

Introduction
Medical students come to the field with a range of pre-existing competencies, attitudes, cultural assumptions, privilege and values. Medical educators must teach, train, supervise and assess, but they may also hold other roles simultaneously, acting as managers, employers and senior colleagues. Because of the breadth of workplace-based learning required in medicine, most doctors teach, beginning when they are in quite junior roles. Almost invariably, clinicians take on these roles without any training or experience in management, education, or assessment. Medical educators also facilitate professional identity formation, acting as mentors and role models. Some of these roles may be difficult to integrate, because they have contradictory goals and require different pedagogy. The situation is made more complex by the increasing role of interprofessional learning across the variety of clinical disciplines and professions present in the health care workplace.
In this chapter, we examine several core responsibilities of medical educators in the field of professionalism. First, medical educators are responsible for teaching and assessing professional conduct, and where possible, remediating poor performance. They are also responsible for selecting suitable medical students, and graduating doctors who demonstrate appropriate professional conduct. Finally, medical educators lead educational teams, managing the multiple roles of supervising, teaching, assessing and managing learners, and in doing so, they create, sustain and manage the hierarchies in which sexual harassment often occurs.
Professionalism in the Curriculum: Defining Competencies
Professionalism is a conceptually complex idea, that encompasses a number of dimensions that appear easy to understand in principle, but remarkably difficult to operationalise in practice. At its most basic, professionalism ‘signifies a set of values, behaviours, and relationships that underpins the trust the public has in doctors’. (Reference Birden, Glass, Wilson, Harrison, Usherwood and Nass1) While it is easy to agree that doctors should demonstrate psychologically safe interpersonal behaviours, defining what those behaviours are in any given context of place and time can be challenging. This complexity is represented in the multiple codes of conduct under which doctors train and work. Integrating expectations from workplaces, training institutions, regulatory organisations, legislation and other codes requires enormous flexibility on the part of medical educators in a highly dynamic area of practice.
At present, there is an emphasis on competency-based curriculum and assessment, and so professionalism tends to be captured in these expected codes of practice (see chapters 6 and Reference Wilkinson, Wade and Knock13). These competencies are represented in the written curriculum, where expected behaviours are defined, taught and assessed. Ideally, of course, the doctor in training will demonstrate their knowledge of expected behaviour, but will also consistently demonstrate these skills in an authentic professional environment. (Reference Epstein and Hundert2; Reference Bird and Gilligan3) The problem with codes is that it is easy to incorporate aspirational goals that are poorly defined, resulting in standards that are difficult to interpret and impossible to meet. In the past, medical organisations such as colleges, universities and regulatory bodies were the final arbiters of whether a trainee could be recognised as a professional. Now, assessments of professionalism need to match contemporary expectations of defensible assessment, particularly if a doctor in training is removed from a programme.
Unfortunately, professionalism can easily be described in practice as ‘hard to define, but I’ll know it when I see it’. (Reference Ferguson4) This subjectivity is no longer acceptable as a benchmark. (5; 6) Difficulties arise when highly intelligent learners mimic professional competencies but generate ill-defined unease in their colleagues and supervisors, often due to their attitudes or expressed values. Detecting and quantifying the risk of sexual misconduct is complex. Medical educators need to address the challenge of capturing valid subjective perceptions by members of the teaching team without introducing unacceptable bias or perceptions of bias. In some countries, given the cost of training, failing a student may result in litigation, which inevitably means assessments must be legally robust in addition to being educationally valid and reliable.
Because professionalism is much broader than definable competencies, many codes of conduct include ‘competencies’ that are actually attitudes, personal character traits, or aspirational goals, and they may even pose ethical conflicts. For instance, in the Australian context, the good practice guide requires doctors and medical students to provide ‘constructive and respectful feedback to colleagues, trainees, international medical graduates and students, including when their performance does not meet accepted standards’. (5) It is unrealistic to expect doctors in training to give ‘constructive and respectful feedback’ to their seniors, colleagues or interprofessional teams unless there is a recognition of established hierarchies, acceptable modes of communication (including interprofessional communication) and a high degree of existing psychological safety. In the UK, the General Medical Council has produced similar standards, including the following: ‘you must be compassionate towards colleagues who have problems with their performance or health. But you must put patient safety first at all times.’ (6) It is understandable how difficult this statement may be to implement in practice. Both sets of standards place the responsibility of working safe hours on the individual, requiring a doctor to recognise the impact of fatigue on the doctor’s health and ability to care for patients, and requires them to endeavour to work safe hours wherever possible. (5; 6) Placing the responsibility of managing workload on an individual ignores the role of organisational culture and expectations, and is particularly unrealistic for junior doctors with little institutional power. Clearly, behavioural competencies may not, and perhaps cannot, extend across the entire field of professional expectations.
Sociologists may comment that professionalism can be understood as a role that doctors play in society. (Reference Martimianakis, Maniate and Hodges7) This perspective implies that professionals build trust by demonstrating ‘trustworthiness’ and an attitude of service to the needs of the community. (Reference Swick8) At the same time, professionalism can be understood as an expression of power and a means of social control. (Reference Martimianakis, Maniate and Hodges7) ‘Professionals profess’ writes Hughes, in the 1950s, ‘They profess to know better than others the nature of certain matters, and to know better than their clients what ails them or their affairs.’ (Reference Hughes9) This positioning of the doctor within the health care social system, and society more broadly, is part of the hidden curriculum. (Reference Martimianakis, Maniate and Hodges7) There are boundary issues between professions to be negotiated and understood, but also issues around race, gender and class. (Reference Hill, Samuels, Gross, Desai, Zelin and Latimore10; Reference Nieblas-Bedolla, Christophers, Nkinsi, Schumann and Stein11) When doctors learn to be doctors, operating within the social systems that medicine inhabits, they learn to inhabit systems of power and privilege. (Reference Rabinowitz, Reis, Van Raalte, Alroy and Ber12) This is where the hierarchies in which sexual harassment occur and can thrive. No wonder medical educators require considerable skill in teaching, assessing and remediating professional conduct with doctors in training.
