

Introduction
Much ink has been spilled over how mental health issues intertwine with aging as a biological and social phenomenon and the manifold intricacies deriving from this particular intersectionality. Despite the general and scholarly interest in the mediatization of mental disorders, such academic perspectives tend to remain circumscribed to the dominant Western and white-centric approach. As a less investigated and yet frequently scientifically contested taxonomy, culture-bound syndromesFootnote 1 are regarded as “culturally-rooted and nation-specific mental health issues,” thus deviating from the Western-centric academic perspective (Sahoo et al. Reference Sahoo, Rai, Mehra, Grover, Mishra and Parveen2021).
Acknowledged as Japan’s most significant culture-bound syndrome that affects Japanese individuals on a large scale (Sarchione et al. Reference Sarchione, Santacroce, Corbo, Lupi, Martinotti and Di Giannantonio2015), hikikomori (引きこもり) has been broadly defined as “a form of pathological and extreme social withdrawal or social isolation whose essential feature is physical isolation in one’s home” (Kato et al. Reference Kato, Kanba and Teo2019: 2). Furthermore, it is estimated that more than a million “middle-aged and elderly hikikomori” live in Japan nowadays, and the total number is expected to increase (Saito Reference Saito2024: 1).
Within dominant clinical and media discourses, hikikomori has been consistently framed as a distinctly Japanese phenomenon and a culture-bound syndrome, understood through its connection to specific Japanese sociocultural characteristics (Suwa and Suzuki Reference Suwa and Suzuki2013; Kato et al. Reference Kato, Kanba and Teo2019). Although this paper later interrogates and complicates this framing, it is worth examining why these characterizations have taken hold. Cases of extreme social withdrawal exist globally, yet the hikikomori condition manifests in distinctly Japanese ways due to several interconnected cultural factors. First, the phenomenon emerged during Japan’s post-economic bubble era, when traditional societal structures faced unprecedented challenges, creating a distinctive sociocultural context for withdrawal behaviors. Second, the Japanese concepts of sekentei (世間体, social reputation), the particular stigma and shame (haji, 恥) associated with deviating from normative life trajectories, and meiwaku (迷惑, being a burden to others) amplify the psychological impact of failing to meet normative social expectations; even more, the cultural emphasis on group harmony (wa, 和) makes deviation particularly traumatic and stigmatized. Third, the vertical structure of Japanese society (tate shakai, 縦社会) offers limited pathways for reintegration once the individual deviates from standard social expectations, creating unique barriers absent in Western (individualistic) societies.
In this context, the aging hikikomori phenomenon represents more than a mental health issue; it stands as a complex sociocultural response to Japan’s rapidly aging society. This phenomenon emerges from traditional values of lifetime employment (shūshin koyō, 終身雇用), clearly defined social/gender roles, and intergenerational reciprocity that have been interrupted by economic crises and multilayered social transformation.
Previous research has investigated this mental health condition well under the inter- and cross-disciplinary lenses of cultural psychiatry, medical anthropology, and East Asian ethnomedicine. Nevertheless, there is an undeniable scarcity of academic studies that specifically examine how the hikikomori condition is portrayed in Japanese language media, while English-language scholarly endeavors tackling the intersection between age/aging and hikikomori as a culturally mediated mental health disorder are conspicuously absent.
In light of this background, the overarching aim of this study is to address this substantial academic gap and explore the phenomenon of the aging hikikomori through the lens of Japanese language media. Without denying whatsoever the conceptual, semantic, and linguistic differences existing between “aging,” “middle-aged,” “elderly,” “senior,” and “older adult,” throughout this paper, I will use “aging” as an umbrella term to encompass all the age and growing-of-age-related semantic and linguistic nuances. Furthermore, “Japanese language media” is considered here from a wide range of different media genres, formats, products, and outputs delivered and circulated in the Japanese language and within the geographical context of Japan—news, information media, magazines, blogs, to mention a few examples.
This study argues that Japanese media representations of aging hikikomori reflect a complex interplay among medical, social, and cultural frameworks, revealing both institutional perspectives and deeply personal narratives. Through analysis of mainstream media coverage and self-authored blog content, I demonstrate how aging hikikomori are portrayed not simply as individuals with a mental health condition, but as participants in a broader sociocultural phenomenon that intersects with Japan’s aging crisis, changing family dynamics, and evolving healthcare needs. The stark contrast between institutional media portrayals and personal narratives emphasizes the need to understand aging hikikomori through multiple lenses—as a medical condition, a social phenomenon, and a lived experience shaped both by the Japanese sociocultural context and the national language. Furthermore, albeit this analysis identifies distinctly Japanese cultural factors shaping the hikikomori phenomenon, I aim to avoid the essentializing tendencies of Nihonjinron discourses that might portray social withdrawal as somehow inherent to Japanese character. Rather, I examine how specific historical developments, social structures, and cultural concepts create particular conditions that facilitate the emergence and persistence of the aging hikikomori in Japan, in ways distinct from social withdrawal behaviors observed in other societies and cultures.
This paper is organized as follows. The first section provides a brief overview of the hikikomori phenomenon in Japanese and English sources that inquire into the emergence, evolution, symptomatology, media coverage, and sociocultural background of this Japan-specific mental health issue. The following sections provide a qualitative content analysis of Japanese online media sources such as news, articles, interviews, and first-hand testimonies that focus on the aging hikikomori phenomenon in the geographical space of present Japan. The discussion dedicated to the empirical findings starts by examining the Japanese media perspective: the overarching themes, frames, the Japanese sociocultural and linguistic representation of this problem, and the manifold challenges arising from this intersectionality of mental health illness and age. Subsequently, it investigates Japanese language blogging content created and distributed by individuals who self-identify as aging hikikomori. This work concludes by summarizing the results and brings into discussion theoretical limitations and methodological challenges associated with this research topic. Finally, I indicate a set of potential future research directions that adopt an intersectional and cross-disciplinary approach.
Literature review
Previous scholarship on hikikomori tends to fall into two major categories: one that assesses the phenomenon solely as a mental health problem rooted in medical, psychiatric, and clinical practice, and another that repositions it within social and human studies.
The vast expansion and richness of research and publications on hikikomori from the perspectives of cultural psychiatry and medicine—here represented by the first subsection “Hikikomori in psychiatry: A theoretical overview of the phenomenon”—come in stark contrast with the consistent absence—or, at least, undeniable scarcity of academic inquiries that tackle the same phenomenon at the conjunction with various other scholarly fields and traditions, such as cultural studies, popular culture, media and communication sciences, Japanese linguistics, literature, and cinema. Likewise, albeit providing a productive, if often challenging repertoire, intersectional investigations—understood here as analytical examinations of how multiple social categories simultaneously shape individual experience rather than operating as discrete variables (Crenshaw Reference Crenshaw1989; Collins and Bilge Reference Collins and Bilge2016)—connecting hikikomori with gender, sex, social class, age, and other disabilities are notably limited. Whereas the general academic research has predominantly focused on younger hikikomori individuals, there is a significant gap in Anglophone scholarship addressing the lives and needs of older and aging hikikomori. This particular area thus requires substantially more research attention and empirical investigation.
