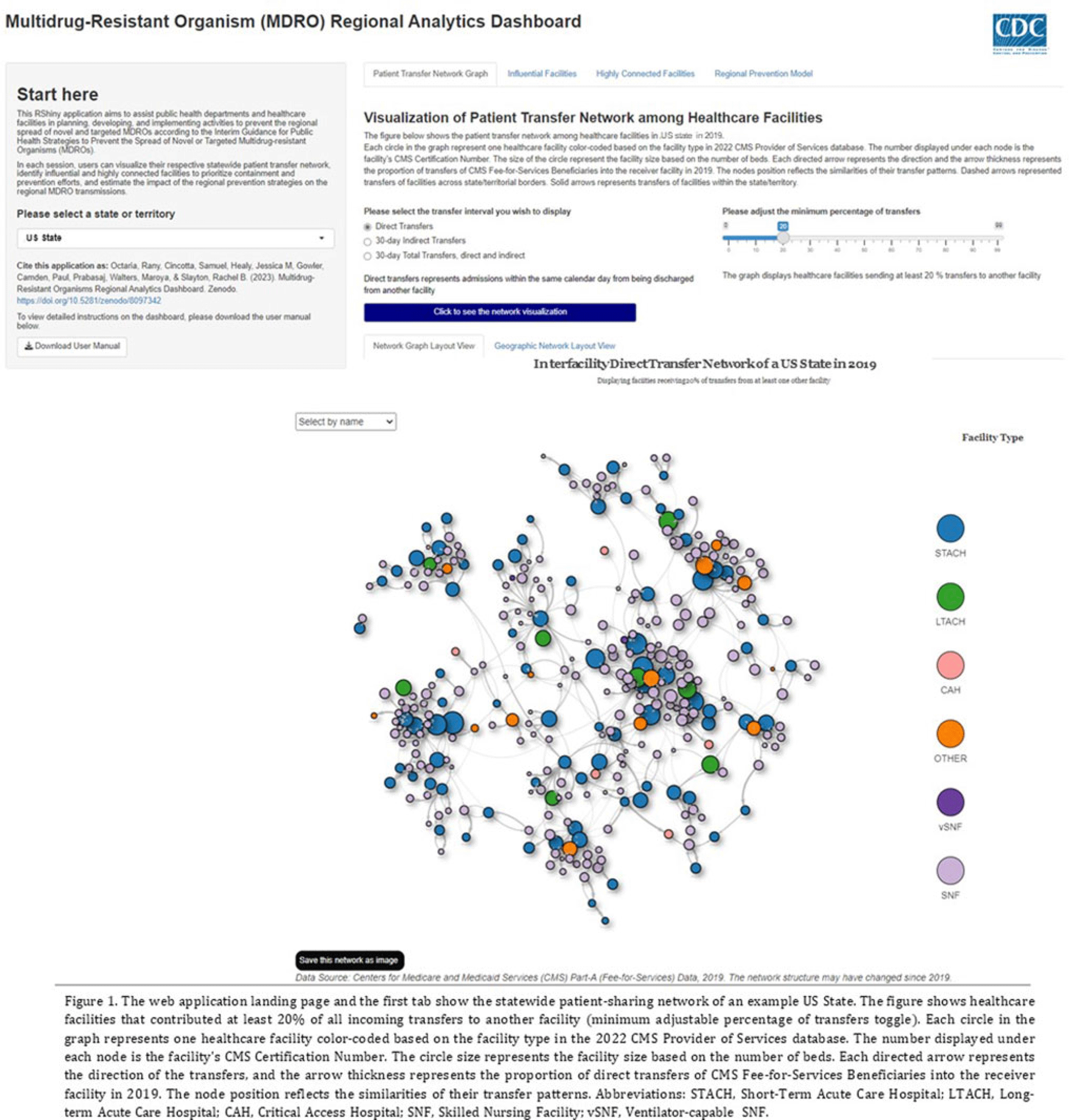
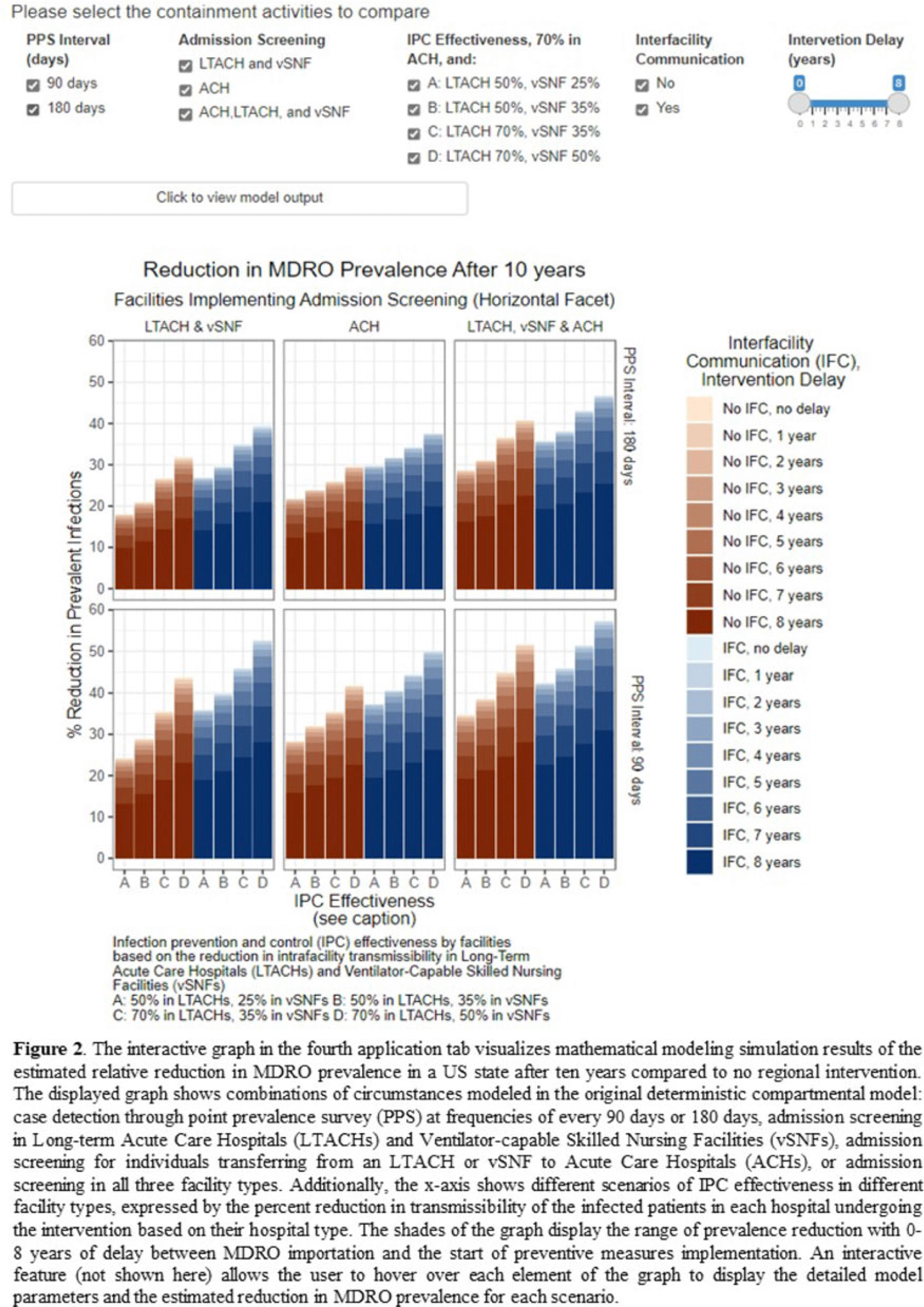
Background: The CDC’s new Public Health Strategies to Prevent the Spread of Novel and Targeted Multidrug-Resistant Organisms (MDROs) were informed by mathematical models that assessed the impact of implementing preventive strategies directed at a subset of healthcare facilities characterized as influential or highly connected based on their predicted role in the regional spread of MDROs. We developed an interactive tool to communicate mathematical modeling results and visualize the regional patient transfer network for public health departments and healthcare facilities to assist in planning and implementing prevention strategies. Methods: An interactive RShiny application is currently hosted in the CDC network and is accessible to external partners through the Secure Access Management Services (SAMS). Patient transfer volumes (direct and indirect, that is, with up to 30 days in the community between admissions) were estimated from the CMS fee-for-service claims data from 2019. The spread of a carbapenem-resistant Enterobacterales (CRE)–like MDROs within a US state was simulated using a deterministic model with susceptible and infectious compartments in the community and healthcare facilities interconnected through patient transfers. Individuals determined to be infectious through admission screening, point-prevalence surveys (PPSs), or notified from interfacility communication were assigned lower transmissibility if enhanced infection prevention and control practices were in place at a facility. Results: The application consists of 4 interactive tabs. Users can visualize the statewide patient-sharing network for any US state and select territories in the first tab (Fig. 1). A feature allows users to highlight a facility of interest and display downstream or upstream facilities that received or sent transfers from the facility of interest, respectively. A second tab lists influential facilities to aid in prioritizing screening and prevention activities. A third tab lists all facilities in the state in descending order of their dispersal rate (ie, the rate at which patients are shared downstream to other facilities), which can help identify highly connected facilities. In the fourth tab, an interactive graph displays the predicted reduction of MDRO prevalence given a range of intervention scenarios (Fig. 2). Conclusions: Our RShiny application, which can be accessed by public health partners, can assist healthcare facilities and public health departments in planning and tailoring MDRO prevention activity bundles.
