


Reviews and meta-analyses indicate that lithium is the most effective treatment for bipolar disorder, Reference Geddes, Burgess, Hawton, Jamison and Goodwin1–Reference Severus, Taylor, Sauer, Pfennig, Ritter and Bauer4 a view endorsed by international clinical guidelines. 5 However, it is substantially underused. Reference Kessing6 One consistently identified barrier to its prescription by clinicians and acceptability to patients is the requirement for regular blood monitoring, particularly of serum lithium levels. Reference Parkin and Thomas7–Reference Gomes, Soleas, Kcomt, Duffy, Milev and Post10 Monitoring is mandatory to reduce the risk of adverse effects caused by blood levels above the therapeutic range and the risk of ineffectiveness due to levels below this range.
Monitoring of lithium levels is relatively frequent when treatment is initiated and becomes less frequent during long-term treatment. Many patients dislike having a venous sample taken and the need to travel to a clinic to have this done. Moreover, because the sample has to be transported to a laboratory and analysed, and the result then has to be returned to the clinician, there is a delay before the clinician and patient are informed of the result and any change in the lithium dose. Clinicians are sometimes reluctant to prescribe lithium because of the additional work associated with regular venous blood monitoring, and because of concerns that patients may not attend monitoring appointments, which increases the risk of serious adverse effects. Surveys of both patients and clinicians indicate that the need for regular blood monitoring is a key factor in lithium being used much less than would be expected. Reference Parkin and Thomas7–Reference Gomes, Soleas, Kcomt, Duffy, Milev and Post10 Even when lithium is used, the demands of the process can lead to monitoring being too infrequent to be useful.
A potential solution to these issues is offered by the advent of devices that can be used to measure lithium levels at the point of care, using a small finger-prick capillary sample instead of a venous one. These small portable devices can analyse a sample without the need to transport blood to a central laboratory and have recently been introduced for monitoring of antipsychotic medications. For example, a point-of-care (POCT) approach for monitoring clozapine levels has been found to be more acceptable to patients and clinicians than venous blood sampling Reference Atkins, Taylor, Harland, Brewer, Williams and Chesney11 and provides results with a similar degree of accuracy. Reference Taylor, Atkins, Harland, Baburina, MacCabe and Salamone12 In recent years, several devices that provide POCT assays for lithium have been developed. Reference Olsson, Hauser, Ribet, Wikström, Görgens and Beck13–Reference Glazer, Sonnenberg, Reinstein and Akers15
In the present study, we assessed the acceptability of a POCT approach to lithium monitoring compared to current practice via two surveys, one of people being treated with lithium and another of clinicians involved in managing lithium treatment. We also compared the technical performance of a POCT device with that of a conventional laboratory assay by collecting both capillary and venous blood samples from the same set of patients. We tested the hypothesis that a POCT approach for lithium would be more acceptable to patients and clinicians than a laboratory-based approach, and that it would deliver a similar level of technical performance.
Method
Acceptability of conventional and POCT methods
Study design and setting
This study comprised two complementary online surveys, one of patients prescribed lithium and one of clinicians who prescribe lithium, conducted within a large mental health National Health Service (NHS) trust and general practice settings in Oxfordshire, UK. Both surveys were designed and reported in line with the Checklist for Reporting Results of Internet E-Surveys. Reference Eysenbach16
Survey development
Both surveys were developed by a multidisciplinary team comprising psychiatrists, a pharmacist, and a Biomedical scientist.
The patient survey comprised three sections (see the Supplementary Material available at https://doi.org/10.1192/bjp.2026.10695 for the full survey):
-
(a) Demographic information (four items);
-
(b) Attitudes towards treatment with lithium and lithium monitoring (six items);
-
(c) Preferences for type of monitoring; impact of using POCT (three items).
The survey was designed in partnership with the Oxford Health NHS Foundation Trust National Institute for Health and Care Research (NIHR) Biomedical Research Centre Data Science Patient and Public Involvement, Engagement and Participation group to ensure patient relevance and clarity.
The clinician survey also comprised three sections (see the Supplementary Material for the full survey):
-
(a) Demographic and professional information (six items);
-
(b) Barriers to lithium treatment (six items);
-
(c) Preferences for type of monitoring; impact of using POCT (11 items).
Clinicians were also asked two open-ended questions:
-
(a) What do you think are the current barriers to lithium use?
-
(b) How might at-home POCT affect patient adherence to lithium?
A pilot study of clinicians (n = 10) was conducted to assess content clarity, variance and item relevance before wider dissemination of the survey. No changes were made to the survey following piloting.
Recruitment and participants
Eligible patients were aged ≥8 years and were currently being prescribed lithium. Patients were approached in person by a pharmacist or nurse, who explained the purpose of the study and provided survey access details. Eligible clinicians were psychiatrists or general practitioners (GPs) who had ever prescribed lithium. Clinicians were recruited from Oxford Health NHS Foundation Trust and from 78 GP practices across Oxfordshire. Clinicians were invited to take part by email.
Survey administration
Both surveys were administered using Qualtrics XM (Provo, Utah, USA; qualtrics.com) 17 and were open for approximately 10–12 weeks. Each took a median of 2 min to complete (interquartile range [IQR]: 1–3 min). Responses were anonymous, and informed consent was obtained electronically before participation.
Validation of lithium POCT
Patient sample
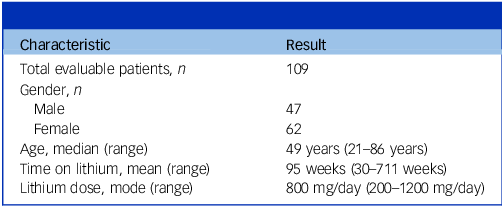
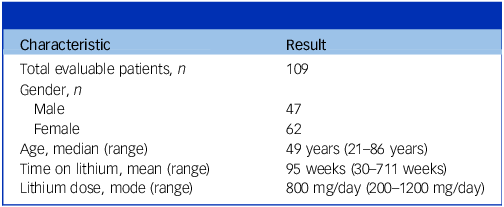
Patients who were being treated with lithium by community and in-patient services within Oxford Health NHS Foundation Trust (n = 109) took part in a service evaluation conducted from June 2024 to June 2025. All patients had a clinical diagnosis of bipolar disorder or depression. The mean age was 48 years, and the mean duration of treatment with lithium was 1.8 years. Overall, 43% of the sample were male and 57% were female (Table 1).
Characteristics of the patient sample
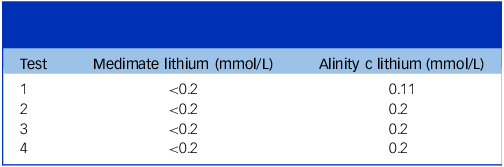
In four patients, the concentration of lithium (measured with the laboratory method) was at or below the limit of quantitation of 0.2 mmol/L for the POCT assay. In three patients, the concentration was 0.2 mmol/L, and in one it was below 0.2 mmol/L (Table 2). Data from 105 patients were therefore available for the comparison of the conventional and POC methods.