Professionalism as a Behaviour: Teaching and Assessment
Because professionalism is an area of practice that is difficult to define, it is exceedingly difficult to assess in a defensible way. ‘The difficulty of its assessment’, writes Tim Wilkinson et al., ‘is nearly as great as the value we place on it.’ (Reference Wilkinson, Wade and Knock13) The risk of a doctor sexually harassing a colleague is usually captured when assessing interpersonal skills and teamwork. (Reference Berger, Niedra, Brooks, Ahmed and Ginsburg14; Reference Jha, Bekker, Duffy and Roberts15) Assessments are designed to test the positive competencies (such as teamwork, respect for diversity, professional manner and appropriate boundaries) as well as detecting ‘red flags’ which may indicate a risk of professional misconduct. (Reference Ainsworth and Szauter16–Reference Karp18)
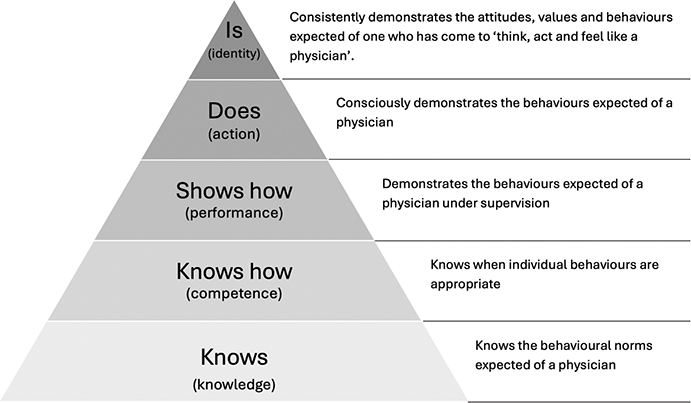
One way of conceptualising professionalism involves a modified form of Miller’s Pyramid. In its early version, Miller proposed a hierarchy of learning, beginning with knowledge. Competence is often demonstrated through applying a skill in a constructed environment, such as simulation, before performing the skill in its usual context, and finally demonstrating competence consistently in the workplace. (Reference Miller19) Since then, other scholars have proposed an additional layer of the pyramid, describing mastery, when a learner now ‘thinks, acts and feels’ like a professional (see figure 14.1). Wilkinson et al. discuss a blueprint for assessing professionalism, mapping assessment techniques and frameworks against professionalism aims. (Reference Wilkinson, Wade and Knock13) In the following, we examine the ‘layers’ of Miller’s Pyramid with respect to sexual safety, and the way pedagogies and assessments intersect.
Amending Miller’s Pyramid to include professional identity formation. Reproduced with permission. (Reference Cruess, Cruess and Steinert20)
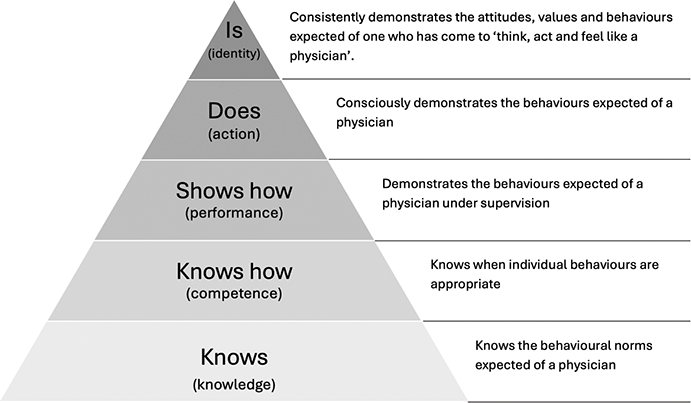
Figure 14.1 Long description
The pyramid diagram represents the progression of physician competencies through five levels, from bottom to top: 1. Knows (knowledge): Knows the behavioural norms expected of a physician. 2. Knows how (competence): Knows when individual behaviours are appropriate. 3. Shows how (performance): Demonstrates the behaviours expected of a physician under supervision. 4. Does (action): Consciously demonstrates the behaviours expected of a physician. 5. Is (identity): Consistently demonstrates the attitudes, values and behaviours expected of one who has come to think, act and feel like a physician.
Knowledge
At its basic ‘layer’, the doctor in training must be able to describe their professional obligations with respect to sexual boundaries, intimate examinations and other potential areas of misconduct. Teaching may involve didactic presentations, readings, and discussions and there may be a requirement to assess knowledge of the codes under which a student must learn. Pen and paper testing and other traditional forms of assessment, such as multiple-choice questions and short answer questions, can determine mastery of the knowledge required. An example of a knowledge task may involve describing the requirements of a particular code of conduct or providing a definition of sexual harassment.
Competence
In Miller’s Pyramid, competence means being able to apply a skill theoretically, such as working with scenarios rather than in authentic practice. (Reference Rethans, Norcini, Barón-Maldonado, Blackmore, Jolly and LaDuca21) In medicine, this is where teaching techniques can diversify. Students may still learn in didactic settings, but increasingly, medical education utilises problem-based learning, a system where groups work together to better understand and solve clinical problems. An example would be drawing a flowchart to represent the process of making a complaint, or defining which examples constitute harassment.
There are a number of self-assessed tools to assist doctors in training to examine and, if necessary, challenge their own professional assumptions and beliefs, and these can enhance their skills in reflective practice. (Reference Guraya, Guraya and Almaramhy22–Reference Launer24)
Performance
Performance involves demonstrating a skill in its appropriate context. In the professionalism space, techniques such as simulation may be used, using role plays, discussions or virtual worlds. These tasks may be addressed in peer groups, interprofessional teams, with actors or virtually. Doctors in training need to grasp the idea that professional conduct is situated in a particular time and place, and therefore medical educators may ask students to adopt a theoretical or personal position, examining the problem with multiple points of view. Although peer-norming is important, the aim is also to build ‘professional reasoning’: the capacity to make and remake one’s professional identity to suit the requirements of the role.
The difference between competence and performance can depend on the environment in which doctors learn. Doctors in training are highly motivated to adopt attitudes and behaviours that seem successful to them. (Reference Bandura25) Apprenticeship in a clinical setting involves taking interpersonal risks in an environment where ambiguity and uncertainty are expected. Tackling dilemmas around boundaries are essential transformational learning opportunities that drive maturation from apprentice to master. (Reference Torralba, Jose and Byrne26) This is often uncomfortable for the learner, and medical educators need to provide supportive spaces where students can take learning risks, including challenging their own beliefs or values.
Culturally, there is a range of discomfort with uncertainty. Given the high stakes of medical assessment, many students will be keen to unearth the ‘right’ answer to any given ethical problem. Greene’s dual-process theory of moral judgment (Reference Conway and Gawronski27; Reference Bago and De Neys28) asserts that both emotional and cognitive processes contribute jointly to moral decision making, with doctors in training deciding what is ‘right’ through analysis but also by their ‘gut feeling’ or ‘conscience’. For many doctors in training, this is a steep learning curve. Most doctors enter medicine with an empirical knowledge-based background, and these individuals can struggle with the nuanced and contextualised nature of ethical decision making and professional conduct.
These types of conversations need to be led by mentors and supervisors: when is it acceptable to have a relationship with a junior colleague? When is an obscene comment from an elderly patient with dementia considered ‘harassment’ and when it is considered frontal lobe disinhibition? Can it be both? What is the ‘professional’ response to a remark from a senior supervisor in the tea-room that you consider inappropriate? How does a doctor manage discomfort, painful interactions and vicarious trauma?
