



Impact statement
This study improves our understanding of school mental health needs, policies and implementation challenges and opportunities in Indonesia with implications for mental health promotion in schools in other resource-poor countries. It also strengthens the evidence base for targeting teacher mental health and well-being. The study reveals how stigma impedes mental health literacy and student help-seeking behaviour, which, along with workforce constraints, reduces the reach of existing mental health programs in schools. These findings prompt targeted investment in school capacity building and accessible referral pathways for various types of schools in Indonesia, particularly under-resourced schools and madrasa. At a national level, this information may encourage governments to prioritise allocating resources to the school health unit (UKS) around mental health, standardise school guidance counsellor-to-student ratios and extend government-facilitated teacher training beyond public schools. The findings could also help prioritise pre-service and in-service mental health training for school guidance counsellors, teachers and school health teams, which could improve early identification, reduce reliance on undertrained peer counsellors and strengthen whole-school preventive actions. By leveraging mental health in schools through promotive and preventive actions, this research may contribute to improving adolescents’ mental health, which is known to be of educational value through enhanced student engagement, reduced absenteeism and improved learning outcomes. Further research is encouraged to build the evidence for how to enhance mental health promotion in schools, which has the potential to reduce the health inequalities experienced by young people in low- and middle-income countries.
Introduction
Since the COVID-19 pandemic, there has been increasing acknowledgement of the importance of mental health promotion in schools, including in Low- and Middle-Income Countries (LMICs). The government of Indonesia, the world’s fourth most populous country, has recognised this challenge and attempted to ensure that mental health is included within its school health policies, which support the health and well-being of 53 million 5- to 19-year-old students (Data Indonesia, 2023). Nevertheless, despite greater appreciation of the importance of schools for mental health in Indonesia and other LMICs, little is known about what school communities perceive as their role in addressing the risk factors for mental health that lie within a school’s purview. There is similarly little knowledge of the partnerships that schools are required to establish within their communities to respond to individual students in need of mental health assessment or treatment. There is also insufficient evidence about the extent to which mental health promotion is implemented in schools in LMICs, and what is needed to enhance this.
These questions are particularly salient for Indonesia, a middle-income country, as most health promotion studies in schools, especially those focusing on comprehensive school health or whole-school approaches to health promotion, have been conducted in high-income countries (Aston et al., Reference Aston, Raniti and Shinde2023). This exploratory study aimed to describe what school communities in Indonesia understand about student mental health problems, the role of schools in promoting mental health and the enablers and barriers experienced within schools around this.
Methods
This study used a qualitative approach and collected data from multiple stakeholders involved in school mental health promotion.
Education context
The study focused on adolescent mental health in Junior high schools (Years 7–9) in Surabaya, the second-largest municipality in Indonesia on the island of Java, which provides education to more than half a million students (Badan Pusat Statistik Kota Surabaya, 2023). In Indonesia, primary education comprises 9 years (Years 1–6 of Elementary school and Years 7–9 of Junior high school), followed by secondary education (Years 10–12). Nationally, formal educational processes are managed by the Ministry of Education, Culture, Research and Technology (MoECRT) and the Ministry of Religion (MoR), with most school health regulations made by the Ministry of Health (MoH). There are three types of regular schools: public, private and madrasa (Islamic religious schools). While primary education is authorised by the Department of Education (DoE) and the Department of Religion (DoR) at the municipality level, secondary education is managed under these departments at the provincial level.
Participants
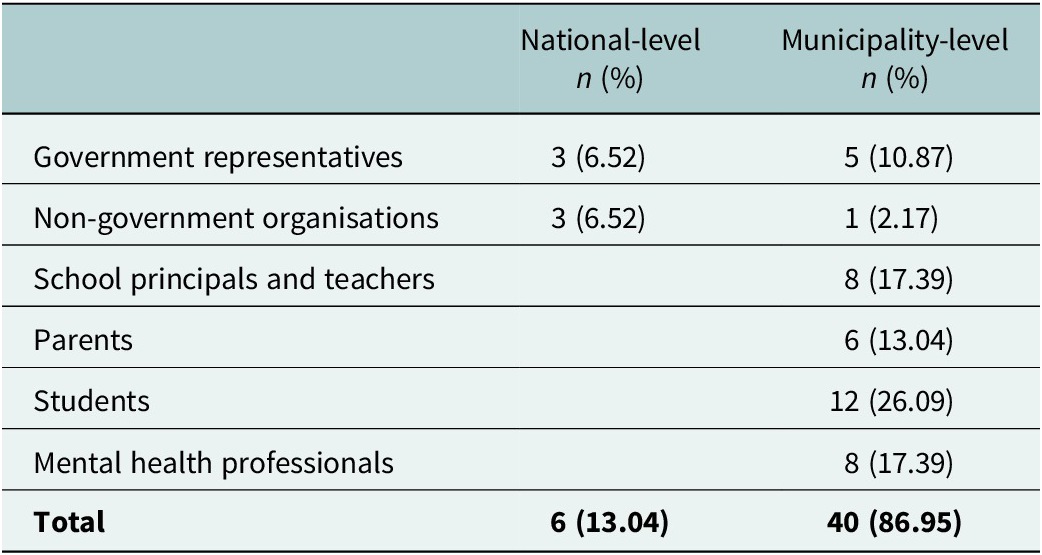
The inclusion criteria were adults with roles (employed or voluntary) in managing and implementing mental health promotion or adolescent-focused mental health programs and/or policy or as advocates within the education or health sectors in Indonesia. Parents and students (11–16 years old) were identified by the participating schools and invited to participate. Written informed consent was required for all participants; eligible students required parental consent. The sample consisted of 46 participants (12 adolescents, 34 adults) who ranged from national to municipality levels (see Table 1).
