

Coffee is one of the most popular beverages consumed worldwide, and it has been part of the human diet for centuries. Coffee is the primary dietary source of caffeine in many populations and contains hundreds of bioactive compounds besides caffeine( Reference Higdon and Frei 1 ). Due to the high prevalence of coffee consumption, even small effects on health could have a large impact on public health. Coffee has for long been considered unhealthful in that caffeine acutely increases blood pressure( Reference Noordzij, Uiterwaal and Arends 2 ) and serum homocysteine levels( Reference Hartley, Lovallo and Whitsett 3 ) and inhibits insulin activity( Reference Higdon and Frei 1 ), and coffee diterpene cafestol in unfiltered coffee increases serum cholesterol levels( Reference de Roos and Katan 4 ). Despite the acute effects of coffee, adverse health outcomes of coffee consumption in the long term have not been found. A growing body of evidence has shown that habitual coffee consumption is associated with a decreased risk of type 2 diabetes( Reference Huxley, Lee and Barzi 5 ), heart diseases( Reference Wu, Ho and Zhou 6 ) and some types of cancers( Reference Yu, Bao and Zou 7 ), which are major causes of death. In addition, there has been suggestive evidence of a lower risk of suicides( Reference Lucas, O'Reilly and Pan 8 ), Parkinson's disease( Reference Sääksjärvi, Knekt and Rissanen 9 ), Alzheimer's disease( Reference Barranco Quintana, Allam and Serrano Del Castillo 10 ) and gallstones( Reference Leitzmann, Willett and Rimm 11 , Reference Leitzmann, Stampfer and Willett 12 ) among coffee drinkers. Overall, habitual coffee drinkers appear to develop tolerance to the acute effects of caffeine and may experience the beneficial effects of other compounds of coffee (e.g. phenolic compounds) that protect against oxidative damage( Reference Gómez-Ruiz, Leake and Ames 13 ), improve insulin sensitivity( Reference van Dam 14 ) and have anticarcinogenic properties( Reference Huber, Scharf and Nagel 15 ).
Many epidemiological studies have suggested that coffee consumption decreases the incidence of chronic diseases, but the association of coffee consumption with all-cause mortality has been less investigated. Due to the strong antioxidant properties of coffee components, long-term coffee consumption may help delay disease progression and thus prolong people's lifespan. Although several prospective cohort studies have been conducted to determine the association between coffee consumption and total mortality( Reference Kahn, Phillips and Snowdon 16 – Reference Lindsted, Kuzma and Anderson 35 ), to our knowledge no comprehensive review and meta-analysis of such studies has been conducted. To elucidate the long-term effects of coffee consumption on mortality and quantitatively assess the association at different levels of coffee consumption, we systematically conducted a meta-analysis of prospective cohort studies.
Methods
Literature search and selection
To identify relevant studies, we carried out a literature search for all articles published (including those ahead of publication) through June 2013 using the PubMed and EMBASE databases, with the following terms: ‘(coffee, caffeine, beverages, dietary factors or risk factors) combined with (total mortality, all-cause mortality, death or survival)’. Furthermore, we reviewed the reference lists of original and review articles to search for additional eligible studies. Only those that were published as full-length articles and published in English were considered. Studies were eligible for inclusion in the present meta-analysis if (1) they had a prospective design, (2) the exposure of interest was coffee consumption, (3) the outcome of interest was defined as total or all-cause mortality and (4) relative risks (RR) with 95 % CI (or data to calculate these) were reported. Since smoking is the most important confounder of the relationship between coffee consumption and mortality, we included studies that provided risk estimates adjusted for smoking status. Among the eligible studies, one study reported risk estimates for only males( Reference Lindsted, Kuzma and Anderson 35 ), while another study carried out in the same cohort reported risk estimates for both men and women combined( Reference Kahn, Phillips and Snowdon 16 ), so we included only the latter study in the meta-analysis. We directly contacted authors for the full text of papers when they were not available( Reference Rosengren and Wilhelmsen 20 , Reference Klatsky, Armstrong and Friedman 21 , Reference Gardener, Rundek and Wright 34 ). A flow diagram of the study selection process is shown in Supplementary Fig. 1 (available online).