Below limit of quantitation point-of-care testing (Medimate) results
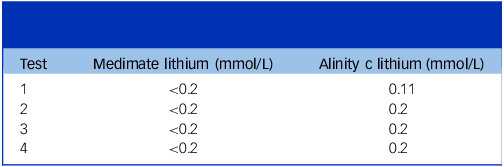
Table 2 Long description
A table with four rows and three columns compares lithium concentrations measured by Medimate and Alinity tests. The columns are labeled ‘Test’, ‘Medimate lithium (mmol/L)’, and ‘Alinity lithium (mmol/L)’. For all four tests, Medimate lithium levels are below 0.2 millimoles per liter. Alinity lithium levels are 0.11 millimoles per liter for Test 1 and 0.2 millimoles per liter for Tests 2, 3, and 4. The table highlights the comparison of lithium concentrations between two testing methods.
Testing procedure
At a routine clinical appointment for the collection of a venous blood sample (5 mL serum separator tube) for lithium monitoring, patients were asked whether they would be willing to provide an additional finger-prick capillary blood sample (20 µL). For those that consented, both venous and capillary whole-blood samples were collected separately, about 1 min apart.
For the standard (reference) method, blood samples (5 mL serum separator tube) were collected from an antecubital vein using a BD Vacutainer Safety-Lok blood collection set. Samples were transported to a central laboratory at Oxford University Hospital and were tested within 6 h of collection. Samples were processed into serum; then, the serum lithium concentration was measured using an Abbott Alinity clinical chemistry analyser (Abbott Laboratories, Abbott Park, IL, USA).
For the POCT method, a Unistik 3 lancet (1.8 mm gauge) was used to obtain capillary blood from the tip of a finger. A Medimate Multireader, a microfluidic capillary electrophoresis device (Fisic BV, Enschede, the Netherlands), was used to measure lithium concentration. This device uses microfluidic capillary electrophoresis glass chips (lab chips) housed in a test cartridge to separate and detect lithium ions in blood using electrophoresis and electrical conductivity. After lancing of the finger, a small volume (20 µL) from the first drop is applied directly to the sample inlet of the lab chip. The cartridge is then inserted into the Medimate Multireader, where an electric field (electrokinetic injection) introduces a precise amount of sample into a narrow, buffer-filled glass capillary within the lab chip. A sustained voltage is then applied across the capillary, causing the ions to migrate at different speeds according to their charge and thus separate into distinct zones (capillary zone electrophoresis). Integrated platinum electrodes connected to an impedance detector pick up changes in conductivity as each ion zone passes, producing a measurable signal that is proportional to the amount of lithium in the sample. The analytical measurement takes just 8 min, from insertion of the test cartridge to a result being generated and displayed on the device.
Reproducibility
The intra-patient repeatability of the Medimate Multireader assay was assessed in a subgroup of five patients. In these patients, a second capillary sample was collected from the second drop of blood arising from the same fingerpick that provided the first drop.
Statistical analysis
Passing–Bablok regression Reference Passing and Bablok18 and Bland–Altman analysis Reference Giavarina19 were conducted for all results obtained from the method comparison. A further partitioned bias analysis Reference Magari20 was conducted to determine the bias at defined intervals across the measuring range.
Analytical performance specification
Assessment of a POCT device requires a demonstration that the analytical performance of the device meets predefined quality specifications. These specifications define the maximum permissible deviation between a measured and true value that will not compromise clinical interpretation. For measurements of lithium, for which therapeutic and toxic ranges are narrow, it is essential to establish and adhere to stringent analytical performance limits to ensure clinical safety and comparability with reference laboratory methods.
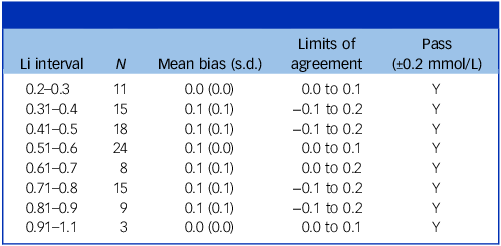
To assess analytical agreement, we performed a partitioned bias analysis across the measurement range of the lithium results (Table 3). This revealed the mean bias and limits of agreement at each measurement interval, enabling comparison with internationally recognised analytical performance standards for lithium measurement. The Clinical Laboratory Improvement Amendments, which set federal quality standards for all US clinical laboratories (∼320 000), define a total allowable error for lithium of ±0.3 mmol/L. 21–23 By comparison, the Royal College of Pathologists of Australasia recommends an analytical performance specification of ±0.2 mmol/L for concentrations ≤2.0 mmol/L. 24 On the basis of these standards, we applied a conservative threshold of ±0.20 mmol/L to evaluate analytical acceptability across the range of lithium concentrations measured by the Medimate Multireader.
Partitioned bias analysis
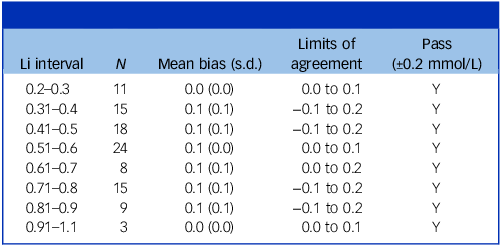
Table 3 Long description
The table presents a partitioned bias analysis for lithium measurements, divided into intervals ranging from 0.2 to 1.1 millimoles per liter. It includes columns for the lithium interval, the number of samples (N), mean bias with standard deviation, limits of agreement, and a pass/fail indicator based on a 0.2 millimoles per liter threshold. Each row details the specific interval, the number of samples analyzed, the mean bias and its standard deviation, the limits of agreement, and whether the results passed the analytical performance standard. The data shows consistent mean bias values and limits of agreement across different intervals, with all intervals passing the specified threshold.
In the UK, analytical performance is assessed through peer-group evaluation (UK NEQAS) rather than using fixed total allowable error limits. Therefore, UK specifications were not included to ensure comparability with quantitatively defined international standards.
Ethics statement
This investigation was defined as a service evaluation by Oxford Health NHS Foundation Trust Clinical Audit Team. Our Trust policy dictates that service evaluations are considered by the Clinical Audit Team and approved or modified by that team. Ethical committee approval is sought only when the Clinical Audit Team considers it appropriate. The Clinical Audit Team approved this investigation as a service evaluation not requiring ethical committee approval or formal written consent from potential participants (AMHT Oxon City And North East/SE/2024-25/02). All participants provided informed verbal consent before participation, in accordance with the Declaration of Helsinki.
