

Context: the IDeA-CTR and community engagement and outreach cores
The National Institute of General Medical Sciences (NIGMS) established the Institutional Development Award (IDeA) in 1993 as a Congressional Mandate to broaden the distribution of National Institutes of Health (NIH) funding for biomedical and behavioral research in states that historically receive limited NIH funding [Reference Gorospé1,2]. The IDeA Program includes the IDeA Clinical and Translational Research Program (IDeA-CTR), which focuses on enhancing and strengthening research infrastructure and human resources to advance clinical and translational research (CTR) that responds to the needs of medically and geographically under-resourced communities [2]. Advancing CTR to address population health challenges requires strong collaboration and partnership between researchers and community members, anchored in trust and engagement [Reference Chinekezi, Andress and Agonafer3–Reference Allen, Frankel and Watanabe-Galloway5]. Consequently, Community Engagement and Outreach (CEO) Cores are mandated as part of the infrastructure within each funded IDeA-CTR program [6].
CEO Cores support multi-directional engagement, partnership, and reciprocity between CTR and community members by integrating communities throughout the research process. Through these efforts, CEO Cores ensure community priorities and health concerns are prioritized and community perspective and lived experiences are honored. To foster and sustain meaningful collaboration and research partnership, CEO Cores develop and implement capacity-building initiatives and activities that empower communities to engage and collaborate with IDeA-CTR investigators on community-engaged research (CEnR) initiatives. CEnR readiness, for both community members and researchers, requires individual competencies (e.g., knowledge, skills, frameworks, and leadership), organizational infrastructure (e.g., culture, policies, incentives, and governance), and societal support (e.g., collaboration across organizations and sectors) [7–Reference Rodriguez Espinosa, Patel and Gay9]. Building individual, organizational, and societal capacity ultimately strengthens CEnR impact by enhancing the ability of community partners and researchers to co-develop, plan, implement, evaluate, and disseminate research that improves health outcomes and informs real-world practice [6,Reference Finn, Gilmore, Sheaf and Vallieres8].
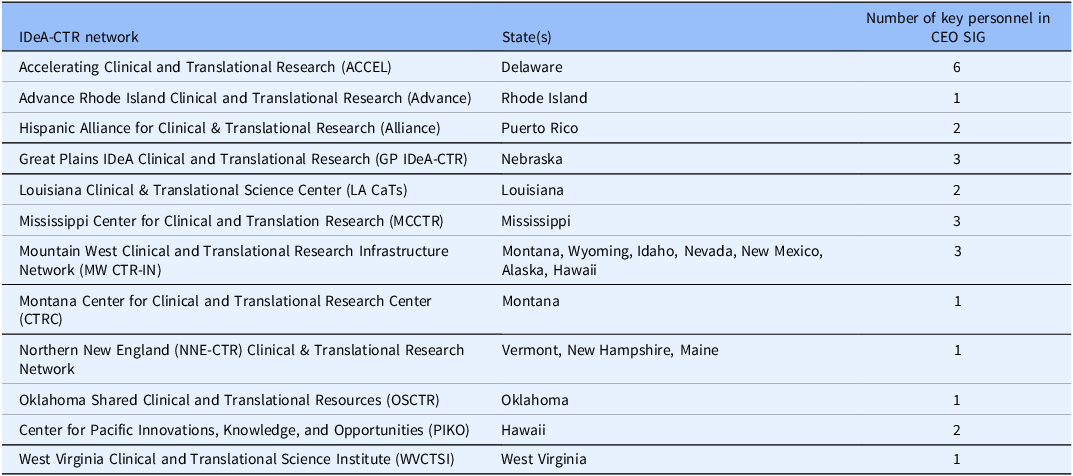
In an effort to strengthen the impact of IDeA-CTR CEO Cores, a CEO Special Interest Group (SIG) was established in September 2022 to facilitate cross-CTR learning, collaboration, and the advancement of CEnR. The CEO SIG is comprised of 26 CEO Core Directors, Co-Directors, and staff, representing 12 IDeA-CTR networks (Table 1). The CEO SIG serves as a community of practice to promote knowledge sharing and peer learning, networking, relationship building, and dissemination of best practices to achieve the overall goals of the CEO Cores. While the guiding principles and CEO Core directives remain constant across the IDeA-CTR networks, the individual Cores often achieve these goals through a range of community engagement (CE) activities. In this paper, we summarize the heterogeneity in CEO Core capacity-building activities across IDeA-CTR programs. Additionally, we highlight innovative initiatives through which CEO Cores tailor programming to meet the unique needs of their community members and CTR investigators, while also identifying gaps where activities could be enhanced to generate greater impact.
