

Key messages
Chapter 3.7 reviews priority-setting. Priority-setting is about taking explicit decisions on where limited public resources should be allocated. Vertical priority-setting focuses on choices for particular sets of health conditions or population groups whereas horizontal priority-setting looks more broadly across types of care, such as primary or secondary care, and broader investments. Key learning includes that:
Defining a health benefits package (HBP) that is affordable and accessible by all implies a horizontal approach to priority-setting.
Countries cannot progress towards universal health coverage (UHC) without horizontal priority-setting and without some form of collective funding and procurement mechanisms.
Horizontal priority-setting is highly context specific. Countries may need to reorganize financing and procurement mechanisms to overcome barriers to progress.
Increasing the total resources for HBP can help with the introduction of more horizontal approaches.
Improving procurement can also support the move towards horizontal priority-setting whether through national efforts (such as better data gathering and use) or international initiatives (i.e. harmonizing regulation across countries or global investment in health security).
Local capacity is key in supporting the pooling mechanisms, HBP design and regulation which enable horizontal priority-setting. Donors can usefully support health systems strengthening by investing in capacity-building and information sharing.
Strong political will and cooperation between stakeholders is critical in progressing towards appropriate priority-setting for UHC and in designing, financing and implementing a comprehensive HBP.
Introduction
Following the 2012 United Nations resolution on UHC, in September 2015 all United Nations Member States reinforced their commitment to UHC by subscribing to Sustainable Development Goal 3.8 – achieving UHC. Moving towards UHC requires investment across three key dimensions identified by the World Health Organization (WHO): (i) extension of health coverage to populations not covered; (ii) improvement in quality and the number of services in the health package provided; and (iii) financial risk protection for poor and vulnerable populations. But, in most countries, scarce resources imply trade-offs between these dimensions, and not everyone in a country may have access to all beneficial health services at affordable prices. Trade-offs mean choices on what and how health care interventions are provided by a health system, for which population groups, in what quantity and at whose expense. Such choices must be made in health care systems in both high and low- and middle-income countries (LMICs) – i.e. some form of rationing of health services takes place in all health systems. A process of priority-setting is therefore essential to ensure that policy-makers align the HBP with both the goals and capacities of their country’s health system.
Priority-setting: definition and role in developing an HBP
Without an explicit priority-setting process, rationing may still happen within a health system at multiple levels. For example, prices faced by patients may limit demand; long travel distances and delays in accessing services (such as waiting lists) may also lead to a reduction in demand. Eligibility rules based on citizenship, population groups or packages of services covered are all forms of rationing within a health system. Priority-setting in health care is the process of making explicit the decisions about allocations of resources in a health system, given that resources are limited – i.e. rationing always takes place. In the context of UHC, priority-setting is required to develop a comprehensive package of health services – an HBP that is aligned with social goals to which all individuals have access (Chalkidou et al., Reference Chalkidou2016). Such HBPs include “the set of health services and products that can be feasibly financed and provided for everyone, given a particular country’s actual circumstances” (Glassman, Giedion & Smith, Reference Glassman, Giedion and Smith2017). Establishing an HBP requires difficult political choices and finding a balance between different suppliers of technologies and services, and claims from patient groups and regions (Savedoff et al., Reference Savedoff2012). Making the process of defining an HBP transparent and based on scientific evidence for the cost–effectiveness of different interventions and products can help mitigate some of the political challenges associated with priority-setting for UHC. However, priority-setting using cost–effectiveness alone focuses only on the maximization of health within a population. Other criteria beyond cost–effectiveness, such as equity and financial protection, can have significant implications for which products and services are included and who has access to the HBP (Norheim et al., Reference Norheim2014).
Many high-income countries (HICs) that have UHC also already have some form of priority-setting process in place (Ham, Reference Ham1997; Seixas et al., Reference Seixas2021). This chapter is primarily concerned with LMICs looking to make the transition to UHC. Decision-makers in LMICs often face severe resource limitations compared to decision-makers in HICs; the challenge is choosing affordable health care products and services to include in an HBP from a wide array of available options (see Chapter 2.2 for more on setting HBPs).
