


Introduction
The professional role of paramedics in Germany has undergone major reform since the implementation of the Emergency Paramedic Act (EPA; Notfallsanitätergesetz) in 2014. This legislation replaced the previous Emergency Medical Technician Act and established a modern, three-year vocational training program that expanded the scope of prehospital clinical practice.
Entry into paramedic training in Germany typically requires completion of secondary education and eligibility for vocational training in health care professions. The nationally standardized program lasts three years and combines theoretical instruction at accredited paramedic schools with practical clinical placements and supervised field training within Emergency Medical Services (EMS) agencies. Clinical rotations commonly include placements in emergency departments, anesthesia, and intensive care units to ensure exposure to airway management, vascular access, and emergency pharmacology. Throughout training, students perform a range of practical procedures under clinical supervision and must demonstrate competency in core emergency skills before final certification.
Paramedics were authorized to independently perform defined medical interventions, including invasive and pharmacological procedures, when immediately necessary to prevent life-threatening deterioration and when no physician was available on scene. 1 The reform aimed to enhance the quality, safety, and continuity of prehospital care within the German EMS system.
Internationally, the expansion of non-physician competencies in prehospital emergency medicine has been driven by similar objectives — improving rapid access to life-saving procedures and optimizing resource allocation in systems with limited physician coverage. Reference Bigham, Kennedy, Drennan and Morrison2–Reference O’Hara, Johnson and Siriwardena4 In Anglo-American EMS systems, paramedics have long performed advanced interventions such as tracheal intubation, intraosseous (IO) access, or drug administration under protocol-based authorization. Reference Dyson, Bray, Smith, Bernard, Straney and Finn5,Reference Wang, Kupas, Hostler, Cooney, Yealy and Lave6 By contrast, the German model has historically been physician-led, with the physician present in a substantial proportion of critical missions. The EPA therefore represents a paradigm shift towards a more competence-oriented and decentralized approach.
The legal framework in §2a of the EPA and the accompanying training and examination ordinance defines which competencies must be taught, practiced, and evaluated during training. Furthermore, the Federal Association of Medical Directors of EMS in Germany (Bundesvereinigung der Ärztlichen Leiter Rettungsdienst, BVÄLRD; Friedberg, Germany) developed the so-called “Pyramid Process” as a national framework to structure the delegation and authorization of medical procedures performed by paramedics. The Pyramid Process categorizes prehospital interventions into hierarchical levels according to clinical risk, procedural complexity, and the required level of medical supervision. 7
Although the Pyramid Process itself is a professional recommendation rather than a statutory regulation, it is widely adopted by regional Medical Directors of EMS and implemented through legally binding regional standard operating procedures (SOPs) within the framework of the EPA.
At the base of the Pyramid are low-risk, high-frequency measures that are routinely taught during paramedic training and can be performed independently under SOPs. These include basic airway management (eg, bag-valve-mask ventilation), oxygen administration, peripheral intravenous (IV) access, or administration of selected medications such as crystalloids or bronchodilators.
The intermediate levels of the Pyramid include procedures that carry higher clinical risk or require more advanced training and experience. Examples include supraglottic airway placement, administration of analgesics such as opioids or ketamine, or management of specific emergency conditions such as hypoglycemia or anaphylaxis. These interventions are typically authorized by the regional Medical Director of EMS and regulated through locally adapted SOPs.
At the top of the Pyramid are high-risk and low-frequency interventions that usually require physician involvement or additional authorization. These include procedures such as endotracheal intubation, IO access, or thoracic decompression in life-threatening situations. In these cases, paramedics may perform the intervention independently only when it is immediately necessary to prevent life-threatening deterioration and when no physician is available in time.
The Pyramid Process therefore functions as a governance model that links paramedic education, competency verification, and clinical authorization. Regional Medical Directors of EMS translate the national framework into operational practice by defining local SOPs, specifying which interventions may be performed independently, under telemedical consultation, or only in physician-attended missions. This catalogue forms the reference standard for local Medical Directors who authorize specific measures via SOPs and ensure quality assurance through recurrent certification. The intervention categories analyzed in the present study were mapped to this competency framework to facilitate interpretation of how frequently different levels of the Pyramid Process are applied in routine EMS practice.
