



Impact statement
Humanitarian and community-based health programs serving displaced populations often include mental health screening as the first step toward care. Yet many screening tools are used without local psychometric evidence or clear guidance on interpretation in conflict-affected settings. This study helps address this gap by evaluating the WHO-5 Well-Being Index among internally displaced persons in Abuja, Nigeria. The findings indicate that the WHO-5 is a brief and reliable measure of well-being in this setting and that low scores may serve as useful proxy markers for elevated depressive symptom burden rather than a clinical diagnosis. By comparing widely used cutoffs, the study shows how threshold selection affects sensitivity and specificity for classifying probable moderate-to-severe depressive symptoms. These findings provide actionable guidance for humanitarian and primary care programs to standardize screening thresholds, strengthen referral pathways and allocate scarce psychosocial resources more efficiently.
Introduction
Depression is among the leading causes of disability worldwide and disproportionately affects populations exposed to conflict and displacement (Bedaso and Duko, Reference Bedaso and Duko2022). Globally, more than 83.4 million internally displaced persons (IDPs) remain within their countries’ borders (Supplementary Figure S1), many of whom have endured repeated trauma, violence, loss of family members and destruction of homes, and continue to face chronic stressors such as food insecurity, overcrowded shelters and precarious futures (2025 Global Report on Internal Displacement [GRID], 2025; Charlson et al., Reference Charlson, Van Ommeren, Flaxman, Cornett, Whiteford and Saxena2019). Approximately one in five individuals in conflict-affected settings meets criteria for a mental disorder, with depression and post-traumatic stress disorder predominating (Charlson et al., Reference Charlson, Van Ommeren, Flaxman, Cornett, Whiteford and Saxena2019). Older adults in such contexts often exhibit even higher rates of depressive symptoms, reflecting cumulative adversity across the lifespan and the erosion of traditional social supports (Van Boetzelaer et al., Reference Van Boetzelaer, Keating, Wasara, Rodriguez, Escobio, Pellecchia, Van De Kamp, Dada, Franco, Fredj, Kagomba Barathi, Akaso, Staunton, Browne, Caleo and Sleit2025).
In Northern Nigeria, over two million people have been displaced (Ezeh, Reference Ezeh2024) by the long running Boko Haram insurgency (Ajayi, Reference Ajayi2020), ethno-religious conflicts (Agbiboa, Reference Agbiboa2013), farmer herder and communal violence (Peter Yikwab and Tade, Reference Peter Yikwab and Tade2022) and natural disasters (Eboreime et al., Reference Eboreime, Anjorin, Obi-Jeff, Ojo and Hertelendy2025). Many IDPs live in government-run camps or informal settlements with severely limited access to essential services and psychosocial support (Gwadabe et al., Reference Gwadabe, Salleh, Ahmad and Jamil2018; Ezeh, Reference Ezeh2024). Compounding these challenges, Nigeria’s mental health system remains under-resourced (Abdulmalik et al., Reference Abdulmalik, Kola and Gureje2016). Specifically, fewer than 300 psychiatrists serve a country of more than 200 million people (Adeleke et al., Reference Adeleke, Akinbode, Aibangbee, Orji, Oluwasanya, Adekunle, Oduniyi, Olabode and Ariba2025), and until recently, there was no cohesive national mental health legislation (Aluh et al., Reference Aluh, Onu and De Almeida2023). Traditional and religious healing practices remain the dominant first point of contact for mental health concerns in Nigeria due to their cultural acceptability and accessibility (Gureje et al., Reference Gureje, Nortje, Makanjuola, Oladeji, Seedat and Jenkins2015), emphasizing that help-seeking often occurs outside of formal health systems rather than not at all (Gidado et al., Reference Gidado, Musa, Ba’aba, Okeke, Nguku, Hadejia, Hassan, Bande, Onuoha, Ugbenyo, Godwin, Usman, Manu, Mohammed, Abdullahi, Bammami, Nuorti and Atkins2023). In this context, early identification of depression is essential so that individuals who screen positive can be linked to appropriate psychosocial support and clinical care in high-need, low-resource humanitarian settings such as IDP camps.
Symptom-focused instruments like the Hopkins Symptom Checklist (HSCL-25) and Patient Health Questionnaire-9 (PHQ-9) are well validated across many populations (Kroenke et al., Reference Kroenke, Spitzer and Williams2001; Sivertsen et al., Reference Sivertsen, Skogen, Reneflot, Knapstad, Smith, Aarø, Kirkøen, Lagerstrøm and Knudsen2024), but their direct questioning about sadness, guilt or anhedonia can be stigmatizing in communities where admitting these feelings carries social risk (Oshodi et al., Reference Oshodi, Abdulmalik, Ola, James, Bonetto, Cristofalo, Van Bortel, Sartorius and Thornicroft2014; Clement et al., Reference Clement, Schauman, Graham, Maggioni, Evans-Lacko, Bezborodovs, Morgan, Rüsch, Brown and Thornicroft2015). Additionally, somatic items related to sleep and appetite may be confounded by the hardships of camp life, for example, overcrowding, food shortages and poor sanitation, potentially undermining specificity (Ventevogel et al., Reference Ventevogel, Jordans, Reis and De Jong2013). Camp-based health workers, who frequently have limited specialized training in mental health, benefit from screening tools that are brief, easy to administer and positively framed (Keynejad et al., Reference Keynejad, Spagnolo and Thornicroft2021).
The World Health Organization’s Five Well-Being Index (WHO-5) (WHO-Reference Adewale5, 2024) is one such instrument. Comprising only five items that assess positive emotional states (e.g., feeling calm, active and rested), the WHO-5 has shown robust internal consistency (Cronbach’s α = 0.85–0.95) and a unidimensional structure across diverse settings (Topp et al., Reference Topp, Østergaard, Søndergaard and Bech2015). In primary care contexts, a score of 13 or less (scaled to ≤50 on a 0–100 metric) indicates good sensitivity and specificity for major depression, while a lower threshold (e.g., ≤7, scaled to ≤28) has been explored to maximize specificity for moderate–severe cases (Hajos et al., Reference Hajos, Pouwer, Skovlund, Den Oudsten, Geelhoed-Duijvestijn, Tack and Snoek2013; Topp et al., Reference Topp, Østergaard, Søndergaard and Bech2015).