Participating IDeA-CTR networks in the CEO SIG

IDeA = institutional development award; CTR = clinical and translational research; CEO = community engagement and outreach; SIG = special interest group.
Approach: landscape analysis of capacity-building activities
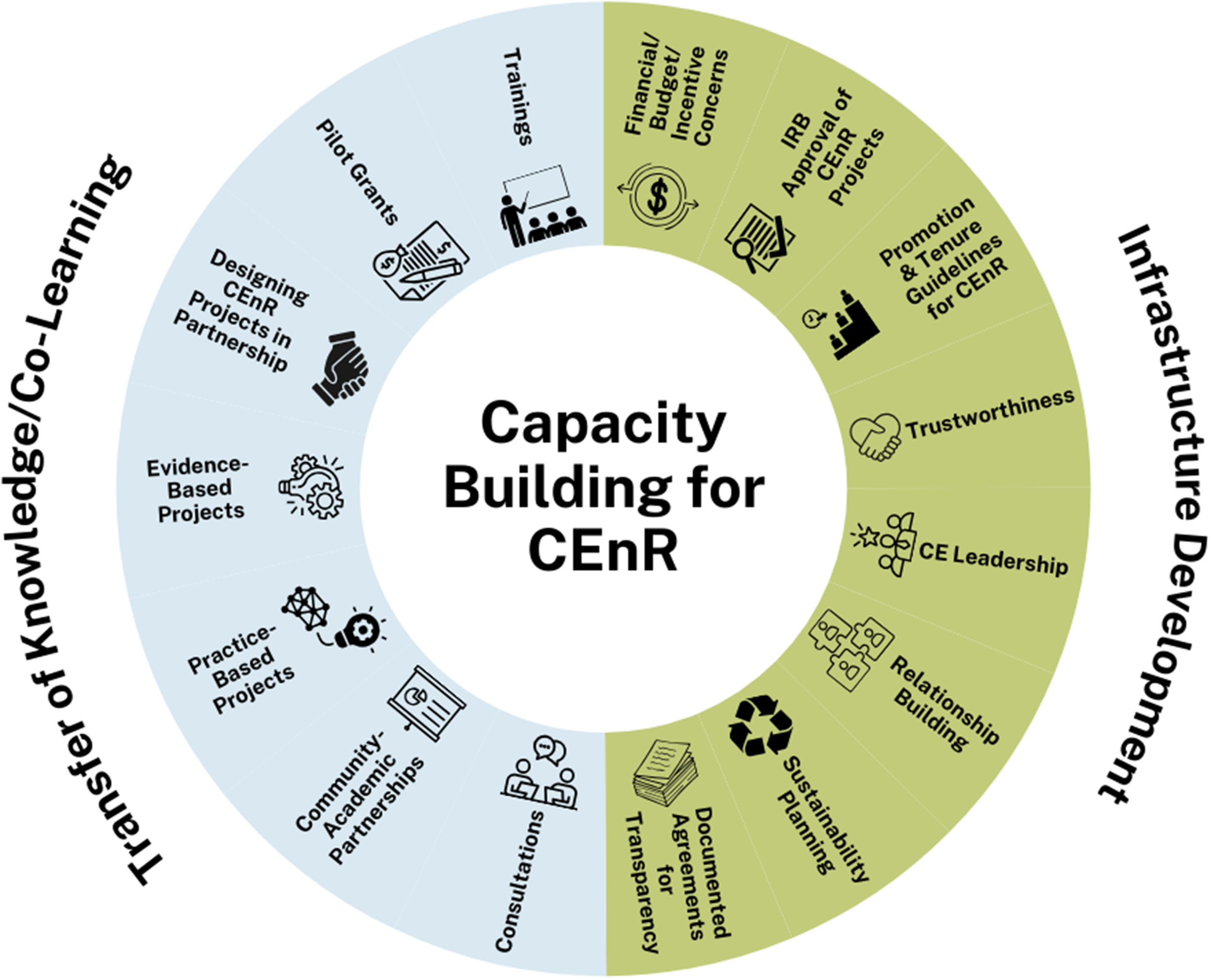
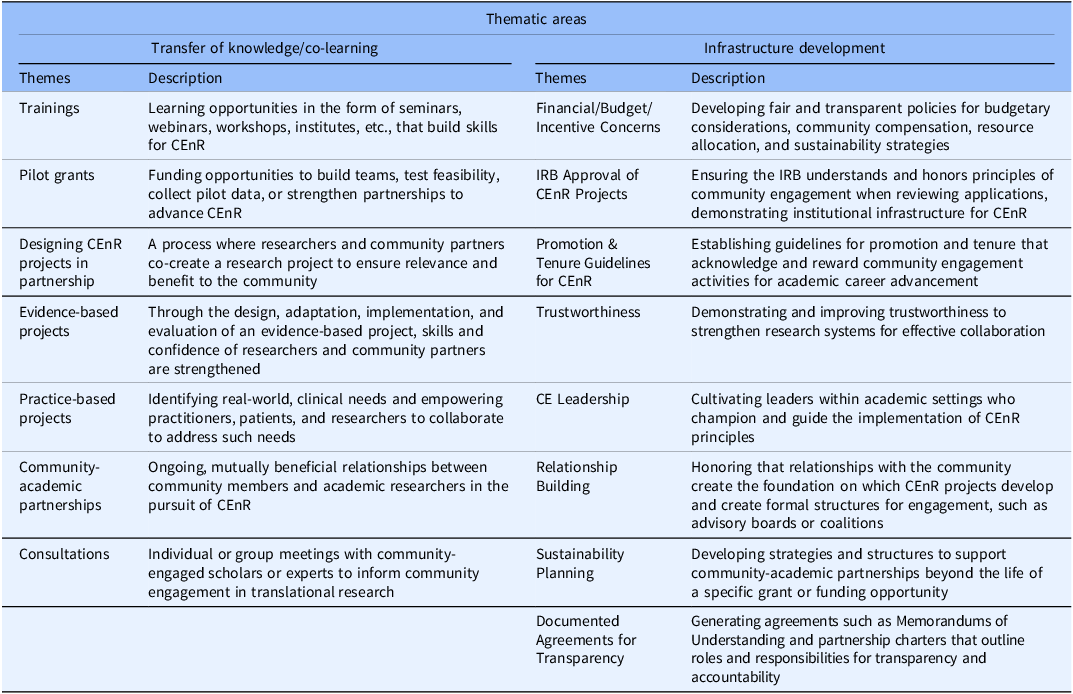
Since September 2022, the CEO SIG has convened quarterly through teleconference meetings. During early meetings, members of the CEO SIG identified a need to conduct a landscape analysis to characterize and systematically document the range of capacity-building initiatives occurring within CEO Cores. Capacity-building activities are those that strengthen skills, systems, structures, and relationships to effectively achieve goals [Reference Smith, Tang and Nutbeam10]. Capacity building is intended to generate change at various levels of the ecosystem through resource allocation and distribution [Reference Ramanadhan, Mahtani and Kirk11]. To initiate the landscape analysis, a data collection tool was developed and circulated to all CEO Cores in October 2023, collecting the following information for each capacity-building activity: (1) Context, (2) Time, (3) Location, (4) Platform (in-person/virtual), (5) Number of participants, (6) Participant demographics, (7) Curriculum/content, (8) Focus/area of emphasis, and (9) Partnerships/collaborators. Concurrently, a deductive approach was used to establish preliminary codes from a comprehensive literature review to identify the essential capacity-building elements in CEnR [Reference Q.12]. Between November 2023 and April 2024, the CEO SIG used meetings to facilitate data collection through iterative facilitated discussions and reviewed capacity-building elements identified in the literature. A classification scheme was then developed according to the themes that emerged from the literature, which were evaluated and adapted to ensure alignment with CE and CEnR principles. The classification scheme included two broad domains: (1) Transfer of Knowledge/Co-Learning and (2) Infrastructure Development [7,Reference Smith, Tang and Nutbeam10,Reference Cole13–Reference Hacker, Tendulkar and Rideout18]. The list of themes, including brief descriptions, was presented to the CEO SIG to confirm face validity and achieve consensus, ensuring clarity and agreement on the thematic framework (Figure 1 and Table 2).
