

Introduction and Context
(Academic) Medicine is believed to have gendered structures, as it was formerly a male-dominated discipline, and is still adhering to a mostly male-connoted idea of career and professional success. (Reference Laurence, Gorlich and Simmenroth1–Reference Siller4) Studies conducted in Austria with medical students and staff working in academic medicine have shown that gender discrimination is to the disadvantage of women (Reference Siller5) and power differentials between genders and professions (Reference Siller6; Reference Tsouroufli7) are still noticeable in academic medicine. These facets of and in medicine are increasingly discussed, but progress to a more equal, diverse, and respectful working environment has been slow. Owing to the #metoo movement, sexualized harassment and sexual abuse in general, (Reference Brunner and Partlow-Lefevre8) but also specifically in medicine, (Reference Jagsi9–Reference Zhang12) have attracted public attention. This chapter analyses sexualized harassment and gender discrimination in academic medicine in Austria.
Reflecting on one’s positioning and making these reflections explicit is important in research and has been widely discussed in feminist research. (Reference Harding13–Reference Sweet16) Our socialization as researchers and as former medical students, respectively, and as women shapes the outline of this chapter. Our research interests focus on uncovering neglected and invisible voices in academia and academic medicine and deconstructing power structures, which impede change and a respectful working environment. This focus is guided by an intersectional framework (Reference Moradi and Grzanka17) to dissect power relations contributing to inequalities, silencing, and marginalization. Our intersectional feminist points of view inform critical insider (due to a background as medical doctors, former medical students) but also outsider (due to a background in psychology) perspectives on medical education and academic medicine.
Gender in Society
Austria is a democratic state and member state of the European Union (EU). To date, Austria has a population of about nine million people, with the majority of the population ranging from nineteen to sixty-four years of age. Austria is often described as a conservative welfare state. (Reference Riederer and Berghammer18; Reference Schmidt19) Regarding gender equality, Austria is marked by formally providing equal access and treatment on the one hand, and traditional and conservative role allocation on the other. For example, access to social services and individual health care is granted by law to all citizens irrespective of their gender; however, some gender inequality persists, for example regarding the allocation of power (in terms of political, social, and economic power and decision-making positions to the disadvantage of women) and unpaid labour affecting women disproportionally. Compared to the EU-average of 70.2, Austria has a gender equality index of 71.2 (100 is full equality), but is lower than the EU-average regarding the dimension of power and gender equality in decision making. (20) Such a result means that gender equality has not yet been reached regarding representation in political positions (e.g. parliament, government), economic positions such as corporate boards of large national corporations or social positions in large research funding organisations. However, compared to the EU-average, Austria has a higher percental share of women in such positions, except for board members of the central bank and in decision-making positions of the national Olympic sport organizations. (21) Increasing gender equality was listed as one of Austria’s three main challenges towards achieving the Agenda 2030 SDG (Sustainable Development Goals) targets. (22) Education is an important aspect, and it can be observed that tertiary education levels are increasing for all genders, (23) with more women than men completing tertiary education. (24) Despite this development, overall employment rates (paid labour) consistently have been more than 10% lower in the female population with more than four times as many women being part-time employed. (25) Women are spending almost 4% more time doing labour each day than men, with paid labour accounting for less than half of it, while the same figure for men is a little below three quarters of their time. (26) These factors contribute to a national gender wage gap of 12.2%, ranking above the OECD-average. (27) Working part-time often turns into a long-term arrangement (Reference Riederer and Berghammer18) and appears strongly connected to women with children and childcare responsibilities, (Reference Schmidt19) representing a major form of unpaid labour. Schmidt (Reference Schmidt19) also refers in this context to the creation of an ideal working norm for women with children/childcare responsibilities.
