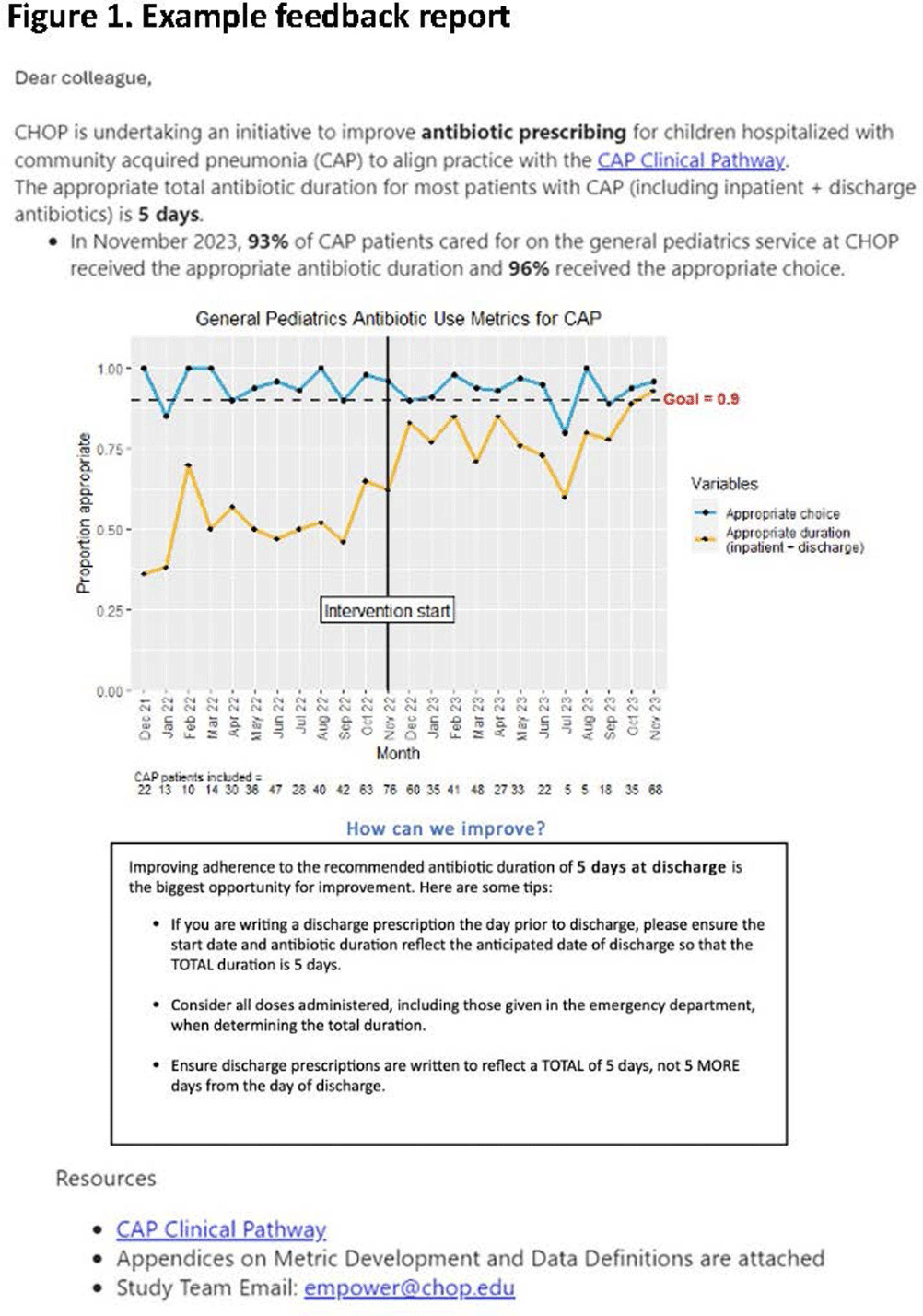
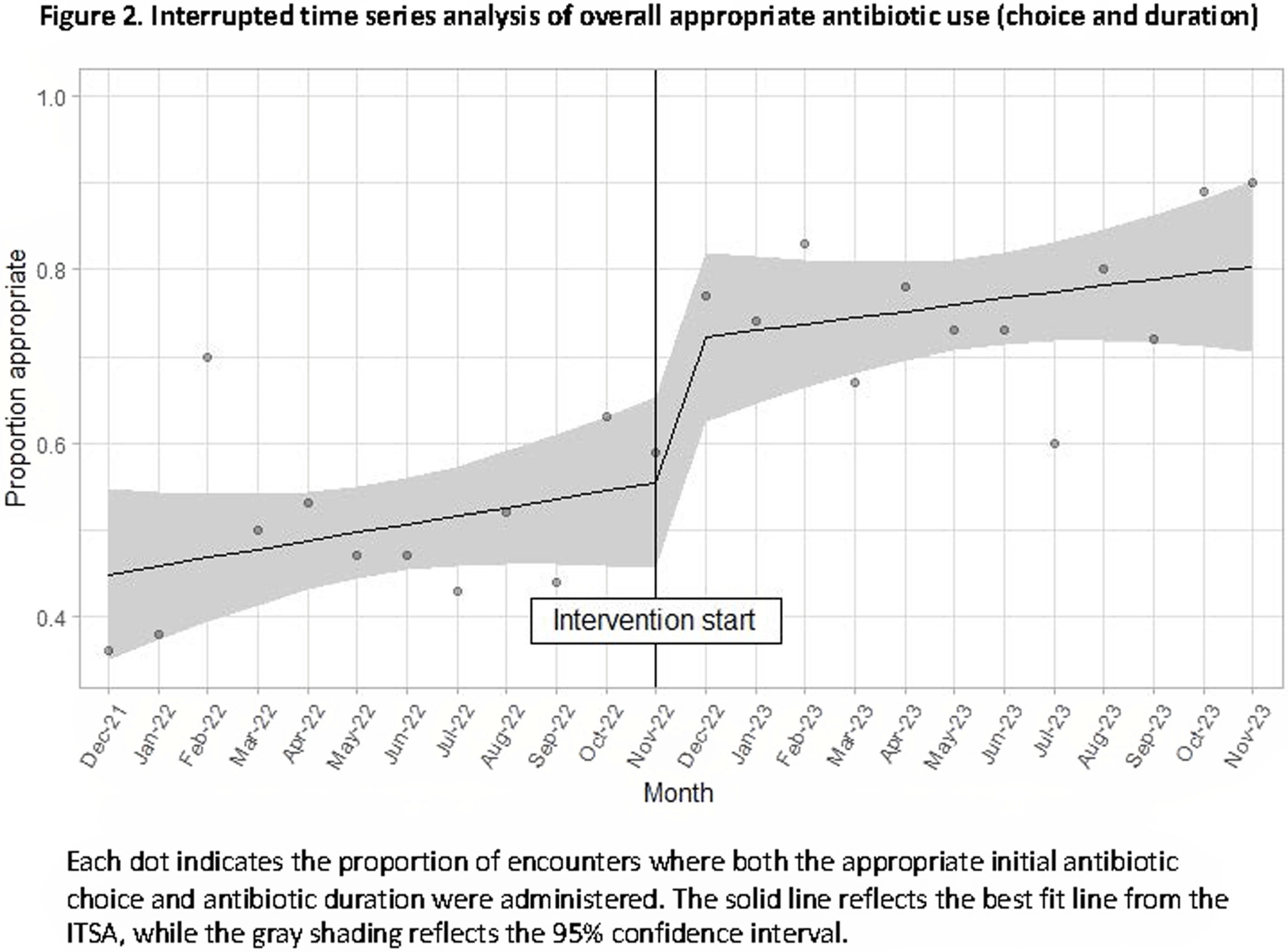
Background: Feedback reports summarizing clinician performance are effective tools to improve antibiotic stewardship in the ambulatory setting, but few studies have evaluated their effectiveness for pediatric inpatients. We developed and implemented feedback reports reflecting electronically-derived measures of appropriate antibiotic choice and duration for community acquired pneumonia (CAP) and measured their impact on appropriate antibiotic use in children hospitalized for CAP. Methods: We performed a single center quasi-experimental study including children 6 months to 17 years hospitalized for CAP between 12/1/2021-11/30/2023. Children with chronic medical conditions, ICU stays >48 hours, and outside transfers were excluded. The intervention occurred in 11/2022 and included clinician education, a monthly group-level feedback report disseminated by email (Figure 1), and a monthly review of clinician performance during a virtual quality improvement meeting. Patient characteristics were compared using chi-square or Wilcoxon rank sum tests. Interrupted time series analysis (ITSA) was used to measure the immediate change in the proportion of CAP encounters receiving both the appropriate antibiotic choice and duration, as well as the change in slope from the preintervention to the postintervention periods. Choice and duration were analyzed separately using ITSA as a secondary analysis. Results: There were 817 CAP encounters, including 420 preintervention and 397 postintervention. Patients admitted in the postintervention period were older (median age 2 years vs 3 years, P=0.03), but otherwise there were no differences