Despite this structured system, it remains largely unknown to what extent paramedics apply these competencies in real-world prehospital care. Previous research has mostly focused on training outcomes or simulation performance rather than field implementation. Reference Lauer, Lier and Eich8,Reference Jensen, Croskerry and Travers9 Several studies have highlighted discrepancies between perceived and actual skill application, particularly in advanced airway management or invasive access. Reference Dyson, Bray, Smith, Bernard, Straney and Finn5,Reference Dyson, Bray, Smith, Bernard and Finn10 Moreover, international comparisons suggest that procedural exposure frequency is a key determinant of long-term competence.
Ten years after the legislative reform, a comprehensive evaluation of how often German paramedics perform invasive and pharmacological interventions in the field is still limited. Such data are essential for describing current scope of practice and for guiding training, certification, and system development. The present study therefore provides a descriptive six-year analysis of invasive and medication-based measures performed by paramedics in three EMS districts in Saxony, Germany.
Methods
Study Design and Setting
This study was designed as a retrospective, descriptive, multicenter analysis of prehospital care documentation from three EMS districts in the German federal state of Saxony: Delitzsch, Oschatz, and Torgau. Together, these districts constitute the Northern Saxony administrative region, covering approximately 200,000 inhabitants and an area of 2,029 km2. The region represents a typical mixed urban-rural setting within the German EMS system, with both physician-based response units and paramedic-led ambulance services.
In the German dispatch system, ambulance units staffed by paramedics respond to the majority of emergency calls, while emergency physicians are dispatched selectively based on pre-defined dispatch criteria or clinical suspicion of life-threatening conditions. Dispatch decisions are typically based on nationally recommended indication catalogues used by emergency medical dispatch centers.
Data were extracted from digital EMS protocols recorded from January 1, 2019 through December 31, 2024. All missions documented during this period were screened. Missions were included if a paramedic served as lead provider and no physician was present on scene. Physician-attended missions and non-emergency interfacility transports were excluded.
In the German EMS system, the majority of emergency missions result in transport to hospital. However, paramedics may in selected situations treat patients on scene or document patient refusal of transport according to regional protocols and medical oversight.
Cases were excluded if essential procedural variables (performed interventions, medication/therapeutic administrations, or provider role) were missing or incomplete.
Legal and Organizational Framework
Under §2a of the EPA, paramedics are authorized to perform defined invasive and pharmacological procedures independently when these measures are:
-
• Taught and assessed during formal training;
-
• Mastered with proven competence; and
-
• Immediately necessary to prevent life-threatening deterioration until physician arrival.
Local Medical Directors of EMS in Saxony define detailed SOPs and authorize paramedics for specific procedures based on the Federal Association of Medical Directors of EMS “Pyramid Process” catalogue. Reference Lauer, Lier and Eich8
Many procedures within the lower and intermediate levels of the Pyramid Process are performed autonomously under SOPs without real-time physician involvement.
In addition to protocol-based authorization, paramedics may consult an emergency physician via the dispatch center or telemedical support systems when clinical uncertainty exists or when advanced interventions are considered. The dataset used in this study did not contain structured information on whether telemedical consultation occurred during individual missions.
In accordance with regional SOPs, paramedics may administer epinephrine in specific life-threatening situations such as cardiac arrest or anaphylaxis. These interventions are typically authorized under standing protocols defined by the Medical Director of EMS and may be performed without prior physician consultation when immediate treatment is required.
In most emergency missions within the German EMS system, patients are transported to hospital after on-scene assessment and initial treatment. However, paramedics may in selected situations leave patients at the scene when hospital transport is not required or when a competent patient refuses transport. Such decisions must be carefully documented and are typically regulated through regional protocols and medical oversight. Depending on local regulations, consultation with an emergency physician via dispatch center or telemedical support may be required before a patient is left on scene.
Data Collection and Variables
Data were retrieved from the regional digital patient care documentation system (NIDAS; Rescue Track GmbH, Germany).