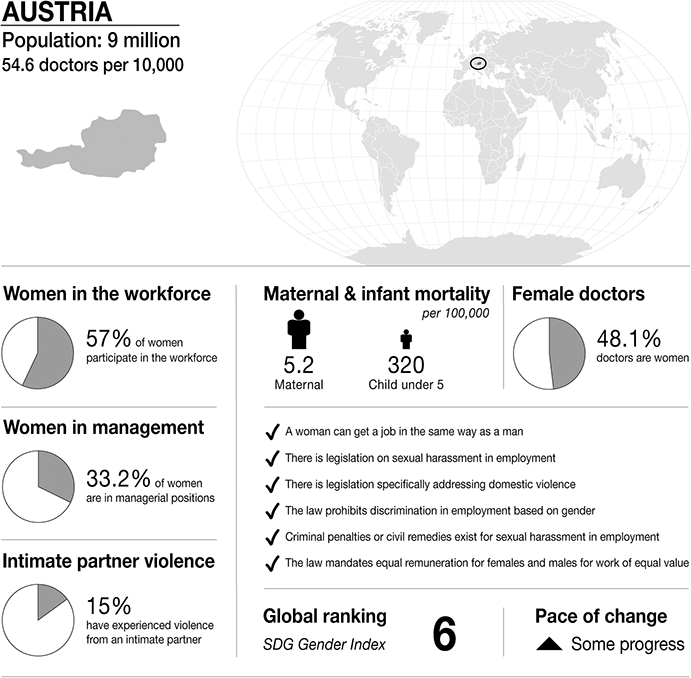
Infographic Austria. Infographics were provided by CartoGIS Services, The Australian National University. Population: from World Bank https://databank.worldbank.org/source/population-estimates-and-projections. Sustainable Development Progress, global ranking and statistics on women in the workplace, women in management and intimate partner violence: from United Nations SDGs Data Portal https://unstats.un.org/sdgs/dataportal. Female doctor percentage: from Global health workforce statistics www.who.int/data/gho/data/themes/topics/health-workforce. Legislation and law statements: from the World Bank gender data portal 2023 https://genderdata.worldbank.org/en/indicators. Maternal mortality statistics: from the Global Health Observatory 2020 https://mmr2020.srhr.org. Infant mortality statistics: from United Nations International Children’s Fund (UNICEF) https://data.unicef.org/topic/child-survival/under-five-mortality
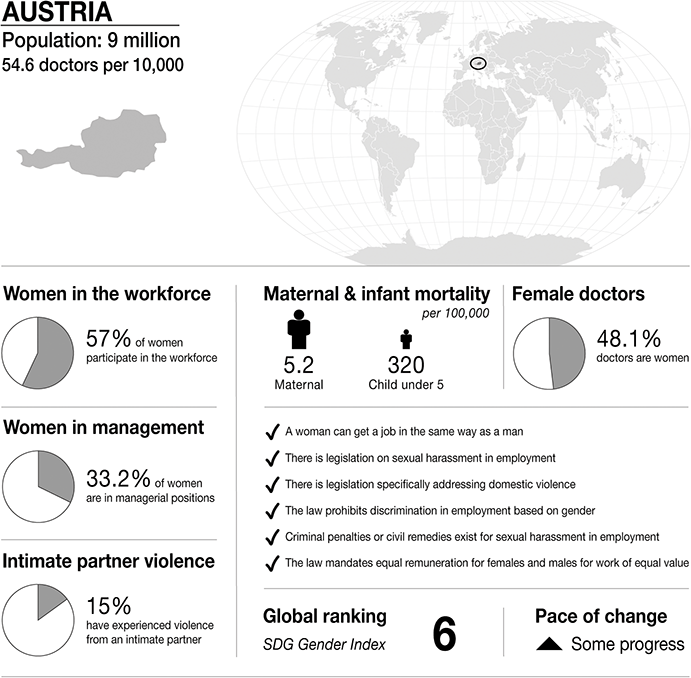
Figure 19.1 Long description
The infographic provides information about Austria, with a population of 9 million and 54.6 doctors per 10,000 people. It highlights several gender-related statistics. 57 per cent of women participate in the workforce. 33.2 per cent of women are in managerial positions. 15 per cent of women have experienced intimate partner violence. Maternal mortality is 5.2 per 100,000. Infant mortality under 5 is 320 per 100,000. 48.1 per cent of doctors are women.
The infographic lists the presence or absence of law and policy on gender equality. In Austria:
– a woman can get a job in the same way as a man.
– there is legislation on sexual harassment in employment.
– there is legislation specifically addressing domestic violence.
– the law prohibits discrimination in employment based on gender.
– criminal penalties or civil remedies exist for sexual harassment in employment.