Vertical and horizontal priority-setting: definitions
In the priority-setting process, distinction can be made between vertical and horizontal priority-setting. In vertical priority-setting, the choice typically concerns which health care interventions and services to offer for the same or similar set of health conditions (Ham, Reference Ham1997) or to specific population groups. In contrast, horizontal priority-setting involves choices between health care interventions and services for different diseases, across types of care (primary or secondary care) and broader investments in health system strengthening. But the definitional boundaries between the two are hardly clear cut when it comes to actual implementation. If we take HIV/AIDS prevention and treatment, for example, these occur across different care settings, making a programme focused on treatment with antiretroviral therapies (ARTs) more vertical than one that deals with the whole spectrum of the disease. Disease-specific donors often cover prevention and treatment for multiple diseases and may practise horizontal priority-setting within their portfolio of services. For example, the Global Fund to Fight AIDS, Tuberculosis and Malaria covers three diseases and, recently, COVID-19. The Global Fund’s investment has also been shown in large part to support pandemic preparedness and health system strengthening (Boyce et al., Reference Boyce2021). The same applies for Gavi, the Vaccine Alliance, as investment in vaccines also helps strengthen national procurement systems. However, as we discuss later in this chapter, a recipient country may face significant challenges in incorporating these donor-funded services within a more integrated (horizontal) priority-setting exercise. On the other hand, a health insurance package which caters mostly to the wealthy or urban population or a health care fund which is predominantly noncommunicable disease-focused, such as a cancer treatment fund as proposed in Nigeria (Onyejia & Adebowale, Reference Onyejia and Adebowale2019) or the Indian dialysis programme (NHSRC, 2018), is more vertical, and in some cases may be less pro-poor than a broader HIV or malaria programme. Another form of verticalization can occur where federal states devolve financing and delivery of care to provinces/regions with inequity across states in terms of access and outcomes.
Horizontal priority-setting and UHC
Within the UHC framework, defining an HBP that is affordable and accessible to all implies a primarily horizontal approach to priority-setting. For countries which may already have several, often large, vertically set priority programmes, moving towards an HBP which takes a more integrated, horizontal approach will require reorganization of existing financing and procurement mechanisms.
Most countries that have horizontal priority-setting processes in place (regardless of explicitly stated or implicitly defined HBPs) have some form of collective funding and procurement mechanisms – for example, centralized tax financing as in Denmark, New Zealand, Sweden and the United Kingdom – while others, such as Germany or the Netherlands, rely on forms of compulsory health insurance (see Chapter 2.1). In contrast, countries looking to move to UHC through horizontal priority-setting have limited collective funding and are financed by a wide range of sources, including taxes (income or value-added tax (VAT)), international donors and a large share of out-of-pocket (OOP) payments (see Chapters 1.4 and 2.4). The two groups also differ in their health product procurement strategies. Those that have horizontal priority-setting processes in place typically have a national procurement strategy with well-established supply chain mechanisms, enabling market-shaping power due to volume of purchasing. Countries pursuing UHC through horizontal priority-setting tend to have highly decentralized and fragmented procurement and supply chain systems with poor demand forecasting and supply management abilities (Silverman et al., Reference Silverman2019).
The definition of procurement in this chapter encompasses product (not service) selection, regulation, price negotiation and purchasing. It begins with a discussion of prevalent funding and procurement arrangements that pose a challenge for countries looking to move towards horizontal priority-setting for UHC. It then discusses potential ways forward, highlighting successes from countries making this transition. Emphasis is also placed on limitations and unintended consequences that have occurred during the transition. The chapter concludes with policy recommendations for donors and countries working towards a transition from vertical to horizontal priority-setting.
Challenges in moving to horizonal priority-setting
The role of financing arrangements
As organization and funding arrangements within a health system are built up over time, the nature of the health financing system has practical implications for horizontal priority-setting. Horizontal priority-setting assumes that there is some form of collective financing mechanism (general taxation/social insurance/employer scheme) where utilization is independent of funding contribution. Moving towards a collective financing mechanism requires a health financing transition. The transition involves a rise in total health spending per person financed through pooled resources, accompanied by a gradual decrease in OOP spending (Fan & Savedoff, Reference Fan and Savedoff2014). However, this delineation does not always exist in practice and most systems use some mixture of funding mechanisms. These funding mechanisms often affect social goals and can pose challenges to ensuring that prioritized services are provided. For example, certain types of financing arrangements can influence provider or patient behaviour by stimulating or suppressing demand for specific health services (e.g. curative services) or for services that may be of priority to specific population groups (e.g. the wealthy). They may also impact the size of the revenue base. To illustrate these issues, we consider challenges to horizontal priority-setting with three types of internal funding mechanisms that coexist with collective financing: private insurance, complementary insurance and user charges.
In many countries that have collective health financing schemes, individuals can choose to also have voluntary (private) health insurance (see Chapter 1.3). For example, the United Kingdom has private health insurance alongside collectively financed health care; individuals can use private insurance to replace collective coverage with insurance premiums set by the private provider based on the individual’s risk. Individuals choose private insurance if the benefits/services covered under private insurance are perceived as greater than those from the collective HBP given the cost of the premium. In this case, the collective HBP may receive less political support from wealthy individuals who prefer and obtain private insurance. To garner political support for the collective HBP, policy-makers may be forced to design packages that are attractive to wealthy individuals, which can result in trading off equity and limiting coverage for interventions that are deemed to represent the best value for money.
