Clinical approaches, from Jasperian phenomenology to van Os’s continuum theory, can only go so far. There comes a point where they have to give way to attempts to identify the psychological abnormality or abnormalities that cause patients to experience delusions. The literature in this field is relatively rich, in the sense that several different lines of investigation have been pursued and methodological standards have generally been high. But it is also fair to say that it is very much a hotchpotch, with some more or less fortuitous empirical findings on the one hand, and on the other a clutch of theories that have been subjected to widely different amounts of testing.
The more or less fortuitous empirical findings grew out of a slowly dawning realization that schizophrenia is associated with cognitive impairment. Although it had been known since the 1930s that, as a group, patients with the disorder performed poorly on virtually any cognitive test they were given, it was only from the late 1970s onwards – coinciding with psychoanalytical psychiatry’s fall from grace in America – that it became acceptable to view this as being due what it obviously was due to, the presence of varying degrees of general intellectual impairment. As further investigations were undertaken, it became clear that impairment was particularly marked in certain areas of cognition, including executive or frontal lobe function, long-term memory and sustained attention. If the disease process of schizophrenia could cause specific cognitive deficits, some of which are associated with damage to particular parts of the brain, might it be, it was wondered, that these deficits could also give rise to the symptoms of the disorder? The focus of attention quickly became executive impairment, and a whole industry sprang up devoted to drawing parallels between different clinical features of schizophrenia and the symptoms and signs of the frontal lobe syndrome (e.g. Seidman, Reference Seidman1983; Weinberger, Reference Weinberger1988; Robbins, Reference Robbins1990; McGrath, Reference McGrath1991; Frith, Reference Frith1992). As will be seen, however, delusions were not destined to yield to an analysis.
Even when it was at the height of its influence, the stranglehold of psychoanalysis over thinking about schizophrenia was not total and a few scientific approaches to delusions managed to eke out an existence. Since its fall many more have been proposed. Some of these continue to be rooted in the concept of a brain-based psychological dysfunction, but do not assume a simple one-to-one mapping between particular regions and symptoms; these are the so-called cognitive neuropsychological or cognitive psychiatric approaches. Others ignore brain localization altogether, and simply aim to discover a cognitive abnormality that is present in patients who are deluded. An important by-product of both these latter approaches is that the abnormal function is no longer constrained to being a deficit, as it is in neuropsychological theories, but is now free to take the form of hyperactivity, or altered processing of information in a system, or any of the various other ways in which cognitive psychologists are accustomed to thinking.
A convenient place to start a discussion of the psychology of delusions is with the neuropsychological approach, where the concepts are simple and straightforward. This then lays the groundwork for the somewhat more complicated cognitive neuropsychological approach. Only two proposals of this type are considered here; discussion of a third important approach is postponed to Chapter 7, partly because it is mainly devoted to delusions and delusion-like symptoms in neurological patients rather than those with psychiatric disorders, and partly because it needs a whole chapter to itself. Finally, the success or otherwise of some of the more important purely cognitive approaches is examined.
The Neuropsychology of Delusions
In 1980, Crow galvanized the world of schizophrenia research by arguing that the many and varied symptoms of the disorder showed a previously unsuspected underlying order. Specifically, he drew a conceptual distinction between positive symptoms, i.e. those that were characterized by the presence of an abnormality – such as delusions, hallucinations and formal thought disorder – and negative symptoms, where there was an absence or diminution of a normal function, such as lack of volition, poverty of speech and flattening of affect. Making such a distinction seemed to have deeper implications: for example, positive symptoms were characteristic of acute schizophrenia, which tended to be episodic and responded to treatment with antipsychotics, whereas negative symptoms were typically seen in chronic schizophrenia, where they were enduring and drug treatment was at best only marginally effective. This in turn suggested that there were two different pathological processes in schizophrenia, one reversible and perhaps neurochemical in nature and the other, which Crow (Reference Crow1980) speculated (wrongly as it turned out) might be related to the lateral ventricular enlargement seen in the disorder, which he and his colleagues (Johnstone et al., Reference Johnstone, Crow, Frith, Husband and Kreel1976) had recently discovered.
Two years later Andreasen and co-workers (Andreasen, Reference Andreasen1982; Andreasen & Olsen, Reference Andreasen and Olsen1982) were able to show that, whatever the distinction between positive and negative symptoms meant aetiologically, it was valid at the clinical level – positive symptoms tended to correlate significantly with other positive symptoms but not with negative symptoms, and vice versa. True, there were some minor anomalies. One of these was that delusions and hallucinations appeared to be considerably more strongly associated with each another than with formal thought disorder. Another was that an uncommon symptom, inappropriate affect, did not correlate with symptoms in either category.
The true significance of these irregularities became apparent when Liddle (Reference Liddle1987a) used a more sophisticated method for examining associations among multiple variables, factor analysis. He applied this to detailed ratings of the symptoms of 40 chronic schizophrenic patients with stable clinical pictures, and found that three factors emerged. Two of these were immediately recognizable as positive and negative symptoms: one had high loadings on auditory hallucinations, delusions of persecution and delusions of reference; Liddle termed this factor reality distortion. The other, which he called psychomotor poverty, loaded heavily on poverty of speech, decreased spontaneous movement, unchanging facial expression, paucity of expressive gestures, affective non-responsivity and lack of vocal inflection. The third factor was composed of various elements of formal thought disorder, plus inappropriate affect. Liddle termed this the disorganization syndrome.
The validity of Liddle’s three syndromes is now widely accepted. Most subsequent factor analytic studies (see Andreasen et al., Reference Andreasen, Arndt, Alliger, Miller and Flaum1995; Thompson & Meltzer, Reference Thompson and Meltzer1993) have continued to isolate three factors; the small minority that have not have either tended to split the positive or negative factor in some not very intuitive way, or merely found additional factors corresponding to depressed or elated mood. Three studies using confirmatory factor analysis, which tests the goodness-of-fit of different models, all found that more than two factors were needed to satisfactorily account for the pattern of correlations among schizophrenic symptoms and that there was little to choose mathematically between three- and four-factor models (Brekke et al., Reference Brekke, DeBonis and Graham1994; Dollfus & Everitt, Reference Dollfus and Everitt1998; Peralta & Cuesta, Reference Peralta and Cuesta1994).
Just as Crow (Reference Crow1980) argued with positive and negative symptoms, the existence of three distinct constellations of symptoms in schizophrenia implies the presence of three different underlying pathological processes. Liddle (Reference Liddle1987b) tested this prediction neuropsychologically. In 47 chronic schizophrenic patients, negative symptom and disorganization scores were found to be associated with poor performance on a number of different cognitive tests, with the pattern of correlations being somewhat different for the two syndromes. In contrast, reality distortion correlated with impairment on only one test (which measured figure – ground perception). For some reason, Liddle (Reference Liddle1987b) did not actually include any tests of executive function in his battery, even though by then this had become the main focus of interest in neuropsychological schizophrenia research. However, this omission was put right in a subsequent study (Liddle & Morris, Reference Liddle and Morris1991), which used four executive tests. Once again significant correlations were found with negative symptoms and disorganization, but not with reality distortion.
The present author and a colleague (McKenna & Oh, Reference McKenna and Oh2005) reviewed the many further studies that have examined the associations among the positive, negative and disorganization syndromes and a wide range of cognitive test measures. The results are shown in Table 5.1. Both negative symptoms and disorganization were often, though by no means always, found to show significant correlations with impairment on tests of executive function, and also with tests of memory, language, visual and visuospatial function and even general measures such as IQ. However, only three studies found evidence for an association with reality distortion.