Crucially, because the WHO-5 measures positive emotional functioning rather than symptom pathology, it is well-suited for depression screening in Nigerian displacement settings. Its nonstigmatizing, well-being focus aligns with African collectivist values that prioritize communal harmony, social connectedness and resilience, while its positive framing may also improve acceptability and disclosure in contexts where these bonds have been fractured by conflict and violence (Bech et al., Reference Bech, Olsen, Kjoller and Rasmussen2003; Jansen et al., Reference Jansen, Niyonzima, Gerbarg, Brown, Nsengiyumva, Niyonsenga and Nsabimana2024; Salihu et al., Reference Salihu, Chutiyami, Bello, Wong, Pich, Alsharari, Ali, Sulaiman and Kwan2024).
Validation studies in low- and middle-income countries (LMICs) lend strong support to the WHO-5’s adaptability for depression screening. In Ethiopia, the Amharic WHO-5 demonstrated high internal consistency (α = 0.83) and good screening performance relative to the PHQ-9 (Garland et al., Reference Garland, Deyessa, Desta, Alem, Zerihun, Hall, Goren and Fish2018), while recommended cutoffs of ≤50 and ≤28 for detecting depressive symptoms are described in the broader WHO-5 literature (Topp et al., Reference Topp, Østergaard, Søndergaard and Bech2015). Additionally, clinical validation in Lebanon showed that the WHO-5 achieved good discrimination for depression among patients with schizophrenia (area under the curve [AUC] = 0.84), with acceptable sensitivity (0.80) and specificity (0.70) when compared against a structured clinical rating scale (Fekih-Romdhane et al., Reference Fekih-Romdhane, Al Mouzakzak, Abilmona, Dahdouh and Hallit2024).
Together, these findings highlight the WHO-5’s potential utility across diverse LMIC contexts and support evaluating both ≤50 and ≤28 thresholds to determine the optimal balance of sensitivity and specificity in resource-constrained, high-distress settings.
Despite this promise, to our knowledge, no study has psychometrically evaluated the WHO-5 for depression screening among IDPs in Nigeria or across Hausa-speaking communities in the Sahel. Given the cultural and linguistic continuity from Northern Nigeria through Mali, Niger, Chad and Cameroon (Bhui, Reference Bhui2012), establishing a locally validated cutoff for the WHO-5 in Northern Nigerian IDP settings would enable more accurate depression screening and could inform practice in similar humanitarian contexts (Kohrt and Kaiser, Reference Kohrt and Kaiser2021a) across West and Central Africa. A brief, positively framed tool like the WHO-5 can be administered by nonspecialist health workers to support early identification of depression and referral to limited psychosocial services, and it can be feasibly integrated into primary care and humanitarian programs serving displaced populations (Petagna et al., Reference Petagna, Marley, Guerra, Calia and Reid2023; Raghuram et al., Reference Raghuram, Rajguru, Pathiyil, Brahmbhatt, Bhan, Spagnolo and Naslund2025).
To address these aims, this study had three objectives: (1) to describe the distribution of depression (PHQ-9) and well-being (WHO-5) scores by age and sex to provide demographic context for interpreting mental health patterns among IDPs; (2) to evaluate the reliability and validity of the WHO-5 as a depression screening tool among Hausa speaking IDPs in Abuja, Nigeria; and (3) to determine the optimal WHO-5 screening cutoff for depression by comparing the conventional ≤50 threshold with the more stringent ≤28 threshold.
Materials and methods
Study design, setting and participants
This study analyzed baseline cross-sectional (pre-intervention) data from the Rebuilding Emotional Stability and Strength Through Therapeutic and Life-Skills Education for Internally Displaced Persons in Nigeria (RESETTLE-IDPs) trial (NCT06412679 [https://clinicaltrials.gov/study/NCT06412679]) (Eboreime et al., Reference Eboreime, Obi-Jeff, Orji, Ojo, Iyamu, Harri, Said, Oguntimehin, Ibrahim, Anjorin, Duke, Musami, Liebenberg, Crider, Wagami, Dahiru, Uneke, Yaya and Agyapong2024). The initiative focuses on improving psychosocial well-being, resilience and integration of IDPs affected by conflict in Northern Nigeria and supports their long-term adjustment by promoting coping strategies and improving access to humanitarian aid (Eboreime et al., Reference Eboreime, Obi-Jeff, Orji, Ojo, Iyamu, Harri, Said, Oguntimehin, Ibrahim, Anjorin, Duke, Musami, Liebenberg, Crider, Wagami, Dahiru, Uneke, Yaya and Agyapong2024). Participants were recruited from two IDP camps in Durumi and Wassa, within Abuja, Federal Capital Territory (FCT), North Central Nigeria.
Abuja has become a major destination for displaced individuals escaping the conflict-ridden northeastern states of Borno, Adamawa and Yobe (BAY states) (Adewale, Reference Adewale2016a). Approximately 20,659 IDPs from these states reside across 18 informal settlements within Abuja’s six local government areas, with each settlement averaging 2,000 inhabitants (Adewale, Reference Adewale2016b; Oyinwola et al., Reference Oyinwola, Ahmed, Odusanya and Oyasakin2022a). This concentration of IDPs from multiple conflict epicenters makes Abuja a strategically relevant location for studying mental health outcomes among displaced populations.
Durumi and Wassa IDP camps offer similar, albeit distinct, environments while accommodating displaced communities. Durumi, situated in the urban Area 1 of Abuja Municipal Area Council, hosts a majority of IDPs from Borno State who fled the Boko Haram insurgency (Ifeanyi, Reference Ifeanyi, Mawere and Nhemachena2018). This settlement benefits from urban infrastructure and educational initiatives, such as the School Without Walls program by the Life Builders Initiative (Adewale, Reference Adewale2016c; Oyinwola et al., Reference Oyinwola, Ahmed, Odusanya and Oyasakin2022b). In contrast, Wassa, located in a more remote area within the same municipal council, faces significant infrastructural deficits (Ekoh et al., Reference Ekoh, Okoye, George, Chukwuemeka and Agbawodikeizu2023). Many residents live in temporary shelters with limited access to essential services (Olaoye, Reference Olaoye2022; Ofoma et al., Reference Ofoma, Audu and Nkata2025). While both camps rely on nongovernmental organizations (NGOs) for healthcare and humanitarian assistance, Wassa’s remote location presents additional barriers to accessing these services compared to Durumi’s more centrally positioned settlement (Ifeanyi, Reference Ifeanyi, Mawere and Nhemachena2018; Agbaje, Reference Agbaje2020).
Participants were selected using a probability-based approach implemented in two stages, based on the official household registers for each camp. First, simple random sampling was applied to the complete household registers in Durumi and Wassa (Durumi: 387 households; Wassa: 743 households) to select 150 households per camp, yielding 300 sampled households overall. Second, within each selected household, field staff enumerated all residents who met eligibility criteria and randomly selected one eligible individual to participate. Eligibility required residence in the selected household and age 13 years or older. Recruitment emphasized adults aged 18 years or older. Adolescents aged 13–17 years were enrolled when present, contingent on written assent and written parental or guardian consent. No upper age limit was imposed. Of the 300 households approached, 264 individuals enrolled, yielding an 88.0% response rate.