The acquisition of values, attitudes, behaviours and skills that represent ‘the way we do things around here’ is known as the hidden curriculum (see chapter 6). The hidden curriculum represents norms and values built into the training process, sociocultural behaviours and relationships that students need to master to effectively function in a social role. (Reference Wren29) Because doctors in training cover a very broad range of learning environments from primary to tertiary settings, and ‘cradle to grave’, their cultural and social immersion is complex and evolving. Acceptable behaviour in community paediatrics may be quite inappropriate in a tertiary intensive care unit. Doctors in training are influenced through a spectrum of observed and experienced situations which may range from extremely positive to negative. (Reference Rees, Alfes and Gatenby30–Reference McGurgan, Calvert, Narula, Celenza, Nathan and Jorm32)
Pedagogy in this space needs to involve some form of reflective learning, usually accompanied by opportunities to debrief with peers and colleagues, so that each learner can begin to build their own professional identity and test their assumptions in their future workplace. Medical educators may facilitate these discussions using lectures, workshops, formal discussions, peer debriefing and other forms of learning to enable learners to test their assumptions against their peers and their senior colleagues. Learners often need to ‘out’ the hidden curriculum, making the implicit explicit in order to examine its values, assumptions and impact, so they can decide whether to incorporate these ideas or discard them in the formation of their own identity.
Good medical educators have considerable skill in examining, describing and communicating tacit knowledge, but not all teachers do. Schön’s vision of ‘professional artistry’ includes different kinds of competence that practitioners display in unique, uncertain, and conflicted situations of practice. (Reference Schön33; Reference Schön34) Not all clinicians can consciously understand and describe how and why they are performing a skill while they are doing it, so the thinking required to rationalise professional performance is not always available to a doctor in training. This is one reason why the hidden curriculum is so powerful. Without insightful educators, and time to teach and reflect, hidden assumptions remain unexamined, unnamed and potentially unconscious. This means the doctor in training lacks the words and concepts to make sense of their experience, and may not question the cultural assumptions they have absorbed.
One difficulty that occurs in this area is that such discussions can easily replicate existing forms of privilege and hegemony. Team members from more privileged backgrounds can fail to recognise the microaggressions that are experienced daily by their less privileged colleagues.(Reference Michalec and Hafferty35–Reference Chuang, Nuthalapaty, Casey, Kaczmarczyk, Cullimore and Dalrymple37) Hierarchies based on gender, class or race may worsen if those people who are unaffected by them are allowed to dominate discussions, because important narratives of harassment and discrimination will be lost. These narratives need to be heard, because sexual harassment is more common for doctors in training who have lived experience of discrimination and disprivilege; all team members have a role in addressing this.
Assessing the acquisition of professional skills is challenging. Some skills are easily demonstrated (e.g. observing a student seeking informed consent). Others require a portfolio of complementary assessment techniques. Multi-source feedback, from supervisors, interprofessional colleagues, patients and peers, along with self-reflection, can identify doctors in training who are having difficulty acquiring the necessary professional skills. Clinical supervisors are good at making global assessments, identifying the learner whose interpersonal skills seem less professional or appropriate. The challenge is that the assessment needs to be defensible, and where possible, objective, as multi-source feedback is easy to interpret as a scapegoating exercise for students who may be socioculturally diverse. The reverse is also true. A student who is privileged has the potential advantage to use their social network and hegemony to optimise their ratings. Balancing the validity of an assessment with its reliability is always a challenge in the professionalism curriculum.
Action
As the learner becomes more senior, consistent professional conduct is expected. Assessments may focus on particular requirements of training, such as managing a team of learners in a psychologically safe way, or responding to inappropriate comments from patients on the wards. The education team need to have a way to manage critical incidents at this level, e.g. where a doctor in training has crossed sexual boundaries with a patient or colleague, or is perceived as unsafe by members of their team. There is professional learning for those reporting, as well as those who are reported.
Assessment can occur at multiple levels, and with multiple tools and techniques. (Reference Mak-Van Der Vossen, Van Mook, Van Der Burgt, Kors, Ket, Croiset and Kusurkar38) Milder forms of sexual harassment, such as inappropriate humour, can often be assessed and managed through conversation with the learner and their team, and with private feedback. More serious and/or persistent inappropriate behaviour can be escalated to any of the organisations involved in training. (Reference Brennan, Price, Archer and Brett39) Depending on the context and severity, these often require formal reporting processes, including law. Boundary crossing will often require targeted remediation, where the learner is subject to more intense supervision and further assessment. (Reference Launer24; Reference Regan, Hexom, Nazario, Chinai, Visconti and Sullivan40; Reference Arnold, Sullivan, Quaintance, Cruess, Cruess and Steinert41)
The more challenging issue is developing skills in recognising and managing sexual harassment. When a learner finds the behaviour of a colleague uncomfortable, there is an ethical and professional skill in knowing how to respond. In medical education, the training about professionalism and the development of professional identity are often related to issues that come up in difficult interactions with patients, such as inappropriate medication requests, patients who are angry, or people who offer inappropriate gifts. Being able to manage these interactions is important, but there is also an unspoken assumption that difficult behaviours and interactions always come from patients, seldom from colleagues, and especially not from supervisors or trainers.
Identity
At this point, learners embody the role of doctor, and should be experienced in managing contextual complexity. Often at this point, doctors are teaching as well as learning, and have highly developed professional values. They have also developed an understanding of the differences between the overt and hidden curriculum and the written and enacted professional expectations in any workplace.
The growing gap between what is taught and what is learned in the hidden curriculum, what is said and what is done in policy and what is expected and what is achievable in clinical practice means a doctor may have become inured against trusting organisational statements, policies, processes and codes. Medicine constantly evolves, but the pace of change has increased. On the ground, there is fragmentation of clinical responsibilities, a rise in consumer expectations, worsening inequity and fewer resources for care. However, the professionalism codes present what Michalec and Hafferty see as a ‘nostalgic’ view of professionalism, with doctors expected to deliver highly individualised, bespoke care in resource poor environments that can’t afford it. (Reference Michalec and Hafferty35) The outcome of this gulf between what is expected and what can be delivered means an understandable loss of trust. In this environment, the willingness of a doctor to report professional misconduct is significantly reduced. Medical educators need to have advanced skills in describing hidden assumptions and values. In this way, medical education may be able to lead cultural change by challenging inappropriate attitudes within learning teams.
