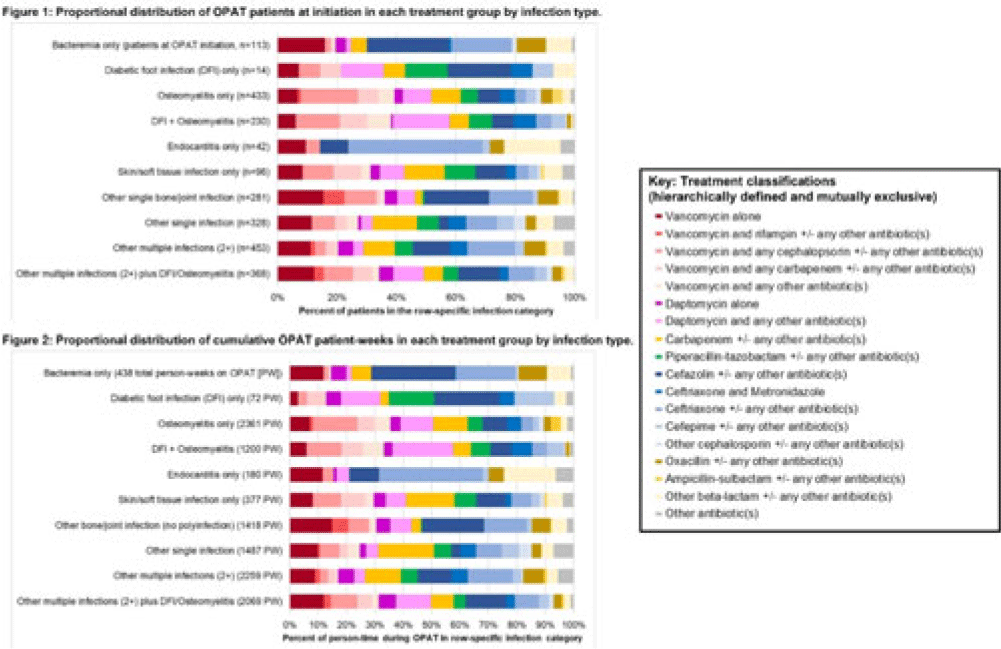
Background: Patients receiving outpatient parenteral antimicrobial therapy (OPAT) are often medically complex and require carefully tailored treatments to address severe and often concomitant infections. Our objective was to illustrate the heterogeneity in antimicrobials used for patients in OPAT, within and across infection diagnosis groups. Methods: We abstracted electronic health record data regarding day-level treatment into a registry of 2,358 OPAT courses (n = 2,072 unique patients) treated in the University of North Carolina Medical Center OPAT program during 2015–2022 (total, 11,861 person weeks; average, 7 OPAT weeks per patient). We classified infection diagnoses into 10 hierarchical or mutually exclusive categories (eg, bacteremia only, diabetic foot infection (DFI) only, osteomyelitis only) (Fig., vertical axes). Accounting for 64 antimicrobial medications and 520 cocktails administered for at least 1 patient day in our OPAT registry, we also defined 18 hierarchical or mutually exclusive classifications of treatment (eg, “daptomycin alone” or “daptomycin and any other antibiotic(s)” (Fig. key). We conducted 2 stratified analyses to describe the heterogeneity across infection diagnoses with respect (1) to medications used at OPAT initiation (patient as unit of analysis) and (2) to medications used throughout OPAT (person time as unit of analysis, allowing for differential OPAT course to other treatment classifications during follow-up). We present stacked bar charts to visualize the intersection between infection diagnosis and treatment group. Results: Among patients in this OPAT registry, 34.6% had osteomyelitis and/or DFI, 4.8% had bacteremia, and 44.6% had multiple infections (Fig. 1). The most common medications in initial OPAT regimens were vancomycin (30.8% of OPAT patients), ceftriaxone (15.0%), and daptomycin (10.9%). We observed overall similarity between the distribution of treatment groups at initiation compared to cumulative person-time during the OPAT course (Figs. 1 and 2). However, we observed heterogeneity in medications by infection diagnosis (Figs. 1 and 2); for example, vancomycin was used in 39% of osteomyelitis cases but only 14% for endocarditis (Fig. 2). For several infection groups (eg, osteomyelitis, DFI, multiple infections, “other” single infections), no treatment classification exceeded 20% use (Figs. 1 and 2). Conclusions: Day-level data on medication use in this monitored registry of patients provided evidence of heterogeneity in the types of medications used throughout treatment in OPAT, which varies within and across infection diagnoses. These data highlight the need for multilayered ascertainment of medication exposure in this medically complex patient population to inform surveillance for adverse effects and guide comparative effectiveness research for postdischarge antibiotic treatment.