Disclosures: None
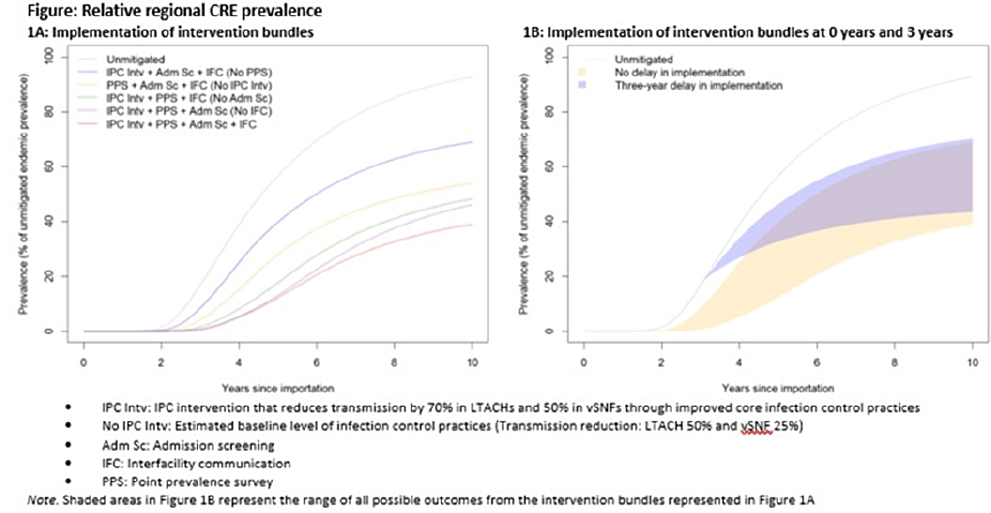
Background: Multidrug-resistant organisms (MDROs), such as carbapenem-resistant Enterobacterales (CRE), can spread rapidly in a region. Facilities that care for high-acuity patients with long average lengths of stay (eg, long-term acute-care hospitals or LTACHs and ventilator-capable skilled nursing facilities or vSNFs) may amplify this spread. We assessed the impact of interventions on CRE spread within a region individually, bundled, and implemented at different facility types. Methods: We developed a deterministic compartmental model, parametrized using CRE data reported to the NHSN and patient transfer data from the CMS specific to a US state. The model includes the community and the healthcare facilities within the state. Individuals may be either susceptible or infected and infectious. Infected patients determined to have CRE through admission screening or point-prevalence surveys at a facility are placed in a state of lower transmissibility if enhanced infection prevention and control (IPC) practices are in place. Results: Intervention bundles that included periodic point-prevalence surveys and enhanced IPC at high-acuity postacute-care facilities had the greatest impact on regional prevalence 10 years into an outbreak; the benefits of including admission screening and improved interfacility communication were more modest (Fig. 1A). Delaying interventions by 3 years is predicted to result in smaller reductions in prevalence (Fig. 1B). Increasing the frequency of point-prevalence surveys from biannually to quarterly resulted in a substantial relative reduction in prevalence (from 25% to 44%) if conducted from the start of an outbreak. IPC improvements in vSNFs resulted in greater relative reductions than in LTACHs. Admission screening at LTACHs and vSNFs was predicted to have a greater impact on prevalence if in place prior to CRE introduction (~20% reduction), and the impact decreased by approximately half if implementation was delayed until 3 years after CRE introduction. In contrast, the effect of admission screening in ACH was less (~10% reduction in prevalence) and did not change with implementation delays. Conclusions: Our model suggests that interventions that limit unrecognized MDRO introduction to, or dispersal from, LTACHs and vSNFs through screening are predicted to slow distribution regionally. Interventions to detect colonization and improve IPC practices within LTACHs and vSNFs may substantially reduce the regional burden. Prevention strategies are predicted to have the greatest impact when interventions are bundled and implemented before an MDRO is identified in a region, but reduction in overall prevalence is still possible if implemented after initial MDRO spread.
Funding: None
Disclosures: None