Professionalism as a Trait: Managing Selection and Exclusion
Selection is a complex process which should reflect the academic, clinical, personal and professional potential of students without entrenching systemic bias. (Reference Cleland, Blitz, Cleutjens, oude Egbrink, Schreurs and Patterson44) Medical Schools are increasingly trying to attract students who have the personality characteristics that suit the professional requirements of medicine. Professionalism has been described as a feature of the doctor’s character, not just their behaviour. (Reference Asil, Bannatyne, Craig, Forrest, Stokes-Parish and Szkwara42; 43) Personal traits (Reference Rabinowitz, Reis, Van Raalte, Alroy and Ber12) have become a part of many selection processes, in the hope that a medical school can ‘weed out’ candidates who do not demonstrate the appropriate attitudes or values. This is a challenging enterprise, because many defensible tools used to demonstrate personal characteristics can be manipulated by those who choose to do so, or use norms based on white, privileged cohorts that disadvantage those with diverse backgrounds. Interviews, a mainstay of selection, can be rehearsed, and rehearsal can be more effective if the candidate has links with previously successful candidates, another example of privileging those who already live with privilege. (Reference Cleland, Blitz, Cleutjens, oude Egbrink, Schreurs and Patterson44)
Some universities use situational judgment tests (SJTs), which seem to be less influenced by socioeconomic status than other forms of assessment. (Reference de Leng, Stegers-Jager, Born and Themmen45) The SJT presents applicants with challenging situations they may encounter during medical school, and claim to measure traits like integrity, honesty, humility and sincerity. (Reference de Leng, Stegers-Jager, Born and Themmen45) There is some evidence that the presence of some personality traits predicts clinical performance, (Reference McLarnon, Rothstein, Goffin, Rieder, Poole and Krajewski46) and an example of using emotional intelligence screening is given in Table 14.1. However, there is considerable doubt in the academic literature that any process of this type is able to detect those with sociopathic or other dysfunctional personality traits. (Reference Knights and Kennedy47)
| Bond University in Queensland, Australia has introduced emotional intelligence (EI) testing as part of the selection process for its medical programme, with the aim of enrolling a cohort of students with the strong social skills needed to succeed at university and in the workplace. Bond University is a full fee paying university and has over 1,000 applications for its 120 places. In the past, it used a combination of academic performance and Multiple Mini Interviews to select students. However, it recently introduced an EI test, using this test and a test of academic performance to screen candidates prior to interviews. (Reference Asil, Bannatyne, Craig, Forrest, Stokes-Parish and Szkwara42) |
| Interpersonal skills, such as the ability to recognise one’s own emotions, help others understand theirs, display a breadth of emotional vocabulary and communicate well, are critical to a medical career. Professor Kirsty Forrest, who leads the programme, believes this approach means they select students who will have a better bedside manner, and better teamwork and collaboration skills. |
| ‘It is also about kindness. We believe that the competitiveness just to get into a medical programme can result in students being very unkind to each other. If they are kinder to each other during their years of education – and kind to themselves – it will lead to them displaying compassion when they are in the workforce and dealing with patients.’ |
| ‘There has often been a perception that medical professionals should display no emotion, and this is likely contributing to the higher instances of poor wellbeing and mental health issues in medical students and practising doctors. |
| ‘There has been talk of how medical school “knocks” the empathy out of students and we are looking at the bigger picture of how to ensure that is not the case. We are discussing the possibility of changing the way we test students to put the focus on the learning process rather than assessment, so we remove some of that competitiveness.’ (43) |
Professionalism as a Value: Learning to Balance Rights and Obligations
Medicine has deep ethical roots, but also has persistent ethical challenges. It is notable that the Hippocratic Oath codifies doctors to ‘abstain from all intentional wrong-doing and harm, especially from abusing the bodies of man or woman, bond or free.’ (Reference Minar48) Yet as with all institutions, what is codified may not be followed, and even if it was, the original version of the oath also commits the student ‘to hold my teacher in this art equal to my parents … when he is in need of money to share mine with him …’, so it is easy to imagine how abusive supervisory relationships developed and even flourished with these types of messaging.
In training, self-care takes a secondary role to patient safety. Its notable that it was not until 2017 that the World Medical Association added any wording related to health professional personal wellbeing (49) in their Physicians’ Pledge. (Reference Parsa-Parsi50) The 2017 World Medical Association’s decision to add ‘I will attend to my own health, well-being, and abilities in order to provide care of the highest standard’ to the Physicians’ Pledge (Reference Parsa-Parsi, Kloiber, Kurihara, Greco and Dhai51) indicates the importance that doctors now place on this aspect of their contract with society. (Reference Minford and Manning52) However, in an environment where it is normalised to subordinate one’s own needs in the interests of the patient, this emphasis can be problematic. Learners are expected to tolerate abusive power structures, starting with the simple reality of long hours. The idea of medicine being a vocation rather than just a job valorises the idea of self-sacrifice, ‘setting yourself on fire to keep others warm’.
In Stone et al.’s study of survivors of sexual harassment in medicine, (Reference Stone, Phillips and Douglas53) they describe a case where a young doctor is offered an opportunity to learn to suture. Her supervisor stood behind her as she attended to the patient, who was conscious. While she was suturing, her supervisor was fondling her bottom. ‘There was nowhere to go, it was a bed up against a wall, so you’re in a very small space’, she said. ‘But I think, also, because the patient was conscious, it felt like the right line to take was to continue looking very professional with everybody.’ For this doctor, it meant literally placing her body between the abuser and the patient, and silencing her needs ‘to continue looking very professional’.
The more junior a doctor is, the more unhealthy or harmful experiences become normalised. (Reference McGurgan, Calvert, Celenza, Nathan and Jorm54) Early in most junior doctor careers, traumas are part of the job. New doctors witness humanity at its most vulnerable and authentic, experiencing suffering, grief, loss and death, perhaps for the first time. The doctor is expected to tolerate this emotional, philosophical and potentially spiritual load, be a stable support for the patient and those around them, and then ‘get on with their job’. Once it is normal to dehumanise and compartmentalise the accepted horrors of a career in medicine, it is not a huge step to do the same with other behaviours – the wandering hand, the lingering gaze or worse.
