analyzed in Evidence-Based Public Health (Brownson et al., Reference Brownson, Anjali and Deshpande2018), health institutions rely heavily on scientific evidence as the foundation of their communication. Scientific evidence, with both philosophical and empirical dimensions (Taper and Lele, Reference Taper and Lele2010), is generated through rigorous methods such as clinical trials, epidemiological studies, and systematic reviews. A key institutional responsibility is to keep pace with research and innovation, integrating emerging findings into communication on medical technologies, treatments, and public health interventions. Evidence provides the basis for informing the public about efficacy, safety, and benefits, and institutions also reason analogically on prior knowledge (Cummings, Reference Cummings2014b). Evidence-based practice, understood as reliance on the best available science (Glasziou and Longbottom, Reference Glasziou and Longbottom1999; Brownson et al., Reference Brownson, Anjali and Deshpande2018), remains the cornerstone of credible communication, maximizing health outcomes while minimizing harm (Killoran and Kelly, Reference Killoran and Kelly2009).
Yet communication extends beyond pure science. Institutions also draw on expert consensus statements and guidelines (Shekelle et al., Reference Shekelle, Woolf, Eccles and Grimshaw1999; Bourrée, Michel, and Salmi, Reference Bourrée, Michel and Salmi2008), which distil scientific knowledge into actionable advice. By integrating such recommendations, they provide guidance relevant to both professionals and the public. Public health data and statistics are another pillar, offering authoritative perspectives on disease trends, risk factors, and the need for preventive measures (Friis and Sellers, Reference Friis and Sellers2020). Risk assessments and modeling add further depth, especially in emergencies: mathematical models quantify risks and project outcomes, helping shape protective behaviors when communicated effectively (Southall et al., Reference Southall, Ogi-Gittins, Kaye, Hart, Lovell-Read and Thompson2023).
Complexities emerge, however, when discussing “evidence-based knowledge.” Data availability and quality often remain contested, creating uncertainty about which sources should guide interventions (Loon and Bal, Reference van Loon and Bal2014). Tailoring evidence to populations is another challenge: while research yields generalized findings, implementation requires contextualization to local determinants and cultures. As McHugh et al. (Reference McHugh, Riordan and Kerins2023) note, evidence must be adapted to specific contexts to be effective. Ethical issues add further layers: balancing individual rights and public health goals is particularly salient given persistent health disparities. This debate, framed by Anand, Peter, and Sen (Reference Anand, Peter and Sen2004) and revived during COVID-19 (Lukmanova and Sotkina, Reference Lukmanova and Sotkina2022), underscores the need to integrate equity and social determinants into evidence-based strategies.
Finally, evidence does not operate in a political vacuum. Policymaking is shaped by stakeholder interests and power dynamics, raising debates about which evidence is prioritized and how it is translated into action. These tensions at the intersection of health and politics will be explored further in Section 3.
1.4 The Approach: From Top-Down Authority to Interactive Engagement
At this juncture, it is crucial to address a pivotal point. Despite their reliance on evidence-based information, institutional communication is not – and should not be – top-down. There are many reasons for this, not least because health institutions cannot compel people to follow advice. Furthermore, a top-down approach often lacks persuasiveness. This phenomenon has been extensively addressed by Thomas Tufte, who calls for a “participatory” approach (Tufte and Mefalopulos, Reference Tufte and Mefalopulos2009), and has been noted by other main authors in the field (Arkin, Reference Arkin2009; Schiavo, Reference Schiavo2013).
In the past, health institutions’ communication predominantly followed a top-down approach, where information flowed primarily in one direction, from the institution to the public in what Neuhauser and Kreps (Neuhauser and Kreps, Reference Neuhauser and Kreps2003a) call the “one-size-fits-all” format. This traditional model emphasizes the authority and expertise of the institutions, assuming that the public would passively receive and comply with the provided information. With the advent of the internet and social media, individuals have become active seekers and generators of health information. People now have access to a vast array of health-related content, ranging from credible sources to misleading or inaccurate information. Often, people now seek out information that aligns with their values, beliefs, and personal experiences and are more likely to trust peer recommendations and online communities (Neuhauser and Kreps, Reference Neuhauser and Kreps2003b; Kreps and Neuhauser, Reference Kreps and Neuhauser2010). For instance, during the COVID-19 pandemic, people turned to various online platforms and social media for information and support, engaging in conversations, sharing personal experiences, and seeking advice from peers (Dahiya et al., Reference Dahiya2021). Clearly, traditional top-down approaches struggled to effectively reach and engage with the public in this dynamic environment.
Another reason for the ineffectiveness of the top-down approach is the complexity of health information. Institutional health communication often relies on scientific evidence and technical language, which can be challenging for the public to understand and apply to their daily lives. This information gap between institutions and the public can create a barrier to informed decision-making. Individuals may feel overwhelmed or disconnected from the information presented, which can lead to confusion and mistrust. For example, when communicating about treatment options for a specific condition, institutions may focus on delivering scientific evidence and technical details. However, patients and the general public may require clear explanations, practical examples, and personalized guidance to comprehend and apply the information effectively. This information gap can sometimes create an environment where people seek simplified and easily understandable explanations, potentially leaving room for the emergence of low-quality information and misconceptions. This is one of the reasons why, as the literature shows, good scientific communication and dissemination are fundamental (Grene, Cleary, and Marcus-Quinn, Reference Grene, Cleary and Marcus-Quinn2017; National Academy of Medicine, 2017; Wilson et al., Reference Wilson2017).
Today, health institutions increasingly recognize the need for two-way communication, actively involving the public in decision-making processes. This shift emphasizes participatory approaches, shared decision-making, and the co-creation of health messages. Rather than simply transmitting information in a one-directional manner, institutions are now aware of the importance of listening to the public, addressing their concerns, and involving them in shaping health policies, programs, and research. This dialogic approach values the public’s input, acknowledging their autonomy and agency, and fostering greater engagement in managing their own health and well-being (Palmer-Wackerly et al., Reference Palmer-Wackerly, Krok, Dailey, Kight and Krieger2014; Cyril et al., Reference Cyril, Smith, Possamai-Inesedy and Renzaho2015; Gonah, Reference Gonah2020).
1.5 Shared Decision-Making
This evolution, rooted in the shift from top-down authority to interactive engagement, is particularly visible in healthcare communication, where interactions between healthcare providers and patients increasingly rely on dialogue rather than unilateral authority. The participatory approach, which is becoming the standard for institutional health communication, is mirrored in the changing dynamics of the patient–provider relationship.
With the rise of consumerism and the movement toward patient empowerment, Shared Decision-Making (SDM) has emerged as the gold standard in healthcare. It represents a collaborative process in which healthcare professionals and patients work together to make informed choices that reflect the patient’s values, preferences, and individual needs. Notably, Sandman and Munthe (Reference Sandman and Munthe2009) explore various models of SDM within the broader context of patient autonomy. At its core, the SDM process involves a mutual exchange of information regarding treatment options, including associated risks and benefits, enabling both parties to deliberate and reach a decision together. In this model, patients are not passive recipients of medical advice but active participants who contribute their knowledge and preferences, while healthcare providers offer their expertise to guide the decision-making process. SDM is characterized by mutual respect, open communication, and a partnership that recognizes the patient’s autonomy and expertise in their own health. This collaborative approach has gained prominence as healthcare increasingly values patient-centered care, emphasizing that decisions should be made jointly, reflecting both the best available evidence and the individual patient’s personal circumstances and values (Edwards and Elwyn, Reference Edwards and Elwyn2009; Elwyn et al., Reference Elwyn, Frosch and Thomson2012; Bomhof-Roordink et al., Reference Bomhof-Roordink, Gärtner, Stiggelbout and Pieterse2019).
Extending the concept beyond the patient–provider relationship, shared decision-making can also refer to a collaborative process in which health institutions and organizations actively involve the public in decision-making processes that shape health policies, programs, and research. This type of dialogue requires several key elements, as discussed in the following.
First, information transparency: Health institutions must ensure transparency by providing accurate, accessible, and comprehensible information about policies, procedures, and available options. Although it is challenging because maintaining information updates requires significant effort, investments in ensuring that the public receives the best information empower individuals to make informed decisions and actively participate in the public health arena (Lee and Li, Reference Lee and Li2021; Kerr et al., Reference Kerr, Schneider, Freeman, Marteau and van der Linden2022; de Barra and Brown, Reference de Barra and Brown2023).
Second, as introduced earlier, engagement and participation: Institutions need to create opportunities for public engagement and participation, encouraging individuals to provide feedback, express their needs and preferences, and contribute to decision-making processes. This may involve soliciting input through surveys, focus groups, public forums, or social media channels, or interviewing individuals in advisory boards or committees. Institutions can establish effective communication channels that enable bidirectional dialogue between the public and decision-makers. As seen during the COVID-19 pandemic, this involves leveraging various mediums such as online platforms, social media, public meetings, and interactive discussions (Kim et al., Reference Kim, Saffer and Liu2022; Nan et al., Reference Nan, Iles, Yang and Ma2022).
Third, as also introduced earlier, collaboration and partnership: Institutions can benefit from actively seeking collaborations and partnerships with community organizations, advocacy groups, and individuals to collectively address health challenges, co-create solutions, and ensure diverse perspectives are considered. Indeed, intersectoral collaboration is key to successfully acting in public health (Townsend et al., Reference Townsend, Tenni, Goldman and Gleeson2023).
Overall, shared decision-making requires providing individuals with the necessary support and resources to participate actively. This may include educational materials, decision aids, access to relevant data, and guidance to facilitate understanding and informed decision-making.
In today’s environment, as well represented in the self-determination theory (Deci and Ryan, Reference Deci and Ryan2008), the principles of autonomy and self-determination must underpin any strategic thinking regarding institutional communication by health institutions and organizations. The recognition of individuals’ rights to make decisions about their own health is paramount. It is, thus, essential to provide people with the best available information, empowering them to make informed choices that align with their values and preferences (Rubinelli et al., Reference Rubinelli, Fiordelli, Zanini and Fiordelli2022, 2023).
However, as discussed below, for this participatory approach to be effective, health institutions must also confront the rising challenges presented by the digital landscape, which can undermine informed decision-making (see, especially, Schulz and Nakamoto, Reference Schulz and Nakamoto2024).
1.6 Confronting the Challenge of Poor-Quality Health Information in the Digital Age
Building on the need for transparent and participatory communication in shared decision-making, poor-quality health information is a central concern. In today’s digital landscape, health institutions must navigate an environment saturated with false, misleading, and suboptimal health content. This challenge arises not only in crises but also in contexts marked by uncertainty, fear, and information overload – conditions that fuel the spread of inaccurate or deceptive material that is difficult to counter (Zhou and Shen, Reference Zhou and Shen2025).
The term infodemic gained prominence during COVID-19 to describe the overabundance of information – both accurate and false – that made it difficult to identify trustworthy sources. Closely related are misinformation (unintentional spread of inaccuracies) and disinformation (deliberate falsehoods with malicious intent). Other concepts include fake news, or fabricated content presented as journalism, and conspiracy theories, which attribute events to hidden plots without evidence (Rubinelli et al., Reference Rubinelli, Myers, Rosenbaum and Davis2020; Briand et al., Reference Briand, Cinelli and Nguyen2021; Purnat, Nguyen, and Briand, Reference Purnat, Nguyen and Briand2023). Ensuring high-quality information is now a priority across health communication and public health, in both theory and practice (Ratzan et al., Reference Ratzan, Larson and Batista2025).
Several factors explain why people believe and propagate misleading health information. Uncertainty heightens the desire for clarity, making individuals receptive to alternative narratives, even if lacking credibility (Beauvais, Reference Beauvais2022). Fear and anxiety can impair critical thinking, prompting reliance on simplistic explanations. Cognitive biases such as confirmation bias (favoring information consistent with preexisting beliefs) and availability bias (relying on readily available information) reinforce acceptance of suboptimal claims (French, Storey, and Wallace, Reference French, Storey and Wallace2023a).
The digital landscape, with its algorithms and echo chambers, further amplifies poor-quality information (Diaz Ruiz and Nilsson, Reference Diaz Ruiz and Nilsson2023). Social media platforms and search engines often prioritize sensational content, creating bubbles that perpetuate confirmation bias. Moreover, deliberate “bad actors” exploit divisions, fears, and biases with sophisticated strategies to spread false narratives, complicating individuals’ ability to assess quality (French, Storey, and Wallace, Reference French, Storey and Wallace2023b; Rubinelli, Reference Rubinelli2025a).
The abundance of often contradictory health information also challenges institutional communication. Easy access to alternative narratives, particularly for chronic or difficult-to-manage conditions, draws individuals to nonevidence-based sources. The persuasive appeal of suboptimal information lies in its framing: it offers immediate answers that resonate with confusion, fears, and skepticism (Tandoc, Reference Tandoc, Jayakumar, Ang and Anwar2021; Peng, Lim, and Meng, Reference Peng, Lim and Meng2023). Such narratives may appear more attractive than evidence-based guidelines, especially when risks seem minimal or behaviors run counter to public health recommendations. Effective institutional communication must therefore prioritize transparency, engagement, and evidence-based information to counter poor-quality content, foster trust, and support shared decision-making. At its core, this requires the rigorous use of scientific knowledge – a foundation explored in the Section on the role of science in institutional health communication (see Table 1).
Key takeaways
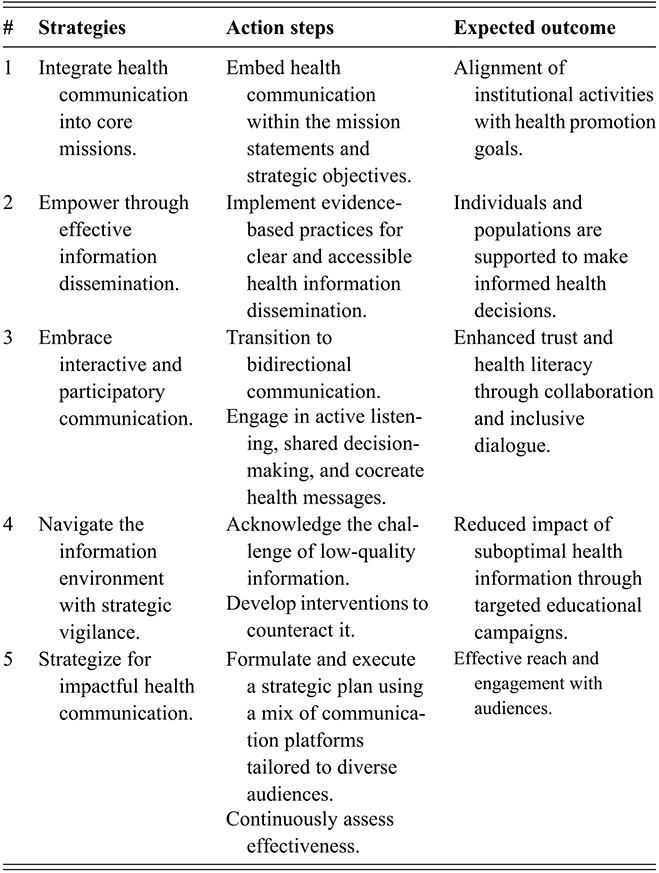
Table 1 Long description
The table presents five core strategies for institutional health communication, each paired with specific action steps and expected outcomes. The first strategy focuses on integrating health communication into institutional missions to align activities with health promotion goals. The second emphasizes evidence-based dissemination of clear and accessible information to support informed decision-making. The third highlights participatory communication through active listening, shared decision-making, and co-creation, leading to increased trust and health literacy. The fourth addresses the challenge of low-quality information by proposing targeted interventions to mitigate its impact. The fifth outlines the need for strategic communication planning using diverse platforms and continuous evaluation to ensure effective audience reach and engagement.
2 Science and Institutional Communication
2.1 Overview
Science communication is a moral obligation, ensuring that scientific knowledge reaches those who can benefit from it the most.
This Section examines the crucial relationship between science and institutional communication, highlighting the fundamental role of health institutions in making scientific knowledge accessible and credible.
2.2 Science as a Technical Field
As established in classical epistemology (Copi, Cohen, McMahon, Reference McMahon and Cohen2016), science is the systematic pursuit of knowledge through observation, experimentation, and analysis. It involves the accumulation of evidence, the formulation of theories, and the ongoing effort to understand natural and social phenomena. In health, scientific research underpins interventions, treatments, and policies that can significantly improve public outcomes. Section 1 has shown that health institutions function as intermediaries, translating complex concepts into accessible language, disseminating accurate information, and promoting health literacy (National Academies of Medicine, 2017).
The relationship between science and institutional communication is multifaceted: institutions rely on science to inform their messages, but their framing and language also shape how science is perceived by the public. Communicating science, however, faces barriers, including its intrinsic complexity, the rapid spread of information via digital platforms, and the circulation of misleading content. A key challenge lies in the technical nature of science, with its specialized methods, terminology, and discourse. Understanding or contributing meaningfully to it requires years of training. This complexity extends even within the scientific community itself (Rubinelli, Schulz, and Nakamoto, Reference Rubinelli, Schulz and Nakamoto2009). Increasing specialization creates silos: scientists from different fields may struggle to understand each other’s methods, theories, and language. Quantitative researchers, focused on objectivity and measurement, may find qualitative approaches difficult to grasp, while qualitative scholars, emphasizing context and lived experience, may struggle with abstract statistical models.
As Kagan (Reference Kagan2009) notes, this reflects deeper epistemological divergences about what constitutes valid knowledge and how it should be interpreted. Quantitative scholars may question the generalizability of qualitative findings, while qualitative scholars may argue that quantitative methods overlook human complexity. These internal debates, although vital for science, are especially difficult to communicate to lay audiences.
2.3 Communicating Scientific Results
2.3.1 Accuracy and Simplicity
The challenge of communicating scientific results in health institutions is a delicate act of balancing accuracy with simplicity, a task made all the more complex by the technical nature of science itself. This technicality, which is essential for precision within the scientific community, can create barriers to public understanding. Thus, when health institutions endeavor to communicate scientific findings, they must make this specialized knowledge accessible to a broader audience without compromising the integrity of the information (Grundmann and Cavaillé, Reference Grundmann and Cavaillé2000; Hanafiah, Reference Hanafiah2018). The process of translating scientific jargon and complex concepts requires a careful blend of expertise in both science and communication, ensuring that the essence of the research is preserved while the language used is clear and relatable. Recent research by Fick, Rudolph, and Hendriks (Reference Fick, Rudolph and Hendriks2025) highlights the complexity of this task: while avoiding jargon can enhance comprehension and foster trust by increasing perceptions of the communicator’s integrity and benevolence, it may also unintentionally lead to audience overconfidence, underscoring the double-edged nature of simplification in science communication.
Consider the example of communicating a new research finding about a medical treatment. A well-crafted message that takes into account important characteristics of scientific information might read like the following:
New research conducted by leading experts in the field highlights the potential benefits of treatment X in managing condition Y. The study, involving a large and well-designed sample, indicates that treatment X may improve [specific outcomes]. However, it is important to note that further research is needed to validate these findings and understand the long-term effects. We encourage you to consult with healthcare professionals, who can provide personalised guidance based on your unique circumstances.
This message begins by establishing the credibility of the research, noting the expertise involved and the robustness of the study design. The potential benefits of the treatment are outlined in layperson’s terms, making the information accessible without oversimplifying it. The message also responsibly acknowledges the need for further research and encourages consultation with healthcare professionals, providing a balanced and nuanced view of the findings.
In contrast, an oversimplified message might read as follows:
New study proves treatment X works! Get it now!
At first glance, these counterexamples might seem banal; however, this apparent simplicity reflects their real-world nature. Such oversimplified messages are commonly encountered and fail to convey the nuances of the research. They imply a certainty that may not be warranted and omit crucial information about the study’s context and limitations.
Similarly, in the examples in the next section, the counter-messages might appear simplistic or obvious, but this underscores the very issue being addressed.
2.3.2 Uncertainty and Conflicting Evidence
As seen in Section 1, health institutions often face the challenge of communicating scientific findings marked by uncertainty and sometimes conflicting evidence. Science inherently embraces uncertainty as part of discovery: knowledge is dynamic, refined through observation, experimentation, and analysis (Loon and Bal, Reference van Loon and Bal2014). In Popper’s terms, science involves systematic inquiry into the unknown, with discoveries that reshape existing understandings (Popper, Reference Popper2005). Communicating this helps the public see uncertainty not as a flaw but as an integral feature of science.