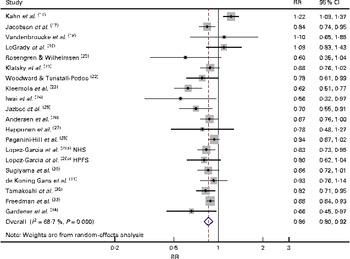
Fig. 1 Forest plot of the prospective cohort studies of total mortality for high v. low/no coffee consumption. A total of thirteen studies( Reference Jacobsen, Bjelke and Kvale 17 – Reference Kleemola, Jousilahti and Pietinen 23 , Reference Andersen, Jacobs and Carlsen 26 , Reference Happonen, Läärä and Hiltunen 27 , Reference Lopez-Garcia, van Dam and Li29a,b , Reference de Koning Gans, Uiterwaal and van der Schouw 31 , Reference Freedman, Park and Abnet 33 ) used ≥ 5–9 cups/d as a cut-off for the highest category and seven studies( Reference Kahn, Phillips and Snowdon 16 , Reference Iwai, Ohshiro and Kurozawa 24 , Reference Jazbec, Simić and Corović 25 , Reference Paganini-Hill, Kawas and Corrada 28 , Reference Sugiyama, Kuriyama and Akhter 30 , Reference Tamakoshi, Lin and Kawado 32 , Reference Gardener, Rundek and Wright 34 ) used ≥ 2–4 cups/d as a cut-off for the highest category. RR, relative risk; NHS, Nurses' Health Study; HPFS, Health Professionals Follow-up Study. (A colour version of this figure can be found online at http://www.journals.cambridge.org/bjn).
Data extraction
Data were extracted independently by two investigators (Y. J. and E. G.) according to the Meta-analysis of Observational Studies in Epidemiology guidelines( Reference Stroup, Berlin and Morton 36 ), and any discrepancies were resolved by reviewing the original reports and holding further discussions. We counted one report( Reference Lopez-Garcia, van Dam and Li 29 ) as two prospective studies, as it provided separate RR from two large US cohorts, the Nurses' Health Study (NHS)( Reference Lopez-Garcia, van Dam and Li29a ) and the Health Professionals Follow-up Study (HPFS)( Reference Lopez-Garcia, van Dam and Li29b ). For each study, the following information was extracted: first author's last name; year of publication; geographical region; follow-up period; number of cases; number of subjects or person-time; adjustment factors; RR and 95 % CI for association between various levels of coffee consumption and total mortality. For studies that did not provide 95 % CI, but provided the number of cases and subjects across coffee consumption categories, we used the latter information to calculate the standard error of the crude RR and then approximate CI for the reported adjusted RR( Reference Kahn, Phillips and Snowdon 16 , Reference Jacobsen, Bjelke and Kvale 17 , Reference LeGrady, Dyer and Shekelle 19 , Reference Woodward and Tunstall-Pedoe 22 ). For those reporting several RR for this association, we used the RR that reflected the greatest degree of adjustment for potentially confounding variables.
Statistical analyses
To estimate pooled RR of total mortality for the highest v. lowest category of coffee consumption, the natural logarithm of the RR from each study was combined using the DerSimonian and Laird random-effects models, which incorporate both within-study and between-study variations( Reference DerSimonian and Laird 37 ). If the original studies had not used the lowest category as a reference, the RR and its 95 % CI were recalculated relative to the lowest category, as has been done previously in a meta-analysis of coffee consumption and CHD( Reference Wu, Ho and Zhou 6 ). Since each study used different levels of coffee consumption as a cut-off for the highest category, we conducted a stratified meta-analysis by cut-offs for the highest coffee consumption categories of 5–9 cups/d (n 13 studies)( Reference Jacobsen, Bjelke and Kvale 17 – Reference Kleemola, Jousilahti and Pietinen 23 , Reference Andersen, Jacobs and Carlsen 26 , Reference Happonen, Läärä and Hiltunen 27 , Reference Lopez-Garcia, van Dam and Li29a,b , Reference de Koning Gans, Uiterwaal and van der Schouw 31 , Reference Freedman, Park and Abnet 33 ) and 2–4 cups/d (n 7 studies)( Reference Kahn, Phillips and Snowdon 16 , Reference Iwai, Ohshiro and Kurozawa 24 , Reference Jazbec, Simić and Corović 25 , Reference Paganini-Hill, Kawas and Corrada 28 , Reference Sugiyama, Kuriyama and Akhter 30 , Reference Tamakoshi, Lin and Kawado 32 , Reference Gardener, Rundek and Wright 34 ). We also conducted a separate meta-analysis to determine whether moderate coffee consumption (1–2 cups/d) is associated with a low risk of death (n 12 studies)( Reference Kahn, Phillips and Snowdon 16 , Reference Woodward and Tunstall-Pedoe 22 , Reference Iwai, Ohshiro and Kurozawa 24 , Reference Jazbec, Simić and Corović 25 , Reference Happonen, Läärä and Hiltunen 27 – Reference Sugiyama, Kuriyama and Akhter 30 , Reference Tamakoshi, Lin and Kawado 32 – Reference Gardener, Rundek and Wright 34 ). To examine the long-term health benefits of consuming coffee not containing caffeine, we identified prospective studies that provided data on decaffeinated coffee consumption and total mortality and conducted a small meta-analysis( Reference Andersen, Jacobs and Carlsen 26 , Reference Paganini-Hill, Kawas and Corrada 28 , Reference Lopez-Garcia, van Dam and Li29a,b , Reference Gardener, Rundek and Wright 34 ).