in race, ethnicity, sex, ICU admission, or complicated pneumonia. Preintervention, 52% of encounters received both the appropriate antibiotic choice and duration; 96% of encounters received the appropriate antibiotic choice and 54% received the appropriate duration. The ITSA demonstrated an immediate 16% increase in the proportion of patients receiving both appropriate antibiotic choice and duration (95% confidence interval, 1-31%; P = 0.047) and no significant further increase over time following the intervention (P = 0.84) (Figure 2). When antibiotic choice was analyzed separately by ITSA, there was no immediate change or change over time in the proportion of patients receiving the appropriate antibiotic choice. In the ITSA of duration alone, there was an immediate 17% increase in the proportion receiving the appropriate duration (95% confidence interval, 2-33%; P = 0.03) and no change over time. Conclusion: Feedback reports generated from electronically-derived metrics of antibiotic choice and duration, combined with ongoing clinician education, increased the proportion of children with CAP treated with the appropriate antibiotic duration. Electronic feedback reports are a scalable and impactful intervention to improve antibiotic use in children hospitalized with CAP.
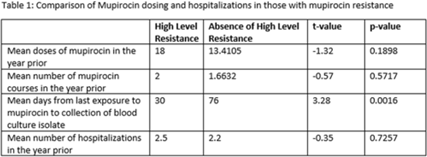
Methicillin-resistant Staphylococcus aureus (MRSA) is a common etiology of hospital-acquired infections (HAIs). One strategy to reduce HAIs due to MRSA involves a multistep decolonization process. This often involves nasal application of mupirocin 2% ointment. In our institution, when individuals meet criteria for decolonization, we recommend 5 days of treatment given twice