The distribution of participants across camps reflects the underlying camp structure documented in the household registers. Wassa is substantially larger than Durumi, with 743 registered households compared with 387, and any predominance of participants from Wassa is consistent with this larger sampling frame and the broader RESETTLE-IDPs study context.
All adult participants provided written informed consent. Adolescents aged 13–17 years were required to give assent with parental consent before enrollment. Participants who lacked capacity, were severely cognitively impaired and unable to give consent or assent, or were with acute medical or mental health crises necessitating immediate intervention or referral were excluded.
Data collection and analysis
Data collection and analysis occurred between October 2024 and November 2025. Data were collected through structured, interviewer-administered surveys.
Language administration and instrument adaptation
Trained personnel administered the surveys to ensure comprehension and accuracy. The instrument adaptation process included consultation with various stakeholders (e.g., IDPs, camp leaders and content experts). Transcript coding using content analysis continued until thematic saturation was reached (Penton et al., Reference Penton, Dayson, Hulme and Young2022). Hausa translations of the WHO-5 were back-translated to verify semantic equivalence with the original English version (Mallinckrodt and Wang, Reference Mallinckrodt and Wang2004; Yu et al., Reference Yu, Lee and Woo2004). The Hausa version of the WHO-5 (Supplementary Table S5.1) was psychometrically validated in this sample.
Statistical software
All statistical analyses were performed using Stata version 18.0 (StataCorp, College Station, TX) (Stata: Release 18. Statistical Software., 2023) and R version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria). Confirmatory factor analysis (CFA) was conducted in R using the lavaan package. The CFA path diagram was produced using semPlot (Epskamp, Reference Epskamp2015).
Internal consistency
The internal consistency of the WHO-5 was assessed using Cronbach’s alpha (α). Because WHO-5 items are ordinal, α was computed from a polychoric correlation matrix. McDonald’s omega ( ω) total was also computed as a complementary reliability estimate for the total score. Corrected item total correlations were examined to evaluate the contribution of each item to the overall scale.
Construct validity
Construct validity was assessed using Spearman’s rank correlation coefficient (ρ) between WHO-5 total scores and PHQ-9 total scores. A moderate-to-strong negative correlation was hypothesized because higher well-being is expected to correspond to lower depressive symptom severity (Weijers et al., Reference Weijers, Rasing, Creemers, Vermulst, Schellekens and Westerhof2022).
To evaluate whether this association was consistent across demographic subgroups, that is, whether the direction and magnitude of the WHO-5 and PHQ-9 association were similar across age groups and sex, we produced a stratified descriptive plot. We grouped age into five categories (13–19, 20–24, 25–29, 30–34, and ≥ 35 years [35+]), and coded sex as male or female based on the recorded variable.
For each age stratum, we plotted WHO-5 scores against PHQ-9 scores, and included sex-specific fitted lines with 95% confidence intervals overlaid. Point jittering was applied to reduce overlap.
Factorial validity
Factorial validity was assessed using CFA within a structural equation modeling (SEM) framework to evaluate whether the WHO-5 functioned as a unidimensional measure of well-being. A single latent factor, “Well-being,” was specified with the five WHO-5 items as ordered categorical indicators.
Estimation and model fit indices
CFA models were estimated using the weighted least-squares mean and variance-adjusted estimator (WLSMV), which is appropriate for ordinal indicators (Nussbeck et al., Reference Nussbeck, Eid and Lischetzke2006). Model fit was evaluated using the chi-square goodness-of-fit test, Comparative Fit Index (CFI), Tucker–Lewis Index (TLI), root mean square error of approximation (RMSEA) with 90% confidence intervals, and standardized root mean square residual (SRMR). Values of CFI and TLI at or above 0.95, RMSEA at or below 0.06 and SRMR at or below 0.08 were used to indicate acceptable fit.
Local dependence, modification indices and sensitivity analysis
To avoid model overfitting, the primary CFA model was estimated without correlated residuals. Modification indices (MIs) were examined to identify potential localized misfit, together with the expected parameter change (EPC), which estimates how much a fixed parameter would change if freely estimated, and the standardized EPC to aid interpretation of magnitude (Nussbeck et al., Reference Nussbeck, Eid and Lischetzke2006; Goretzko et al., Reference Goretzko, Siemund and Sterner2024). A sensitivity model was then estimated, allowing correlated residuals only between item pairs suggested by modification indices and judged substantively plausible due to overlapping item content. A CFA path diagram was used to display standardized factor loadings from the primary model.
Receiver operating characteristic analysis
The performance of the WHO-5 in classifying participants with probable moderate-to-severe depressive symptoms was evaluated using receiver operating characteristic (ROC) curve analysis (Weinstein et al., Reference Weinstein, Berwick, Goldman, Murphy and Barsky1989; Wyshak et al., Reference Wyshak, Barsky and Klerman1991). ROC analysis is a widely used method for assessing a screening tool’s ability to discriminate between individuals above and below a prespecified reference threshold (Weinstein et al., Reference Weinstein, Berwick, Goldman, Murphy and Barsky1989; Wyshak et al., Reference Wyshak, Barsky and Klerman1991). The area under the ROC curve (AUC) was calculated to quantify discrimination ability, with values ≥0.70 indicating acceptable performance, ≥0.80 indicating good performance and ≥0.90 indicating excellent discrimination (Carter et al., Reference Carter, Pan, Rai and Galandiuk2016).
WHO-5 cutoff thresholds
Two WHO-5 cutoff scores were evaluated for screening: WHO-5 ≤ 28 and WHO-5 ≤ 50. These thresholds were chosen based on previous research demonstrating their utility for identifying low well-being and elevated depressive symptom burden in relation to depression screening outcomes (Lowe, Reference Lowe2004; Topp et al., Reference Topp, Østergaard, Søndergaard and Bech2015; Sischka et al., Reference Sischka, Costa, Steffgen and Schmidt2020a). WHO-5 scores ≤50 are commonly used to indicate low well-being consistent with elevated depressive symptom burden that may warrant further clinical assessment, while WHO-5 scores ≤28 indicate very low well-being and have been used as a more stringent threshold in validation studies (Lowe, Reference Lowe2004; Topp et al., Reference Topp, Østergaard, Søndergaard and Bech2015; Sischka et al., Reference Sischka, Costa, Steffgen and Schmidt2020b).