Yet humans tend to be intolerant of uncertainty, which can generate anxiety and confusion (Gu et al., Reference Gu, Gu, Lei and Li2020). Institutions must therefore acknowledge uncertainty openly and honestly (Cummings, Reference Cummings2015; Sopory et al., Reference Sopory, Day, Novak, Eckert and Wilkins2019). For example:
The latest research suggests a potential link between lifestyle factor X and health condition Y. Although these findings are significant, science is ongoing and uncertainties remain. Additional studies are needed. We understand uncertainty can be unsettling, and we are committed to keeping you informed as new information emerges.
This reassures by acknowledging both uncertainty and its emotional impact. In contrast:
Lifestyle factor X causes health condition Y! Take action now!
Such oversimplification hides uncertainty and risks misleading audiences.
Health institutions also face challenges when communicating conflicting evidence. For lay audiences, scientific disagreement may be misinterpreted as a lack of knowledge. Media talk shows often exacerbate this by presenting opposing voices for entertainment, amplifying fringe views, and creating false equivalency. This fosters polarization (Williams et al., Reference Williams, Hooker, Gilbert, Hor and Degeling2023) and public skepticism (Hiam, Dorling, and McKee, Reference Hiam, Dorling and McKee2023).
Institutions must explain that conflicting evidence is part of science’s self-correcting process. For example:
Studies on treatment A for condition B have shown mixed results. Some suggest benefits, others limited effects. We know this may be confusing. Please consult healthcare professionals who can consider your circumstances and the latest evidence.
Or:
Recent studies challenge earlier views on diet and health. Although results may seem contradictory, science evolves through new findings. We are committed to sharing the latest evidence, even when it conflicts with established knowledge, to support your well-being.
These examples both acknowledge conflict and reassure through transparency. By contrast:
Treatment A is the best choice for managing condition B!
This oversimplifies and may prompt poor decisions. Similarly:
New study challenges everything we knew about diet and health! Ignore previous recommendations!
This sensationalizes conflict, creates confusion, and erodes trust.
Such situations are easily exploited by conspiracy theorists and disinformation actors, who use scientific disagreement to sow doubt, spread falsehoods, and undermine trust in credible institutions (Lewandowsky et al., Reference Lewandowsky, Ecker, Seifert, Schwarz and Cook2012, Reference Lewandowsky, Cook, Ecker, Albarracín and Kendeou2020).
2.3.3 Rapidly Evolving Nature
The quick pace of scientific advancements complicates the communication of accurate and simplified information. This is particularly true in the health-related fields, where new studies, technological advances, and shifting scientific consensus can frequently update and revise people’s understanding of health issues. Health institutions must constantly monitor the latest scientific findings, re-evaluate their communication strategies, and adjust their messages to reflect the most current information. For example, consider the evolving guidelines during the COVID-19 pandemic, where initial recommendations regarding mask usage and social distancing were updated as new information emerged about virus transmission. Sources of confusion have been reported in the literature (Yong, Reference Yong2020; Overton et al., Reference Overton, Ramkeesoon, Kirkpatrick, Byron and Pak2021). Another example is the field of nutrition, as explained by Feinman (Feinman, Reference Feinman2019), who covers how evolving research has led to changes in dietary guidelines over time, reflecting new understandings of how certain foods affect health.
To avoid confusion, health institutions could form specialized teams, each dedicated to scouring the latest scientific publications and findings. These teams could ensure the institution remains at the forefront of research, integrating cutting-edge insights into their communication. Simultaneously, the institution itself should strengthen its bonds with the scientific community, fostering collaborations with researchers and institutions and gaining early access to emerging studies and trends in health science. This symbiotic relationship would provide a beneficial two-way street of information and resources.
The effort to do this is not minimal because, to recognize the dynamic nature of information, the institutions must adopt agile communication strategies. Health institutions can craft flexible plans and be ready to adapt to new findings at a moment’s notice. Websites, informational materials, and public advisories should be continuously updated, ensuring the public receives the most current information. This means a planned and implemented investment in communication to strengthen and benefit public health literacy (Caeiros et al., Reference Caeiros, Ferreira, Chen-Xu, Francisco and Telo de Arriaga2024). Parallel to these efforts, institutions could embark on a mission to enhance public education and invest in initiatives aimed at improving scientific literacy among the general population (Rubinelli et al., Reference Rubinelli, Fiordelli, Zanini and Fiordelli2022). This approach not only arms the public with the knowledge to understand complex health information, but it also prepares them to adapt to changes in health guidelines.
2.4 The Role of Scientists
A special focus within this context is on the following question: How can scientists augment the efforts of health institutions in disseminating robust and high-quality information? This query beckons an exploration into the complex dynamics between the scientific community and public communication channels.
As in the past (Bik and Goldstein, Reference Bik and Goldstein2013), a reluctance among many scientists to use social media for scientific discourse persists due to several concerns. First, there is the challenge of condensing complex scientific principles into concise posts without oversimplifying them, which can lead to misunderstandings. Social media’s informal nature also poses a risk of misinterpreting scientific information because these platforms are not typically designed for detailed, nuanced discussions. Scientists might worry that the subtleties and complexities of scientific research might be lost in this format, leading to an erosion of the depth and accuracy that science requires. In essence, the challenge lies in maintaining scientific integrity in an environment geared toward brevity and simplicity. Another aspect of scientists’ hesitation toward using social media for scientific dissemination is the nature and time constraints associated with their work. Many scientists do not see themselves as online influencers and might lack the inclination or skills to engage audiences in these platforms (Ho, Looi, and Goh, Reference Ho, Looi and Goh2020; Rose, Markowitz, and Brossard, Reference Rose, Markowitz and Brossard2020).
There is, however, a social “responsibility” for scientists to engage in public communication (Loroño-Leturiondo and Davies, Reference Loroño-Leturiondo and Davies2018). Society now engages in science within the public arena, necessitating a shift in the scientific community’s approach. Scientists must ponder their role in this dialogue, understanding that their responsibilities extend beyond the laboratory to the broader societal context. This shift requires scientists to not only be rigorous researchers but also effective communicators, bridging the gap between complex scientific knowledge and the societal discourse. Recent evidence suggests that how scientists present themselves on social media significantly affects public perceptions: scientists are generally seen as more authentic and qualified than influencers, especially when they engage in professional rather than personal self-disclosure (Zhang and Lu, Reference Zhang and Lu2023). Such findings underscore the importance of strategic communication in building trust, encouraging engagement, and fostering informed parasocial relationships. This transformation is crucial in meeting the needs of a society that actively discusses and scrutinizes scientific developments and that needs to be guided on how to do this effectively.
Clearly, the complexity of their message must be carefully woven, ensuring it remains clear while retaining the integrity of scientific truth. This is why empowerment in communication is increasingly a key skill for scientists (Bettencourt-Dias, Reference Bettencourt-Dias and Claessens2007; Schiebel et al., Reference 89Schiebel, Stone, Rossi and Smisek2021). There are also guides to assist scientists in the use of social media (Bowater and Yeoman, Reference Bowater and Yeoman2012; Heemstra, Reference Heemstra2020), and scientists are called to develop standards for their online presence (Pagoto and Nebeker, Reference Pagoto and Nebeker2019).
Scientists might consider alternative avenues to social media. Engaging in public dialogues, crafting articles tailored for a lay audience, or participating in interviews offer platforms where scientific rigor need not be compromised for the sake of accessibility. For instance, a virologist penning a thought-provoking piece in a widely-read magazine and elucidating the nuances of a novel virus strain or an epidemiologist leading an interactive webinar to demystify the latest developments in vaccine research can give a main contribution to lay audiences’ knowledge. Indeed, these efforts not only disseminate knowledge but also foster a culture of informed discussion. In concert with health institutions, scientists can forge a symbiotic relationship. Such a collaborative approach, eschewing the brevity of social media for more substantial forms of engagement, promises to enhance the efficacy of public health communication.
2.5 People’s Barriers toward the Content of Scientific Information
In scientific communication, a major barrier arises when evidence conflicts with personal behaviors. Institutions often communicate results that highlight the harmful nature of enjoyable or ingrained activities such as smoking, sugary diets, or sedentary lifestyles. This creates a tension between acknowledging evidence and continuing behaviors that provide gratification or cultural belonging. The literature on this challenge is extensive, spanning psychology, sociology, public health, and behavioral economics (Laverack, Reference Laverack2017; Sheeran, Klein, and Rothman, Reference Sheeran, Klein and Rothman2017; Rubinelli and Diviani, Reference Rubinelli and Diviani2020). As key texts illustrate (Rollnick, Mason, and Butler, Reference Rollnick, Mason and Butler2010; Glanz, Rimer, and Viswanath, Reference Glanz, Rimer and Viswanath2015), behaviors that are culturally rooted and pleasurable are particularly resistant to change, as they involve motivation, self-discipline, social influence, and emotion.
When scientific communication is unclear or uncertain, individuals often seek more definitive answers outside institutional channels, where pseudoscience can appear appealing despite lacking evidence (Shermer, Reference Shermer2002). This is compounded by cognitive biases that distort how people process institutional messages (Rubinelli, Diviani, and Fiordelli, Reference Rubinelli, Diviani and Fiordelli2020b). As shown in seminal work (Gilovich, Griffin, and Kahneman, Reference Gilovich, Griffin and Kahneman2002; Kahneman, Reference Kahneman2011), biases act as filters that shape interpretation based on beliefs or perceptions rather than evidence. Confirmation bias leads individuals to favor information supporting preexisting views (Meppelink et al., Reference Meppelink, Smit, Fransen and Diviani2019), while the Dunning–Kruger effect leads those with limited knowledge to overestimate their understanding (Canady and Larzo, Reference Canady and Larzo2023). The availability heuristic prioritizes vivid or recent reports over robust studies (Botzen et al., Reference Botzen, Duijndam, Robinson and van Beukering2022). Anchoring bias gives undue weight to initial, often optimistic, claims about new treatments (Ludolph and Schulz, Reference Ludolph and Schulz2018). The bandwagon effect aligns people with perceived group norms, even when these contradict health advisories – for example, when groups collectively dismiss mask use as harmful (Lechanoine and Gangi, Reference Lechanoine and Gangi2020). Indeed, Lechanoine and Gangi (Reference Lechanoine and Gangi2020) describe a “pandemic of biases” shaping COVID-19 decision-making.
These challenges are intensified when health communication is politicized. Political instrumentalization of science exacerbates biases, dividing audiences along ideological lines (Gligorić et al., Reference Gligorić, van Kleef and Rutjens2025). Health guidelines may thus be accepted or rejected not on evidence but on political loyalty. In such cases, scientific facts risk being overshadowed by political beliefs, undermining institutional credibility and public trust – a theme addressed in the next section.
2.6 Pseudoscience
An examination of cognitive biases and the politicization of health information reveals that these factors can significantly distort the public’s perception and acceptance of scientific data. This intricate interplay of personal beliefs, social conformity, and political leanings sets the stage for the emergence and appeal of pseudoscience.
As Scott Lilienfeld and colleagues (Lilienfeld, Lynn, and Ammirati, Reference Lilienfeld, Lynn, Ammirati, Cautin and Lilienfeld2015) and Brian Hughes (Hughes, Reference Hughes2017), among others, show, pseudoscience often masquerades as legitimate science, captivating audiences through a blend of superficial plausibility and appealing narratives. Pseudoscience thrives by exploiting cognitive biases and filling gaps in scientific understanding with seemingly straightforward answers. Pseudoscience often lacks adherence to the scientific method, which is evident in practices like astrology, which claims to predict personality or life events based on celestial bodies without empirical testing. It frequently relies on anecdotal evidence, similar to some alternative medicine practices that promote cures based on individual success stories rather than controlled studies, and typically eschews peer review and reproducibility, as seen in the promotion of certain diets or health products that have not been rigorously tested or replicated in scientific studies. Indeed, it often involves sensationalism and emotional appeal, akin to the exaggerated claims about the efficacy of certain supplements, which are marketed with compelling personal testimonies rather than scientific evidence (Rubinelli et al., Reference Rubinelli, Fiordelli, Zanini and Fiordelli2022).
There are a lot of important publications about the problems and risks of pseudoscience, but here, it is important to notice that the promoters of pseudoscience are often masterful communicators who are adept at crafting messages that are both engaging and convincing. They excel in simplifying complex ideas into digestible, relatable content, making it more accessible than the often complex and technical language used in scientific discourse. For instance, a pseudoscientific diet plan might be presented with compelling before-and-after photos and easy-to-understand guidelines as opposed to a scientifically backed diet that comes with detailed research studies and statistical data, which can be overwhelming for the average person. The book by Massimo Pigliucci (Pigliucci, Reference Pigliucci2010) well illustrates some dynamics of the presentation of pseudoscience, as does Melinda Moyer (Moyer, Reference Moyer2019), who illustrates why people believe in this type of health information considering how it is communicated.
Additionally, these communicators often utilize emotional storytelling and personal anecdotes, which can be more persuasive to the general public than empirical evidence. An example of this is the use of personal testimonials in promoting alternative medicine, where individual success stories are highlighted over clinical trial results. This emotional and narrative-driven approach resonates deeply with human psychology because people are naturally drawn to stories and personal experiences rather than abstract data or complex scientific principles. By leveraging these communication techniques, promoters of pseudoscience create a persuasive appeal that can overshadow the lack of scientific validity in their claims, making their messages compelling to a wide audience.
2.7 Investment of Health Institutions in Strengthening People’s (Digital) Health and Scientific Literacy
Following from the analysis made above, in today’s intricate communication landscape, health institutions are confronted with the urgent need to enhance public health, scientific, and digital literacy. This task is not merely an educational challenge but a foundational investment in fostering a society capable of navigating the pervasive threats of misleading health information, pseudoscience, and politicized health narratives. While health information may often appear accessible due to simplified communication formats, it remains inherently technical, requiring different layers of expertise to be correctly interpreted and applied. The issue of health literacy is therefore far from marginal – and not because people lack intelligence, but because understanding health information is comparable to learning a complex skill, like playing a musical instrument or interpreting a foreign language. It demands sustained education, guided practice, and contextual understanding. In a world where health information is increasingly democratized and widely disseminated, this presents a significant challenge: ensuring that accessibility does not come at the cost of comprehension or accuracy. The ability to discern credible information, interpret complex data, and make informed decisions is paramount for empowering individuals to actively engage in their own health management and in broader public health initiatives (Rubinelli et al., Reference Rubinelli, Ort, Zanini, Fiordelli and Diviani2021; Fiordelli et al., Reference Fiordelli, Diviani, Farina, Pellicini, Ghirimoldi and Rubinelli2023). Achieving this goal requires a multifaceted and programmatic approach.
Health institutions must champion initiatives that go beyond imparting knowledge to cultivating critical thinking skills and resilience against biases. Community-based educational programs can play a vital role, offering workshops and resources to help individuals scrutinize health information, understand scientific methodology, and recognize the hallmarks of evidence-based practices (Rubinelli et al., Reference Rubinelli, Fiordelli, Zanini and Fiordelli2022). Digital health literacy, in particular, must be prioritized. As the internet and social media have become primary sources of health information, the public must be equipped with the skills to evaluate the credibility of online content, identify manipulative tactics, and navigate the digital environment responsibly. Schools are indispensable in this effort, serving as incubators for the next generation of critical thinkers. However, integrating health, scientific, and digital literacy into existing curricula demands substantial reform. This integration requires collaboration between health institutions, educational authorities, and curriculum developers to design interdisciplinary programs that seamlessly weave these competencies into the academic fabric. Such programs must be both context-sensitive and inclusive, recognizing the diverse needs and cultural backgrounds of learners.
Despite the promise of these initiatives, significant challenges remain. Resource constraints often limit the scope and reach of literacy programs, with urgent health crises frequently overshadowing the long-term value of education. Furthermore, some sensationalist tendencies of mass media and the politicization of health information can undermine these efforts, eroding trust in institutional messages and complicating public engagement. Partnerships with media outlets, NGOs, and community leaders can amplify accurate messaging while addressing systemic barriers to health literacy. As highlighted by the World Health Organization’s competency framework for managing poor-quality information (World Health Organization, 2021; Rubinelli, Purnat et al., Reference Rubinelli, Purnat and Wilhelm2022), health institutions must adopt a proactive stance.
As shown in the next section, health institutions do not operate in isolation; their messages, policies, and public engagement are often influenced – sometimes constrained – by political agendas and governance structures (see Table 2).
Key takeaways
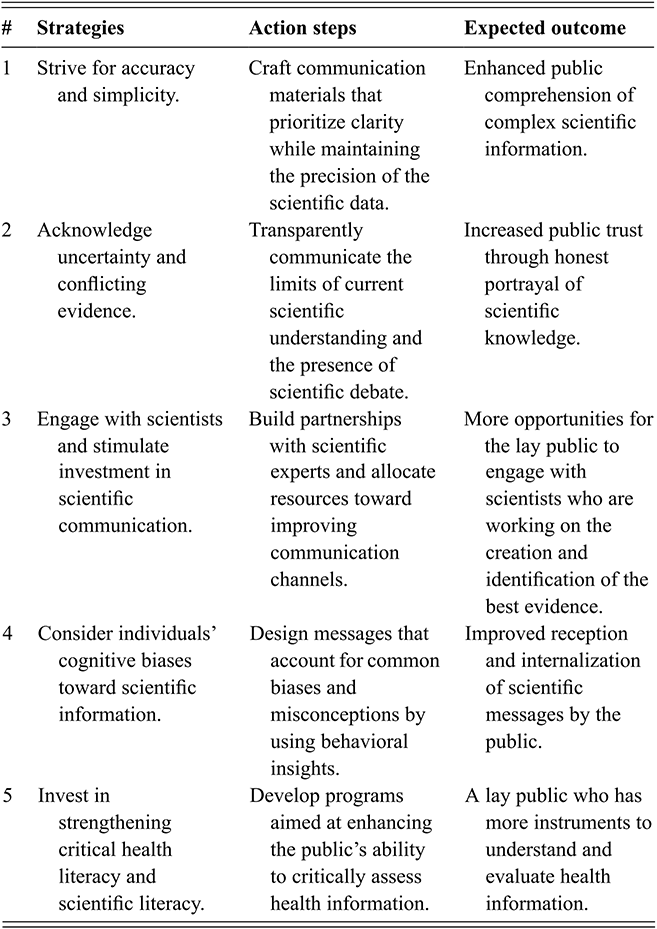
Table 2 Long description
The table outlines five strategies to bridge science and public understanding, each linked to action steps and expected outcomes. The first strategy focuses on balancing accuracy and simplicity to improve comprehension of complex scientific information. The second emphasizes transparent communication of uncertainty and conflicting evidence to build trust. The third promotes engagement with scientists and investment in communication to increase public access to expertise. The fourth considers cognitive biases, encouraging the use of behavioural insights to improve message reception. The fifth highlights the importance of strengthening critical health and scientific literacy, enabling individuals to better evaluate information and make informed judgments.
3 The Dialogue between Politicians and Health Institutions
3.1 Overview
The power of politics can either be a force for positive change or a hindrance to public health progress. It is the responsibility of everyone to ensure it serves the greater good.
This section examines the complex dynamics between politicians and health institutions, highlighting their interdependence and the challenges of aligning political priorities with public health goals.
3.2 The Relationship between Public Health and Politics
Understanding the complex relationship between health institutions and politics is of the utmost importance in today’s world. The practice of public health within these institutions is intricately linked to the dynamics of politics, making it essential to comprehend and navigate this relationship effectively. On the one hand, the main role of health institutions is to promote and safeguard the health, functioning, and well-being of populations. Politics, on the other hand, involves the processes and activities associated with governance, decision-making, and policy formulation. Political systems shape the social, economic, and environmental contexts in which health institutions operate. Political actors, such as government officials and policymakers, have the authority to make decisions that impact healthcare policies, resource allocation, and regulatory frameworks (see, for instance, Levitt, Reference Levitt2020).
Health institutions and politics are deeply interconnected, influencing each other in critical ways (Baggott, Reference Baggott2010; Turnock, Reference Turnock2012). Political decisions shape the operations of health institutions, while health outcomes should inform political priorities. Both share a commitment to public well-being: health institutions focus on delivering care and addressing public health issues, while politics governs work across multiple sectors, including healthcare.
Key differences lie in their mandates and decision-making processes. Health institutions operate within evidence-based frameworks, relying on scientific research and expertise, whereas political decisions can be shaped by ideology, public opinion, economic factors, and electoral dynamics (Greer et al., Reference Greer, Bekker and de Leeuw2017; Field, Reference Field2024). Accountability also differs: health institutions answer to regulatory bodies and the public for service quality, while politicians are accountable through elections and democratic mechanisms (Borrell et al., Reference Borrell, Espelt, Rodríguez-Sanz and Navarro2007). Moreover, health institutions often address immediate needs, whereas political processes prioritize long-term societal goals and are influenced by election cycles.