Disclosures: None
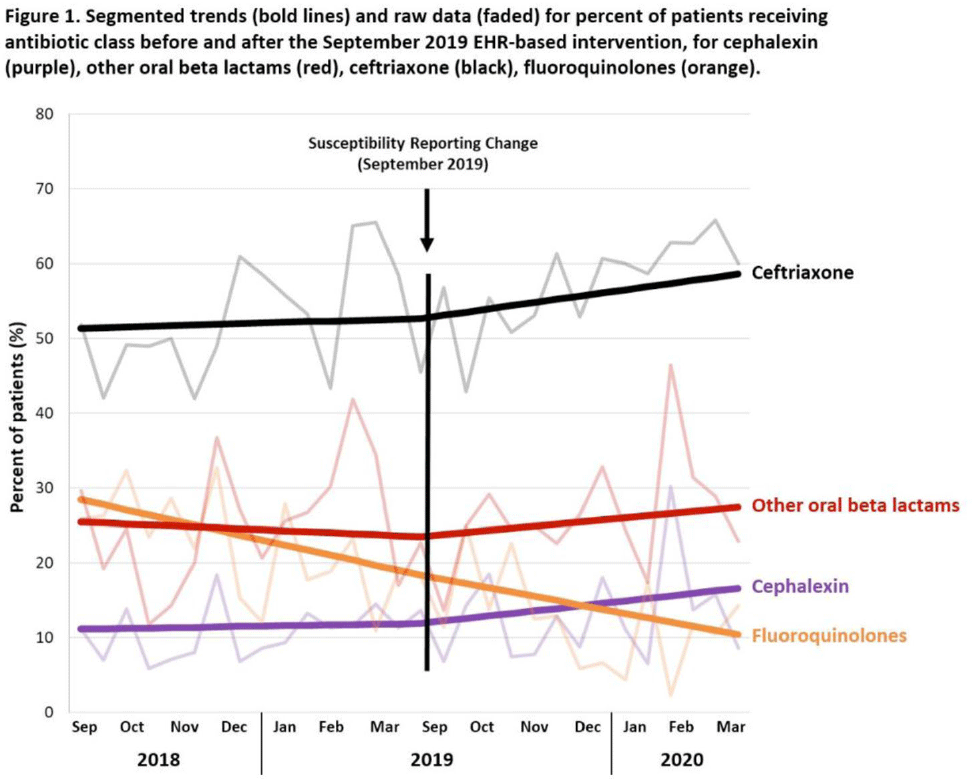
Background: Urinary tract infections (UTIs) are common in the inpatient, observation, and emergency department settings. Although many UTI-causing pathogens are susceptible to oral β-lactams, these agents are not tested directly, and susceptibility is extrapolated from other agents. To improve the use of these agents, the University of North Carolina Medical Center (UNCMC) added cephalexin to the susceptibility profile generated with urine culture results in the electronic health record (EHR). We evaluated prescribing trends of cephalexin, other oral β-lactams, fluoroquinolones, and other antibiotics for UTIs in the inpatient setting, before and after the susceptibility reporting change. Methods: An interrupted time-series analysis was conducted. Among 1,491 patients who had positive urine cultures with susceptibilities and received at least 1 antibiotic with a listed UTI indication during their inpatient stay at UNCMC, we measured the weekly prevalence (%) of patients who received each antibiotic group: cephalexin, other oral β-lactams (amoxicillin-clavulanate, cefdinir, cefuroxime), fluoroquinolones (levofloxacin, ciprofloxacin), and ceftriaxone. The study comprised a preintervention period (September 2018–March 2019) and a postintervention period (September 2019–March 2020). The prevalence of each antibiotic or group was plotted over time, and segmented linear regression was used to estimate the impact of the intervention on each antibiotic groups’ time trend. Results: At study baseline in September 2018, the weekly prevalence of antibiotic use was 11% for cephalexin, 26% for other oral β-lactams, 51% for ceftriaxone, and 29% for fluoroquinolones. Fluoroquinolone use decreased steadily throughout the study period, by 11% during the 7-month preintervention period (95% CI, −17% to −5%) and by 8% (95% CI, −13% to −3%) after the intervention (P for trend deflection, .70). In contrast, during the preintervention period, trends were flat for cephalexin, ceftriaxone, and other oral β-lactams (all P for nonzero preintervention slope were >.40). During the postintervention period, use increased for ceftriaxone (6%; 95% CI, 3%–9%). Post-intervention use also increased for cephalexin (5%; 95% CI, −3% to 12%) and other oral β-lactams (4%; 95% CI, −8%, 15%), but these trends were imprecise and not statistically significant at α = .05. Fig. 1 displays trends and raw data for each antibiotic group. Conclusions: The urine culture susceptibility reporting change was associated with small increases in cephalexin and ceftriaxone use, coincident with continued decreasing use of fluoroquinolones, for hospitalized patients with positive urine cultures and a listed UTI indication. Low-resource EHR-based interventions may confer considerable benefit for antimicrobial stewardship efforts in this clinical setting, and larger real-world studies are needed to replicate and contextualize these findings.
Funding: None
Disclosures: None