Professionalism as Power: Supervisory Hierarchies and the Risk of Harassment
Doctors are in training for over a decade, in a series of highly hierarchical teams. These teams create an ideal opportunity for the misuse of power. When exploitation is normalised, it is challenging for junior doctors to manage inappropriate or harmful behaviour. Each team has a nested code of norms and relations within and between members and systems. Doctors in training are ‘itinerant workers’, engaging fleetingly with these nested systems – short rotations give little opportunity for them to build trust and understanding within a workplace, or to develop a sense of belonging and integration into teams comprised of more permanent members in each clinical placement. (Reference Gafson, Sharma and Griffin55) These nested systems of team and workplace have more permanence for members like nurses who can expect to ‘outlast’ the doctor in training. Doctors in training are short term investments: they enter a team which has its pre-existing systems of power and privilege already firmly in place, and then they leave, to become ‘someone else’s problem’. The more permanent team members are fluent in the currencies of informal power that flow in that team and workplace, while doctors in training are necessarily just starting to learn the language. Meanwhile, new and relatively inexperienced doctors are unaware of the usual or normative culture, workload or expected degree of functioning, and are therefore unable to identify what is ‘normal’ from a worker’s rights perspective. (Reference Epstein and Hundert2)
The Training Environment
Doctors train in a series of rotations over many years, and may only stay with a team for a few months at a time; this creates potential for a high degree of stress and vulnerability. (Reference Bernabeo, Holtman, Ginsburg, Rosenbaum and Holmboe56) The doctor in training is in a precarious social and professional position. There is a level of invisibility and a lack of support if they encounter poor workplace culture. They have a short period of time to become part of the team, to ‘fit in’, to build relationships, to impress key individuals, and to achieve certain goals such that they are either furthering their own career or are in a position to do so. This often comes at the expense of their wellbeing and autonomy. The well-documented infantilisation of doctors in training reduces the capacity of a doctor in training to raise concerns, as they are often seen as too junior to make valid judgments. (Reference Chervenak, McCullough and Grünebaum57)
Training has been likened to an extended job interview, and can be as long as fifteen to twenty years. If unprofessional behaviours that everyone has either normalised or chosen to ignore are reported, the ‘whistleblower’ (Reference Jones, Blake, Adams, Kelly, Mannion and Maben58) will always be known as the one who broke trust. They are also at the mercy of the more permanent members of the team, who are often responsible for providing the assessments that will allow the learner to progress in training. Even the most motivated doctors recognise that there is a risk to their reputation if they raise concerns, and this means many will just try to get through a toxic experience or rotation. ‘I don’t think it will make a difference’, they say, ‘I don’t want to make a fuss. I don’t want it to ruin my career.’ (Reference Hewitt, Chreim and Forster59; Reference Rich, Viney and Griffin60)
Pressures grow as trainees have their own families and dual-career partnerships that dictate their location. Raising concerns about sexual misconduct or workplace culture problems within a specialty runs the risk of a trainee being ‘blacklisted’ within the community, particularly if those involved are core to the community. Despite this, during postgraduate training there are some protections afforded by being in a formal programme. Trainees typically have points of contact outside of their clinical training, such as training programme directors and/or specialist college liaison officers that may be based outside of their unit and able to provide confidential advice and assistance.
If not in a formal training role, a doctor’s position is even more perilous. These doctors are often directly employed and educated by the department they work in, typically for three to six month contracts that may or may not be extended. These positions are rarely accredited for training, so the specialist colleges have no governance in determining whether the job descriptions and/or support provided is suitable for a doctor in training. This vulnerability is further accentuated if the doctor is working on a visa, as their employment is critical to visa validity. Being out of formal training or on a visa can therefore make a doctor extremely vulnerable. As international medical graduates are more likely to be in these positions, this introduces an element of racism into which doctors are most vulnerable to sexual misconduct in medicine.
Managing Learning Environments
Medical education teams play a core role in establishing and maintaining quality control over learning environments. Bullying, harassment and discrimination in learning environments are connected to culture, and can go beyond the unprofessional behaviour of one individual. (Reference Rich, Viney and Griffin60) It therefore makes sense to have systems in place which capture and monitor the ‘health’ of the workplace, in terms of the safety and inclusion of groups of trainees who are required to work there. This process involves the development and operation of trusted and reliable reporting systems which collect data in an ongoing way, and which include mechanisms to investigate and intervene in areas where concerns are highlighted. This is not a ‘one size fits all’ approach; these systems need to be appropriately tailored to fit the needs and nuances of each particular workplace and its stakeholders.
There are a variety of approaches which have been adopted and evaluated at different levels, with varying degrees of success. Systems in place can include one or both components (gathering information and taking action), and can be at the level of the team or the institution or across state of national jurisdictions. In New Zealand, HOTSPOTS, a system designed to identify and tackle bullying, discrimination and harassment for medical students from one university, has now been implemented at a national level. Although focused on medical students’ experiences, it covers clinical workplaces in half of New Zealand’s District Health Boards, plus around 200 general practices. HOTSPOTS was implemented in clinical placement sites in New Zealand’s North Island in 2019, with an aim of improving psychological safety in clinical learning environments. Longitudinal data indicates that this has been achieved, with the number of HOTSPOTS reducing over time. (Reference Shionoya61)
HOTSPOTS is an anonymous, online, system for collecting and reporting medical students’ experiences of bullying, discrimination, harassment, inclusion and respect (BDH & IR) on clinical placements. Definitions of BDH are taken from the University’s definitions for those constructs. Quantitative data is collected by a six-monthly survey sent to senior students, which also contains links to existing pathways for making informal and formal complaints regarding BDH as well as links to support services, giving a clear ‘zero tolerance’ message and highlighting support services. This also makes the point that HOTSPOTS is an additional reporting mechanism to other existing processes. Aggregated student data allows identification of clinical sites which are ‘outliers’ in terms of concerning or excellent practices. Individualised reports are made for senior staff, containing that site’s data with some comparator data (but not disclosing data from other clinical sites). Meetings are scheduled between the medical programme and clinical leaders (chief medical officers and heads of departments), where HOTSPOTS reports are discussed, actions planned and follow-ups put in place. A summary of all actions taken is reported back to all students and staff, cementing trust in the HOTSPOTS system and boosting future response rates.
The HOTSPOTS system takes the known drivers of unprofessional behaviour into account. It tackles harmful workplace cultures, empowers ‘workers’ by giving them a method of speaking up, encourages social responsibility and increases managers’ awareness and urgency of issues. (Reference Deal and Kennedy62) HOTSPOTS also incorporates the essential elements of an intervention designed to address these issues. Although systematic reviews and meta-analyses in this area are lacking and therefore there is minimal evidence about the most effective interventions, previous studies have identified likely effective elements: a focus on behaviour change and methods of addressing systemic contributors.
HOTSPOTS incorporates the key dynamics to consider in an intervention designed to address unprofessional behaviour, such as harassment. (Reference Collier63) It seeks and addresses systemic issues without identifying individuals, has a clear mechanism of action with safe, anonymous reporting, is inclusive and not designed to target one specific group of people, and encourages bystander engagement. In addition, it was designed using a mixture of theory and implementation science with flexible components, where leaders can choose the most appropriate actions for their own context, as well as have transparent reporting mechanisms of issues identified and actions taken.
There are, however, challenges to the creation and implementation of such systems. Importantly, there is the fact that there are many stakeholders, who may have differing views about what information should be reported and what should not be reported, who collects the data, who is able to access it and how it might be followed up; therefore successful systems need significant collaboration. Data regarding health and safety issues are regarded as highly sensitive as it may be linked to complaints. This includes human resources processes or key performance indicators, and there may be legal issues as well as ethical ones to be taken into account. Indeed, the way in which a new reporting system might fit in with any already existing systems and policy is one of the key considerations in its design and implementation. The New Zealand experience of creating and implementing the HOTSPOTS system was that consultation took over two years for stakeholders to reach agreement.
