



Background
Dementia is a global issue and is described by the World Health Organization (WHO) as a syndrome in which cognitive function deteriorates at a rate faster than would be expected as consequence of ‘normal’ ageing (WHO, 2022). There are many such causes of the dementia syndrome and in Western countries, Alzheimer's disease is the most common, followed by vascular dementia and mixed dementia (WHO, 2022). Whilst dementia is sometimes diagnosed in mid-life, the risk of developing the symptoms of dementia is closely associated with increasing and advanced old age with one in four people over the age of 80 living with the condition (Alzheimer's Society, 2014). Presently, 55 million people are living with dementia worldwide and this is projected to increase to 78 million by 2030 (Alzheimer's Disease International, 2021). In the United Kingdom (UK), it is estimated that around 1 million people live with a dementia, with that figure set to rise to 1.2 million by the year 2040 (Livingston et al., Reference Livingston, Huntley J, Sommerlad, Ames, Ballard, Banerjee, Brayne, Burns, Cohen-Mansfield, Cooper, Costafreda, Dias, Fox, Gitlin, Howard, Kales, Kivimäki, Larson, Ogunniyi, Orgeta, Ritchie, Rockwood, Sampson, Samus, Schneider, Selbæk, Teri and Mukadam2020). Typically, post-diagnostic life expectancy is estimated at 2.9–8.0 years for women (median = 5.1 years) and 2.3–7.0 years for men (median = 4.3 years) (Haaksma et al., Reference Haaksma, Eriksdotter, Rizzuto, Leoutsakos, Olde Rikkert, Melis and Garcia-Ptacek2020), with these authors highlighting that this life expectancy will be dependent upon several contextual factors, including age of onset, stage of dementia and the presence of any co-existing co-morbid condition(s), such as cardio-vascular problems, stroke and cancer.
As a syndrome, dementia is usually described as transitioning through early, middle and late/advanced stages (WHO, 2016), with the weight of public, social policy and biopsychosocial research aimed at the early stages of the condition where there is an opportunity to maximise and extend personal choice(s) and decision-making. It is here where the public narrative of ‘living well with dementia’ is mainly located (for a review, see Martyr et al., Reference Martyr, Nelis, Quinn, Wu, Lamont, Henderson, Clarke, Hindle, Thom, Jones, Morris, Rusted, Victor and Clare2018) although, of course, it is possible to live well with dementia throughout the trajectory of the experience with recent attention focused on the importance of dying well (Mamun et al., Reference Mamun, Hirakawa, Saif-Ur-Rahman, Hong, Song, Yoshida and Yatsuya2023). That said, people living through the moderate to late/advanced stages of dementia are more likely to experience a progressive decline in memory, cognitive function, emotional stability and behaviour, such as expressed through excessive walking, unpredictable aggressive acts, intrusiveness and disproportionate vocalisation (James and Jackman, Reference James and Jackman2017; Jones et al., Reference Jones, Cullum, Watson and Keady2023a). As Wolverson et al. (Reference Wolverson, Dunn, Moniz-Cook, Gove and Diaz-Ponce2021) point out, these occurrences have many different language descriptions in both the literature and practice, such as ‘behaviours that challenge’, ‘changed behaviour’, ‘behaviours of concern’ and ‘behavioural and psychological symptoms of dementia’, with the latter terminology adopted in the most recent dementia guideline by the National Institute for Health and Care Excellence (NICE, 2018: 8). However, these linguistic descriptions seemingly put the focus on the person living with dementia rather than on aspects of the person's physical, social or psychological environment that may stimulate such behaviours and, as such, the terminology of ‘unmet need(s)’ has been put forward as a more person-centred way of interpreting such life events (Cohen-Mansfield et al., Reference Cohen-Mansfield, Dakheel-Ali, Marx, Thein and Regier2015; Wolverson et al., Reference Wolverson, Dunn, Moniz-Cook, Gove and Diaz-Ponce2021); a terminology we will also adopt in this article.
Around 90 per cent of people living with dementia will experience behaviours of concern caused by some degree of unmet need(s) during their condition (Keady and Jones, Reference Keady and Jones2010; NICE, 2018). This occurrence, coupled to the risk that is posed to others, and/or to the person themselves, is often seen as a trigger for a range of outcomes to occur, such as: increasing the home-based social and health-care support to the person living with dementia and any family carer(s); conducting more frequent risk assessments at home, especially if the person with dementia lives alone; predicting the breakdown of a domestic care-giving relationship; seeking care home admission for the person living with dementia; and conducting further mental health assessments about the cause of the exhibited unmet needs in the person living with dementia (see James and Jackman, Reference James and Jackman2017; NICE, 2018; James et al., Reference James, Mahesh, Duffy, Reichelt and Moniz-Cook2021; Odzakovic et al., Reference Odzakovic, Kullberg, Hellström, Clark, Campbell, Manji, Rummery, Keady and Ward2021; Jones et al., Reference Jones, Cullum, Watson and Keady2023a, Reference Jones, Cullum, Watson and Keady2023b). In the UK, depending on a risk assessment and the person living with dementia's capacity to consent, this latter situation will usually see the person living with dementia compulsorily admitted to a National Health Service (NHS) psychiatric/mental health inpatient dementia assessment ward (dementia assessment ward hereafter) under an appropriate section of the Mental Health Act (Department of Health, 1983) to allow for further assessment and treatment to take place.
As the previous paragraph implies, in the UK, dementia assessment wards are hospital-based services usually provided by NHS Mental Health Trusts for mainly, but not exclusively, older people with care provided in wards by mental health professionals, such as psychiatrists, mental health nurses, clinical psychologists, psychiatric social workers, occupational therapists and health-care support workers (Wolverson et al., Reference Wolverson, Dunning, Crowther, Russell and Underwood2022). Staff surveys indicate that registered mental health nurses and health-care support workers are the largest professional staff groups working on dementia assessment wards (Edmans et al., Reference Edmans, Wolverson, Dunning, Slann, Russell, Crowther, Hall, Yates, Albert and Underwood2022). In service design terms, dementia assessment wards are usually locked environments (i.e. entry to, and access from, the ward is secured) and they can be structured either as a ‘dementia-only’ ward environment or as a ‘mixed’ ward environment where older patients with functional mental health conditions, such as late-life depression, may also be receiving assessment and treatment (Jones et al., Reference Jones, Cullum, Watson and Keady2023a, Reference Jones, Cullum, Watson and Keady2023b). Some time ago, the Royal College of Psychiatrists (2006) called admission to a dementia assessment ward ‘a last resort’ to symbolise when all other options to keep people living with dementia at home, including in care homes or other supported living arrangements, have failed and more intensive and specialist support and assessment is necessary to better understand what is being experienced.