Results
Patient survey
A total of 72 patients were invited to take part, of whom 52 (27 males, 24 females, one non-binary) completed the survey; this represented a response rate of 72%. Of those who took part, the median age was 41 years (IQR 27–50), and the median duration of treatment with lithium was 5.5 years (IQR 3–8).
The frequency of lithium monitoring varied widely across patients. For most patients (52%), the interval between successive lithium measurements was 6 months or more. Specifically, 14 patients (27%) were monitored every 6 months, 13 (25%) once per year, and nine (17%) less often than once per year. In a minority of patients (31%), levels were checked every 3 months (n = 6; 12%) or more frequently (n = 10; 19%).
Attitudes towards lithium treatment and monitoring
Most respondents (36, 69%) indicated that monitoring affected their social or work life, whereas 16 (31%) reported no impact. Similarly, 35 (67%) considered regular monitoring to be a burden, whereas 17 (33%) did not. In addition, 35 (67%) said they were worried about frequent blood tests, with 17 (33%) expressing no concern. Finally, regarding perceptions of lithium, the majority (39, 75%) disagreed that it seemed outdated or unsafe, and 13 (25%) agreed.
Preferences and impact of POCT lithium capillary monitoring
Most of the patients (n = 37, 71%) indicated that they would be more likely to take lithium if levels were monitored via POCT rather than a conventional venous blood method. Only three respondents (6%) indicated that they would not be more likely to take lithium if capillary monitoring were available, and 12 (23%) were unsure. Most respondents (n = 34; 65.4%) thought that getting the test results at the point of care would be ‘Useful’; nine (17.3%) indicated that this would be ‘Not useful’ and nine (17.3%) did not express an opinion. Most (n = 38, 73%) patients indicated that they would prefer lithium level monitoring at home with remote follow-up; only four (8%) indicated that they would not, and ten (19%) did not mind either way.
Clinician survey
A total of 128 clinicians accessed the survey, of whom 86 completed it (response rate 67%). The median age of respondents was 43 years (IQR 33–53). Overall, 39 were male, 45 were female, with one non-binary and one preferring not to say. Fifty-two were consultant psychiatrists (61%), 21 were trainee psychiatrists or GPs (24%) and 13 were fully trained GPs (15%). Most respondents had more than 10 years of post-qualification experience (n = 44, 53%); the next most frequent experience range was 5–10 years (n = 16, 19%).
Barriers to lithium use
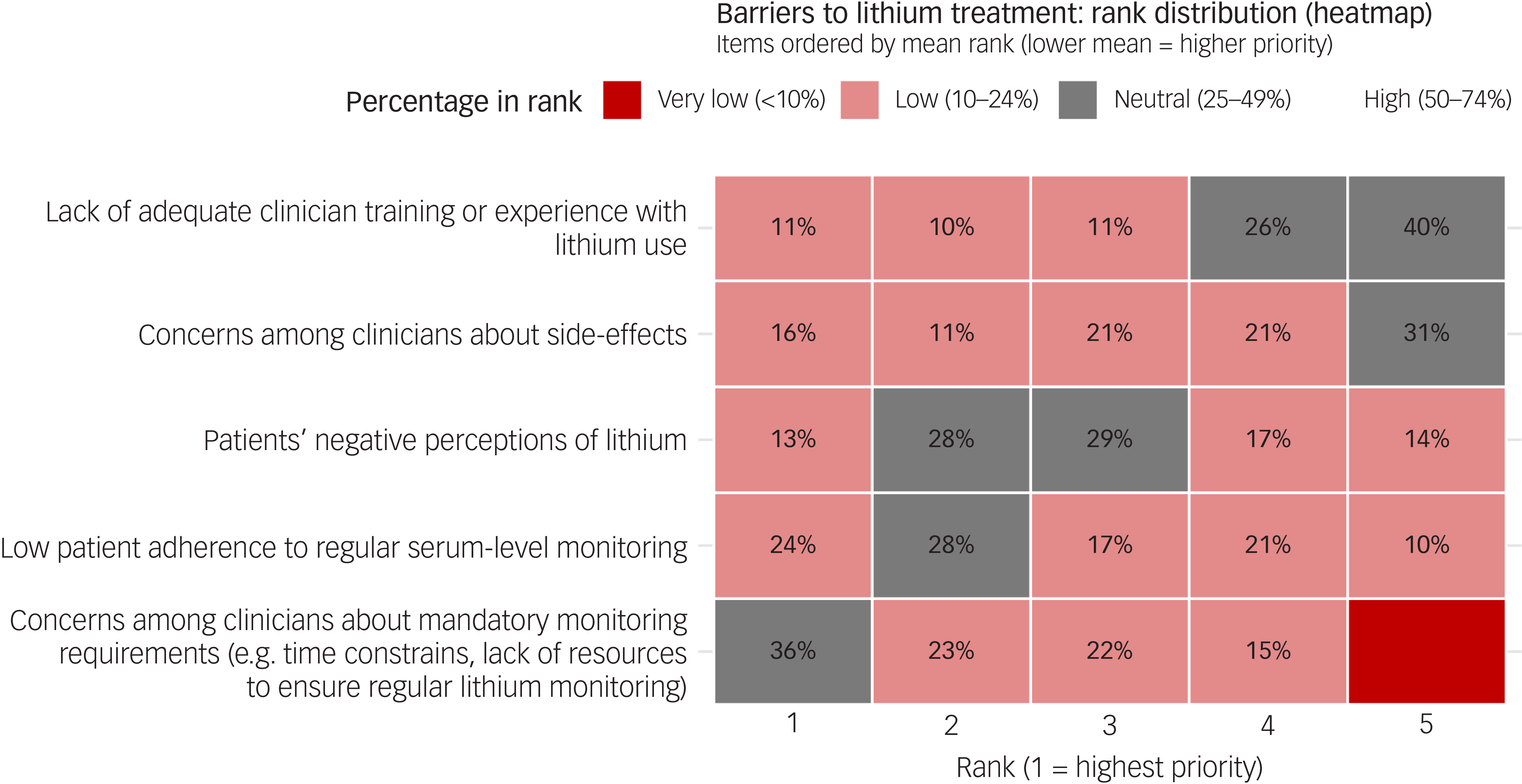
The logistical demands of lithium monitoring were identified as the biggest barrier to its prescription (36% ranked this first, and 59% ranked it in the top two; median rank 2). Low expectations about levels of patient adherence to lithium monitoring was the next largest barrier (24% ranked this first and 52% in the top two; median rank 2). Patients having a negative perception of the value of lithium treatment, clinician concerns about side-effects, and a lack of experience in prescribing lithium were much less significant barriers (40% ranked last; median rank 4). These patterns were consistent across respondents. Figure 1 shows the distribution of ranked barriers.
