


Background
Societal conditions and the environments in which people live, learn, and work shape health1 and can have significant effects on health across the lifespan.Reference Singh2 Addressing these social drivers of health has been shown to improve health outcomes.Reference Williams3 In the United States, economic incentives such as Accountable Care Organizations4 and tax exemption status5 have led health systems to screen for and address social drivers of health (SDH). National efforts are underway in the US to complete SDH screening and documentation in the health care setting; for example, in 2023, the Department of Health and Human Services issued a call to action to address health-related social needs, and multiple agencies across the department created programs and policies in response.6 The White House7 and the Centers for Medicare & Medicaid Services8 simultaneously released documents on the importance of identifying and addressing SDH in health care. Screening and tracking SDH in the health care setting can assist with referral to services, identify population health needs, support planning and implementation of interventions, and collect data on patient health outcomes.9
In the clinical setting, health professionals are most likely responsible for screening, documenting, and addressing the social needs of the patients/families they serve.Reference Schickedanz10 While many clinicians agree on the importance of screening for SDH, they lack the confidence to address SDH once identified, particularly because they feel unequipped to address the social needs of patients/families.Reference Schickedanz11 One program that helps facilitate intervention is the medical-legal partnership.12 The medical-legal partnership (MLP) model embeds a lawyer into the clinical setting, where the lawyer and clinician work together to screen and address health-harming legal needs, the subset of social drivers of health that are amenable to legal intervention.Reference Regenstein13 Examples of health-harming legal needs that can be addressed by medical-legal partnerships include access to federal and state benefits,Reference Shchetinina14 utility assistance,Reference Rosenberg15 housing stability,Reference Arora16 and intimate partner violence/family law.Reference Cené17 As of this writing, there are 450 known medical-legal partnerships across 49 states and Washington, DC in the US.18 Medical-legal partnerships have been implemented in a variety of clinical settings, including but not limited to neonatal intensive care units,Reference Gievers, Mutrie and Klawetter19 primary care,Reference Sauaia20 pediatrics,Reference Beck21 oncology care,Reference Dowling22 HIV care,Reference Muñoz-Laboy23 critical care,Reference Eynon, Robinson and Smith24 and Veterans Affairs Medical Centers.Reference Tsai25 Emerging research has demonstrated that MLPs have a positive impact on healthReference Shchetinina26 and legalReference Tsai27 outcomes for patients and their families, support clinicians with addressing SDH when delivering care,Reference Eynon28 and provide cost savings for patients and health systems.Reference Richman29 In addition to directly addressing patients’ health-harming legal needs in the clinical setting, MLPs have worked more broadly addressing the contexts presented in the socio-ecological modelReference McLeroy30 by cross-educating between disciplines and working upstream to advocate more broadly for groups of patients at the organizational/institutional and policy level.Reference McLaren31 For example, MLPs encompassing the criminal legal needs of patients have included not only addressing warrants for arrest and mitigating sentencing around substance use related charges, but also advocating for broader local and state level policy change.Reference Puglisi and Bhandary-Alexander32
Over the last 30 years,Reference Teitelbaum and Lawton33 clinicians and researchers have developed and implemented MLPs in the clinical setting, establishing modelsReference Regenstein34 and fostering an understanding around the core infrastructureReference Marple35 required to start, strengthen, and sustain an MLP. Starting and maintaining an MLP remains challenging because of the coordination needed to support medical and legal professionals working together,Reference Morrison36 a lack of buy-in at the staff and health system level,Reference Liaw37 difficulties associated with information sharing between the medical and legal professionals,Reference Arora38 and because the roles of clinicians in the MLP are not fully defined.Reference Friley39 Prior researchReference Arora40 and the National Center for Medical Legal Partnership toolkitReference Marple41 identified that medical champions, those clinicians who support, advocate, and lead the implementation of the intervention at clinical sites,Reference Morena, Gaias and Larkin42 have an important part in the implementation and sustainment of an MLP. Yet there is a gap in the literature about the responsibilities/actionable steps that a medical champion can use to best support an MLP.
The goal of this exploratory study is to characterize the mechanisms which a medical champion can use to best serve an MLP, forming possible roles and responsibilities of medical champions to help mitigate challenges and support the success of an MLP. By using the Delphi methodology,Reference Jones and Hunter43 this study: (1) explores the mechanisms by which medical champions may best support a medical-legal partnship, and (2) assigns priority level to identified potential roles and responsibilities of a medical champion.
Methods
This study uses the Delphi methodology, which is an iterative process used to form consensus, in this case about the mechanisms through which a medical champion can best serve the MLP.44 Delphi methodology has been widely used in medical and health services research and contributes to knowledge and decision-making where empiric data are unavailable but expert opinion exists.Reference Niederberger and Spranger45 In a Delphi study, experts in the field are asked to share their opinions on the topic being studied, which are then summarized at the group level.46 The process is repeated until a predefined consensus point is reached.47 The study was deemed exempt by Yale University’s Institutional Review Board.