Nevertheless, once admitted to a dementia assessment ward, the literature to both describe and support practice is surprisingly sparse, with most studies sharing the results of evaluations and/or audits conducted on the ward rather than the findings of primary research per se (Wolverson et al., Reference Wolverson, Dunning, Crowther, Russell and Underwood2022). As an illustration, Edmans et al. (Reference Edmans, Wolverson, Dunning, Slann, Russell, Crowther, Hall, Yates, Albert and Underwood2022) conducted a multi-centre retrospective service evaluation of dementia assessment ward practice using routinely collected data from four diverse sites in the UK. In reporting their analysis, Edmans et al. (Reference Edmans, Wolverson, Dunning, Slann, Russell, Crowther, Hall, Yates, Albert and Underwood2022: 3) found that inpatient assessments were lengthy, with a mean duration of 100 days, and that assaults on staff were reported around once every two days which was ‘higher than for UK prison officers’. In relation to practice-based research, Jones et al. (Reference Jones, Cullum, Watson and Keady2023a, Reference Jones, Cullum, Watson and Keady2023b) conducted a multi-methods study on two dementia assessment wards in the North of England and suggested that a narrative of complexity framed everyday clinical practice and the presentation of people living with dementia on these wards. This finding echoed the earlier work of McGeorge (Reference McGeorge2010) and Ross and Dexter-Smith (Reference Ross and Dexter-Smith2017), as well as reports by the Royal College of Psychiatrists (2006, 2015). Recently, Wolverson et al. (Reference Wolverson, Dening, Dunning, Crowther, Russell and Underwood2023) conducted a qualitative study that interpreted the family carer's experience of being a visitor to the ward. Wolverson et al. (Reference Wolverson, Dening, Dunning, Crowther, Russell and Underwood2023) found this to be a largely negative experience where carers struggled with feelings of stress and guilt over the compulsory admission, and they suggested that carers would themselves benefit from therapeutic intervention during the period of admission.
Taking an alternative research design standpoint, Schneider (Reference Schneider2017) worked alongside health-care support workers on a dementia assessment ward to develop a play that interpreted and performed caring practices experienced in these environments. Public performances of the play then helped to raise the profile and visibility of the dementia assessment ward, whilst also giving voice to the caring skills of this staff group. This more performance-based view of care starts to dovetail into the field of care aesthetics and a more ‘in the moment’ frame of understanding a caring dynamic and interactive process (Keady et al., Reference Keady, Campbell, Clark, Dowlen, Elvish, Jones, Kindell, Swarbrick and Williams2022; Thompson, Reference Thompson2022). In developing his theory and approach to care aesthetics, Thompson (Reference Thompson2022) proposes that it draws on the fields of everyday aesthetics (Saito, Reference Saito2008, Reference Saito2017), which analyses the importance of everyday heightened sensory and emotional experiences for making meaning in people's lives, and relational aesthetics (Bourriaud, Reference Bourriaud2002), an idea taken from contemporary arts which argues that human relations have an aesthetic quality that is adaptable and refinable. In aesthetic theory there has been a move away from a sole reliance on distal senses to evaluate the quality of an experience (e.g. sight or the visual) to combine proximal and distal senses in a more fully rounded analysis (see Shusterman, Reference Shusterman2012). Therefore, care aesthetics is not just an acknowledgement of the appearance of care, as a proxy for its quality, but an account of how it involves all senses, including touch, hearing, movement and taste. Thompson (Reference Thompson2022) goes on to suggest that the care moment is one made of interconnected embodied practices that combine to create the resulting sensory experience. As such, the care moment comprises the actions of all present at that moment in time and how these are situated to the wider environment. This includes the interaction of different materials, how a space is organised and the physical activities that combine to create an atmosphere in a health, social care or community-based setting, including, in this context, the dementia assessment ward.
Care aesthetics therefore does not seek an artificial ‘artistic’ reading of care but aims to point to the sensory register that is already at play in a claim that attention to this helps focus on elements of care vital to its person-centred quality which are too rarely fully acknowledged (Thompson, Reference Thompson2022). These sensory and embodied actions were evident in a study by Buse and Twigg (Reference Buse and Twigg2018) exploring dressing in the context of dementia care. Their research exploring the ‘dilemmas and tensions regarding the visibility and aesthetics of care’ noted the importance of ‘relational and processual elements’ (Buse and Twigg, Reference Buse and Twigg2018: 349) in person-centred care and echoes the attention to ‘one-to-one interaction, sensory engagement’ (Buse and Twigg, Reference Buse and Twigg2018: 350) proposed in this article. Similarly the research of Ward et al. (Reference Ward, Campbell and Keady2016a, Reference Ward, Campbell and Keady2016b) on hair dressing in dementia care settings, including on the dementia assessment ward, used, we would argue, an implicitly sensory aesthetic register in its close analysis of interpersonal care work. These authors' description of the ‘theatre of body work’ (Ward et al., Reference Ward, Campbell and Keady2016a: 1292) overlaps with the focus on the aesthetics of care and their discussion of the relationship between ‘looking good’ and ‘feeling good’ (Ward et al., Reference Ward, Campbell and Keady2016b: 406) demonstrates the importance of the interactions between different (proximal and distal) sensory registers for understanding the dynamics of care practices.
To help commence a body of work using care aesthetics as an overarching explanatory lens in dementia studies, this study reports on a single case study taken from a larger dataset with the aim of providing a more in-depth and summative understanding about the experience of being a patient on a dementia assessment ward. This understanding is contextualised with the contribution of stakeholders involved in that person's care and support. Data were collected by a highly experienced mental health nurse and Advanced Nurse Practitioner (ANP), LJ, who, at the time of data collection, in 2018, had over 20 years' experience in working frontline on a dementia assessment ward, including time as a ward manager. For clarification, an ANP is a registered nurse who is educated at Masters Level in clinical practice and assessed as competent in practice using their expert clinical knowledge and skills, including, in LJ's case, being an independent prescriber.
Methods
Study design and setting
The authors refer to a previous publication ‘Introducing the “3Fs Model of Complexity” for people with dementia accessing an NHS mental health in-patient dementia assessment ward: an interpretive description study’ by Jones et al. (Reference Jones, Cullum, Watson and Keady2023a). Drawing on the involvement of several UK-based stakeholders, this first article reported on the full three phases of a one-year, mixed-methods, interpretive description study (Thorne, Reference Thorne2008) that addressed the original research question, namely to explore the meaning and construction of complexity as experienced by people living with dementia admitted to a dementia assessment ward. In this first paper, the three ‘Fs’ in the generated practice model stood for ‘Fixed’, ‘Flexible’ and ‘Fluctuating’ domains of complexity (Jones et al., Reference Jones, Cullum, Watson and Keady2023a) and contained supplemental material drawn from each phase of the study design which fleshed out the components, practice relevance and meaning of each domain. This current paper focuses on the phase three data of the larger study which used a range of qualitative methods to report on the experiences of four people living with dementia admitted to the recruited dementia assessment ward; all participants at this phase of the study were compulsorily detained on a section of the Mental Health Act (Department of Health, 1983). As indicated by Sally Thorne (Reference Thorne2008, Reference Thorne and Leavy2014), incorporating a case study within the practice-based methodology of interpretive description is seen as being particularly useful in ‘getting under the skin’ of a poorly described clinical area and making visible existing care practices. However, before we develop the study methods further, we will first outline the location and context of the recruited dementia assessment ward.