Heatmap of perceived barriers to lithium treatment.
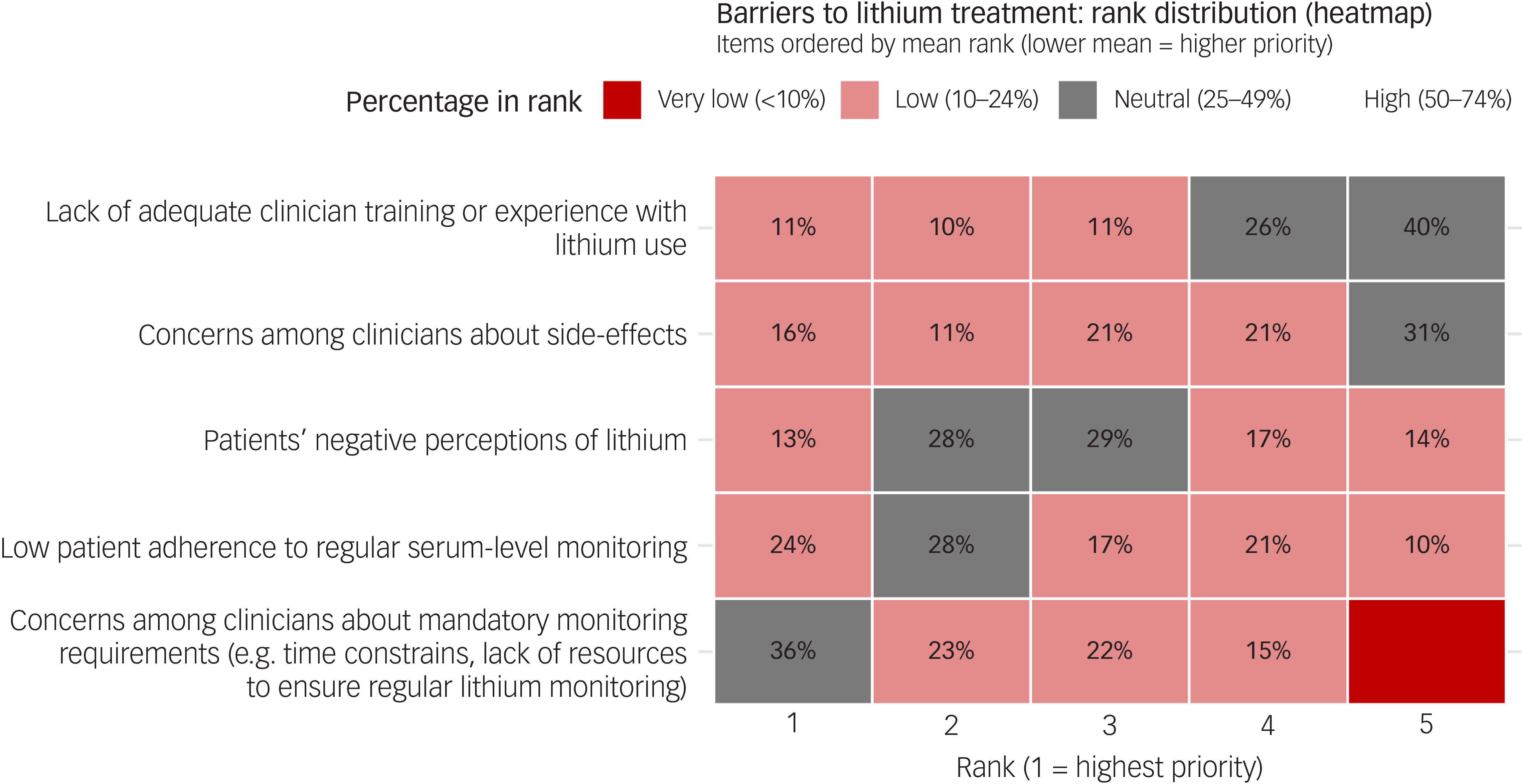
Fig. 1 Long description
The heat map illustrates barriers to lithium treatment, ranked by distribution. Items are ordered by mean rank, with lower mean indicating higher priority. The map uses a color scale to represent the percentage in rank: very low (less than 10 percent), low (10 to 24 percent), neutral (25 to 49 percent), and high (50 to 74 percent). The barriers include lack of adequate clinician training or experience with lithium use, concerns among clinicians about side-effects, patients’ negative perceptions of lithium, low patient adherence to regular serum-level monitoring, and concerns among clinicians about mandatory monitoring requirements. Each barrier is ranked from 1 to 5, with 1 being the highest priority. The color intensity indicates the percentage of respondents who ranked each barrier at that level, highlighting areas of significant concern.
Benefits of POCT
Overall, 81 participants completed the benefit of POCT section. Most clinicians (n = 54, 64.3%) believed that POCT for lithium would be beneficial in general, although 28.0% (n = 24) were unsure. Only 10.7% felt it would either not make any difference (3.6%, n = 3) or would not be beneficial (7.1%, n = 6). Regarding specific benefits of lithium POCT, 90% (n = 73) believed it would allow easier and rapid dose adjustments, 79% (n = 64) believed it would enhance patients’ engagement in their treatment, 75% (n = 61) believed it would allow better control of side-effects, 75% (n = 61) believed it would increase frequency of monitoring and 68% (n = 55) believed it would improve patient adherence to lithium.