– the law mandates equal remuneration for females and males for work of equal value.
S D G Gender Index global ranking is 6, and there has been some progress.
Intimate relations and founding a family with children are often marked by traditional gender role allocation. An Austrian study on three cases of differently shared parental leave in heterosexual couples (Reference Schmidt28) showed that negotiating parental leave is father-led, thus focusing on father’s parental leave as a bonus. Simultaneously, masculinity ‘remains hegemonic in being superior to femininity’ (28, p. 382). Pursuing non-normative, more gender-equal, care and parental leave arrangements was also found to be associated with relationship challenges. (Reference Mauerer and Schmidt29) Additionally, some restrictive gender roles are represented in several aspects of everyday life. For example, Kollmayer, Schober and Spiel (Reference Kollmayer, Schober and Spiel30) argue that teachers should be better equipped with knowledge about gender roles and gender bias and should reflect on gender differences in students’ performance and motivation to prevent (unintentional) reinforcement of limiting and restrictive gender roles and gender beliefs.
In the EU-wide study on violence against women, physical and /or sexual violence from a partner or a non-partner was experienced by about 20% of adult women in Austria. Thirty-eight per cent of women reported having experienced psychological violence in adulthood. (31) A more recent survey on gender-based violence in the EU has shown even higher numbers of physical and/or sexual violence by a partner or non-partner: about 35% of adult women in Austria reported these. Additionally, this survey included violence in the workplace and showed that almost 27% of working adult women experienced sexual harassment at work. (32) The numbers indicate that harassment and violence are considered more or less acceptable. But higher numbers of reported violence and harassment also indicate less acceptability of violence and harassment. (33) Austria has several pillars to respond to violence, including legislation, inter-agency collaboration, and non-governmental and governmental actors. The second GREVIO report on addressing violence against women in Austria has shown that Austria has made progress regarding improved legislation to prevent and respond to violence, increased funding of activities and interventions, training of specific professional groups (e.g. medical doctors) and creating specialized counselling services throughout Austria. Further recommendations target, for example, long-term action plans and evaluation. (34)
Gender in Medicine
Overall, the medical profession attracts women in increasing numbers. Currently, more women than men study medicine in Austria. (35; 36) However, change in gender composition in medical personnel is not true for all qualification levels and ranks in academic medicine. Despite quotas, which are implemented in national legislation and at EU-level, affirmative action plans and monitoring committees in hiring processes, gender gaps persistent in higher ranks. The gender gap in high-ranking positions in medicine is discussed with reference to parenthood, lack of (female) role models and the need to improve working conditions towards a better work-life balance and more individualized career paths. (Reference Steiner-Hofbauer and Holzinger37) Currently, women are (and expect to continue to be) underrepresented in higher ranks and in specialist careers (Reference Kuhlmann38) despite the increasing numbers of female medical doctors.
Structures of academic medicine are embedded in historical, cultural, social, and gendered contexts and processes. These contexts and processes intersect. In Austria, academic medicine is described as having gendered structures that also determine different career outcomes to the disadvantage of women. In this context power was mostly ascribed to and accumulated by men. (Reference Siller6) Such a setting enables the accumulation of power over others, but also results in maintaining a system of disadvantaging those perceived as ‘weaker’. Strict hierarchies, decision-making as individual – but not collaborative – responsibility and privilege, non-transparent communication, competition at the cost of collaboration, and mistrust may occur in medicine and strengthen such a system. It can be hypothesized that safe learning environments may counter a transgenerational repetition of a system that disadvantages some over others. (Reference Kumagai, Jackson and Razack39; Reference Torralba, Jose and Byrne40) However, ‘old boys’ clubs’, gendered structures in (academic) medicine and gender stereotypes discriminating against women in advancing in their careers are still noticeable in studies on medicine and medical structures. (Reference Siller6; Reference Komlenac41) Humiliation and harassment of medical students in medical education is also occurring in Austria (Reference Siller4) – a finding which is reflected internationally, as bullying, harassment and discrimination are found in several studies. (Reference Scott42; Reference Averbuch, Eliya and Van Spall43)
Medical Education