Jasmine Ward
This study took place on Jasmine Ward (not its real name), a dementia assessment ward situated in a community hospital in the North of England.Footnote 1 Jasmine Ward is part of a large NHS Mental Health Trust and provides assessment, care and treatment for people living with dementia from a defined regional catchment area. At the time of the study, Jasmine Ward was an 18-bedded mixed-sex ward for people living with dementia requiring assessment for their dementia. The catchment area for Jasmine Ward was mainly drawn from an urban population with large pockets of deprivation and ethnic diversity. The average length of stay on Jasmine Ward was 160 days although at the time of conducting the study in 2018, some patients on the ward had been resident for considerably longer than this.
Jasmine Ward had a multi-disciplinary team which was comprised of a ward manager, two deputy ward managers, staff nurses, health-care support workers, an occupational therapist, an occupational therapy assistant, and two consultant psychiatrists and their junior doctors. At the time of data collection, there was also a senior nurse practitioner, physical health nurse, assistant practitioner, physiotherapist, physiotherapy assistants and psychology input. The ward was overseen by a matron. In addition, several ‘bank’ and ‘agency staff’ were regularly employed on each shift to deal with the fluctuating needs of the patients on Jasmine Ward. Depending on numbers of patients and their acuity, ward staff numbers ranged from six to nine in the morning and four to eight in the afternoon and at night.
Hand drawn by LJ at the time of her periods of observation, Figure 1 shares the main layout and day area of Jasmine Ward and where the periods of observation took place.
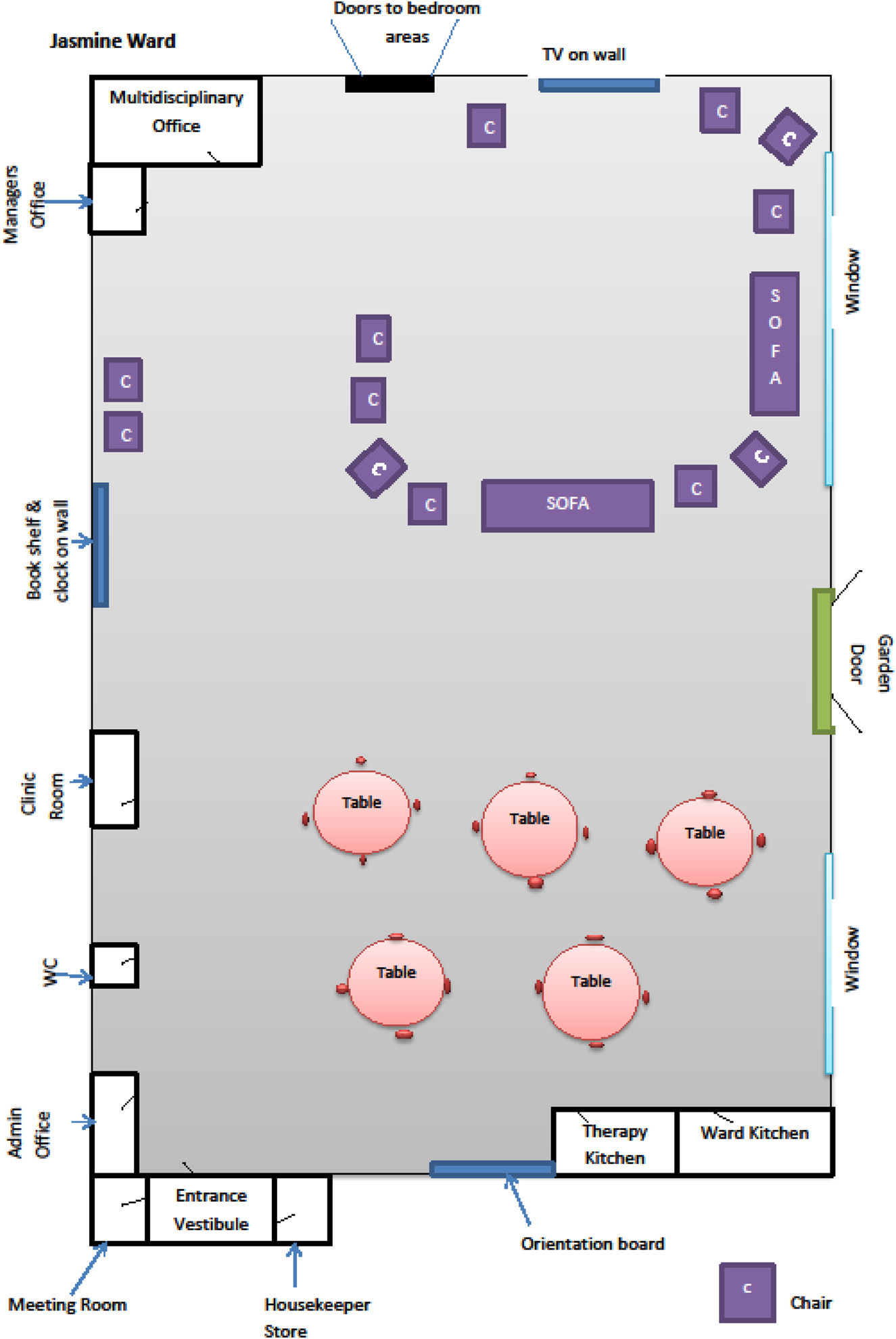
Figure 1. Layout of Jasmine Ward day area.
Jasmine Ward was a secured and locked care environment, and it was entered by ringing a bell on the outside door to alert ward staff on the inside of the ward to unlock the entrance door. Access to, or exit from, Jasmine Ward was not possible without following these procedures. All patients on Jasmine Ward were formally detained under a section of the Mental Health Act (Department of Health, 1983) and throughout the period of data collection, Jasmine Ward ran at maximum capacity.
Recruitment
One of the challenges we faced in conducting research on a dementia assessment ward was that these are areas that have been routinely excluded from research attention (Wolverson et al., Reference Wolverson, Dunning, Crowther, Russell and Underwood2022) and this is probably because they are seen as hard to reach. From our experience in setting up this study, it was important to build in a long lead-in time to the research planning phase of the study. For example, before any research design writing was attempted, we spent time in gaining the trust of the ward staff and other key stakeholders, such as the ward managers, and making certain that staff were clear about the study intentions. This included an opportunity for ward staff to ask questions about the proposed research and feel invested in its outcomes. In our case, it was perhaps helpful that the lead researcher and first author was also a mental health nurse and ANP, but this level of experience and exposure to clinical practice should not be seen as a prerequisite for conducting this type of work in this specific setting.