However, Japanese-language academic studies—briefly covered in the second subsection, “Hikikomori in the human and social sciences”—are more varied and diverse in their multidisciplinary focus, gathering data from numerous intersection spaces and contexts—mental health clinics, community, and private/personal environments. Noting these initial theoretical limitations, I deliver hereinafter a cursory and selective review of the existing literature, which will encompass both the above-mentioned categories.
Hikikomori in psychiatry: a theoretical overview of the phenomenon
The word “hikikomori” (引きこもり) was coined in the late 1990s by Japanese psychiatrist Saitō Tamaki, who provided in his pioneering study “Hikikomori: Adolescence Without End” (Saito Reference Saitō1998) a first working definition and a sociopsychological portrait of this atypical mental health issue when one ceases all forms of social activities and refuses to leave one’s home (or even room) for more than six months (Kato et al. Reference Kato, Kanba and Teo2019). In addition to this withdrawing condition, it is also employed “as a psychiatric term describing the symptom of withdrawal in autistic, schizophrenic, depressive or aged patients” (Suwa and Suzuki Reference Suwa and Suzuki2013: 2).
The prevalence of hikikomori has steadily grown, reaching an estimated 1.46 million people (日本放送協会 2023). Since 2003, the Japanese Ministry of Health, Labour and Welfare has established a set of defining criteria to assist mental health specialists in the diagnostics and treatment process (Suwa and Suzuki Reference Suwa and Suzuki2013). The defining criteria are as follows: The individual (a) mainly spends time at home, (b) exhibits a lack of will or possibility to engage in social activities (e.g., attend school or go to work), (c) maintains a self-isolation state for a period longer than six months and (d) does not present signs of “neither a psychotic pathology nor medium to lower level mental retardation” (Suwa and Suzuki Reference Suwa and Suzuki2013: 2). Based on “[the] estimated continuous duration of social withdrawal” and the frequency of leaving one’s home, the condition can be categorized as mild (leaving one’s home two to three days/week), moderate (going out one day/week or even less) or severe (refusing to leave one’s room at all) (Kato et al. Reference Kato, Kanba and Teo2020: 117). Furthermore, extended epidemiological data have also revealed that “males [hikikomori] outnumber females by a 3:1 margin or [even] more” (Kato et al. Reference Kato, Kanba and Teo2019).
Besides physical withdrawal and social isolation, which are the main features of this condition, recent psychiatric findings indicate that Japanese hikikomori patients do not purposely avoid social contact and thus maintain “few meaningful social relationships and little social interaction” (Kato et al. Reference Kato, Kanba and Teo2020: 117). Moreover, clinical in-depth interviews have revealed how patients “feel content in their social withdrawal, particularly in the earlier phase of the condition” and even “describe a sense of relief at being able to escape from the painful realities of life outside the boundaries of their home” (Kato et al. Reference Kato, Kanba and Teo2020: 117). Nonetheless, once the duration of social withdrawal is prolonged, the patients state they experience anxiety, depression, and feelings of loneliness (Hamasaki et al. Reference Hamasaki, Pionnié-Dax, Dorard, Tajan and Hikida2020).
Suwa and Suzuki (Reference Suwa and Suzuki2013: 3) propose an alternative framework by introducing “[the] primary hikikomori” to refer to “[the] manifestation of the phenomenon that cannot be described using current concepts in psychiatric disease” and to describe “[the Japanese] youth do not have any serious diagnosable psychopathology, yet they are unable to enter society or adapt to their surroundings.” Likewise, “[the] secondary hikikomori” applies to “individuals suffering [not only from social isolation but also] from a variety of severe mental disorders including affective disorder, anxiety disorder, obsessive-compulsive disorder, personality disorders and pervasive developmental disorders” (Suwa and Suzuki Reference Suwa and Suzuki2013: 3).
Some scholars have focused on online gaming as a triggering factor in the onset and aggravation of the condition, whereas others have extended discussions to correlate internet and smartphone addiction with the risk of severe social withdrawal and hikikomori in Japanese young adults (Tateno et al. Reference Tateno, Teo, Ukai, Kanazawa, Katsuki, Kubo and Kato2019; Rosliana and Widiandari Reference Rosliana and Widiandari2020).
Finally, cross-cultural and cross-national studies broaden the examination to engage with a comparative perspective: Teo et al. (Reference Teo, Fetters, Stufflebam, Tateno, Balhara, Choi, Kanba, Mathews and Kato2014) have compared treatment preferences and psychosocial characteristics of participants across India, Japan, Korea, and the United States, and the empirical findings emphasize “[the] cross-national existence of hikikomori, as a phenotype of severe social withdrawal.” Other similar scholarly endeavors, increasingly emphasizing that hikikomori is not a phenomenon limited to Japan (Figueiredo Reference Figueiredo2024), have adopted the transnational trend by shifting the focal point to disparate countries where cases of the condition have been reported: China (Hu et al. Reference Hu, Fan and Shao2022), Denmark (Eckardt Reference Eckardt2023), Italy (Ranieri Reference Ranieri2015), South Korea (Wong et al. Reference Wong, Wan, Kroneman, Kato, Lo, Wong and Chan2019), Spain (Amor et al. Reference Amor, Córcoles, Sabaté, Moreno, Bergè, Martín-López and Victor2014), Taiwan (Kato et al. Reference Kato, Tateno, Shinfuku, Fujisawa, Teo, Sartorius and Akiyama2011), and others. However, although cases of extreme social withdrawal have been documented globally, Japan continues to report the highest rates of hikikomori worldwide, with its distinctive patterns of prolonged social isolation that align best with the clinical definition of the condition.
Hikikomori in the human and social sciences
From a mass communication perspective, Krysinska (Reference Krysinska2002: 2) was among the first to examine “[the] discourses of media and scholars.” However, as the author herself admits, “[the study] is based on a higher number of media articles published outside of Japan” and adopts a general perspective by ignoring any age or gender intersections (Krysinska Reference Krysinska2002: 40).
Pereira-Sanchez et al. (Reference Pereira-Sanchez, Alvarez-Mon, del Barco, Alvarez-Mon and Teo2019) examined international perceptions of hikikomori by analyzing content on the former social media platform Twitter (now X) in five Western languages—Catalan, English, French, Italian, and Spanish (Pereira-Sanchez et al. Reference Pereira-Sanchez, Alvarez-Mon, del Barco, Alvarez-Mon and Teo2019). Their qualitative and quantitative analysis of the publicly available tweets employing the hashtag #hikikomori revealed that, although the phenomenon is widely perceived as a social and mental problem, the public perspectives maintain a high degree of heterogeneity (Pereira-Sanchez et al. Reference Pereira-Sanchez, Alvarez-Mon, del Barco, Alvarez-Mon and Teo2019).