Table 5.1 Neuropsychological Correlations with Positive, Negative and Disorganization Syndromes in Different Studies
| Reality Distortion | Disorganization | Negative Symptoms | |
|---|---|---|---|
|
Executive function | |||
| Wisconsin Card Sorting Test | ✓3✓19✓5✓22✓23✓6✓21✓18✓24✓9 | ✓12✓13✓4✓17✓24✓9 | |
| Verbal fluency | ✓9 | ✓3✓9✓2✓16 | ✓3✓12✓13✓19✓4✓23✓16✓17✓9 |
| Stroop test | ✓10 | ✓3✓14✓22✓10✓26 | ✓3✓7 |
| Trailmaking test (B) | ✓3✓18✓22✓23✓9 | ✓13✓19✓4✓23✓9 | |
|
Short-term and working memory | |||
| Verbal (digit span) | ✓18✓22✓4✓20 | ✓8✓21 | |
| Non-verbal (Corsi blocks) | ✓1 | ||
| Working memory | ✓23✓24 | ✓23 | |
|
Long-term memory | |||
| General memory | ✓15 | ✓13 | |
| Verbal memory | ✓12 | ✓1✓8✓18✓25 | ✓12✓13✓19✓17 |
| Visual memory | ✓12✓13 | ✓8✓13✓19✓17 | |
| Other | ✓2 | ✓1 | |
|
General intellectual function | |||
| Full scale IQ | ✓13✓19 | ✓13 | |
| Verbal IQ | ✓8 | ✓8 | |
| Performance IQ | ✓17 | ||
| Other IQ | ✓7✓8✓2 | ✓1✓2✓7 | |
|
Miscellaneous | |||
| Language | ✓8 | ✓1 | |
| Visual/visuospatial function | ✓11 | ||
| Sustained attention | ✓1✓18✓2✓21 | ✓19✓18✓2✓21 | |
1 Liddle (Reference Liddle1987b);
2 Frith et al. (Reference Frith, Leary, Cahill and Johnstone1991);
3 Liddle and Morris (Reference Liddle and Morris1991);
4 Brown and White (Reference Brown and White1992);
5 Van der Does et al. (Reference Van der Does, Dingemans, Linszen, Nugter and Scholte1993);
6 Bell et al. (Reference Bell, Lysaker, Milstein and Beam-Goulet1994);
7 Brekke et al. (Reference Brekke, Raine and Thomson1995);
8 Cuesta and Peralta (Reference Cuesta and Peralta1995);
9 Himelhoch et al. (Reference Himelhoch, Taylor, Goldman and Tandon1996);
10 Joyce et al. (Reference Joyce, Collinson and Crichton1996);
11 Cadenhead et al. (Reference Cadenhead, Geyer and Butler1997);
12 Norman et al. (Reference Norman, Malla and Morrison-Stewart1997);
13 Basso et al. (Reference Basso, Nasrallah, Olson and Bornstein1998);
14 Baxter and Liddle (Reference Basso, Nasrallah, Olson and Bornstein1998);
15 Clark and O’Carroll (Reference Clark and O’Carroll1998);
16 Robert et al. (Reference Robert, Lafont and Medecin1998);
17 Mohamed et al. (Reference Mohamed, Paulsen, O’Leary, Arndt and Andreasen1999);
18 Eckman and Shean (Reference Eckman and Shean2000)Rowe and Shean (Reference Rowe and Shean1997);
19 O’Leary et al. (Reference O’Leary, Flaum and Kesler2000);
20 Tabares et al. (Reference Tabares, Sanjuan, Gomez-Beneyto and Leal2000);
21 Guillem et al. (Reference Guillem, Bicu and Bloom2001);
22 Moritz et al. (Reference Guillem, Bicu and Bloom2001);
23 Cameron et al. (Reference Cameron, Oram and Geffen2002);
24 Daban et al. (Reference Daban, Amado and Bayle2002);
25 Pollice et al. (Reference Pollice, Roncone and Falloon2002);
26 Woodward et al. (Reference Woodward, Ruff, Thornton, Moritz and Liddle2003).
Even this minimal support for an association between reality distortion and cognitive impairment vanished in a meta-analysis examining the relationship between Liddle’s three syndromes and executive function. Dibben et al. (Reference Dibben, Rice, Laws and McKenna2009) found that the pooled correlation between tests of executive function and reality distortion scores was +0.01 in 34 studies. In contrast there were small but significant pooled correlations with negative symptoms (-0.21 in 83 studies) and disorganization (-0.17 in 40 studies).
The conclusion is stark: while neuropsychological theories of negative symptoms and disorganization are possible, reality distortion, and so by extension delusions, cannot be explained in such a way. The lack of correlation between reality distortion and measures of general intellectual function like IQ also makes it unlikely that delusions could be associated with some as yet undiscovered aspect of neuropsychological function; general intellectual impairment would by definition also affect this unknown cognitive system. The only way that a neuropsychological deficit might be able to play a role in the development of delusions appears to be in the special case that it is merely one step in a more complicated chain of cognitive events. This idea forms the basis of the class of cognitive neuropsychological theories discussed in Chapter 7, but for the time being something beyond a simple deficit account of delusions seems to be required.
Beyond Neuropsychology: The Cognitive Neuropsychology of Delusions
Any theory that tries to explain delusions in terms of impaired neuropsychological function is, it seems, doomed to failure. But perhaps this is just a reflection of the rather simplistic approach to neuropsychology that has so far been taken. After all, not all of the symptoms of localized brain damage take the form of loss of function. One obvious example is fluent dysphasia; another is confabulation in patients with amnesia (a topic which is revisited in Chapter 7). The idea of mapping cognitive functions to discrete areas of the brain may also be too simple in another way – many specific neuropsychological functions are likely to depend on the joint operation of widely dispersed brain areas. As the network of regions involved becomes more complicated, the potential ways in which dysfunction might manifest itself might also become more varied, and it becomes possible to think about release from inhibition or lack of monitoring or some other consequence of failure of the normal interaction between modules making up a cognitive system.
This, at any rate, is the hope of cognitive neuropsychiatry. As described by two of its founders, Halligan and David (Reference Halligan and David2001), this discipline aims to explain psychopathology in terms of altered function of normal cognitive mechanisms, based on the assumption that ‘complex interactions between neural systems presumably underlie most psychological processes [and] no neuropsychological account of how the brain “works” would ever be complete without this cognitive level of analysis’. They also make it clear that alterations in the interactions between neural systems will result in something more than just impaired function: ‘Psychological disturbances experienced by psychiatric patients are slowly coming to be understood in terms of disturbances – excesses as well as deficits – to recognized information-processing systems.’
For Halligan and David (Reference Halligan and David2001) the paradigmatic example of how the cognitive neuropsychiatric approach can be applied to delusions was the Capgras syndrome, the belief that one’s wife, husband or other family member has been replaced by an almost identical double, which occurs in patients with a range of neurological diseases as well as in psychiatric disorders like schizophrenia, and is discussed in detail in Chapter 7. Leaving this aside, they identified semantic memory as a promising area for a cognitive neuropsychology of delusions. They also felt that the concept of theory of mind might also be a good place to look, although not specifically in relation to this symptom.
Semantic Memory
Semantic memory is the store for all knowledge about the world. The concept dates back to a famous observation by Tulving (Reference Tulving, Tulving and Donaldson1972) concerning the two different ways in which the term memory can be used. On the one hand there is episodic memory or memory for events, i.e. memory for one’s own individual happenings and doings, such as what one had for breakfast and who one met on holiday last year. On the other hand, everyone has a vast store of impersonal knowledge which, like episodic memory, is held outside consciousness but can be accessed into it when required. For Tulving, this impersonal knowledge was originally knowledge of the meaning of words, but he and others (Kintsch, Reference Kintsch and Nickerson1980; Tulving, Reference Tulving1983) soon realized that the concept also applied to all other knowledge, from simple factual information such as knowing the capital of France or the chemical formula for salt, to abstract concepts such as truth and justice.
A cognitive system concerned with what we know to be factually true clearly has potential as a theory of delusions, specifically propositional delusions. This is particularly so when it when it is realized that a there is a recognized subdivision of semantic memory which holds one’s knowledge about oneself. The most basic item held in personal semantic memory is one’s name, but this type of knowledge extends to all kinds of personal data ranging from what one does for a living and where one lived at different times of one’s life, to what kind of restaurants one likes to go to and which political party and football team one supports.
