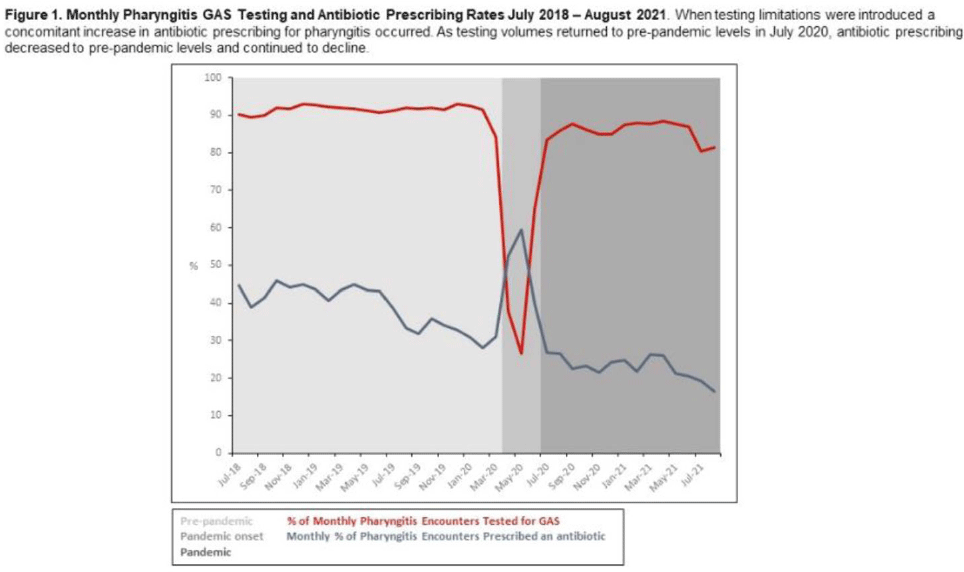
Background: Pharyngitis is 1 of the most common conditions leading to inappropriate antibiotic prescriptions. When personal protective equipment (PPE) was at first constrained during the COVID-19 pandemic, Intermountain Healthcare recommended limiting rapid group A streptococcal pharyngitis (GAS) testing in urgent-care clinics to preserve PPE. Notably, the percentage of pharyngitis encounters prescribed an antibiotic and that underwent GAS testing is a key Healthcare Effectiveness Data and Information Set (HEDIS) measure. We have described our experience with urgent-care pharyngitis encounters and the impact of temporarily reducing GAS testing on antibiotic prescribing before and during the COVID19 pandemic. Method: We identified all urgent care encounters between July 2018 and August 2021 associated with a primary diagnosis of pharyngitis using ICD-10 CM codes and a validated methodology. Pharyngitis encounters were assessed for antibiotic prescriptions ordered through the electronic health record (EHR) and the use of point-of-care rapid GAS tests. Pharyngitis encounters were analyzed monthly. We assessed the percentage of encounters associated with an antibiotic prescription regardless of testing and the percentage of encounters associated with an antibiotic prescription when a GAS test was or was not performed. We examined 3 periods relating to COVID-19 and GAS testing recommendations: the prepandemic period (July 2018–March 2020), the pandemic onset period (April 2020–June 2020), and the pandemic period (July 2020–August 2021). Results: Prior to the pandemic, the monthly percentage of pharyngitis encounters for which rapid GAS testing was performed was nearly 90% (Fig. 1). The average monthly percentage of urgent-care pharyngitis encounters prescribed an antibiotic was 38.9%, and the average percentage of monthly pharyngitis encounters prescribed an antibiotic that also underwent GAS testing was 90.4%. This HEDIS measure declined from 90.4% during the prepandemic period to 29.8% in the pandemic onset period when GAS testing was limited. Following resumption of routine testing practices the monthly percentage of urgent-care pharyngitis encounters for which rapid GAS testing was performed returned to levels ≥80% by July 2020 (Fig. 1). The average percentage of monthly pharyngitis encounters prescribed an antibiotic that also underwent GAS testing rose to 87.3% during this period. Conclusions: Limited PPE in our urgent care centers during the initial months of the COVID-19 pandemic was associated with a mandated substantial decline in rapid GAS testing. As testing volume decreased, we noted a simultaneous relative increase of >30% in antibiotic prescribing for pharyngitis. These findings suggest that rapid streptococcal testing promotes appropriate antibiotic prescribing.