Keeping the focal point on the same social media platform, Correia Lopes et al. (Reference Correia Lopes, da Costa, Fernandez-Lazaro, Lara-Abelenda, Pereira-Sanchez, Teo and Alvarez-Mon2024: 1) “[have explored] the hikikomori phenomenon in Portuguese, utilizing a mixed-methods approach encompassing content analysis, emotional analysis, and correlation analysis.” Their findings revealed that
Among the total of 13,915 tweets generated, in terms of tone, 10,731 were classified as “negative” and 3184 as “positive.” Regarding content, “curiosities” was the most posted, as well as the most retweeted and liked topic. Worldwide, most of the hikikomori-related tweets in Portuguese were posted in Europe, while “individuals with hikikomori” were the user’s most active posting. Regarding emotion analysis, the majority of tweets were “neutral” (Correia Lopes et al. Reference Correia Lopes, da Costa, Fernandez-Lazaro, Lara-Abelenda, Pereira-Sanchez, Teo and Alvarez-Mon2024: 1).
Additionally, sociology and anthropology scholarship has taken an interest in first-hand testimonies, revealing engaging insights regarding how hikikomori individuals feel socially excluded and marginalized. In his analysis of the autobiographies and private papers written by hikikomori, Kōki Itoh (Reference Itoh2012) connects several narrative frames to the social and national identity discourse of the typical Japanese hikikomori, together with a series of concerns and issues one faces daily: (a) seniority and age difference make even more difficult establishing interpersonal relations at one’s workplace; (b) the existence of blank periods in work and education history negatively impacts future job prospects; (c) the sufferers yearn for finding a partner and there can be much anxiety in respect to love and sexuality (Itoh Reference Itoh2012).
Fong Yong and Kaneko (Reference Fong Yong and Kaneko2016) explored individual experiences from first- and second-person perspectives of people who experienced social isolation and hikikomori syndrome. Their qualitative, in-depth interviews with international participants from Austria, China, and South Korea revealed a complex framework of coping mechanisms, centered on two main categories: “stasis” and “expression.” The stasis category represents a state of psychological paralysis where individuals feel unable to move forward in life. This manifests through four interconnected elements: “hopelessness” (a profound sense of defeat and inability to meet social demands), “relationship fatigue” (exhaustion from social interactions and identity struggles), “inevitability” (a perception of having no alternatives to withdrawal), and “fear” (deep anxiety about social judgment and interaction) (Fong Yong and Kaneko Reference Fong Yong and Kaneko2016). The expression category, on the other hand, describes how these individuals manage their social withdrawal through online spaces. This category encompasses “mistrust” (a defensive mechanism born from past negative experiences), “hindrance” (self-imposed barriers to social interaction), “anonymity” (preference for hidden identity in online interactions), and “transposition” (the shift from real-world to virtual social interactions where they can maintain greater control). Together, these categories reflect how hikikomori individuals both experience their withdrawal and attempt to maintain some form of social connection under their own terms (Fong Yong and Kaneko Reference Fong Yong and Kaneko2016).
Running alongside these investigations of individual testimony and coping experience, a distinct body of scholarship has approached hikikomori through sustained qualitative and ethnographic fieldwork, sharing a methodological orientation that consistently privileges lived experience over diagnostic categorization and resists the reduction of social withdrawal to a clinical entity. What ultimately links these otherwise methodologically diverse contributions is the recognition that hikikomori cannot be reduced to a single register of explanation. Foundational in this regard is Horiguchi (Reference Horiguchi, Holthus and Manzenreiter2017, Reference Horiguchi, Ronald and Alexy2011, Reference Horiguchi, Goodman, Imoto and Toivonen2012), whose ethnographic engagement with hikikomori spans more than two decades and offers one of the most significant accounts in English-language scholarship of how private isolation becomes a public concern. Her research traces how withdrawal is experienced, narrated, and managed within the fabric of Japanese family and social life. It is precisely this entanglement of the private and the public that Tajan (Reference Tajan2021, Reference Tajan2015) pursues into the clinical domain, drawing on extensive interview research with practitioners and a thorough review of the psychiatric literature to argue for reconceptualizing hikikomori not as a syndrome with a coherent clinical profile, but as an idiom of distress. That the clinical and the familial are not separable spheres is further borne out by Rubinstein (Reference Rubinstein2016) and Rubinstein and Sakakibara (Reference Rubinstein and Sakakibara2020), whose 14 months of ethnographic fieldwork with hikikomori families in Japan demonstrates that parents actively construct narrative frameworks around their children’s withdrawal, and that hikikomori operates simultaneously as a social, moral, and medical category—a finding that substantially complicates any reading of the phenomenon as either purely pathological or purely sociocultural. If Rubinstein reveals the moral work done within the family, Dziesinski (Reference Dziesinski2004, Reference Dziesinski2003) pushes outward to interrogate the broader discursive field, examining the gendered and class-inflected dimensions of hikikomori discourse, questioning its predominantly male-focused framing, and exposing the normalizing logics embedded in rehabilitation practices.
Rosemary Overell adopts a queer-centered framework in portraying “hikikomori as willful subjects [who] constitute a challenge to dominant national imaginaries of Japan as a ‘corporate-family system’” (Reference Overell2018: 206). Although this approach represents an ambitious departure from mainstream research, it misses key contributions and media representations pertaining to Japanese popular culture and media, as it focuses solely on Takimoto’s emblematic novel “Welcome to N.H.K” (N.H.Kにようこそ!) and several clinical accounts. Furthermore, Overell claims without any further theoretical support that “[in] Japanese media and popular clinical accounts, hikikomori are framed as childishly lazy—as parasaitô (parasites) whose willful withdrawal drains both their immediate family and the national family of the Japanese state” (Overell Reference Overell2018: 206). Nonetheless, my previous in-depth analysis of hikikomori representations in Japanese popular culture-specific genres has emphasized that
The [media] productions create a congruent, vocal, and safe space of empowerment and self and collective healing [by] giving a voice to the sufferers and their families. [In fact, one of the significant functions of Japanese popular culture is to provide] an alternative and safe place for dialogue, reflection, and a metaphoric and subtle critique of Japan’s most stringent contemporary problems that would otherwise be difficult to approach directly” (Pelea Reference Pelea and Pelea2024: 40).
While examining “hikikomori” and “tojikomori” (閉じこもり), Yong et al. note important differences between these conditions. “Tojikomori” is commonly defined as “going out less than once a week and not requiring nursing care,” while hikikomori involves more severe and prolonged social withdrawal. Furthermore, the aggravation of hikikomori is closely linked to systemic issues in Japanese society, including deficiencies in the social support system and persistent community prejudices (Yong et al. Reference Yong, Nomura, Takatsuka, Imuta, Taniguchi, Ito, Ohira and Tatsumi2022).