Participant characteristics (N = 46) by administrative level (national, municipality)

Note: Mental health professionals were represented by school counsellors, psychologists, psychiatrists and general practitioners in community health centres (Puskesmas) and hospitals. The 12 students consisted of 5 boys and 7 girls. Governments came from Education (MoECRT/DoE) and Health (MoH/DoH) agencies from the national to municipality levels. Nine schools participated: four public schools, four private schools, and one madrasa.
Selection and recruitment
Following ethics approval, we engaged with the relevant representatives of school communities, including government ministries and departments, school principals and non-government organisations (NGOs) at the national level and in Surabaya. The municipal authorities (DoE, DoR) selected potential schools following the request by the research team to include a mix of school types (public, private and madrasa), capacity (large to small) and resources (poorly resourced to well-resourced). We mapped NGOs involved in any aspect of mental health at the national and municipality levels. An invitation letter was emailed to each group, followed by a phone call or email 2 weeks later to ascertain their interest in the study. Participants were recruited between June and July 2022.
Data source and collection procedure
Focus Group Discussions (FGDs) were used to probe participants’ responses simultaneously as individuals and as part of a group (Boateng, Reference Boateng2012; van and Angehrn, Reference van Eeuwijk and Angehrn2017). Mental health is a sensitive and variably stigmatised health issue in Indonesia; mental health literacy cannot be assumed, and participants may be diffident about proffering their opinions (Jaya and Wulandari, Reference Jaya and Wulandari2018; Brooks et al., Reference Brooks, Syarif, Pedley, Irmansyah, Lovell, Opitasari, Ardisasmita, Tanjung, Renwick, Salim and Bee2022). Therefore, we began each FGD with a discussion of a vignette of a hypothetical adolescent who had experienced mental health problems, with the expectation that this would help promote engagement and discussion (Barter and Renold, Reference Barter and Renold2000; Jackson et al., Reference Jackson, Harrison, Swinburn and Lawrence2015). Two FGD guides (students, adults) were constructed, with the main differences being around the vignettes and the language used (see Supplementary materials for the FGD blueprint and protocol). FGDs were held in Bahasa Indonesia (each for 180 min using Zoom Meeting). Additional details were collected through one-on-one interviews with key informants. To neutralise susceptibility to bias, the researcher engaged in reflexivity, a set of continuous and multifaceted practices in which researchers self-consciously appraise and evaluate how their subjectivity and context influence the research processes (Ben-Ari and Enosh, Reference Ben-Ari and Enosh2011; Gentles et al., Reference Gentles, Jack, Nicholas and McKibbon2014; Olmos-Vega et al., Reference Olmos-Vega, Stalmeijer, Varpio and Kahlke2023). In addition, two summary meetings were held to validate key findings (one each for students and adults), where the researcher shared reflective notes and collected participant feedback and reflections.
Theoretical approach and data analysis
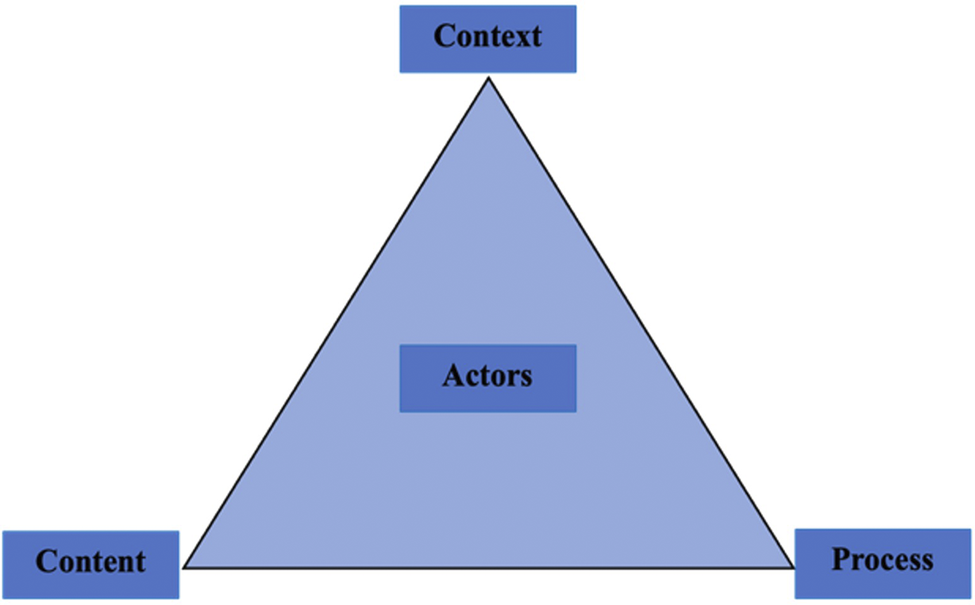
Recognising the complexity of mental health in schools, the Health Policy Triangle (Figure 1) was selected as the analytic framework through a detailed examination of policy content, context, processes and actors (Walt and Gilson, Reference Walt and Gilson1994). Recordings of FGDs and interviews were transcribed verbatim in Bahasa Indonesia. The data were analysed manually since the discussion used informal Bahasa Indonesia mixed with Javanese, the local language of some participants. Transcripts were thematically analysed using a deductive approach (Saldaña, Reference Saldaña and Seaman2013). First, transcripts were read and re-read to develop an initial coding frame, followed by individual coding of transcripts. These codes formed the final coding framework. Next, transcripts were coded line by line, and a data summary was entered into the framework. Then, the framework was reviewed to identify key themes, sub-themes and their relationships. Finally, quotes were selected to illustrate key themes (Supplementary Tables 2–4).