The RR from each study as well as a pooled RR are presented as forest plots, where the size of data markers (squares) corresponds to the inverse of the variance of the natural logarithm of RR from each study and the diamond indicates a pooled RR. Statistical heterogeneity among the studies included in the meta-analysis was assessed using the Cochran Q statistic( Reference Cochran 38 ) and inconsistency was quantified with the I 2 statistics (100 % × (Q− df)/Q)( Reference Higgins, Thompson and Deeks 39 ). To examine the variations in risk estimates by study characteristics, we conducted subgroup analyses by sex (men/women), geographical region (USA/Europe/Japan) and follow-up time ( ≤ 14 years or >14 years; median follow-up time). As a way of assessing the quality of the prospective cohort studies included in the meta-analysis, we examined whether the studies had adjusted for important confounders such as age, sex, smoking status, alcohol consumption and BMI and calculated pooled RR for studies with strong or weak adjustment separately. To test for variations in the pooled RR of the subgroups, we conducted a meta-regression analysis with the log (RR) modelled as a dependent variable and study variables modelled as explanatory variables. In addition, we carried out sensitivity analyses excluding one study at a time to determine whether the results were driven by a single study.
We examined dose–response relationships based on studies( Reference Kahn, Phillips and Snowdon 16 , Reference LeGrady, Dyer and Shekelle 19 , Reference Klatsky, Armstrong and Friedman 21 – Reference Iwai, Ohshiro and Kurozawa 24 , Reference Andersen, Jacobs and Carlsen 26 – Reference Gardener, Rundek and Wright 34 ) that provided data on at least three levels of coffee consumption including the reference category, number of cases and participants or person-time, and effect estimates, using the method developed by Greenland and Longnecker( Reference Berlin, Longnecker and Greenland 40 – Reference Orsini, Bellocco and Greenland 42 ). We used the two-stage generalised least-squares trend estimation method to estimate the study-specific slope lines first and then derive an overall average slope( Reference Orsini, Bellocco and Greenland 42 ). We assessed for potential non-linearity between coffee consumption and risk of death by adding a quadratic term of coffee consumption to the model. A P value for non-linearity was calculated by testing the null hypothesis that the coefficient of the quadratic term is equal to 0, as has been done previously in a meta-analysis of coffee consumption and the risk of endometrial cancer( Reference Je and Giovannucci 43 ). Finally, publication bias was evaluated through visual inspection of a funnel plot (i.e. a plot of study results against precision) as well as Begg & Mazumdar's( Reference Begg and Mazumdar 44 ) and Egger et al.'s( Reference Egger, Davey Smith and Schneider 45 ) tests. A two-tailed P< 0·05 was considered to be statistically significant. All the statistical analyses were carried out using the Stata/SE version 12.0 software (Stata Corporation).