Setting
On March 2–3, 2023, the Solomon Center for Health Law and Policy at Yale Law School, the Georgetown University Health Justice Alliance, and Penn State Dickinson Law cohosted a conference, “Medical-Legal Partnerships: Equity, Evaluation, and Evolution,” at Yale Law School in New Haven, CT.48 A total of 225 people from 18 states attended the conference. These attendees represented 75 different organizations, of which 40 were MLP programs. A workshop at the conference about medical champions was hosted and facilitated by five of the authors (LP, RM, AS, RV, AMF) who are medical champions in the MLPs at their institutions and are MLP experts (Appendix Table 1).49
Delphi Round One
Workshop attendees were asked to complete a form that collected data about their experience with MLPs, their identified discipline, and their experience within that discipline. The workshop attendees were then introduced to the topic of medical champions through a short didactic, wherein the workshop leaders described their own MLPs and their roles within those MLPs.
The workshop attendees were then split into five groups, with approximately five people per group, to perform a gallery walk exercise. Each group had a workshop leader who was also an expert on MLP (LP, RM, AS, RV, AMF) and accompanied attendees to different stations throughout the room. Each station had a large piece of paper labeled with a topic, four of which were paraphrased from the National Medical-Legal Partnership’s range of activities: (a) medical champions and larger-scale advocacy, (b) medical champions and health center transformation, (c) medical champions and education, (d) medical champions and direct patient care.50 The fifth station had a piece of paper seeking to explore interactions between the medical and legal side: medical champions and relations with the legal team. Attendees were asked to write their thoughts directly upon the paper to share ideas and comments about the mechanisms by which a medical champion can best serve the partnership for each of the stations’ topics. After eight minutes, attendees rotated to the next station. Attendees were encouraged to modify the concepts they found written by others, add or comment upon the written concepts, or add new concepts. Each group had the chance to comment at each station.
Characteristics of Workshop Attendees and Identification of Possible Mechanisms by Which a Medical Champion Can Best Serve a Medical-Legal Partnership
The data from the conference workshop were analyzed by a pediatrician/MLP expert and a public health researcher (AMF, CFA). Using SAS 9.4 software (SAS Institute, Inc., Cary, North Carolina), we used descriptive analysis to summarize the workshop attendees’ characteristics. Using Microsoft Excel 2019 (Microsoft Corporation, Redmond, Washington), the data from the five stations were reviewed to identify overlap of ideas/comments about how a medical champion can best serve a MLP, synthesizing these into possible mechanisms formulated as either responsibilities or actionable steps.Reference Thorn51
Delphi Round Two
Once these possible mechanisms were identified, the Delphi round two survey was created. The panel of experts who facilitated the workshop at the MLP conference were asked to rank the possible mechanisms using a Likert scale to consider their utility for an MLP: (a) high priority (must have/critical), (b) medium priority (important to have/very useful), (c) low priority (nice to have), and (d) unnecessary (anything that is not relevant for an MLP or already a global need for all persons). In July 2023, the expert rankings were electronically captured in the Delphi round two survey (Qualtrics, Provo, Utah). If the majority (>60%) voted the same ranking of the possible mechanism, then that was the level of priority designated.52
Delphi Round Three and Concept Mapping
The rankings of mechanisms from Delphi round two were presented to the panel of experts in October 2023. The experts were asked to share their thoughts, with the opportunity to change their ranking after reviewing the results from Delphi round two.53 Mechanisms that had no consensus at the completion of Delphi round two were discussed in a meeting with the experts. The meeting was moderated so that all voices were heard, and views were exchanged from all participants to allow the group to reach consensus. Finally, the medium and high priority mechanisms were mapped to the socio-ecological model54 by a pediatrician/MLP expert and a public health researcher (AMF, CFA).