Sensitivity and specificity
Sensitivity and specificity were calculated for each cutoff to determine how well the WHO-5 classified individuals with and without probable moderate-to-severe depressive symptoms, using a PHQ-9 score ≥ 10 as the reference standard (Manea et al., Reference Manea, Gilbody and McMillan2012; Levis et al., Reference Levis, Benedetti and Thombs2019). Sensitivity measures the proportion of reference-positive individuals correctly identified, while specificity measures the proportion of reference-negative individuals correctly identified (Payne et al., Reference Payne, Barry, Creedon, Stone, Sweeney, O’ Brien and van O’ Sulli2007; Michel et al., Reference Michel, Schultze-Lutter and Schimmelmann2014). This approach assesses agreement between screening thresholds and does not constitute a clinical diagnosis of depression.
Youden’s index, likelihood ratios and predictive values
To determine the most effective cutoff point for screening in this population, Youden’s index (J) was calculated for WHO-5 ≤ 28 and WHO-5 ≤ 50. Youden’s index is defined as J = sensitivity + specificity − 1 (Mitchell and Coyne, Reference Mitchell and Coyne2007; Michel et al., Reference Michel, Schultze-Lutter and Schimmelmann2014; Poole et al., Reference Poole, Liao, Larson, Hedt-Gauthier, Raymond, Bärnighausen and Smith Fawzi2020). A higher Youden’s index indicates a better balance between sensitivity and specificity (Mitchell and Coyne, Reference Mitchell and Coyne2007; Michel et al., Reference Michel, Schultze-Lutter and Schimmelmann2014; Poole et al., Reference Poole, Liao, Larson, Hedt-Gauthier, Raymond, Bärnighausen and Smith Fawzi2020). Positive likelihood ratios and negative likelihood ratios were also computed. The positive likelihood ratio (+LR) reflects how much more likely a positive WHO-5 screen is among individuals with probable moderate-to-severe depressive symptoms compared with those below the reference threshold, while the negative likelihood ratio (−LR) reflects how much less likely a negative WHO-5 screen is among individuals with probable moderate-to-severe depressive symptoms (Mitchell and Coyne, Reference Mitchell and Coyne2007; Michel et al., Reference Michel, Schultze-Lutter and Schimmelmann2014). Positive predictive value and negative predictive value were calculated to estimate the probability of PHQ-9 ≥ 10 given a positive or negative WHO-5 screening result, respectively.
Cutoff comparison and selection
The performance metrics of the two WHO-5 cutoffs were compared to determine the most appropriate cutoff for screening in this setting. The final selection was based on sensitivity, specificity and the practical implications of misclassification in a resource-limited humanitarian context (Poole et al., Reference Poole, Liao, Larson, Hedt-Gauthier, Raymond, Bärnighausen and Smith Fawzi2020; Kohrt and Kaiser, Reference Kohrt and Kaiser2021b).
Results
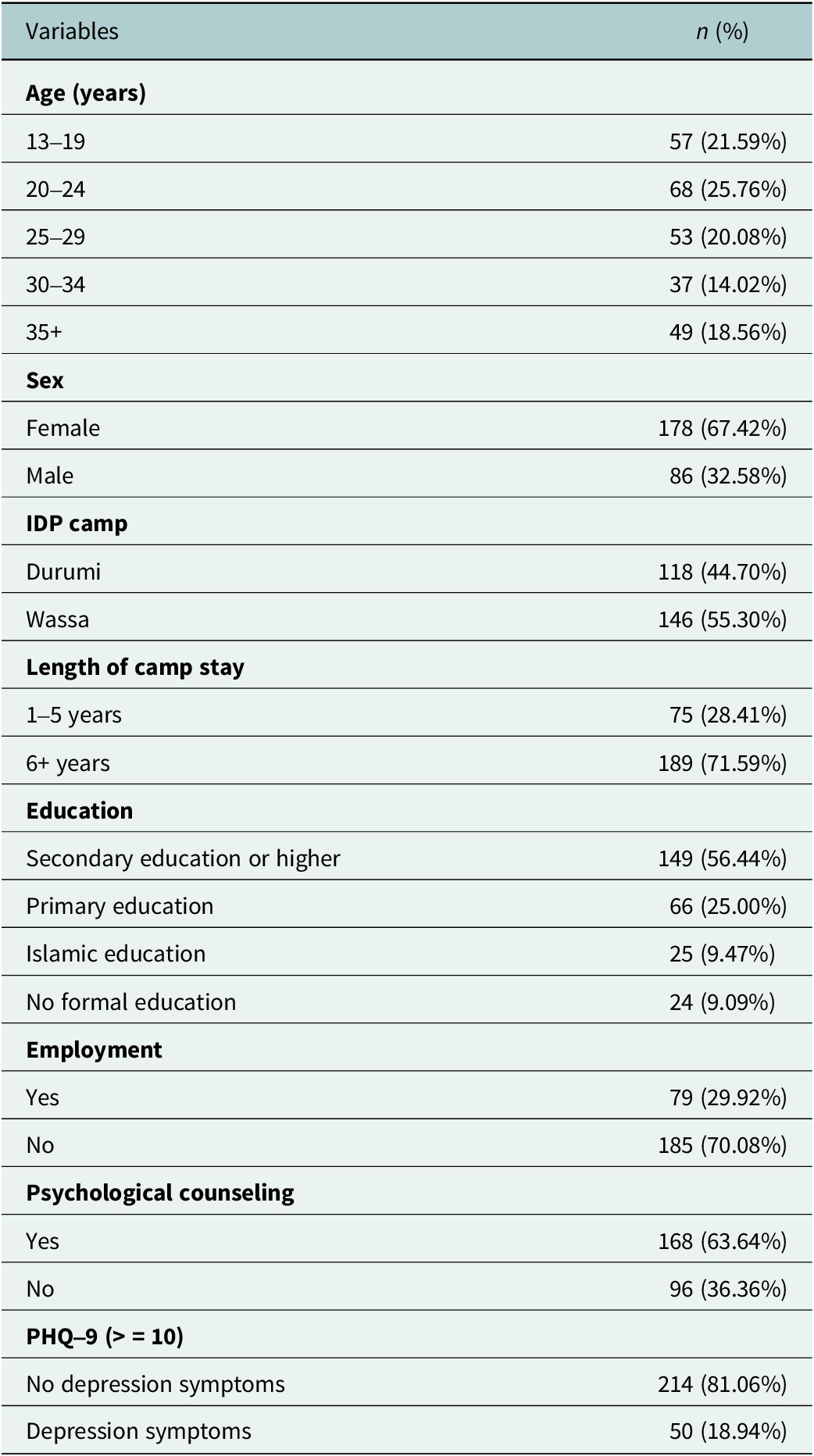
There were 264 IDPs (67.4% female; 55.3% from Wassa and 44.7% from Durumi). Age distributions were as follows: 13–19 years (21.6%), 20–24 years (25.8%), 25–29 years (20.1%), 30–34 years (14.0%) and 35+ years (18.6%). Most participants had lived in the camp for 6+ years (71.6%). Over half had at least a secondary education (56.4%), 70.1% were unemployed and 63.6% had received psychological counseling. Based on PHQ-9 ≥ 10, 18.9% met the threshold for probable moderate-to-severe depressive symptoms (Table 1).