The Health Policy Triangle (adapted from Walt & Gilson, Reference Walt and Gilson1994). This framework was used to analyse how health policies are shaped, implemented and changed by context, content, process and actors (the four inter-connected elements form a triangle).

Results
Forty-six participants took part in five FGDs (Table 1). Three individual in-depth interviews also took place to enable elaboration on several government policies and their perceived implementation from representatives of the MoH, DoE and Community Health Centres (Pusat Kesehatan Masyarakat; Puskesmas). By the last FGD for school communities, no new themes emerged. As there was only one FGD for students, we are unable to comment on saturation. Three themes were identified: adolescent mental health problems and their impacts, limited implementation of mental health promotion in schools, and enablers and barriers (see Figures 2– 4 for selected quotes).
-
1. Understanding adolescents’ mental health problems and their impacts
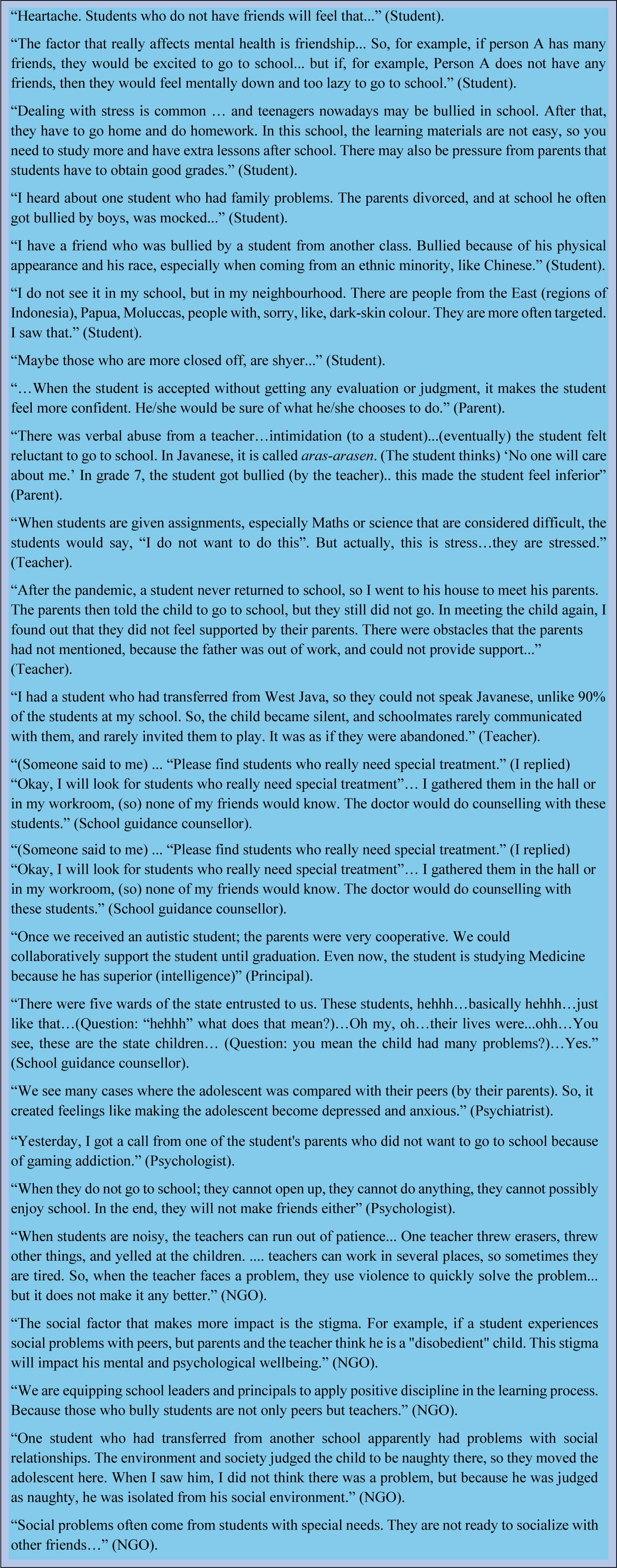
Selected quotes to illustrate understanding of the social context of mental health from students, parents, school staff and non-government organisation employees.