The successful social reintegration of hikikomori requires a complex, person-centered approach that considers each individual’s unique life circumstances (kobetsusei, 個別性) and personal values (taishōsha no kachikan, 対象者の価値観) (Yong et al. Reference Yong, Nomura, Takatsuka, Imuta, Taniguchi, Ito, Ohira and Tatsumi2022). Whereas Japan has established various support systems, there remains a critical need for better coordination among different professional sectors. Treatment practices would be most effective through systematic interdisciplinary collaboration among professionals from mental health, clinical care, nursing, social work, sociology, and anthropology, to name but a few (Yong et al. Reference Yong, Nomura, Takatsuka, Imuta, Taniguchi, Ito, Ohira and Tatsumi2022). Nonetheless, at this moment such services often operate in isolation rather than as an integrated support system, thus limiting their effectiveness in addressing the multifaceted and complex necessities of hikikomori individuals.
Additional scholarly contributions have expanded understanding of aging hikikomori through various methodological approaches. Yakabe and Murakami (Reference Yakabe and Murakami2020) employ quantitative analysis to examine the life challenges faced by middle-aged and elderly hikikomori. Hasegawa et al. (Reference Hasegawa, Sakuramoto, Nagai, Tamaoka, Sawada, Kishimoto, Ono and Shimmura2019) investigate the relationship between oral health deterioration and social withdrawal, suggesting that difficulties in eating, speaking, and swallowing may increase isolation among elderly individuals by limiting their social interactions. Hiyoshi (Reference Hiyoshi2023) provides a comprehensive review of research on social isolation and loneliness in Japan, while Kotsuji (Reference Kotsuji2022) and Tsujimoto et al. (Reference Tsujimoton.d.) further contribute to this growing body of literature examining the intersections of aging and social withdrawal.
Methodology
Primary objectives, research questions, and method of analysis
The primary objectives of this analysis are to examine (i) the representation and (ii) the self-representation of aging hikikomori individuals across Japanese language media. To complement the general aim and the objectives, I pose the following research questions.
-
1. How do Japanese language media outlets portray the aging hikikomori individuals?
-
2. What are the main themes and narrative framings associated with this phenomenon in Japanese language media?
-
3. How do aging hikikomori individuals describe themselves and communicate in Japanese language media and the blogosphere?
-
4. What are the dominant topics within the media and blogging content authored by the Japanese aging hikikomori individuals?
-
5. Are there any significant differences between representations of aging hikikomori in Japanese language media and their self-representation in online spaces?
As a working method, qualitative content analysis was deemed most appropriate. This method not only facilitates a thorough and comprehensive examination of Japanese written media sources, but also offers distinct advantages for analyzing online content. Digital media sources provide real-time updates, enable access to a broader range of voices including personal blogs and social media, and allow for the examination of interactive elements such as comments and responses—features not available in traditional print media. Additionally, blogging platforms often contain more informal and candid discussions of hikikomori experiences than conventional media outlets.
Search method, data collection, selection, and coding procedure
A Google-based search was conducted using the following Japanese language keywords: 引きこもり and ひきこもり (hikikomori) AND 高齢者 (elderly person) OR 中高年 (middle and old age) OR 高齢化 (aging) OR シニア (senior) in combination with other keywords that helped to generate Japanese language media content: メディア (media) OR 新聞 (newspaper) OR 記事 (newspaper article) OR ニュース (news) OR 社説 (editorial) OR 主張 (opinion) OR インタビュー (interview) OR マスコミ (mass communication) OR ブログ (blog). Various combinations were used to compile the database.
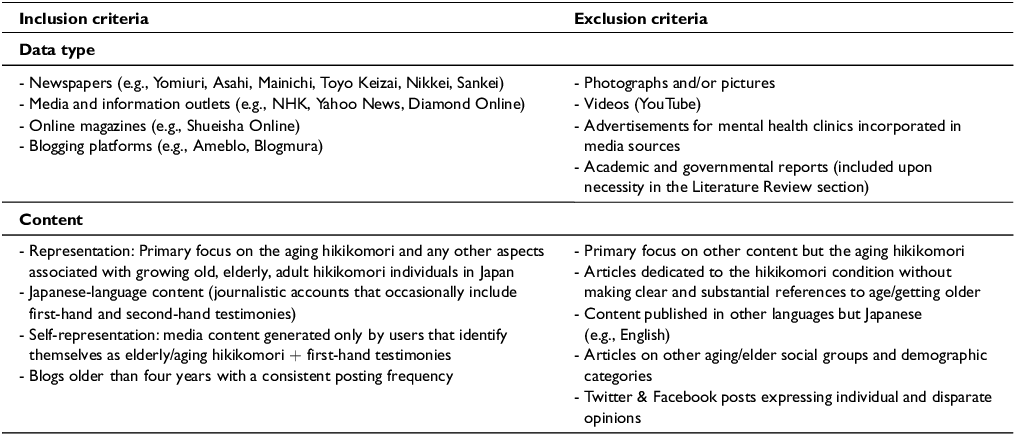
The data collection process took place between May 15 and June 1, 2024, and targeted media content was published from January 1, 2019, to May 15, 2024. All sources included in the dataset were freely accessible online at the time of data collection and did not require subscription or institutional access. Table 1 provides a summary of the inclusion and exclusion criteria employed throughout the search data process and compilation of the database.
Summary of the inclusion and exclusion criteria

Table 1. Long description
The table presents the inclusion and exclusion criteria used in a data collection process. It includes two main columns: Inclusion criteria and Exclusion criteria. The Inclusion criteria column lists data types such as newspapers, media and information outlets, online magazines, and blogging platforms, along with specific examples. It also details content criteria, focusing on the representation of aging hikikomori individuals in Japan, Japanese-language content, self-representation in media, and blogs with consistent posting frequencies. The Exclusion criteria column lists items such as photographs, videos, advertisements, academic and governmental reports, content not focused on aging hikikomori, articles without clear references to aging, content in languages other than Japanese, articles on other social groups, and social media posts expressing disparate opinions. The table has multiple rows under each criterion, detailing specific examples and conditions. The data collection process took place between May 15 and June 1, 2024, targeting freely accessible online media content published from January 1, 2019, to May 15, 2024.
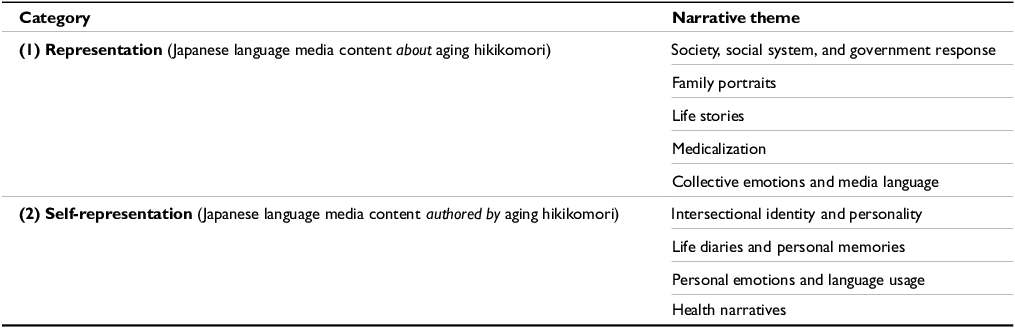
In the first stage, the coding procedure adopted a deductive approach by organizing the content into the following categories: (1) representation and (2) self-representation. The first category encompasses 106 Japanese language media articles about the chosen topic, whereas the second category comprises 82 media articles authored by individuals who identify themselves as Japanese and aging hikikomori individualsFootnote 2 —in most cases, blog posts corresponding to 8 blog sources, situated within a broader tōjisha self-representation tradition that includes dedicated platforms such as HIKIPOS (ひきポス). The second stage of the coding procedure—the inductive approach—generated narrative themes for each category mentioned above based on content similarities and overarching directions. The themes are neither strictly delimited nor mutually exclusive and may overlap or intersect by case. The findings are listed in Table 2.