In this nested case study (Schwandt and Gates, Reference Schwandt, Gates, Denzin and Lincoln2018), the sample consisted of a person living with dementia resident on Jasmine Ward, their visiting family carer, the named clinician on the ward involved in that person's care and a care record review. The inclusion criteria for people living with dementia resident on Jasmine Ward to be approached about participation in the study were threefold, namely: (a) they had been an inpatient for a minimum of five days; (b) the care team had to have commenced their assessment and care interventions at the time of recruitment; and (c) the person living with dementia was regarded as ‘complex’ in their presentation by the care staff. Consent was obtained to both observe and interview people living with dementia about their feelings/experiences of being on Jasmine Ward.
As shared, four people living with dementia on Jasmine Ward were consented into this phase of the study together with their main family carer and the named clinician responsible for their care. Of these four participants, Charlotte has been selected by the authorship to be the focus of this more detailed case study owing to her complex presentation and the practice and professional learning that could be accrued by further exploring her lived experience. Charlotte was assessed as lacking the capacity to consent and therefore required personal consultee consent to take part in the study, in line with the Mental Capacity Act (Department of Health, 2005) and the study protocol. Charlotte's personal consultee was her husband, Harry, who also consented to be interviewed as part of the study. In the event, owing to the complex presentation of Charlotte, it was not possible to interview her about being a patient on Jasmine Ward. However, Charlotte's involvement is represented in the article via a series of time-stamped observations made by LJ, and in the prefix to the article title which is our interpretation of her lived experience on Jasmine Ward.
Data collection
Data collected about Charlotte's experience on Jasmine Ward consisted of: (a) eight periods of observation on Charlotte over a two-month period totalling 7 hours 55 minutes (shortest observation period 30 minutes, longest 1 hour 5 minutes); (b) an interview with Harry; (c) an interview with Charlotte's named nurse Linda; and (d) a review of Charlotte's care record. LJ undertook all the observations and approached these observations in a way that was minimally disruptive to everyday activities on Jasmine Ward. For example, all interviews were undertaken in the ward day area (see Figure 1) and to protect Charlotte's dignity, a decision was made not to undertake observations during the provision of direct care which required privacy, e.g. washing, dressing, bathing and using the toilet. In addition, prior to undertaking any period of observation, permission was gained from the ward team and from Harry, as Charlotte's personal consultee. All staff on Jasmine Ward received ongoing study awareness-raising sessions by LJ about what the observations would entail and their purpose. Field notes were captured in a notebook as events happened in real time or were reflected upon shortly after the event. All notebook entries were dated and used as data. Permission was also granted to undertake a care record review so that a documentary analysis of Charlotte's clinical notes could form part of the developed case study.
Data analysis
Analysis of the dataset was informed by a combination of sensory ethnography (Pink, Reference Pink2009), interpretive description (Thorne, Reference Thorne and Leavy2014) – to focus on the practice aspects of the study and its reporting – and narrative analysis using the guiding framework suggested by Hunter and Emerald (Reference Hunter and Emerald2016). This guiding framework distils the narrative research process into three distinct research moments, namely: (a) field texts; (b) interim research texts; and (c) research texts. Here, the first research moment of ‘field texts’ refers to the collection and collation of all data on the study, including, in the context of our work together, the sensory and reflective notes collected by LJ on Charlotte's actions and interactions on Jasmine Ward. This activity created a large dataset which was used to inform the second research moment of ‘interim research texts’.
In Hunter and Emerald's (Reference Hunter and Emerald2016) guiding framework, this second research moment is the ‘doing’ of narrative analysis and was initially a shared enterprise between two members of the authorship, LJ and JK, who separately read through the study transcripts, reflective notes and care record. As our intention was to produce separate narrative accounts of each of the four data strands (i.e. Charlotte's observation data including LJ's reflective notes, interview with Harry, interview with Linda and care records review), and then present them as a descriptive and storied account told from different perspectives, the dataset was individually collated under each of these four data strands. Thorne (Reference Thorne and Beck2013) discourages the use of any data sorting software and we therefore worked manually with the individually collated transcripts and/or copies of the care record using ‘post-it’ notes and other textual markers, such as different coloured highlighter pens, to begin to find storylines and connections within each data strand.
At this point in the narrative analysis, LJ and JK held joint meetings over several months to constantly apply the questions ‘why is this here?’, ‘why not something else?’, ‘what does this mean?’ to the individual dataset(s) until a descriptive and storied ‘truth claim’ (Thorne, Reference Thorne and Leavy2014: 107) emerged. This constant ‘pushing and pulling’ of the data was regularly shared with the remaining members of the authorship, and the study advisory group, who acted as a sounding board to test and agree the meaning and representativeness of the ongoing, and then agreed, storied accounts. For clarification, the study advisory group was established during the length of the project and consisted of two registered mental health nurses with experience of dementia assessment wards, a clinical psychologist, two old-age consultant psychiatrists, a person living with dementia, a previous carer who has cared for her husband and father-in-law with dementia, and a volunteer co-ordinator with extensive experience of supporting people living with dementia to become involved in developments and research.
Finally, in Hunter and Emerald's (Reference Hunter and Emerald2016) guiding framework, the third research moment is ‘research texts’ and this refers to the dissemination of the research which, in our case, relates to the meaning, experience and practice of Charlotte's presentation of complexity whilst being a patient on Jasmine Ward. In sharing Charlotte's experience, and in keeping with this aspect of the study design, this storied ‘truth claim’ will be presented both sequentially and descriptively, and told from the narrative position of each participant who took part in the research, starting with Charlotte, with space at the end for a section on the care record review.
Ethical approval
Ethical approval to conduct this study was obtained from North West Haydock NHS Research Ethics Committee. All data, including the ward name as indicated previously, are anonymised in this article in line with the study protocol and all participants consented to take part. In phase three of the study, where concerns were expressed about an individual's capacity to consent, the consent process was carried out following the Mental Capacity Act (Department of Health, 2005) and inviting a relevant consultee to consider providing consent on behalf of the identified participant. In this study, and as previously highlighted, Harry, as Charlotte's husband and personal consultee (i.e. the person who advised the research team on what Charlotte would have wanted to do before she lost capacity), gave consent to report on the observations of his wife in the public areas of Jasmine Ward and chose her assigned pseudonym. The sensitive nature of the data collection resulted in an ongoing discussion with Harry over what data could, and could not, be shared in the reporting of the research process and how this was to be framed. This article is respectful of this consultation.