Medical education starts with an undergraduate degree with, mostly, twelve semesters (six years at public universities), including internships, and completed by a year of clinical rotations as well as a diploma thesis. Thereafter, postgraduates who want to practise as a medical doctor complete nine months of basic training in different specialties, comprising at least three months in surgery and internal medicine each, followed by several years of specialty training and one or more exams. Whereas the undergraduate programme is anchored at medical universities or medical faculties, practical and postgraduate training may be completed at general hospitals or specialized institutions as defined in the Hospital Act. The contents and requirements of the training are regulated by the Austrian Medical Chamber. (Reference Ärztekammer44)
The considerable duration of training prolongs the time trainees are dependent on evaluations and having to progress in training. According to legislation, a person responsible for training, either a specialist or family practitioner depending on the type of training, oversees progress in training. (45) The perception of being exposed to extensive dependency is also underlined by students’ reports. (Reference Sarcletti and Schäfer46; Reference Kelm47) Additionally, in a study on medical students at the Viennese medical university in Austria, students reported the highest stressor to be performance pressure and self-set standards. (Reference Steiner-Hofbauer and Holzinger37) Another study on medical students in one Austrian teaching hospital has shown that about half of the students were reluctant to speak up when having a concern about patient safety. The authors connected these findings with hierarchical structures in hospitals and low perception of an encouraging environment to speak up. (Reference Schwappach48)
Law
In the context of the workplace, sexual harassment, discrimination based on sex/gender, equal treatment and equal pay are covered by equal treatment legislation. (Reference Thomasberger49) Austria has also introduced legislation to fight violence against women in the private sphere (in 1996) and has signed and ratified the Istanbul Convention Action on violence against women and domestic violence. (50) Sexual rights and gender equality are still marked by ambivalence. For example, conservative parties and groups have also subjected processes of liberation to protests, for example regarding decriminalization of abortion, and marriage and child adoption rights for same-sex couples, as well as gender-inclusive language. (Reference Mayer, Sauer, Kuhar and Paternotte51) Additionally, Thomasberger (Reference Thomasberger49) has summarized that ‘(t)he ratification of the Istanbul Convention did not result in any major changes in the existing legislation’, (49 p.49) which signals that Austria is already equipped with equal treatment and violence prevention legislation, but that there is also opportunity for further improving legislation. Thus, despite strong achievements in legislation and policy on violence prevention, discrimination and harassment, there is still the potential to improve gender equality and violence prevention, particularly regarding, for example, adopting comprehensive approaches or closing gaps and barriers for survivors to receive support. (52)
Sexual harassment and sexual discrimination are subsumed as discrimination based on sex/gender and are regulated in equal treatment acts – thus containing a non-discrimination rule. Sexual harassment and discrimination may also be criminal offences and be covered in the criminal code. (Reference Thomasberger49) Within the academic context, the University Act prescribes that public universities have an equal treatment committee, which monitors discrimination based on gender, sexual orientation, religion/worldview, ‘race’/ethnicity or age. To promote gender equality and equal treatment at universities, additional policies, such as the affirmative action plan for the promotion of women and equal treatment policies, are published in universities’ statutes. (53)
Sexual harassment is one form of discrimination based on gender and is prohibited at the workplace. It encompasses any sexual(ized) behaviour that denigrates a person and is not wanted, is inappropriate or is offensive. (54) If an employee is reporting sexual harassment, the employer has to act. These actions can be manifold but have to prevent further sexual harassment and must not be of disadvantage for the person reporting harassment (see e.g. Gleichbehandlungsanwaltschaft). These legal and regulatory frameworks are only some aspects to counteract sexual(ized) harassment and sexual(ized) violence. Other aspects may include the organizational culture, awareness of the prevalence of sexual harassment, safe spaces to report incidents and a supportive environment for the survivor.
Medical Regulation
As per the Federal Doctors’ Law, the Austrian Medical Chamber has to establish a mediation committee in every state in Austria. The main task of the committee is to solve disputes and to reach agreement between parties. If a disciplinary offence is suspected, the disciplinary council of the Austrian Medical Chamber should be involved. (Reference Ärztekammer55) Disciplinary sanctions range from a written reprimand to being removed from the professional register. (45)
Several councils (e.g. Ethics and Complaints Council; Working Group on Patients’ Safety) are in place to protect patients’ rights and to ensure that medical doctors comply with the doctor’s law and professional code. When medical errors occur, they are treated as an organizational issue, and not as an individual issue. (Reference Ärztekammer56)
Legal regulations, particularly regarding sexual harassment and discrimination, have been discussed in the previous section on law in this chapter.