The existence of a large(r) private insurance sector (such as in the USA) can also have profound consequences for the horizontal priority-setting process. The existence of an opt-out option from the public system can mean significantly lower revenues for the collective HBP, limiting the services that can be provided and the population who can be covered. Private insurance tends to attract wealthier individuals, who are generally healthier and whose needs may not be covered by the collective HBP. Thus, the budget available for a collective HBP through horizontal priority-setting is intrinsically linked to the benefits being offered.
Alternative arrangements to private insurance are supplementary and complementary health insurance alongside a collective HBP. For example, in many Latin American and Caribbean countries, private health insurance is a secondary source of coverage for some of the population. Its role is supplementary, i.e. covering health goods and services not covered in the basic HBP in Belize, Ecuador, Guyana, Peru, Suriname and Uruguay. However, in others, such as Argentina, Brazil, Chile, Honduras and Peru, its role is complementary, i.e. covering cost-sharing for health goods and services covered in the basic HBP (Lorenzoni et al., Reference Lorenzoni2019). In this scenario, establishing a comprehensive package of services that is affordable and accessible to all may be challenged by a need to offer services which are not covered by supplementary or complementary health insurance or a package that predominantly meets the needs of those who are unable to afford private health insurance. The sustainability of such an offering may also be in question if the services covered by the collective HBP are those that are likely to result in catastrophic health expenditure.
A third type of funding mechanism may influence the success of a comprehensive collective HBP: user charges (see Chapter 2.4). User charges are OOP payments for services or contributions towards the cost of a service. Within a collective HBP, they can be used to try to regulate demand for health care and generate revenue for the health system. If user charges are implemented within the HBP without exemptions in place, they result in catastrophic payments for individuals who cannot afford the charges, exacerbating inequity within the health system. On the other hand, the removal of user charges or widespread exemptions may result in decreased revenue for the health system, limiting the ability to provide a wider range of services or cover a large population.
In many countries, the provision of public health interventions, mental health services and diagnosis and treatment of communicable disease has been vertically arranged, with corresponding vertical allocations of funding for these specific areas. This arrangement offers little flexibility for allocations across areas and can present significant challenges in incorporating these services within a more integrated priority-setting exercise. In LMICs, the vertical arrangement of certain services, particularly those for communicable diseases, are due to their reliance on external funding. External funding from bilateral, multilateral and philanthropic organizations have typically been targeted to specific disease areas or priority groups. Examples include the Global Fund, Gavi, the United States President’s Emergency Plan for AIDS Relief (PEPFAR) and the Bill & Melinda Gates Foundation (Atun, Bennett & Duran, Reference Atun, Bennett and Duran2008).
Furthermore, the level and availability of external funding may dictate which health issues are placed high on national health agendas as well as the types of interventions that are selected to address them. Donors with disease-specific priorities may limit the extent to which health systems can leverage economies of scope in the delivery of services through a shared platform (horizontally). Such arrangements also pose a challenge for setting a cost–effectiveness threshold that reflects the budget constraint across horizontal interventions. Cost–effectiveness thresholds set by national policy-makers will reflect the limited domestic budget. Interventions selected according to these cost–effectiveness criteria must be highly cost-effective (reflecting the narrow domestic budget), but the limited budget may also narrow the scope of services covered.
The role of procurement arrangements
Low-income and lower-middle-income countries are estimated to spend around US$ 50 billion per year on global health products (Silverman et al., Reference Silverman2019, based on estimates from Rosen et al., Reference Rosen2017). Despite this, access to essential medicines and health products in these countries remains insufficient, leaving individuals and families to access them in the private sector from OOP payments (Ewen et al., Reference Ewen2017). Health product procurement in low-income countries is also highly dependent on donors or privately purchased in lower-middle-income countries. Moving towards a horizontally set HBP implies fundamental changes to how health products and medicines are financed, transitioning away from OOP payments towards pooled financing and procurement.
In implementing a package of services that will expand access and coverage, countries need to procure a wide range of products to meet the needs of horizontally set benefits plans. In doing so, countries must justify the selection of products that meet the goals of wider access to services and coverage within their budgets. Health technology assessments and cost–effectiveness analyses can play a useful role in product selection, but not all health-improving products will be locally cost-effective within highly constrained government budgets (Wirtz et al., Reference Wirtz2017). Furthermore, problems may be compounded by transition away from donor aid as income levels rise. Public sector spending in LMICs accounts for around 50% of expenditure on health products. Global health institutions and nongovernmental organizations, however, account for a large share of this public sector funding (Silverman et al., Reference Silverman2019). These funding mechanisms are not guaranteed to persist, and their support is usually based on countries becoming self-reliant over time (Wirtz et al., Reference Wirtz2017). As support from donors wanes, countries will not only have to make up for their share but raise additional resources to expand services and products covered under the benefits plan.