We also need to say that the documentation necessary to gain Health Research Authority (HRA) ethical approval to conduct the study in an NHS dementia assessment ward was an extensive and lengthy process, especially as we wanted to include people living with dementia who were sectioned under the Mental Health Act (Department of Health, 1983) and whose capacity to consent was highly likely to be compromised. For future researchers intending to develop research on a dementia assessment ward, key learning points from our study were twofold: first, to make sure that time and relationship-building are central to developing and shaping the research protocol and accompanying documentation for the HRA ethics submission; and second, to allow significant time for relatives to agree to act as a personal consultee. This was because relatives wanted to share their own life story as well as their experiences of being alongside the person living with dementia, and perhaps more importantly in this context, their life and time together before dementia became an ever-present feature. Going forward, respecting and valuing the ‘personal’ in the ‘personal consultee’ terminology should not be underestimated.
Findings
About Charlotte
Charlotte is 71 years of age, married and has a son. She was diagnosed with young onset Alzheimer's disease when she was 64 years old. Charlotte had initially been admitted to an acute hospital ward following an adverse reaction to a medication that she had been taking at home and which had caused her to stop mobilising. However, for the two weeks that she had been an inpatient on the acute hospital ward, nursing staff had expressed concerns over her behaviour and their inability to manage it; a psychiatric assessment was therefore requested and performed. Following this assessment, Charlotte was compulsorily admitted to Jasmine Ward on section 2 (28 days) of the Mental Health Act (Department of Health, 1983) for assessment, a section that was later regraded to a section 3 (six months' detention order for assessment and treatment which can be renewed) whilst on Jasmine Ward.
Prior to her hospital admissions, Charlotte had been living at home with Harry, her husband, who was her main carer. On initial contact with LJ, Charlotte had been a resident on Jasmine Ward for four months. Charlotte appeared to be in good physical health and whilst she had previously been a smoker, she had stopped this habit three years prior to her acute hospital admission. A recent blood test had identified that Charlotte had raised calcium levels, but this did not require treatment. Charlotte was prescribed several regular and pro re nata (PRN; i.e. as required) medications, with the PRN medication including the anxiolytic Lorazepam (Ativan®).
Whilst on Jasmine Ward, and throughout the two months period of observation, Charlotte was visited by her husband, son, brother and uncle.
Charlotte's admission to Jasmine Ward: observations
The following three examples from LJ's field notes are shared to represent the diversity of Charlotte's everyday life on Jasmine Ward and pointers towards practice and professional learning. The field notes were taken on different days and contain personal pronouns that relate to LJ.
Example 1: ‘Love and pie’
A Monday afternoon in early November
14:04: There are 16 patients on Jasmine Ward and three of these are on continuous observations (i.e. are always being watched by designated members of the ward staff because of the assessed level of risk). The doorbell to the ward rings. A member of staff lets in some visitors; it is Harry and Charlotte's brother. Charlotte recognises them immediately and she gets up and walks towards them. She has a big smile as they are moving towards each other. Harry hugs her and they walk out of the day area holding hands.
14:15: Charlotte is in the lounge with her family. She is sitting in one of the armchairs and her brother is in another. Harry has pulled up a chair and is sitting on it directly in front of Charlotte. He is very close to her, and his legs are positioned either side of her legs. Charlotte appears calm and is smiling at Harry. Harry opens a small flask and takes out a bag with a pie in it. He breaks off a piece of pie and puts it to her mouth. He tells Charlotte to take a bite. He also rubs her cheek and calls her ‘chuck’. Charlotte accepts the piece of pie and starts chewing slowly. All the while her gaze has not left Harry's face.
14:30–15:00: Charlotte, Harry and her brother remain in the lounge. Harry has stayed in the same position and, very slowly, Charlotte has accepted a pie and a hot drink from him. She continues to look relaxed and content in their company. Occasionally, Harry and Charlotte's brother break away from being with Charlotte and they start to chat to one another. However, when they do this, they always include Charlotte in the exchange and periodically, Charlotte will look at her brother and smile. Whenever Charlotte verbally interacts with any of the visiting family, Harry immediately responds with a word to her or reaches out to touch her face, stroke her hair, kiss her face or use a pet name for her. It is very humbling to see.
Example 2: ‘Biscuits and medals’
A Wednesday morning in early December
11:00: There are six staff on duty, two of whom are qualified. The ward is full and I am sitting in a corner of the lounge area. Charlotte is wearing a skirt, t-shirt and slippers and she is sitting in a chair in the lounge. Occasionally, she will speak out loudly. It is usually one or two words, and they are difficult to make out. Charlotte looks at me and smiles. She continues to look around the ward, watching.
11:15: The ward doorbell rings and two paramedics, a nurse and a female patient in a wheelchair turn up. It is a new admission. The staff nurse and physiotherapist greet the new patient and help her to sit in a chair in the lounge. They offer her a drink. The new admission sits in a chair opposite Charlotte. Charlotte is intently watching the staff talking to the new admission and suddenly she laughs out loud and noisily.
11:25: Charlotte leans forward and stretches her arm out to pick up a cup of tea which is near her. It is not hers. It was left there untouched by another patient a while ago. I wonder if it is still warm. The agency health-care support worker hands it to Charlotte and she takes the cup from him. The health-care support worker tries to guide the cup to Charlotte's mouth, but she moves away by leaning back in the chair. The health-care support worker asks her what she has been doing this morning. Charlotte does not answer.
11:27: Christmas carols are now being played on the music system in the lounge. A female health-care support worker who has come into the day area jokes with Charlotte and asks if she has a feather. Charlotte responds by saying ‘I have no medal!’ I can see that the health-care support worker has a file and is writing in it. She tells Charlotte that she is doing the register; in effect, it is a location list for all patients on Jasmine Ward to make sure everyone is present and accounted for, a task that is completed each hour. Charlotte repeats the word ‘register’ out loud.
11:30: A female health-care support worker brings Charlotte a biscuit. She breaks a piece off and offers it to her to taste. Charlotte says to her ‘don't be daft’; the health-care support worker responds, ‘if I taste it will you?’ Charlotte responds by saying, ‘I'm not that daft’ and the health-care support worker says, ‘your husband sent it’. Charlotte laughs out loud but she does not take the biscuit and forcibly pushes it away from her.
Example 3: ‘Swearing and asserting’
A Thursday in late December
16:28: There are 11 patients in the lounge area and one visitor. There are no staff in this area. A male patient is walking around trying all the door handles – his manner seems restless and angry. Two staff are with a patient in the toilet. The atmosphere in the lounge feels tense and busy. Charlotte suddenly says, ‘fxxx off’. This does not appear to be directed at anyone. The female patient who is sat across from Charlotte responds by saying, ‘stupid bxxch’. Charlotte looks around and swears some more.
16:35: Charlotte is still sat in the same chair. She now has her head in her hands. Her voice is very loud, her pitch angry and cadence quick. She is saying ‘fxxxing hell, fxxxing hell, blah, blah, it's not yours, fxxx off, fxxx off and don't go in’. I wonder if the last three words have been triggered by a health-care support worker on the ward that she had overheard saying ‘don't go in’ elsewhere in the day area.