As befits a candidate for a cognitive neuropsychiatric theory, semantic memory is firmly anchored in regional brain function. This became clear only relatively recently, however, when Warrington (Reference Warrington1975) described three patients whose unusual pattern of perceptual, language and memory deficits could be understood as a progressive breakdown of semantic knowledge. Subsequently semantic dementia, or the temporal lobe variant of fronto-temporal dementia, has become a well-established clinical and pathological entity (e.g. Hodges, Reference Hodges2007; Snowden et al., Reference Snowden, Goulding and Neary1989). As described by Hodges et al. (Reference Hodges, Patterson, Oxbury and Funnell1992) and Snowden et al. (Reference Snowden, Neary and Mann1996), it typically starts with an inability to remember the names of people, places and things. The deficit is not restricted to naming, however, and patients also perform poorly when asked to give definitions of words, with their responses being grossly impoverished and often containing elementary factual errors. Although the patients complain that they ‘can’t remember anything’, episodic memory remains intact until late in the course of the illness, and they are able to find their way around, keep appointments, and have no difficulty remembering day-to-day events.
Many studies (reviewed and meta-analysed by Doughty and Done, Reference Doughty and Done2009) have documented that semantic memory is an area of impairment in schizophrenia. Of course, the fact that reality distortion is not associated with neuropsychological deficits in general makes it unlikely that there would an association between delusions and semantic memory impairment in particular, and this is exactly what was found by Mortimer et al. (Reference Mortimer, Bentham and McKay1996) in a study using the Sentence Verification or ‘Silly Sentences’ Test (Collins & Quillian, Reference Collins and Quillian1969), where subjects have to indicate whether statements such as Rats have teeth and Onions crush their prey are true or false. The task is very easy and performance is measured in terms of speed of verification of the sentences. Fifty-three chronic schizophrenic patients showed no significant correlation between speed of verification and scores on a delusions scale.
On the other hand, a hint that semantic memory dysfunction in schizophrenia might involve more than just impairment came from a further examination of the findings from the same group of 53 schizophrenic patients by Tamlyn et al. (Reference Tamlyn, McKenna and Mortimer1992). As expected, the patients were found to be significantly slower at verifying the sentences than a group of 38 age-matched healthy controls. More interestingly, whereas none of the controls made more than two verification errors, 14 (26 per cent) of the patients made three or more errors, with 5 making them in large numbers (>10); these were often but not always in the direction of verifying false statements as true. Errors were seen particularly in patients with formal thought disorder, but also in a small number of patients who had clinical pictures dominated by florid delusions.
There were further hints in a study by Chen et al. (Reference Chen, Wilkins and McKenna1994) with the title ‘Semantic memory is both impaired and anomalous in schizophrenia’. They used a task in which the subjects had to decide, by pressing a button, whether or not a word displayed on a screen belonged in a particular semantic category. For example, the subjects would see the category bird, which on different trials would be coupled with exemplars such as robin (typical of the semantic category), turkey (atypical but still within the category), penguin (borderline), aeroplane (related but outside the category) and bell (unrelated). Twenty-eight healthy controls showed increasing response times as they moved from the typical to the atypical and the borderline exemplars, with response times then decreasing again progressively in the related and unrelated categories. Thirty-nine schizophrenic patients were found to be overall slower than the controls, but additionally their response times increased progressively up to the related but outside category, and only decreased again in the unrelated category. The same pattern was found when errors rather than reaction time were analysed. In this study, however, in contrast to that of Tamlyn et al. (Reference Tamlyn, McKenna and Mortimer1992), the apparent outward shift of semantic category boundaries in schizophrenia was not associated with any symptom.
The definitive study examining semantic memory in relation to delusions was carried out by Rossell et al. (Reference Rossell, Shapleske and David1998). They used the Silly Sentences task but modified it in two ways. First, they made it harder, so that not only patients but also controls would make significant numbers of errors. This was achieved by including not only obviously true and obviously false sentences but also a third category of statements that could be true in some situations, for example Leaves are red. Secondly, they manipulated the emotional content of all three types of sentences so that some of them touched on common delusional topics. Accordingly, there were sentences with a violent or dangerous themes such as Knives are dangerous (true); A cactus can bite (false); and Joy riders can return the cars they steal (unlikely); those with themes associated with superiority, such as Inventors are talented and clever (true), Scientists can turn grass blue (false) and Dentists can be talented artists (unlikely); and those with a religious dimension, such as Vicars work on Sundays (true); The bible is a car catalogue (false); and Monks are alcoholics (unlikely). Other sentences had a political, sexual or health content. The predictions were that deluded schizophrenic patients would show more errors than controls, particularly when the sentences had an emotional content, and that they would tend to accept ambiguous sentences as true if they were congruent with their delusional ideas.
Sixty-three patients meeting DSM-IV criteria for schizophrenia or schizo-affective disorder were compared to 66 well-matched healthy controls. Both groups made small numbers of errors (<10 per cent) on the true and false sentences, but many more (>50 per cent) on the unlikely ones. The schizophrenic patients did not make more errors overall, and there were no marked differences between the groups with respect to emotional type. The crucial comparison concerned the relationship with the schizophrenic patients’ delusions. To examine this, the patients’ two to three most common past or present delusions were classified as persecutory, grandiose, political, religious, or involving relationships or bodily function, and any errors they made on the emotional sentences were rated as ‘delusion congruent’ or ‘delusion incongruent’. An initial analysis showed that the patients made similar numbers of errors on emotional sentences that were congruent with and not congruent with their delusions. However, they also showed a small but significant tendency to incorrectly accept false statements (i.e. answering true to nonsense sentences) and incorrectly reject true statements (i.e. answering false to true and unlikely sentences). The findings are shown in Figure 5.1.
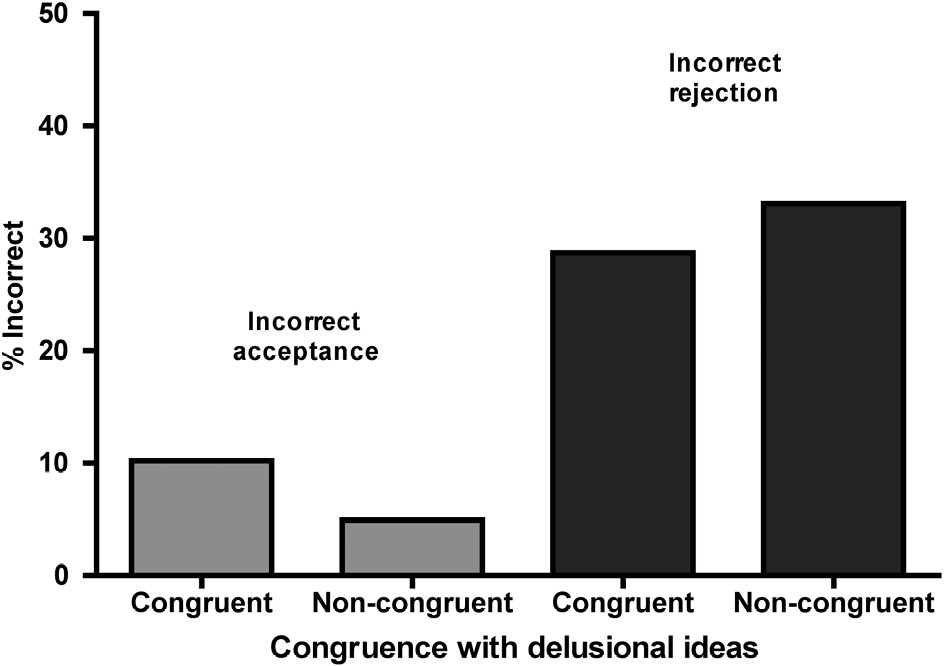
Figure 5.1 Schizophrenic patients’ errors in sentence verification as a function of whether they were congruent with their delusions. The interaction term in the ANOVA was significant.