Capacity-building activities for CEnR. CEnR = community-engaged research; IRB = institutional review board; CE = community engagement.

Figure 1. Long description
This circular infographic is divided into two domains; Transfer of Knowledge/Co-Learning and Infrastructure Development. The Transfer of Knowledge/Co-Learning domain is further divided into 7 themes: 1. trainings, 2. pilot grants, 3. designing CEnR projects in partnership, 4. evidence-based projects, 5. practice-based projects, 6. community-academic partnerships, and 7. consultations. The Infrastructure Development domain is further divided into 8 themes: 1. financial/budget/incentive concerns, 2. IRB approval for CEnR project, 3. promotion and tenure guidelines for CEnR, 4. trustworthiness, 5. CE leadership, 6. relationship building, 7. sustainability planning, and 8. documented agreements for transparency.
CEnR capacity-building domains, themes, and their descriptions

CEnR = Community-Engaged Research; IRB = Institutional Review Board; CE = Community Engagement.
Six of the 26 CEO SIG members formed a project analysis group, meeting monthly from April 2024 and December 2024, to translate the CEO SIG’s ideas and discussions into documented projects and deliverables, ensuring structured progress and clear communication outcomes. The project analysis group used a team-based coding approach to systemically aggregate and classify the reported capacity-building activities within the a priori themes presented in Table 2. If the capacity-building activity did not align with one of the a priori themes, it was assigned to one of two new themes, “Knowledge Transfer: Other” or “Infrastructure: Other.” Each activity could be assigned to more than one capacity-building domain and theme. The thematic classifications were returned to the broader CEO SIG to ensure validity and accuracy.