Results
Workshop Attendees
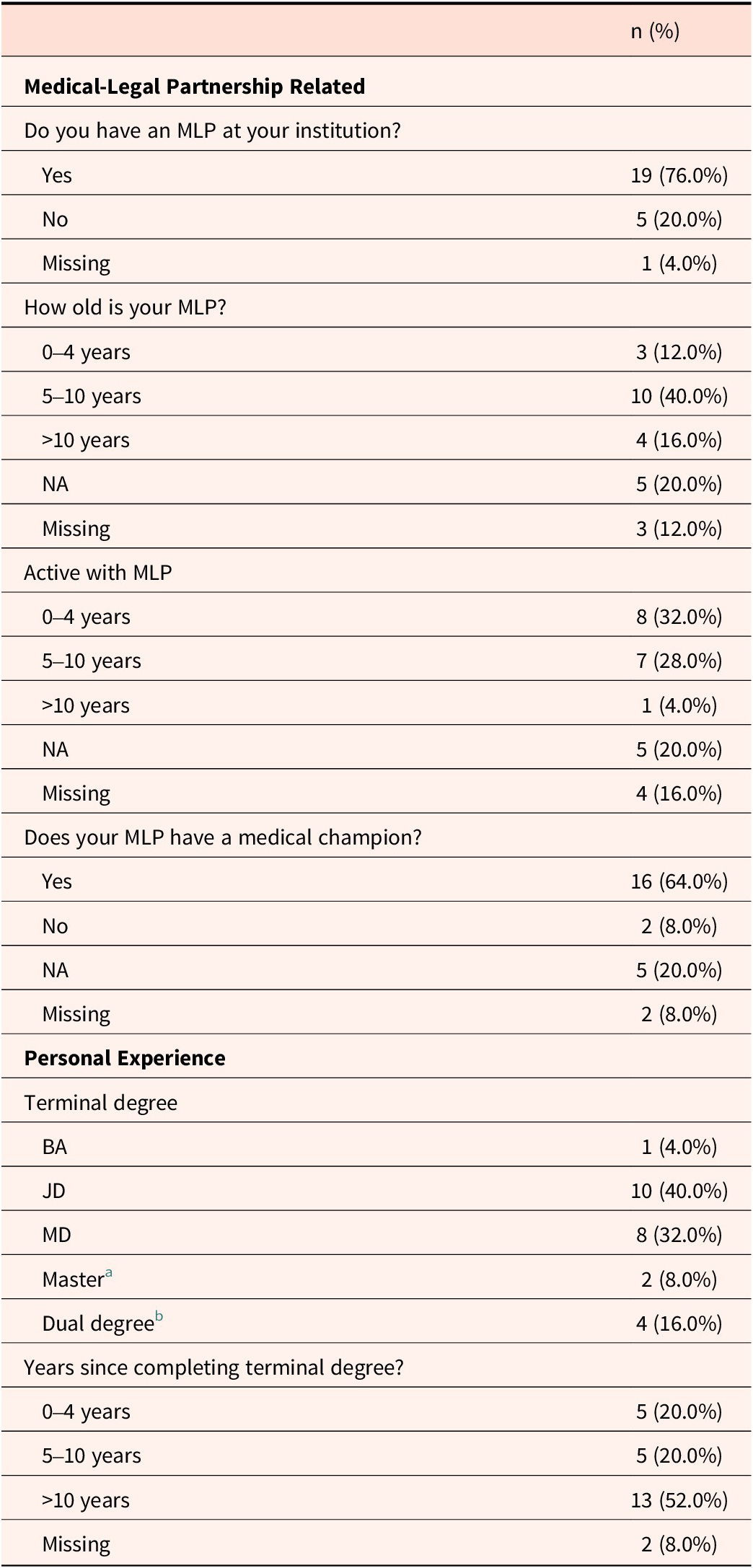
Table 1 presents the descriptive characteristics of the conference workshop attendees. Twenty-five individuals attended the workshop, of which 52% had completed JD training, 32% had completed MD training, 76% had an MLP at their institution, and 64% reported that their MLP had a medical champion.
Descriptive characteristics of workshop attendees (n=25)

Table 1. Long description
From the top, the table is divided into two sections: Medical-Legal Partnership Related and Personal Experience. Under Medical-Legal Partnership Related: ‘Do you have an M L P at your institution?’ shows Yes 19 (76.0 percent), No 5 (20.0 percent), Missing 1 (4.0 percent). ‘How old is your M L P?’ lists 0 to 4 years 3 (12.0 percent), 5 to 10 years 10 (40.0 percent), greater than 10 years 4 (16.0 percent), N A 5 (20.0 percent), Missing 3 (12.0 percent). ‘Active with M L P’ shows 0 to 4 years 8 (32.0 percent), 5 to 10 years 7 (28.0 percent), greater than 10 years 1 (4.0 percent), N A 5 (20.0 percent), Missing 4 (16.0 percent). ‘Does your M L P have a medical champion?’ lists Yes 16 (64.0 percent), No 2 (8.0 percent), N A 5 (20.0 percent), Missing 2 (8.0 percent). Under Personal Experience: ‘Terminal degree’ includes B A 1 (4.0 percent), J D 10 (40.0 percent), M D 8 (32.0 percent), Master 2 (8.0 percent) with footnote a (M A 1, M P H 1), Dual degree 4 (16.0 percent) with footnote b (J D/Ph D 1, J D/L L M 1, J D/M P H 1, M B A/M P H 1). ‘Years since completing terminal degree’ shows 0 to 4 years 5 (20.0 percent), 5 to 10 years 5 (20.0 percent), greater than 10 years 13 (52.0 percent), Missing 2 (8.0 percent). Abbreviations: M L P is Medical-Legal Partnership, N A is Not Applicable.