A reasonable interpretation of Rossell et al.’s (Reference Rossell, Shapleske and David1998) findings might be that while deluded patients may show erroneous knowledge about the world in areas of semantic memory related to their delusions, this is subtle to the point of testing the limits of the technique used. However, it might be wrong to dismiss the possibility altogether. This is because another study has had quite similar findings. Laws et al. (Reference Laws, McKenna and McCarthy1995) carried out a single case study (a respectable research strategy in neuropsychology) on a schizophrenic patient with a clinical picture consisting almost entirely of grandiose delusions. The patient was a 39-year-old man who believed he was a Baron, and that he was, or was about to become, a Conservative MP (and also manager of a football club). His general intellectual function was relatively well preserved (estimated premorbid IQ 107, current IQ 99), but, like many patients with schizophrenia, he showed mild to moderate impairment in executive function and long-term memory. More unusually, he also showed a moderately severe deficit in recognition of faces. For example, when presented with a series of 53 photographs of famous people (e.g. Marilyn Monroe, Nelson Mandela, Mother Theresa, James Dean), he named only 18, in comparison to mean of 39.6 in 20 age and premorbid IQ matched healthy subjects. Even when he recognized the faces as familiar without being able to name them, his knowledge about the people concerned was obviously impaired: he was able to give their occupation in 39 cases, but produced specific identifying information in only 19, and what he said sometimes contained gross errors, as shown in Table 5.2. The normal controls were at ceiling on these two aspects of the task.
Laws et al. (Reference Laws, McKenna and McCarthy1995) noticed that many of the faces the patient named correctly were of politicians. When subsequently shown a new set of photographs of 34 domestic and international politicians (e.g. Anthony Eden, Dwight Eisenhower, Harold Wilson, Indira Gandhi, Ayatollah Khomeini), he correctly named 19/34 (55.9 per cent) of them, in contrast to 15/76 (19.7 per cent) of a set of famous people from other walks of life. As also shown in Table 5.2, the responses he gave in response to the names of the politicians (at least the British ones) were much richer in detail than for the non-politicians. At the same time, however, his descriptions showed a tendency to include fabricated material that was often highly unlikely, e.g. that David Owen, a prominent member of the Social Democratic Party, was also leader of the Scientologists and that the leader of the Liberal Party, David Steel, had stood in the Italian elections. The presence of such material was more frequent for the politicians than for the non-politicians (57 per cent vs 17 per cent).
Table 5.2 Laws et al.’s (Reference Laws, McKenna and McCarthy1995) Patient’s Knowledge about Famous People
A. General
| Name | Information Provided |
|---|---|
| Marilyn Monroe | American actress I think. I wouldn’t know if she was dead or alive, but I think she’s still alive. |
| Elvis Presley | I think he’s an American singer and musician, still alive. |
| John F. Kennedy | Former president who was killed in Dallas in 1963, killed by Oswald Mosley, it was tragic. I’m not sure if Mosley was found guilty or not. |
| Telly Savalas | ‘Ironside’, he was bald, he played ‘Ironside’, detective, he was in a wheelchair. |
| Luciano Pavarotti | A ballet dancer I think. |
| Yasser Arafat | Don’t know much about him, except that he’s the Israeli Prime Minister. |
| Nelson Mandela | He’s made a comeback recently, Kenyan leader, he won the Nobel Peace Prize, sharing it with someone else, he’s been in prison as well. |
B. Domestic politicians
| Name | Information Provided |
|---|---|
| Margaret Thatcher | Ah, Mrs T, best Prime Minister in my lifetime, leader of the Conservative Party since 1979. Former MP for Finchley, she came from Grantham, you know. Married to a Dennis, a millionaire. She wrote to me, asking me to take the Plaid Cymru seat. We should not have got rid of her. I feel personally responsible for the demise of Mrs Thatcher because I voted against her in the second ballot. Now known as Baroness Thatcher, a member of the House of Lords. |
| John Major | I’ve met him in Huntington, he smiled at me, but his wife ignored me. Wrong choice as Prime Minister. Dubious whether he’s suited to being an MP, never mind Prime Minister. He was chief secretary to the treasury before. Also foreign secretary for six months. Never even went to University. |
| David Steel | He was a famous leader of the Liberal party. Went on with David Owen to form the Alliance – SDP – Social Democrat Alliance. David Owen is now in Bosnia, trying to arrange peace. He [Owen] is the leader of the Scientologists. They wrote to me recently asking me to stand as their MP in Wales. The SDP lasted for a while and he and Owen bust up, maybe in 1983, after that election. David Steel represents a constituency on the Scottish Border. He was a candidate in the elections in Italy, came fourth out of 16 – I guess he must have made a lot of money from that. |
This case could be considered nothing more than a curiosity – most patients with schizophrenia do not show marked impairments in familiar face processing, although another such patient has been reported (Shallice et al., Reference Shallice, Burgess and Frith1991) – but it is intriguing that, in the midst of a marked deficit in semantic memory for people, the patient showed an island of preserved knowledge for British politicians, which also happened to be one of the themes of his delusions. Here, in line with what might be expected from a cognitive neuropsychiatric theory of delusions, some of the stored information also appeared to be corrupted.
Theory of Mind
The concept of theory of mind, the ability to infer the mental states of others, is not something that grew out of observations on patients with brain damage. Instead its origins were in primate psychology and the ideas were later applied to developmental psychology, leading to the spectacularly successful theory that theory of mind impairment is the key cognitive deficit in autism. Only belatedly have circumscribed theory of mind deficits been identified in patients with brain damage, especially those with the frontal lobe syndrome and fronto-temporal dementia (Brüne & Brüne-Cohrs, Reference Brüne and Brüne-Cohrs2006; Kipps & Hodges, Reference Kipps and Hodges2006).
How theory of mind abnormality came to be a theory of delusions is due mainly to the work of Frith. In his book, The Cognitive Neuropsychology of Schizophrenia (Frith, Reference Frith1992), he argued that schizophrenic symptoms which involved a feeling of alien control could potentially be understood as a disorder of self-monitoring, specifically a failure to label movements as being self-generated (see Chapter 1). In a similar but more complicated way, he argued that another failure of self-monitoring, this time of inner speech, could give rise to auditory hallucinations. He then made a conceptual leap and suggested that self-monitoring is just one example of a more general failure in the representation of mental states, encompassing both a failure to represent one’s own mental states (previously self-monitoring) and now also a failure to represent the mental states of others. Representation of other people’s mental states is simply another way of saying theory of mind, and this led Frith to propose that impairment in this ability, arising de novo in adult life, could give rise to both referential and propositional delusions:
The failure of metarepresentation associated with adult schizophrenia may well be qualitatively different from that associated with childhood autism. The autistic child does not try to infer the mental states of others. In contrast, adult schizophrenic patients, because their early development has been relatively normal, will continue to make inferences about the mental states of others, but will often get these wrong. They will ‘see’ intentions to communicate when none are there (delusions of reference). They may start to believe that people are deliberately behaving in such a way as to disguise their intentions. They will deduce that there is a general conspiracy against them and that people’s intentions towards them are evil (paranoid delusions).
Frith’s (1992) proposal set in motion a wave of studies investigating theory of mind in schizophrenia. These quickly established that performance was impaired on tests ranging from adult versions of the classical false belief task used in autistic children (Frith & Corcoran, Reference Corcoran and Frith1996; Doody et al., Reference Doody, Götz, Johnstone, Frith and Owens1998), to those examining the ability to understanding implied meaning (Corcoran et al., Reference Corcoran, Mercer and Frith1995), or to get jokes that depend on understanding what is in a person’s mind (Corcoran et al., Reference Corcoran, Cahill and Frith1997). Two meta-analyses (Sprong et al., Reference Sprong, Schothorst, Vos, Hox and van Engeland2007; Bora et al., Reference Bora, Yucel and Pantelis2009) later found that the degree of impairment was substantial and larger than could be attributed to any accompanying general intellectual impairment.
The important question, however, is not whether performance on theory of mind tasks is impaired in schizophrenia, but whether it is related to delusions. On the face of it, the answer would be predicted to be no, since this would violate the principle established above that reality distortion is not associated with any kind of cognitive deficit. And so it proved: while initial studies by Frith and co-workers (Corcoran et al., Reference Corcoran, Mercer and Frith1995; Corcoran & Frith, Reference Corcoran and Frith1996; Frith & Corcoran, Reference Frith and Corcoran1996; Corcoran et al., Reference Corcoran, Cahill and Frith1997) tended to support the view that patients with symptoms such as alien control and persecutory delusions showed poor performance on theory of mind tests, a later meta-analysis of six studies examining the correlations between performance on various theory of mind tests and Liddle’s three syndromes (Ventura et al., Reference Ventura, Wood and Hellemann2013) revealed the familiar pattern of significant correlations with negative symptoms (r = -0.25) and disorganization (r = -0.32) but not reality distortion (r = -0.08).