Comparison of analytical methods
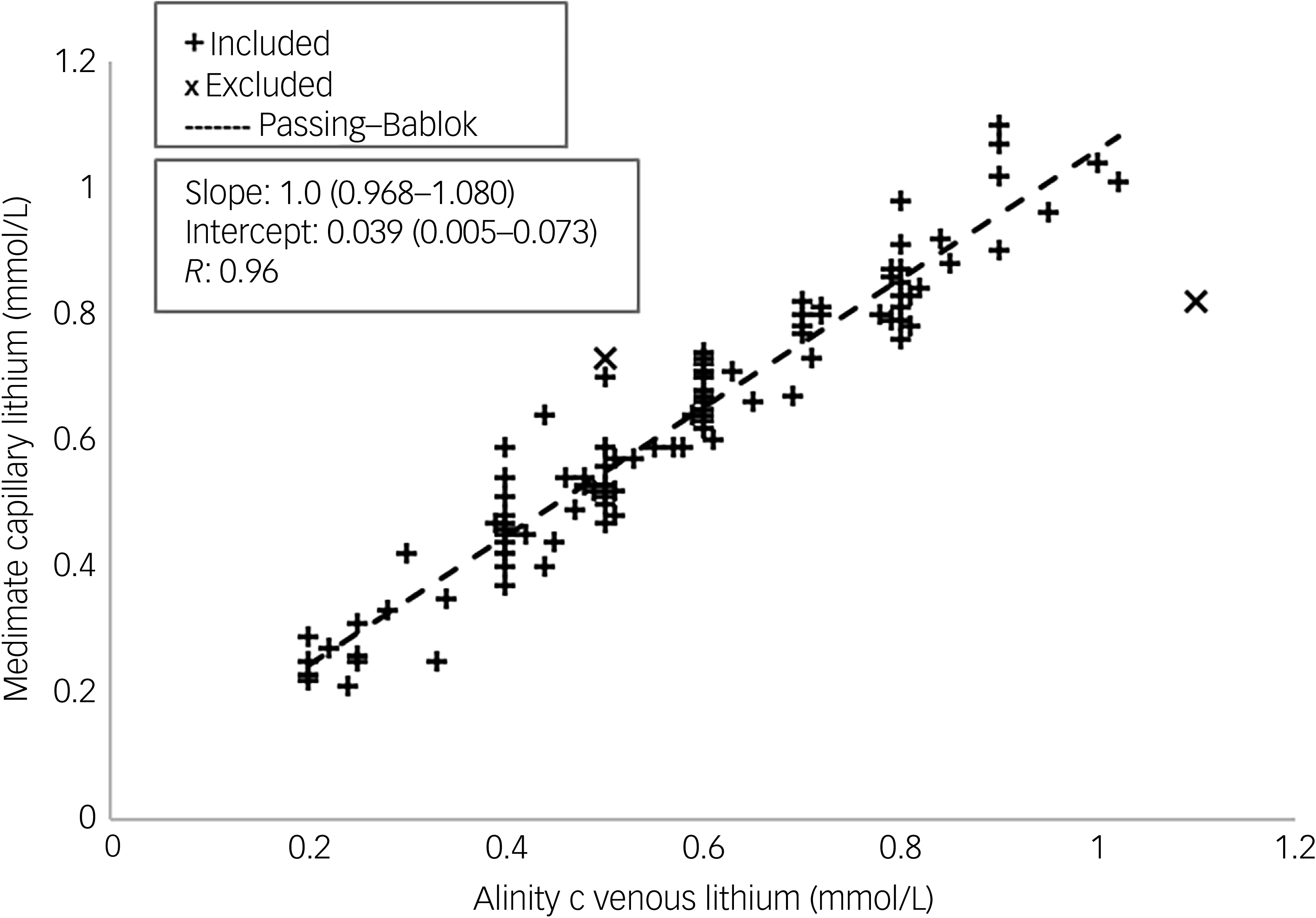
Lithium concentrations measured using the conventional laboratory-based method (Abbott Alinity c) ranged from 0.2 to 1.1 mmol/L, whereas those measured by the POCT device (Medimate Multireader) ranged from 0.21 to 1.1 mmol/L. After exclusion of two outliers (1.9%), we observed a strong correlation (r = 0.96) between the venous serum lithium concentrations obtained with the Abbott Alinity c assay and the capillary whole-blood lithium measurements made by the Medimate Multireader. The slope of the regression line was 1.0 (95% CI 0.968–1.080) with an intercept of 0.039 mmol/L (95% CI 0.005–0.073), indicating a direct and proportional relationship between the two methods (Fig. 2).
Method comparison: Medimate point of care testing versus Abbott Alinity c (excluded (x) n = 2; included (+) n = 103).
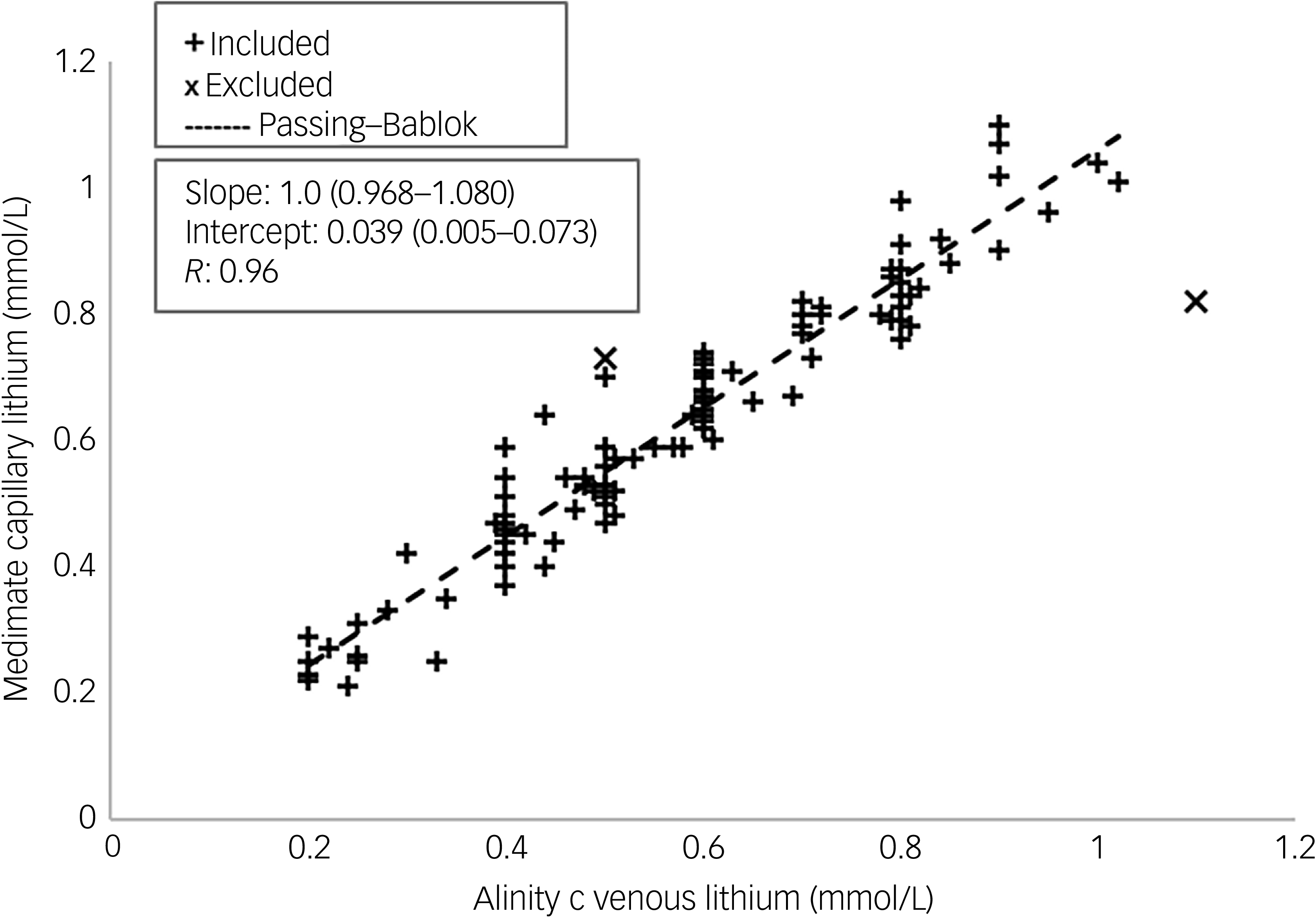
Fig. 2 Long description
A scatter plot compares Medimate capillary lithium levels to Alinity C venous lithium levels. The plot includes approximately one hundred and five data points, with a few outliers. The x-axis represents Alinity C venous lithium levels in millimoles per liter, ranging from zero to one point two. The y-axis represents Medimate capillary lithium levels in millimoles per liter, ranging from zero to one point two. Data points are marked with plus signs for included measurements and x marks for excluded measurements. A dashed Passing-Bablok regression line is present, indicating a positive correlation. The slope is one point zero with a confidence interval of zero point nine six eight to one point zero eight zero, and the intercept is zero point zero three nine with a confidence interval of zero point zero zero five to zero point zero seven three. The correlation coefficient R is zero point nine six. All values are approximated.