Case Study
This fictional case study examines the interconnectedness and intersections of sexualized harassment and gender discrimination in academic medicine in Austria. To explore the stages of sexualized harassment and gender discrimination, the case study presented here is fictional, but inspired by studies on power abuse, discrimination, and harassment in academic medicine. (Reference Siller4; Reference Siller6; Reference Sarcletti and Schäfer46; Reference Kelm47; Reference Mayr57).
Sexualized harassment is defined as any sexually related behaviour which impedes a person’s dignity, and which is inappropriate, unwanted or offensive. This definition includes acts as well as sexually connoted inappropriate verbal and non-verbal behaviour. (54) We use the term ‘sexualized harassment’ to emphasize its implication of objectifying a person and misusing sexualities to construct power differentials.
Prelude
Maria studied medicine because she wanted to help others and to interact with people. However, during her medical education she noticed that the profession was also about power displays in the workplace. For example, she experienced the pressure to show an impeccable performance, to compete with others, and to adhere to a strict hierarchy. Additionally, medicine was gendered in terms of women being seen as ‘the others’, whereas men were often displayed as the norm or as an example of how to perform or act. Thus, career paths were mostly presumed to follow a linear path, which was most often associated with men’s career trajectories.
Maria often noticed that sexualized harassment in academic medicine was not seen as acceptable. Nevertheless, she hardly overheard others talking about such incidents; if it happened it was tabooed and hushed.
When Maria was in her final year of medical education, she already knew about strict hierarchies and the requirement to comply with instructions. She knew that as a student and as a medical doctor in training, she would be on the lower end of the food chain. Criticizing and complaining about a senior doctor might come with a cost – she told herself that she would not jeopardize her training spot and be compliant so she could learn and finally practice as a medical doctor in the specialty of her choice. After successfully completing her medical education, Maria found a training spot for her postgraduate basic training at a university hospital including her desired specialty as the final rotation. It was a small team which had a strong and competitive research strand as well as a patient care strand. The senior doctor had vast experience in research and a very good reputation in his field. Maria was happy to learn from him and to be supervised by him.
Assault
After some time, Maria noticed rumours and remarks being spread within her team. The women in her team were more often assigned to patient care, whereas the men spent more time in the lab to conduct research. If one of the female staff spent time in the lab, she heard others muttering about the ‘tyranny of quotas’, that women are better with patients than with cells, and that they would get pregnant anyway. One day, Maria was assigned to go to the lab instead of spending her time at the ward. She shared the lab with two of her colleagues, who were already more advanced in their training than she was. Maria was already nervous about coming to the lab, because of the remarks about women’s (in)ability to do research or pursue a career in research, or comments hypothesizing a sexual affair with the senior doctor, so they (the women) get assigned to the lab.
In the lab she felt her male colleague standing next to her, watching her every move. He looked up and down at her, telling her that he could help her whenever she needed it. Maria felt very uneasy, as the words by themselves sounded harmless, but him standing so very close to her and whispering with a coarse voice left her feeling dirty. When she got home that day, he called her asking if she wanted to get together to celebrate her day in the lab. She declined. The next evening, he called and asked her to meet because he was lonely, and he felt that there was a spark between them. She declined again. After that she got text messages and voice messages saying he missed her or that he was looking forward to meeting her in the lab. At work she felt increasingly tense, dreading to see him again. In the lab he kept his distance, but whenever she looked at him, he smiled and winked at her. Wherever she was, he was there too. The next day, she walked up to him, telling him to stop harassing her. He laughed and asked her if she was so tense because she ‘hadn’t gotten any in quite some time’ and to loosen up. Maria felt unsure if she overreacted. Nobody appeared to have seen or noticed anything as everyone kept working quietly.