A known challenge to reporting systems is lack of engagement by those who are being asked to provide data. This is commonly due to fears of lack of confidentiality, damage to reputation or career retribution. A system which is perceived as unsafe and untrusted, or where data can be accessed by those with a conflict of interest – such as a role involving trainee assessment or appointment – is unlikely to be successful. Unclear leadership is another factor, as lack of clarity regarding oversight, accountability, motivation to take action and following through with interventions will not effect change. Lastly, if reporting systems do not report meaningful data back to those at the frontline, this can foster doubt that actions are taken, and decrease trust and engagement with the system.
Supervision and the Problem of Hierarchy
Perpetrators often use the implicit trust in the student–teacher relationship to initially groom, then habituate their target to increasing sexual related contact. (Reference Stone, Phillips and Douglas53). Although emphasis on ‘trust’ in medical professionalism is apt, like most virtues it is a nebulous construct, which can be manipulated and abused. (Reference Shionoya61) Culture is defined by Deal and Kennedy, as ‘the way we do things around here’. (Reference Deal and Kennedy62) When the doctor in training has constantly shifting contexts, and ‘the way we do things around here’ is fluid, so it is understandable that professional norms are confusing and difficult to interpret. Medicine has a number of cultural norms and organisational structures which can be manipulated by sexual predators. Historically, doctors and medical students have been encouraged to repress their own needs for the ‘greater good’ of others. There is a view that professionalism is all about subordinating personal identity for a greater ideal. Michael Yeo, a philosophy professor at Laurentian University in Sudbury, Ontario describes this perspective on professionalism: ‘I subordinate my personal identity to the role – that is, essentially, what I think professionalism comes down to. If the core idea is symbolically putting on the white coat, you are able to put aside your own identity.’ (Reference Collier63)
As the more powerful person in the relationship, all medical educators, whether they are hospital-based or university-based, are responsible for managing student–teacher relationship boundaries. The boundaries between doctors in training and medical educators are personal, as well as professional. Learners in medicine have close relationships with their supervisors, partly due to the long hours and residential requirements of medicine, but also due to the nature of learning. Medicine can raise highly personal challenges. The nature of the work includes ethical, personal, spiritual and emotional threats, and doctors in training can turn to their senior colleagues for advice and support. This can mean a blurring of personal and professional relationships that can lead to highly positive interactions that shape a doctor’s career, or unacceptable boundary violations. Medical Educators should be guardians of safety, acting in the best interests of students. They are accountable should violations occur. Students, because of unequal power relations, may find it difficult to negotiate boundaries or to defend themselves against boundary crossing.
Boundaries are therefore negotiated, and contexts and roles change throughout training. This means the learner is highly vulnerable to boundary violation, because their understanding of appropriate boundaries fluctuates. It may be quite normal, for instance, for a rural supervisor to invite visiting students to a family dinner, particularly if the town has few options for an informal meeting and the supervisor is concerned that the student is feeling isolated and lonely. The same student may not realise that a similar invitation to the home of the Professor of Surgery in a busy urban teaching hospital may be a significant breach of acceptable professional boundaries.
The supervisory hierarchy is often the context in which sexual harassment occurs, because the learner is vulnerable; they depend on their seniors for teaching, supervision and academic progression. Medical educators may hold considerable institutional power and prestige, holding influential positions within a region or their specialty. In some medical training cultures, exploitation is expected. In return for learning opportunities and positive formative assessments, some will be expected to donate labour, including the ubiquitous unpaid overtime. This exploitation may even be formalised as patronage, where a patron expects their junior colleague to assist with domestic tasks, such as shopping, cooking, or childminding, in return for learning opportunities. (Reference Blunt, Turner and Lindroth64) Bribery is not uncommon. When exploitation is normalised like this, and hierarchical systems are not clear, junior colleagues are particularly vulnerable to other forms of abuse, including sexual exploitation.
In the literature around sexual misconduct, it is common to hear that the person responsible for safety or reporting was inappropriate or conflicted, perhaps because they were a friend or partner of the perpetrator, or were perpetrators themselves. Many in the education space feel profound senses of guilt, anger and shame about the knowledge that sexual assault, sexual harassment and rape are happening in spaces where the most vulnerable learners in the medical community exist. To manage these feelings, bystanders may ‘turn a blind eye’ to harassment to preserve their own power, prestige, privilege, and position in the professional community and/or succumb to cognitive dissonance to maintain their view of the profession as collegiate, professional and safe.
Interpersonal Dynamics in the Supervisory Relationship
Supervisory relationships are complex, and not all learners are treated equitably. (Reference Recupero, Cooney, Rayner, Heru and Price65) Doctors and doctors in training come into these relationships primed by broader expectations, and framed by the cultural norms of the workplace. Supervisors can express highly dominant behaviour, fuelled by existing privilege and reinforced by the hierarchical system in which they work. Gendered cultural norms can be reinforced by religion, science, morality, media, education, legal systems, culture and tradition. Because supervisors are often cossetted in their dominant position, there may be little motivation to change. (Reference VeneKlasen, Miller and Milligan66)
When supervisors exhibit dominant behaviour, learners can reflexively exhibit subordinate beliefs and behaviour, avoiding confrontation and resorting to indirect forms of responding. In focusing on what the supervisor wants and needs, they may be increasingly silenced, and develop self-deprecating and self-defeating beliefs, which can be weaponised to increase vulnerability when supervisors sexually harass or abuse their subordinates.
Power and Leadership
The shadow side of leadership is the misuse of power, (Reference Saxena, Meschino, Hazelton, Chan, Benrimoh and Matlow67) including sexual harassment, which is essentially an act of power and dominance. While there are many ways of understanding how power operates in medicine, in this chapter, we explore VeneKlasen et al.’s model of ‘power, people and politics’. (Reference VeneKlasen, Miller and Milligan66). The advantage of the model is that it grounds an approach to advocacy, using mutual support and collaboration to reduce social conflict and promote equity; VeneKlasen et al. believe that there is the potential for common ground if communities build collective strength.
VeneKlasen et al. describe four types of power:
1. Power over describes the formal and informal power structures that create hierarchy and increase or decrease agency in individuals.
2. Power with describes the ability of individuals to work together to advocate for change. Collective strength can be utilised to create change, and reduce the risk of the powerless being harmed in the process.
3. Power to describes the potential of an individual to shape their own lives and the world around them. The positive use of this capacity is the ability of individuals to provide and receive mutual support, and contribute to joint agency. When weaponised, it describes the ability of an individual with power to act on others in a way that increases their own agency, and diminishes or harms the other.