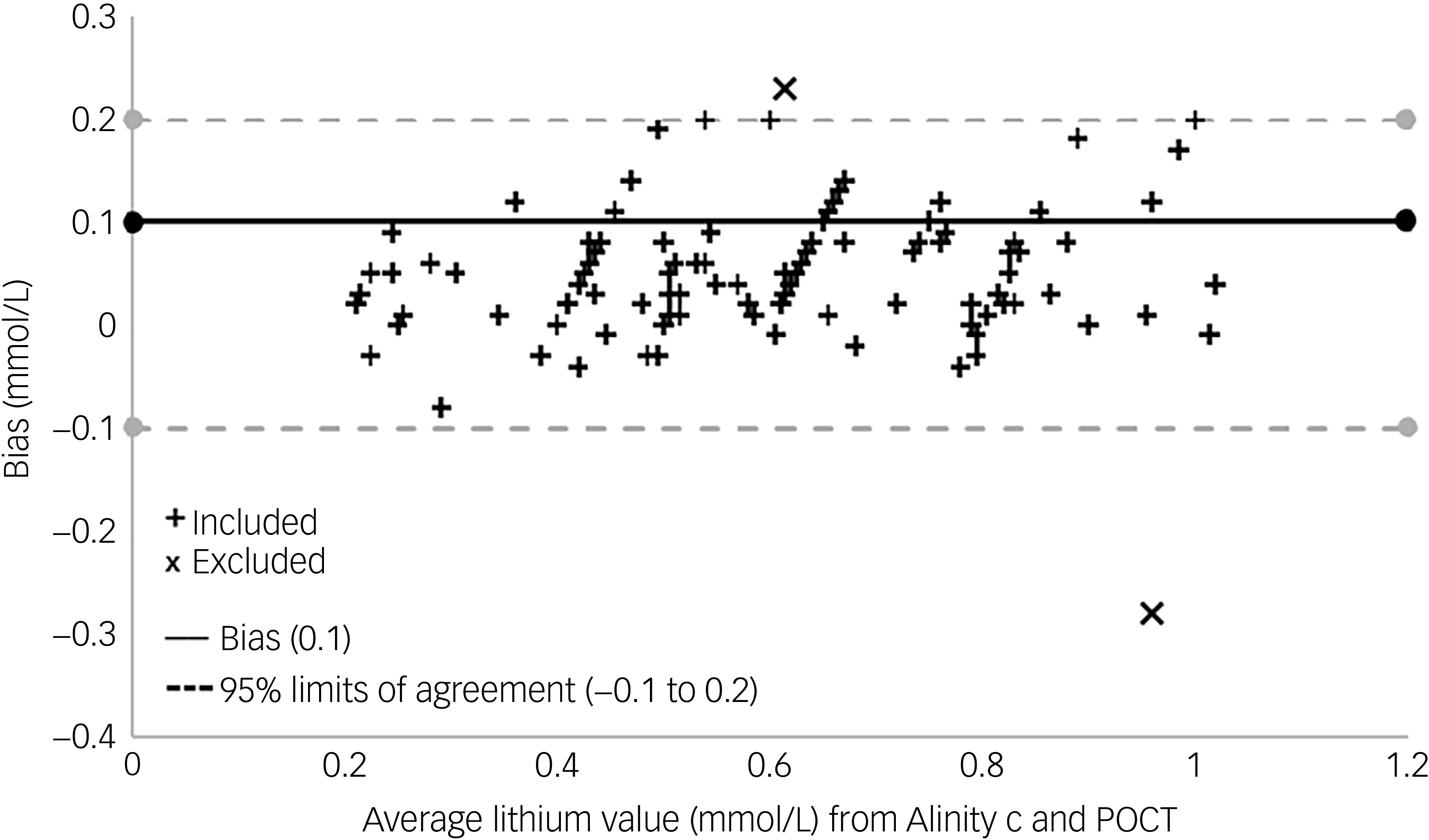
Bland–Altman analysis demonstrated a mean bias of 0.1 mmol/L (−10.1%), with 95% limits of agreement from −0.1 to 0.2 mmol/L (Fig. 3), confirming good agreement between the two methods. Partitioned bias analysis across defined concentration intervals (Table 3) showed that the bias remained consistent across the measurement range, with no detectable bias in the 0.2–0.3 mmol/L or 0.91–1.11 mmol/L interval. All mean biases and associated 95% limit of agreement values across the measurement intervals were within ±0.2 mmol/L (Table 3), meeting the predefined analytical performance specifications for method comparison (as detailed in the Methods section). These results indicate that lithium measurements obtained using the Medimate Multireader POC device are analytically comparable to those from the Abbott Alinity c across the full measurement range.
Bland–Altman plot for the difference between point-of-care testing (POCT) and Alinity c against the mean of both methods (excluded (x) n = 2; included (+) n = 103).