Some countries have come together to use pooled procurement systems to aggregate demand for pharmaceutical products. Pooled procurement, sometimes also called group purchasing or group contracting, combines decentralized decision processes on required volumes with centrally negotiated prices (Dubois, Lefouili & Straub, Reference Dubois, Lefouili and Straub2021; Nemzoff, Chalkidou & Over, Reference Nemzoff, Chalkidou and Over2019). For example, the Organization of Eastern Caribbean States Pharmaceutical Procurement Scheme, established in the 1980s, aggregates demand for products on the essential medicines list of 10 Caribbean states. Similarly, the Pan American Health Organization Revolving Fund (for vaccines, syringes and related supplies) and the Strategic Fund (for vector control medicines, diagnostic kits and related equipment) aggregate demand across several Latin American and Caribbean countries. This approach has also been adopted by global health institutions such as the Global Fund, UNITAID and Gavi, who in some shape or form have adopted product “market-shaping” strategies aimed at lowering prices through volume guarantees, combining demand across countries or ensuring continuous supply by contracting multiple suppliers. Countries no longer eligible for or reliant on such organizations and arrangements for health products may be faced with higher prices for these products due to their limited negotiating power and smaller-scale purchases. Apart from facing higher transaction costs due to lower volumes, unorganized demand may also deter suppliers from low-volume markets and/or from offering preferential pricing arrangements. This lack of organization from the demand side may also discourage investment in development of new products or manufacturing capacity (Silverman et al., Reference Silverman2019). To be fit for purpose, procurement processes in a horizontally set plan will need to optimize for quality, price, supply security and efficiency. Many LMICs have fragmented supply chains with purchasing, distribution and delivery processes vertically arranged across funders or programme/disease areas. Silverman and colleagues (Reference Silverman2019) provide the example of Nigeria, which has parallel funding, purchasing and distribution systems by commodity area, for example essential medicines, maternal and child health and HIV, tuberculosis (TB) and malaria. These duplications prevent the organization of demand and obstruct planning and delivery of a unified HBP. Further inefficiencies in procurement processes due to institutional and administrative challenges such as difficult tendering procedures or delayed payments to suppliers may result in increased prices due to the higher transaction cost associated with operating in such markets.
Existing financing and procurement arrangements can pose challenges to successfully moving from vertical to horizontal priority-setting. In the next section, we discuss potential ways of addressing these challenges and highlight efforts already being made by international donors to assist countries transitioning from donor funds or those never eligible for funding for; for example, the Global Fund’s Wambo platform for COVID-19 products, or Gavi’s purchasing agreements for transitioning countries.
Moving towards horizontal priority-setting
Reducing fragmentation by integrating financing schemes
In countries with multiple financing streams, fragmentation of financing streams can be reduced by merging existing ones where possible, thus reducing overlaps and generating a wider risk pool, so improving equity (see Chapter 2.1 for more on pooling). Amalgamation of existing schemes requires strong political will and there is potential for resistance from existing beneficiaries of the different schemes. Such resistance may arise if a unified benefits package implies fewer services covered than any of the separate schemes or higher levels of contributions for the same or fewer services. To overcome resistance to the consolidation, sometimes new legislation may be required. Such legislation may place the management of financing of different schemes with a single institution while paving the way for eventual consolidation (Towse, Mills & Tangcharoensathien, Reference Towse and Tangcharoensathien2004). Such an approach was implemented by Thailand when trying to consolidate four existing schemes in a move towards UHC (Box 3.7.1). However, full consolidation has not been achieved and three separate schemes still exist. Despite the extended coverage of Thailand’s UHC scheme, its benefits package is still less generous than those offered by two of the existing schemes – civil servants and social security schemes – making consolidation unlikely to take place soon.
Prior to the introduction of UHC in 2001, Thailand had four separate health coverage schemes:
1. a tax-financed scheme providing medical benefits for civil servants;
2. a tax-financed medical welfare card scheme for those with low incomes;
3. a voluntary health card scheme for households predominantly in rural areas; and
4. a contributory social security scheme, mandatory for all private employees.
Prior to UHC, these schemes benefited 43.5 million of Thailand’s population of 62 million. In its attempt to merge the four schemes, the government met strong resistance from members of the civil servants’ and social security scheme, who feared a reduction in their entitlements. To proceed with UHC, the government amalgamated the voluntary health card scheme and medical welfare schemes to give coverage to 47.8 million people (roughly 72% of the population). The UHC scheme established a unified benefits package covering essential services in preventive, curative and palliative care for all age groups. More recently, it has extended coverage to high-cost services, such as renal replacement therapy, cancer therapy and stem-cell transplants. Furthermore, the National Health Security Act, which was passed by Thailand’s Parliament in 2002, created a new institution to regulate the quality and financial aspects of the UHC scheme. Under this legislation, while benefit entitlements of the civil service and social security schemes remained unchanged, the financing of these two schemes was placed with the National Health Security Office, which oversees the UHC scheme, thus paving the way for eventual consolidation when it becomes politically acceptable to do so.