16:40: I can see two staff nurses in the office with a doctor. Charlotte starts to shout, ‘get out, get out, get out, get out, you dirty bxxxxxd’. I am not sure if this is now in response to a male patient who is in her vicinity, reliving an emotion from earlier or if she is hallucinating. A female staff nurse comes out of the office, but she does not stay in the day area – she walks through it and leaves Jasmine Ward. Charlotte watches her.
16:45: Charlotte is now sat down but continues to shout. It is a mixture of swear words and command words such as ‘shut up’ and ‘get off’. There were words that were also neologisms that I could only try to write down and spell out. There are now three health-care support workers in the day area. They are talking. Their conversation is about Charlotte and whether her shouting is because she needs the toilet. They decide to try to take her. Two of the health-care support workers approach Charlotte and ask her to go to the toilet. They lean into her and get her up. She stands up for them but continues to swear. The health-care support workers walk either side of Charlotte and link their arms with hers and take her through to the bedroom area where the ladies' toilet is situated. Even though she has moved out of the main day area and into the bedroom part of Jasmine Ward, I can still hear Charlotte shouting.
16:55: Charlotte is now in the lounge area. The two health-care support workers sit her in a chair and move on to start tea as the tea trolley has arrived. Charlotte continues to look angry and upset; she is also looking tired. The health-care support workers are inviting patients to the table for their evening meal. Charlotte begins to shout ‘bagstall, bagstall, bagstall’ and ‘fxxx off’. The ward feels noisy and busy with the tea activity. Charlotte remains seated and does not respond to the invitation.
Charlotte's admission to Jasmine Ward: Harry's (family carer) perspective
When Charlotte was in the acute hospital, Harry was made aware that she was going to be transferred to Jasmine Ward as the staff had trouble in caring for Charlotte. As Harry shared:
When she [Charlotte] was on [acute hospital ward's name] she really kicked off and they were having a time to control her. When I went to visit from walking, you know, 100 yards away from the ward, I could hear her. She had really, really, kicked off.
Following her compulsory admission to Jasmine Ward, Harry said that Charlotte resisted all staff attempts at help such as ‘changing her pad [continence aid] or dressing her or feeding her’. For the first month of Charlotte's admission to Jasmine Ward, Harry visited the ward every day as he was needed to feed and give drinks and medication to his wife. As Harry shared, this was because she ‘wouldn't allow anyone else to do it’ and when staff on Jasmine Ward tried, Charlotte ‘moved their hands out of the way and would give of a lot of bad language, swearing, pushing, and the like’.
During the interview, Harry explained that when he used to care for Charlotte at home, he had developed his own approach to managing the situation when she became angry, upset and agitated, and this consisted of ‘waiting for her to settle down before I could even look her directly in the eye and talk to her’. As Harry explained, finding opportunities for Charlotte to have ‘a bit of space’ and ‘calm down’ were crucial as if the timing was wrong, he described the changes in his wife's behaviour as ‘like knocking a switch on and off’. Once Charlotte's assessment on Jasmine Ward was eventually complete, Harry wanted her to return home as he was concerned that a nursing home would not be able to meet Charlotte's needs. As Harry shared, ‘the only way I can be sure that she's ok is if I can have her with me, but I know that I would need help’.
It was clear that the instability in Charlotte's presentation in recent months caused Harry significant distress and a feeling of ‘letting her down because I know I'm not there for her’.
Charlotte's admission to Jasmine Ward: Linda's (named nurse) perspective
Charlotte's named nurse, Linda, believed that by the time Charlotte was admitted to Jasmine Ward she was ‘probably, sort of, fairly advanced in her dementia’ and because of this, she was not able to make any informed choices about ‘attending to her own personal care and recognising her own needs’. From a nursing perspective, this meant that if Charlotte was left on her own, she would not recognise that she needed to change her clothes, take herself to the toilet, get up and dressed, or ask for a drink or food. Linda felt that Charlotte's admission to Jasmine Ward for an assessment was appropriate and, if anything, ‘she could have done with being admitted a little bit sooner’ because of the high degree of anger, and aggression, that Harry had been dealing with when she was at home.
When Charlotte was admitted to Jasmine Ward, Linda recalled that Charlotte was ‘really angry, very angry, all of the time’ and from Linda's perspective, the purpose of Charlotte's admission was:
To try and reduce this agitation, to try to get her used to accepting assistance with her personal care and for her to take regular diet and fluids. We thought that, at that time, maybe the use of appropriate medication would help this.
Charlotte's refusal to accept food, fluids and medication from nursing staff had been present since admission to Jasmine Ward and this remained unchanged despite ongoing attempts from nursing staff to change the situation. Linda talked with worry and concern about this everyday reality as she went on to explain:
It's so difficult really. She [Charlotte] persists in not taking much diet from us [nursing/care team] at all. She will take some things. She'll have the occasional biscuit, a bit of a banana maybe. She might have a little bit of dessert now and again, but it's not that consistent that it would meet her needs really.
Consequently, Harry and close family members came to Jasmine Ward twice a day to undertake this pivotal role with/for Charlotte. Linda acknowledged that if the family were not able to do this, then nursing staff would really struggle and Charlotte would become ‘a lot more complex because we wouldn't have an identified intervention that worked’. When reflecting upon Charlotte's admission and ongoing time on Jasmine Ward, Linda described her as being ‘one of the most challenging people that I have ever had to look after’.
Charlotte's admission to Jasmine Ward: care record review
Charlotte's care record reported that she was ‘transferred [to Jasmine Ward] from the general hospital where she had been admitted for a fall’ and that she ‘had also had Haloperidol [major tranquiliser used in the control of agitation, amongst other symptoms] at home and could not move the day after’. They furthermore made reference as to why Charlotte was admitted to Jasmine Ward insofar as Charlotte's behaviour was ‘difficult to manage on the general ward and admission on a section 2 [of the Mental Health Act 1983] was arranged for assessment’. On the general ward, Charlotte was displaying unmet needs that challenged staff and was non-compliant with medication and diets. Her immediate presentation on admission to Jasmine Ward was summarised as ‘presenting as very agitated, shouting and swearing’.
Words and phrases frequently appearing in Charlotte's progress notes included: ‘verbally aggressive’, ‘refused diet and fluids until husband visited’, ‘refused diet and fluids’, ‘assisted to wash and dress but was resistive throughout’, ‘assisted to wash and dress by three members of staff’, ‘shouting and spitting during care interventions’. The most frequent of entries were ones which were concerned with Charlotte consistently refusing all offers of diet and fluids from staff, her restiveness to personal care interventions, of being unsettled in the ward environment, and shouting and swearing at staff and patients.