Overview of the empirical findings: narrative themes across each category

Table 2. Long description
A table with two rows and five columns compares narrative themes across two categories of Japanese language media content about aging hikikomori. The first category, representation, includes themes such as society, social system, and government response, family portraits, life stories, medicalization, and collective emotions and media language. The second category, self-representation, includes themes such as intersectional identity and personality, life diaries and personal memories, personal emotions and language usage, and health narratives.
Worth noting is the temporal fluidity that characterizes several of these self-representations: some bloggers describe their condition using “former/current” language, and several explicitly document within their posts the experience of relapsing into more severe withdrawal after periods of partial recovery. Rather than constituting a methodological flaw, this fluidity reflects the non-linear and unstable trajectory of hikikomori well-documented in clinical literature (Kato et al. Reference Kato, Kanba and Teo2019, Reference Kato, Kanba and Teo2020), and is itself analytically significant—capturing the lived experience of a condition defined not by fixed states but by oscillation, partial recovery, and relapse, in which the blog functions as a longitudinal record of ongoing negotiation rather than a stable identity.
Finally, clarifications regarding the ethical dimension of the methodology are required. Albeit working with mental health-related data connected with particular individuals, I operated with online media content that was already publicly available. Thus, I did not need to obtain any ethical approval or informed consent before undertaking this study. Direct quotations of first and second-hand testimonies are followed by the web source—title, link, publication date, and other relevant information that allow the identification and localization of the statements in public cyberspace.
Empirical findings: Japanese media framings and overarching themes
Before presenting the thematic findings, an analytical observation about the nature of this dataset itself is warranted. Identifying as aging hikikomori, the bloggers analyzed below are, by clinical definition, withdrawn from society—and yet what they collectively produce is unmistakably public: posts addressed to readers, content organized chronologically and tagged by life phase, autobiographical narratives constructed to be followed over time. Crucially, this is not private journaling. Humor, self-deprecation, moral argument, social greeting—none of these communicative acts function without an audience. What these bloggers are doing, in other words, is not simply making content available but performing for readers, actively constructing a public self through sustained, organized, socially addressed writing.
Equally revealing is what anonymity actually does in this context. Rather than operating as concealment, it functions as selective disclosure: a mechanism for controlling what is revealed, to whom, and under what conditions—including, significantly, whether a post remains visible at all. Coexisting with a preference for hidden identity are explicit disclosures of sexuality, psychiatric diagnoses, developmental disorders, and family conflict—precisely the intersectional dimensions that institutional media, as demonstrated in the preceding section, systematically flattens or ignores. Digital space enables here not a substitute for offline sociality but a structurally different mode of self-presentation: one in which layered, complex identities can coexist without the social consequences that offline disclosure in Japan would carry. Where face-to-face interaction imposes the simultaneous visibility of all aspects of a self, the blog permits their careful, sequential, self-governed revelation.
What this points toward, crucially, is not avoidance of social interaction as such, but avoidance of uncontrolled social interaction. The terms of engagement belong entirely to the blogger—when to write, what to share, whether to respond, whether to delete. Far from marking absence, the chronological organization of posts into navigable life histories suggests something fundamentally social: these individuals are constructing autobiographies for an audience, not withdrawing from one. Digital environments, in this light, do not simply compensate for lost offline sociality—they reconfigure the conditions of social participation entirely, making possible forms of self-expression and community-building that the structures of offline Japanese social life foreclose.
The two categories structuring this study are therefore not merely methodological—they reflect two distinct subject positions that the data makes difficult to collapse. Institutional media produces the aging hikikomori as a passive object of medical concern, familial burden, and social crisis. The blogosphere produces the same individual as an active, articulate speaking subject, constructing a public self on their own terms. Both populations are simultaneously isolated in institutional terms—physically absent from workplaces and public spaces—and yet can be socially present through sustained communicative practice. The blog is not where this paradox is resolved. It is the site where both conditions are lived at once, and where the clinical equivalence between physical withdrawal and social absence breaks down most visibly.
Representation of the aging hikikomori phenomenon in Japanese language media
Society, social system, and government response
One of the most recurrent themes is referring to the condition as a “serious and social problem” (社会的な問題 ・深刻な問題), which becomes unavoidably connected with other stringent issues, such as Japan’s “super-aged society” (超高齢化社会) and the nation’s fast-aging speed (超高齢社会の加速) (Nikkei 2022). The coined expression “the 8050 problem” or its close alternative, “the 9060 problem,” echoes this media tendency to problematize the identity of aging hikikomori, and succinctly encapsulates the image of a struggling household—or even on the verge of poverty—in which parents in their 80s/90s support their unemployed and usually self-isolated children, who are in their 50s/60s (Nikkei 2022). Furthermore, what seems to perpetuate the pervasive negative depictions surrounding this phenomenon is the intensive media coverage that connects manifold forms of physical and psychological violence in relation to the sufferers. As such, many news articles cover details about extreme forms of violence, such as parental and filial homicide or improper storing of human remains. In this regard, the following headlines are illustrative and certainly not exhaustive:
Spending 35 years in self-isolation, without smartphone or internet: The confession of a 61 years old who killed his parents (Uchiyama Reference Uchiyama2023) [and] hid [their] bodies in the refrigerator (Yotemira 2022).
“My parents are to blame for me turning into a hikikomori.” Recounting the murder of his parents (Daily Sun New York 2023).
What drove a 79-year-old woman to kill her elderly sister and her hikikomori son: Excessive spending [of the son] and [the necessity to] provide care [for the sister] (Takahashi Reference Takahashi2023).
The absence of adequate institutional support mechanisms, slow-moving legislative processes that fail to deliver stronger social protection, and an overall deficient welfare system are depicted as primary causal agents behind the domestic violence embedded within the self-isolation pattern. One article, for instance, discusses the issue of aging and self-isolating individuals as arising from a far larger and more complex problem, the institutional, systemic failure of nursing the elderly:
Elderly people living alone are more likely than teenagers to become hikikomori. Being of old age is a hell in Japan. Every year, there are 200–300 suicides while under nursing care. 5% of the murder events are connected with nursing. How did this happen (Wada Reference Wada2023)?