Funding: None
Disclosures: None
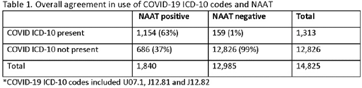
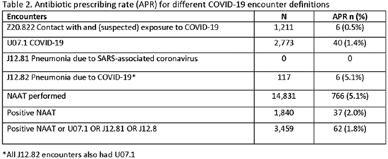
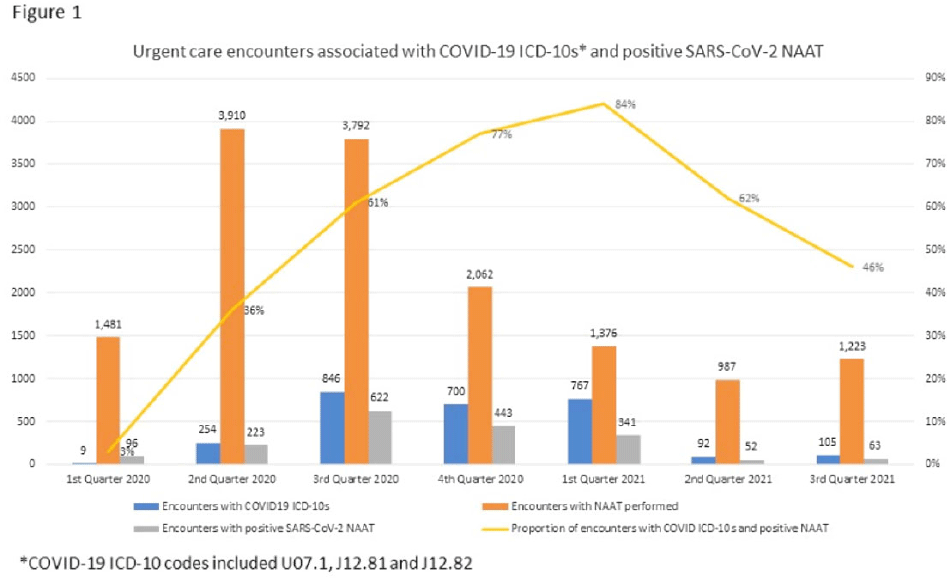
Background: Billing data have been used in the outpatient setting to identify targets for antimicrobial stewardship. However, COVID-19 ICD-10 codes are new, and the validity of using COVID-19 ICD-10 codes to accurately identify COVID-19 encounters is unknown. We investigated COVID-19 ICD-10 utilization in our urgent care clinics during the pandemic and the impact of using different COVID-19 encounter definitions on antibiotic prescribing rates (APRs). Methods: We included all telemedicine and office visits at 2 academic urgent-care clinics from January 2020 to September 2021. We extracted ICD-10 encounter codes and testing data from the electronic medical record. We compared encounters for which COVID-19 ICD-10 codes were present with encounters for which SARS-CoV-2 nucleic acid amplification testing (NAAT) was performed within 5 days of and up to 2 days after the encounter (Fig. 1). We calculated the sensitivity of the use of COVID-19 ICD-10 codes against a positive NAAT. We calculated the APR as the proportion of encounters in which an antibacterial drug was prescribed. This quality improvement project was deemed non–human-subjects research by the Stanford Panel on Human Subjects in Medical Research.
Funding: None
Disclosures: None
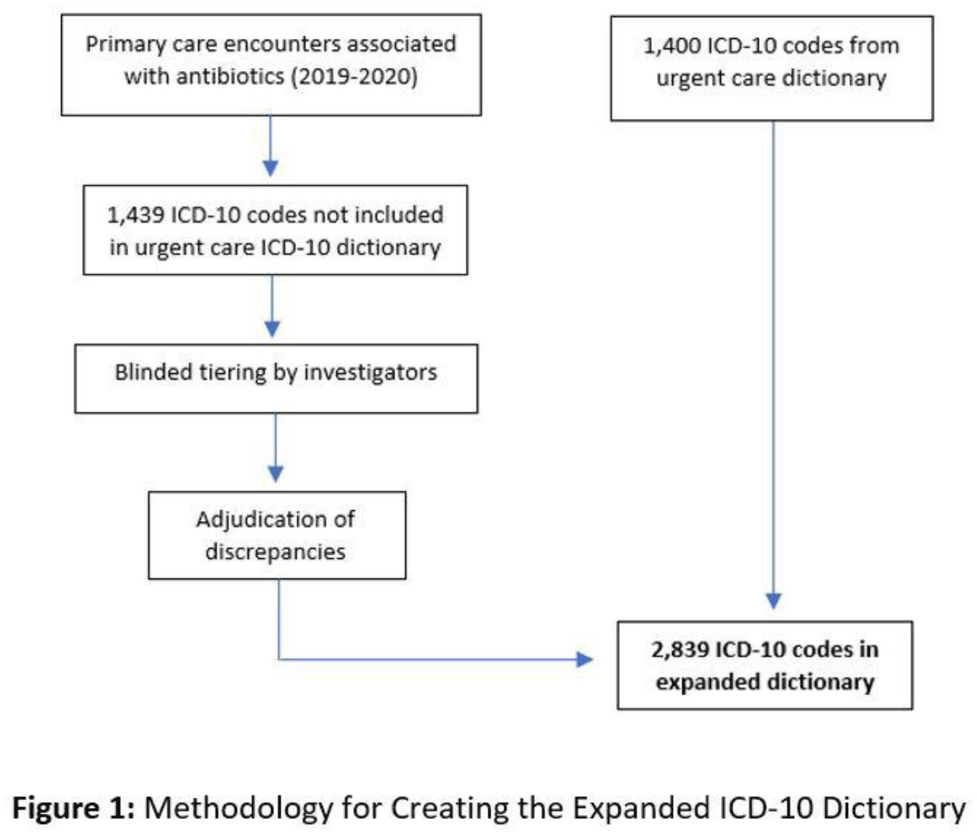
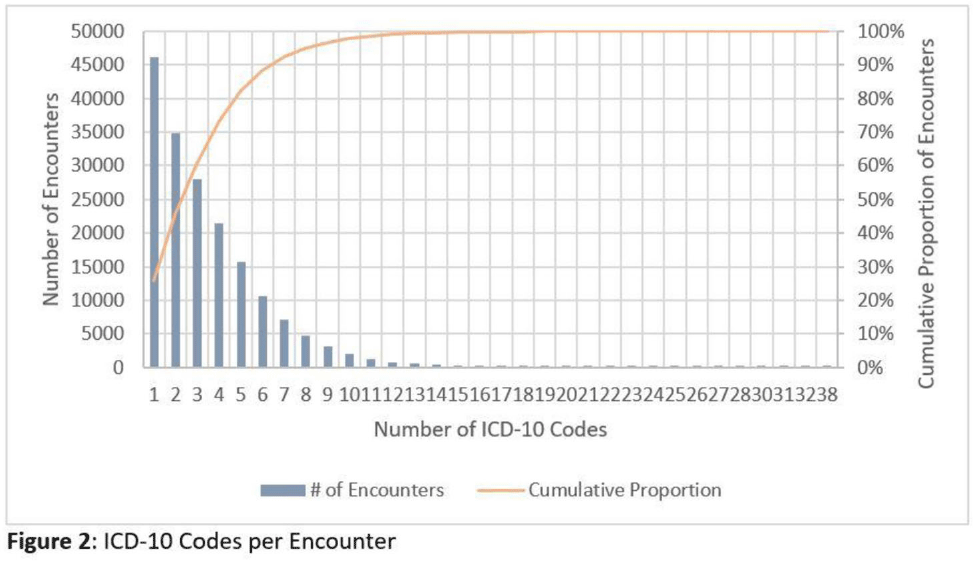
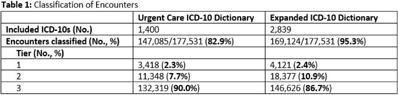
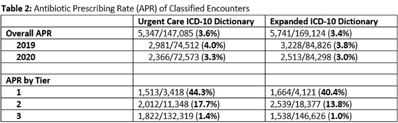
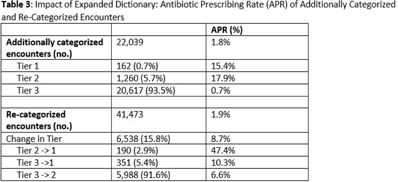
Background: Emerging evidence supports the use of billing data to identify stewardship targets in primary care. Standardizing an approach to antibiotic prescribing rate (APR) calculations could facilitate external benchmarking. Methods: Using methodology and an ICD-10 dictionary validated in urgent care clinics,1 we created an expanded ICD-10 dictionary to incorporate additional ICD-10 codes from primary care associated with antibiotic prescriptions (Fig. 1). We then compared antibiotic prescribing rates using the urgent care and expanded dictionaries. We included all