Participant characteristics

Among females, mean PHQ-9 scores increased from 4.86 (SD 4.65) in 13–19 year olds to 7.87 (SD 5.95) in participants aged 35 years or older, while mean WHO-5 scores decreased from 71.03 (SD 24.86) in 13–19 year olds to 44.00 (SD 27.81) in participants aged 35 years or older. Among males, mean PHQ-9 scores ranged from 3.50 (SD 4.06) in 13–19 year olds to 6.84 (SD 5.18) in participants aged 35 years or older, and mean WHO-5 scores ranged from 64.71 (SD 30.19) in 13–19 year olds to 52.42 (SD 29.30) in participants aged 35 years or older (Supplementary Table S1).
Internal consistency
The WHO-5 demonstrated excellent internal consistency. Ordinal Cronbach’s alpha, computed from a polychoric correlation matrix, was 0.908 based on 264 complete observations. McDonald’s omega total was 0.909. Corrected item total correlations were uniformly high and ranged from 0.714 to 0.793. Item 1 (I have felt cheerful and in good spirits) was 0.792, Item 2 (I have felt calm and relaxed) was 0.793, Item 3 (I have felt active and vigorous) was 0.766, Item 4 (I woke up feeling fresh and rested) was 0.779 and Item 5 (My daily life has been filled with things that interest me) was 0.714.
Construct validity
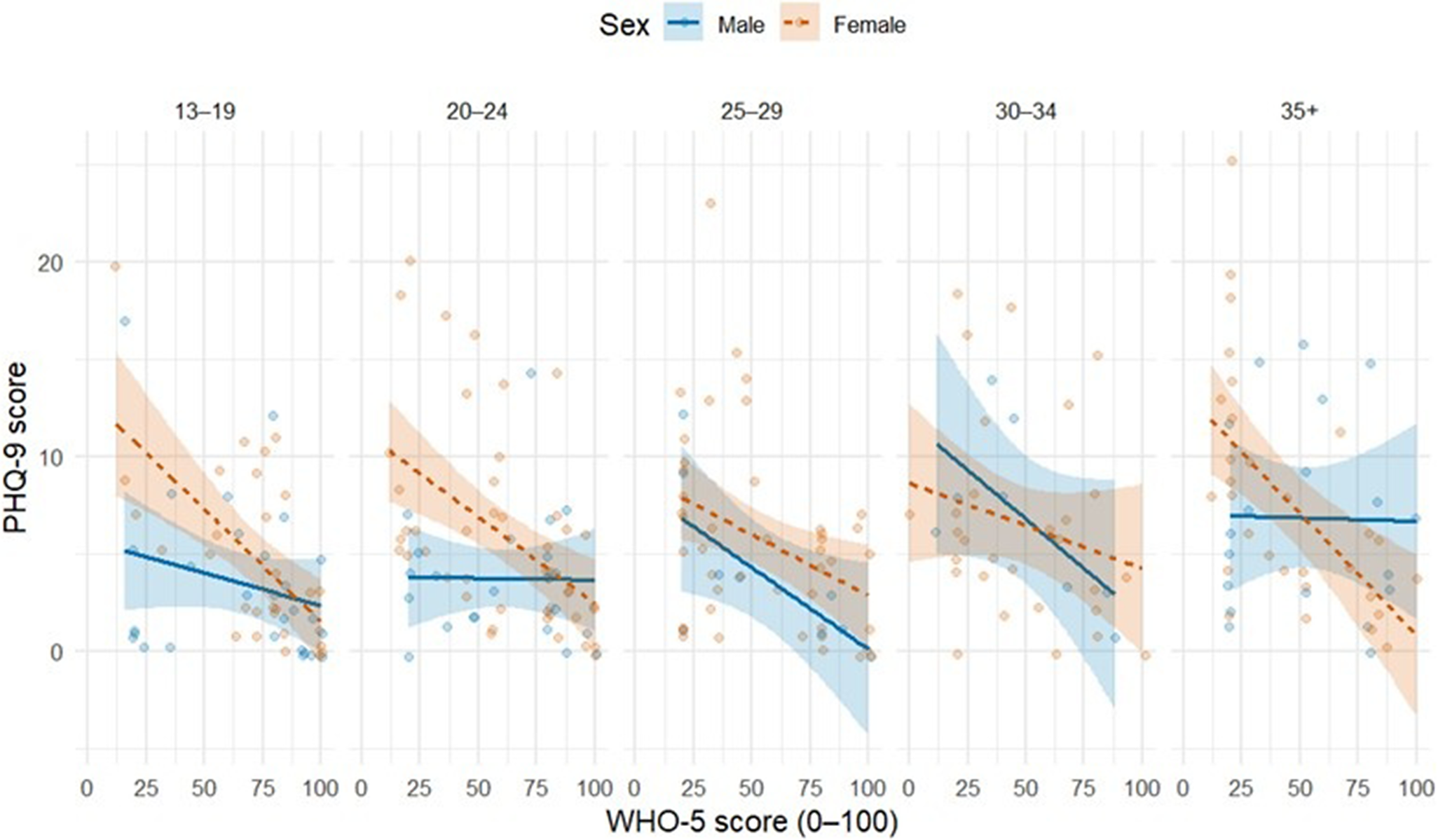
WHO-5 total scores were inversely associated with PHQ-9 total scores (Spearman’s rho = −0.474, p < 0.001). In the age- and sex-stratified plot, the fitted associations were negative for males and females in the 13–19, 20–24 and 25–29 age groups. In the 30–34 age group, the fitted association was strongly negative among males and negative among females. In the 35+ group, the fitted association remained negative among females, whereas it was comparatively flat among males, with wider confidence intervals (Figure 1).
PHQ-9 and WHO-5 score distributions stratified by age and sex (n = 264 IDPs).

Factorial validity
A one-factor CFA estimated using the weighted least-squares mean and variance-adjusted estimator supported a unidimensional structure for the WHO-5. The primary model without correlated residuals showed excellent fit, chi-square(5) = 8.013, p = 0.156, Comparative Fit Index = 0.999, Tucker–Lewis Index = 0.999, root mean square error of approximation = 0.048 with a 90% confidence interval from 0.000 to 0.11 and standardized root mean square residual = 0.021 (Supplementary Table S2).