3.3 The Prevention Power of Politics
A pivotal aspect of the interaction between politics and public health is that political strategies and policies can prevent specific outcomes or issues in society. Politics has a main power in preventing negative (health) outcomes in the sense that public health issues, whether they be disease outbreaks, environmental hazards, or social determinants of health, are inextricably linked to political factors. Thus, the prevention or solutions to these challenges often require political strategies, policies, and actions (Navarro et al., Reference Navarro, Muntaner and Borrell2006; Borrell et al., Reference Borrell, Espelt, Rodríguez-Sanz and Navarro2007; Toth, Reference Toth2013).
At its core, this type of prevention works by harnessing the influence of political systems to create conditions that promote health, prevent diseases, and enhance overall well-being. Indeed, as shown, for instance, in the framework of the World Health Organization’s Classification of Health, Functioning, and Disability, health and functioning cannot be effectively addressed through biomedical or individual-focused interventions alone (WHO, 2001; Üstün et al., Reference Üstün, Chatterji, Bickenbach, Kostanjsek and Schneider2003). In the literature on health inequalities, Graham and Kelly (Graham and Kelly, Reference Graham and Kelly2004) show how the roots of many public health disparities lie within the broader social, economic, and environmental contexts in which people live. This emphasizes the need for comprehensive, systemic, and population-level interventions that target the underlying causes of health inequities and strive for health equity (World Health, 2008).
As a driving force behind decision-making, politics plays a pivotal role in shaping these social determinants of health. Political choices influence the allocation of resources, the design of policies, and the distribution of power, factors that significantly impact population health outcomes. The ecological models of health behavior (Glanz, Rimer, and Viswanath, Reference Glanz, Rimer and Viswanath2015) show how policies related to education, housing, transportation, and employment can directly affect health behaviors, access to healthcare, and overall well-being. Moreover, political actors possess the authority to implement regulatory frameworks and public health interventions that promote preventive measures; they can enact legislation, allocate funding, and coordinate multisectoral collaborations to tackle health challenges on a population-wide scale. Political leaders also bear the responsibility of setting agendas, raising awareness, and engaging in public discourse to prioritize and advocate for preventive approaches to public health (Health and Organization, 2008; Kickbusch and Gleicher, Reference Kickbusch and Gleicher2012; Frenk and Moon, Reference Frenk and Moon2013; Greer et al., Reference Greer, Bekker and de Leeuw2017).
Crucially, public health crises, such as the COVID-19 pandemic, can serve as pivotal moments for political leaders to prioritize preventive measures and enact substantive change. These crises heighten public awareness and demand for action, creating an environment that fosters political will for preventive interventions. Furthermore, political prevention fosters multisectoral collaborations and partnerships; it encourages engagement with a diverse array of stakeholders, including government agencies, nonprofit organizations, private sector entities, and community groups. This collaborative approach allows for the pooling of resources, expertise, and influence, enabling a comprehensive addressing of public health challenges. However, as will be illustrated below, implementing political prevention can be a formidable challenge because there are certain key factors that can create tensions between politicians and health institutions.
3.4 Instances of Disagreement
The COVID-19 pandemic has highlighted the tension between political decision-making and scientific guidance from health institutions. During this global health crisis, a divergence emerged: Although health experts grounded their recommendations in scientific research, advocating for measures like widespread testing, social distancing, and mask mandates, political leaders often are moved by other factors, including public sentiment and political, pragmatic considerations, and economic parameters (Cairney and Wellstead, Reference Cairney and Wellstead2021). These discrepancies arose from a complex interplay of factors, reflecting a primary challenge in balancing public health priorities and political considerations.
First, political considerations and priorities play a role as leaders face the challenge of balancing public health concerns with other competing interests such as economic stability and public sentiment (Greer et al., Reference Greer, Bekker and de Leeuw2017; Kavanagh and Singh, Reference Kavanagh and Singh2020). There have been scenarios in which a country experienced a resurgence of COVID-19, and public health officials, relying on scientific data and models, recommended maintaining strict lockdown measures to control the spread of the disease. However, the political leaders of the country were facing pressure from various groups, including business owners, workers who were losing income, and segments of the public who were frustrated with the restrictions. In this situation, the political leaders decided to prioritize economic concerns and public sentiment over strict public health guidelines. They argued that the economic damage caused by prolonged lockdowns was too severe and that the mental and financial well-being of the citizens was equally important as their physical health. As a result, they could opt to reopen businesses, relax social distancing rules, and ease other restrictions more quickly than what the public health officials recommended (Bambra et al., Reference Bambra, Riordan, Ford and Matthews2020; Crabu et al., Reference Crabu, Giardullo, Sciandra and Neresini2021; Flores et al., Reference Flores, Cole and Dickert2022; Koch and Durodié, Reference Koch and Durodié2022). This decision leads to a conflict between the political leaders and public health officials. The health experts warned that easing restrictions prematurely could lead to a spike in infections, overwhelming the healthcare system and potentially causing more deaths. Meanwhile, political leaders argued that their approach was balanced and necessary to prevent economic collapse and societal unrest.
Differing risk perceptions and tolerance levels between political leaders and health institutions can also lead to discord. Again, during the COVID-19 pandemic, some political leaders often publicly downplayed the severity of the virus, comparing it to less serious illnesses and suggesting it would soon pass without having a major impact. This attitude aligned with a broader strategy to avoid economic downturn and public panic. As a result, the leaders and some regional administrators advocated for relatively relaxed restrictions, pushing for the early reopening of businesses and schools and showing reluctance toward enforcing mask mandates and social distancing (van Holm et al., Reference van Holm, Monaghan, Shahar, Messina and Surprenant2020; Tung, Chang, and Lin, Reference Tung, Chang and Lin2022). Political ideologies also impact the spread of conspiracy theories and vice versa (Havey, Reference Havey2020; Sutton and Douglas, Reference Sutton and Douglas2020; Zoran et al., Reference Zoran, Pavlović, Todosijević and Stanojević2021). Contrastingly, the national health institutions and public health took a more cautious approach: They emphasized the seriousness of the pandemic based on evolving scientific data. Their recommendations included prolonged lockdowns, social distancing measures, widespread mask usage, and, later, a strong push for vaccination.
The discord between these two approaches became evident in several ways. When the health institutions released detailed guidelines for safely reopening the economy, there were reports of these being sidelined or modified by political leaders for being too stringent. Additionally, at times, the political leadership publicly contradicted the advice of health experts, including promoting unverified treatments and downplaying the necessity of scientifically backed preventive measures (de Swielande, Reference Struye de Swielande2020; Rutledge, Reference Rutledge2020; Andrews, Reference Andrews, Smith, Clarke, Tilley and Williams2021; Blitt, Reference Blitt2021; Brenner, Reference Brenner2021; Marzi and Sessa, Reference Marzi and Sessa2021). Clearly, public opinion and electoral considerations further contribute to disagreements. Political leaders are accountable to public sentiment, and during election cycles, their decision-making may be influenced by the preferences of their constituents (see, for instance, Zanotti and Meléndez, Reference Zanotti, Meléndez, Albertazzi and McDonnell2022).
3.5 A Chaotic Information Environment
A chaotic health information landscape complicates the relationship between health institutions and political entities. While institutions aim to disseminate accurate, science-based information, the space is often crowded with unverified or deliberately misleading messages (Brenner, Reference Brenner2021). Political leaders may exploit this by downplaying crises for economic stability, spreading unverified optimism for political gain, or amplifying false claims to undermine rivals. Such practices fragment public response, align health beliefs with political identities, and hinder cohesive public health strategies.
Politicians also face the dilemma of which experts to endorse. Conflicting scientific views – for example, between strict lockdowns and lenient approaches – become entangled with political agendas, economic concerns, and stakeholder interests. Business owners prioritize recovery, healthcare professionals patient safety, educators continuity of learning, scientists rigorous standards, and community leaders social cohesion.
Four additional sources of mismatch are notable. First, jurisdictional differences between national, regional, and local authorities create inconsistent policies. For example, a central government may call for nationwide lockdowns, while regional leaders advocate tailored measures, producing confusion and noncompliance. Second, cultural factors shape both public and political responses. In societies valuing individual freedom, lockdowns and mandates face resistance, while collectivist cultures show higher compliance (Laverack, Reference Laverack2017). Trust in institutions also varies: some cultures accept scientific authority, while others are more receptive to unsupported claims due to skepticism of government or medicine. Leaders often tailor messages to these expectations, which can lead to misleading communication. Third, scientific uncertainty and evolving knowledge (as noted in Section 2) create tension between health institutions updating recommendations and political leaders preferring stable messaging. Fourth, disagreements at the international level exacerbate fragmentation. Competing interests around vaccine distribution, travel restrictions, and pandemic strategies reflect geopolitical considerations, producing patchwork responses that weaken global coordination and the credibility of health institutions.
These dynamics show how political agendas, cultural expectations, and geopolitical rivalries entangle with science, undermining the unified, evidence-based communication needed for effective health policy.
3.6 Politics, Fallacies, and Suboptimal Health Information
While politics can mobilize resources and shape health systems, it can also generate problematic communication practices. This section examines fallacious reasoning and questionable persuasion in political discourse. Political rhetoric is often not outright false but lacks empirical grounding, as seen during COVID-19 when leaders promoted narratives misaligned with science. Politics thus became a breeding ground for suboptimal information with consequences for public perception and policy.
One motivation is political expediency: leaders seeking popularity or power may use unsupported claims or fallacies to sway opinion or deflect responsibility (Barsamian and Chomsky, Reference Barsamian and Chomsky2001; Davis, Reference Davis2010). Ideological bias also drives the promotion of claims that fit political convictions rather than evidence (Bennett and Livingston, Reference Bennett and Livingston2020; Lopez-Garcia et al., Reference Lopez-Garcia, Campos-Domínguez, Palau-Sampio and Palomo Torres2021). A further factor is image management: statements crafted to project competence or maintain confidence, even if inaccurate, add to the spread of poor-quality information (Lees-Marshment, Reference Lees-Marshment2024).
Argumentation theory highlights how fallacies become tools of political rhetoric (Jason, Reference Jason1989; Zurloni and Anolli, Reference Zurloni, Anolli and Poggi2013; Zhou, Reference Zhou2018; Hamblin, Reference Hamblin2022). Cummings (Reference Cummings2020) showed how analyzing good versus bad arguments helps explain responses to health communication, and later argued that even fallacies may sometimes support reasoning under uncertainty (Cummings, Reference Cummings2024). Yet, fallacies can be more persuasive than evidence-based arguments, especially when promoted by trusted leaders, thereby influencing public decision-making (Rubinelli et al., Reference Rubinelli, Ort, Zanini, Fiordelli and Diviani2021).
Examples from the COVID-19 pandemic illustrate their impact. The false analogy compared COVID-19 to the flu, minimizing its severity despite differences in transmission, mortality, and treatment (Bump, Reference Bump2020). The appeal to emotion was widespread, as leaders invoked fear, anger, or sympathy to resist lockdowns or frame narratives of enemies and victims (Manfredi-Sánchez, Amado-Suárez, and Waisbord, Reference Manfredi-Sánchez, Amado-Suárez and Waisbord2021; Widmann, Reference Widmann2022; Campolongo, Scanni, and Tarditi, Reference Campolongo, Scanni and Tarditi2025). The cherry-picking of data presented selective statistics, downplaying severity or emphasizing economic costs (Hansson, Reference Hansson2017; Wigley, Reference Wigley2023; Marinho and Billig, Reference Marinho and Billig2024). The false-cause fallacy linked COVID-19 to 5 G or conspiracy plots, exploiting public fears (Gerli, Reference Gerli2021). The appeal to authority appeared when political figures relied on their own status or non-expert endorsements, such as promoting untested drugs like hydroxychloroquine (Madanay, McDevitt, and Ubel, Reference Madanay, McDevitt and Ubel2022), or endorsing conspiracy theories about engineered viruses and global plots (Marzi and Sessa, Reference Marzi and Sessa2021; León, López-Goñi, and Salaverría, Reference León, López-Goñi and Salaverría2022).
As these cases show, fallacious reasoning, while persuasive, distorts scientific reality, undermines institutional credibility, and risks harmful public health behaviors.
3.7 Political Language That Divides
Following the analysis of various types of suboptimal information propagated by political leaders in previous sections, this section explores how the divisive rhetoric used by political figures can also exacerbate public health challenges.
Political rhetoric is beautifully illustrated in the book Divisive Discourse by Joseph Zompetti (Zompetti, Reference Zompetti2015). To summarize some prominent aspects, divisive political rhetoric, which is characterized by language and messaging that intentionally fosters division and polarization, can have significant repercussions, especially in the context of public health messaging. It is often employed when discussing sensitive topics or issues that have the potential to create strong emotions or polarized opinions within society. It is designed to appeal to a specific audience or reinforce preexisting beliefs and attitudes. This type of rhetoric may involve framing complex issues in a simplistic, black-and-white manner, using derogatory language to describe certain groups or individuals, or employing fear-based messaging to create divisions.
To give a couple of examples of how divisive rhetoric can work, imagine the two scenarios below. During a contentious debate on vaccine policies, a prominent political figure took the stage. With a flair for dramatics, they sharply divided the issue into black-and-white terms. “Vaccines,” they proclaimed, “are either our saviours or our worst nightmare.” This is an oversimplification, ignoring the layers of scientific research and nuanced understanding, polarizing the audience into extreme positions. In another instance, amid a rising wave of a new infectious disease, a leader can use their platform not just to inform but to incite fear. They can spin tales, subtly pointing fingers at specific ethnic groups, painting them as the carriers of this plague. This fear-mongering not only creates a chasm of distrust and bias in society but also detracts from the genuine public health efforts needed to combat the disease. Thus, divisive language during the pandemic has disproportionately affected marginalized communities. When political figures use terms that target specific regions or groups about COVID-19, it can fuel xenophobia and discrimination (e.g., “The China virus”). This stigmatization not only reinforces harmful stereotypes but also impedes efforts to address the unique health needs of these communities. This, in turn, can result in disparities in testing, access to healthcare, and access to support systems (Roberto, Johnson, and Rauhaus, Reference Roberto, Johnson and Rauhaus2020; Bhanot et al., Reference Bhanot, Singh, Verma and Sharad2021; Koller et al., Reference Koller, Villinger and Lages2021).
The consequences of divisive political rhetoric extend, of course, beyond the COVID-19 pandemic, impacting debates on various public health issues. In discussions related to mental health, substance abuse, and other critical topics, divisive language can perpetuate stigma and hinder the development of effective prevention and treatment strategies. Here, the review of Sickel et al. (Sickel, Seacat, and Nabors, Reference Sickel, Seacat and Nabors2014) on mental health is valuable. For instance, in the realm of mental health, the use of divisive language by political figures can stigmatize individuals struggling with psychological well-being. Referring to mental health challenges as a mere “weakness” or suggesting that individuals can “snap out of it” implies a lack of understanding of the complexity of mental health issues. Such rhetoric can create a culture of shame and discourage those in need from seeking help, leading to untreated mental health conditions and potential crises. In the context of substance abuse, divisive language can hinder efforts to combat addiction effectively. Labeling individuals with substance use disorders as “junkies” or “criminals” perpetuates harmful stereotypes and further marginalizes those who are affected. Such language can also contribute to the criminalization of addiction rather than a public health approach, limiting access to treatment and support services and exacerbating the substance abuse epidemic.
The use of derogatory terms or framing complex health issues in a simplistic, divisive manner contributes to a culture of shame, discouraging individuals from seeking help. Political leaders who engage in such language may inadvertently hinder funding for essential programs and reinforce misconceptions, thereby worsening existing health crises (Bhanot et al., Reference Bhanot, Singh, Verma and Sharad2021; Schneider et al., Reference Schneider, Wilson, Dayton, Anderson Goodell and Latkin2021). Last but not least, when repeated and amplified, especially in times of crisis, such rhetoric can evolve into hate speech, severely undermining social cohesion. (UNESCO, 2023).
3.8 Some Moral and Ethical Questions
Navigating the ethical landscape surrounding the dissemination of suboptimal health information by politicians presents a complex set of challenges and considerations. Indeed, the issue of whether politicians disseminate suboptimal health information intentionally or unintentionally is a complex and challenging one. It is difficult to definitively determine politicians’ motivations, and this is outside the scope of the present work. However, what matters here is the problem linked to the dissemination of fallacious and unsupported health information and how to address it. There are clear questions that further research and analysis would need to explore, and that can be presented at the end of this section to prompt further thinking and research, as follows:
Responsibility and accountability: To what extent are political leaders responsible and accountable for the spread of poor-quality health information? How can they ethically navigate their duty to address falsehoods and suboptimal health information in an effective manner?
Transparency: How transparent are politicians about the sources of their information and their decision-making processes? How does transparency influence the public’s trust in their leadership?
Resisting manipulation: To what extent do political leaders resist the temptation to present misleading health information for personal or political gain? How can they demonstrate ethical integrity in information provision?
Building trust and fostering critical thinking: How do leaders navigate the challenge of overcoming resistance to evidence-based information, particularly when unsupported health claims align with existing beliefs or partisan narratives? What strategies can and should they employ to build trust and foster critical thinking within their communities?
The answers to these ethical questions can ultimately contribute to responsible and ethical political leadership in the realm of public health. Overall, political leaders have a profound influence on public perception, and their commitment to transparency, accountability, and ethical communication can either reinforce or erode trust in health institutions. This brings to the next critical dimension: trust. As the focus of the next section, trust serves as the foundation for effective health communication, shaping public confidence in health institutions, policies, and professionals (see Table 3).
Key takeaways
| # | Key strategies | Action steps | Expected outcome |
|---|---|---|---|
| 1 | Leverage political influence for public health. | Develop policies that prioritize health outcomes and invest in public health infrastructure. | Improved population health and preparedness for public health emergencies. |
| 2 | Align political and health objectives. | Ensure political decisions are informed by evidence-based health research. | Healthier societies with decisions that reflect public health best practices. |
| 3 | Foster cooperation between sectors. | Facilitate regular communication and collaborative platforms between sectors. | A unified response to health crises and a consistent message to the public. |
| 4 | Promote ethical health communication. | Promote transparency and accountability in health-related communications. | Increased public trust in health information and improve information quality. |
| 5 | Combat low-quality information effectively. | Collaborate across political and health institutions and invest in public education that strengthens media and health literacy. | A more informed public capable of discerning accurate health information. |
4 Trust in Health Institutions
4.1 Overview
In the healthcare landscape, trust is paramount, linking the expertise of professionals to the well-being of the community.
This section examines the critical role of trust in the relationship between health institutions and the public, highlighting its importance as a cornerstone of effective healthcare systems, public health campaigns, and community well-being.
4.2 Conceptualizing Trust
Trust is the foundation of any successful relationship, fostering cooperation, credibility, and confidence. In health, it is not abstract but a vital asset underpinning effective healthcare systems, public health initiatives, and individual well-being. Trust in institutions is based not on blind acceptance but on the belief that they possess the expertise and dedication to protect health, act as reliable sources of information, and provide life-saving interventions (Gilson, Reference Gilson2006; Rădoi and Lupu, Reference Rădoi, Lupu and Maturo2017).
In the digital age, this trust faces challenges. Health institutions encounter skepticism, misinformation, and dissatisfaction, particularly online. Resistance to vaccination programs (Raffini and Penalva-Verdú, Reference Raffini, Penalva-Verdú, Eslen–Ziya and Giorgi2022; Bory et al., Reference Bory, Giardullo, Tosoni and Turrini2023), debates on lockdowns and masks (Al-Ramahi, Elnoshokaty, and El-Gayar, Reference Al-Ramahi, Elnoshokaty and El-Gayar2021; Erdemandi and Leach, Reference Erdemandi and Leach2021), promotion of alternative therapies (Sobo, Reference Sobo2021), and concerns about pharmaceutical influence have all eroded confidence. Privacy breaches and politicization of health decisions further undermine institutional credibility (Hsu, Reference Hsu2020).