Abbreviations: MLP: Medical-legal partnership; NA: Not applicable.
a MA=1, MPH=1
b JD/PhD=1, JD/LLM=1, JD/MPH=1, MBA/MPH=1
Delphi Results
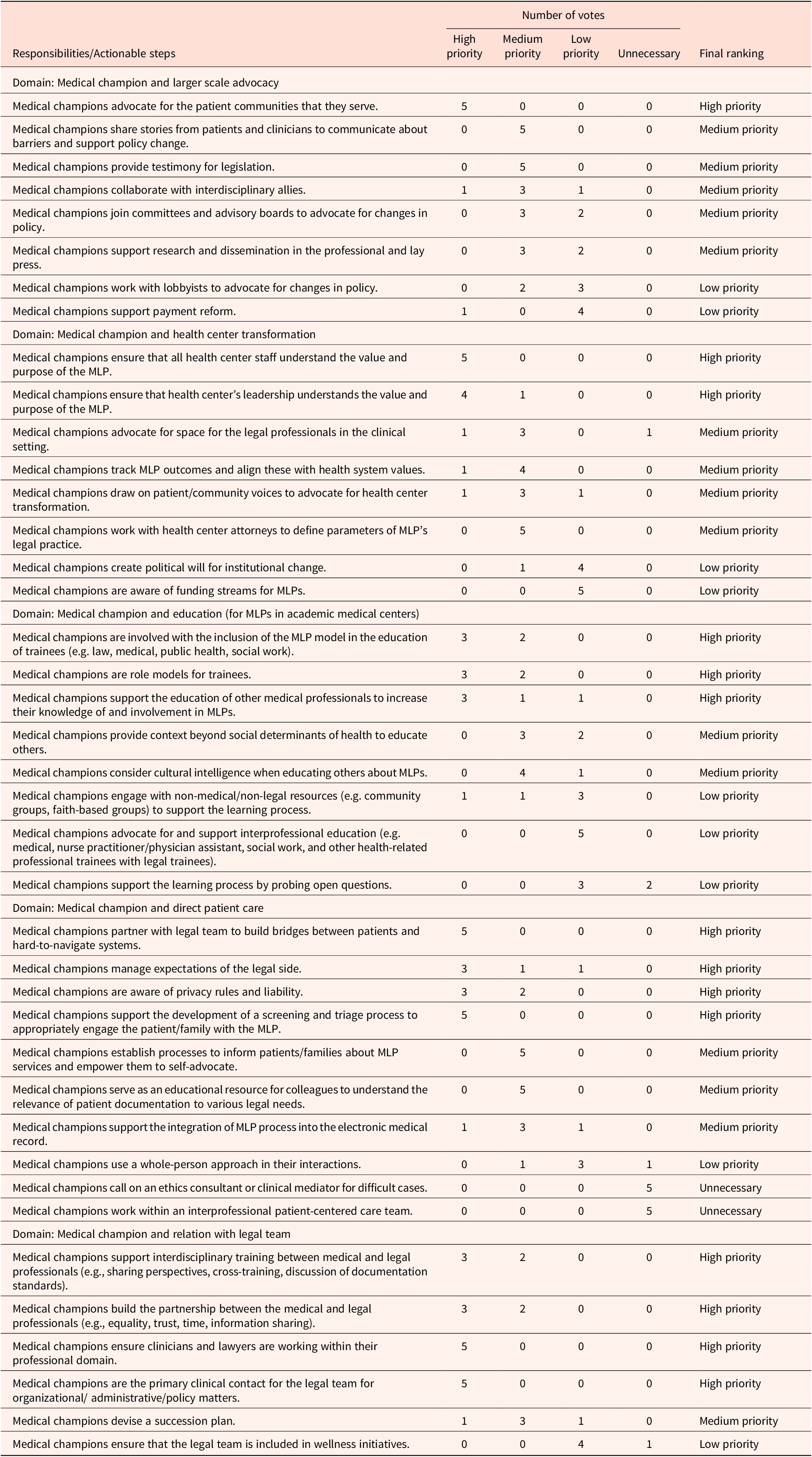
A total of 107 concepts were written at the conference workshop topic stations. Similar ideas/comments were synthesized to create statements about the mechanisms by which a medical champion might support a MLP.Reference Thorn55 For example, for the gallery walk topic about medical champions and larger-scale advocacy, the concepts “Help testify on important bills (gather data for testimony),” “Testify on a bill,” and “Be willing to testify” were combined to form the responsibility/actionable step “Medical Champions provide testimony for legislation.” From the concepts gathered during the workshop, a total of 40 mechanisms were identified. In the second round of the Delphi method, the expert panel reached consensus on the ranking of 25 mechanisms. During the final Delphi round, the expert panel reviewed and confirmed with the voting results from the previous round and achieved voting consensus on the remaining 15 mechanisms (Appendix Table 2). Table 2 presents the final rankings, while Figure 1 maps the high and medium priority mechanisms to the socio-ecological model.