Most students reported that socialisation problems (i.e. difficulties in engaging in certain social situations) greatly impacted their mental health, well-being and academic experiences (Figure 2). Students shared the awareness that people their age were dealing with mental health problems that reflected relationship problems with peers, poor relationships with teachers, high academic demands from parents and problems at home. Problems at home were a significant mental health challenge, described as conflict with parents and siblings, interpersonal violence, family breakdown, and physical and emotional neglect. Within schools, bullying was reported to occur frequently, which was particularly acknowledged by students to affect those from ethnic minority backgrounds or low socioeconomic status. Bullying not only took place between students but was also reported to be perpetrated by teachers.
Teachers observed that some students’ mental health needs occurred within the context of developmental challenges such as neurodiversity (e.g. autism) or other special needs (e.g. learning difficulties, giftedness). Nevertheless, while participants were able to name various student mental health problems, several school professionals appeared to have limited vocabulary to discuss these concerns. Some teachers used euphemistic language such as ‘special treatment’ to suggest mental health interventions. Even some school guidance counsellors found it difficult to find the words to explain the behavioural problems they observed in their students, suggesting poor health and mental health literacy among school professionals.
Parents, teachers, health professionals and principals reported that the accumulation of worries and loneliness over time created significant psychological problems, with the acknowledgement that students with more social problems had lower self-esteem and could struggle to adjust to the academic and social demands of school. Mental health was also recognised as impacting learning. For example, some students missed school when they were unable to manage their problems and did not receive the needed support. Added to these complications was the problem of stigma around mental health problems, which was a challenge for teachers, parents and students. Stigma was identified as contributing to the reluctance of some students to ask for help. Poor student help-seeking behaviour was also reported to make it difficult for teachers and school guidance counsellors to identify students with problems and provide them with support. While mental health issues were typically viewed as problematic, some parents reported the value of emotional learning, self-actualisation and personal growth that could accompany the resolution of these issues.
-
2. Limited implementation of mental health promotion in schools
School and community-based participants were generally mindful of the various ways that schools can promote mental health and well-being (Figure 3). Most schools reported using a variety of approaches, from promotive (e.g. socio-emotional education, health seminars for students), preventive (e.g. screening to identify students at risk of mental health or academic problems, access to peer counsellors) and curative (e.g. individual counselling, referral to health services, access to a local NGO Hotline to manage violence-related or other clinical problems). Notwithstanding this scope, predominantly reported activities were in response to individual students who were identified with mental health problems (e.g. referral to Community Health Centres). Indeed, we found that a clinical orientation (a focus on pathology rather than well-being) was the focus of five out of the eight school mental health programs reported by participants (see Supplementary Figure 1). Nevertheless, consistent with stigma compounding low mental health literacy and poor help-seeking behaviour, students had not optimally accessed these services.
Scope of school mental health promotion actions.

The most commonly reported routine school mental health activity was assessment. Schools reported that routine screening to identify students with problems was an approach that drove referrals and led to case management. Two types of referrals were reported: internal referrals (case management within a school) and external referrals (working collaboratively with community-based agencies to provide support). Establishing networks with the community was appreciated as a mechanism that enabled a more comprehensive set of actions, such as teacher training and student health promotion activities. Through these collaborations, schools reported that they were able to equip teachers with health-promotion skills and a greater ability to solve problems.
-
3. Barriers and enablers to school mental health promotion
The School Health Unit (UKS) appeared to be Indonesia’s best-implemented school health policy. Mandated nationally, UKS aims to promote students’ comprehensive health and integrates mental health promotion strategies into various roles (i.e. delivering mental health-related psychoeducation, mental health risk screening and counselling services). As the UKS policy sits under the community health system, Community Health Centres can be accessed by students who receive support from UKS. Community Health Centre staff are expected to reach out to schools to deliver mental health promotion and obtain data from schools on student mental health and well-being. However, Community Health Centre staff reported a lack of personnel to work with schools; consequently, health assessments were not always optimally managed or used to inform the wider mental health programs at schools. Several schools reported unfamiliarity with the role of Community Health Centres in assisting schools to promote mental health (see Figure 4).