Trust is dynamic, shaped by interactions, experiences, and perceptions (Falcone et al., Reference Falcone, Colì and Felletti2020; Gilles et al., Reference Gilles, Le Pogam and Perriraz2022; Skirbekk, Magelssen, and Conradsen, Reference Skirbekk, Magelssen and Conradsen2023). It is context-dependent and fragile: breaches can rapidly erode it, but sincere efforts can rebuild confidence (Cummings, Reference Cummings2014a; Purnat, Nguyen, and Briand, Reference Purnat, Nguyen and Briand2023). Key dimensions include competence, integrity, benevolence, and reliability (Gilson, Reference Gilson2006). Importantly, trust is reciprocal – institutions must demonstrate trustworthiness, while individuals must be willing to extend trust.
The importance of trust spans multiple relationships. For patients, it underpins reliance on accurate diagnoses, effective treatments, and compassionate care. For the public, it ensures confidence in prevention campaigns, evidence-based guidelines, and crisis responses. In research collaborations, trust in the ethics and expertise of universities, pharmaceutical companies, and partners is essential. Philanthropic support depends on confidence that resources are used ethically. Collaboration with government agencies requires mutual trust to ensure effective campaigns, disaster preparedness, and policy development. Finally, partnerships with insurance providers demand trust in fair financial practices to guarantee patient access to care.
4.3 Eroding Trust
Trust between the general public and health institutions is a delicate thread woven from a complex tapestry of actions and perceptions. The credibility of health institutions is finely attuned to their ability to deliver on promises, demonstrate ethical practices, and act in the best interests of patients and the public. It is a dynamic balance, one where trust is neither given nor taken for granted but is instead nurtured through a commitment to honesty, competence, and empathy. In this intricate dance, health institutions hold the responsibility of preserving and reinforcing trust, recognizing that the fragility of this bond demands unwavering dedication to the well-being of those they serve.
As discussed in previous sections, however, the proliferation of poor-quality health information poses a significant threat to trust in health institutions. The dissemination of false or misleading information can engender confusion, sow doubt, and cultivate public skepticism regarding health recommendations. Furthermore, inconsistency in health messaging has the capacity to weaken trust (for a general overview, see Bhutto, Reference Bhutto2024). When health institutions provide contradictory or conflicting information, the public may become uncertain about what to believe, fostering a sense of distrust and uncertainty (Purnat, Nguyen, and Briand, Reference Purnat, Nguyen and Briand2023). In addition to these challenges, a lack of transparency in decision-making processes, data sharing, and communication can nurture suspicion and corrode trust in health institutions. When the public perceives a dearth of openness, questions regarding the motives behind certain health initiatives may arise (Rubinelli et al., Reference Rubinelli, Fiordelli, Zanini and Fiordelli2022). The way health institutions handle crises, such as disease outbreaks or public health emergencies, can have a profound impact on trust. A sluggish or inadequate response, mixed messaging, or perceived mismanagement can lead to public dissatisfaction and a reduction in trust.
Failing to involve the public in decision-making and ignoring community perspectives can cause alienation and reduce trust. Communities may feel disconnected and excluded from health initiatives that directly impact them. Additionally, when health institutions are seen as being influenced by political interests rather than evidence-based practices, trust can deteriorate. Public health decisions should focus on the well-being of the population rather than political gains to maintain and strengthen public trust.
4.4 Building Strong Connections between Health Institutions and Communities
Considering the above, transparency is a key element in building trust (Spalluto et al., Reference Spalluto, Planz and Stokes2020). Health institutions that communicate openly and honestly with the public, sharing both successes and challenges, are more likely to gain credibility. Providing clear and understandable information about health risks, interventions, and uncertainties creates an environment of trust where individuals feel empowered to make informed health decisions. Additionally, health organizations that demonstrate a high level of competence and expertise are more likely to earn the public’s trust (Eiser et al., Reference Eiser, Stafford, Henneberry and Catney2009). This involves showcasing a strong track record of successful health interventions, using evidence-based practices, and engaging with reputable experts in the field. Trust is also linked to consistency (Cantarutti and Pothos, Reference Cantarutti and Pothos2023). Indeed, health organizations that deliver consistent information and follow through on their commitments are perceived as reliable sources of health information and support.
In the age of interactivity, showing empathy and understanding of the community’s concerns and needs builds trust between health institutions and the public (Purnat, Nguyen, and Briand, Reference Purnat, Nguyen and Briand2023). This includes actively listening to community feedback, recognizing cultural and individual differences, and integrating community perspectives into health interventions. For example, a health organization that conducts community focus groups and surveys to better understand the specific health needs and cultural contexts of a diverse community demonstrates empathy and dedication to addressing their unique concerns.
Similarly, involving the public in the decision-making process creates a sense of ownership and investment in health initiatives and in community engagement, especially with vulnerable populations (Gilmore et al., Reference Gilmore, Ndejjo and Tchetchia2020; Wieland, Doubeni, and Sia, Reference Wieland, Doubeni and Sia2020). Collaborative approaches that engage communities in the design and implementation of health interventions are more likely to be embraced and supported by the public. For example, a health organization that partners with community leaders, local organizations, and stakeholders in codesigning health campaigns tailored to the community’s preferences and needs fosters trust through shared decision-making.
In general, as illustrated by Purnat et al. (Purnat, Nguyen, and Briand, Reference Purnat, Nguyen and Briand2023), there are several actions that institutions can take to strengthen ties with communities. Collaborative initiatives are vital for fostering effective community engagement in healthcare. By working with various stakeholders within the community, healthcare providers can create more impactful and sustainable health programs. Establishing community health committees composed of healthcare professionals, community leaders, local NGO representatives, and community members can help identify pressing health issues, plan targeted interventions, and monitor progress. This is a key strategy to ensure that health initiatives meet the community’s needs and foster a sense of ownership among members. Partnering with local schools and educational institutions to incorporate health education into their curricula is also crucial for educating children and young adults about important health topics such as nutrition, hygiene, mental health, and disease prevention. The creation of mobile health clinics to provide accessible healthcare services – including screenings, vaccinations, and basic medical care – for those with limited access can enhance the impact of institutional efforts. Additionally, organizing health fairs in collaboration with local businesses, religious organizations, and relevant stakeholders offers a platform for healthcare providers to engage directly with the community while raising awareness of various health issues and services. As discussed in the next section, collaboration with traditional mass media is also essential in all these efforts.
4.5 The Impact of Healthcare Professionals on Public Trust in Health Institutions
4.5.1 Poor-Quality Information by Health Professionals
In exploring trust within health institutions, a crucial aspect that can sometimes influence trust in unexpected ways is the role of healthcare professionals themselves. While they are generally seen as trusted sources of medical information and guidance, their actions and endorsements can occasionally undermine trust in health institutions. In 2021, the American Medical Association implemented policies to address poor-quality health information from professionals and specifically highlighted the risks of damaging the credibility of trusted health sources for patients and the public. There is substantial evidence on this issue, especially evident in the rise of medical influencers and practitioners who use their expertise to promote views or practices that may contradict established medical evidence or lack solid support (Coleman, Reference Coleman2022; Rubin, Reference Rubin2022; Sule et al., Reference Sule, DaCosta, DeCou, Gilson, Wallace and Goff2023). The sections below examine the complex ways healthcare professionals, including influencers and practitioners, can shape public perception and trust in health institutions. These sections explore the factors that contribute to these situations, their potential impacts on public trust, and the challenges they create in the healthcare landscape. Although healthcare professionals are central to shaping health-related discussions, their actions and endorsements are not beyond scrutiny, particularly in the digital age where information spreads quickly and widely. Analyzing these complexities reveals that trust in health institutions depends not only on external factors but also on internal influences within the healthcare community. By examining instances in which healthcare professionals (whether inadvertently or not) contribute to the erosion of trust, valuable insights can be gained into how a stronger and more resilient foundation of trust between health institutions and the public might be built.
4.5.2 Contributing Factors
Constant advancements and growing knowledge typically characterize medicine and healthcare. Consequently, healthcare professionals may have diverse viewpoints on certain medical topics or treatment options. These differences can appear in public discussions, such as debates among healthcare workers about how effective a particular treatment is. While these debates are a natural part of scientific progress, they can sometimes cause uncertainty and confusion among patients and the public, potentially eroding trust in health institutions. For example, conflicting opinions about using a specific medication can make patients unsure about which advice to follow.
Healthcare professionals are, first and foremost, individuals with their own beliefs and values. Sometimes, these personal convictions can conflict with established medical guidelines or evidence-based practices. When healthcare professionals openly support treatments or practices without scientific backing, it can cause confusion and mistrust among the public. For example, a healthcare provider promoting unproven alternative therapies may weaken trust in the evidence-based treatments recommended by health organizations. Here is the question, as posed by Grimes and Greenhalgh (Reference Grimes and Greenhalgh2024), regarding the need for regulatory bodies to limit and take action. Healthcare professionals, including medical influencers, can reach a vast online audience through various media platforms. Although this can be a powerful tool for disseminating accurate information and raising health awareness, it also provides a platform for the amplification of nonevidence-based views or controversial medical practices. Moreover, media outlets often feature healthcare professionals expressing unconventional views or advocating for treatments that challenge established medical norms, as this is often attractive to their audience.
Additionally, healthcare professionals, like many others, might not be immune to the allure of success, visibility, and an expanding online following. The chance to reach and connect with a broad audience has become an increasingly tempting opportunity. Some healthcare professionals, like many individuals, can be inspired or motivated by the desire for success and a growing online presence. Those seeking recognition and visibility may find social media particularly appealing. One notable aspect in this context is the appeal of unconventional views and alternative content. This type of content can spark discussions, stimulate curiosity, and attract greater engagement compared with traditional health information. In their effort to grow their online presence and followers, healthcare professionals may realize that their expertise goes beyond simply sharing traditional health information. Their diverse experiences and knowledge enable them to explore various related topics. This may include examining alternative therapies, discussing health-related controversies, sharing personal stories, or advocating for holistic well-being – topics that often generate significant public interest.
4.6 When Health Professionals’ Communication Can Erode Trust in Institutions
There are several key instances where health professionals’ communication might inadvertently or intentionally erode trust in institutions that promote information contrary to evidence (Gobo and Sena, Reference Gobo and Sena2022). Below, some hypotheses are presented that have been inspired by real examples easily found on social media.
Healthcare professionals may selectively cite scientific studies or research to support their views while ignoring a broader body of evidence that contradicts their stance. For instance, in the areas of nutrition and dietetics, a healthcare professional who advocates for a specific diet may cherry-pick studies that seem to support the diet’s effectiveness in weight loss; they emphasize small, short-term studies that show some positive results. However, they conveniently overlook larger, long-term studies that reveal the diet’s negative effects on overall health, including potential nutrient deficiencies and increased risks of heart disease. For example, restricted carbohydrate diets often marketed in popular books and websites can have health consequences (Janowska et al., Reference Janowska, Rogacka, Pyrak and Kornelia2022).
The echo chamber effect on social media platforms can strengthen existing beliefs and hinder critical thinking. When healthcare professionals mainly interact with like-minded individuals or groups, this can lead to the spread of unverified or biased information, further damaging trust. For example, a group of chiropractors creates an online community on social media. They share and discuss alternative treatments for various health conditions, often emphasizing the benefits of spinal manipulation for many ailments. Within this community, members eagerly support and validate each other’s posts, promoting chiropractic care as a cure-all for all health problems.
Despite the lack of solid scientific evidence supporting many of these claims, the echo chamber effect within the group can strengthen their beliefs (Jiang et al., Reference Jiang, Karami, Cheng, Black and Liu2021). Group members rarely engage with opposing viewpoints or critical discussions about the limitations and potential risks of chiropractic practices. As a result, they keep spreading unverified or biased information about the effectiveness and safety of their treatments. This insular online environment reinforces their existing beliefs, discourages critical thinking, and maintains a one-sided narrative. When the public encounters content from this group, they may be exposed to a skewed perspective that does not align with established medical evidence. It is also easy for people to express opinions based solely on authority, without citing relevant literature or considering supporting evidence. This can have a significant impact, especially when individuals trust experts’ judgments because of their professional credentials (Labinaz, Reference Labinaz2023). However, there is a need to differentiate between expertise in a specific field and broader healthcare knowledge (see, e.g., the case of Italy in Rovetta and Castaldo, Reference Rovetta and Castaldo2021).
4.7 Hero or Misguided: The Dilemma of Discredited Health Professionals
In recent years, a notable phenomenon has emerged in which, after facing disciplinary actions or bans by official bodies, some health professionals portray themselves as heroes or victims to their followers. These professionals often claim that their punitive measures result from speaking the truth or challenging established scientific norms rather than from professional misconduct or an intention to manipulate people (Milhazes-Cunha and Oliveira, Reference Milhazes-Cunha and Oliveira2023). One common scenario involves health professionals advocating for treatments or cures that are not supported by mainstream science or are outright disproven. For example, a doctor might promote a particular drug or natural remedy as a cure for a serious illness, despite a lack of scientific evidence or evidence to the contrary.
When regulatory bodies step in to prevent potential harm to patients, these professionals may claim that they are being persecuted for challenging the pharmaceutical industry or conventional medical wisdom. Another notable example is the case of health professionals who take an antivaccination stance. Despite overwhelming scientific consensus on the safety and efficacy of vaccines, some practitioners have spread fake information about vaccines, leading to public health concerns (Grimes and Greenhalgh, Reference Grimes and Greenhalgh2024). When medical boards or health organizations act against them, they often present themselves as martyrs, fighting against what they portray as the corrupt or misguided medical establishment. Some health professionals might misinterpret or deliberately misrepresent scientific research to support their claims. When their interpretations are challenged or debunked by peers or regulatory bodies, they may frame these rebuttals as a suppression of innovative thinking or an attack on their integrity rather than as part of the normal scientific process of peer review and critique. This narrative of being a hero or victim appeals to certain segments of the public, especially those who are skeptical of mainstream medicine or who believe in alternative health practices.
4.8 Counteracting Poor-Quality Information by Health Professionals
There is one important point to emphasize again. Healthcare professionals with many years of education and clinical experience can develop individual perspectives on medical practices and treatments. This variety of views is a natural and valuable part of scientific discussion, as it can lead to innovative approaches and critical reviews of existing practices. Such differences in opinions may arise due to personal experiences, interpretations of new evidence, or theoretical disagreements with prevailing medical norms. It is common for experienced practitioners to hold certain opinions that may not fully align with established evidence-based guidelines. This becomes problematic when these personal views – rather than encouraging constructive analysis and dialogue within scientific and professional communities – are directly shared with the public and turn disagreement into a way to gain followers. The challenge becomes greater when healthcare professionals use their authority and credibility to influence public opinion, often bypassing peer-reviewed scientific discussion.
How can institutions deal with this? Here, the approach varies significantly depending on whether these professionals operate in private practice or are part of larger healthcare institutions. For health professionals in their practice, the responsibility primarily falls on regulatory bodies and licensing authorities. These organizations play a crucial role in monitoring and ensuring that practitioners adhere to standards; they have the authority to conduct investigations, impose sanctions, or even revoke licenses in cases of serious misconduct. However, their reach is often limited to formal professional conduct, and they may struggle to control what practitioners say or promote outside of their clinical practice. In these scenarios, professional associations also play a vital role. They can offer guidance, education, and peer review mechanisms to encourage adherence to best practices. They can also exert peer pressure and provide platforms for professional discourse, which can help in realigning errant practitioners with established medical norms.
The situation is markedly different in healthcare institutions, such as hospitals or clinics. These entities have more direct control and oversight over their staff and can enforce strict policies regarding patient care and the dissemination of information. If a staff member is found to be promoting fake or misleading information, the institution can take immediate disciplinary action, which may include retraining, suspension, or termination of employment. These institutions also have a responsibility to provide ongoing education and training to their staff, ensuring that they are up to date with the latest medical research and practices. Moreover, healthcare institutions often have dedicated ethics committees or boards that can evaluate complex cases, ensuring that decisions are not just administratively sound but also ethically justified. These bodies can serve as forums for discussing and resolving conflicts related to medical health information. The existence of ethical guidelines for health professionals is a crucial foundation for ensuring responsible and accurate health communication. These guidelines typically emphasize the importance of providing evidence-based information, maintaining patient confidentiality, respecting patient autonomy, and avoiding conflicts of interest. They serve as a blueprint for maintaining the integrity and trustworthiness of the medical profession.
The challenge of countering communication that not only impacts public trust but can also cause real harm to people requires ongoing and concerted efforts beyond existing guidelines (see, for instance, Saver, Reference Saver2023 and Reference Saver2024). Although the guidelines can lay the groundwork, their effectiveness in the digital age is increasingly being tested. Regulatory bodies must actively monitor health communication by professionals, particularly in public and digital spaces. This involves not just checking for adherence to guidelines, but also for the potential impact of the information shared. Some boards in various parts of the world have started to focus on this, as mentioned earlier, such as the American Medical Association. However, more action is, of course, needed: Enforcement mechanisms should be robust and responsive, with clear consequences for spreading fake or misleading information (Baron and Ejnes, Reference Baron and Ejnes2022). At the same time, reinforcing public trust cannot rely solely on regulation; it also requires strategic and effective communication. While social media has amplified both credible and misleading voices, traditional mass media – television, radio, and newspapers – remain a powerful tool for shaping public health narratives. These platforms continue to play a crucial role in disseminating timely, accurate, and evidence-based information to broad audiences, including those less engaged with digital media. However, as shown in the next section, the priorities of health institutions and mass media often diverge, with the latter favoring immediacy and engagement over depth and scientific accuracy (see Table 4).
Key takeaways
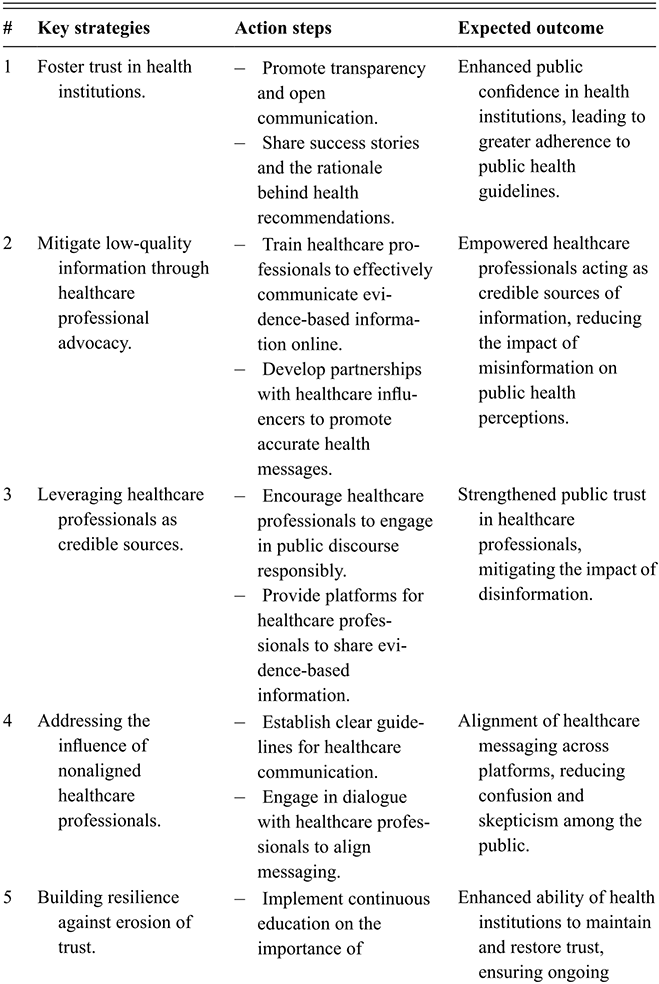
Table 4 Long description
The table presents five strategies to strengthen public trust in health communication, each with action steps and expected outcomes. The first strategy focuses on fostering trust through transparency, open communication, and sharing the rationale behind recommendations. The second highlights the role of healthcare professionals in countering low-quality information through training and collaboration with influencers. The third emphasizes leveraging healthcare professionals as credible sources by encouraging responsible public engagement and providing communication platforms. The fourth addresses the challenge of nonaligned professionals by promoting guidelines and dialogue to ensure consistent messaging. The fifth focuses on building resilience through continuous education and strategies to restore trust after misinformation events.
5 Health Institutions and the Traditional Mass Media in Public Health Communication
5.1 Overview
In the nuanced interplay between traditional media and healthcare communication, health institutions must harness the dual forces of rigorous scientific evidence and compelling narratives. By doing so, they not only illuminate the path to informed public engagement but also embrace the enduring legacy of the media’s role in shaping societal perceptions of health.
This section shifts focus to the role of traditional mass media – such as television, radio, and newspapers – in shaping public health communication.