Life stories
This theme reflects how Japanese language media communicates personal memories, first-hand testimonies, biographical perspectives, and statements of the aging hikikomori individuals. While focusing on the personal identity and psycho-emotional torment of the sufferers, this content inevitably reveals intersectionality related concerns, more precisely, long-term unemployment, social alienation, marginalization, extreme poverty, depression, suicide ideation, and even death by starvation. The following media account from Yahoo News Japan provides a glimpse into the impoverishment that accompanies this solitary lifestyle:
“I watch nothing but Korean dramas every day.” [As] a 65-year-old single person living alone with a retirement allowance of 10 million yen (approximately $67,000) and a pension of 130,000 yen (approximately $826) … I can’t [afford to go] to a nursing home. (…) The elderly hikikomori → the certain trajectory to dying alone (Yahoo News Japan 2024a).
The financial struggles and the haunting fear of poverty and starvation become stereotypical depictions, and successful recovery stories are few to notice:
[I am] living from day to day on my 92-year-old father’s monthly pension of 230,000 yen… in a dimly lit room… I’m not afraid of dying alone. I don’t think it can be helped if I run out of food and can’t do anything. (…) Even after I quit my job, my father continued to contribute to the national pension plan out of concern for my future, so when I add in the employee pension from my former job, it comes to about 100,000 yen a month. I also have a life insurance from my father. [Even after turning 65], I [should have something] to eat. What should I do? What do you think I should do? (Yahoo News Japan 2024b)
Family portraits
First-hand testimonies and narratives focusing on family voices reveal a dominant media framing: intergenerational trauma within families affected by hikikomori. This framing consistently emphasizes the emotional and financial burden on elderly parents who must continue providing care and support for their aging hikikomori children well into their own retirement years. The Japanese expression “old people providing care for old people” (老老介護, rōrō kaigo) captures this dynamic and takes on particular significance in hikikomori cases, where aging parents face a double burden: managing their own aging-related needs while sustaining adult children unable to live independently. The cultural expectation that adult children support their aging parents is thereby inverted, placing sustained strain on the family unit.
Likewise, healthy siblings face difficult decisions once their parents pass away (Kuroda Reference Kuroda2023). One relevant example can be observed in the writings of freelance journalist Masaki Ikegami, the founder and vice-president of an organization dedicated to the families of the hikikomori (KHJ National Federation of Hikikomori Family Associations 2024, hereinafter KHJ NGO), who has been covering this topic for 28 years (Ikegami Reference Ikegami2023a). His writing, inspired by the personal experience of having a hikikomori younger brother who passed away at the age of 49, is accompanied by photographs and represents the portraits of other struggling families and their accounts of silent suffering:
My younger brother also died [because of his long-term condition as a] hikikomori, so I can understand the feelings of the siblings. (…) I should have told him that I wish him to live. (…) What families need to understand is that the most important thing is to live (Ikegami Reference Ikegami2023b).
In other cases, scanned pages of the parents’ diaries re-memorizing the unbearable anguish, torment, and worries (Morita Reference Morita2022) imbue the media articles with a documentary and literary value of “realness” that seem to function both as a self-therapeutic strategy for the grieving families and as a stimulus for collective empathy and raising social awareness:
A man who was a hikikomori for 18 years discovers a note from his parents who passed away: “Our family just can’t take it anymore” (Nishinippon 2022).
Such rhetoric highlights how culturally embedded concepts such as sekentei (social reputation) and haji (shame) intensify the stigma surrounding the phenomenon, explaining why parents often conceal their children’s condition from outsiders.
Medicalization
By predominantly framing the condition as a “health problem,” a wide range of published media content adopts a health communication perspective, delivering medical information and healthcare knowledge in an accessible manner to support aging individuals facing self-imposed social isolation. Critical information about support services is disseminated through multiple channels reaching millions of Japanese households: major national newspapers (with combined circulation of over 20 million), public broadcasting networks (NHK reaches 99% of households), regional health centers (480 nationwide), and nonprofit organizations’ websites and social media platforms. This information includes guidance about public health services, details about nonprofit support organizations, self-coping methods (e.g., advice on building self-confidence, joining “shopping clubs,” 買い物グループ, or practicing e-sports, e スポーツ), and family support resources (Chunichi Newspaper 2023; Ueda Reference Ueda2023; 47 News 2024).
Nonetheless, medicalization here adopts a multidisciplinary and holistic care approach, for it integrates information useful to ease one’s mental condition and educate and increase social awareness, family communication, society reintegration, and community support. Oftentimes linked with the health frame is another Japanese-specific culture-bound syndrome, taijin kyofusho (対人恐怖症). This social anxiety disorder frequently co-occurs with hikikomori and receives similar medical attention in Japanese healthcare contexts. Both conditions are approached through the health communication framework, with medical professionals treating them as interrelated mental health challenges that require coordinated clinical intervention. Like hikikomori, taijin kyofusho is characterized by social withdrawal behaviors, though specifically driven by “intense fear that one’s body parts or functions displease, embarrass or are offensive to others” (Essau et al. Reference Essau, Sasagawa, Ishikawa, Okajima, O’Callaghan and Bray2011).
The triggering factors and mechanisms that exacerbate an aging person’s overall fragile mental health status seen in culture-bound syndromes such as hikikomori as well as social anxiety disorder are of various types. The first category is predominantly connected to one’s social co-participation. As such, in the case of the middle-aged group, retirement, job loss, unstable work environment, and work-related anxiety are highly likely to be connected with the onset of the cultural syndrome (Sagasix 2020). The second category reflects the psychological component and one’s (in)-ability to establish and maintain social relations, face-to-face conversations, and overall distrust in human relations (ningen fushin, 人間不信) (Sagasix 2020). The third type of high-risk factors includes physical, mental, and chronic associated illnesses and time-consuming recovery that increase the difficulty of the patient’s (re)-integration into society. Finally, sociocultural implications are not overlooked: Family members might express fear and avoidance in disclosing their aging children’s sensitive situation. Such parental attempts to hide the issue reveal, to some extent, the perpetuated sociocultural prejudice and stigma attached to the condition (Sagasix 2020).
Collective emotions and media language
In addition to the above-identified narrative directions that compartmentalize social and medical framings, national perceptions, and individual and family experiences, Japanese media construct and circulate what I identify as collective emotional responses—shared feelings, affects, and anxieties that emerge in reporting about aging hikikomori. The emotions encompassed within the broader media assemblage negotiate from a sociolinguistic perspective the existing tensions experienced and articulated nationally by public audiences and highlight a Japanese-specific and socioculturally structured way of reacting toward this phenomenon. Albeit not impossible, translating emotions and affect-related terms is highly likely to encounter translatability difficulties and the risk of losing Japanese-cultural-specific nuances and subtleties. Without necessarily aiming to deliver hereinafter a detailed semantic analysis, several examples reveal translational challenges into Western languages and across other geographical contexts: 孤立感 (koritsukan, feeling of being isolated), 孤独感 (kodokukan, feeling of loneliness and isolation), 絶望 (zetsubō, despair, hopelessness), 不安 (fuan, anxiety, worry, fear), 迷惑 (meiwaku, bother, nuisance), 孤独死 (kodokushi, dying alone), 罪悪感 (zaiakukan, feelings of guilt), and 地獄 (jigoku, hell, misery).