Each record contained demographic information, dispatch category, clinical problem, performed procedures, administered medications/therapies, and provider role. Data extraction was performed using pre-defined queries within the NIDAS database. All variables were extracted in a structured and standardized manner.
To ensure data validity and reliability, plausibility checks were conducted, including range checks and consistency verification between related variables. In addition, a subset of records was cross-checked against the original documentation to confirm accuracy of data extraction.
All invasive interventions (eg, peripheral IV access, IO access, airway interventions including supraglottic airway and endotracheal intubation, defibrillation, and thoracic decompression) and pharmacological/therapeutic administrations (eg, crystalloids, analgesics, antiemetics, bronchodilators, glucose, epinephrine, and oxygen therapy) were identified.
Airway interventions included basic airway management (eg, bag-valve-mask ventilation), supraglottic airway devices, and endotracheal intubation. In the studied EMS systems, rapid sequence intubation using neuromuscular blocking agents is typically performed by emergency physicians rather than paramedics. Paramedic-performed endotracheal intubation therefore usually occurred in specific clinical situations, most commonly during cardiopulmonary resuscitation or in deeply unconscious patients without protective airway reflexes. Sedative and neuromuscular blocking agents for rapid sequence intubation were not routinely administered by paramedics in the analyzed EMS districts. The database did not contain detailed information on individual airway medications; therefore, airway management was analyzed at the procedural level.
Each intervention was classified according to the Federal Association of Medical Directors of EMS catalogue (2024 edition) into:
-
• Airway/Breathing interventions;
-
• Circulation/Vascular access procedures; or
-
• Pharmacological and therapeutic administrations.
Frequencies were calculated as absolute numbers and percentages of all paramedic-led missions per year and per district. Rates per 1,000 missions were additionally calculated.
Data Completeness Assessment—Data completeness was systematically assessed for core procedural variables. Completeness exceeded 98.0% for intervention and medication/therapy fields. Missing values were not imputed; analyses were performed using available-case methodology for each variable.
Statistical Analysis
All data were processed and analyzed using Microsoft Excel 2021 (Microsoft Corp.; Redmond, Washington USA) and SPSS Statistics (Version 29.0, IBM Corp.; Armonk, New York USA). Descriptive statistics were used to summarize frequencies and proportions; temporal changes were visualized using trend plots.
Temporal trends (2019-2024) were explored using the non-parametric Mann–Kendall trend test due to low event frequencies and non-normal distributions. Regional differences were explored using one-way ANOVA with Tukey HSD post hoc testing after evaluating assumptions of normality and homogeneity of variance. Effect sizes were reported as Hedges’ g.
All inferential analyses were exploratory and hypothesis-generating. No multivariable regression modelling or subgroup analyses (eg, by age group, diagnosis, or dispatch category) were performed.
Ethics Approval and Consent to Participate
This study was reviewed by the Ethics Committee of the Faculty of Medicine at Philipps University Marburg (Germany; reference number: AZ 26-34 ANZ). The committee determined that formal ethical approval was not required due to the use of fully anonymized secondary data without patient identifiers; therefore, no individual informed consent was required.
Results
Overview of Included Missions
From January 2019 through December 2024, a total of 197,842 missions were documented across the three EMS districts. Of these, 156,417 cases (79.1%; 95% CI, 78.9% - 79.3%) were led by paramedics without direct physician presence and were included in the analysis.
Mean patient age was 64 (SD = 21) years; 52.0% were male and 48.0% were female. The most common dispatch categories were cardiovascular emergencies (27.0%), neurological emergencies (19.0%), respiratory distress (14.0%), and trauma (11.0%).