5.2 Traditional Mass Media
For health institutions, engaging with the media is critical. Mass media outlets possess the unique capability to rapidly reach a vast and diverse audience. They also have the unique ability to engage with audiences that are less active on digital platforms, thereby bridging informational gaps within the wider population. By collaborating with the media, health institutions can amplify their messages and recommendations, thereby increasing the chances of effectively disseminating crucial health information. Thus, for instance, there is rich literature on the potential of television for public health communication (Burzyńska, Binkowska-Bury, and Januszewicz, Reference Burzyńska, Binkowska-Bury and Januszewicz2015; Catalan-Matamoros and Peñafiel-Saiz, Reference Catalan-Matamoros and Peñafiel-Saiz2019; Gollust, Fowler, and Niederdeppe, Reference Gollust, Fowler and Niederdeppe2019). Especially during health emergencies, such as disease outbreaks or natural disasters, the media serve as a crucial channel for timely communication, enabling health institutions to provide real-time updates, safety instructions, and guidance to the affected population (Anwar et al., Reference Anwar, Malik, Raees and Anwar2020). They are a powerful tool for raising awareness about health issues, preventive measures, and public health campaigns, contributing to enhanced public knowledge and awareness on a larger scale. This is why the media have the potential to influence public behavior and encourage positive health practices. Being featured in reputable media outlets adds credibility to the information provided by health institutions, validating their expertise and authority, which, in turn, can strengthen public trust in the information being shared. Here, they can act as a platform for institutions to engage directly with the public through interviews, expert opinions, and interactive sessions, allowing, for instance, for health professionals to address public concerns, clarify misconceptions, and provide valuable insights.
The integration of traditional media into health communication strategies is, however, not without challenges (Reynosa Navarro et al., Reference Reynosa Navarro, Guerra-Ayala and Casimiro-Urcos2021). As shown below, a key issue is the differing definitions of “newsworthiness” between health institutions and traditional media outlets, as well as the different agendas that health institutions and mass media can have. These divergences often center around the alignment of health messages with media priorities, which can significantly differ from the health-centered perspective of institutions.
5.3 Newsworthiness
The concept of “newsworthiness” plays a crucial role in shaping the information landscape, which is defined in the online Oxford Dictionary as “the extent to which some event, occurrence, statement, or observation has the potential to become news.” The concept determines what becomes a headline and what remains in the shadows. Newsworthiness is defined by a set of criteria that influence whether a story is reported and how it is presented to the public (Zoch, Reference Zoch2014). Clearly, these criteria can vary significantly between different types of organizations, particularly between mass media and health institutions.
The mass media’s approach to newsworthiness encompasses several key elements that profoundly shape health reporting. This has been documented in several case studies in different nations that analyze how certain information is presented as “news” to the public (Usher, Reference Usher2018; Prosser, Reference Prosser2021; Shahid, Reference Shahid2022; Blanco-Herrero et al., Reference Blanco-Herrero, van der Meer and van den Putte2025). Immediacy, a core principle in the media, plays a crucial role in the rapid dissemination of health information, particularly during urgent events like pandemics. Although immediate reporting is essential for public awareness and safety, it can sometimes prioritize speed over in-depth analysis, potentially resulting in superficial coverage that lacks context and nuance. Sensationalism, another characteristic of newsworthiness, aims to capture audience attention by provoking strong emotional reactions. In health reporting, sensationalism can manifest as an exaggeration of health risks or the efficacy of treatments. This exaggeration may distort the public’s perception and understanding of health issues, leading to unwarranted fears or unrealistic expectations. Conflict-driven narratives, which are often prevalent in media coverage of healthcare policies or vaccine skepticism, are designed to engage audiences through polarizing debates and disputes, as occurred in the public disagreement of experts during the COVID-19 pandemic (Labinaz, Reference Labinaz2023). Although such narratives capture attention, they can oversimplify complex health matters. For instance, media coverage that emphasizes conflicts between pro- and antivaccine groups may fail to provide a nuanced understanding of the benefits and risks associated with vaccination.
In addition to these aspects, the concept of newsworthiness in the media extends to other dimensions, including the preference for dramatic stories and narratives that involve famous individuals. The category “famous people” encompasses celebrities from the entertainment industry, public figures such as politicians and government officials, influential business leaders, renowned scientists and researchers, dedicated activists and advocates, prominent sports figures, popular influencers and social media personalities, and even historical figures of significance. Media outlets often find narratives involving these individuals to be newsworthy because their actions, achievements, health-related matters, or societal impact hold substantial interest for the public and align with the media’s quest for engaging stories. In general, human-interest stories, which often spotlight individual health experiences, add a relatable dimension to health reporting but can inadvertently neglect wider public health contexts.
Overall, the interplay of these various aspects of newsworthiness can significantly impact health reporting, influencing the tone, depth, and accuracy of media coverage on health-related topics. This media lens, which is effective in garnering public interest, challenges accuracy and balance in health reporting; it underscores the necessity for health institutions to engage critically with media processes and strive for communications that counterbalance sensationalism with scientific accuracy and depth.
On the contrary, health institutions’ approach to newsworthiness significantly contrasts with the mass media’s sensationalist strategy. As presented in Section 2, health institutions’ focus centers on public health impact and scientific accuracy, prioritizing content that educates and informs. This approach emphasizes the dissemination of reliable, evidence-based information, which includes advancements in medical research, critical health policy updates, and crucial public health advisories.
Again, as discussed in Section 1, health institutions aim to enhance public understanding and promote positive health behaviors. Their strategy involves a nuanced presentation of health issues that are often characterized by in-depth analysis and contextualization. This approach allows them to address complex health topics, such as epidemiological trends, the efficacy of new treatments, or the implications of health policy changes, providing the public with comprehensive insights. The main reference work in health communication, particularly in risk communication, provides guidance on disseminating health information effectively (Thornton et al., Reference Thornton, Glover, Cené, Glik, Henderson and Williams2016; Kreps, Reference Kreps2021; Thompson and Schulz, Reference Thompson and Schulz2021; Qiu and Chu, Reference Qiu and Chu2019). In stark contrast to the media’s focus on immediacy, health institutions place a premium on factual depth and the educational value of their communications (Schiavo, Reference Schiavo2013). This focus is aligned with the tenets of health literacy, which emphasize the importance of enabling individuals to access, understand, and use health-related information to make informed decisions (Ishikawa and Kiuchi, Reference Ishikawa and Kiuchi2010; Baker, Wolf, and Davis, Reference Baker, Wolf, Davis, Thompson, Parrott and Nussbaum2011; Connelly and Speer, Reference Connelly, Speer, Connelly and Turner2017). Through this lens, health institutions craft messages that are not only informative but also actionable, thereby significantly contributing to public health outcomes.
The academic discourse surrounding this dichotomy emphasizes the importance for health institutions to effectively manage these contrasting approaches. Striking a balance between the immediacy and attractiveness of mass media and the depth and accuracy of health communication is essential. Health institutions must craft strategies that make their messages engaging for mass media audiences without sacrificing their scientific integrity and educational objectives. Otherwise, information problems can occur.
For instance, a health institution publishes an in-depth report on a new vaccine’s efficacy. The mass media, favoring immediate impact, focus on a minor side effect, stripping away the nuanced context. This can result in heightened public anxiety and reluctance toward the vaccine, overshadowing the institution’s efforts to highlight the vaccine’s benefits. In another instance, a health institution cautiously reports a small outbreak of a new disease. The mass media, however, escalates the narrative, drawing premature parallels to past pandemics. This sensationalized portrayal can trigger unnecessary public panic, warping the institution’s balanced communication. Furthermore, when a health institution endorses a policy for clearer sugar content labeling, the media spotlights the ensuing clash between health authorities and food manufacturers. This shift in focus from health benefits to regulatory debates might skew public understanding and acceptance of the policy. When a nutritional study’s findings are released, the media’s oversimplification, exemplified by sensational headlines like “Superfoods that prevent cancer,” can lead to public misconceptions, ignoring the study’s intricate conclusions.
5.4 Strategic Alignment: Mass Media Priorities in Health Communication
To effectively align their communication strategies with the priorities of mass media while ensuring the accuracy and educational value of their content, health institutions can adopt various strategic approaches. There are several guidelines on how to interact with the mass media to present scientific information. For instance, the book by Richard Hayes and Daniel Grossman (Hayes and Grossman, Reference Hayes and Grossman2006), as well as the guide “How to get comfortable talking with the media” by Helen Santoro for the American Psychological Association (2022), provides important strategies for institutional health communication. These strategies are designed not only to enhance the appeal of health messages within the media landscape but also to uphold the integrity and informative nature of the content being disseminated. Specifically, these strategies include a few key points, as discussed below:
Human interest framing is a strategic approach to enhance the accessibility and relatability of complex medical data. This method involves sharing patient stories and transforming impersonal medical statistics into engaging narratives. An exemplary case would be portraying an individual’s journey with diabetes, offering insights into daily life challenges and the impact of treatment. This personalization of medical information forges a connection with the audience, presenting health conditions through the lens of real-life experiences. Such stories resonate emotionally and personally with audiences, significantly improving engagement and information retention. Moreover, as seen earlier, human interest stories hold appeal for the media because of their compelling nature and ability to evoke emotional responses. These narratives cater to the media’s objective of presenting content that deeply resonates with audiences, often resulting in higher engagement levels. When health institutions share such patient experiences, they provide the media with stories that are not only informative but also human and relatable.
Timely hooks are essential for gaining media traction with health messages. By aligning health campaigns with current events or significant dates, health institutions can capitalize on the public’s existing focus, thereby enhancing the relevance and impact of their messages. For instance, a mental health institution launching a campaign during Mental Health Awareness Month can effectively tap into heightened public interest in mental health topics at that time. This strategic timing ensures that the campaign is not only timely but also aligns with a period when the audience is more receptive to the message, significantly increasing its potential reach and influence.
To boost the appeal of their messages to the media, health institutions can transform complex health data into more media-friendly formats, such as press releases, infographics, or short videos. This approach involves simplifying detailed medical research into visually engaging, easy-to-understand content; it aligns with the media’s preference for quick, digestible information, ensuring greater accessibility and interest. By taking this approach, health institutions can communicate more effectively in the fast-paced media environment, balancing deep informational content with the need for concise, engaging material. For example, a detailed study on heart disease prevention could be summarized into an eye-catching infographic that highlights key facts and statistics, making it more likely for media outlets to share.
Providing media outlets with access to health experts for interviews or Q&A sessions is a valuable strategy for health organizations. This method ensures accurate information is shared, adding depth and authority to media reports. Direct interactions with experts give the audience credible insights, boosting the trustworthiness of the information. For example, a health organization could arrange for a leading epidemiologist to discuss new findings on a health talk show, thereby directly communicating complex medical insights to the public in an accessible and authoritative way.
Finally, joint educational efforts between health organizations and media outlets are an effective way to blend educational goals with a wide audience. These partnerships enable the broad and engaging distribution of health information. For instance, a joint campaign about the benefits of vaccination could utilize the media’s large reach, ensuring accurate and compelling delivery of crucial health messages to a diverse audience.
Concretely, crafting effective press releases for health institutions involves a detailed and strategic approach that can be summarized in the following steps:
First, identify the core message by defining the key message clearly. It should be newsworthy and relevant, aligning with the institution’s broader goals. For example, if the focus is on a new health study, the core message could revolve around its unique findings and implications for public health.
Second, determine the target demographic for the message. For a pediatric health update, for instance, the content should be tailored to parents, educators, and pediatricians.
Third, craft a compelling headline that can grab attention while summarizing the press release’s essence. For instance, “New paediatric study offers new insights into ….”
In addition, the body of the press release should be straightforward, addressing the key aspects of who, what, when, where, why, and how while being devoid of technical jargon. Statistics and quotes from health experts could add credibility. In addition, it is always important to highlight any warning people should pay attention to, for example, to discuss with their doctors and provide detailed contact information for further inquiries, ensuring it is easy for media personnel to reach out.
Importantly, health institutions should prioritize thorough review and approval of their communications before sharing them through mass media channels, recognizing the critical importance of this process for several key reasons. Maintaining accuracy and credibility is essential, with health institutions carefully ensuring that press releases and other information are accurate, evidence-based, and aligned with established medical guidelines. Deviating from these standards, such as spreading false or misleading information, can damage public trust and potentially cause health risks. Additionally, the review process acts as a safeguard for complying with legal and ethical standards. It enables health institutions to meticulously examine materials to ensure adherence to regulations and to protect patient confidentiality, thereby reducing legal risks. Consistent messaging is also vital, helping to prevent contradictions or mixed messages in their communication efforts. Overall, the rigorous review and approval procedures play a crucial role in protecting and maintaining the institution’s reputation. Equally important is the commitment to transparency about uncertainty. When evidence is still developing or data is incomplete, health institutions should avoid creating an illusion of certainty. Acknowledging what is known and what remains uncertain strengthens institutional integrity and builds public trust. Clear and responsible communication of uncertainty promotes informed engagement rather than confusion and fosters a culture of openness and resilience in public health discussions.
One last aspect to highlight: Leveraging traditional media to influence social media. The interconnected nature of traditional and social media offers a strategic opportunity for health institutions to amplify their communication impact. Traditional media, with its established credibility and broad reach, often serves as a primary source of information that influences discussions and trends on social media platforms. For instance, news segments or articles on health topics frequently spark conversations and sharing on platforms such as Facebook or Instagram, extending the reach of public health messages.
Targeting traditional media as part of a broader strategy can help shape the narratives that dominate social media (see, for instance, Al Quran, Reference Al-Quran2022). When health institutions ensure that accurate, evidence-based information is featured in traditional media, it creates a foundation for these narratives to be echoed and disseminated across digital platforms. For example, a televised interview with a health expert discussing vaccine efficacy can trigger widespread sharing and discussion online, countering misinformation and reinforcing public trust. Moreover, the symbiotic relationship between these media forms highlights the potential to engage different audience segments effectively. As mentioned at the beginning of this section, traditional media often reaches demographics less active on social media, while the viral nature of social media content ensures that key messages from traditional outlets can penetrate diverse online communities. By aligning communication strategies across both mediums, health institutions can enhance message consistency and broaden their influence.
All in all, while traditional media still play a key role in setting agendas, they are increasingly interwoven with digital platforms and social media dynamics. In this interconnected ecosystem, media narratives often find new life through shares, comments, and reinterpretations by a new generation of communicators presented in the next section: The influencers (see Table 5).
Key takeaways
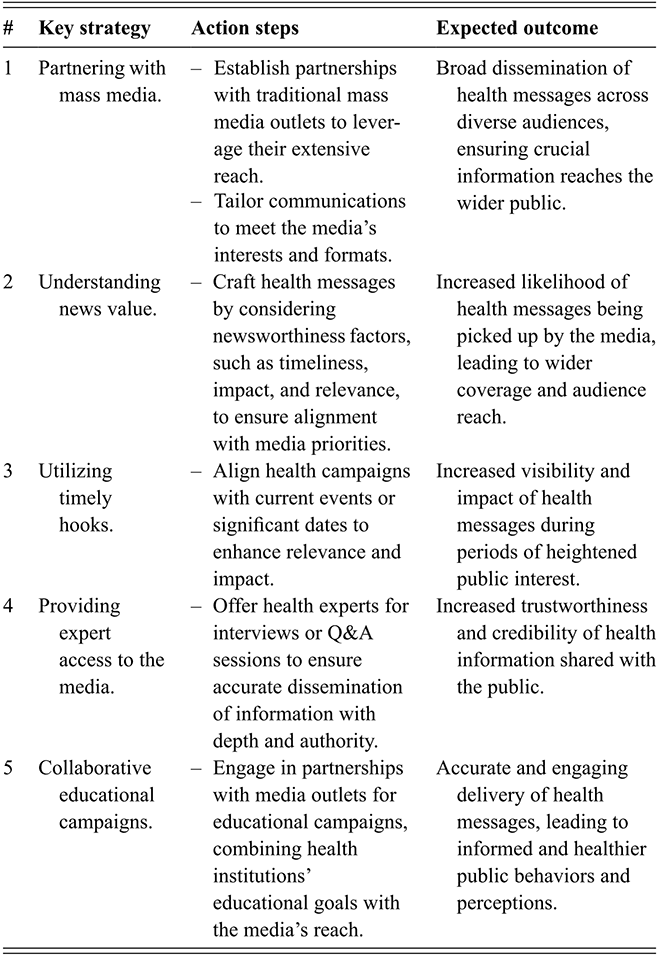
Table 5 Long description
The table outlines five strategies for enhancing public communication through traditional mass media, each with corresponding action steps and expected outcomes. The first strategy focuses on partnering with media outlets to leverage their reach and tailor messages to media formats. The second emphasizes understanding news value by aligning messages with timeliness, impact, and relevance to increase coverage. The third highlights the use of timely hooks, such as current events, to improve visibility and engagement. The fourth promotes providing expert access to ensure accurate and authoritative communication. The fifth strategy involves collaborative educational campaigns with media partners to deliver engaging and reliable health information, supporting informed public behaviours.
6 The World of Influencers
6.1 Overview
The path of communication is illuminated by the charisma of these digital era storytellers, yet is shadowed by divergences from evidence-based guidance. Embracing the art of engagement, health institutions must weave the rigor of science with the allure of narrative, crafting a harmony of authenticity and accuracy. In this delicate balance lies the power to transform public health landscapes.
This section explores the powerful role of influencers in shaping public health communication, focusing on the persuasive techniques they employ and the potential risks of manipulation.
6.2 Crafting Compelling Narratives in the Digital Age
Who is an influencer? The term refers to an individual who leverages social media platforms to shape public opinions, behaviors, and trends by engaging with a substantial online audience. These individuals often establish themselves as trusted voices in their areas of focus, ranging from health and wellness to lifestyle and advocacy (Kaňková, Binder, and Matthes, Reference Kaňková, Binder and Matthes2024a; Rubinelli, Reference Rubinelli2025b).
Today, influencers have become modern-day storytellers (Borchers, Reference Borchers, Borchers and Enke2021). They possess a unique set of skills that can capture and hold the interests of their vast online audiences. These persuasive communication techniques, which are reminiscent of the captivating artistry seen in TED Talks (Gallo, Reference Gallo2014), have created a new home in the dynamic realm of social media. There, influencers’ communication is adapted, amplified, and personalized to engage and inspire in the blink of an eye. As explained elsewhere (Rubinelli et al., Reference Rubinelli, Häfliger, Fiordelli, Ort and Diviani2023), there are specific persuasive techniques in public speaking that influencers implement, presented below.
Storytelling: Influencers often kick off their content with a story, a tale of personal growth, transformation, or relatable everyday experiences. For instance, a fitness influencer might share her journey of weight loss, highlighting not just the physical changes but also her emotional transformation. This narrative resonates deeply with her audience, fostering a powerful connection based on shared aspirations for self-improvement (Abidin, Reference Abidin2015).
Emotional appeal: Emotions play a significant role in online content. Influencers skillfully tap into emotions such as humor, empathy, or awe to craft messages that strike a chord with their audience (Rubinelli, Reference Rubinelli2025b). Take, for example, a mental health advocate who shares her struggles with anxiety, offering hope and support to others facing similar challenges.
Clarity and simplicity: In the online world, clarity is crucial. Communication by influencers excels at simplifying complex ideas, avoiding jargon, and ensuring that their content remains accessible to a broad audience. Consider a nutrition influencer who breaks down the science of a balanced diet into plain language, empowering followers to make healthier food choices.
Visuals: Visuals are paramount in effectively conveying messages. Indeed, online narratives are often accompanied by images, videos, and graphics to breathe life into their narratives. For instance, a skincare influencer demonstrating the step-by-step application of skincare products through visually appealing video tutorials can make the content more engaging and easy to grasp.
Passion and enthusiasm: Authenticity is the heart of online influence (Abidin, Reference Abidin2015). The pages of the most followed influencers convey genuine passion and enthusiasm for their subjects, inspiring and motivating their audience. Think of a sustainability influencer whose zeal for eco-friendly living sparks enthusiasm among followers to adopt more sustainable practices.
Structure: Influencers often follow a well-defined structure in their content, guiding their audience through introductions, key points, and memorable conclusions. Imagine a parenting influencer offering organized tips on managing children’s screen time, hence making what could be challenging information logical and digestible.
Interactivity: Engaging the audience is a must. Thus, influencers create a sense of community and participation through interactive elements such as polls, questions, or weekly challenges. Think of a fitness influencer who hosts engaging workout challenges, encouraging followers to join in and share their progress (Abidin, Reference Abidin2015).
This is close to their Call to action: Influencers often conclude their content with a call to action, motivating their audience to take specific steps or make positive changes. For instance, a climate change activist can convince followers to sign petitions, attend environmental events, and make eco-conscious choices.