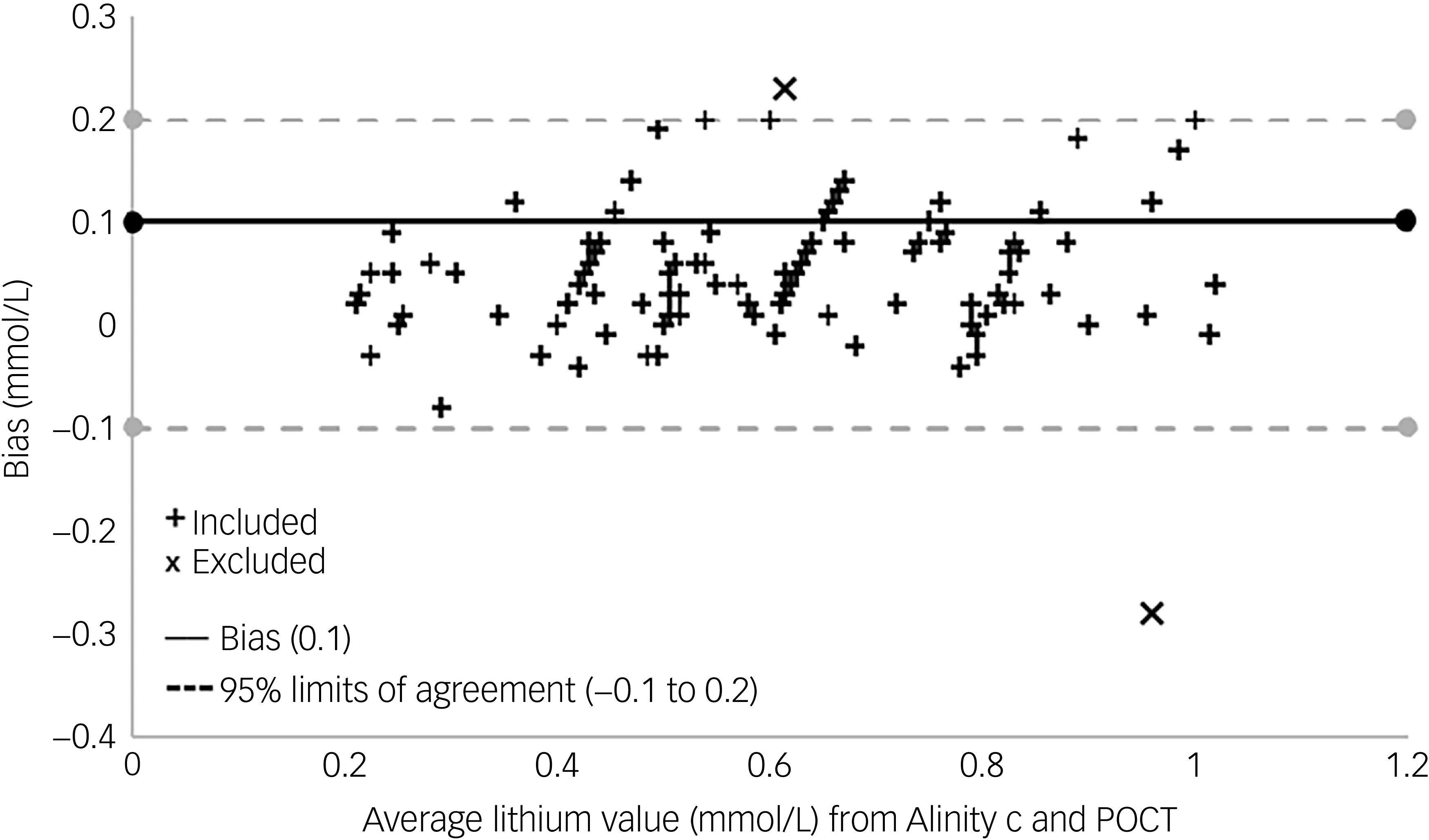
Fig. 3 Long description
A scatter plot titled BlandAltman analysis demonstrates a mean bias of 0.1 millimoles per liter (10.1%), with 95% limits of agreement from 0.1 to 0.2 millimoles per liter. The x-axis represents the average lithium value in millimoles per liter from Alinity c and POCT, ranging from 0 to 1.2 millimoles per liter. The y-axis represents the bias in millimoles per liter, ranging from -0.4 to 0.3 millimoles per liter. The plot includes 103 data points marked with plus signs and 2 excluded data points marked with x’s. A solid line indicates the mean bias of 0.1 millimoles per liter, and dashed lines indicate the 95% limits of agreement. The data points are scattered around the mean bias line, with some clustering around the 0.4 to 0.6 millimoles per liter range on the x-axis and near the 0 bias on the y-axis. There are a few outliers, particularly one notable outlier below the -0.1 bias line. The overall trend shows no strong correlation, with data points spread relatively evenly within the limits of agreement.
Two results showed unusually large differences between the Medimate Multireader POCT method and the Abbott Alinity c reference method, with one result higher and one lower on the Medimate system (Supplementary Table 1). These results were investigated to determine whether they represented true measurement differences or atypical values that could distort the overall comparison. The comparison analysis followed the Clinical and Laboratory Standards Institute EP09c guideline (2018), 25 which recommends first identifying potential outliers by visual inspection and then confirming them using statistical criteria. Visual review of the Bland–Altman plot showed that these two results fell outside the range of most other data points, suggesting that they were not consistent with the general pattern of agreement between the methods. To confirm this objectively, we examined how much each result differed from the average difference between the two methods. Values that differ by more than three standard deviations from the mean are extremely unlikely to occur by chance in normally distributed data and are therefore commonly considered to be outliers. Both results exceeded this threshold (Supplementary Figure 1), confirming that they were statistical outliers; they were consequently excluded from further analysis.
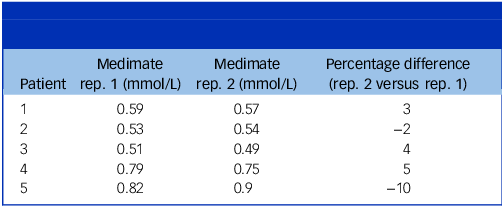
Within-patient differences in lithium concentrations in capillary blood measured using Medimate Multireader were ≤10% (Table 4).
Within-patient differences in capillary blood lithium concentration measured using Medimate
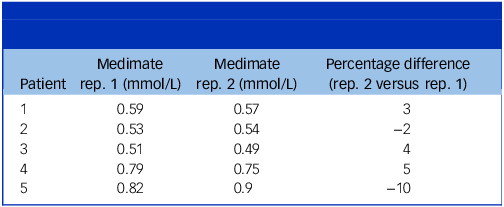
Table 4 Long description
The table presents data on within-patient differences in capillary blood lithium concentration measured using Medimate. It includes five patients with two repetitions of measurements in millimoles per liter. The table has four columns: Patient, Medimate rep. 1 (mmol/L), Medimate rep. 2 (mmol/L), and Percentage difference (rep. 2 versus rep. 1). The percentage differences range from -10 to 5. Row 1: Patient 1, Medimate rep. 1 0.59, Medimate rep. 2 0.57, Percentage difference 3. Row 2: Patient 2, Medimate rep. 1 0.53, Medimate rep. 2 0.54, Percentage difference -2. Row 3: Patient 3, Medimate rep. 1 0.51, Medimate rep. 2 0.49, Percentage difference 4. Row 4: Patient 4, Medimate rep. 1 0.79, Medimate rep. 2 0.75, Percentage difference 5. Row 5: Patient 5, Medimate rep. 1 0.82, Medimate rep. 2 0.9, Percentage difference -10.