Frequency of Invasive Interventions
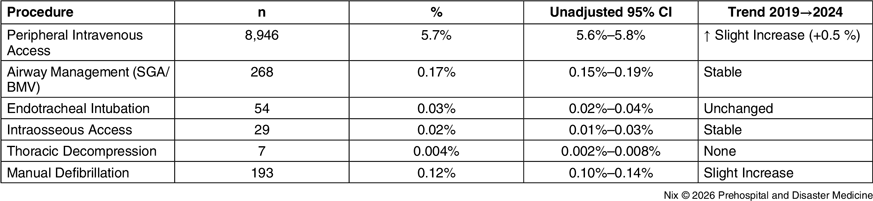
Across all districts, invasive procedures were performed in 11,545 of 156,417 paramedic-led missions (7.6%; 95% CI, 7.5% - 7.7%). The most frequent invasive measure was peripheral IV access (8,946 cases, 5.7%; 95% CI, 5.6% - 5.8%), while advanced airway interventions and IO access were rare (<0.1% of missions; Table 1). Advanced invasive procedures remained uncommon throughout the observation period.
Invasive Procedures Performed by Paramedics (2019-2024)

Abbreviations: SGA, supraglottic airway; BMV, bag-valve-mask ventilation.
Pharmacological and Therapeutic Administrations
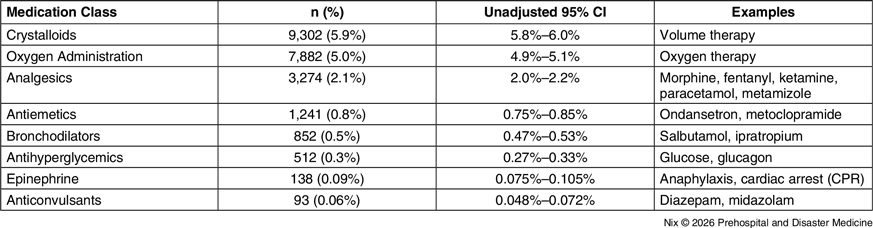
Pharmacological and therapeutic administrations occurred in 17,670 of 156,417 missions (11.3%; 95% CI, 11.1% - 11.5%). The majority involved standard emergency treatments such as crystalloids (5.9%; 95% CI, 5.8% - 6.0%), oxygen administration (5.0%; 95% CI, 4.9% - 5.1%), and analgesics (2.1%; 95% CI, 2.0% - 2.2%); Table 2.
Pharmacological and Therapeutic Administrations (2019-2024)

Abbreviation: CPR, cardiopulmonary resuscitation.