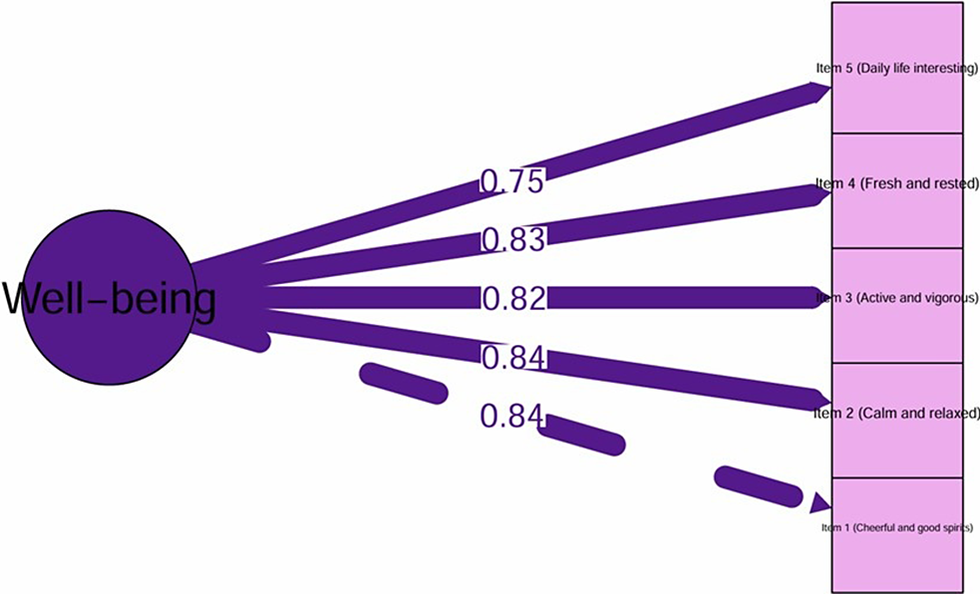
Standardized factor loadings were high across all items and ranged from 0.751 to 0.845. Item 1 (I have felt cheerful and in good spirits) was 0.845, Item 2 (I have felt calm and relaxed) was 0.843, Item 3 (I have felt active and vigorous) was 0.820, Item 4 (I woke up feeling fresh and rested) was 0.830 and Item 5 (My daily life has been filled with things that interest me) was 0.751. The standardized factor structure is shown in the CFA path diagram (Figure 2).
Path diagram of the Hausa version of the WHO-5 (n = 264).

Because the primary model already met conventional fit criteria, correlated residuals were evaluated only as a sensitivity analysis to assess potential localized dependence.
Residual correlation and sensitivity analysis
MI from the primary model suggested localized misfit primarily for the residual covariance between Item 3 (I have felt active and vigorous) and Item 4 (I woke up feeling fresh and rested), with MI = 6.508, expected parameter change = 0.099 and standardized expected parameter change = 0.311. The next largest suggested residual covariance was between Item 1 (I have felt cheerful and in good spirits) and Item 2 (I have felt calm and relaxed), with MI = 3.389, expected parameter change = 0.074 and standardized expected parameter change = 0.256. The residual covariance between Item 4 (I woke up feeling fresh and rested) and Item 5 (My daily life has been filled with things that interest me) was not supported, with MI = 0.065, expected parameter change = 0.011 and standardized expected parameter change = 0.030.
A sensitivity model allowing correlated residuals only for Item 1 (I have felt cheerful and in good spirits) with Item 2 (I have felt calm and relaxed), and Item 3 (I have felt active and vigorous) with Item 4 (I woke up feeling fresh and rested), also showed excellent fit, chi-square(3) = 1.123, p = 0.771, Comparative Fit Index = 1.000, Tucker–Lewis Index = 1.001, root mean aquare error of approximation = 0.000 with a 90% confidence interval from 0.000 to 0.069 and standardized root mean square residual = 0.009. Conclusions regarding unidimensionality were unchanged (Supplementary Table S2).
Screening performance of WHO-5 cutoffs
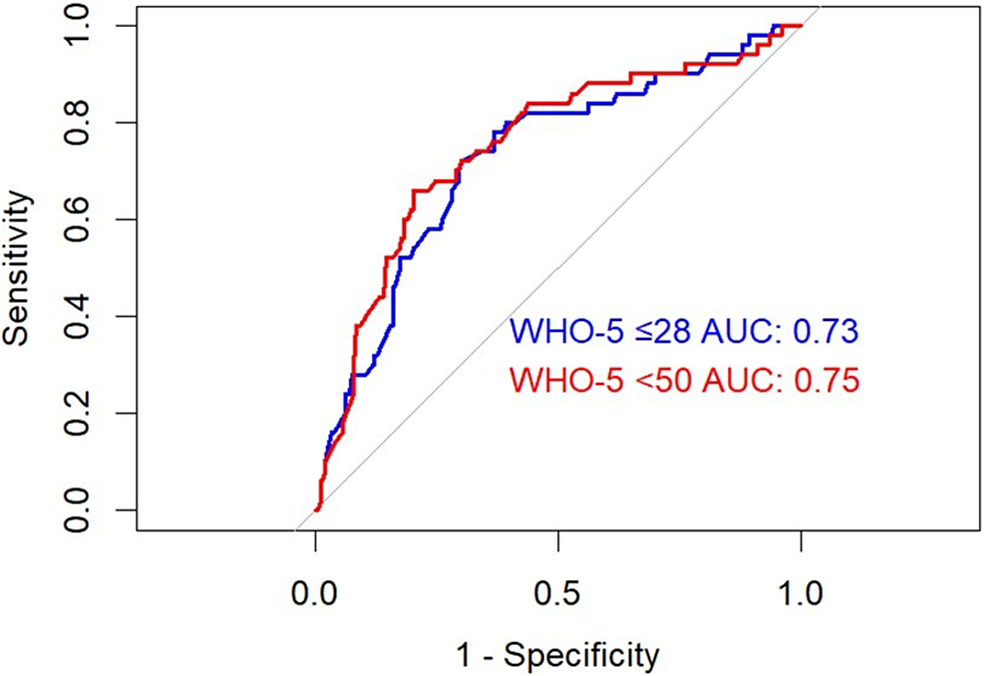
The performance of the WHO-5 for detecting depression, as defined by a PHQ-9 score ≥ 10, is presented in Table 2. The WHO-5 ≤ 28 cutoff yielded a specificity of 78.0% (95% CI: 72.5–83.5%), ensuring better identification of nondepressed individuals, but its sensitivity was 40.0% (95% CI: 40.0–53.6%), limiting its ability to detect all cases. The positive likelihood ratio (+LR) was 1.82 (95% CI: 1.19–2.78), and the negative likelihood ratio (−LR) was 0.77 (95% CI: 0.62–0.96), with a Youden’s index of 0.18, reflecting a moderate screening trade-off. In contrast, the WHO-5 ≤ 50 cutoff had a higher sensitivity (70.0%, 95% CI: 57.3–82.7%) but lower specificity (62.1%, 95% CI: 55.6–68.6%), meaning it captured more cases of depression but also produced more false positives. The +LR was 1.85 (95% CI: 1.44–2.37), and the −LR was 0.48 (95% CI: 0.31–0.75), with a Youden’s index of 0.32, suggesting a better overall balance between sensitivity and specificity. The ROC curve in Figure 3 illustrates these findings, with AUC values of 0.73 for WHO-5 ≤ 28 and 0.75 for WHO-5 < 50, respectively, confirming moderate discriminatory power.