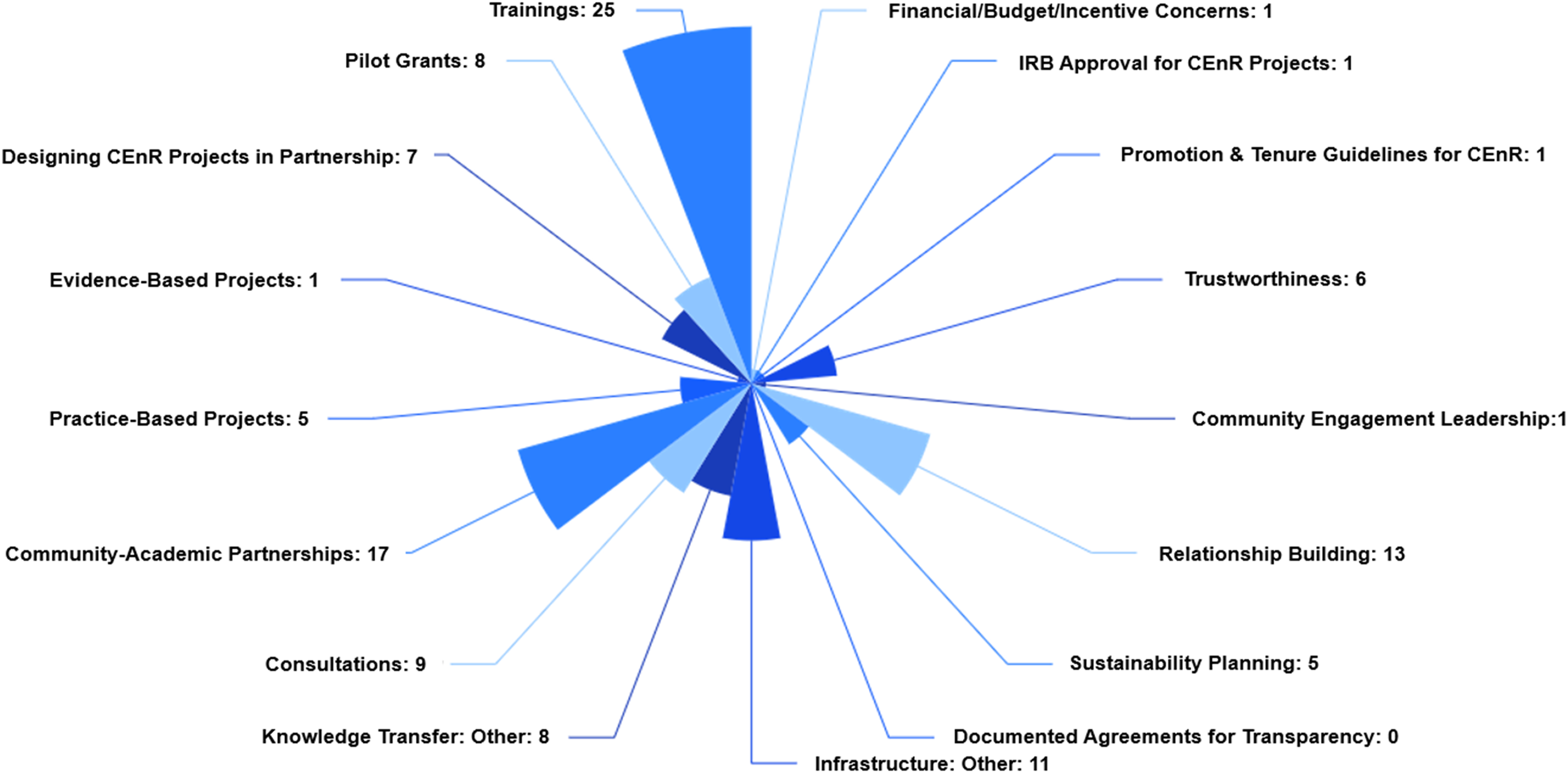
The project analysis group integrated the data collection tool and thematic classification into a single deliverable (Appendix A), organizing activities by (1) Activity name, (2) Capacity-building theme(s), (3) Audience, and (4) Objectives. Descriptive statistics were used to summarize activities across the a priori themes. Since activities could be assigned to more than one capacity-building theme, the sum of percentages exceeded 100%. A Nightingale Rose Chart was generated using the web platform, Agents for Data, to illustrate categorical variation and the magnitude of activities corresponding to the capacity-building themes (Figure 2).
Nightingale Rose Chart of frequency of capacity-building activities. Activities included trainings (n = 25), pilot grants (n = 8), designing community-engaged research (CEnR) projects in partnership (n = 7), evidence-based projects (n = 1), practice-based projects (n = 5), community-academic partnerships (n = 17), consultations (n = 9), knowledge transfer: other (n = 8), financial/budget/incentive concerns (n = 1), institutional review board (IRB) approval for CEnR projects (n = 1), promotion and tenure guidelines for CEnR (n = 1), trustworthiness (n = 6), community engagement leadership (n = 1), relationship building (n = 13), sustainability planning (n = 5), documented agreements for transparency (n = 0), and infrastructure: other (n = 11).