One study seems particularly damning in this respect. Walston et al. (Reference Walston, Blennerhassett and Charlton2000) conducted a search for patients with psychotic illnesses characterized only by delusions. They were able to find four such cases; none of them showed other schizophrenic symptoms, and they would probably have qualified for a diagnosis of delusional disorder (although the authors did not apply diagnostic criteria). They were all intellectually relatively intact, defined in terms of scores above the cut-off for cognitive impairment on a widely used measure of this (the Mini-Mental State Examination, MMSE). All four patients scored at ceiling or close to this on three theory of mind tests. A summary of one of the patients is shown in Box 5.1, which also makes it clear that he had no difficulty attributing mental states to his imaginary persecutors.
Box 5.1 Theory of Mind in a Patient with Delusions and No Other Symptoms (Walston et al., Reference Walston, Blennerhassett and Charlton2000)
Case A was 40-year-old married man who was married with three children. His delusional beliefs started to form the day after he was involved in a fight in which he seriously injured a man. He thought that he was overheard making disparaging remarks about drug dealers whilst at work one day, and that this conversation was reported back to the drug ‘mafia’ who concluded that he must be a police informer. After this incident, he began to notice that he was being followed by groups of young men who operated from a fleet of cars, both of which changed over time, and he came to believe that they wanted to catch and kill him because they believed he was a ‘supergrass’. As a result, he ran away from home and began to live rough, hiding out in remote country areas, and moving frequently from place to place. After some days, however, he became physically and emotionally exhausted, and returned home where he became depressed, consumed large quantities of alcohol, and made a suicide attempt. This led to him being admitted to hospital where he was treated with neuroleptics and antidepressants.
Since his initial stay in hospital, Case A has been readmitted and continues as an outpatient. Three years on, after further in-patient and out-patient care, he was hopeful that the drug mafia may have realized – as a result of their intense surveillance – that they had been targeting an innocent man.
The three theory of mind tests used in the study included two sets of humorous cartoons, one of which involved ‘physical’ i.e. slapstick humour and the other of which required making inferences concerning mental states to get the joke. The second test involved interpretation of theory of mind narratives, and the third was designed to measure understanding of the meaning of hints. Case A scored 10/10 on the hinting task, 17/17 on the narratives, and 5/5 on each on the physical and theory of mind cartoon tasks. One of the theory of mind cartoons pictured a house with a sign at the front gate saying ‘Beware of the bog’ instead of the typical ‘Beware of the dog’. However, in the garden a man is in fact sinking in a bog. Case’s A’s explanation was: ‘“Beware of the bog” and he’s laughing because he thinks they’ve spelt it wrong.’
Analysis of Case A’s description of his persecution also revealed that he was able to make sophisticated ToM inferences concerning the mental states of others, specifically his pursuers:
-
1. They must think to themselves now they’ve made right plonkers [idiots] of themselves, mustn’t they? I’m not a supergrass...
-
2. When that happened they must have thought, ‘it’s that swine over there, he’s tipped them off, he’ll know’.
-
3. They must watch me twenty-four hours a day and think, ‘We know he’s a police informer, we think we know he is, but by God we’ve never seen him talk to the Police, or anything like that.’
Of course, the cognitive neuropsychological approach permits and even encourages thinking in terms of abnormalities that are not impairments. Frith (Reference Frith2004) himself acknowledged this in relation to theory of mind:
It is misleading to refer to the problem as a theory of mind deficit in the case of schizophrenia. A person who does not have a theory of mind takes no account of the beliefs and desires of other people when trying to understand their behaviour. Indeed, he may not have any concept of beliefs and desires. This may be the case in schizophrenic patients with predominantly negative features, but not in those with positive symptoms. The patient with paranoid delusions has no problem ascribing intentions to other people. His problem is that he ascribes the wrong intentions. He has a theory of mind since he explains the behaviour of others in terms of their intentions. The fault lies in the mechanism that is used to discover what these intentions are.
The problem is that very few studies have ventured into such territory. In a small study of 12 patients with persecutory delusions (8 with schizophrenia and 4 with affective disorder) and 10 without persecutory delusions (3 with schizophrenia and 7 with affective disorder), Blakemore et al. (Reference Blakemore, Sarfati, Bazin and Decety2003) found that the former group tended to read intentions into the movements of two abstract shapes that moved around a screen when there was nothing in the shapes’ movements to actually suggest this. In another, larger study (Montag et al., Reference Montag, Dziobek and Richter2011), 80 schizophrenic patients and 80 well-matched controls watched videotaped scenes of social interactions involving false belief, faux pas, metaphor or sarcasm. When asked about what had happened in the scenes, the patients made more errors than the controls, not only on probe questions that referred to a lack of awareness of the characters’ intentions, but also on questions where the wrong intentions were attributed to the actors. There was some evidence of an association between these latter ‘overmentalizing’ responses and delusions, but this was not robust (i.e. it disappeared when potential confounding factors were controlled for).
Into the Realm of Cognitive Psychology
For some aspects of cognitive function, trying to make an explicit link with particular parts of the brain is neither necessary nor desirable. Of course, like everything else these processes depend ultimately on brain function being intact, but they reflect the contribution of many different underlying systems. In the same way as for cognitive neuropsychological approaches but even more so, the concept of malfunction in such systems is freed from the straitjacket of loss of function: it now becomes relatively easy to think in terms of hyperfunction and the novel concept of biased function also begins to make an appearance. Three approaches to delusions stand out as being purely cognitive psychological in this sense. As it happens, they break down quite neatly according to the time period when they arose: the old if not particularly venerable tradition of disordered logic in schizophrenia, followed by Maher’s theory of the deluded patient as a naïve scientist, and finally the proposal that delusions are due to probabilistic reasoning bias, or ‘jumping to conclusions’ as it is popularly known.
Delusions = Disordered Logic
The possibility that delusions might be the result of a problem with logical reasoning was first formally proposed by Von Domarus (Reference von Domarus and Kasanin1944), in a somewhat whimsical article that seems to have been cited much more frequently than it has actually been read. After an introduction that took in the developmental theories of Vygotsky, the behaviour of an elephant in a zoo that wanted a piece of sugar from a visitor, and the role of mime in mute mentally handicapped patients, he went on to describe two schizophrenic patients who showed a peculiar disturbance of logic. The first believed that the number that 21 meant bathing station. His reasoning went as follows: 21 = 12, 12 means the twelfth month, and the twelfth month is the end of the year; one bathes at the end of the year, and the new year is no longer the old or the reverse of the old year. The second patient considered that Jesus, cigar boxes and sex were identical. Questioning revealed a link involving the idea of being encircled. Thus, the head of Jesus is encircled by a halo, a package of cigars is encircled by a tax band, and a woman ‘is encircled by the sex glance of a man’.
Von Domarus (Reference von Domarus and Kasanin1944) identified these two patients’ underlying problem as a failure of Aristotelian syllogistic reasoning. Thus, the syllogism ‘All men are mortal; Socrates is a man; therefore Socrates is mortal’ is true. In contrast ‘Certain Indians are swift; stags are swift; therefore certain Indians are stags’ is false. Some people (including the present author) might find it difficult to put their finger on just what the crucial difference between the two sets of propositions is, but the important point is that if there is a failure of logical reasoning in schizophrenia, delusions could plausibly be the result.
Over the next thirty years or so, chronically hospitalized schizophrenic patients across America found themselves being challenged with the kinds of logical problems shown in Box 5.2. Nearly all the studies (Gottesman & Chapman, Reference Gottesman and Chapman1960; Williams, Reference Williams1964; Coyle & Bernard, Reference Coyle and Bernard1965; Ho, Reference Ho1974) were carried out in the days before there were diagnostic criteria for schizophrenia. Nor was much consideration given to the possible confounding effects of general intellectual impairment on performance, although two of the studies did match the patients and controls for current IQ (Coyle et al., Reference Coyle and Bernard1965; Watson & Wold, Reference Watson and Wold1981). The results were not very encouraging: three studies found no significant difference from controls (Williams et al., Reference Williams1964; Coyle et al., Reference Coyle and Bernard1965; Watson et al., Reference Watson and Wold1981), and in the other two (Gottesman and Chapman, Reference Gottesman and Chapman1960; Ho, Reference Ho1974) differences were only found on some of the tests used.