Mastering these techniques is difficult but not impossible. Today, there are tons of material on public speaking, and it is easy to study the style of influencers who have amassed significant followings across various social media platforms (Borchers, Reference Borchers, Borchers and Enke2021). However, although the fundamental communication strategies remain consistent, the way in which influencers apply them can significantly vary. As shown below, communication by influencers might become a problem for health institutions.
6.3 Partnering with Influencers?
There is evidence that partnering with social media influencers can bring significant value to health institutions in their efforts to communicate with and promote public health (Lutkenhaus, Jansz, and Bouman, Reference Lutkenhaus, Jansz and Bouman2019; Nguyen Zarndt, Guo, and Benoza, Reference Nguyen Zarndt, Guo and Benoza2023). Influencers have established themselves as trusted voices among their followers, and their ability to reach and engage diverse audiences is a valuable asset. By collaborating with influencers, health institutions can leverage influencers’ reach, relatability, and authenticity to amplify important health messages. Influencers can also make health information more accessible and engaging with a wide range of demographics. Moreover, such partnerships can help health institutions tap into the latest trends and communication strategies, staying relevant and responsive in the ever-evolving digital landscape (Kostygina et al., Reference Kostygina, Tran and Binns2020).
Yet when health institutions contemplate partnering with social media influencers, several key considerations are instrumental to a fruitful collaboration. First, it is about finding a harmonious match in terms of relevance and alignment. The chosen influencer should resonate with the institution’s mission and goals. Their content and audience should be pertinent to the health topic at hand. Imagine an influencer specializing in fitness and wellness aligning with a campaign on physical health – their expertise and audience are perfectly in sync with the institution’s objectives (Albalawi and Sixsmith, Reference Albalawi and Sixsmith2017; Pourkarim et al., Reference Pourkarim, Nayebzadeh, Alavian and Hataminasab2023).
Credibility and trustworthiness stand as the key pillars in this partnership. Institutions must delve into the influencer’s history, assessing their track record for accuracy and reliability. It is not just about their words, but their actions and reputation over time. Consider an influencer known for their evidence-based approach to health information: they can become a beacon of reliability in a context where lots of suboptimal health information often plays a role.
Understanding the influencer’s audience demographics is key. The age, gender, location, and interests of their followers should align with the target demographic of the health message. This is akin to choosing the right messenger for the right audience. Engagement and reach, while often misconstrued as mere numbers, tell a deeper story. A vast following is impressive, but the true measure lies in how actively followers tend to interact and respond. An influencer with a smaller but highly engaged audience can sometimes be more effective than one with a larger, passive following. Clearly, ethical standards are nonnegotiable. The influencer must uphold transparency, especially in disclosing partnerships and potential conflicts of interest. This commitment to ethics not only builds trust, but it also sets a standard for content integrity.
It follows that, when health institutions consider partnering with social media influencers, a strategic and thoughtful approach is crucial for successful collaboration. This starts with an in-depth review of the influencer’s content quality, consistency, and messaging style. It is essential that their content not only aligns with the tone and style of the health message but also resonates with the intended audience.
Next, there is a need for a clear understanding and agreement on message alignment. It involves discussing and ensuring that the influencer comprehends the accuracy and evidence-based nature of the health information being conveyed. The goal is to maintain the integrity and accuracy of the health message. Understanding and adhering to legal and regulatory requirements is also paramount. This includes ensuring that the influencer’s content, as mentioned above, complies with the advertising and disclosure regulations relevant to the region.
Setting clear goals and key performance indicators is another critical step. It is about defining what success looks like and how it will be measured. This could range from the number of engagements to the quality of audience interactions. This also involves implementing robust monitoring and evaluation mechanisms. Indeed, regular assessments to ensure that the influencer’s content remains aligned with the institution’s goals and values are crucial for maintaining the integrity and effectiveness of the partnership.
Finally, an often-overlooked challenge lies in the question: Do influencers actually want to partner with health institutions? For many public figures (such as actors, athletes, or lifestyle icons), the decision to endorse institutional messages can be fraught with risk. Aligning with public health institutions may expose them to political backlash or alienate segments of their audience who are skeptical of official narratives. In a digital ecosystem that rewards popularity and engagement, taking a clear stance on sensitive health issues can lead to unfollows, negative comments, or reputational tension. This can create a dilemma for influencers whose success is deeply tied to maintaining broad appeal. As a result, even those personally committed to public health may hesitate to formalize partnerships, unless institutions can offer both content support and strategic protection for navigating potential reputational risks.
6.4 Mismatches
Although influencers can be valuable allies in promoting public health messages, a significant challenge arises when some influencers actively oppose or contradict the recommendations and information provided by health institutions (Figueiredo et al., Reference Figueiredo, Rodrigues, Pontes, Oliveira and Oliveira2022; Woolley, Reference Woolley2022; Kaňková et al., Reference Kaňková, Binder and Matthes2024b). These influencers, who can be seen as a kind of alternative health advocates, employ various techniques to gain visibility and attract many followers who question or reject established health guidance. Understanding these techniques is crucial for health institutions seeking to effectively address the ensuing communication dilemmas.
First, influencers opposing health institutions often create emotionally charged content designed to resonate with their target audience’s fears, anxieties, or frustrations. They may share personal anecdotes or stories that evoke strong emotional responses, making it challenging for followers to remain impartial. Thus, for instance, consider the following scenario:
An antivaccine influencer may share a heart-wrenching story of a child who allegedly suffered adverse effects from a vaccine, playing on parental fears and emotions.
Some influencers propagate conspiracy theories related to health institutions, suggesting hidden agendas or ulterior motives behind their recommendations. This tactic preys on skepticism and fosters mistrust, as in the following:
An influencer may claim that health institutions are colluding with pharmaceutical companies to conceal harmful vaccine side effects for financial gain.
In addition, there are influencers who often provide alternative explanations or solutions to health issues, positioning themselves as the arbiters of unorthodox but purportedly superior approaches to well-being. For instance, consider the following:
An alternative health advocate might promote natural remedies and holistic therapies as alternatives to conventional medical treatments.
Similarly, they may selectively present scientific studies or data that appear to support their viewpoints while ignoring a vast body of evidence. This cherry-picking of information creates a distorted perception of scientific consensus. For instance, consider the following:
An influencer might highlight a single study with inconclusive results as evidence against the safety of vaccines, disregarding numerous comprehensive studies confirming their safety.
Paradoxically, there are influencers who develop a cult-like following by positioning themselves as the sole bearers of “hidden truths.” They create an aura of authority and exclusivity, encouraging followers to rely solely on their guidance. For instance, consider the following:
An influencer may refer to themselves as the “only source of unfiltered health information” in a certain field and urge followers to distrust mainstream sources.
Very often, this type of influencer exploits concerns about freedom of speech and censorship to galvanize support. They claim that health institutions and social media platforms suppress dissenting voices with messages that, for instance, frame any action taken by social media platforms to limit the spread of misleading health information as an attack on free speech. Finally, they can oppose health institutions by fostering communities and supporting networks that align with their ideologies. This sense of belonging can be a powerful motivator for followers because they find affirmation and validation within these groups. Thus, for instance, antivaccine influencers often create closed online communities where followers can share experiences, reinforce beliefs, and offer support.
Understanding the techniques employed by these influencers is essential for health institutions seeking to counteract poor-quality information and strengthen the trust of their target audience. Indeed, recognizing the emotional appeal, alternative narratives and persuasive tactics used by these influencers enables health institutions to craft more effective and empathetic communication strategies (Rubinelli, Reference Rubinelli2025b).
6.5 Behind Manipulation
Influencers, just like any other communicator, have a range of motivations and intentions when sharing information on social media platforms. Although some genuinely aim to educate, inform, or entertain their audience in a responsible way, others may have different objectives. In some instances, influencers may prioritize sensationalism, virality, or personal gain over the accuracy of the information they disseminate (Powell and Pring, Reference Powell and Pring2024).
As mentioned earlier, manipulation is a reality in the realm of many health influencers. This could involve spreading unfounded health claims, promoting pseudoscientific remedies, or distorting facts to align with their own beliefs or agendas (MacDonald and Brianna, Reference MacDonald and Brianna2023; Field-Springer et al., Reference Field-Springer, Striley and Byerly2024). This type of low-quality information becomes manipulated when it involves influencing the perceptions, behaviors, or decisions of the audience through cunning or deceptive tactics for personal gain. Influencers may employ various psychological techniques to achieve this, such as appealing to emotions, exploiting cognitive biases, or creating a false sense of urgency. For example, an influencer using emotionally charged language to persuade their followers to purchase a particular product with exaggerated or unfounded benefits is practicing manipulation.
Detailed Wikipedia pages about some influencers, among other sources, or fact-checking platforms may meticulously document their history of dubious claims and the harmful narratives they have perpetuated. These tools are of value for guiding readers (Porter and Wood, Reference Porter and Wood2021). However, despite such efforts to highlight their lack of credibility, some of the influencers often continue to attract and maintain a substantial following. This is part of the phenomenon known as the “continued influenced effect” (Lewandowsky et al., Reference Lewandowsky, Ecker, Seifert, Schwarz and Cook2012).
The resilience of people who continue to maintain large audiences despite the low quality of their communication can be perplexing, but, again, it is rooted in their skillful ability to forge emotional connections with their audience. In fact, a paradoxical effect can occur, where the more institutional sources criticize the actions of certain influencers, the more these influencers are followed by individuals skeptical of institutions (Lewandowsky et al., Reference Lewandowsky, Ecker, Seifert, Schwarz and Cook2012). This counterintuitive phenomenon is often exacerbated by influencers who are adept at leveraging such criticism to their advantage. They can frame institutional condemnation as a validation of their credibility or as an expression of alternative, contrarian viewpoints, thereby attracting an audience that distrusts traditional authority figures (Zollo et al., Reference Zollo, Bessi and Del Vicario2017). Moreover, the communities formed around such characters serve as echo chambers in which dissenting voices are muted, and contrary information is met with skepticism or dismissal. Within these digital enclaves, followers find validation of their beliefs and become further entrenched in their allegiance to the influencer. The sense of belonging and shared identity within these communities reinforces trust in the influencer’s messages, regardless of their factual accuracy.
Understanding the dynamics at play in the digital landscape is essential for health institutions. The challenge lies not only in debunking false claims but also in addressing the underlying emotional and social factors that sustain the influence of such individuals within their dedicated communities.
6.6 Should Health Institutions Respond?
In the intricate landscape of health communication, the decision of how and when health institutions should respond to contradictory messages is laden with complexities. The topic of when to answer and how is beautifully addressed by Vraga et al. (Reference Vraga, Ecker, Žeželj, Lazić, Purnat, Nguyen and Briand2023). What follows below is a synthesis of some key aspects.
Consider a scenario where an influencer with a vast audience begins advocating for a do-it-yourself treatment for a serious illness devoid of any scientific backing. This situation is not merely a case of differing opinions, but it represents a tangible risk to public health. The influencer’s substantial reach and persuasive power can lead to widespread adoption of ineffective – or even harmful – practices among their followers. In these instances, health institutions have not just an opportunity but a responsibility to intervene.
Clearly, it is fundamental to identify the potential impact of distorted health information (Vraga et al., Reference Vraga, Ecker, Žeželj, Lazić, Purnat, Nguyen and Briand2023). This process begins with meticulous monitoring of social media trends. By scrutinizing the ebbs and flows of conversations on these platforms, institutions can identify emerging narratives and track the reach of potentially misleading health information. In the next step, they can ponder the possible consequences of suboptimal health information: Could it lead to harmful health behaviors? Might it disrupt ongoing public health efforts or instigate unwarranted panic? This careful consideration is essential to gauge the severity of certain information’s potential effects. Simultaneously, health institutions can turn to a council of wisdom, consulting medical experts, epidemiologists, and public health professionals. These experts can dissect the accuracy of the information and unravel the potential health risks tied to it, offering a scientific lens through which the content can be evaluated.
Understanding the audience is another key aspect. Delving into who is consuming and sharing suboptimal information helps in understanding their vulnerability. Are specific groups more susceptible to certain types of information not in line with recommendations? This audience analysis is pivotal in shaping the institution’s response. Here, historical precedents can serve as valuable guides. Past incidents where similar low-quality information resulted in public harm offer crucial insights and can help predict the potential outcomes of current scenarios. Finally, legal and ethical considerations are meticulously examined. Do the misleading messages violate any laws or regulations? What are the ethical obligations of the institution in this context? This legal and ethical review ensures that the response is not only effective but also aligns with societal standards and expectations.
In answering the question “when to respond?”, determining the timing of a response is crucial. Health institutions should consider that, if unsupported claims are spreading rapidly and can cause immediate harm, a swift response is essential to counteract its impact. For instance, an influencer starts a social media campaign promoting a dangerous dietary trend that could lead to health risks. Given the rapid spread of this trend and its potential harm, health institutions should respond swiftly to provide accurate information and warnings. Of course, staying silent is an option for health institutions. Indeed, for health institutions, choosing to stay silent can sometimes be a strategic response to certain health-related claims, particularly when what is in question is absurd or only believed by a marginal segment of the population.
In general, health institutions must also be mindful of the potential risks associated with their responses. These risks include at least three main problems:
First, amplification: When health institutions respond to influencers who have big audiences, there is a risk of inadvertently amplifying false claims by drawing more attention to them. It is crucial to carefully consider the potential for this effect when deciding whether to respond (National Academies of Sciences, Engineering, and Medicine, 2022). For example, if a health institution responds to a small, relatively unknown influencer who has made false claims about a particular medical treatment, the response might draw more attention to the influencer’s message, inadvertently amplifying it. This phenomenon is akin to the “Streisand effect,” where an attempt to suppress information can lead to greater publicity (Broniatowski, Dredze, and Ayers, Reference Broniatowski, Dredze and Ayers2021; Innes and Innes, Reference Innes and Innes2023).
Second, the backfire effect: Responses to unsupported claims may not always achieve their intended outcome and can sometimes backfire. In some cases, attempts to correct false information can actually entrench individuals’ existing beliefs, leading to what psychologists refer to as the “backfire effect.” Health institutions should carefully craft their responses to minimize this risk. For instance, when a health institution responds to an influencer promoting false claims on vaccines, some of the influencer’s followers may become more committed to their antivaccine beliefs, despite the institution’s efforts to correct the information (Lewandowsky et al., Reference Lewandowsky, Ecker, Seifert, Schwarz and Cook2012, Reference Lewandowsky, Cook, Ecker, Albarracín and Kendeou2020).
Third, resource allocation: Responding to every suboptimal health claim in the online world is impossible, and, even in small scenarios, resource-intensive. This was very much stressed, for instance, in all important work by the World Health Organization on how to manage low-quality information during the COVID-19 pandemic (Calleja et al., Reference Calleja, AbdAllah and Abad2021; Organization, 2021; Rubinelli, Purnat et al., Reference Rubinelli, Purnat and Wilhelm2022)
Overall, it is critical to address emotional concerns and engage with empathy (Vraga et al., Reference Vraga, Ecker, Žeželj, Lazić, Purnat, Nguyen and Briand2023). Acknowledging and addressing the concerns of those exposed to false information, empathizing with their worries, and providing emotional support alongside the correction of facts is essential. Similarly, it is important to approach interactions, even with hostile or confrontational individuals, with empathy and respect to avoid making the divide bigger. Maintaining professionalism and resisting getting drawn into personal conflicts or heated arguments is strategic communication.
Indeed, it is well known that social media platforms can also be breeding grounds for anger, hostility, and heated exchanges (Chuai and Zhao, Reference Chuai and Zhao2020; Horner et al., Reference Horner, Galletta, Crawford and Shirsat2021). One of the reasons for this phenomenon is the anonymity and detachment that online interactions provide. When individuals communicate through screens rather than face-to-face, they may feel less inhibited and more inclined to express anger and frustration openly. Moreover, the nature of social media algorithms and user engagement often rewards sensational or controversial content. Posts that evoke strong emotions, including anger, tend to receive more likes, comments, and shares, increasing their visibility on users’ feeds. As a result, some users may deliberately craft provocative content to garner attention or promote their viewpoints, further fuelling heated discussions and negative interactions.
In addition to these factors, what could be defined as the “outrage culture” has become prevalent on social media. This refers to a tendency for online communities to quickly amplify anger and outrage over various issues, often in response to news events, public figures’ actions or even seemingly innocuous posts (Middaugh, Reference Middaugh2019; Serrano-Puche, Reference Serrano-Puche2021). When one post sparks anger, it can lead to a cascade of comments and replies, each more incensed than the last, creating a cycle of escalating anger and hostility. The forms that anger and hostility take on social media can vary widely; these may include personal attacks, name-calling, and derogatory comments aimed at individuals or groups. It can also manifest as “cancel culture,” where individuals are collectively criticized and shamed for their actions or statements, sometimes resulting in real-world consequences such as job loss or social ostracization.
When individuals associated with health institutions, especially prominent figures like the Director-General of the World Health Organization (WHO), come under attack or criticism on social media, it is crucial for these institutions to respond with tact and professionalism. The first rule is to stay composed and avoid reacting emotionally. Quick, emotional responses can exacerbate conflicts and further harm an institution’s reputation. In addition, it is important to determine if the criticisms arise from misunderstandings, personal attacks based on false beliefs, or legitimate concerns. This evaluation helps tailor an appropriate response. In sum, the concerns must be addressed with empathy by crafting a factual, respectful, and professional response that directly addresses the points raised in the criticism while avoiding personal attacks or defensive language (see Table 6).
Key takeaways
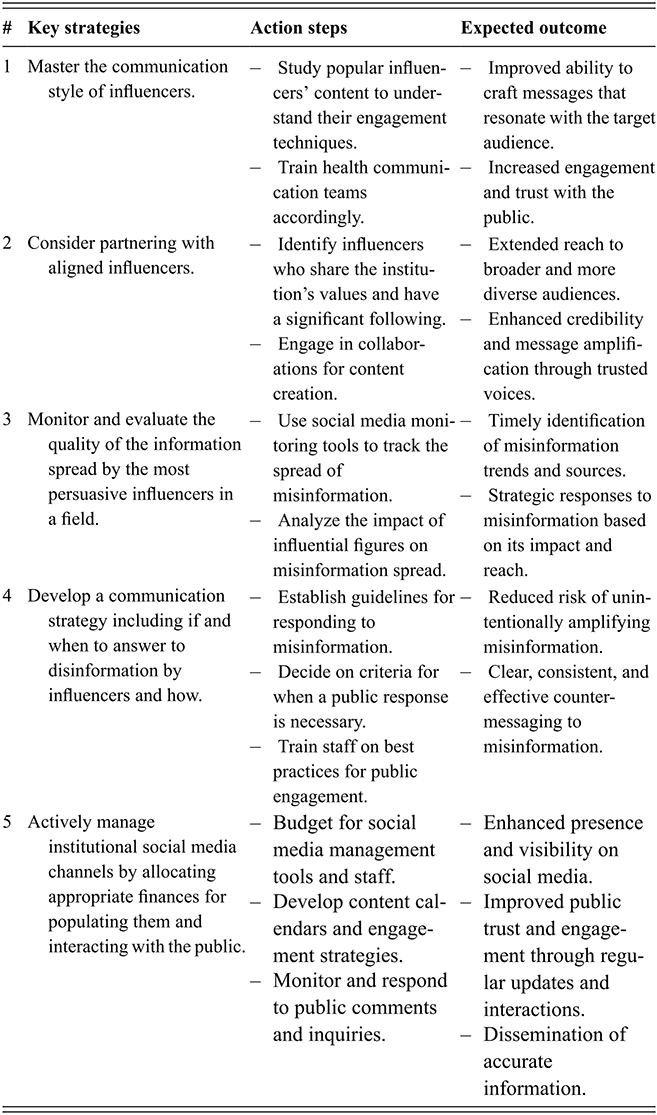
Table 6 Long description
The table outlines five strategies related to the role of influencers in health communication, each with action steps and expected outcomes. The first strategy focuses on understanding and adopting influencer communication styles to improve engagement and trust. The second emphasizes partnering with aligned influencers to expand reach and credibility. The third highlights monitoring the quality of information shared by influential figures to detect misinformation trends and respond strategically. The fourth addresses the need for structured responses to misinformation, including guidelines and staff training to ensure effective counter-messaging. The fifth focuses on actively managing institutional social media channels through adequate resources, planning, and engagement, enhancing visibility, trust, and dissemination of accurate information.