Medical-legal partnership (MLP) expert voting results for the mechanisms by which medical champions may best support an MLP

Table 2. Long description
The table is divided into five domains of responsibility for medical champions in an M L P. The columns include Responsibilities or Actionable steps, Number of votes across High priority, Medium priority, Low priority, and Unnecessary, and a Final ranking.
Domain: Medical champion and larger scale advocacy
* Advocate for patient communities: 5 High priority votes. Final ranking: High priority.
* Share stories for policy change: 5 Medium priority votes. Final ranking: Medium priority.
* Provide testimony for legislation: 5 Medium priority votes. Final ranking: Medium priority.
* Collaborate with interdisciplinary allies: 1 High, 3 Medium, 1 Low priority votes. Final ranking: Medium priority.
* Join committees and advisory boards: 3 Medium, 2 Low priority votes. Final ranking: Medium priority.
* Support research and dissemination: 3 Medium, 2 Low priority votes. Final ranking: Medium priority.
* Work with lobbyists: 2 Medium, 3 Low priority votes. Final ranking: Low priority.
* Support payment reform: 1 High, 4 Low priority votes. Final ranking: Low priority.
Domain: Medical champion and health center transformation
* Ensure staff understand M L P value: 5 High priority votes. Final ranking: High priority.
* Ensure leadership understands M L P value: 4 High, 1 Medium priority votes. Final ranking: High priority.
* Advocate for space for legal professionals: 1 High, 3 Medium, 1 Unnecessary votes. Final ranking: Medium priority.
* Track M L P outcomes: 1 High, 4 Medium priority votes. Final ranking: Medium priority.
* Draw on patient voices: 1 High, 3 Medium, 1 Low priority votes. Final ranking: Medium priority.
* Work with health center attorneys: 5 Medium priority votes. Final ranking: Medium priority.
* Create political will: 1 Medium, 4 Low priority votes. Final ranking: Low priority.
* Aware of funding streams: 5 Low priority votes. Final ranking: Low priority.
Domain: Medical champion and education
* Inclusion of M L P in trainee education: 3 High, 2 Medium priority votes. Final ranking: High priority.
* Role models for trainees: 3 High, 2 Medium priority votes. Final ranking: High priority.
* Support education of other medical professionals: 3 High, 1 Medium, 1 Low priority votes. Final ranking: High priority.
* Provide context beyond social determinants: 3 Medium, 2 Low priority votes. Final ranking: Medium priority.
* Consider cultural intelligence: 4 Medium, 1 Low priority votes. Final ranking: Medium priority.
* Engage with non-medical or non-legal resources: 1 High, 1 Medium, 3 Low priority votes. Final ranking: Low priority.
* Advocate for interprofessional education: 5 Low priority votes. Final ranking: Low priority.
* Support learning by probing open questions: 3 Low, 2 Unnecessary votes. Final ranking: Low priority.
Domain: Medical champion and direct patient care
* Partner with legal team to build bridges: 5 High priority votes. Final ranking: High priority.
* Manage expectations of legal side: 3 High, 1 Medium, 1 Low priority votes. Final ranking: High priority.
* Aware of privacy rules and liability: 3 High, 2 Medium priority votes. Final ranking: High priority.
* Support screening and triage process: 5 High priority votes. Final ranking: High priority.
* Establish processes to inform patients: 5 Medium priority votes. Final ranking: Medium priority.
* Educational resource for colleagues: 5 Medium priority votes. Final ranking: Medium priority.
* Support integration into electronic medical record: 1 High, 3 Medium, 1 Low priority votes. Final ranking: Medium priority.
* Whole-person approach: 1 Medium, 3 Low, 1 Unnecessary votes. Final ranking: Low priority.
* Call on ethics consultant: 5 Unnecessary votes. Final ranking: Unnecessary.
* Work within interprofessional care team: 5 Unnecessary votes. Final ranking: Unnecessary.
Domain: Medical champion and relation with legal team
* Support interdisciplinary training: 3 High, 2 Medium priority votes. Final ranking: High priority.
* Build partnership: 3 High, 2 Medium priority votes. Final ranking: High priority.
* Ensure professionals work within domain: 5 High priority votes. Final ranking: High priority.
* Primary clinical contact for legal team: 5 High priority votes. Final ranking: High priority.
* Devise succession plan: 1 High, 3 Medium, 1 Low priority votes. Final ranking: Medium priority.
* Include legal team in wellness initiatives: 4 Low, 1 Unnecessary votes. Final ranking: Low priority.