Box 5.2 Examples of Logical Problems Used in Studies of Reasoning in Schizophrenia
All Tom’s ties are red.
Some of the things Ada is holding are red.
Therefore:
1. At least some of the things Ada is holding are Tom’s ties.
2. At least some of the things Ada is holding are not Tom’s ties.
3. None of these conclusions is proved.
4. None of the things Ada is holding are Tom’s ties.
5. All the things Ada is holding are Tom’s ties.
If some frogs are poetic, and some frogs are bullies, then:
1. All bullies are poetic.
2. Some poetic animals are not bullies.
3. No valid conclusion possible.
4. Some bullies are poetic.
5. Some poetic animals are bullies.
Two hundred students in their early teens voluntarily attended a recent weekend student conference in a Midwestern city. At this conference, the topics of race relations and means of achieving lasting world peace were discussed, because these were the problems the students selected as being most vital in today’s world. For each inference below respond true, probably true, insufficient data, probably false or false.
1. As a group, the students who attended this conference showed a keener interest in broad social problems than do most other students in their early teens.
2. The majority of the students had not previously discussed the conference topics in their schools.
3. The students came from all sections of the country.
4. The students discussed mainly labor relations problems.
5. Some teenage students felt it worthwhile to discuss problems of race relations and ways of achieving world peace.
If the radio is on, then there is no music.
(a) If the radio is not on, then there is no music.
(b) If the radio is on, then someone must be around.
(c) The radio is on, and there is no music.
(d) If there is music, then the radio is on.
(e) None of the above.
All dogs are animals. All animals eat. Therefore (choose one):
1. All animals are dogs.
2. All dogs eat.
3. Eating animals are dogs.
4. Only dogs eat.
What none of these studies investigated was whether logical reasoning impairment in schizophrenia was related to delusions. Years later this omission was rectified by Kemp et al. (Reference Kemp, Chua, McKenna and David1997). They examined 16 chronically psychotic patients who showed prominent delusions (according to DSM-III-R criteria 14 had schizophrenia, one had delusional disorder and one had atypical psychosis). They were all of average or above-average estimated premorbid IQ and none showed evidence of generalized intellectual impairment as measured, somewhat crudely, using the MMSE. They and 16 matched controls were given a series of syllogisms and conditional logical problems similar to those in Box 5.2. As in the study of Rossell et al. (Reference Rossell, Shapleske and David1998), some of the problems were also deliberately altered to make them emotional, touching on themes of religion, illness and violence. The authors also added a third form of reasoning test based on Tversky and Kahneman’s work on heuristics (see Chapter 4). This involved problems of the following type:
Linda is 31 years old, single, outspoken and very bright. She got a degree in philosophy. As a student she was deeply concerned with issues of discrimination and social justice, and also participated in antinuclear demonstrations. Linda:-
(a) is a bank clerk and is active in the feminist movement.
(b) is a plumber.
(c) is a bank clerk.
The correct answer is (c). Many people choose (a) although it is wrong, because by definition there are more women who are bank clerks than who are bank clerks and active in the feminist movement – the so-called conjunction fallacy. This test is notorious for its ability to induce incorrect responding, even among intelligent and sophisticated people (it is said, possibly apocryphally, that statisticians perform especially poorly on it).
The patients and controls were found to perform equally well on the syllogisms and conditionals, or rather equally badly since they both endorsed high numbers of wrong answers. There were some, although not very clear, suggestions of a pattern of worse performance by the patients on the emotional problems. In contrast, the deluded patients actually performed slightly better than the controls on the problems involving heuristics, in the sense of not being misled by the normal tendency to opt for the conjunction fallacy. Overall, the authors concluded that differences in reasoning between deluded patients and controls were surprisingly small.
The Deluded Patient as Naïve Scientist
In retrospect, the disordered logic theory never had much hope of being successful, for the simple reason that it essentially proposed that delusions were related to a cognitive deficit, albeit a rather esoteric one. This trap was avoided in the next historically important approach, which actually made a virtue out of intactness in a cognitive system. This was Maher’s (1974; Maher & Ross, 1984) proposal that delusions arise when processes fundamentally indistinguishable from those used by normal individuals to explain novel events are brought to bear on the abnormal perceptual experiences that occur in schizophrenia.
According to the theory, the process of delusion formation begins when a patient in the early stages of schizophrenia finds him- or herself having strange experiences. These experiences appear important, partly because they are new and mysterious, and partly because of the fact that they are often overwhelmingly intense. They demand an explanation, and this is achieved by a process of data collection and hypothesis testing which is similar in all important respects to the methods used in science. The process typically takes place in the following stages:
1. Initial observation: Unexpected or anomalous events create a feeling of significance in the observer that requires explanation.
2. Experience of puzzlement: The individual experiences a state describable as puzzled, curious, confused and surprised. This leads to first checking that the observation is actually what it seems to be and not something else, and secondly a search for other events that might be related to it. During this stage the individual begins to develop a tentative hypothesis about the event.
3. Additional observations: The state of puzzlement prompts a search for additional data. This may support the initial hypothesis, but if not it is rejected or amended, and the process is repeated until one hypothesis begins to gain ground.
4. The explanatory insight: Sooner or later the individual arrives at a point where the mystery seems to be solved – a kind of eureka moment where everything suddenly becomes clear. This has an emotional component, which may be marked (Maher and Ross (1984) quoted a biochemist who described the moment of scientific discovery as ‘a pure and primitive happiness deeper than anything of this kind which can ever be granted to a human being to experience’).
5. The process of confirmation: An explanation has now been arrived at, but its adequacy still needs to be tested. Although this might be expected to be an objective process, the reality is that once a firm conclusion has been reached it is likely to be held on to tenaciously in the way that normal beliefs tend to be, as described in Chapter 4. Another factor might be the belief’s quasi-scientific nature; Maher and Ross (1984) noted how important scientific discoveries are often rejected by the discoverer’s contempories before ultimately being hailed as works of genius.
The end result would be a propositional delusion. According to Maher (1974), the content of this – religious, political or quasi-scientific – would reflect the patient’s particular cultural background. Persecutory delusions might additionally arise as a result of the patients finding that other people do not seem to share their experiences, leading them to conclude that they are being lied to. Or they might decide that they are extraordinary because they have been selected to have experiences denied to others. Events in the patients’ own history could also play a part: a person who had a guilty secret might conclude that he or she was being punished for this.
For Maher the abnormal experiences that the patient needed to explain were principally a range of perceptual anomalies that occurred in the early stages of schizophrenia. He cited the case of Schreber, a judge who wrote about his own psychotic illness (in a book that later formed the basis of Freud’s psychoanalytic explanation of delusions): his initial symptoms were bodily sensations which ultimately led him to conclude that he was changing into a woman. In other cases it could be pains or the smelling of unpleasant odours. Maher also placed considerable emphasis on an alleged heightening of perception in the early stages of schizophrenia that had been described in a paper by McGhie and Chapman (Reference McGhie and Chapman1961).
An obvious difficulty for the naïve scientist theory is what happens when there no perceptual abnormalities of any kind, as can sometimes be the case in schizophrenia (and is the rule in delusional disorder). Maher and Ross (1984) got round this problem by proposing that in these circumstances there was a ‘central neuropathology’, which caused normal experiences to be imbued with a feeling of special significance; he explicitly identified the resulting state as delusional mood. The same hypothesis testing machinery could then be brought into play to produce an explanation for this experience.
Even with this patch, Maher’s theory faced problems. One was that it predicted that patients with full-blown hallucinations would always develop delusional explanations of them, something that is by no means always the case. It also predicted that non-psychotic individuals with conditions such as tinnitus and the phantom limb syndrome ought to develop delusions based on these experiences. Nothing of the kind has ever been described so far as the present author knows. Finally, it failed to explain why schizophrenic delusions tend to be bizarre or fantastic – an essentially normal hypothesis-testing process should produce explanations that incline to the mundane and plausible.