Limbo
A few days later, Maria talked to one female colleague in her team, and told her about her interactions with said male colleague. The female colleague shrugged it off and reported that this particular colleague always tries to push the boundaries with the ‘new ones’. She told Maria to forget about it as he was harmless, and it was some kind of rite of passage every woman in this team must go through. She also told Maria that there is not much she could do and that it might also just be a misunderstanding. After talking to her, Maria felt unsure if she should talk to the senior doctor. She did not want to embarrass herself if it was indeed a misunderstanding.
At first Maria tried to let it go, but even after weeks she felt tense at work and startled when her phone rang. She sought out the equal treatment committee at the university. Unfortunately, she had deleted all texts and voice messages, and there were no witnesses in the room with her when he talked to her. The committee took her report and provided her with first steps that could be taken, which included talking to the head of the team, or talking to the accused aggressor.
Exposure
Maria felt unsure if she wanted any actions being taken. At work, everyone appeared to keep a distance from her. She felt that everyone avoided her. One day she overheard how the male colleague told another person that she, Maria, hit on him, and that she was now embarrassed about his rejection. Maria felt increasingly insecure. She told the equal treatment committee that she renounced her accusations and that she did not want any steps being taken. Maria feared retaliation by her male colleague and that this might impact her career opportunities. Her contract was only for a few more weeks so she decided to sit it out.
Aftermath
After her contract ended, Maria sought another training position, which was further away from this hospital. She felt embarrassed and powerless about what happened. After some time, she talked to close friends about it. They encouraged her and told her that it was not her fault. They also named it sexual harassment, but Maria had difficulties accepting it as sexual harassment. It did not fit her assumptions of sexual harassment.
Discussion
Sexualized harassment and discrimination in medicine, particularly if occurring among medical doctors, are known but often concealed phenomena. Within the context of abuse in medicine and between (future) medical doctors, Austria reflects the experiences of many (future) doctors internationally.
Those affected by sexualized harassment are often women and have junior positions, which is also found on an international level. (Reference Vargas11) Abuse may occur in intense and long supervising relations, which may facilitate harassment due to prolonged dependency on others to progress in training. These relations may simultaneously hinder reporting harassment due to fear of retaliation and fear of ineffective sanctions for perpetrators. Similar findings have been reported by a qualitative study on junior medical doctors in Ireland. (Reference Crowe, Clarke and Brugha58) It is learnt behaviour that hierarchies should not be challenged and those in lower positions, such as students or trainees, learn to endure abuse. Studies on medical doctors’ wellbeing and (improving) working conditions are increasing, but due to the scope of this chapter cannot be discussed here.
Our case study shows that sexualized harassment is an expression of power and domination over others. Regarding the Austrian sociocultural context, several levels reinforce power differentials and thus potentially harassment: legislation and regulations (e.g. training regulation) promote prolonged dependency during training and accountability in senior positions, which result in power differentials, hierarchies and potentially unchallenged instructions. At an organizational level, medical students face staff who must balance research, teaching, administration and – particularly in clinical positions – patient care. In this setting, students may learn that their wishes and needs as individuals and students have less priority. (Reference Sarcletti and Schäfer46) Additionally, harassment during medical education and fear of speaking out about it creates a vicious circle of normalizing such harassment and minimizing its effect on individual as well as on structural levels. Low numbers of reporting harassment appear to be connected to lack of safe spaces, dependency during undergraduate and postgraduate training – thus fear of retaliation – learnt compliance and not challenging instructions, little awareness about unacceptable behaviour and uncertainty about definitions of sexual harassment.
At a societal level, Ehalt (Reference Ehalt59) describes that adherence to authority has been replaced by neoliberalism and envy. Additionally, the importance of personal networks in professional lives might also hinder reporting abuse out of fear of being labelled as a whistle-blower and impeding one’s reputation and/or networking opportunities. Therefore, not wanting to attract negative attention has priority. Moreover, conservative gender role allocation in Austria as well as the gendered structures in medicine shape further inequalities for some groups that are assumed to have less power (e.g. minorities, women, persons in junior positions, students).
Others (Reference Moutier60–Reference Moutier63) have focused on the work climate in academic medicine and discussed interventions to increase a culture of respect. These efforts have proven effective in reducing many unprofessional or uncivil behaviours among faculty in academic medicine. (Reference Moutier63) Most interventions to reduce unprofessional behaviour, such as raising awareness, focused on individuals rather than institutional or organizational change. (Reference Tricco64) Additionally, changes in organizational culture, policy and process must occur in a sustainable way.