Discussion
This article is drawn from a larger interpretive description study conducted on a dementia assessment ward and where the intention was to create a model of complexity to help guide practice (see Jones et al., Reference Jones, Cullum, Watson and Keady2023a; and for more information on interpretive description, see Thorne, Reference Thorne2008). For this phase of the study, a nested case study (Schwandt and Gates, Reference Schwandt, Gates, Denzin and Lincoln2018) was assimilated into the interpretive description to summarise how Charlotte, as a patient on Jasmine Ward, may have experienced complexity and a life on the ward; an experience that also rippled through to the visiting family, ward staff and other patients. The study has also started to lift the lid on an under-researched and overlooked aspect of dementia care policy and care practices, namely the compulsory admission of people living with dementia for a period of assessment and treatment on a dementia assessment ward (for a broad review and discussion, see Akther et al., Reference Akther, Molyneaux, Stuart, Johnson, Simpson and Oram2019). Moreover, the article can also be seen as part of a tradition in the use of single case study data in dementia studies to illuminate previously unseen and difficult to reach groups, such as in HIV-associated dementia (McLean et al., Reference McLean, Aradi, Waknin, Rea and Camacho2022), young onset dementia (Williams et al., Reference Williams, Keady and Nolan1995) and semantic dementia (Kindell et al., Reference Kindell, Sage, Wilkinson and Keady2014). Furthermore, the mixed qualitative methods used in this case study have revealed the individuality of such admissions to a dementia assessment ward and that the admission has an impact on caring practices, including those of family carers and as seen by the actions of Harry and how he lovingly, and patiently, encouraged his wife to eat and drink when ward staff were simply unable to achieve this task – and this is not meant as a criticism of the staff's nursing/caring practices.
Recently, Thompson (Reference Thompson2022) has linked these intuitive and sensory/embodied skills to the field of care aesthetics. We will therefore predominantly develop and conceptualise the discussion through this lens as it gives voice to the skilled, person-centred practices (Kitwood and Brooker, Reference Kitwood and Brooker2019) that were happening on the ward during the care of Charlotte (by both family and ward staff), but which were not, perhaps, fully visible or articulated as such at the time. In the case of Charlotte, care aesthetics notes how sensory practices intersect to produce her experience and response to her care (Thompson, Reference Thompson2022). This interpretative lens is referred to as aesthetics, not in the common sense of a practice connected to the arts, but as a term that describes the creation of a complex sensory experience. As an illustration, in this article, the field notes are full of awareness of these elements, suggesting the importance of ‘hugs’, ‘holding hands’, being ‘very close’, rubbing cheeks, touching faces, stroking hair, tone of voice, and gaze or eye contact. There are different volumes and tones of the speaking voice documented both from carers and the recipients of care. There is ‘chat’ and there are ‘out of ear’ conversations; there are requests and there is shouting. There are multiple forms of movement, including care workers leaning in with their bodies and linking arms with the person they are supporting. At one time, the wider environment has an atmosphere of tension. The point to make here is that the aesthetic register exists within these field notes and, in themselves, the field notes are a reflection of everyday nursing and caring practice on Jasmine Ward.
Related to the previous point, it is important to state that the aesthetic register needs to be understood as an interaction of multiple parts, rather than a series of individual sensory practices. It reveals what Buse and Twigg (Reference Buse and Twigg2018: 341) refer to as the ‘close tactility of care’ but demonstrates that these interpersonal practices are embedded in a wider sensory environment. In Charlotte's case study, we can see the importance of touch across the different descriptions, and at one level the practice of different forms of procedural, intimate and supportive touch are a crucial dynamic for caring for a person living with dementia. However, what is worth highlighting is that it is touch in partnership with other senses that changes the quality of the experience. So, touch plus taste (e.g. Harry feeding his wife pie and then rubbing her cheek), illustrates the importance of interrelated sensory practices for the experience of this care. Care aesthetics is seeking to focus on these interactions – moving someone as you use a certain tone of voice or holding of a patient while feeding them – to focus on a fully embodied practice of care that meets the demands of people living with complex needs. Arguably, it is at this point where care documentation could be positioned to more fully capture such fluid, intimate and dynamic moments of care. Nursing scholar Pam Smith (Reference Smith2012: 2) refers to these practices as ‘gestures of caring’ which are too often overlooked as they ‘slip unnoticed in the daily routines and hustle and bustle of institutional life’. The proposal here is that noticing is the first step to valuing and supporting these interpersonal practices.
What is most notable in the field notes is how the aesthetic register changes so markedly in the reporting on the moments with the family members and those with the care staff on Jasmine Ward. In the description of Charlotte in the lounge with her family, we have comments on the position of the chairs, the proximity of each person to the other, the smiling, the sense of contentment and then multiple mentions of different acts of tenderness. When describing the interactions with the care staff, we get more reported speech and more instrumental language, e.g. the health-care support worker guides the cup to Charlotte's mouth, and more descriptions of doing care, i.e. taking to the toilet, inviting patients to an evening meal and so on. These are, of course, both aesthetic registers, but one appears more fully sensory with multiple senses at play across it, and the other reads as more functional. This illustrates a key dilemma with Charlotte's care as the focus on a relational, intimate moment with people with whom she is familiar, enables a process whereby Charlotte has her needs met and can remain calm. Her lack of familiarity with the care staff means that it will always be difficult for them to create those moments of calmly executed care created by her husband. That said, the way the field notes here so richly document a rounded sensory moment between her and her family hints at how the complex needs of a patient like Charlotte might be supported. It is the attention to the interaction of each sensory element and the gentle combination of different sensory acts of calming, of tenderness and proximal support that might be deployed more consistently.
Interestingly, one of LJ's ethnographic field notes ends with the description of the family care moment as, ‘it was humbling to see’. While acknowledging that this was a subjective response on behalf of the lead researcher, it is an important clue to how, when the aesthetics of care is richly executed, it has a surprising or noteworthy quality. It was ‘humbling to see’ perhaps because in that instant there is a created moment of care (Thompson, Reference Thompson2022) when the dignity of a person living with dementia is fully realised and care becomes authentically positioned as person-centred (Kitwood and Brooker, Reference Kitwood and Brooker2019). Moreover, the case study in the article also highlights the relationship between atmospheres and care. The interaction between atmosphere and aesthetics has been analysed by the German philosopher Gernot Böhme (Reference Böhme2020) as a means to understand the interrelation of architectural and design elements and human behaviour, and this in turn has been applied to health-care spaces by Martin et al. (Reference Martin, Nettleton and Buse2019). Crucially, atmosphere is intersubjective and both of the human body and the space in which it operates. To understand the aesthetics of care at work in the care of Charlotte, we note that it was both the range of sensory actions undertaken by the people in her life and the relation all had with the material environment. This includes the small objects (teacups), wider material components (the position of the chairs) and the broader design of the environment (the space of the lounge). Indeed, at one point in the field notes, the lounge is described as ‘tense’ and ‘busy’ and this is followed by Charlotte swearing. The point to emphasise here is that tension is a subjective feeling of the observer, so a sensory response to the combination of human activity and environment, but it is also likely to be experienced to different degrees by others in that context. It is a personal perception, and yet co-produced by the interaction of all elements of the space. Sensitivity to atmospheres is not static but changes over time, and as we have seen in this article, it changes according to the different sensory capacities of those present.