None of these problems is necessarily insurmountable, and it is possible that more sophisticated versions of Maher’s proposal could have found ways to deal with them. However, no such revised theory has ever been presented, something that probably reflects the fact that even the simple form of the theory has never been subjected to any kind of empirical testing. This does not mean, however, that it has not been influential. For example, it features in the integrative model of delusions proposed by a group of contemporary British researchers (Garety et al., Reference Garety, Kuipers, Fowler, Freeman and Bebbington2001; Freeman et al., Reference Freeman, Garety, Kuipers, Fowler and Bebbington2002; Freeman, Reference Freeman2007). Maher’s suggestions as to how propositional delusions can form out of abnormal significance and be coloured by the patient’s culture and life experiences also crop up again in the salience theory of delusions discussed in Chapter 8.
Probabilistic Reasoning Bias
The origins of the third cognitive approach to delusions go back to a theoretical paper by Hemsley and Garety (Reference Hemsley and Garety1986) in which they considered the question of whether delusions could be understood as an alteration in the way in people normally reach conclusions based on the balance of probabilities. Their argument was inspired by a mathematical treatment of such hypothetical processes using the principles of Bayesian inference (Fischhoff & Beyth-Marom, Reference Fischhoff and Beyth-Marom1983). They were also impressed by a study of patients with obsessive-compulsive disorder, which had found that they required more evidence than healthy controls to reach a decision in a task requiring judgement under uncertainty (Volans, Reference Volans1976). It seemed at least possible that patients with delusions might require less evidence than normal to do so.
Two years later Hemsley, Garety and co-workers published the results of a study designed to answer this question (Huq et al., Reference Huq, Garety and Hemsley1988). Fifteen schizophrenic patients with delusions, 10 patients with other psychiatric diagnoses and 15 healthy controls were shown two jars, one of which, the experimenter explained, contained 85 beads of one colour and 15 beads of a different colour, and the other of which contained beads in the reverse proportions. The containers were then hidden from view and the subjects were informed that beads would be drawn from one jar only, replaced, the jar shaken, another bead drawn, and so on, until they felt confident they knew which jar the beads were being taken from. (In fact, unknown to the subjects, the beads were always drawn in the same pre-arranged sequence that favoured a decision after several draws). The experimental design is summarized in Figure 5.2. As predicted, the schizophrenic patients were found to require significantly less draws to decision than both the healthy subjects and the psychiatric controls. Some of them reached a decision after only seeing one bead.
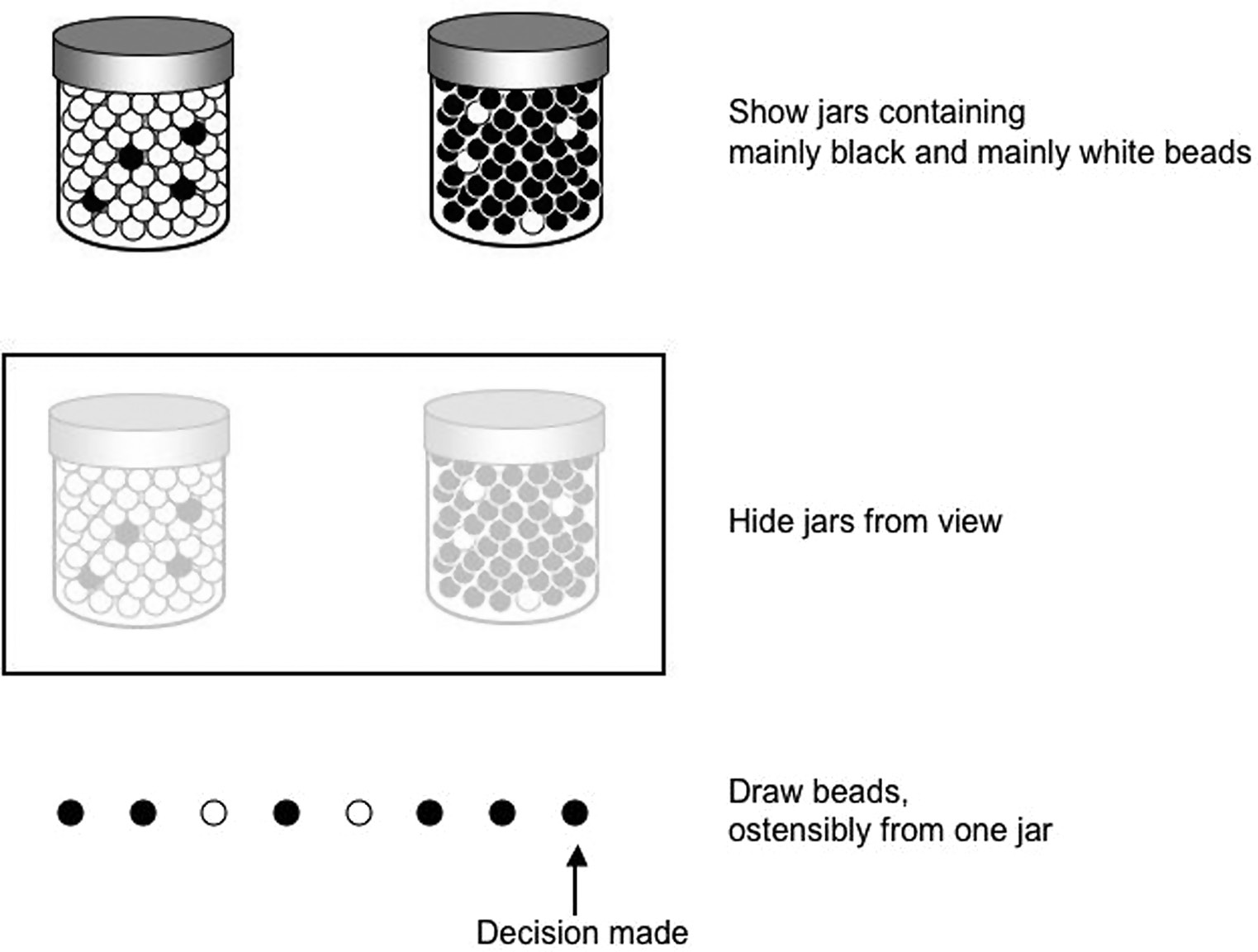
Figure 5.2 The probabilistic reasoning task.
Eleven years later, Garety and Freeman (Reference Garety and Freeman1999) reviewed this and seven more studies that had since been carried out. These studies all used the beads task, although sometimes in proportions such as 60:40 or 75:25, and one study also employed additional versions of the task designed to be either more realistic (deciding whether children’s names were from a ‘mainly boys’ or ‘mainly girls’ category) or more emotionally salient (deciding whether comments about people were from a ‘mainly positive’ or ‘mainly negative’ survey). All but one of the studies replicated the finding of ‘jumping to conclusions’ in schizophrenic patients. One study also found the effect in patients with delusional disorder.
Another ten years or so later, the same authors (Garety & Freeman, Reference Garety and Freeman2013) reviewed the literature again, by which time the number of studies had ballooned to nearly 70. Many studies continued to use beads, but by now there were a number of paradigms involving two kinds of fish, or words with both neutral and emotional content. The ratio of positive to negative findings was less favourable than in their earlier review, but the authors still found that a clear majority of studies found evidence for jumping to conclusions, with on average about half of patients with schizophrenia coming to a confident decision in two draws or less.
By this time, and bearing in mind the experience with theory of mind, the question on everyone’s lips was whether jumping to conclusions was a function of being deluded, or just of having schizophrenia. Garety and Freeman (Reference Garety and Freeman2013) felt that there was every reason to believe that the former was the case, pointing out that the larger studies usually found evidence of an association with delusions. The study they singled out in this respect, however, was less than reassuring: Lincoln et al. (Reference Lincoln, Ziegler, Mehl and Rief2010) examined 71 psychotic patients and found that draws to decision was not significantly correlated with any clinical variable in the easy 80:20 condition. There was a significant correlation with delusion scores in the harder 60:40 condition; however, when either negative symptoms or current IQ, which were also correlated with draws to decision, were controlled for in the analysis, the result became non-significant.