Findings: summary of capacity-building activities
Domains and themes
An analysis of the literature on capacity-building elements for CEnR yielded several themes that were grouped into two thematic areas: (1) Transfer of Knowledge/Co-Learning and (2) Infrastructure Development [7,Reference Smith, Tang and Nutbeam10,Reference Cole13–Reference Hacker, Tendulkar and Rideout18]. Within the thematic area of Transfer of Knowledge/Co-Learning, the following themes emerged: (1) Trainings, (2) Pilot grants, (3) Designing CEnR projects in partnership, (4) Evidence-based projects, (5) Practice-based projects, (6) Community-academic partnerships, and (7) Consultations, reflecting how knowledge is shared and applied. Infrastructure Development was characterized by the following themes: (1) Financial/budget/incentive concerns, (2) IRB approval for CEnR projects, (3) Promotion and tenure (P&T) guidelines for CEnR, (4) Trustworthiness, (5) Community engagement leadership, (6) Relationship building, (7) Sustainability planning, and (8) Documented agreements for transparency, highlighting systems and resources to support CEnR.
Capacity-building themes
A total of 64 unique capacity-building activities were offered across the 12 IDeA-CTR networks. Many activities (N = 25) spanned multiple capacity-building themes, some of which (N = 15) were dually classified as Transfer of Knowledge/Co-Learning and Infrastructure Development, accounting for a total of 119 thematic classifications. Transfer of Knowledge/Co-Learning activities were most frequently reported (N = 80, 67.2%). Trainings (N = 25, 31.3%) and community-academic partnerships (N = 17, 21.3%) emerged as the most common Transfer of Knowledge/Co-Learning activities, demonstrating a priority for strengthening practical skills and promoting cross-sector partnerships. Fewer Transfer of Knowledge/Co-Learning activities focused on research projects, such as practice-based projects (N = 5, 6.3%) and evidence-based projects (N = 1, 1.3%), demonstrating an emphasis on strengthening foundational capacity necessary to support and sustain CEnR projects and engagement (Figure 2). Infrastructure Development activities were less frequently reported (N = 39, 32.8%), with relationship building occurring at the greatest frequency (N = 13, 33.3%). The emphasis on relationship-building activities underscores the importance of collaboration and partnership in CEnR. In contrast, systems-level and organizational infrastructure, financial/budget/incentive concerns (N = 1, 2.6%), IRB approval for CEnR projects (N = 1, 2.6%), P&T guidelines for CEnR (N = 1, 2.6%), community engagement leadership (N = 1, 2.6%), and documented agreements for transparency (N = 0, 0%), were reported less often (Figure 2).
Audience
Across the CEO Core activities, capacity-building activities reached a broad representation of key partners, including junior and senior investigators, community members, clinicians, public health professionals, students and trainees, patients, community engagement leadership, and staff. Most activities were geared towards diverse audiences, representing two or more key partner groups (N = 43, 67.2%). A majority of activities incorporated community members and patients as key audience members (N = 47, 73.4%).
Objectives
The objectives of capacity-building activities ranged in breadth and depth. Some activities had specific objectives (e.g., administer community-engaged pilot awards, build a customer relationship management database, and establish community-driven health priorities), while other activities had broad objectives (e.g., training on CEnR, provide support for CEnR, build relationships, and mentoring). The majority of objectives were oriented towards building individual capacity (N = 43, 67.2%), while some focused on societal capacity (N = 19, 29.7%), and few addressed organizational capacity (N = 2, 3.1%).
Implications: strengths, innovations, and opportunities for growth
This landscape analysis of CEO Core capacity-building activities assessed the range of activities implemented across IDeA-CTR networks. Findings from this analysis revealed heterogeneity in activity scope, intended audience, and objectives. While CEO Cores share a common goal to develop and implement capacity-building initiatives to advance CEnR, approaches vary in their focus, delivery method, duration, target audience, and intended outcomes. The range of capacity-building activities reflects the flexibility of the IDeA-CTR program to tailor activities to each networks’ unique communities, partner needs and priorities, network resources, available infrastructure, and existing societal capacity.