Results
Study characteristics
We identified a total of twenty prospective cohort studies including 973 904 participants and 129 538 deaths that met the inclusion criteria of the present meta-analysis( Reference Kahn, Phillips and Snowdon 16 – Reference Gardener, Rundek and Wright 34 ). The main characteristics of the studies included in the meta-analysis are summarised in Table 1. All the studies were prospective cohort studies with follow-up periods of 7·1–28 years with a median follow-up time of 14·1 years. The study subjects were all adults (age ≥ 20 years) at baseline. Of the twenty prospective studies, nine studies were conducted in the USA( Reference Kahn, Phillips and Snowdon 16 , Reference LeGrady, Dyer and Shekelle 19 , Reference Klatsky, Armstrong and Friedman 21 , Reference Andersen, Jacobs and Carlsen 26 , Reference Paganini-Hill, Kawas and Corrada 28 , Reference Lopez-Garcia, van Dam and Li29a,b , Reference Freedman, Park and Abnet 33 , Reference Gardener, Rundek and Wright 34 ), eight in Europe( Reference Jacobsen, Bjelke and Kvale 17 , Reference Vandenbroucke, Kok and van 't Bosch 18 , Reference Rosengren and Wilhelmsen 20 , Reference Woodward and Tunstall-Pedoe 22 , Reference Kleemola, Jousilahti and Pietinen 23 , Reference Jazbec, Simić and Corović 25 , Reference Happonen, Läärä and Hiltunen 27 , Reference de Koning Gans, Uiterwaal and van der Schouw 31 ) and three in Japan( Reference Iwai, Ohshiro and Kurozawa 24 , Reference Sugiyama, Kuriyama and Akhter 30 , Reference Tamakoshi, Lin and Kawado 32 ). All the studies, except four( Reference Jacobsen, Bjelke and Kvale 17 , Reference LeGrady, Dyer and Shekelle 19 , Reference Rosengren and Wilhelmsen 20 , Reference Andersen, Jacobs and Carlsen 26 ), included both male and female participants, but only ten studies reported separate death outcomes for men and women( Reference Vandenbroucke, Kok and van 't Bosch 18 , Reference Woodward and Tunstall-Pedoe 22 – Reference Jazbec, Simić and Corović 25 , Reference Lopez-Garcia, van Dam and Li29a,b , Reference Sugiyama, Kuriyama and Akhter 30 , Reference Tamakoshi, Lin and Kawado 32 , Reference Freedman, Park and Abnet 33 ). In addition to smoking status, most of the studies adjusted for potential confounders such as alcohol consumption( Reference Vandenbroucke, Kok and van 't Bosch 18 , Reference Rosengren and Wilhelmsen 20 , Reference Klatsky, Armstrong and Friedman 21 , Reference Iwai, Ohshiro and Kurozawa 24 , Reference Andersen, Jacobs and Carlsen 26 , Reference Paganini-Hill, Kawas and Corrada 28 – Reference Gardener, Rundek and Wright 34 ) and BMI (kg/m2)(18,20,21,22,26–34).
Table 1 Characteristics of the prospective studies included in the present meta-analysis (Relative risks (RR) and 95 % confidence intervals)
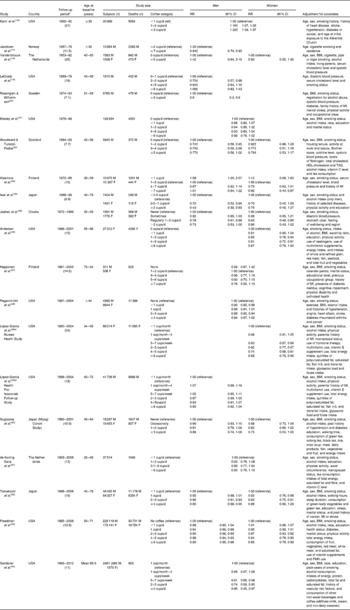
M, male; F, female; MI, myocardial infarction; PMH, postmenopausal hormone.
* Mean or median duration of follow-up in parentheses (years).
† Standard errors were calculated based on the data.
Pooled relative risk for high v. low coffee consumption
The multivariable-adjusted RR for each study and all studies( Reference Kahn, Phillips and Snowdon 16 – Reference Gardener, Rundek and Wright 34 ) combined for the high v. low category of coffee consumption are shown in Fig. 1. Under the random-effects model, the pooled RR of total mortality for all studies combined was 0·86 (95 % CI 0·80, 0·92; P< 0·001). The pooled RR for studies using 2–4 cups/d as a cut-off for the high category was similar to that for studies using 5–9 cups/d as the cut-off (P for category difference = 0·63; Table 2).