Frequently describing the hikikomori biographical accounts circulated by the media are emotions whose cultural specificity lies not in the feelings themselves but in their socioculturally structured discursive articulation within the Japanese context (Essau et al. Reference Essau, Sasagawa, Ishikawa, Okajima, O’Callaghan and Bray2011; Suwa and Suzuki Reference Suwa and Suzuki2013)—notably 不安 (fuan, anxiety) and 迷惑 (meiwaku, nuisance).
Likewise, 孤独死 (kodokushi, dying alone), 引きこもり死 (hikikomori-shi, hikikomori death), and associated emotionally intense repertoire become a salient textual motif that emphasizes the sociopsychological vulnerability of such individuals. On the one hand, the sufferers are portrayed as presenting signs of inevitable physical and psychological weakness due to a variety of factors—age, decaying physical condition, financial restrictions, and prolonged self-isolation. On the other hand, they exhibit (nationalized) fears and worries that iconically echo Japanese culture-specific moral values, obligations of social relationships, and, overall, deeply embodied social customs. This observation draws upon numerous Japanese media discursive stances seeped with the sufferer’s apprehension and guilt that one might become a [social] burden (家族に厄介をかけている ・家族に迷惑をかけている) or fail to contribute to one’s family and society as a whole (自分の世話のために家族が仕事を辞めた ・自分のせいで娘や嫁が家事や子育てを十分できない) (Wada Reference Wada2023). Nonetheless, some media sources are making important efforts to challenge and deconstruct the prevailing negative stereotypes and derogatory labels traditionally used when discussing hikikomori. What describes these labels are well-ingrained sociocultural and semantic markers that portray the hikikomori as being “a spoiled and immature teenager” (amae-wakamonotokuyū no shinri, 甘え ・若者特有の心理) or the failing result of deficient parental education (NHK 2022).
Self-representation of aging hikikomori individuals in Japanese language media
Intersectional identity and personality
Whereas the above-described diversity of Japanese journalism practices typically focuses on self-isolation as the primary characteristic of hikikomori, with only occasional attention to gender, sexuality, disability, or social class, aging hikikomori individuals themselves often emphasize how these multiple aspects of identity intersect and shape their experiences. For example, one blogger self-describes as gay and hikikomori: “What was I first? Gay or hikikomori? I am a gay and former/current hikikomori man in his 50s, and I write about my thoughts” (Gay or Hikikomori Blog 2024). Likewise, a profile I identified at the point of intersection belongs to a disabled mother, aged 59, who claims to struggle with manifold “mental and physical disabilities” (Noaah 96178 Muragon Blog 2024a). Another one links emotional and developmental disabilities with his state of prolonged and voluntary isolation:
[I am] a 46-year-old NEET with a history of 15 years as a hikikomori, no working experience and a developmental disorder. [I have] been fighting depression for 30 years. [I write] about depression, hikikomori, family problems, communication and developmental disorders. For some reason, I couldn’t adapt to society, and I reflect upon the past and how to recover from depression (Asitaba Blog 2024).
In addition to the limited working experience and absence of proper education, the geographical factors, more precisely, the rural-urban divide, entangle with other forms of marginalized identity and can predetermine economic disparities and precarious living circumstances:
Is there a tomorrow for the hikikomori people? [I am] a 49-year-old man who has a 29-year history as a hikikomori. [I also suffer from] depression, schizophrenia and taijin kyofusho. (…) Living in the countryside in the Hokkaido. My target is social rehabilitation and reintegration into the society (Hikikomori 1220 Blog 2023).
Addictions to video games, alcohol, or painkillers are also mentioned and thus speak of the intersectional complexity of the sufferers and their identities, which prove to include more than old age and self-isolation.
Life diaries and personal memories
A common element shared by many narratives across the blogging spaces indexed by the present research is the overwhelming emphasis placed on recounting personal memories and unfolding trauma rooted in one’s past. Commenting on the development and evolution of personal trauma and suffering, the following account connects toxic parenthood with the worsening of his hikikomori condition:
My parents have morally harassed me. When I was younger, I was a hikikomori, and to fix me, my parents tried to take me to various psychiatrists. I think that all began when I didn’t want to follow the career path my parents wanted (…). And I turned into a hikikomori. I had to go to psychotherapy, but it was too much for me. When I refused to go, my parents lost their temper and started yelling at me. It went on for hours. My heart was utterly broken. I thought I lost any hope to recover. It was then I relapsed even harder as a hikikomori, and this triggered my panic disorder and depression. It’s been thirty years since then, and when I think back to those days, all I can feel is anger (Pchan59 Blog 2024).
Likewise, the link between prolonged and voluntary self-isolation, problematic family relations, and deficient communication is further compounded by another account as follows:
Born in 1972, I am a middle-aged gay man. About 30 years ago, when I was 19 years old, I was a shut-in for about two and a half years. After that, I worked intermittently but became unemployed again for four years. I am currently living with a partner who became physically disabled due to side effects of anti-cancer drugs. I think that I became a hikikomori not because of bullying, parental abuse or power harassment but because of the overprotection and over-interference [exerted by] one of my parents (Gay or Hikikomori Blog 2024).
In fact, many blogs provide means to frame life stories and thus become personal and almost intimate spaces that allow autobiographical writing, usually enhanced by photographs. Therefore, the reader can easily navigate through the published content by using tags specific to different phases of life, such as “childhood,” “adolescenthood,” “high school years,” and so on.
Personal emotions and language usage
Hikikomori autobiographies prove to be a fruitful source of insight into the sufferers’ emotional states, which tend to link illness closely in its manifold variations with depression (clinically diagnosed but also undiagnosed), anxiety, fear of failure, future-related anxieties, stress, memories of trauma, death, and even suicide ideation.
Probably, I’ll die soon. This is the reason why I’m writing a farewell note. It is a farewell note for me in my future life. [Something] I wish I would read in my future life (Pchan59 Blog 2024).
Similarly, another blogger states:
The Naoki Prize-winning author Aiko Sato [once] said, ‘Dying feels like a relief.’ She also added, ‘(…) because life isn’t something that special.’ I feel the same way. It doesn’t mean I disregard [neither] life [nor] death. [But there is this idea that] living a long life is a valuable and precious thing and (…) if you commit suicide, you will go to hell. Very important for me are to live a good and wealthy life, become someone respected and honorable, and be hardworking (Cqe 22242 Muragon Blog 2024).
As these and many other narratives illustrate, a pessimistic and fatalistic outlook on life and the future is among the most adequate to characterize the predominant tone of the blog posts.
However, a salient and culture-specific feature of the communication style involves the frequent presence of the self-deprecating and humble language (kenjōgo, 謙譲語). Whereas Japanese mainstream newspapers and magazines operate near political correctness-imposed boundaries, bloggers face no constraint and write according to their wishes. Their language choices often include terms that would be considered inappropriate or too informal for public broadcasting: “fool” (baka, バカ) (Cqe 22242 Muragon Blog 2024), “poor” (binbō, 貧乏), regionally marked language such as “from the countryside” (inaka, 田舎) (Hikikomori 1220 Blog 2023)—a term typically avoided in mainstream media’s broadcasting guidelines (hōsō kinshi yōgo, 放送禁止用語)—and casual age-related descriptors like “bald, old man” (oyaji, おやじ) when referring to themselves (Cqe 22242 Muragon Blog 2024). This linguistic freedom reveals expressions of identity that diverge significantly from the carefully regulated discourse of institutional media.