The majority of capacity-building activities focused on individual capacity through trainings, emphasizing the networks’ shared commitment to enhancing research skills, and fostering collaborative learning. Activities such as West Virginia’s ECHOs and design studios, Northern New England’s Boot Camp Translation Training, and Hawaii’s Institute showcase novel training platforms that increase knowledge, build confidence, and enhance peer support. A similar emphasis on trainings have been observed in prior literature examining capacity development, emphasizing the necessity and importance of knowledge and skills acquisition to effectively conduct meaningful CEnR [7,Reference Cole13,17,Reference Doshmangir, Mostafavi and Behzadifar19]. Individual capacity is essential for building competence to effectively engage in CEnR, often resulting in increased trust, research literacy, and mutual understanding [7,Reference Hacker, Tendulkar and Rideout18,Reference Simmons, Reynolds and Swinburn20,Reference Strekalova, Kornetti and Wang21].
Other frequently reported capacity-building activities emphasized enabling community-academic partnerships and relationship building. Both activities encompass individual, organizational, and societal capacity, serving as the linkage between all three layers. At the individual level, community-academic partnerships and relationship building are rooted in trust, enhance communication, strengthen cultural humility, and require shared decision making [7,Reference Hacker, Tendulkar and Rideout18,Reference Simmons, Reynolds and Swinburn20,Reference Strekalova, Kornetti and Wang21]. At the organization level, partnerships and relationships require formalized commitments and agreements between universities, health departments, and community-based organizations with a shared governance structure [Reference Shapiro, Metzger, Jones and Duane22]. Community-academic partnerships and relationships are generally cross-sector in nature and aim to address multi-faceted community priorities, demonstrating societal-level partnership capacity [Reference Khatib, Shah, Mendhe, Whisner and Buman23,24]. In the scope of CTR, these partnerships and relationships are often derived from Practice-Based Research Networks (Rhode Island, Montana, Mountain West region, Hawaii, and Oklahoma), Community Advisory Boards (Delaware, Rhode Island, Nebraska, Northern New England, Hawaii, and West Virgina), and partnership programs (Delaware, Puerto Rico, Nebraska, Mountain West region, and West Virgina).
Innovative capacity-building activities unique to CEO Cores emerged, demonstrating flexibility, responsiveness, and commitment to addressing community-identified priorities. Of note, Delaware’s Junior Investigator Network (JIN) focuses on CEnR mentorship and training for early-career investigators, who may otherwise face challenges or barriers navigating the research ecosystem. Rhode Island launched a community engagement database, mimicking a customer relations management system to align organizational resources with community needs and activities. Louisiana developed a Community Research for Optimal Wellness Network (CROWN) to close the research loop by disseminating CEnR outputs back to communities of interest. Mississippi developed CEnR e-modules, allowing asynchronous, continuous learning reaching a broad audience. Together, these activities highlight the IDeA-CTR and CEO Cores’ ability to adapt, evolve, and respond to the needs of network and community members.
This landscape analysis also revealed areas of opportunity and growth for CEO Core activities. Across all CEO Cores, there were no activities geared towards agreements for transparency, such as memorandums of understanding, business associate agreements, or other partnership contracts, a critical component of CEnR for defining partnerships, structure, and governance [Reference Shapiro, Metzger, Jones and Duane22]. Only one CEO Core worked with university and CE leadership to address P&T guidelines for CEnR. Nebraska’s CEO Core intentionally convened CE leadership to discuss revisions of P&T guidelines to include CE and CEnR as an “Area of Review for Health Professions and Special Appointments,” to accompany teaching, research, and service. The limited number of capacity-building activities at the organizational level aligns with previous literature, emphasizing the persistent gap in institutional recognition and support of CEnR [Reference Hallmark, Bohn, Hallberg and Croisant25,Reference Carter-Edwards, Grewe and Fair26].
To increase sustainable, impactful CEnR, there must be a concerted effort to enhance organizational capacity [Reference Hacker, Tendulkar and Rideout18]. We can leverage proven models for adaptation and implementation, such as Cedars-Sinai Cancer Center’s Certificate in Community Outreach and Engagement Training Program, which standardizes education and learning for early-career staff to enable a skilled workforce [Reference Thompson, Ashing and Barrett27]. The Advancing Research Impact in Society (ARIS) Organizational Research Impact Capacity (ORIC) Program offers another model for increasing organizational capacity by building skills, systems, and processes within an institution to communicate research impact. Through a community of practice, the ARIS ORIC promotes faculty development, research communication, and funding models for sustainability [Reference A.R.I.S.28].