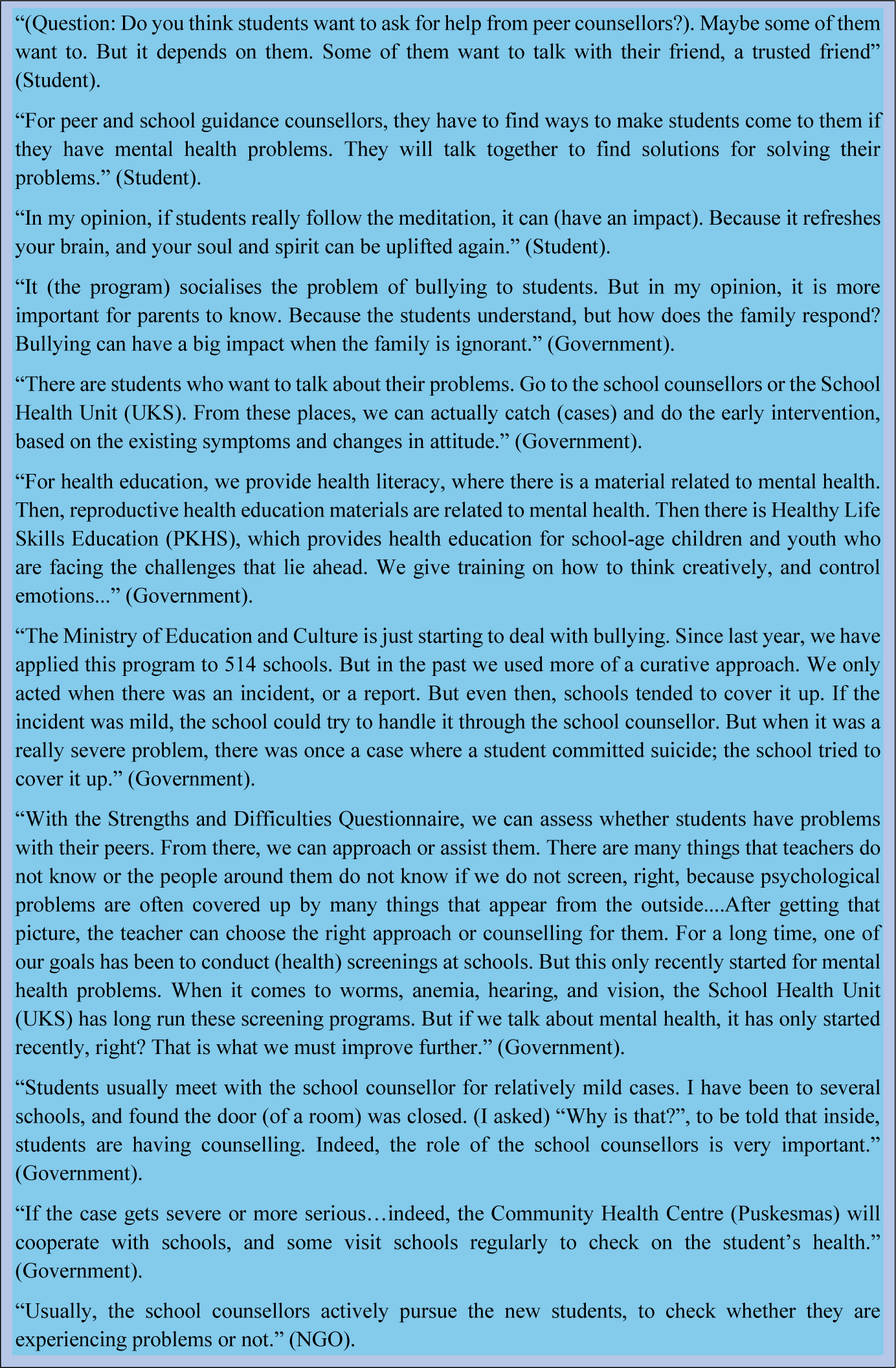
Examples of barriers and enablers to school mental health promotion reported by students, government representatives and non-governmental organisations.

The Peer Counsellor Program (Konselor Sebaya; KS), facilitated by the DoE Surabaya, was positively received by teachers and students. However, in the context of heavy workloads, most school guidance counsellors reported that they overly relied on peer counsellors to provide mental health support to students. This situation was acknowledged to create risks for student counsellors, some of whom were denigrated for participating in these roles and who carried responsibilities beyond their very limited training.
Some contextual barriers were also reported. As noted earlier, mental health stigma appeared to hinder students from seeking help, which appeared to reflect poor mental health literacy within school communities. Schools lacked understanding of how best to respond to students with different health and behavioural concerns, and there was a notable absence of consistent, responsive pathways to mental health care when issues were identified. The lack of personnel responsible for responding to student mental health concerns was apparent, as most schools reported that their student–school guidance counsellor ratio was below the national standard (ideally 150:1) (Ministerial Regulation No.111 Guidance and Counselling in Primary and Middle Schools, 2014). Despite these barriers, several participants appreciated the work of some school guidance counsellors who persisted in proactively identifying students in need. Students also seemed to appreciate this gesture as it created a more supportive environment that encouraged them to seek help.
Teacher well-being was rarely addressed as part of mental health promotion in schools. In Surabaya, teachers dealing with personal mental health problems were expected to access support under the DoE’s management-oriented procedure, which primarily supports teachers to take leave or access community mental health services. This may contribute to teachers avoiding seeking mental health support, especially when stigma is already high.