Sensitivity, specificity, +LR, −LR, PPV, NPV, accuracy for two WHO-5 cutoff points and Youden’s index

Receiver operator characteristics (ROC) curve for the performance of the World Health Organization-Five Well-Being Index (WHO-5) at two cutoffs ≤ 28 and < 50.

Discussion
This study provides evidence that the Hausa version of the WHO-5 functions as a reliable, internally coherent measure of well-being among Hausa-speaking IDPs in Abuja, Nigeria.
Internal consistency was high (Cronbach’s α and McDonald’s ω, estimated from polychoric correlations), and corrected item-total correlations were consistently strong, indicating that all five items contributed meaningfully to the total score.
The one-factor structure was supported by an ordinal CFA, with excellent fit in the primary model, uncorrelated residuals and high standardized loadings across items. An inverse association between WHO-5 and PHQ-9 scores supported the construct validity of the WHO-5. We observed similar associations across all female age groups and most male age groups.
As a screening-tailored measure rather than a diagnostic instrument, the WHO-5 serves as a concise index of positive subjective well-being. In this sample, the mean WHO-5 score and its wide dispersion indicate substantial heterogeneity in well-being among camp residents. A higher proportion of participants scored ≤50, a commonly used threshold for low well-being in validation and screening contexts (Topp et al., Reference Topp, Østergaard, Søndergaard and Bech2015). In contrast, a smaller proportion of participants scored ≤28, a more stringent threshold used in some validation work (Lowe, Reference Lowe2004).
WHO-5 score distributions can overlap across depression severity levels, and sensitivity and specificity estimates for alternative cutoffs, such as ≤50 versus ≤28, can be imprecise, increasing the risk of misclassification (De Jesus Mari and Williams, Reference De Jesus Mari and Williams1986; Papassotiropoulos and Heun, Reference Papassotiropoulos and Heun1999). In low-resource humanitarian settings, cutoff selection should also consider downstream consequences of false positives, including distorted prevalence estimates and an unmanageable assessment and referral burden that can divert scarce clinical capacity (Kohrt et al., Reference Kohrt, Luitel, Acharya and Jordans2016; Negeri et al., Reference Negeri, Levis, Sun, He, Krishnan, Wu, Bhandari, Neupane, Brehaut, Benedetti and Thombs2021). Applying the WHO-5 ≤ 50 as the primary depression screening threshold is preferable because it prioritizes sensitivity and identifies mild-to-moderate symptom presentations that are typically appropriate for low-intensity, scalable interventions delivered through stepped care pathways (Van Straten et al., Reference Van Straten, Hill, Richards and Cuijpers2015; Patel, Reference Patel2017; Domenech et al., Reference Domenech, Kasujee, Koscielny and Griffiths2025). A more stringent threshold, such as WHO-5 ≤ 28, can then be reserved to flag probable moderate-to-severe depressive symptomatology for expedited clinical assessment or higher-intensity referral when resources are limited (Omani-Samani et al., Reference Omani-Samani, Maroufizadeh, Almasi-Hashiani, Sepidarkish and Amini2019; Domenech et al., Reference Domenech, Kasujee, Koscielny and Griffiths2025).
The WHO-5 has been translated into over 30 languages (The World Health Organization-Five Well-Being Index [WHO-5], 2024) and shown to be a psychometrically sound cross-cultural measure of subjective well-being for adults and adolescents (Sischka et al., Reference Sischka, Martin, Residori, Hammami, Page, Schnohr and Cosma2026). The WHO-5 has also been used across different disease areas (Domenech et al., Reference Domenech, Kasujee, Koscielny and Griffiths2025). Subjective well-being and potential mental health problems of Hausa-speaking displaced persons in Niger were measured using the English version of the WHO (Fiscone et al., Reference Fiscone, Vigliaroni, Rania and Veronese2024). Similarly, well-being and associated factors among adult Nigerians during the first wave of the COVID-19 pandemic were measured using the WHO-5 (Folayan et al., Reference Folayan, Ibigbami, Oloniniyi, Oginni and Aloba2021). Yet neither of those studies, nor any other published Nigerian studies to date (Eric et al., Reference Eric, Oghenebrorien, Onogimesike and Suoke2020; Seb-Akahomen et al., Reference Seb-Akahomen, Okogbenin, Obagaye, Erohubie and Aweh2021), used locally validated Hausa versions of the WHO-5 or were conducted in a displacement context, which may compromise cultural validity, delay early intervention and limit care, and represent a significant evidence gap (Heim et al., Reference Heim, Kohrt, Koschorke, Milenova and Thornicroft2020; Stowell et al., Reference Stowell, Ramalho, Manuela, Newcombe and McCool2025).
Furthermore, Nigeria is a very culturally and linguistically diverse country with ~232.7 million people (Obono, Reference Obono2003; Nigeria Development Update Building Momentum for Inclusive Growth, 2025). At least 50 million people speak Hausa in Nigeria and elsewhere (Lambu, Reference Lambu, Brunn and Kehrein2020). While there are no official estimates of the number of Hausa speakers in Abuja, Hausa is used for communication across ethnic groups and as a first language throughout the Federal Capital Territory and surrounding regions. To ensure accuracy, cultural relevance, effective depression screening and the facilitation of future validation studies among conflict-affected people, local validation of a Hausa version of the WHO-5 in a displacement context is crucial (Kaiser et al., Reference Kaiser, Ticao, Anoje, Minto, Boglosa and Kohrt2019).