Furthermore, as the following example shows, one commonly employed tactic is humour and self-irony: “I am an old man with no hair left on his head, no money, no children, and a wife. Nice to meet you [all]” (Cqe 22242 Muragon Blog 2024). Misogynistic comments—“Are women stupid or what?” (Pchan59 Blog 2024)—and ironic and critical opinions related to either sensitive socio-political and historical issues (e.g., related to South Korea) or national political figures reveal, on the one hand, the low degree of self-censorship of the bloggers, and on the other hand, the emotional distress and high dissatisfaction, otherwise suppressed and silenced in real life.
Health narratives
This theme encompasses health-related aspects, concerns, and issues prominent in many blog posts: physical health (asthma, cancer, stroke, hay fever, and ureteral stones), mental health (depression, schizophrenia, smoking, video games, and pachinko addiction), or therapy and healing (counseling and regular medical check-ups) (Asitaba Blog 2024). Negative experiences with doctors become a source of incredible frustration for many bloggers, who complain of a perceived lack of empathy, responsibility, and respect within the patient–doctor dynamic. One has even described her interaction with the medical staff as “the worst,” with healthcare professionals acting “very arrogant” and laughing at her medical condition and “lack of knowledge” (Noaah 96178 Muragon Blog 2024b). Additionally, the content touches upon the financial hardships, which are looked upon as a significant hindrance in having access to proper medical treatment and sufficient therapy resources.
Conclusions and future research avenues
Very little is known—empirically speaking—regarding how Japanese language media frames the social phenomenon of the aging hikikomori. In addition to filling this gap by delivering the first-of-its-kind empirical-rooted research on this topic, two major categories emerged from the qualitative content analysis: representation and self-representation.
While Japanese media tends to frame the phenomenon from a central perspective, bloggers’ discursive strategies rely more on intersectionality and intertwine this issue with other mental, behavioral, and physical disorders and disabilities. The choice of language and terminology depends on the media type. In other words, in the case of traditional media outlets—newspapers, magazines, and television broadcast websites—the use of the Japanese language is regulated to match the standards of political correctness. However, Japanese bloggers who self-identify as “aging hikikomori” individuals reject any form of euphemistic lexicon and embrace a self-derogatory linguistic style.
Although this is among the first English-language studies to empirically investigate the Japanese language media framing of the aging hikikomori, this research is necessarily constrained in scope and thus presents several limitations. In order to ensure the proper management of the database, I have purposely ignored audio-video media sources (e.g., television documentaries) and have limited the working sample to online media articles.
Considering the richness and high availability of blogging content authored by individuals who self-describe as “aging hikikomori,” the self-representation category could readily have been extended into an independent study. For these individuals, blogging appears to serve multiple vital functions: it provides a controlled environment for self-expression where they can manage social interaction on their own terms, offers a platform for processing trauma and personal memories, and creates a quasi-extension to the outside world without the pressures of direct social contact.
Unlike traditional media portrayals that often emphasize the medical or social welfare aspects of aging hikikomori, these blogs reveal intimate personal narratives that showcase how individuals navigate their identities at the intersection of aging, social withdrawal, and various other personal circumstances such as disability, gender, and sexuality. This digital self-representation thus becomes not merely a diary of isolation, but rather a carefully constructed bridge between complete withdrawal and selective social engagement—one that, by its very nature, can only be built by those whose condition still permits some degree of outward communicative engagement. Those at the most acute end of the withdrawal spectrum, for whom any sustained public expression remains impossible, are structurally absent from blog-based datasets—not by virtue of social or material disadvantage, but because the condition itself at its most severe forecloses the very communicative capacity that blogging requires.
Beyond these immediate concerns, aging hikikomori individuals face increasingly complex challenges as their elderly parents—often their sole caregivers and financial supporters—become unable to provide care due to their own aging-related health issues or death. Media reports document troubling cases of what some call “hidden homelessness” (kakureta hōmuresu, 隠れたホームレス)—aging hikikomori continuing to live in family homes after their parents’ deaths, sometimes without utilities or proper nutrition, surviving on inherited savings until resources are depleted. The most severe cases involve complete social isolation with no institutional awareness of their existence, creating risks for what has been termed as “lonely deaths” (kodokushi, 孤独死)—unreported deaths discovered only months or years later.
Government initiatives to address these challenges remain underdeveloped, with only 56 specialized support centers nationwide as of 2023, creating critical service gaps particularly in rural areas (Ministry of Health, Labour and Welfare 2023). The 2022 expansion of the framework through the “Hikikomori Support Station” program represents an attempt to address these shortcomings by integrating consultation support, community space creation, and network building at the municipal level. However, a fundamental disconnect persists between the design of these systems—which presuppose individuals actively seeking assistance—and the defining characteristic of hikikomori, which is extreme reluctance to engage with social institutions (Ministry of Health, Labour and Welfare 2023). Thus, despite the multilayered approach including satellite offices, financial assistance to smaller municipalities, and resources such as the “Hikikomori VOICE STATION” portal site, the practical reach of these initiatives remains limited. In addition to the Community Mental Health Support Centers (Chiiki Seishin Hoken Fukushi Sentā, 地域精神保健福祉センター), which have developed programs specifically targeting older hikikomori and provide opportunities such as community gardening projects and traditional crafts workshops, nonprofit organizations like the KHJ National Federation of Hikikomori Family Associations have pioneered family-centered support systems that work within Japanese family structures, acknowledging the cultural complexities of dependency and obligation.
Finally, in terms of future research directions, cross-cultural and cross-linguistic comparative studies on the same topic regarding media’s discursive strategies can be further developed in the future to examine locale-specific discursive configurations and framings: Are there any differences in the way South Korean, Hong Kong, Chinese, and Taiwanese media report on hikikomori individuals across various Asian geographical contexts?
Note
The translations from Japanese to English presented in this paper are the author’s original work, unless stated otherwise, and were specifically prepared for the purpose of this research.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Competing interests
The author declares no competing interests.
Author Biography
Dr. Cringuta Irina Pelea is a Lecturer in Communication Sciences at Titu Maiorescu University, Romania. Her research examines power dynamics, marginalized identities, and the representation of vulnerable populations across discourse and cultural contexts, with a particular focus on Japan and Japanese-language media. She is the editor of Culture-Bound Syndromes in Popular Culture (Routledge, 2023) and an editorial board member for the Routledge Handbook of Language and Mind Engineering (2024). Her work appears in the Routledge Companion to Literature and Social Justice (2023), the Routledge Handbook of Endangered and Minority Languages (2025), Future of Media in Asia (Springer, 2025), Fashioning the Asian Century (Bloomsbury, 2025), and Discourse & Society (2026).

 Open access
Open access