There was a noticeable difference in preparedness between school types. Through reflective questioning in the summary session, teachers from private schools and madrasas acknowledged receiving little government support. Teacher training and mental health literacy programs, facilitated by the government, were primarily accessed by public schools. The scarcity of teacher training for private schools and madrasas left some teachers feeling left behind. Working in silos appeared to significantly limit awareness of different government policies and community resources, resulting in the undermining of schools’ capabilities to implement various mental health policies. Ineffective communication, due to relatively rigid hierarchical authority structures, appeared to exacerbate poor coordination within ministries and between ministerial bodies, as well as between schools and supporting agencies, and even among elements within a school community.
At all levels, participants generally acknowledged that significant improvements are needed to better promote mental health and well-being in schools. They suggested that schools could be more capable implementers were they better enabled by support and resources from government and external parties and able to deal with wider barriers from both within and beyond the school.
Discussion
This exploratory study mapped the perceived landscape of school mental health promotion for adolescents by school communities in Surabaya, Indonesia. Despite challenges as a middle-income country, we found that school communities had a common understanding of the challenges around student mental health, the significance of stigma and poor mental health literacy, and their impacts on academic and developmental achievements. Notwithstanding government policies that support the full scope of mental health promotion in schools, ranging from preventive efforts to health promotion and responsive actions, there was a limited focus beyond responsive actions. Furthermore, while the predominant focus was on identifying and responding to students’ mental health problems, there was little evidence of consistent approaches to this and no evidence that it occurred well. Consequently, although students have begun to acquire mental health awareness, pathways to mental health services were limited. There was a notable difference in the capabilities reported between different types of schools, which, at least to some extent, reflected different lines of accountability and disparities in resources. The diverse capabilities of schools in Surabaya demonstrate the importance of understanding contextual enablers and barriers, as well as the need to navigate local strategies to leverage implementation (Kaku et al., Reference Kaku, Sibeoni, Basheer, Chang, Dahanayake, Irarrazaval, Lachman, Mapayi, Mejia, Orri, Jui-Goh, Uddin and Vallance2022).
A common challenge was that school communities and their related health services were struggling with stigma and poor mental health literacy, which limited appropriate help-seeking from students. This was compounded by few adolescent-responsive health services, whether within schools or in the community. Similar observations have been made in other LMICs (Nishio et al., Reference Nishio, Kakimoto, Bermardo and Kobayashi2020; Jorns-Presentati et al., Reference Jorns-Presentati, Napp, Dessauvagie, Stein, Jonker, Breet, Charles, Swart, Lahti, Suliman, Jansen, Van Den Heuvel, Seedat and Groen2021; Hamoda et al., Reference Hamoda, Hoover, Bostic, Rahman and Saaed2022), where the inadequate inclusion of mental health within school health services reflects insufficient resources (Turan et al., Reference Turan, Vinikoor, Su, Rangel-Gomez, Sweetland, Verhey, Chibanda, Paulino-Ramírez, Best, Masquillier, van Olmen, Gaist and Kohrt2023; Kearney, Reference Kearney2024). In this study, participants attributed this challenge to poor capabilities in dealing with mental health problems rather than an absence of policy or programs. As in other studies, stigma against people with mental disorders among teachers and parents was also found to impede the provision of care for students. Efforts to counteract stigma have been shown to benefit from mental health literacy training for school staff (Jegannathan et al., Reference Jegannathan, Dahlblom and Kullgren2014) as well as efforts to improve help-seeking behaviours of students (Lee et al., Reference Lee, Goh and Yeo2023; McPhail et al., Reference McPhail, Thornicroft and Gronholm2024). Efforts to reduce stigma, prejudice and discrimination against people with mental disorders could also create a ripple effect in improving mental health support for teachers, which is still much needed in LMICs (Pau et al., Reference Pau, Ahmad, Tang, Jusoh, Bin and Tat2022; Ratanasiripong et al., Reference Ratanasiripong, Ratanasiripong, Nungdanjark, Thongthammarat and Toyama2022).
Currently in Surabaya, school guidance counsellor roles focus more on career planning and student personal development than on mental health and well-being (Ministry of Education Culture Research and Technology Republic of Indonesia, 2022). While this role is intended for graduates with a bachelors’ degree in guidance counselling (Ministerial Regulation No.111 Guidance and Counselling in Primary and Middle Schools, 2014), in reality, these positions are often filled by teachers without mental health or guidance training, which contributes to persisting poor mental health literacy and stigma against mental health issues. This finding suggests that investment is needed to ensure that school guidance counsellors in Indonesia, along with the whole school health team, receive appropriate mental health training and supervision from pre-service education through to post-service training, a challenge that is also apparent in high-income countries (Bandilovska et al., Reference Bandilovska, Aston, Sawyer and Raniti2025). Such support should be readily accessible for all, including under-resourced schools and madrasas.
These findings suggest that mental health training for school health teams is needed to enhance their ability to influence their school’s social and academic environments. This will require teams to understand the scope of mental health promotion, which ranges from activities focused on promotion, prevention and treatment, as well as how to collaborate with external clinical and community partners in resource-poor settings. Equipping non-clinical school staff with the basic skills to respond to students’ emotional and mental health needs is considered best-practice in dealing with personnel shortages and improving accessibility to mental health care, as is the importance of schools knowing how to refer students to community-based providers (Galagali and Brooks, Reference Galagali and Brooks2020; World Health Organization, 2020).