Despite the successes of Thailand’s UHC scheme it faces several challenges. As a noncontributory, predominantly tax-financed scheme, its sustainability is affected by the adequacy of tax revenues in the face of rising health care costs. Thailand continues to rely on funding from the Global Fund for specific programmes such HIV prevention programmes because of the difficulties in getting certain interventions for key populations funded by government.
Expanding the fiscal space
Implementing a horizontally set benefits plan often requires an increase in resources. In general, with tax-financed health systems, simply improving tax collection could generate more resources for health. However, such expansions, even if feasible, may not guarantee a larger allocation or more consistent support for health care. One potential solution may be for governments to leverage OOP spending; for example, by enticing those paying OOPs to join a collective scheme for a small premium, through which certain frequently used services or purchased drugs could be accessed at better negotiated prices. Such an approach is an alternative to the more commonly used insurance for health financing approach and facilitates greater efficiency in spending. Health insurance for raising funds has been shown to be unlikely to raise revenues commensurate with the requirements of providing adequate coverage for financial risk protection in LMICs (Barasa et al., Reference Barasa2021; Gheorghe et al., Reference Gheorghe2019). Another option is the creation of new taxes or the earmarking of existing tax sources for health spending (Box 3.7.2). Earmarking “involves separating all or a portion of total revenue – or revenue from a tax or group of taxes – and setting it aside for a designated purpose” (WHO, 2017a). Some obvious candidates include levying or increasing taxes on unhealthy products, such as tobacco and alcohol, or a reduction in subsidies for fossil fuels. The use of this earmarked revenue can be channelled to specific health-related priorities rather than to general health spending. The main advantage of earmarking unhealthy products is that in the short-to-medium term they can be a source of continuous, regular funding that is not affected by budgetary reviews. There is also likely to be political support for tax increases on such products when the proceeds are channelled towards health care (WHO, 2016). Over the longer term, revenues may fall as consumption falls or a black market thrives. Such an approach may also generate small revenues in countries where certain unhealthy behaviours (such as smoking) are not dominant. One of the main criticisms of earmarking revenues is that they limit budgetary flexibility and earmarked funds could potentially have been channelled towards more deserving programmes or projects. In this case, soft earmarking for certain priorities may be an option. For example, Thailand’s Health Promotion Foundation is funded directly through a 2% earmarked tax on alcohol and tobacco. Opponents also highlight the importance of determining public spending based on policy decisions rather than by the amount of revenue raised by an earmarked tax. Cases studies on earmarking tobacco tax revenues in nine countries have shown some evidence that when revenues are channelled directly into an autonomous fund dedicated to public health, such as into the overall pool of funds for a UHC benefits plan, then those revenues successfully add funding for health (WHO, 2017a).
Ghana was the first country in sub-Saharan Africa to introduce a National Health Insurance Scheme (NHIS). The NHIS was constituted in 2003 and all residents of Ghana are eligible for NHIS coverage, which has a generous benefits package covering 95% of diagnosed conditions including all outpatient, inpatient and emergency care. The scheme has no cost-sharing requirements, including for pharmaceuticals associated with the covered health conditions (Wang, Otoo & Dsane-Selby, Reference Wang, Otoo and Dsane-Selby2017).
The NHIS is primarily funded from:
VAT (70%);
deductions from the Social Security and National Insurance Trust (SSNIT) (20%) which mainly includes formal sector workers;
premium contributions (3%);
and the remainder from donor funds (Wang, Otoo & Dsane-Selby, Reference Wang, Otoo and Dsane-Selby2017).
Claims payments account for 77% of NHIS expenditure. By deriving funding for the NHIS from taxes on specific goods and services, Ghana’s health insurance scheme is the only in the world that is funded by VAT. This ensures that revenues keep pace with economic growth, while risk and cost pooling occur at the national level. However, reliance on VAT funding means revenue does not rise with an expansion in coverage.
Since its inception, the NHIS has faced several challenges to its financial sustainability. These include the small revenue base arising from high levels of premium exemptions. Over 60% of active NHIS members are exempt from premiums (Alhassan, Nketiah-Amponsah & Arhinful, Reference Alhassan, Nketiah-Amponsah and Arhinful2016). Premium exemptions apply to SSNIT contributors, enrollees under age 18 or over age 70, indigent people, institutionalized people and beneficiaries of some social protection programmes. Adverse selection and enrolee turnover has also been a problem. Wang and colleagues (Reference Wang, Otoo and Dsane-Selby2017) report that NHIS members are more likely to be in high-risk age groups (under 5s and over 55s). Their analysis of membership data shows that only 42% of enrollees from January 2014 remained in the scheme in January 2015 with members aged 15–24 years (least likely to have high medical expenditures) being the least likely to remain enrolled for a full year. A further challenge is the increasing cost of health products and service delivery. Health care providers under the NHIS rely on reimbursements to cover their operational expenditures. Providers are reimbursed using capitation payments for primary care services while all inpatient care and speciality outpatient services are reimbursed using the Ghana Diagnosis-Related Group (G-DRG) tariff scheme. However, pharmaceuticals are reimbursed using a fee for service (FFS), encouraging the use of prescription drugs. While the capitation payment for primary services provides some incentive for providers to be cost-efficient, these outpatient services account for only one third of all claims expenditures. The G-DRG and pharmaceutical FFS account for the remainder, with little incentive for providers to be effective in their referrals for secondary care or to curb overprescribing of curative services and pharmaceutical products. Thus, the combined effects of a generous benefits package, small and inconsistent enrolee base along with weak provider incentives continue to threaten the financial sustainability of the NHIS in Ghana (Durairaj, D’Almeida & Kirigia, Reference Durairaj, D’Almeida and Kirigia2010).