Prior studies have demonstrated how organizational capacity and infrastructure foster sustainability, enhance efficiency, and promote engagement [Reference Finn, Gilmore, Sheaf and Vallieres8,Reference Hacker, Tendulkar and Rideout18,Reference Doshmangir, Mostafavi and Behzadifar19]. Organizational capacity is anchored in structures, policies, and intra-institutional culture, which are essential for aligning individual motivation with societal commitment [7,Reference Cole13,17]. Insufficient organizational capacity renders engagement activities superficial, academic focus hampers sustainable community relationships, and power imbalances diminish community voices, undermining long-term impact and genuine participation [Reference Towfighi, Orechwa and Aragon29,Reference Sanchez-Youngman, Adsul and Gonzales30]. Strengthening organizational capacity would promote and recognize community engagement efforts, reflected in strategic plans, promotion requirements, and internal funding opportunities. Furthermore, organizational capacity would lead to sustainable partnerships and collaborations anchored on shared missions and goals, rather than individual grants or funding opportunities [7,Reference Cole13,17].
While this landscape analysis generated robust insight into CEO Core activities, notable challenges and limitations should be acknowledged. Due to the lack of standardized tracking and evaluation across IDeA-CTR activities, data collection relied on self-reports from members of the CEO SIG who were active participants in the quarterly meetings. This resulted in variable data quality, incomplete data, and inconsistency in reporting. The project analysis group was organized to overcome some of these limitations, but without historical knowledge of each activity, limitations arose. Additionally, due to the composition of IDeA-CTR networks, capacity-building activities may be housed and led by other cores, such as the Professional Development Core, resulting in missing data due to cross-core collaborations. CEO Cores are constantly innovating and implementing new activities, so this landscape analysis provides a snapshot of the activities administered between October 2023 and April 2024. Finally, the IDeA-CTR networks are not on the same funding cycles, leading to subtle nuances in program requirements and expectations. Despite these limitations, this landscape analysis offers valuable insight into the uniqueness of capacity-building activities across CEO Cores and highlights opportunities for growth, enhancement, and collaboration to maximize the impact of activities.
Future work should prioritize standardized reporting, metrics, and evaluation to assess and communicate the reach, effectiveness, outcomes, and sustainability of capacity-building activities across IDeA-CTR networks and the broader CEnR community. Establishing shared metrics will enable comparability and benchmarking across networks, track progress and growth over time, facilitate evidence-based decision-making, promote best practices and shared learning, and aid in identifying gaps in programming that can lead to unmet needs, inefficiencies, and missed opportunities for innovation.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cts.2026.10781.
Acknowledgments
The authors thank members of the CEO SIG, their respective IDeA-CTR Networks, and the communities that drive our mission. The project described is supported by the National Institute of General Medical Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Author contributions
Emily Frankel: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing; Stephanie Broyles: Conceptualization, Data curation, Methodology, Writing – review & editing; Stephenie Kennedy-Rea: Conceptualization, Data curation, Writing – review & editing; Casey Solsrud: Data curation, Visualization, Writing – review & editing; Elizabeth Woods: Data curation, Writing – review & editing; Deborah Goebert: Data curation, Writing – review & editing; Zsolt Nagykaldi: Data curation, Writing – review & editing; Holly Huye: Data curation, Writing – review & editing; Lee M. Pachter: Data curation, Supervision, Writing – review & editing.
Funding statement
The project described is supported by the National Institute of General Medical Sciences, U54 GM115458 which funds the Great Plains IDeA-CTR, U54 GM104940 which funds LA CaTS, U54 GM104942 which funds WVCTSI, U54 GM115516 which funds the NNE CTR, U54 GM138062 which funds PIKO, U54 GM104938 which funds the OSCTR, U54GM115428 which funds MCCTR, and U54 GM104941 which funds ACCEL. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Competing interests
The authors have no conflicts of interest to disclose.



 Open access
Open access