Discussion
This study combined a comprehensive evaluation of attitudes towards lithium monitoring among patients and clinicians with a rigorous analytical validation of a novel POCT device for assessing lithium levels. We found that both patients and clinicians would prefer a POCT approach to venous blood monitoring, and that POCT could provide very similar levels of accuracy to conventional methods.
The patient and clinician surveys revealed that although lithium remains a valued and effective treatment, its continued use is constrained by the burden of regular venous blood sampling and laboratory monitoring. Many patients described the conventional monitoring process as inconvenient and disruptive, and most reported that they would be more willing to take lithium if POCT was available, especially if this could be done at home. Clinicians identified the frequency and logistical demands of venous blood monitoring as the most significant barrier to lithium use, and most believed that access to POCT would improve adherence. Overall, these findings highlight a shared recognition of a need for better means of monitoring lithium levels. Reference Dodd, Pedraza-Sanabria, Paredes Castro, Williams, Giraldo-Cadavid and Bustos26,Reference Sheikh, Qassem, Triantis and Kyriacou27
These high levels of patient and clinician acceptability with respect to a POCT approach were complemented by the technical performance of the Medimate Multireader, which produced results that were in excellent agreement with those obtained with the reference laboratory-based method: the correlation coefficient was 0.96, and the mean bias and limits of agreement were well within the predefined analytical performance specification of ±0.2 mmol/L 23,24 across the measurement range; in addition, within-patient reproducibility results supported the suitability of the device for clinical use.
Policy implications
A particular feature of the Medimate Multireader is that it can be used by a patient alone, without a clinician being present. This allows the testing to be done at home, without the need for the patient to travel to a clinic. The testing process and discussion of the result could be done with a clinician remotely – for example, via telephone or video consultation – with results communicated by the patient or transmitted using digital health platforms already available in routine care. The ability of the POCT device itself to transmit results electronically was not assessed in this study. However, our survey indicated that this approach was appealing to many patients.
The NHS Long Term Plan (2019–2029) 28 calls for digitally enabled, personalised and community-based models of care. By bringing lithium testing closer to the patient, either in clinics or at home, POCT technology exemplifies the plan’s vision of delivering care ‘closer to home’ through innovation. 29,30 It empowers patients to take an active role in managing their treatment, reflecting the commitment to self-management and shared decision-making that underpins the NHS’s transformation agenda. 31 Moreover, by reducing dependence on central laboratory infrastructure and phlebotomy services, POCT supports the drive for efficiency and workforce optimisation. Reference Plebani, Nichols, Luppa, Greene, Sciacovelli and Shaw32 In mental healthcare, in which lithium remains a gold-standard treatment yet is often underutilised owing to monitoring challenges, this approach offers a practical solution to improve access, safety and adherence, which are key objectives within the NHS Long Term Plan and Community Mental Health Framework. 28,29,33
Strengths and limitations
This study offers a comprehensive assessment of POCT for lithium by combining patient and clinician attitudes with a rigorous analytical evaluation of a novel device. The use of predefined analytical performance criteria and direct comparison with a reference laboratory method strengthens confidence in the accuracy and reliability of the findings. Insights from both patients and clinicians provide valuable context on the practical barriers to lithium treatment and the potential role of POCT in improving adherence and acceptability.
However, as the surveys were conducted within a single NHS trust, they may not capture the full diversity of perspectives across different regions or service settings, Reference Welsby and Weatherall34 and the sample sizes were relatively modest. Although the analytical performance of the Medimate Multireader was confirmed under controlled conditions, further work is needed to assess its cost-effectiveness when used at scale in routine clinical care. Reference Lingervelder, Koffijberg, Kusters and IJzerman35,Reference Dózsa, Horváth, Cserni and Cseh36 Health economic evaluations and real-world implementation studies will be essential to determine its broader clinical utility. Furthermore, although the Medimate Multireader is technically capable of measuring creatinine, sodium, potassium, TSH and serum calcium from the same test sample, these parameters were not analytically available for comparison with the laboratory reference method at the time of this evaluation; they are currently under development by the manufacturer. In clinical practice, this means that although POCT lithium measurements may be substituted for some scheduled laboratory lithium level checks (for example, interim or 3 monthly lithium-only assessments in stable patients), they cannot currently replace comprehensive laboratory monitoring, which remains necessary at regular intervals (typically 6 monthly) to assess renal, thyroid, electrolyte and calcium status.
Consequently, any future health economic evaluation of POCT lithium monitoring will need to account for its role as a partial rather than complete substitute for laboratory testing under current assay availability. Potential benefits may therefore relate to reduced phlebotomy, faster clinical decision-making, and improved convenience at selected monitoring visits, rather than elimination of routine laboratory testing.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10695
Data availability
The data supporting the findings of this study are available within the article and its supplementary material.
Author contributions
M.A. and P.M. conceived the study; M.A., P.M., C.L., E.O., C.C., D.M., D.O. and A.C. contributed to study design; C.L. undertook all patient testing; M.A., E.O., P.M. and C.L. contributed to the data analysis; and M.A., E.O. and P.M. drafted the manuscript.
Funding
This study was funded by NIHR Oxford Health Biomedical Research Centre (grant NIHR203316). The funding body had no role in the design, execution, analysis or reporting of the study.
Declaration of interest
All authors have completed the ICMJE uniform disclosure form at https://www.icmje.org/disclosure-of-interest/ and declare support from Oxford Health NHS Foundation Trust NIHR Biomedical Research Centre Data Science Theme; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; and no other relationships or activities that could appear to have influenced the submitted work. M.A. reports consultancy fees from Saladax Biomedical. A.C. is supported by the NIHR Oxford Cognitive Health Clinical Research Facility, an NIHR research professorship (grant RP-2017-08-ST2-006), the NIHR Oxford and Thames Valley Applied Research Collaboration, the NIHR Oxford Health Biomedical Research Centre (grant NIHR203316) and the Wellcome Trust (Global Alliance for Living Evidence on Anxiety, Depression and Psychosis Project) and has received research, educational and consultancy fees from INCiPiT (Italian Network for Paediatric Trials), CARIPLO Foundation, Lundbeck and Angelini Pharma. P.M. reports consultancy fees from Takeda, Janssen, GW Pharmaceuticals, Roche and Sunovion. P.M. is an editorial advisor to the British Journal of Psychiatry but had no involvement in the editorial, peer review or decision-making process for this manuscript.



 Open access
Open access
eLetters
No eLetters have been published for this article.