Cooperation between donors and countries
Cooperation between countries and international donors is vital to successfully implementing horizontal priority-setting. Ochalek and colleagues (Reference Ochalek2018) suggest estimating the scale of the health opportunity costs associated with any restrictions and conditions on donor assistance to facilitate a more informed and accountable negotiation between stakeholders, including careful examination of the reasons for restrictions. However, a more pragmatic and sustainable approach may be a change in the role of donors in countries transitioning from donor-dependent to fully domestically funded. Such a role may include supporting interventions that are marginally cost-ineffective, i.e. subsidizing key cost-ineffective interventions to make them cost-effective for a country’s threshold. Such an approach has been shown to be an equitable and sustainable model, especially for middle-income countries (Morton, Arulselvan & Thomas, Reference Morton and Thomas2018). Kanpirom and colleagues (Reference Kanpirom2017) also highlight the importance of not assuming value for money is a static property of interventions. Interventions implemented by a donor that are deemed initially cost-ineffective for a country due to their high start-up costs may become more cost-effective over time due to economies of scale, improvements in efficiency, etc. To ensure sustainability of donor-funded services after eligibility for donor funds ends, both countries and donors should monitor cost–effectiveness over time. This would enable countries to justify continued support for such cost-effective interventions within a horizontally set benefits package.
Donors also have a role alongside national health insurance schemes in ensuring equitable access to services. National schemes often do not prioritize the poorest, sickest or minority groups, resulting in unequal coverage (Schneider, Nakamura & Wu, Reference Schneider, Nakamura and Wu2019). Because of their emphasis on high-priority diseases and conditions by disease burden, national schemes and other UHC programmes may disregard important disease burdens in small populations (Kanpirom et al., Reference Kanpirom2017). For example, poor and marginalized groups living with HIV may not be able enrol in a national scheme as premiums may be unaffordable, or due to the limited regional coverage of the scheme (Global Fund, 2018). Donors supporting countries could focus their conditions or restrictions on requiring access for these groups, or where not feasible within the country’s budget, support such access themselves. Donors such as the Global Fund who invest in specific diseases (HIV, TB and malaria in this case) could pay for the three diseases through insurance funds, as is currently done in Viet Nam, where the Global Fund pays the insurance premiums of people living with HIV through their social health insurance (SHI), with a commitment from the government to absorb these premiums over time under domestic resources. ART and HIV-related care and services became reimbursable under Viet Nam’s SHI in late 2014. Over 70% of people living with HIV were due to receive ARTs via SHI by 2020 (Global Fund, 2020a). In Thailand, through a similar arrangement, migrant populations irrespective of registration status are covered by health insurance (Herberholz, Reference Herberholz2020).
Improving procurement and supply chain management
Improving procurement and supply chain management is critical to making health systems fit for delivering a unified HBP. Such improvements can reduce costs and limit supply shortages (WHO, 2015). Changes can include reducing fragmentation by centralizing procurement and improving data systems to monitor, manage and forecast demand for health products (Seidman & Atun, Reference Seidman and Atun2017). For example, the Nigeria Supply Chain Integration Project was established in 2015 with a mandate to coordinate product supply management across health programmes and funders with the aim of improving cost-efficiencies, reducing waste and minimizing stockouts. The project created and continues to maintain a logistics database on health products and pharmaceuticals across all health programmes in Nigeria, using it to monitor stock levels. The process also involved the creation and coordination of warehousing and transportation systems for health products across local, state and federal levels. Dubois and colleagues (Reference Dubois, Lefouili and Straub2021) further analysed the effect of centralized procurement on drug prices using data from seven LMICs. They found centralized procurement of drugs does lead to lower prices. However, if there are high levels of supply-side concentration, then the extent of price reduction is lower. In some cases, decentralization of financial management and procurement directly to the health facility level has been shown to be effective in improving the availability of medicines and medical equipment in health facilities (Kajuni & Mpenzi, Reference Kajuni and Mpenzi2021).