Analgesic therapy in the studied EMS systems typically included opioid analgesics (eg, morphine or fentanyl), ketamine for analgesia and sedation, and non-opioid analgesics such as paracetamol or metamizole, depending on regional protocols.
Epinephrine administrations were rare (0.09%) and typically occurred in resuscitation scenarios or suspected anaphylaxis.
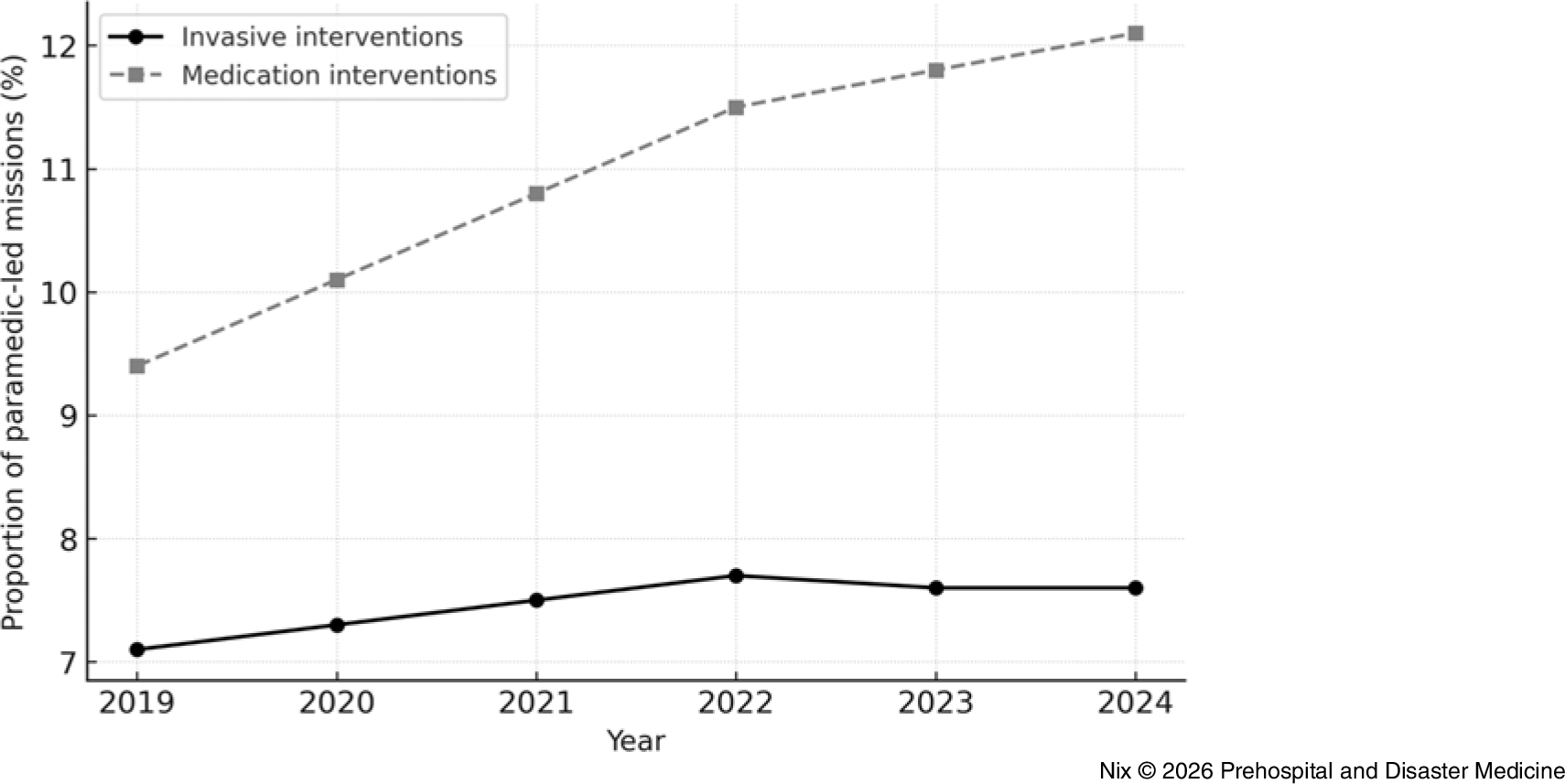
Across all categories, medication administration increased from 9.4% in 2019 to 12.1% in 2024, representing a modest but consistent upward trend.
Regional Comparison
Regional variation was observed (Table 3). Invasive procedures were most frequent in Delitzsch (8.2%; 95% CI, 8.0% - 8.4%) and least frequent in Oschatz (6.3%; 95% CI, 6.1% - 6.5%). Pharmacological and therapeutic administrations were highest in Torgau (12.3%; 95% CI, 12.0% - 12.6%) and lowest in Oschatz (9.8%; 95% CI, 9.5% - 10.1%).
Invasive and Pharmacological/Therapeutic Interventions by District (2019-2024)

Temporal Trends (2019-2024)
The longitudinal analysis revealed a stable utilization pattern for invasive procedures with minimal year-to-year variation (<1.0%) and no significant monotonic trend in the overall invasive rate (Table 4).