7 The Bases of Effective Health Message Design
7.1 Overview
Even the most brilliant ideas, if poorly expressed, risk falling flat like seeds scattered on barren soil. Today, more than ever, their impact depends on the ability to reach people clearly, engage with them, and take root in their understanding.
Merging insight from the classical and modern traditions, this section offers general insights and practical guidance on health message design that relate to the themes covered earlier.
7.2 Some Lessons from Classical Rhetoric
In the realm of persuasive communication, the Rhetoric of Aristotle, the Greek philosopher who first conceptualized the art of persuasion, may seem an unlikely or even outdated reference in today’s fast-paced and digitally dominated communication landscape. Yet, his classical principles remain a cornerstone, illuminating timeless strategies for influence through spoken and written word.
Aristotle posited that effective persuasion hinges on three pivotal elements: ethos, logos, and pathos (Rubinelli, Reference Rubinelli2009, Reference Rubinelli2018). These elements are more necessary than ever in contemporary health communication, where trust, clarity, and emotional resonance are critical to breaking through the noise. Ethos pertains to the credibility and ethical character of the speaker, underscoring the importance of trustworthiness and authority in the eyes of the audience. For health institutions, establishing a strong ethos means demonstrating not only scientific competence but also a genuine commitment to the community’s well-being. Logos, the backbone of effective communication, revolves around presenting data and arguments with clarity, logic, and coherence. This entails distilling complex health information into accessible, actionable insights that empower individuals to make informed decisions. Finally, pathos speaks to the emotional connection between the communicator and the audience, tapping into feelings such as hope, fear, or solidarity to motivate health-positive behaviors.
Similarly, Cicero, the Roman rhetorician and philosopher, offers lessons that resonate powerfully with contemporary health communication. He outlined five processes of effective communication, three of which are particularly relevant today: inventio (discovery), dispositio (arrangement), and elocutio (style) (Kennedy, Reference Kennedy2009; Rubinelli, Reference Rubinelli2009). Inventio involves the discovery or identification of the right content to speak or write about a certain topic. In the context of health institutions, this means, for instance, harnessing public health data and understanding the information needs and values, knowledge, attitudes, and beliefs of the target audience. Dispositio concerns arranging and structuring content in a logical and coherent flow. Health communication benefits greatly from this process, ensuring complex topics are broken down and delivered in a way that leads audiences to clear, actionable conclusions. Elocutio is where the art of communication truly shines. Beyond accuracy and informativeness, the way a message is expressed, its rhetorical style and flavor, influences its impact. As mentioned in many previous sections, health institutions must embrace storytelling, metaphors, and rhetorical devices to create messages that are not only clear but also compelling and relatable. This is particularly important in an era where attention spans are short and audiences are inundated with competing information.
7.3 The Framework of Social Marketing for Behavior Change
The field known as “social marketing” bridges the gap between timeless rhetorical principles and the demands of modern public health communication, offering a structured framework for achieving measurable behavior change. While classical concepts like ethos, logos, and pathos guide the how of persuasion, social marketing emphasizes the who, what, and where – ensuring messages are tailored, impactful, and delivered through the most effective channels. In institutional health communication, social marketing is not only about raising awareness but also about inspiring action that fosters healthier behaviors and improves community well-being (see, for instance, Lee and Kotler, Reference Lee and Kotler2019).
At its core, social marketing serves a dual purpose. First, it informs by creating awareness about critical health issues, such as risks, preventive measures, or available services. These messages provide individuals with the knowledge to make informed decisions. For instance, an awareness campaign about the importance of hand hygiene during a health crisis could outline best practices and their role in preventing disease transmission. Second, social marketing motivates action by designing campaigns that address specific behaviors. Behavior-change messages delve deeper, targeting beliefs, motivations, and barriers. A campaign to reduce smoking among teenagers, for example, might highlight the health risks of smoking, address social pressures, and offer strategies to resist those pressures, empowering adolescents to make healthier choices.
7.3.1 Message Design and Testing
The effectiveness of social marketing lies in its systematic approach to message design, which involves several key steps, among which the most important reported in traditional texts on social marketing (Lee and Kotler, Reference Lee and Kotler2019) are the following.
Audience segmentation is a step in designing effective health communication that involves dividing the general population into distinct subgroups based on characteristics such as age, gender, socioeconomic status, behaviors, cultural background, or health status. The goal is to ensure that communication efforts are not generic but targeted. For example, messaging about vaping risks may be directed specifically at teenagers; campaigns about preventive health screenings may focus on middle-aged adults; and flu vaccination initiatives may be tailored to older adults. To guide this process, it is essential to draw on established theories of behavior change, see Section 7.4, which help identify the psychological or contextual factors that need to be targeted. These theories offer a structured lens to determine whether a message should focus, for instance, on increasing perceived benefits, reducing perceived barriers, enhancing self-efficacy, or reshaping social norms.
Messages are then crafted to be culturally sensitive, relatable, and visually engaging. The language, tone, and format must align with the preferences of the target audience, be it visually rich social media posts for younger demographics or detailed brochures for older populations.
Channel selection: Choosing the appropriate communication channels is essential for effectively reaching the target audience. Digital platforms like Instagram or TikTok might be ideal for engaging younger audiences, while traditional media such as radio and print may be more effective for reaching rural or older demographics.
Pre-testing messages: Before full-scale implementation, pre-testing ensures that messages resonate with the target audience. Methods such as focus groups, pilot campaigns, and cognitive testing help evaluate clarity, relevance, and potential effectiveness (e.g., Lapka et al., Reference Lapka, Jupka, Wray and Jacobsen2008). Feedback from this phase allows institutions to refine and optimize messages, improving their likelihood of success.
Post-campaign evaluation is essential for assessing the actual impact of a health communication intervention. It allows institutions to determine whether the campaign achieved its intended outcomes within the target audience. This phase typically involves collecting and analyzing data through surveys, interviews, web analytics, or health service usage statistics. Evaluating both intended and unintended effects provides valuable insights into what worked, what didn’t, and why.
7.3.2 The 7Cs of Communication
When speaking about the form and expression of certain content, the 7Cs of communication – clarity, conciseness, concreteness, correctness, coherence, completeness, and courtesy – offer another set of foundational principles that can greatly enhance the efficacy of health communication strategies. These elements, codified by John Baird and Jim Stull (Reference Baird and Stull1992), contribute to the overall form of health messages, and they are described in what follows.
Clarity is achieved by using simple language and avoiding jargon, making the health information accessible to all. For instance, instead of saying “hypertension,” “high blood pressure.” This approach is important to talk to a broad audience, irrespective of their medical knowledge.
Conciseness, while maintaining the integrity of the message, means delivering information succinctly. In a health advisory about pandemic safety, for example, saying “Wear masks, maintain distance, and sanitize hands regularly” communicates essential actions without overwhelming the audience with details.
Concreteness strengthens the message by providing specific examples or actionable steps that the audience can follow. Telling people to “Eat a diet high in fruits and vegetables to reduce the risk of chronic diseases” gives clear direction on how to improve their health.
Correctness is crucial in maintaining the trust of the audience. It entails ensuring that health communication is factual, up-to-date, and evidence-based. For example, updating guidelines as new research becomes available on a virus ensures that the public receives accurate and current health advice.
Coherence ties the message together, ensuring that all parts of the communication are logically connected. In a campaign promoting vaccination, coherence means that messaging from various channels – social media, press releases, and public service announcements – should consistently support the benefits and safety of vaccines.
Completeness requires that all necessary information be included in the message, leaving no crucial questions unanswered. A health alert about an outbreak, including symptoms, prevention strategies, and what to do if one is sick, provides a comprehensive guide for the public.
Courtesy, the final C, involves respecting the audience’s perspectives and feelings. Addressing vaccine hesitancy with empathy and understanding, rather than dismissal, encourages open dialogue and builds trust between health institutions and the public.
7.4 Insights for Precision Messaging
Building on the foundational principles of classical rhetoric and the structured, audience-centered strategies of social marketing, behavioral and cognitive sciences provide additional essential tools for refining health communication. As explained in Rubinelli et al. (Reference Rubinelli, Myers, Rosenbaum and Davis2020), there are important behavior models that instruct on how to design and tailor health-related messages. Below, there is a short introduction of the four most know.
The Health Belief Model (HBM) is foundational for addressing individuals’ perceptions of health risks and the benefits of taking action. Messages based on the HBM target four key constructs: perceived susceptibility, perceived severity, perceived benefits, and perceived barriers. For example, a vaccination campaign could highlight susceptibility (“Without vaccination, you are X times more likely to contract this illness”), emphasize severity (“This disease can lead to long-term complications”), and underscore the benefits (“Vaccines protect you and your loved ones from serious illness”). To address barriers, the campaign could reassure audiences with evidence-backed information about side effects.
The Theory of Planned Behavior (TPB) complements the HBM by focusing on the roles of attitudes, subjective norms, and perceived behavioral control in shaping intentions. Effective messages under TPB aim to influence attitudes positively (e.g., “Quitting smoking improves your health and boosts your energy”), leverage social norms to encourage behavior (e.g., “The majority of adults in your community are choosing to quit smoking”), and address barriers by enhancing self-efficacy. For instance, providing access to support groups or practical quitting strategies can help audiences feel confident in their ability to change.
The Transtheoretical Model, also known as the stages of change model, is particularly valuable for tailoring messages to individuals based on their readiness for action. Messages can be customized for different stages, from raising awareness of risks for those in the precontemplation stage to offering actionable steps for those in the preparation stage. For example, a sedentary individual might receive a message that raises awareness about the dangers of inactivity, while someone preparing to exercise could be encouraged to “Start with a 15-minute walk each day and gradually increase your activity.”
Understanding how people perceive and respond to risks is the next critical step for designing effective health messages. The Extended Parallel Process Model provides a valuable framework by balancing perceived threat and efficacy. Health messages should credibly articulate risks (e.g., “Exposure to secondhand smoke significantly increases the risk of lung cancer”) while simultaneously empowering individuals with actionable solutions (e.g., “Protect your family by making your home smoke-free today”). By addressing both threat and efficacy, this approach can ensure that audiences understand the seriousness of the issue while feeling confident in their ability to take appropriate action.
7.5 Framing: Shaping Perceptions Through Messaging
The next concept that requires consideration is “framing” in health message design. Framing involves the selection of certain aspects of reality and making them more salient in a communicating text in such a way that they promote a particular problem definition, causal interpretation, moral evaluation, and/or treatment recommendation (see, for instance, Updegraff and Rothman, Reference Updegraff and Rothman2013). Framing is a powerful tool that shapes how information is perceived and understood by the public (Salovey and Wegener, Reference Salovey, Wegener, Suls and Wallston2003). It’s not just about what is communicated, but how it is communicated, influencing the audience’s attitudes and behaviors toward health issues.
For instance, framing a health issue through a loss perspective (“If you don’t vaccinate, you are at risk of serious illness”) versus a gain perspective (“Vaccination protects you from serious illness”) can lead to different responses from the public. Similarly, framing messages around collective benefits (“Our community is safer when we all vaccinate”) versus individual benefits can alter the appeal of health behaviors. Specifically, gain-framed messages, such as “By getting vaccinated, you’re taking a proactive step toward protecting yourself and your loved ones from severe illness,” focus on the benefits of taking action. This can be contrasted with addressing barriers, as seen in messages like, “Even if you’re concerned about vaccine side effects, the benefits of vaccination far outweigh the minor discomforts, protecting you from severe disease.”
Positive emotional framing can be illustrated by campaigns that encourage healthy behaviors with hopeful messages, like “Join the millions who have quit smoking and breathe easier, feeling the pride of a healthier life.” Conversely, negative emotions should be used carefully; for instance, a campaign might state, “Ignoring the flu vaccine puts you and your loved ones at risk,” which uses fear to emphasize the importance of vaccination without causing panic. Thus, as Luise Cummings illustrated (Reference Cummings2012), the use of threats and fear appeals arguments is valuable for public health messages. Framing around social norms can also be effective, as seen in campaigns like, “9 out of 10 people in our community wear masks to protect each other. Join them and show you care.” This message leverages the influence of perceived social behavior to encourage conformity to health-positive actions.
While framing offers a powerful tool for health communication, its application is not without pitfalls. For instance, overly simplistic or emotionally charged messages might be misconstrued as manipulative, such as a campaign overstating the immediate benefits of a new health supplement without adequate evidence, which could lead to public skepticism. Moreover, the diversity of audiences means that a one-size-fits-all approach to framing may not work. A campaign that effectively motivates one demographic through the use of community-focused messages, like “Our town is healthier when we all get vaccinated,” may not resonate in the same way with a younger audience that values individuality and might respond better to messages emphasizing personal freedom and choice, such as “Take control of your health by getting vaccinated.”
7.6 Crisis Communication Frameworks
Finally, public health emergencies require effective risk communication strategies to guide public behavior, minimize harm, and build trust. The literature and guidelines on risk communication are extensive. Here, it is important to highlight some examples of established frameworks of risk communication to illustrate what they involve, but also to discuss some overall limitations that need to be addressed to improve institutional communication. Specifically, below is a brief description of the Centers for Disease Control and Prevention’s Crisis and Emergency Risk Communication (CERC) model, the US Environmental Protection Agency’s Strategic and Effective Risk Communication (SALT) framework, and the Food and Drug Administration’s (FDA) Evidence-Based Risk Communication Approach.
The CERC model (Center for Disease Control and Prevention, 2018) emphasizes six core principles – Be First, Be Right, Be Credible, Express Empathy, Promote Action, and Show Respect – which guide health institutions in navigating the phases of crisis communication: Preparation, Initial, Maintenance, and Resolution. CERC is particularly strong in its emphasis on empathy and trust-building, making it effective for addressing public fears and fostering compliance during emergencies.
The SALT framework (US Environmental Protection Agency, 2021) extends the principles of risk communication through its Strategy, Action, Learning, and Tools approach. SALT prioritizes proactive planning, continuous evaluation, and iterative learning. While CERC focuses heavily on immediate and clear messaging during crises, SALT adds a reflective component to ensure long-term improvements in communication strategies. It places particular emphasis on understanding audience-specific factors, such as cultural norms, literacy levels, and trust dynamics, making it a highly adaptable tool.
The FDA’s Evidence-Based Risk Communication approach (Fischhoff, Brewer, and Downs, Reference Fischhoff, Brewer and Downs2011) further complements these frameworks by grounding communication efforts in rigorous scientific evidence. This model emphasizes tailoring messages to specific audiences and using narratives to engage the public and persuasion techniques. It excels in balancing the presentation of risks and benefits, ensuring the public is well-informed to make decisions, such as during food recalls or medical emergencies.
In the rapidly evolving field of crisis communication, these frameworks and models provide invaluable foundations for managing public health emergencies. They provide a structured approach, offering step-by-step processes that ensure consistency and coherence in messaging across diverse crises. Yet, these frameworks face significant challenges in today’s fast-paced, digitally fragmented communication landscape. The spread of information poses a direct threat to their effectiveness. There is little time for the careful planning of health messages, as communication needs to be fast to overcome the viral nature of digital content and algorithm amplification. Social media’s dominance has further splintered audiences into micro-communities, each with unique needs and perspectives, making it difficult to tailor messages. Additionally, there is still a focus on one-way communication in these frameworks that leaves a gap in addressing the demand for interactivity.
Health institutions must think beyond traditional campaigns and launch dynamic, immersive initiatives to enhance digital health literacy. To foster meaningful two-way communication, health institutions should develop conversational ecosystems that actively engage the public. This could include AI-driven chatbots for real-time interaction, virtual town halls, and user-driven feedback loops. Such ecosystems allow audiences to voice concerns, share insights, and feel heard, turning passive information recipients into active participants in the communication process.
As explained in Section 6, collaborating with influencers requires more than ad hoc partnerships. Institutions should establish long-term alliances with diverse, credible influencers, training them to effectively communicate evidence-based messages. A decentralized approach to communication can enhance trust by leveraging voices already embedded within communities. Leveraging predictive analytics, institutions can identify trends and harmful information outbreaks before they gain traction. This could involve proactive messaging, deploying preemptive content tailored to counter emerging narratives, and reducing the reactive burden during crises. On a practical level, all this emphasizes the need to establish dedicated, multidisciplinary task forces that bring together experts from fields such as communication, technology and data science, behavioral psychology, and community engagement. These teams can function as rapid-response units, monitoring social media, collaborating with influencers, and creating adaptable, audience-focused messages.
7.7 A Note on Technological Innovation
Technology and innovation have revolutionized institutional health communication, offering unprecedented tools to expand the reach, relevance, and impact of health messages. These advancements (ranging from Artificial Intelligence (AI) and big data analytics to Virtual Reality (VR) and gamification) are reshaping how health institutions engage with diverse audiences in an increasingly complex communication landscape.
Among the most disruptive developments is the rise of generative AI tools such as ChatGPT, which are transforming how individuals access, process, and interact with health information. These large language models can support institutional communication by answering health-related queries, summarizing complex data, drafting educational content, and even simulating patient–provider interactions (Kahambing, Reference Kahambing2023; Li and Guenier, Reference Li and Guenier2024). More broadly, AI-powered chatbots exemplify how technology can streamline communication, delivering evidence-based responses in real time, whether addressing public concerns during health crises or offering personalized behavioral guidance. Similarly, mobile health (mHealth) apps integrate tailored insights with behavior change strategies, empowering individuals to adopt healthier lifestyles. Wearable technologies, such as fitness trackers and smartwatches, support proactive health management by offering immediate feedback on physical activity, sleep, and other health metrics. Gamification, too, holds significant promise, using interactive and immersive experiences to engage users and enhance health literacy (see, for instance, Tesi et al., Reference Tesi, Donia and Covelli2023).
Emerging technological trends suggest an increasingly personalized and interactive future. Predictive analytics and machine learning enable institutions to anticipate public health trends and intervene proactively. Virtual reality and Augmented Reality are revolutionizing health education and training, from immersive simulations for first responders to virtual health fairs in underserved communities. Blockchain technology promises to improve transparency and trust in data sharing, while telehealth continues to bridge geographic and economic barriers, expanding access to healthcare for remote and vulnerable populations (see, for instance, Attaran, Reference Attaran2022).
Clearly, as these tools evolve, health institutions must invest not only in their adoption but also in ethical frameworks, interdisciplinary governance, and media literacy initiatives to ensure that innovation enhances, and not undermines, public trust and equitable access to reliable health communication. However, the integration of technology into health communication is not without challenges.
First, the application of these innovations must go beyond novelty; their use must be purposeful, evidence-based, and equitable. Without careful planning, there is a risk of perpetuating or exacerbating health inequities. For example, populations with limited access to high-speed internet or digital devices may be excluded from the benefits of digital health initiatives. Bridging the digital divide through investments in affordable technology, digital literacy programs, and infrastructural improvements is critical to ensuring inclusivity. Data privacy and ethical concerns also loom large. AI and predictive analytics often rely on vast amounts of sensitive health data, raising issues of confidentiality and security. Institutions must implement robust data governance frameworks, comply with privacy regulations, and maintain transparency about how data is collected, stored, and utilized. Moreover, algorithmic bias poses a significant risk. Without careful oversight, AI systems may replicate societal inequities, resulting in biased or unfair communication practices that disproportionately impact vulnerable populations. Low-quality information further complicates the digital landscape. Social media algorithms can amplify false information, often outpacing corrections or evidence-based messaging. To counter these dynamics, health institutions must adopt agile and adaptive strategies, such as real-time monitoring, collaboration with trusted community voices, and leveraging AI to detect and debunk misinformation before it spreads.
As mentioned above, AI, including the large language models, holds undeniable potential. Yet these tools do not replace human judgment, knowledge, or ethical reasoning. Messages generated by AI are only as valuable as the expertise guiding them. Without human insight, they risk being generic, inappropriate, or even harmful. The success of any technological intervention in health communication ultimately depends on the minds that shape its use. In moving toward the ethical dimensions of institutional communication, one principle remains fundamental: technology should serve humanity. It must be embedded within human-centered frameworks that prioritize empathy, accountability, and equity. Even the most advanced tools can only enhance, not substitute, the deliberate, reflective, and relational work of responsible health communication (see Table 7).