Any integration of vertical, particularly donor-financed services into a horizontal HBP requires a realignment of procurement arrangements. There are several possible actions for donors to facilitate such integration. For instance, donors can incorporate value-for-money assessments such as those for health technologies into their selection and price negotiation processes. Currently, many donors such as the Global Fund rely mainly on price negotiations based on bulk purchasing. In the longer term using value for money can help countries making the transition away from donor funding avoid the trap of investing in low-cost technologies that may have minimal impact or pay higher prices due to their inability to meet the bulk purchasing requirements for donor-negotiated prices (Kanpirom et al., Reference Kanpirom2017). Gavi, for example, assists countries transitioning away from its funding with access to multiyear supply agreement prices through manufacturer commitments via UNICEF or the Pan American Health Organization (Gavi’s designated procurement agents). However, currently this arrangement only applies to select vaccines, and is time-limited with varying lengths. Keller and Glassman (Reference Keller and Glassman2019) discuss other strategies that Gavi might adopt, including offering incentives to manufacturers to ensure steady vaccine supply, or permitting buy-ins from non-eligible countries. The latter may enable Gavi to globally negotiate tiered pricing agreements for countries, based on local affordability and cost–effectiveness. Delivering on horizontal priority-setting also requires access to safe, effective, good quality and affordable health technologies, medicines and vaccines. WHO (2017b) estimates at least 10% of medicines in LMICs are substandard or falsified, costing approximately US$ 31 billion annually. This is because many developing countries do not have the technical, institutional or financial capacities to regulate health product markets. Donors can facilitate alignment across countries and, where relevant, diseases, through the pooled procurement of products (such as vaccines or antiretrovirals) that meet World Health Organization requirements for international product safety and quality. Such market-shaping activities can benefit not just countries within the pool, but also those outside signalling good quality health products. One such example is the Wambo pilot for transactions not funded by the Global Fund, which was expanded to include COVID-19 products (Global Fund, 2020b).
Within a country, national regulatory authorities play a key role in selecting and approving health products. Thus, ensuring strong country regulatory systems is critical to ensuring countries are using good quality, safe and efficacious health products. Donors, in their efforts to strengthen health systems, could support investments in improving governance, technical competence, monitoring and evaluation capabilities. They could also make on-budget spending a key performance indicator for countries. Finally, donors can facilitate broader information sharing across countries, both within and outside pooled procurement arrangements, so addressing information asymmetry in product quality and safety. Countries, on the other hand, should lead the way in implementing regulatory reforms with donor support, resulting in less reliance on branding as a signal of quality and encourage high-quality generic suppliers (Silverman et al., Reference Silverman2019). They may also leverage models used by international donors such as organizing demand, volume guarantees and pooled procurement on a regional or global basis (Kim & Skordis-Worrall, Reference Kim and Skordis-Worrall2017; Seidman & Atun, Reference Seidman and Atun2017).
Health system strengthening and global health security (GHS)
In recent years there has been a lot of debate around the extent of true dichotomy in global health between either prevention and treatment or primary versus specialized care or, specific to this chapter, vertical versus horizontal financing and delivery of health services (Frenk & Gómez-Dantés, Reference Frenk and Gómez-Dantés2017; Dhillon, Karen & Marten, Reference Dhillon, Karan and Marten2019). The previous contention has been that vertical funding by donors for disease-based programmes could compromise the integrity and equity of recipient health systems (Daniels, Reference Daniels2006). However, evidence shows there are significant lessons and benefits to health systems from vertical programmes in how they strengthen, support and operationalize horizontal systems. For example, the response to the HIV/AIDS epidemic has shown vertical programmes can be effectively integrated into horizontal (in this case primary health care) systems. Such integration has enhanced the quality of the wider primary health care infrastructure, filled workforce gaps and improved patient flows between services (Pfeiffer et al., Reference Pfeiffer2010). Morton and colleagues (Reference Morton, Thomas and Smith2016) also demonstrate how investments in health system strengthening can be built into priority-setting exercises and highlight the complementarity between horizontal and vertical programmes.
Priority-setting implies difficult choices must be made. It also raises important ethical and equity considerations. In setting horizontal priorities and moving towards UHC, decision-makers are required to agree on criteria and establish transparent and fair priority-setting processes (WHO, 2014). As part of their priority-setting agenda, countries should invest in improving their GHS – preparedness for the prevention and management of outbreaks and epidemics, limiting the need to rely on external financing for emergencies and diversion of resources from horizontal priorities (see Chapter 3.8). Both priority-setting for UHC and GHS have intersecting agendas – both UHC and GHS aim at mitigating risk either to individuals (UHC) or populations (GHS) (Wenham et al., Reference Wenham2019). Low or no financial barriers to accessing health care improves access to services for infectious diseases while financial risk protection is an important social deterrent to the spread of infectious diseases. The recent Ebola outbreak in the Democratic Republic of the Congo and the COVID-19 pandemic have more than ever highlighted the importance of GHS and resilient health systems (Meyer et al., Reference Meyer2020). They have highlighted frailties in even the most advanced health systems, reinforcing the importance of successfully functioning health systems to detect and respond to health crises. Recent evidence has also highlighted the extensive contribution by vertical disease-specific international donors such as the Global Fund towards health security efforts through their investments in health system strengthening (Boyce et al., Reference Boyce2021).