4. Power within describes the internalisation of beliefs about personal power and agency that shape and maintain vulnerability and agency. Power within describes a person’s sense of self-worth and self-knowledge and includes an ability to recognize individual differences while respecting others.
In the Table 14.2, the various roles of a supervisor are described using VeneKlasen’s model. It is normal to take multiple simultaneous roles in medical education. In Australian general practice, for instance, a supervisor may be an employer, teacher, mentor, sponsor and role model, as well as a supervisor. This means power can be augmented, but it can also be confusing. Supervisors can use multiple forms of power to influence the target, and this can mean the target is deeply vulnerable in the relationship.
Table 14.2 focuses on the negative implications of each relationship, but each relationship is grounded in a positive educational role. Ideally, supervisors provide exceptional workplace training, modelling good practice and facilitating learning. Mentors, sponsors and role models can be remembered for a doctor’s entire career, having a deep impact on their confidence, competence and career trajectory. It is this positive influence that means learners typically enter these relationships with optimism, openness and trust; it is an unfortunate reality that at times this trust is misplaced. Good supervisors can inadvertently enable grooming by others who are perpetrators, because the learner allows themselves to be vulnerable and trusting on the basis of previous positive supervisory relationships.
| Role | Power over | Power with | Power to | Power within |
|---|---|---|---|---|
| Supervisors have legitimate organisational power, which means they can control access to learning tasks (e.g. allocating doctors in training to certain patients with certain needs). They can use this power to coerce juniors to comply by granting or withholding learning opportunities, or using feedback forms/incident reports to reward or punish. Senior doctors hold expert power by virtue of their knowledge, skills and abilities and can offer or withhold their knowledge and skills from doctors in training. They can also humiliate or embarrass learners. | Supervisors are in a workplace, and therefore exercise their power in public spaces. This means they can leverage the power of the team, and the social power of stigma and shame when they supervise in front of clinical teams and patients. They are members of a profession that the learner aspires to join, and have the organisational weight of the institution behind them. | Supervisors can use feedback processes to impede progression and restrict access to essential learning opportunities. They can build or destroy a learner’s confidence and reputation by disciplining them in front of colleagues. They can give or withhold the learning young doctors need. They can also provide formal or informal handover to future supervisors, affecting a doctor’s reputation. | Supervisors have the power to affect a learner’s sense of self-esteem and self-efficacy. They can organise a learner’s work schedule so that learning is more difficult, or the learner is less able to succeed. |
| Teachers have organisational and informational power, and are able to design and deliver curriculum according to their perceptions of the needs of doctors in training. Medical teaching can enforce hierarchies, especially when they use humiliation and flattery to manage their students. Teachers can teach or withhold teaching on equity, diversity and inclusion principles, and can emphasise/de-emphasise the importance of professionalism in practice. Teachers can give learners mental models to manage interpersonal conflicts in the workplace and encourage or discourage peer learning and peer support. They are usually responsible for managing reports of misconduct from teachers and learners. | Medical teachers operate in institutions, like universities or professional colleges. There is considerable referent power in the name of those institutions that allow them to exercise control over the learners. They also have the organisational power of evidence-based educational practice, which enables them to teach confronting material like equity, diversity, inclusion, ethics and professionalism. Some jurisdictions have the weight of Medical Boards, and their codes of conduct mandated, influencing curriculum and educational design. | Teachers decide who is taught through selection and how they are taught, including the use of peer learning, which can come with its own layers of power and influence. Teachers can prescribe remediation, and advance or restrict academic careers. Teachers set the dominant attitudes attached to a professional identity, and decide how learners understand what is expected in terms of interpersonal behaviour. Teachers manage the discipline of learners who don’t demonstrate appropriate behaviour and ensure learning environments are safe. | Teachers have the power to affect a learner’s sense of self-esteem and self-efficacy. This is particularly the case if the curriculum is overloaded, the teaching is not fit for purpose, or discrimination is normalised. They can model discriminatory attitudes that cause harm, and make certain students feel alienated and inadequate. |
| Role | Power over | Power with | Power to | Power within |
|---|---|---|---|---|
| Assessors have legitimate organisational power, and career progression provides a powerful opportunity for coercion. Soft skills, like communication and teamwork, are particularly subject to conscious and unconscious bias in workplace assessments. In designing assessments, assessors have the opportunity to foreground or background unprofessional conduct | Assessors work with teachers and supervisors to regulate access to the profession by mobilising other educators and supervisors. They use institutional power to ground their assessment processes and decisions, and have institutional policies in place to support their decisions to remove learners from training. | Assessors have the power to remove learners from training and require them to undertake remediation. They also drive learning by setting assessment tasks. | Assessment is a high stress, high stakes activity, which is also expensive. Doctors are often perfectionistic and self-critical. Failure on assessment can have significant consequences for their careers and wellbeing |
| Managers have legitimate organisational power, making decisions around workload, work placement, accommodation and facilities, and work opportunities. Access to accommodations like leave and part-time work are subject to managerial approval. Managers also interpret and act on feedback from supervisors, patients and peers, and enact the policies of their organisation, including the management of consequences for employees who breach professional guidelines. | Managers work in a hierarchy, and use this institutional power to regulate learning. Managers use external sources of power, like law and regulation, to ground their policies, but also regulate when they are used. | Managers have the power to negotiate salaries and working conditions. They also employ the supervisors, so they are able to discipline supervisors who demonstrate sexual misconduct. They may also choose to discipline the survivor. | When managers follow institutional sexual harassment policies, many survivors report feeling invalidated and retraumatised. Many feel their privacy has been breached and experience stigma and shame. |
| Role models are granted informal referent power, using their influence to inspire and motivate others. They often operate via the hidden curriculum. By modelling particular attitudes and behaviours, they can improve trust in the team. They can also leverage their professional reputations to normalise less desirable attitudes like discrimination or hide less desirable behaviours, like sexual harassment. | Role models work within clinical teams, and can have significant groups of followers. In dysfunctional teams, this can mean weaker members of the team experience alienation, bullying and harassment by the ‘gang’ of followers. | Role models have the power to shift the dominant narrative in the workplace. In medicine, a role model can be an excellent clinician, but demonstrate harmful interpersonal behaviours. This can lead to inappropriate team behaviour and an unsafe workspace. | Poor role models can cause alienation, shame and loss of self-esteem in learners who are not accepted by the team. |
| Role | Power over | Power with | Power to | Power within |
|---|---|---|---|---|