Sexualized harassment among doctors may be perceived as ‘individual problems’, but it interacts with systemic-organizational, societal, and historical facets. It is embedded in the gendered history and the present of medicine as a profession which may create inequalities. (Reference Siller6; Reference Riska65) The legal context in medicine produces and enables strict hierarchies and dependencies. The social status and prestige connected to the profession might result in a ‘need’ to accumulate power to protect one’s status and to gain control. Consequently, these aspects conceal abuse of power relations. Individual vulnerability aspects are embedded in such systems. Vulnerabilities due to gender or junior status (student or trainee) are reflections of artificially created dependencies and historical reproductions of ‘how things used to be’ regarding status and gender differences. The numerical increase of women in medicine has not changed this yet – and will not change the current systems – because it is not only about a mere numerical increase of women and minorities, but also about changing the culture in medicine. (Reference Leape62; Reference Bynum and Lindeman66; Reference Krugman, Jones and Lowenstein67) However, we should be aware that change occurs slowly and is most often met with resistance, resulting in the persistence of mistreatment. (Reference Fried68) Based on these considerations, the question arises: how can we break out of this vicious cycle and use our agency to help change the system for the better?
To answer this question, several measures are suggested in the current legal and societal context. However, it must be noted that these suggestions are not unique for the Austrian context and similar proposals have also been presented by others (Reference Zhang12; Reference Leape62). Additionally, such interventions to counteract sexualized harassment are not restricted to medicine, but implementation of interventions should consider the hierarchical context in which harassment takes place.
Raising Awareness and Knowledge on Sexualized Harassment
Global awareness raising was also activated by the #metoo movement, which helped spark discussions on sexualized harassment, discrimination, and abuse. (Reference Brunner and Partlow-Lefevre8) The movement can be a basis to build interventions. Every student and all staff should be aware of sexualized harassment, discrimination and abuse, its signs, facets, and its impact and they should know how to counteract it. Obligatory workshops that are offered repeatedly should be tailored so they are relevant and useful for anyone working in academic medicine.
Promoting Collaboration, Connectedness, and Participation
Deconstructing hierarchies is one necessary step to overcome abuse of power and barriers due to dependency and fear of retaliation. These strict hierarchies can be deconstructed by promoting a collaborative working environment with shared decision-making processes. Even though individual accountability in patient care still exists, such individual accountability is not needed in other contexts relating to, for example, teaching, publishing, or doing research. However, this approach is not equated with suspending leadership, but focuses on including all members of the organization in everyday processes.
Uncovering Systems of Abuse
Sexualized harassment, discrimination and abuse thrive in silence and neglect. Publicly demonstrating that sexualized harassment, discrimination, and abuse are serious issues, and that the organization should pursue a zero-tolerance approach, is needed to render this phenomenon visible. Also, others (62; 67; 68) have emphasized the need for visibility and a clear approach to uncovering systems of abuse.
Zero-Tolerance
Visibility should also be reflected in the consequences of sexualized harassment, discrimination, and abuse. Sanctions should be applied without exception. They can be manifold but must focus on the perpetrator and not on the survivor. For example, terminating the perpetrator’s contract or withdrawal of their resources should be chosen over ‘fixing’ the survivor. Additionally, visibility of such actions prevents gossip and misinformation.
Active Support by Contact Points
Committees and contact points that are not bound to directives are essential tools to operate in this field, and should be empowered to ensure action is taken. The head of the organization must be committed and in full support of actions taken. The contact points should also actively provide information on sexualized harassment, discrimination, and abuse, on contact details and on the process if sexualized harassment, discrimination, and abuse are reported. Currently, there are further initiatives on university campuses that focus particularly on sexualized violence.
Conclusion
Although much has already been done, more remains to be done. Sexualized harassment, discrimination, and abuse in medicine, particularly between colleagues, is a known fact few people dare to publicly talk about. Many mechanisms ranging from perceptions of the profession as morally impeccable to fear of retaliation keep the phenomenon hidden. The proposed aspects focus on uncovering abuse and on open management, which are essential for prevention and reduction of sexualized harassment, discrimination, and abuse.

 Open access
Open access