Linking UHC and GHS may also enhance leverage for financing UHC (Ooms et al., Reference Ooms2017). The COVID-19 pandemic resulted in simultaneous global health and economic shocks. To facilitate a sustainable and inclusive longer-term recovery, progress towards UHC and improvements in population health (beyond COVID-19) are essential. Countries need to overcome the immense health and economic opportunity costs of managing the COVID-19 crisis (Appleby, Reference Appleby2020) including setbacks in the progress made over decades in key health outcomes such as maternal and child health and malnutrition. For many countries, health recovery requires an expansion of the government health budget. For a substantial group of LMICs, external financing is essential to recovering from this health shock. But an increase in health spending needs to be accompanied by better spending – reflecting improvements in equity and efficiency (Kurowski et al., Reference Kurowski2021). Such decisions inherently imply priority-setting across populations, diseases and services.
Conclusions and policy implications
Priority-setting involves decisions on the allocation of public resources. This naturally makes it a political issue subject to varying perspectives. For example, individuals may consider any reductions in their access to services as unacceptable, health product manufacturers may perceive priority-setting as a barrier to market access, or health care providers may perceive the exercise as restrictive of their autonomy. The ethical principles of priority-setting may not be easy to convey to the public, who may not also perceive the need for setting priorities.
When such political economy barriers are overcome at least to some extent, a move to horizontal priority-setting with the aim of UHC is possible. The long-term financial sustainability of existing national health insurance schemes, as in these countries, is, as such, unclear and potentially an issue. HBPs must be designed with the budget in mind, but also with consideration of the growth in overall health expenditure. As discussed earlier, finding the correct balance between coverage and revenue is a difficult task.
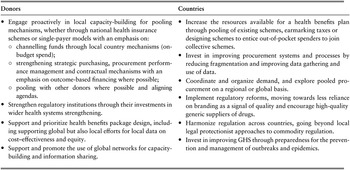
The “best” approach to horizontal priority-setting is context specific. Each country will need to find its own solution to barriers before successfully designing, financing and implementing a comprehensive HBP. But information sharing across countries about their approach and lessons learned can be vital to helping other countries move towards undertaking priority-setting exercises. Global networks like the International Decision Support Initiative can facilitate such information sharing and capacity-building. As both donors and countries have a large role to play in realizing horizontal priority-setting, our key recommendations for policy implementation are given in Table 3.7.1.

Table 3.7.1 Long description
The table has 2 columns: Donors and Countries. It reads as follows. Donors: Engage proactively in local capacity-building for pooling mechanisms, whether through national health insurance schemes or single-payer models with an emphasis on: channelling funds through local country mechanisms (on budget spend); strengthening strategic purchasing, procurement performance management and contractual mechanisms with an emphasis on outcome-based financing where possible; pooling with other donors where possible and aligning agendas. Strengthen regulatory institutions through their investments in wider health systems strengthening. Support and prioritize health benefits package design, including supporting global but also local efforts for local data on cost-effectiveness and equity. Support and promote the use of global networks for capacity building and information sharing.
Countries: Increase the resources available for a health benefits plan through pooling of existing schemes, earmarking taxes or designing schemes to entice out-of-pocket spenders to join collective schemes. Invest in improving procurement systems and processes by reducing fragmentation and improving data gathering and use of data. Coordinate and organize demand, and explore pooled procurement on a regional or global basis. Implement regulatory reforms, moving towards less reliance on branding as a signal of quality and encourage high-quality generic suppliers of drugs. Harmonize regulation across countries, going beyond local legal protectionist approaches to commodity regulation. Invest in improving G H S through preparedness for the prevention and management of outbreaks and epidemics.
In considering the role of vertical programmes and priorities, such vertical efforts can be an efficient way to achieve a time-limited target with explicit plans for future integration into a system-wide benefits plan. Large disease-specific health donors have a big role to play in supporting horizontal priority-setting through investments in building local capacity for its implementation, changing the way they support vertical programmes within a horizontally set benefits plan, and coordinating procurement across countries with lower purchasing power. In addition, more rigorous evaluations of procurement strategies (in addition to pooled procurement) are needed. Countries should also continue to gather and share information either on a regional or global level on health product pricing and quality. Platforms such as the Global Fund’s e-procurement hub (wambo.org) could provide a template for diseases beyond HIV, TB and malaria. It may be that donors can take on the role of coordinating and building or expanding existing platforms to offer global data on health products and market intelligence.Footnote 1

 Open access
Open access