daily. High levels of mupirocin resistance have been reported in some hospital systems, with >80% of tested isolates being resistant. To better understand our resistance levels, we selected 238 MRSA isolates from blood cultures to be tested for mupirocin resistance to correlate the presence of resistance and use of mupirocin for decolonization. We choose to assess MRSA blood isolates rather than nasal swabs given that we aim to prevent invasive MRSA infections, including blood stream infections, with decolonization. The blood cultures were collected from 11 acute-care facilities within our system from March 2021 through June 2022. High-level resistance was defined as an MIC >1,024 μg/mL according to Clinical and Laboratory Standards Institute guidelines. Of those, 7.14% showed high level resistance, and 76.47% occurred in those who were exposed to mupirocin and 23.53% occurred in those without mupirocin exposure (P = .0094). On average, those with high-level resistance had had more recent exposure to mupirocin compared to those without resistance, which was statistically significant. Also, those with high resistance, on average, received more doses of mupirocin, although this was not statistically significant. Conclusions: More recent and higher number of doses of mupirocin were associated with the development of resistance, which is consistent with what we know from pharmacodynamics of antibiotic resistance with other agents. These findings may be particularly important for those patients who have frequent hospitalizations and often require decolonization. Understanding baseline mupirocin resistance levels in an institution can assist with determining decolonization strategies.
Disclosures: None