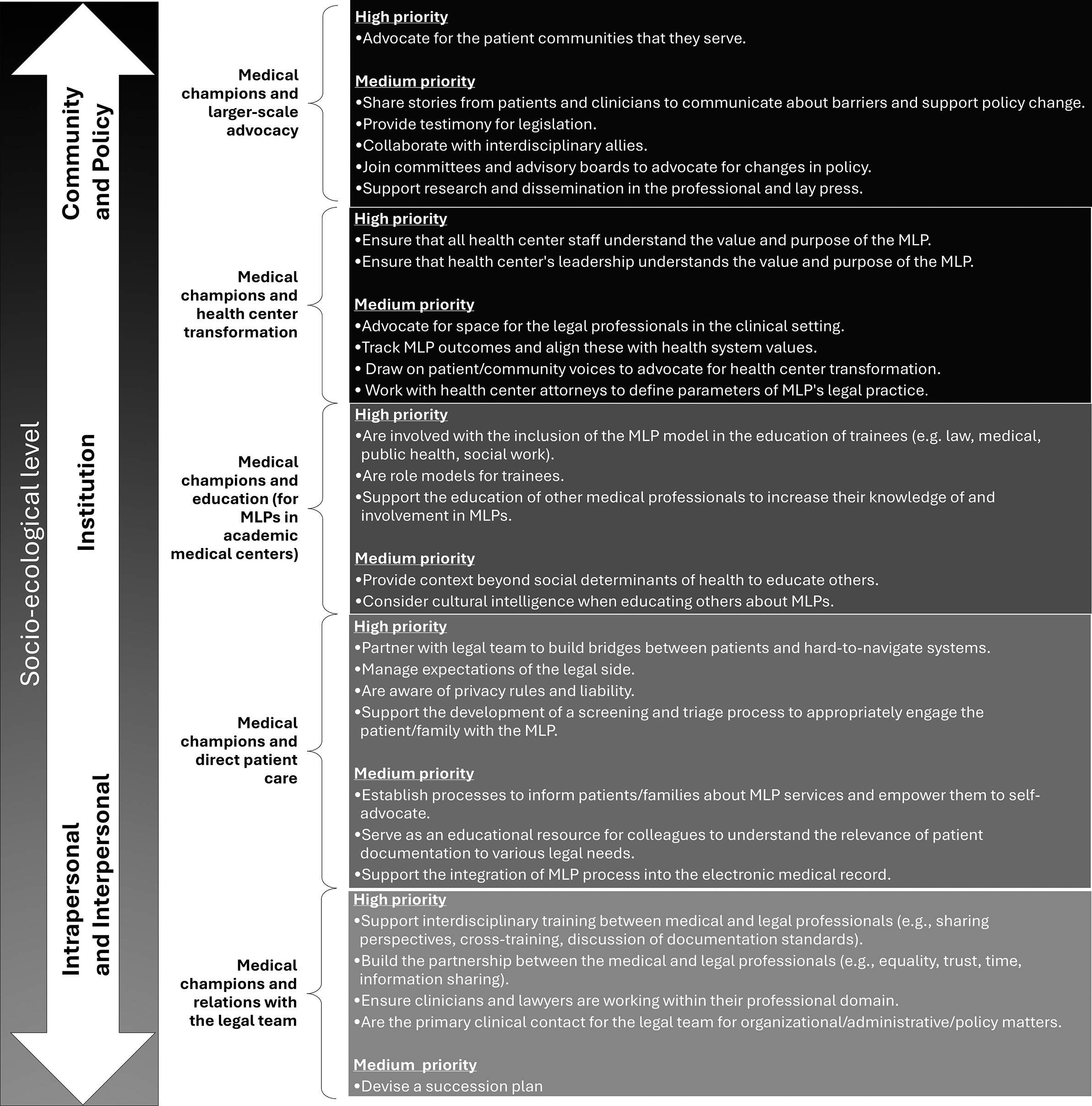
Medical champions’ high and medium priorities mapped to the socio-ecological model.

Figure 1. Long description
The diagram is organized into three vertical columns. The leftmost column is a double-headed arrow labeled Socio-ecological level, divided into three segments. The middle column lists five categories of medical champions. The rightmost column lists specific high and medium priorities for each category.
* Socio-ecological level: Community and Policy.
* Champion Category: Medical champions and larger-scale advocacy.
* High priority: Advocate for the patient communities that they serve.
* Medium priority: Share stories from patients and clinicians to communicate about barriers and support policy change. Provide testimony for legislation. Collaborate with interdisciplinary allies. Join committees and advisory boards to advocate for changes in policy. Support research and dissemination in the professional and lay press.
* Socio-ecological level: Institution.
* Champion Category: Medical champions and health center transformation.
* High priority: Ensure that all health center staff understand the value and purpose of the M L P. Ensure that health center's leadership understands the value and purpose of the M L P.
* Medium priority: Advocate for space for the legal professionals in the clinical setting. Track M L P outcomes and align these with health system values. Draw on patient or community voices to advocate for health center transformation. Work with health center attorneys to define parameters of M L P's legal practice.
* Champion Category: Medical champions and education for M L Ps in academic medical centers.