Most participants, including students, recognised that many of the mental health problems affecting students are rooted in socialisation issues that reflect family and peer environments. Socialisation problems impacting mental health are found in adolescents in other LMICs but are not yet well-acknowledged let alone addressed in Indonesia (Aboagye et al., Reference Aboagye, Seidu, Hagan, Frimpong, Budu, Adu, Ayilu and Ahinkorah2021; Renwick et al., Reference Renwick, Pedley, Johnson, Bell, Lovell, Bee and Brooks2022). Beyond the importance of providing clinical responses to students who are struggling with mental health problems, a range of relatively straightforward mental health promotion approaches could be implemented in schools. These include addressing adolescent relationship problems through school-led efforts to reduce bullying from peers and teachers, enhancing connectedness to school through fairer disciplinary responses from teachers, and greater collaboration with parents and families, which exemplify the opportunities of universal approaches to mental health promotion in schools.
We found that teacher mental health and well-being was rarely addressed within school mental health promotion, notwithstanding that global frameworks such as Health-promoting Schools explicitly include teacher health and well-being (World Health Organization and UNESCO, 2021). Unfortunately, this finding is consistent with reports from both LMICs and HICs (Viac and Fraser, Reference Viac and Fraser2020; Pau et al., Reference Pau, Ahmad, Tang, Jusoh, Bin and Tat2022; Ratanasiripong et al., Reference Ratanasiripong, Ratanasiripong, Nungdanjark, Thongthammarat and Toyama2022). Just like for students, poor mental health literacy and high stigma will constrain teachers’ personal help-seeking. A recent survey in Australia found that many pre-service teachers felt hampered in meeting their personal well-being needs at work due to weak support from colleagues, mentors or supervisors when experiencing distress (Bandilovska et al., Reference Bandilovska, Aston, Sawyer and Raniti2025). These findings suggest that policy frameworks are needed in Indonesia to include teacher well-being, with sufficient resourcing to support appropriate practices (e.g. access to confidential mental health counselling when required).
This study found that, beyond its value as an explanatory framework, the four Health Policy Triangle elements interacted with each other to impact the implementation of school mental health promotion initiatives. First is the context, or the understanding of students’ mental health problems, and how this is used to shape school mental health promotion programs and their scope of action. For example, after acknowledging the increase in bullying and problem behaviours among students, schools have been developing their capabilities through clinical approaches, such as screening for problems and counselling. Second is the content of a mental health program, as this defines the scope of actions and who is involved. We found that clinically oriented interventions were mainstreamed within school mental health strategies, which require collaboration from schools with clinicians in the community, such as counsellors, psychologists and Community Health Centre staff. Third is the actors, who appeared to have a critical impact on generating implementation changes in the content, process and context. This suggests that equipping the range of actors with knowledge, skills and mental health literacy should be prioritised. Certainly, our Health Policy Triangle analysis found that schools were not fully implementing the comprehensive framework guided by global policies (Margaretha et al., Reference Margaretha, Azzopardi, Fisher and Sawyer2023). The gap appears primarily at the level of implementation by schools, as Indonesian policies align with global policies that promote comprehensive school health through universal and whole-school actions.
This study has several strengths. First, while exploratory in nature, it provides a breadth of insights about what is currently being implemented to promote mental health in schools in Surabaya, Indonesia. This is important for other LMICs, as various school mental health frameworks developed by United Nations agencies lack evidence regarding their implementation in LMICs (Ribeiro et al., Reference Ribeiro, Grande, Hoffmann, Ziebold, McDaid, Fry, Peixoto, Miranda, King, Tomasi, Faustino, Leone, Moraes, Schäfer, Alves, Rosa and Evans-Lacko2023). We found that involvement of various actors enables the implementation of school health programs that originate from global policies and national mandates (a top-down approach) as well as initiatives from local governments and schools themselves (a bottom-up approach). Second, this study enriches the evidence on the opportunities for linking school mental health services with primary healthcare for students with mental disorders in LMICs, highlighting the importance of future investment in strengthening primary healthcare and building the capacities of community healthcare providers to work with school mental health teams. Third, this research aligns with calls to better capture the voices of actors related to school mental health, particularly those of adolescents themselves. In the future, we hope the range of roles and responsibilities mapped in this study can be used to develop strategies for involving all stakeholders within school mental health promotion. Finally, as a conceptual contribution, this research confirms that mental health and well-being are perceived as important building blocks of student learning in Indonesia. This study also shows that, in promoting student mental health, there is a significant challenge posed by the gap between policies and implementation due to the fact that schools and teachers are not equipped to promote mental health through a comprehensive scope of actions (promotive, preventive and treatment). To move forward, this study recommends shifting the mindset and ethos from a primarily clinical or problem-focussed orientation to a more promotive approach, which will require investment in teacher training and mental health literacy for all school communities.