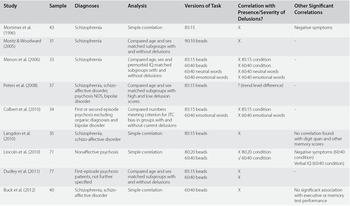
This and other studies examining the relationship between jumping to conclusions and delusions are shown in Table 5.3. Some of them compared matched groups of patients with and without delusions, whereas others took a correlational approach, or used multiple regression analysis which has the advantage of being able to remove the potential confounding effects of other variables also associated with delusions and/or draws to decision. It is clear that their findings are not nearly as supportive as Garety and Freeman (Reference Garety and Freeman2013) would like to believe. Most studies found no significant relationship with delusions. One study found a trend-level association and in two others there was a significant association in only one of the conditions used. A meta-analysis of these and a few other studies (e.g. imaging studies) from which data could be extracted (Dudley et al., Reference Dudley, Taylor, Wickham and Hutton2016) also found the pooled correlation between draws to decision and delusion scores to be insignificant at -0.09.
Table 5.3 Studies Examining the Relationship of Jumping to Conclusions to Delusions
| Study | Sample | Diagnoses | Analysis | Versions of Task | Correlation with Presence/Severity of Delusions? | Other Significant Correlations |
| Mortimer et al. (Reference Mortimer, Bentham and McKay1996) | 43 | Schizophrenia | Simple correlation | 85:15 | ✕ | Negative symptoms |
| Moritz & Woodward (Reference Moritz and Woodward2005) | 31 | Schizophrenia | Compared age and sex matched subgroups with and without delusions | 90:10 beads | ✕ | - |
| Menon et al. (Reference Menon, Pomarol-Clotet, McKenna and McCarthy2006) | 33 | Schizophrenia | Compared age, sex and premorbid IQ matched subgroups with and without delusions | 85:15 beads 60:40 beads 60:40 neutral words 60:40 emotional words |
✕ 85:15 condition ✕ 60:40 condition ✕ 60:40 neutral words ✕ 60:40 emotional words |
- |
| Peters et al. (Reference Peters, Thornton, Siksou, Linney and MacCabe2008) | 37 | Schizophrenia, schizo-affective disorder, psychosis NOS, bipolar disorder | Compared age and sex matched subgroups with high and low delusion scores | 85:15 beads | ? (trend level difference) | - |
| Colbert et al. (Reference Colbert, Peters and Garety2010) | 34 | First or second episode psychosis excluding organic diagnoses and bipolar disorder | Compared numbers meeting criterion for JTC bias in groups with and without current delusions | 85:15 beads 60:40 emotional words |
✕ 85:15 condition ✕ 60:40 emotional words |
- |
| Langdon et al. (Reference Langdon, Ward and Coltheart2010) | 35 | Schizophrenia, schizo-affective disorder |
Simple correlation | 85:15 beads | ✕ | No correlation found with digit span and other memory scores |
| Lincoln et al. (Reference Lincoln, Ziegler, Mehl and Rief2010) | 71 | Nonaffective psychosis | Simple correlation | 80:20 beads 60:40 beads |
✕ 80:20 condition ✓ 60:40 condition |
Negative symptoms (60:40 condition) Verbal IQ (60:40 condition) |
| Dudley et al. (Reference Dudley, Shaftoe and Cavanagh2011) | 77 | First-episode psychosis patients, not further specified | Compared age and sex matched subgroups with and without delusions | 85:15 beads 60:40 beads |
✕ ✕ |
- |
| Buck et al. (Reference Buck, Waramn, Huddy and Lysaker2012) | 40 | Schizophrenia, schizo-affective disorder | Simple correlation | 60:40 beads | ✕ | No significant association with executive or memory test performance |
| So et al. (Reference So, Freeman and Dunn2012)* | 273 | Schizophrenia, schizo-affective disorder, delusional disorder |
Simple correlation | 85:15 beads 60:40 beads 60:40 emotional words |
✕ 85:15 condition ✕ 60:40 condition ✕ emotional words |
- |
| Freeman et al. (Reference Freeman, Startup and Dunn2014) | 123 | Non-affective psychosis | Logistic regression | 60:40 beads | ✕ | Negative symptoms Current IQ Digit span Working memory |
| Ochoa et al. (Reference Ochoa, Haro and Huerta-Ramos2014) | 43 | Schizophrenia | Logistic regression | 85:15 beads 60:40 beads 60:40 emotional words |
✕ 85:15 condition ✕ 60:40 condition ✕ emotional words |
Significant associations with 2 out of 14 neuropsychological measures, not consistent across beads/words conditions |
| Falcone et al. (Reference Falcone, Murray and Wiffen2015) | 108 | First-episode psychosis, one-third with affective diagnoses | Logistic regression | 85:15 beads 60:40 beads |
✓ 85:15 condition ✕ 60:40 condition |
Current IQ Spatial working memory |
* Includes patients from study of Garety et al. (Reference Garety, Joyce and Jolley2013)
What Table 5.3 does reveal are hints that jumping to conclusions is associated with negative symptoms and poor performance on neuropsychological tests. The latter finding, in particular, raises the possibility that probabilistic reasoning bias may not be a bias at all, but instead a cognitive deficit. Further support for this interpretation comes from a study by Lunt et al. (Reference Lunt, Bramham and Morris2012), which gave the beads task to 19 neurological patients with frontal lobe lesions. The patients were found to show significantly reduced draws to decision comparedto 25 healthy controls, and this was associated with poor performance on some but not all of a range of measures of executive functioning also administered as part of the study.
Conclusion: Can Anything Be Salvaged from the Wreckage?
In many ways, a psychological theory of delusions seems as far away as it must have done half a century ago when the first tentative steps in this direction were being taken. The theories themselves are not particularly powerful: only one of them has had anything to say about referential delusions and none of them provide an explanation of why propositional delusions show the typical features of being fixed, incorrigible, bizarre or even fantastic. None of the theories have emerged unscathed from empirical testing, and several of them, it has to be said, have not stood up to it very well at all.
One avenue that seems closed forever is the idea of delusions being due to a cognitive deficit. This applies not just to neuropsychological deficits – including the perennial favourite of schizophrenia research, executive function – but also it seems to any other kind of cognitive disturbance that can be conceptualized in such a way. If such a deficit did exist it would have to be one that (a) is currently unknown and (b) is spared by the general tendency to intellectual impairment that also characterizes schizophrenia. What makes this conclusion especially harsh is that it brings down with it an ingenious and much-loved theoretical approach to delusions, theory of mind impairment. Probabilistic reasoning bias may be another casualty here: its association with neuropsychological test impairment in schizophrenia and the fact that it is also seen in patients with frontal lobe lesions make it look suspiciously like a deficit in disguise.
Cognitive neuropsychiatry offers a potential way out of this impasse. Semantic memory is a plausible place to look for a non-deficit abnormality, if for no other reason than the fact that delusions seem to reside in one particular subdivision of this, personal semantic memory. Nevertheless, in terms of experimental support, the semantic memory theory of delusions hangs by the slenderest of threads – faint signals of altered factual knowledge in areas related to delusions in Rossell et al.’s (Reference Rossell, Shapleske and David1998) study, and suggestions of something not too dissimilar from the single case study of Laws et al. (Reference Laws, McKenna and McCarthy1995). Even if semantic memory is affected, there is no real idea of what form the disturbance might take – disorganization of the network architecture? an excessive tendency to lay down semantic memories? – all possibilities seem to lie deep in the realm of speculation. An ‘overmentalizing’ form of theory of mind dysfunction could also work, but the same theoretical reservations apply, and the almost complete lack of studies investigating this possibility does not inspire confidence.
Maher’s theory remains untested. Patients with schizophrenia have no more problems with logical reasoning than anyone else, and the hints from Kemp et al.’s (Reference Kemp, Chua, McKenna and David1997) study that something more than this is going on are if anything slighter than in the case of semantic memory. Probabilistic reasoning bias is not convincingly associated with presence of delusions. The only remaining candidate for a psychological theory of delusions is the third cognitive neuropsychological approach alluded to at the beginning of the chapter, whose starting point is the occurrence of delusion-like phenomena in neurological disease. Whether this approach can succeed where others have failed, and whether it can get round the problem that deficits are not associated with delusions in psychiatric disorders, is examined in Chapter 7. But before doing so a whole different approach to delusions needs to be considered.