* High priority: Are involved with the inclusion of the M L P model in the education of trainees such as law, medical, public health, and social work. Are role models for trainees. Support the education of other medical professionals to increase their knowledge of and involvement in M L Ps.
* Medium priority: Provide context beyond social determinants of health to educate others. Consider cultural intelligence when educating others about M L Ps.
* Socio-ecological level: Intrapersonal and Interpersonal.
* Champion Category: Medical champions and direct patient care.
* High priority: Partner with legal team to build bridges between patients and hard-to-navigate systems. Manage expectations of the legal side. Are aware of privacy rules and liability. Support the development of a screening and triage process to appropriately engage the patient or family with the M L P.
* Medium priority: Establish processes to inform patients or families about M L P services and empower them to self-advocate. Serve as an educational resource for colleagues to understand the relevance of patient documentation to various legal needs. Support the integration of M L P process into the electronic medical record.
* Champion Category: Medical champions and relations with the legal team.
* High priority: Support interdisciplinary training between medical and legal professionals, for example, sharing perspectives, cross-training, and discussion of documentation standards. Build the partnership between the medical and legal professionals, including equality, trust, time, and information sharing. Ensure clinicians and lawyers are working within their professional domain. Are the primary clinical contact for the legal team for organizational, administrative, or policy matters.
* Medium priority: Devise a succession plan.
This study identified 14 high priority and 15 medium priority mechanisms by which the medical champion can serve an MLP. The domains at the intrapersonal and interpersonal levels of the socio-ecological model (e.g., “Medical champions and direct patient care” and “Medical champions and relations with the legal team”) each had the highest number of high priority mechanisms (n=4). Conversely, the domains at the institution and community/policy level (e.g., “Medical champion and health center transformation” and “Medical champions and larger-scale advocacy”) had the fewest number of high priority mechanisms (n=2 and n=1 respectively). Additionally, this study identified three high priority and two medium priority mechanisms steps for the domain “Medical champion and education” for medical champions who support an MLP in an academic medical center.
Discussion
We obtained consensus on the role of the medical champion in MLPs using a modified Delphi process. From the 107 concepts collected at the conference workshop, 40 mechanisms by which a medical champion can best serve an MLP were identified, of which 14 were ranked as high priority and 15 were ranked as medium priority. The panel of experts reached consensus that communication and relationship-building is a high priority for medical champions to support the daily operation of the MLP. Our study had novel findings providing evidence that medical champions are a cornerstone for the successful development, implementation, and sustainability of MLPs as they understand clinical workflows, are aware of patient population needs, and can support the multidisciplinary team of an MLP to address health-harming legal needs. Prior research has identified that medical champions are important to MLPs, and this study identifies mechanisms that a medical champion can use to support the success of MLPs and help to better define their possible role and responsibilities.
While health care professionals56 and patients/familiesReference Rogers57 have expressed support for screening and addressing SDH in the clinical setting, they have also articulated apprehension, in part perceiving insufficient access to resources to yield actionable steps to address patients’ social needs.Reference Hamity58 As noted earlier, challenges that MLPs have faced include a lack of buy-in at the staff and health system level.Reference Liaw59 The domain “Medical champions and direct patient care” had the highest number of high and medium priority mechanisms, indicating that medical champions have an integral role in supporting colleagues and patients/families to become engaged with all facets of the MLP’s work. For example, the medical champion may “partner with legal team to build bridges between patients and hard-to-navigate systems,” “support the development of a screening and triage process to appropriately engage the patient/family with the MLP,” and/or “establish processes to inform patients/families about MLP services and empower them to self-advocate” (Appendix Table 2). In these ways, the medical champion can help to meaningfully and durably integrate health and social services and smooth the path to learning for medical and legal professionals as well as patients and their families. By creating awareness of the MLP, expanding perceptions of the health care professionals’ roles, and assisting colleagues’ and patients’/families’ access to the MLP, the medical champion may empower health care professionals and patients/families to address health-harming legal needs.Reference Murillo60
While the medical and legal professions have long been thought adversaries due to malpractice litigation, in fact, the two professions have a long history of collaboration to address civil and human rights.61 The domain “Medical champions and relations with the legal team” had the highest number of high priority mechanisms for the medical champion. Research has identified that there is a need to support medical and legal professionals working together for an MLP to be successful.Reference Morrison62 The multidisciplinary nature of MLPs increases the effectiveness of the intervention, as clinicians and lawyers each bring their own trainings and skills to synergistically address health-harming legal needs.63 Barriers for MLPs that have been identified include difficulties associated with information sharing between medical and legal professionals,Reference Arora64 as well as challenges with coordination between medical and legal professionals to support working together in the clinical setting.Reference Morrison65 Some examples of how a medical champion may support the interdisciplinary collaboration between medical and legal professionals include: “Medical champions support interdisciplinary training between medical and legal professionals (e.g., sharing perspectives, cross-training, discussion of documentation standards),” “Medical champions build the partnership between the medical and legal professionals (e.g., equality, trust, time, information sharing),” “Medical champions ensure clinicians and lawyers are working within their professional domain,” and/or “Medical champions are the primary clinical contact for the legal team for organizational/administrative/policy matters” (Appendix Table 2). As noted by Regenstein et al., if the MLP does not become part of the daily workflow, then the intervention can falter.Reference Regenstein66 Since medical champions understand clinical workflows and are aware of patient population needs, they can assist legal professionals with navigating the health care setting.