Key takeaways
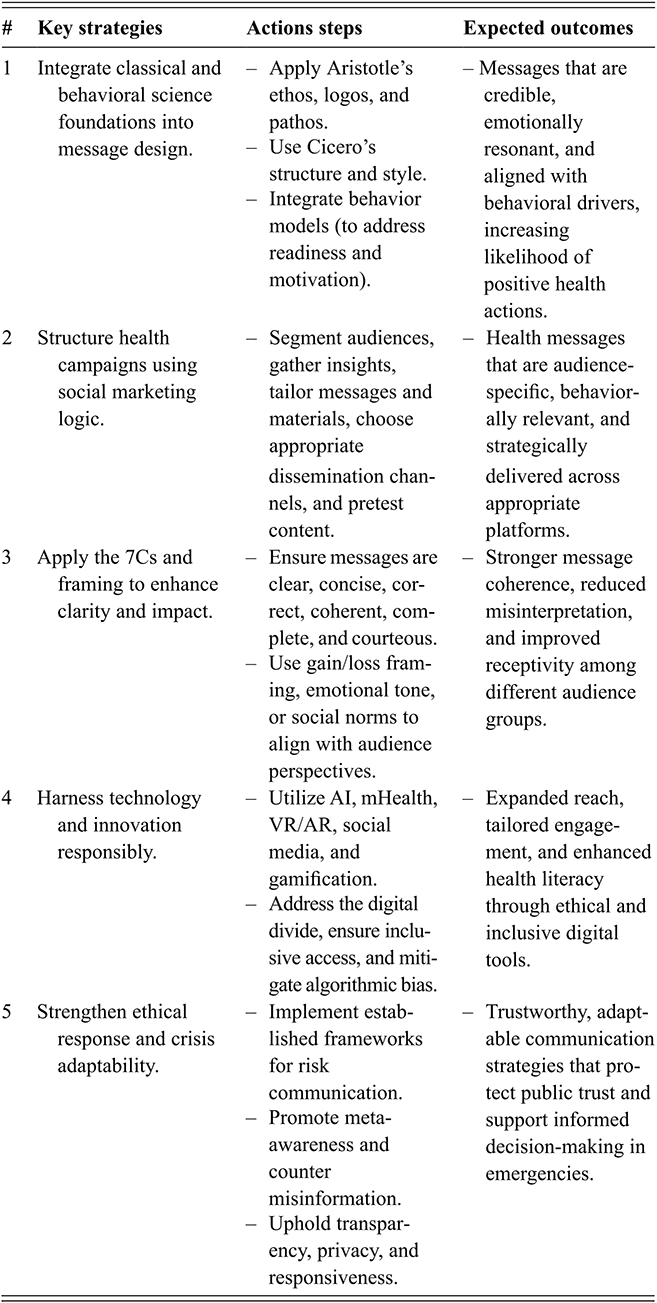
Table 7 Long description
The table outlines five strategies for effective health message design, each with associated action steps and expected outcomes. The first strategy integrates classical rhetoric (ethos, logos, pathos) and behavioural science to create credible and motivating messages. The second applies social marketing principles, including audience segmentation, tailored messaging, and appropriate dissemination channels. The third focuses on clarity and framing through the 7Cs and strategic use of message framing to improve understanding and reception. The fourth highlights the responsible use of technology, including AI and digital tools, while ensuring inclusivity and addressing biases. The fifth emphasizes ethical communication and crisis adaptability through transparency, risk communication frameworks, and responsiveness, supporting trust and informed decision-making.
Concluding Remarks
In the noise and velocity of today’s information age, institutional health communication must be more than functional: it must be human. It must speak not only to the mind but also to the uncertainty, hope, and dignity that shape the human experience of health. This work has outlined the challenges and responsibilities faced by health institutions, offering a vision that is not only grounded in scientific evidence but also in ethical integrity and relational awareness. Health communication is not simply the transmission of facts; it is the delicate art of building trust in a fragmented world, of preserving clarity amid confusion, and of fostering dialogue where division often prevails. The tools used, the voices elevated, the policies supported, and the narratives crafted all contribute to shaping how people come to understand and care for themselves and others.
The hope, and indeed the dream, is that these reflections might serve not only as a guide but as a call: a call for institutions to speak with transparency, for scientists to embrace responsibility in the public sphere, for communicators to engage with expertise and humility, and for communities to be acknowledged as partners, not audiences, in the creation of health meaning. Communication is not an accessory to care. It is already a form of care. In a time when truth is contested and trust is vulnerable, communicating well is not just a strategic choice; it is an ethical imperative.
The solutions are within reach. Many of them are well-articulated, from fostering collaboration between politics and health institutions to strengthening literacy, transparency, and inclusive dialogue. Yet their implementation remains challenging – often hindered not by lack of knowledge, but by fragmented systems, competing agendas, and the complexity of real-world governance. To move from knowing to doing will require courage, patience, and above all, shared commitment.
Funding from Swiss Paraplegic Research made it possible for this book to be published open access, making the digital version freely available for anyone to read and reuse under a Creative Commons license.
Artificial intelligence tools (specifically, OpenAI’s ChatGPT, version GPT-5) were used to assist in improving the clarity, style, and conciseness of the manuscript text. These tools were not employed for data analysis, interpretation of findings, or generation of original scientific content. All ideas, arguments, and conclusions are the author’s own. The author has carefully reviewed and verified all AI-assisted edits and accepts full responsibility for the final content.
Acknowledgments
Aristotle wrote that “Rhetoric may be defined as the faculty of observing in any given case the available means of persuasion” (Rhetoric, Book I, Chapter 2, 1355b). This work has been guided by that understanding: the art of (institutional) health communication lies not only in the accuracy of information but also in the ability to perceive, in each situation, how best to reach and engage others. It is the result of research, reflection, and dialogue, shaped profoundly by the experiences and lessons of the COVID-19 pandemic.
I am deeply grateful to the many individuals whose insights and exchanges have enriched this work. In particular, I thank – in alphabetical order – Jerome Bickenbach, Stefan Boes, Mirjam Brach, Shelly Chadai, Louise Cummings, Nicola Diviani, Frans van Eemeren, Maddalena Fiordelli, Clara Hafliger, Luca Jelmoni, Johannes Kinast, Kent Nakamoto, Enxhi Qama, Gabriela Scherer, Peter Schulz, Gerold Stucki, Claudia Zanini, and the two anonymous reviewers whose constructive feedback helped enhance the clarity and depth of the final text.
I am sincerely grateful to the Faculty of Health Sciences and Medicine at the University of Lucerne and to Swiss Paraplegic Research for their institutional support and for providing the academic environment that made this work possible. I warmly acknowledge the support of the Swiss National Science Foundation for funding the project Developing Standards for Institutional Health Communication During Public Health Emergencies (Grant No. 196736), which provided a strong foundation for this work, and of the World Health Organization for the opportunity to contribute to the development of the competency framework for infodemic management under the lead of Tina Purnat. Finally, I wish to thank the International Association for Communication in Healthcare (EACH), which I had the privilege of serving as president, and my colleagues on the Nature Medicine Commission on Quality Health Information for All, for their continued commitment to advancing the field.
Louise Cummings
York St John University
Louise Cummings is Visiting Professor at York St John University in the UK. She conducts research in pragmatics, clinical linguistics, communication disorders and health communication. She is the author and editor of over 20 books, including most recently the Oxford Handbook of Communication Disorders in Neurodegenerative Diseases (2026), the Handbook of Pragmatic Language Disorders (Springer, 2021), and Language in Dementia (Cambridge University Press, 2020). Prof. Cummings is editor of the book series Routledge Research in Speech-Language Pathology and Cambridge Elements in Health Communication. She is a member of the Royal College of Speech and Language Therapists in the UK.
About the Series
This series brings together a wide range of disciplines that converge on the study of communication in health settings. Each element examines a key topic in health communication and is carefully crafted by experts in their respective disciplines. The series is relevant to students, researchers, and practitioners in humanities, medical and health professions, and social scientific disciplines.
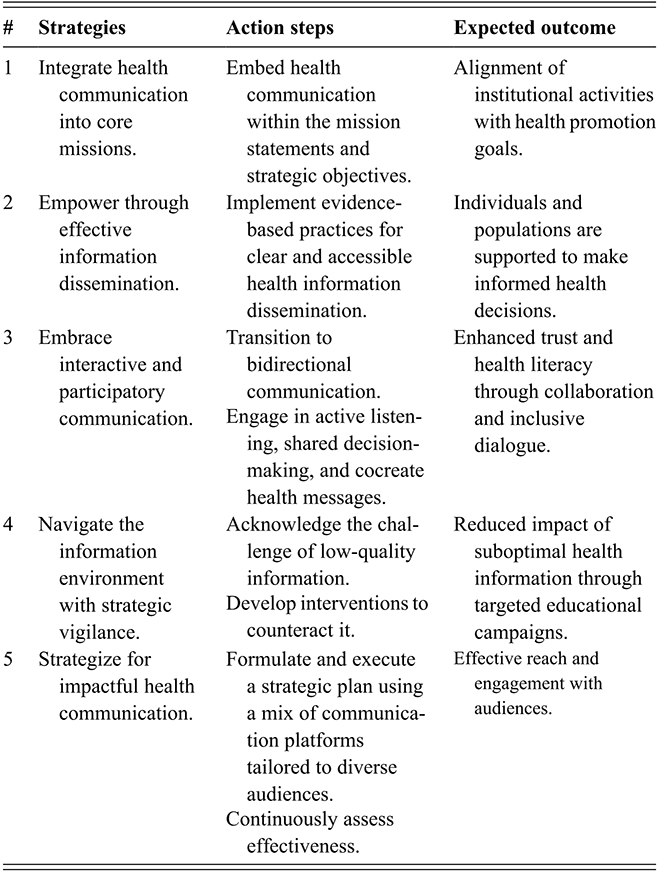
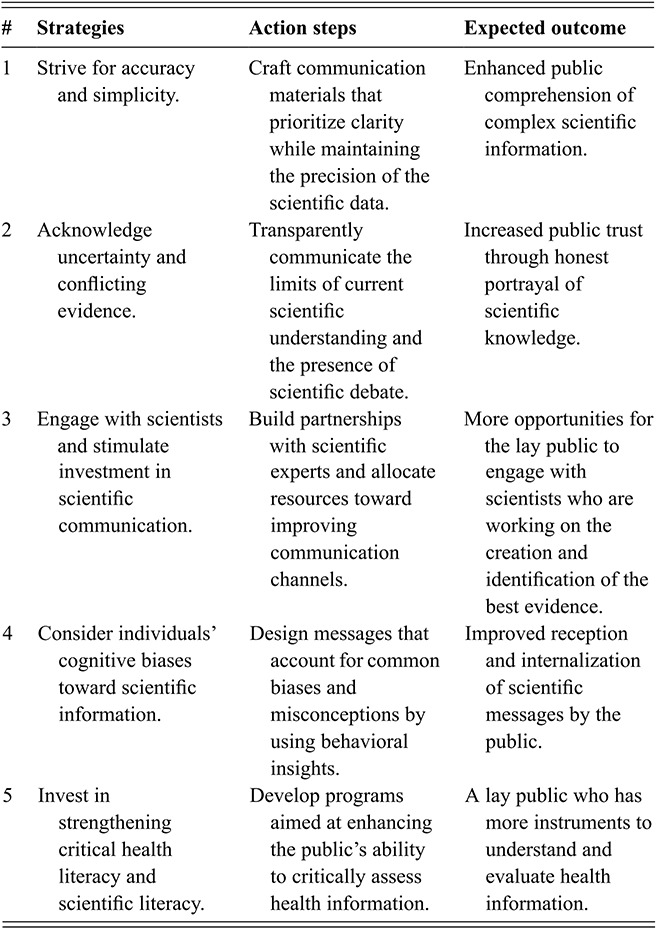
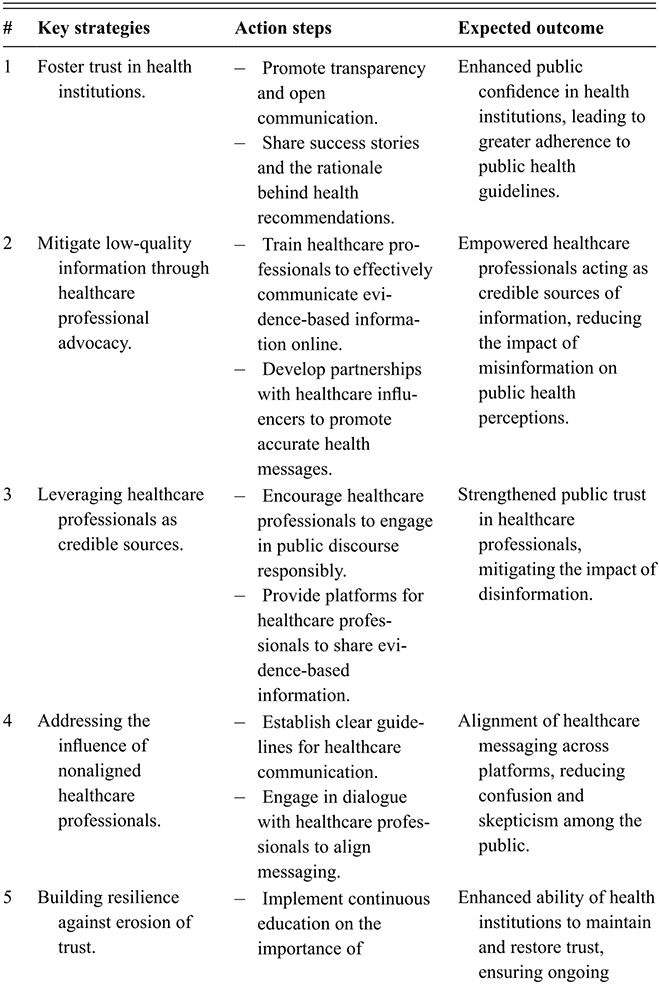
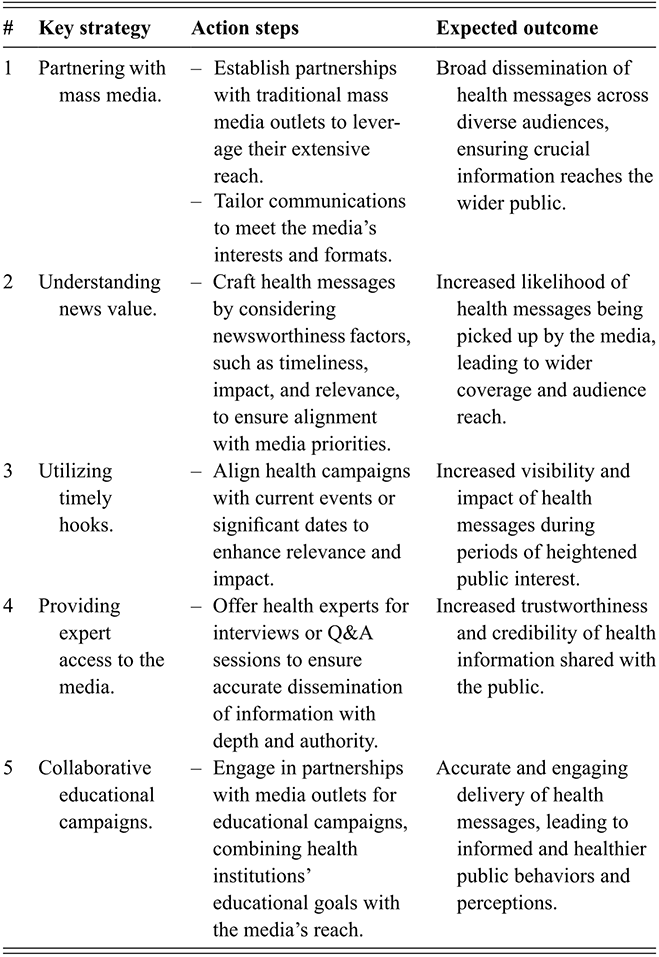
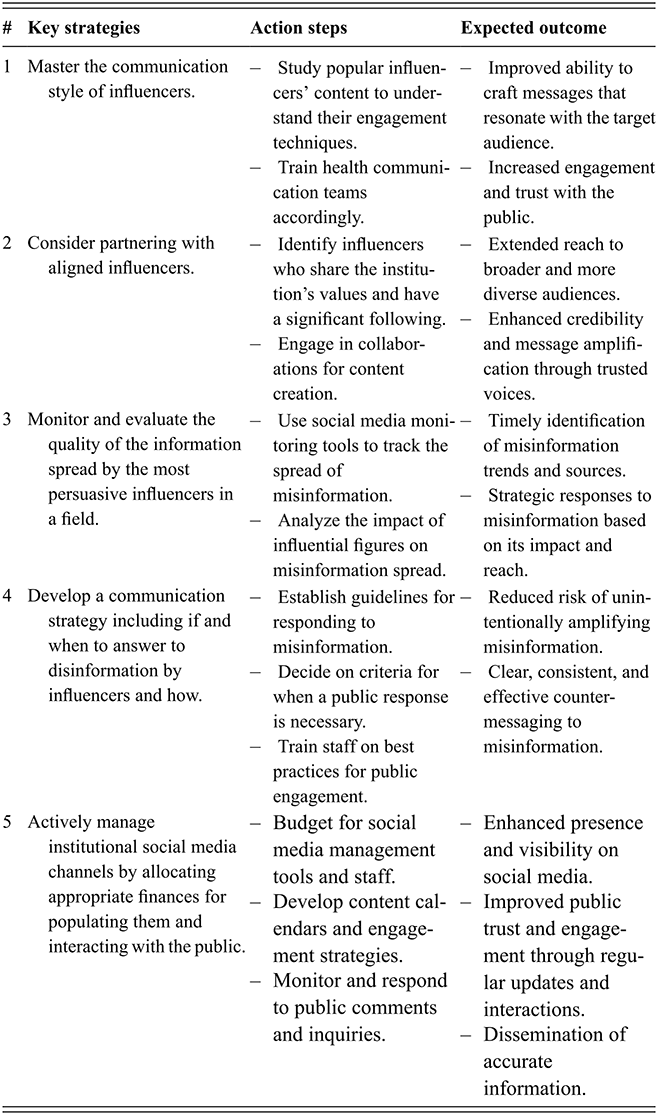
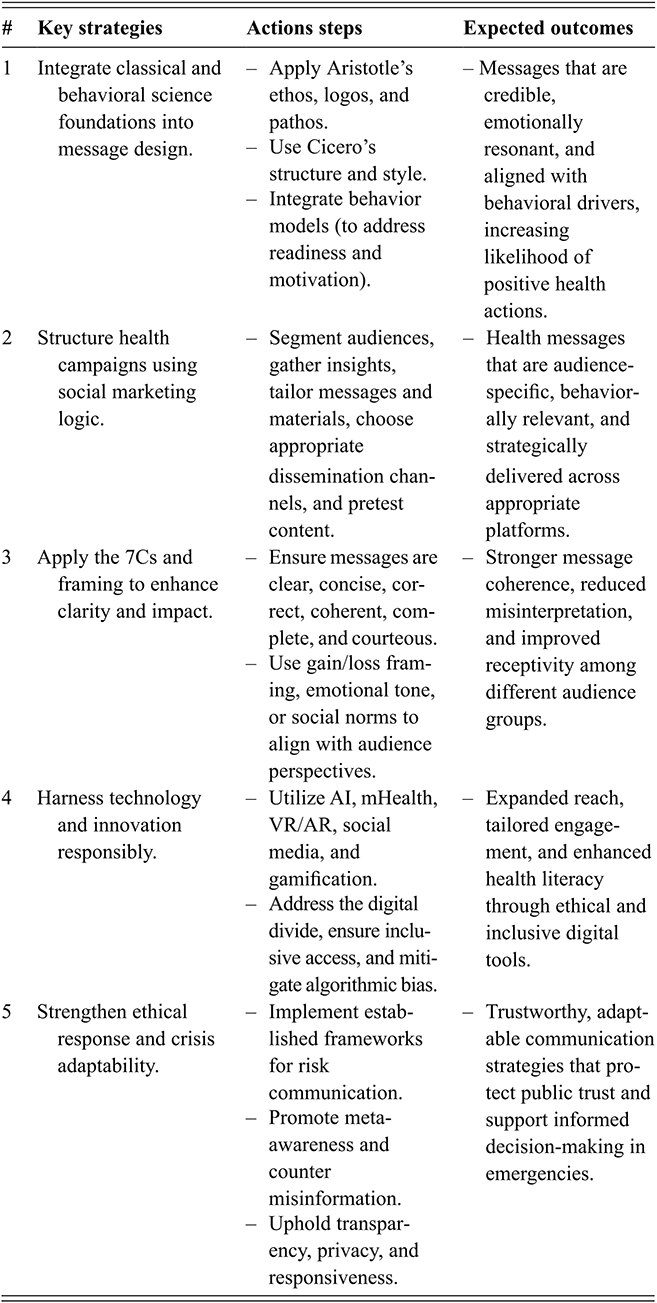

 Open access
Open access