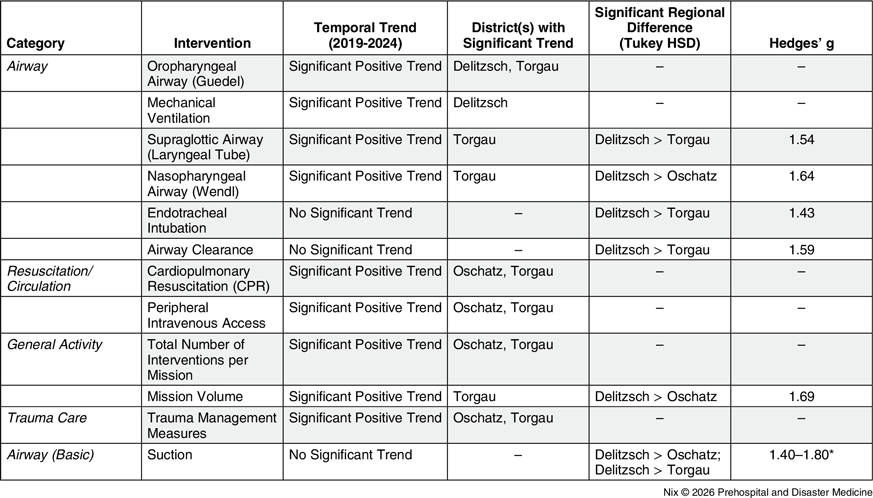
Temporal Trends and Regional Differences in Selected Paramedic-Performed Interventions (2019-2024)

Note: Significant positive monotonic trend over time (Mann–Kendall test, P < .05).
– No statistically significant temporal trend.
Regional comparisons performed using one-way ANOVA with Tukey HSD post-hoc testing (P < .05).
Effect sizes reported as Hedges’ g.
*Range reflects multiple pairwise comparisons.
In contrast, pharmacological and therapeutic administrations showed a modest but statistically significant increase over time. Temporal trends in invasive procedures and pharmacological/therapeutic administrations are shown in Figure 1.
Trends in Invasive Procedures and Pharmacological/Therapeutic Administrations (2019-2024).

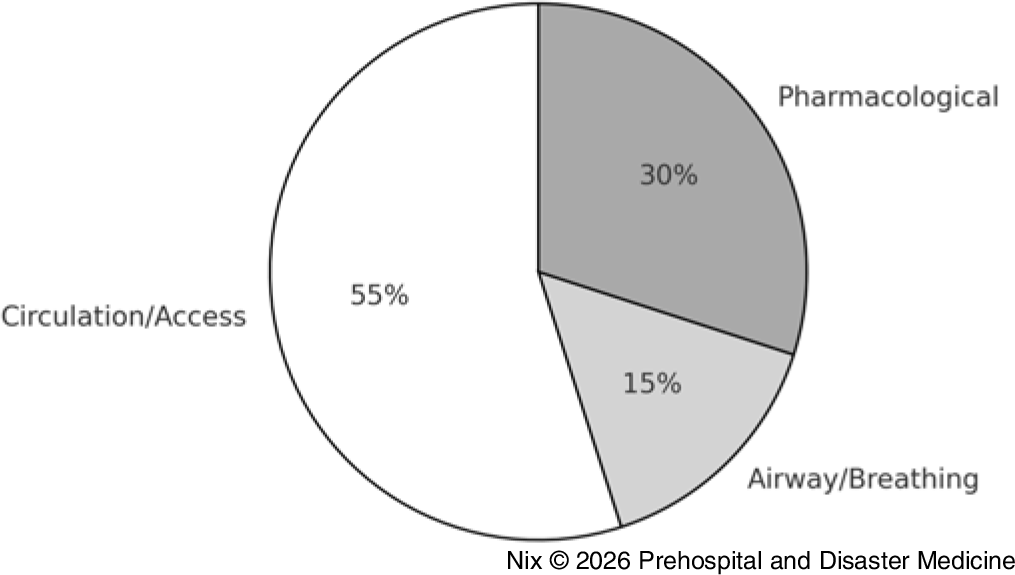
In 2024, circulation and vascular access procedures accounted for 55% of interventions, followed by pharmacological/therapeutic measures (30%) and airway/breathing interventions (15%); Figure 2.
Relative Distribution of Intervention Categories (2024).

Combined temporal and regional analyses demonstrated that overall intervention patterns remained largely stable, while selected procedures showed significant increases within specific districts. Broader increases in overall intervention activity, trauma-related measures, and circulation-related procedures were observed in Torgau and Oschatz. In contrast, Delitzsch exhibited significant increases primarily in selected airway interventions.
Independent of temporal trends, several airway-related procedures were performed significantly more frequently in Delitzsch compared with the other districts, with large effect sizes.