This study found that the mechanisms by which a medical champion can best support a MLP were not highly prioritized at the health system/policy level, as compared to the intrapersonal and interpersonal level. Health is impacted by a complex socio-ecological context, and one of the goals of MLPs is to advocate for policy change to promote health equity.Reference Bhandary-Alexander and Shek67 Completing advocacy work could be challenging for a busy medical champion who is delivering patient care while also supporting the MLP in a clinical setting. Through the medical-legal partnership, the medical champion can work alongside lawyers, who embody legal expertise in the partnership and can perhaps best utilize legal strategies to address policies, practices, and structures that are the root cause of health-harming legal needs.Reference Mitchell and Chopp68 If a medical champion would like to engage in health system transformation or larger-scale advocacy, this study identifies possible actions that the medical champion may complete. For example, the medical champion may “ensure that health center’s leadership understands the value and purpose of the MLP,” be “involved with the inclusion of the MLP model in the education of trainees (e.g. law, medical, public health, social work),” “provide testimony for legislation,” “join committees and advisory boards to advocate for changes in policy,” and/or “ support research and dissemination in the professional and lay press” (Appendix Table 2). Changes at the community, health system, and policy levels are essential to address health-harming legal needs, and medical champions have opportunities through the MLP to engage in health system transformation and larger-scale advocacy.
Strengths of this project include that the five experts who participated in the Delphi process have experience with MLPs and are medical champions for MLPs, serving a variety of patient populations. Criteria for consensus were defined in advance of the Delphi process to ensure the Delphi methodology was followed.Reference Thorn69 Three rounds of the Delphi process were considered to be adequate since agreement was achieved for all identified mechanisms by which a medical champion can best support an MLP during round three.Reference Thorn70 Limitations include the small sample size — the statement-generating round one was collected from 25 individuals who self-selected to join the conference workshop. That said, all individuals in the workshop did so due to interest in MLPs, 77% of the individuals who participated in the data collection process have an active MLP within their institution, and 64% were themselves actively involved with the MLP; participants came from both medical and legal fields, enhancing the reliability of the sample. Research has suggested that a small sample size of “experts who have similar training and general understanding in the field of interest” can have reliable results in the Delphi process.Reference Akins, Tolson and Cole71 A second limitation of the study was that the last two rounds of the Delphi process took place approximately two months apart. However, during the final round of the Delphi process, the experts examined the results of Delphi round two, and the discussion during this round did not indicate that the length of time between the rounds was an issue; in fact, the length of time between successive rounds allowed for reflection on the statements and additional lived experience during that reflection time, perhaps resulting in the split of one of the mechanisms into two independently ranked mechanisms.Reference Thorn72 A third limitation of the study is that consensus for a mechanism was defined as the majority (>60%) of experts voting the same prioritization of the mechanism, while most Delphi studies aim for >75-80% group agreement.Reference Barrios73 For the third and final round of the Delphi process, the rankings from Delphi round two were presented to the panel of experts, and discussion occurred regarding their agreement with the results, with an opportunity to change their ranking vote; in this final Delphi round, all of the votes that occurred for mechanisms had consensus of >80% by the panel of experts. This study has identified and prioritized mechanisms and formed possible responsibilities/actionable steps to assist with defining the role of a medical champion in an MLP. Suggested future projects may aim to understand the impact that the medical champion has on MLP development, implementation, and sustainability, and identify best practices that health systems and organizations can use to support medical champions.Reference Shea74
Conclusion
US health systems are experiencing a paradigm shift as they begin to address SDH. Integrating health services and social services remains a complex challenge. MLPs exemplify innovative multidisciplinary interventions that unite medical and legal professionals to address health-harming legal needs. Findings from this study highlight the pivotal role of medical champions in MLPs. The medical champion is crucial for driving the success and sustainability of an MLP. By gaining a deeper understanding of the possible responsibilities and actionable steps that a medical champion can undertake, it is possible to mitigate the challenges faced by MLPs and enhance their implementation and longevity.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/jme.2026.10245.
Acknowledgements
Thank you to James Bhandary-Alexander for providing data on the overall attendance of the MLP conference held by the Solomon Center at Yale Law School.
Funding statement
Rahul Vanjani is supported by funding through the Macy Faculty Scholarship.
Disclosures
The authors have nothing to disclose.



 Open access
Open access