These findings also address the broader need for locally validated mental health screening tools that are relevant to Hausa-speaking communities that have been displaced throughout the Sahel. Cultural and language ties in this region extend beyond national borders (Newman, Reference Newman and Bernard2018/2018). The WHO-5’s positive wording and emphasis on well-being, rather than just symptoms, align with local conceptions of health, which include social, spiritual and emotional balance (Labinjo et al., Reference Labinjo, Serrant, Ashmore and Turner2020; Ventriglio et al., Reference Ventriglio, Castaldelli-Maia, Caycho-Rodríguez and Torales2026). A culturally informed approach may help mitigate stigma and improve mental health disclosure (Clement et al., Reference Clement, Schauman, Graham, Maggioni, Evans-Lacko, Bezborodovs, Morgan, Rüsch, Brown and Thornicroft2015; Omani-Samani et al., Reference Omani-Samani, Maroufizadeh, Almasi-Hashiani, Sepidarkish and Amini2019; Ogueji et al., Reference Ogueji, Ojo and Gidado2020; Okafor et al., Reference Okafor, Oyewale, Ohazurike and Ogunyemi2022). This is essential for overcoming barriers to care in humanitarian and community health settings (Anyebe et al., Reference Anyebe, Olisah, Garba, Murtala and Danjuma2021; Jidong et al., Reference Jidong, Bailey, Sodi, Gibson, Sawadogo, Ikhile, Musoke, Madhombiro and Mbah2021). By showing that a translated version of a brief, nonstigmatizing tool can retain its psychometric properties and be accepted by people in two IDP camps, this study provides practical evidence for expanding mental health screening in low-resource and crisis-affected areas in West and Central Africa.
The observed inverse association between the WHO-5 and PHQ-9 is consistent with our hypothesis that higher well-being is associated with lower depressive symptom burden. Still, it should be interpreted as evidence of convergent or construct validity relative to a screening standard rather than a diagnostic benchmark (Ali et al., Reference Ali, Ryan and De Silva2016).
While the PHQ-9 depression measure is an accessible, cost-effective screening tool for a low-resource humanitarian setting, its scores are valid only if participants understand and respond to its questions in accordance with its original design (Panayiotou et al., Reference Panayiotou, Razum, Eisele, Wang, Fried and Cohen2025). Inconsistent interpretations of the PHQ-9 questions raise concerns about its validity as a severity measure (Panayiotou et al., Reference Panayiotou, Razum, Eisele, Wang, Fried and Cohen2025). Thus, future studies should approach our use of the PHQ-9 as a construct (convergent) validity measure with caution and consider less ambiguous alternatives.
A major concern in CFA is whether excellent fit is due to post hoc residual correlations rather than the underlying measurement structure (Pan et al., Reference Pan, Ip and Dubé2017). Here, the primary one-factor model already met conventional fit criteria without correlated residuals, and the sensitivity model that permitted only the two residual covariances supported by the modification indices did not change conclusions about unidimensionality. Our findings are consistent with a prevailing subjective well-being factor with limited local item dependence (LID) among content-overlapping item pairs, which occurs in brief instruments (Smith et al., Reference Smith, Combs, Pearson, Cooper, Camic, Long, Panter, Rindskopf and Sher2012; Gonzalez et al., Reference Gonzalez, Canning, Smyth and MacKinnon2020).
Limitations and future directions
The results are based on baseline cross-sectional data, which precludes the establishment of causal relationships between constructs. The sample was drawn from two longstanding IDP camps in Abuja, which may limit generalizability to newer or regionally distinct camps. Use of self-reported instruments to capture well-being and depression might have introduced stigma or social desirability-related response bias among our participants. Although the PHQ-9 was used as a validated comparator, it is not a definitive diagnostic standard for depression.
Because the WHO-5 may map onto depression differently by age, sex or both, future studies should examine these interactions more closely, assess additional psychometric properties such as measurement invariance across key demographic strata, and consider pairing screening tools with structured clinical assessment in a subsample to strengthen evidence for criterion validity.
Conclusions
We provide preliminary information on the psychometric properties of the Hausa version of the WHO-5. The WHO-5 showed strong reliability, validity, screening performance and demographic sensitivity, with older adults showing lower well-being and higher depressive symptom scores. Incorporating the WHO-5 Well-Being Index into mental health screening protocols can help with depression screening among IDPs in Abuja, Nigeria. We found low scores on the WHO-5 to be proxy markers of depressive symptoms. The ≤50 cutoff is a useful finding for early intervention, but not an indication of depression, which is a clinical diagnostic category. These findings reinforce the importance of community-based, culturally grounded screening approaches that nonspecialist health workers can deliver.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10205.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10205.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.
Acknowledgments
Andem Effiong Etim Duke’s work was supported by the Dr. Patrick Madore Traineeship through the Dalhousie Faculty of Medicine 2025 Graduate Studentship program. The authors sincerely thank Brooks Insights, Abuja, Nigeria, for their contributions to this study.
Author contribution
A.E.E.D. and E.E.: Study conceptualization and design. A.E.E.D. and E.E.: Data acquisition. A.E.E.D.: Data interpretation. A.E.E.D.: Data analysis and visualization. A.E.E.D. and E.E.: Raw data verification. A.E.E.D.: Drafting of the original and final drafts of the manuscript. A.E.E.D.: Methodology. R.O. and E.E.: Supervision. E.E.: Resources. A.E.E.D. and E.E.: Full access to the data in the study. All authors provided critical feedback on revising the manuscript for intellectual content. All authors were ultimately responsible for the decision to submit for publication.
Financial support
This work is supported by Creating Hope in Conflict: a Humanitarian Grand Challenge; a partnership of the United States Agency for International Development (USAID), the Foreign, Commonwealth & Development Office, United Kingdom of Great Britain and Northern Ireland (FCDO), the Stabilization and Humanitarian Aid Department, Ministry of Foreign Affairs, of the Netherlands (NL MFA) and His Majesty the King in Right of Canada (“His Majesty”) represented by the Minister for International Development of Global Affairs Canada acting through The Department of Foreign Affairs, Trade and Development of Global Affairs Canada (“DFATD”) with support from Grand Challenges Canada (grant number R-HGC-POC-2408 67,370); and the Government of Canada, Canadian Institutes of Health Research, Institute of Population and Public Health (grant number PAA-192178). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests
The authors declare no competing interests.
Ethics statement
The study was approved by Nigeria’s National Health Research Ethics Committee (NHREC/01/01/2007–2018/01/2024) and the Health Sciences Research Ethics Board at Dalhousie University (REB #2024–7085) and adhered to the principles of the Declaration of Helsinki. Informed consent was obtained from all participants.




 Open access
Open access