There are also some limitations. We were unable to approach schools directly but were reliant on the MoE to do this on our behalf which may have contributed to selection bias. At the time of school selection by the MoE, the research team emphasised the importance of ensuring a variety of schools were selected including more poorly resources schools. While, a variety of views was obtained, this small exploratory study cannot be considered representative of school types in Indonesia, notwithstanding our efforts to include a range of participants from different types of schools and different groups of NGOs. The consistency of views across this relatively wide group of participants provides some confidence in these findings, which were recently reinforced by findings from a larger quantitative study (Margaretha et al., Reference Margaretha, Azzopardi, Fisher and Sawyer2026). Moreover, the study design was not intended to explain the extent or quality of implementation at the school level nor to examine causal relationships between key findings. Transferring evidence from this study to another context should be done cautiously. These FGDs took place immediately following the transition back to school after the COVID pandemic. It is anticipated that the impact of the pandemic on teacher and student mental health may have raised awareness of the importance of mental health promotion in schools (Nuryana et al., Reference Nuryana, Xu and Lu2022; Julianto et al., Reference Julianto, Sumintono, Wilhelmina, Almakhi and Avetazain2023; Juliansen et al., Reference Juliansen, Heriyanto, Muljono, Budiputri, Sagala and Octavius2024), but this was not explicitly explored in the FGDs. The only issue raised in the FGDs related to some teachers questioning the extent to which the School Health Unit was fully functioning after the return to face-to-face schooling.
Conclusion
This study provides evidence that confirms the importance of addressing young people’s mental health in schools in Indonesia. As in other LMICs, schools in Indonesia are expected to contribute to filling the large mental health care gap by implementing multiple mental health programs. Filling this gap in need is challenging, both in providing clinical responses to students in need of mental health care and in offering comprehensive approaches to mental health promotion in schools. The Health Policy Triangle framework applied in this study provides evidence for a range of elements that can be leveraged to promote mental health in schools. There is a central role for a variety of groups and people that are required to conceptualise and operationalise the school as a whole community for promoting mental health, including as recipients. This study also reinforces that while schools need to develop better pathways to care for students with varying mental health problems of different levels of severity, particular attention is needed to support schools to better address primary prevention and health promotion.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10210.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10210.
Data availability statement
Data available within the article or its supplementary materials.
Acknowledgements
The authors wish to thank Dr. Ikhsan, Ir. Yusuf Masruh, Andini Damayanti and the research participants for their support in data collection in Surabaya.
Author contribution
MM led this research as part of her doctoral thesis at The University of Melbourne. SS, PA and JF supervised MM’s doctoral thesis. MM led the drafting of the manuscript. SS, PA and JF contributed to drafts of the paper and approved the submitted version.
Financial support
MM was funded by the Australia Awards Scholarships from the Government of Australia. The funder of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Competing interests
SS contributed to the development of the WHO and UNESCO Global Standards and Systems for Health-Promoting Schools. SS was a member of the WHO Technical Advisory Committee for School Health Services. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethics
Ethics approvals were granted by the Health Research Ethics Committee, Faculty of Medicine, Universitas Airlangga, Indonesia (No. 256/EC/KEPK/FKUA/2021); the Committee of Research and Development of Surabaya, Indonesia (No. 070/1901/S/RPM/436.7.15); and the Office of Research Ethics and Integrity – Human Ethics, University of Melbourne, Australia (Ref No. 2022-2121632-28168-4).
Informed consent
Written informed consent was obtained from the participants of this study.



 Open access
Open access
Comments
Dear Editors,
I am pleased to submit an original research article for consideration for publication in the Cambridge Prisms: Global Mental Health.
Attention to young people’s mental health has greatly increased since the COVID pandemic, with recognition that schools are an important setting for promotion of mental health and wellbeing. In this qualitative analysis, we explored what school communities in Surabaya, Indonesia understand about student mental health challenges, the role of schools in promoting mental health, and the enablers and barriers to mental health promotion in schools. As there is very little evidence about the extent that mental health promotion is implemented in schools in LMICs, we believe that our findings will be of wide relevance.
Our three key findings were, first, that socialisation and relational difficulties at home and school were perceived to contribute to students’ poor mental health, and had an adverse impact on their engagement with learning. Second, while schools reported familiarity with a scope of activities ranging from promotion, preventive interventions and responsive mental health services, the predominantly reported activities were in response to individual students identified with mental health problems. Third, we identified many contextual barriers and enablers that if addressed, could enhance mental health-promoting actions by schools.
The broader policy relevance of this research is the global interest from UN agencies (e.g. WHO and UNESCO) in making every school a health promoting school. This paper is also consistent with calls for greater collaboration between the health and education sectors made by the newly published Lancet Commission on Adolescent Health and Wellbeing. We believe that our findings highlight important opportunities to assist policymakers and practitioners to prioritise the promotion of mental health in adolescents in Indonesia, the Asia Pacific region, and indeed in other LMICs.
We confirm that this work is original and has not been published elsewhere, nor is it currently under consideration for publication elsewhere.
Thank you for your consideration of this manuscript.
Yours sincerely,
Margaretha, on behalf of the authors
Centre of Adolescent Health, Royal Children’s Hospital Melbourne; Department of Pediatrics, the University of Melbourne; Murdoch Children’s Research Institute, Parkville VIC 3010.