| Mentors can be informally chosen, and be granted referent power, but they can also be allocated as part of a mentor scheme, which grants them legitimate organisational power. Mentors have information and skills that can be shared, granting them power to coerce. | Mentors are usually respected members of the profession with considerable referent power. They can be charismatic leaders, which means they have a community in the profession who trust them. This means it can be challenging for the learner to identify them as untrustworthy. | As mentors, they can legitimately ask about personal life and experience, and this may lead to informal meetings in informal settings, which can be unsafe. They can also get to know their mentees well, and this knowledge can be weaponised to coerce learners. | Mentors can interpret and communicate their beliefs about the learner, and this can reduce self-esteem and confidence. Because the mentorship involves personal issues, this can mean interpreting the learner’s feelings and beliefs, and not just their professional performance. This can be a form of grooming. |
| Sponsors are often available to some and not to others. Sponsors have organisational power, including access to opportunities. They can choose to advance a doctor in training by offering opportunities (e.g. a clinical position or promotion, membership of a steering group, or an invitation to a professional dinner). Like patrons, they can use ‘favours’ in exchange for their sponsorship. Sponsors may privilege certain learners over others, leading to discrimination, e.g. the ‘boys club’ culture. | Sponsors usually bring a chosen learner into an existing group as a way of extending their networks and furthering their careers. The ‘boys club’ of medicine is based on this behaviour, and can amplify discriminatory attitudes. The advantages of developing a powerful network means the sponsor holds considerable power. | Sponsors can offer or decline to offer opportunities, and when offered can give or withhold support. | The inclusion or exclusion from powerful social networks affects personal and professional self-esteem. It can also influence a learner’s personal and professional identity. |
| Patrons have considerable organisational power, and in the communities where this role is normalised, learners have little choice but to comply with their requests or demands. In these settings, learners are vulnerable to being exploited, as they rely on their patrons for career progression, or even access to employment. Patrons can escalate their demands, beginning with culturally legitimate requests, but escalating to discriminatory behaviour or frank harassment and abuse. | Patrons exist in a powerful system that reinforces the subordinate role of learners and their own dominance. Patronage occurs in an existing social system where there is already bribery, corruption and favours as currency. Reinforcing that system in medicine reinforces other patriarchal norms and expectations. | Patrons can choose their learners, and can design abusive systems of ‘favours’ in exchange for learning, which increases the vulnerability of learners. | Patronage increases a learner’s sense that they are subordinate and decreases their sense of worth and agency. |
| Role | Power over | Power with | Power to | Power within |
|---|---|---|---|---|
| Leaders allocate precious resources: money, personnel, time and curriculum. They also decide how many people get to train, and who gets to lead. In a sense, they allocate power. However, they also negotiate with overarching organisations, influencing how governments allocate resources to their specialities or schools, and how much power they can wield. Within clinical environments, leaders negotiate the balance between service, research and learning, which can expand or limit their opportunities. | Leaders can influence entire systems, entrenching standards, expectations and structures that privilege some and disprivilege others. They also stand between the profession and the funders, including governments, influencing the impact broader policies have on the medical workplace. Because of their high position, they can be difficult to challenge. | Leaders have the ultimate say in a doctor in training’s selection into the profession, or their exit from the profession. They drive cultural expectations and have the capacity to influence the way the system behaves. | Leaders can have a powerful influence over a doctor in training, because of the steep medical hierarchy. This increases their capacity to silence targets, and increases their ability to cause sexual harm. |
Visible and Invisible Forms of Power and Agency
Senior clinicians have institutional power, but they also have considerable influence simply because their clinical mastery is recognised and respected. Foucault writes that ‘It is not possible for power to be exercised without knowledge; it is impossible for knowledge not to engender power’. (Reference Gordon and Foucault68) It is important to recognise the status this clinical mastery brings. In her victim impact statement, a survivor of sexual assault in Australia clearly articulates the importance of this power differential: ‘Before pleading guilty to these assault charges, the perpetrator used to hold a high position in a well-known cancer centre hospital and he was a respected member of the community. I, on the other hand, was still a trainee.’ (Reference Stone, Phillips and Douglas53)
The perpetrator in this case demonstrates both reputational power, which is invisible, and the power that comes with titles and roles, which in his case included his professorship. Visible power consists of the formal rules, structures, authorities, institutions and processes of institutional decision making. Policies can be part of structural bias, privileging one group over another or making it impossible for a subgroup to participate in the workplace fairly. An example is the capacity to work part-time, or to take maternity leave during training. While cast as ‘fair’, these policies impact women disproportionately, and are one reason why there is such profound gender inequity in medicine. Another is ‘bullying up’, where a more privileged junior doctor may intimidate their supervisor by using the privilege of their social status, such race, gender, class or other forms of privilege.
One unexpected impact of shifts in professional expectations is the over emphasis of individual power to influence systemic problems. For instance, in Australia, Good Medical Practice (69) outlines the professional expectations of doctors and doctors in training, and has made a number of recent modifications that place greater emphasis on the individual’s role in meeting patient needs. The guide details the expectations that the doctor will maintain productive collegiate relationships. It is normal in sexual harassment for survivors to question their role in the abuse, and this contributes to silence and shame. Encoding abuse as an individual problem contributes to this shame by inappropriately placing the responsibility on the survivor to manage their own harm, without recognising the broader roles and responsibilities of the systems in which doctors train.
Conclusion
Medical education is a complex field, with a variety of roles that are often inter-related and inter-connecting. Medical educators are responsible for deciding who enters training, and who graduates as a fully qualified specialist. They determine the curriculum, the way professionalism is taught and assessed, the competencies that are assessed at each level of training, and whether remediation opportunities are offered. In doing so, they manage learning environments, and develop the educational skills within the teaching team. This means they are responsible for monitoring professional conduct in teachers and supervisors, and addressing misconduct when or if it arises. They also take roles in monitoring and supporting the wellbeing of doctors in training.
Medical educators should ideally have advanced skills in describing, assessing, teaching and monitoring implicit and explicit learning. One of their key roles is to find effective, contextually sensitive and specific ways to assess interpersonal skills, behaviours and attitudes, and to use institutional power to manage the perpetrators of unprofessional conduct, including sexual harassment. In order to do so, they need to have sufficient institutional power to act on those assessments, ensuring learning environments are safe and learners are well supported.
Doctors often begin teaching as students during medical school, and as such the ‘medical teachers’ role varies from those with rudimentary near-peer tutoring to educational leadership in large institutions. Medical education is invariably part of larger systems which exercise considerable institutional power, creating hierarchies that can be leveraged to enable abusive behaviour to thrive, and significant potential for blurred boundaries.
Professionals build trust, by demonstrating ‘trustworthiness’ through an attitude of service to the needs of the community. Medical educators teach and model professional conduct from the earliest stages of medical training. Educational leaders ‘teach the teachers’ and should ensure professional behaviours are consistently modelled, whether the educator is a new tutor or the leader in a large institution. The academic work in this space involves developing, assessing and applying educational strategies to promote safe and effective professionalism learning throughout medical training, including the effective assessment and remediation of professional misconduct at all stages of professional development.

 Open access
Open access