These findings suggest both region-specific developments in paramedic practice and persistent structural differences in intervention profiles across EMS districts.
Discussion
This six-year multicenter analysis provides comprehensive insight into how extended paramedic competencies under the EPA are implemented in routine prehospital care within a physician-based EMS system. Despite broad legal authorization, invasive and pharmacological interventions performed independently by paramedics remained relatively infrequent and largely confined to basic procedures. The results reflect both structural and cultural characteristics of the German physician-based EMS model and provide important implications for workforce training, supervision, and system design.
In this system, the allocation of responsibilities between paramedics and emergency physicians is primarily determined by clinical indication rather than simple resource availability. Paramedics manage a broad spectrum of common emergency conditions, while emergency physicians are typically dispatched for cases requiring advanced invasive procedures or complex decision making.
Interpretation of Findings
The overall utilization of invasive procedures (7.6%) and pharmacological/therapeutic administrations (11.3%) indicates that paramedic practice remains conservative. The most frequently performed invasive intervention was peripheral IV access, consistent with lower tiers of the Pyramid Process competency framework. Reference Lauer, Lier and Eich8 Accordingly, the present analysis emphasizes common procedures such as vascular access and medication administration, as these measures constitute the majority of paramedic clinical activity in routine EMS practice.
Advanced airway management, IO access, and other high-acuity invasive procedures were rare, suggesting limited procedural exposure and fewer opportunities to maintain high-risk competencies.
This finding should be interpreted within the structural characteristics of the German physician-based EMS system. Advanced airway management requiring rapid sequence intubation is typically performed by emergency physicians, and paramedic-performed intubation in the analyzed systems occurred primarily during resuscitation scenarios or when immediate airway control was required in the absence of a physician. Similar challenges related to prehospital airway management and provider type have been reported internationally. Reference Crewdson, Lockey, Roislien, Lossius and Rehn11
Notably, crystalloid administrations exceeded the number of IV/IO access placements performed by paramedics. This discrepancy is explainable by interprofessional task allocation: vascular access and fluid administration are not necessarily performed by the same provider. As the documentation system records only the measure performed by the individual paramedic, fluid administration may be documented without the access being placed by that same provider. This pattern therefore reflects operational workflow rather than documentation error.
Several factors likely contribute to the observed pattern. These regional differences may reflect variations in physician availability and SOP authorizations; however, this relationship was not directly measured and should therefore be interpreted as hypothesis-generating.
First, physician availability in potentially critical missions reduces the need for independent high-acuity paramedic interventions. Second, paramedics may act cautiously near the boundaries of legal authorization. Third, regional differences in SOP authorization, supervision, and continuing education may contribute to variability across districts.
In addition, regional SOP authorizations may change over time; therefore, variations in intervention frequencies may partly reflect evolving authorization policies rather than purely clinical factors.
The modest increase in medication/therapy administrations from 2019 to 2024 suggests a gradual integration of extended competencies into practice but did not materially change the overall procedural profile.
Comparison with International Data
Compared with Anglo-American EMS systems, advanced procedure frequencies were markedly lower. In the United States and Australia, paramedics perform endotracheal intubation in approximately two percent to five percent of missions and IO access in up to one percent. Reference Crewdson, Lockey, Roislien, Lossius and Rehn11–Reference Burgos-Esteban, Quintana-Diaz and Cordon-Hurtado16 However, these systems generally lack routine physician involvement and rely on standing orders, while the German EMS system operates as a hybrid model with both physician availability and paramedic autonomy, resulting in a different distribution of responsibilities.