Reflections on the research process
First, despite the lead researcher and first author being an ANP who had engaged in clinical practice for many years using Johns’ (Reference Johns and Johns2017) structured reflective model, this was the first time she had been on a dementia assessment ward with the sole purpose of undertaking research observations. The experience was not always reported as being a positive one. For instance, it was personally confronting for LJ to step back and observe the evident anxiety of some patients in living in such a large, communal space with seemingly unfamiliar furnishings, people, noises, routines and surroundings. This state of bewilderment was amplified by a lack of personalised items or spaces on Jasmine Ward in which to exert agency and control, including in the opportunity to leave through the main front door when desired or turn off the television in the lounge if the noise became overbearing. In LJ's reflective notes, links were made between this state of bewilderment and the actions of ‘watching’ and ‘looking’ by some patients on Jasmine Ward. This was also seen in Charlotte's case study when, for example, she was observed as intently watching the staff talking to the new admission before laughing out loud and noisily. This heightened state of ‘watching’ and ‘looking’ happened at all times of the day and seemed to be concentrated on new and everyday events and on important threshold spaces in Jasmine Ward, such as the location of the main entry and exit doors and who came and went through them. Such a linkage, we would suggest, requires additional exploration and study. Similarly, LJ found it a challenge to suppress the need on occasions to step out of the researcher role and into an ANP role. This was particularly evident in observing the practice of health-care support workers on Jasmine Ward who sometimes found themselves on their own dealing with the consequences of patients' unmet needs and where immediate clinical leadership was necessary.
Second, the observation data gave examples of the use of therapeutic lies by care staff in everyday interaction with Charlotte, such as when a health-care support worker told Charlotte that she was ‘doing the register’ instead of an hourly location list for all patients on Jasmine Ward. In many ways, performance of this ‘truth-telling’ interaction by carers, both family and professional, with people living with more advanced dementia is indicative of everyday communication practices and the ethical dilemmas that may subsequently arise. As Hughes (Reference Hughes2023: 183) has recently argued, such ethical dilemmas are examples of personal values where carers need to justify such communication practices internally so that they ‘cohere with our conceptions of what it is to live humanly’. Hughes (Reference Hughes2023) goes on to suggest that not speaking the truth to people with dementia may be excusable should it stem from virtues such as charity, compassion and practical wisdom. Moreover, the interaction and case study in this article also spotlight the need to leave space in the dementia discourse for a narrative of complexity and suffering to emerge and be an accepted part of the lived experience of dementia (see also Bartlett et al., Reference Bartlett, Windemuth-Wolfson, Oliver and Dening2017; Keady et al., Reference Keady, Campbell, Clark, Dowlen, Elvish, Jones, Kindell, Swarbrick and Williams2022). Put simply, not everyone with dementia lives well with their dementia.
Third, practice on a dementia assessment ward is highly skilled and intensive and appears to be imbued with ethical decision-making on a minute-by-minute basis. Indeed, as an extension to this point, it was an ethical challenge for the authors to know how to both balance and communicate Charlotte's consistent use of profanities in her everyday speech against causing offence to the readership of this article, whilst remaining true to the nature of the realities that ward staff, visiting family(ies) and other patients experienced. Our solution was a compromise insofar as we redacted certain words in the article that somehow diminished their power and descriptive properties. Perhaps this compromise is a microcosm of current practice on a dementia assessment ward as it is hard to always know exactly what to do and say for the best, and from what set of values and ethical/moral standpoints. The language of care aesthetics gives voice to the practice of person-centred care (Kitwood and Brooker, Reference Kitwood and Brooker2019), which, in turn, helps to define the craft of dementia care in the dementia assessment ward. Further work is needed to explore this statement, but we hope that going forward, care practice on the dementia assessment ward is central to this new opportunity in dementia studies.
Strengths and limitations
Data describing patients' experiences on a dementia assessment ward are limited and this study has developed such an understanding as well as illuminating the everyday work of a range of practitioners, including nursing staff, in this environment of care: this is a strength of this study. Conducting research which involved people living with dementia who are compulsorily detained under the Mental Health Act (Department of Health, 1983) is another strength. LJ's experience of working for over 20 years in a dementia assessment ward brought a sensitivity and critical depth to the data that enhanced the findings and the ethnographic observations. The work did not capture ethnic diversity through the shared case study, and this is a limitation. It was not possible to interview Charlotte as a person living with dementia about her experience of being a patient on a dementia assessment ward because of the complexity of her presentation and her refusal to engage with LJ. Despite the clinical and research capabilities in the study team/authorship, this was a limitation and was not foreseen in the research design and planning stages. Future research in this field should be mindful of our experience and seek to integrate a longitudinal engagement process using creative and person-centred communication strategies into the methods of study. No data-sorting software was used for the analysis.
Conclusions
In the UK, knowledge and awareness about dementia assessment wards are needed to help increase the visibility of such settings in everyday care practice, service planning and policy making. Whilst there are studies that have taken place on dementia assessment wards, they have mainly been audits and evaluations of practice rather than primary research studies (Wolverson et al., Reference Wolverson, Dunning, Crowther, Russell and Underwood2022), and there remains substantial gaps in knowledge about the experience of being a patient on the ward, as well as visiting such environments of care. This study contributes to the existing literature by sharing a case study of one patient's experience of being ‘detained’ on a dementia assessment ward under a section of the Mental Health Act (Department of Health, 1983) and observing her interactions and actions with other patients, the care staff and her visiting family members, as well as her connections with/to the physical environment. To give voice to person-centred practices, in this study we have highlighted the importance and value of care aesthetics in articulating the embodied, sensory and relational components of care, and how a sensory register can help showcase these elements. Despite national strategies for dementia worldwide that promote living well with dementia, so far there has been little attention paid to unlocking subjective experiences where this is not the case and where there is seemingly significant personal distress and complexity of need. Taken with an appreciation of care aesthetics, this study can therefore begin to make visible some of these more challenging discourses in the dementia care and studies field. Finally, further research should focus more on the sensory and embodied language of care aesthetics and how it can be used to describe the personal caring moments that are seen every day on the dementia assessment ward, and beyond such environments of care.
Acknowledgements
The authors would like to acknowledge the participation of the family and care staff described in this article, and Dr Sarah Fox at the University of Manchester for comments on an earlier draft of this work.
Financial support
This work was supported by the National Institute for Health Research Clinical Doctoral Research Fellowship programme (CDRF–2012-03-033).
Ethical standards
Ethical approval was gained from the North West Haydock NHS Research Ethics Committee (reference 15/NW/0116).


 Open access
Open access