primary care visits from 2019 to 2020 and extracted ICD-10 codes and antibiotic order data. Using the urgent care and expanded ICD-10 dictionary, we classified each encounter by prescribing tier based on whether antibiotics are almost always (tier 1), sometimes (tier 2), or almost never (tier 3) indicated. For encounters with ICD-10s in multiple tiers, we chose the lowest tier. For multiple ICD-10 codes within the same tier, we chose the first extracted ICD-10 code. We calculated antibiotic prescribing rates as the proportion of encounters associated with ≥ 1 antibacterial prescription. This quality improvement project was deemed non–human subjects research by the Stanford Panel on Human Subjects in Medical Research. Results: The urgent care dictionary has 1,400 ICD-10 codes. We added 1,439 ICD-10 codes derived from primary care encounters to create the expanded ICD-10 dictionary (8.5% tier 1, 9.1% tier 2, and 82.4% tier 3) (Fig. 1). We identified 177,531 encounters; 74% had ≥ 2 associated ICD-10 codes (Fig. 2). In total, 147,085 encounters (82.9%) were classified into a tier using the urgent care dictionary. An additional 22,039 encounters were classified with the expanded dictionary (Table 1). Most added encounters were tier 3 with low 0.7% APR (Tables 1 and 3). In total, 41,473 (28.2%) encounters were classified differently depending on the ICD-10 dictionary used, most commonly changing from tier 3 to tier 2 without an increase in overall tier 2 antibiotic prescribing rate (Tables 2 and 3). Overall antibiotic prescribing rates were similar when using either the urgent care or expanded ICD-10 dictionary (Table 2). Conclusions: The expanded ICD-10 dictionary allowed for classification of more encounters in primary care; however, it did not meaningfully change antibiotic prescribing rates. Antibiotic prescribing rates were likely diluted by classifying more encounters without identifying an associated increase in antibiotic prescribing. A more sophisticated classification system may help to accommodate the diversity and volume of ICD-10 codes used in primary care.
1. Stenehjem E, et al. Clin Infect Dis 2020;70:1781–1787.
Funding: None
Disclosures: None