Nevertheless, low exposure to advanced procedures is a recognized challenge for long-term competence. Evidence from EMS and critical-care transport settings suggests that low annual procedural volume is associated with reduced performance in advanced airway management and that structured quality programs can improve outcomes, supporting a volume-performance relationship. Reference von Vopelius-Feldt, Peddle and Lockwood17–Reference Sollid, Bredmose, Nakstad and Sandberg19 Although no universal threshold can be defined, available data indicate that providers with only a small number of intubations per year are at higher risk of skill decay, whereas maintaining a regular annual caseload (on the order of ∼10 procedures) is more likely to sustain provider proficiency. Reference Gillett, Saloum, Aghera and Marshall20 Simulation-based maintenance training improves both technical and non-technical airway skills and may mitigate decay over time. Reference Maurya, Ahmed and Garg21–Reference Yang, Wei, Xue, Deng and Zhi23
Importantly, as no individual-level data on training exposure, simulation frequency, or re-certification status were available, any interpretation regarding skill retention in this cohort remains theoretical and based on external evidence. In physician-based EMS systems, procedural exposure among emergency physicians is also influenced by individual specialty backgrounds and clinical practice outside the prehospital setting.
Implications for Education and System Development
The findings underscore the necessity of aligning paramedic education with actual clinical practice. The EPA curriculum provides extensive training in invasive skills, yet field exposure remains limited. Bridging this gap requires integrated clinical placements, regular scenario training, and the use of telemedical support to reinforce decision confidence. Moreover, clearly defined outcome monitoring is essential to assess the real-world impact of extended competencies on patient safety and EMS efficiency.
The observed regional differences highlight the importance of harmonizing authorization policies among Directors of EMS jurisdictions. Establishing national benchmarks for paramedic-led interventions, alongside consistent quality assurance metrics, would promote uniform practice and enable interregional comparability.
From a broader system perspective, this study suggests that the German EMS remains in a transitional phase toward greater paramedic autonomy. While the EPA laid the legal foundation, its practical realization depends on continuous dialogue between Medical Directors, educators, and frontline providers. The long-term success of this evolution will rely on balancing patient safety, workforce confidence, and legal accountability.
Strengths and Limitations
A key strength of this study is its large, multicenter dataset covering six years and nearly 200,000 EMS missions. Standardized digital documentation enabled longitudinal evaluation and high completeness of core procedural data (>98.0%).
However, several limitations must be considered. As physician-attended missions were excluded from the present analysis, direct comparisons between paramedic and physician procedural frequencies were not possible. The retrospective design limits causal inference, and the dataset does not include patient outcomes, preventing direct assessment of effectiveness, safety, or success rates (eg, intubation success, complications). In addition, the dataset did not contain a structured variable describing patient transport decisions; therefore, the proportion of missions resulting in hospital transport or treat-and-release could not be analyzed. Documentation accuracy and local SOP differences may affect inter-district comparability.
The study period (2019-2024) includes the COVID-19 pandemic, which likely influenced EMS operations and provider behavior, particularly for aerosol-generating procedures, potentially affecting temporal trends. Finally, no multivariable regression or subgroup analyses were performed; thus, patient-level determinants of procedure utilization could not be evaluated.
Future Research
Future work should explore outcome-related endpoints, such as success rates of paramedic-performed interventions, complications, and patient survival. Qualitative research investigating barriers to independent action, perceptions of legal risk, and decision-making processes among paramedics and Medical Directors could complement the quantitative findings. Comparative studies with international systems may further illuminate how different governance structures influence the utilization of extended competencies.
Conclusion
Ten years after implementation of the EPA, this six-year multicenter analysis demonstrates that invasive and pharmacological interventions performed independently by German paramedics remain relatively infrequent. Most measures are confined to basic procedures and standard treatments, while advanced invasive skills are rarely applied. These findings highlight the continued influence of the physician-based EMS structure and support the need for structured competency maintenance and outcome-focused evaluations to inform on-going EMS role development.
Author Contributions (ICMJE)
Steffen Wolfgang Nix: Study conception and design, data analysis, interpretation of results, and manuscript drafting.
Christian Hohenstein: Data interpretation, methodological supervision, and critical revision of the manuscript.
All authors meet the ICMJE criteria for authorship and approved the final manuscript.
Use of Artificial Intelligence Technology
No artificial intelligence tools were used for data collection or data analysis. AI-assisted language support was used solely for grammatical and stylistic refinement. All content was reviewed and approved by the authors.
Conflicts of interest/funding
No conflicts of interest declared. No external funding was received for this work.


 Open access
Open access