Table 2 Summary of pooled relative risks (RR) of total mortality for high v. low/no coffee consumption (Relative risks and 95 % confidence intervals)
* P value difference in RR for studies carried out in Europe v. the USA.
† P value difference in RR for studies carried out in Japan v. the USA.
‡ Median of follow-up time of the studies is 14·1 years.
§ Adjustment for at least age, sex, smoking status, alcohol intake and BMI (kg/m2) is considered as strong adjustment. Otherwise, it is considered as weak adjustment.
By geographical region, the inverse association tended to be stronger for the eight studies carried out in Europe (RR 0·78, 95 % CI 0·70, 0·88) and three studies conducted in Japan (RR 0·82, 95 % CI 0·73, 0·92) than for the nine studies carried out in the USA (RR 0·92, 95 % CI 0·84, 1·00) (P for Europe or Japan v. USA = 0·06 and 0·24, respectively; Fig. 2). The inverse association was similar for men (RR 0·81, 95 % CI 0·73, 0·90) and women (RR 0·84, 95 % CI 0·79–0·89) (P for men v. women=0·96; Table 2).
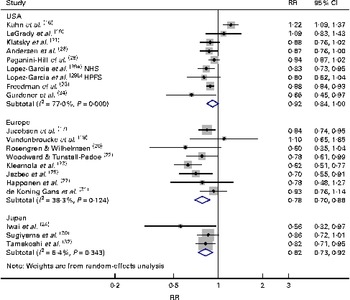
Fig. 2 Forest plot of the prospective cohort studies of total mortality for high v. low/no coffee consumption, stratified by geographical region. RR, relative risk; NHS, Nurses' Health Study; HPFS, Health Professionals Follow-up Study. (A colour version of this figure can be found online at http://www.journals.cambridge.org/bjn).
For the duration of follow-up, we used a median follow-up time of 14 years as a cut-off. The studies with short follow-up durations ( ≤ 14 years) tended to exhibit a stronger inverse association between coffee consumption and total mortality (RR 0·82, 95 % CI 0·76, 0·89) compared with those with long follow-up durations (>14 years) (RR 0·91, 95 % CI 0·82, 1·01) (P for short v. long follow-up duration = 0·11). When limited to thirteen studies that had adjusted for at least age, sex, smoking status, alcohol consumption and BMI, the pooled RR was slightly attenuated to 0·88 (95 % CI 0·85, 0·91), but the inverse association remained significant, and no significant difference by adjustment factor was found (P for strong v. weak confounder adjustment = 0·93). The additional analysis limited to studies that had adjusted for health status including history of some diseases, blood pressure or serum cholesterol levels at baseline showed a pooled RR of 0·85 (95 % CI 0·77, 0·92), which remained similar to that in the main analysis (data not shown).
There was evidence of some heterogeneity among all the cohort studies (P for heterogeneity < 0·001; I 2= 68·7 %). After excluding one study that showed the strongest positive( Reference Kahn, Phillips and Snowdon 16 ) association, the significant heterogeneity decreased (P= 0·05; I 2= 37·9 %). By geographical region, there was no significant heterogeneity among the studies conducted in Europe (P= 0·12; I 2= 38·4 %) or Japan (P= 0·34; I 2= 6·4 %), but there was some evidence of heterogeneity among the studies conducted in the USA (P< 0·001; I 2= 77·0 %). The earliest study carried out by Kahn et al. ( Reference Kahn, Phillips and Snowdon 16 ) seemed to explain most of the heterogeneity found in the studies conducted in the USA. After the exclusion of the Kahn et al. ( Reference Kahn, Phillips and Snowdon 16 ) study, the pooled RR for studies carried out in the USA was 0·89 (95 % CI 0·85, 0·93) and the heterogeneity disappeared (P= 0·31; I 2= 14·8 %).
Pooled relative risk for moderate v. low coffee consumption
The multivariable-adjusted RR for each study and twelve studies( Reference Kahn, Phillips and Snowdon 16 , Reference Woodward and Tunstall-Pedoe 22 , Reference Iwai, Ohshiro and Kurozawa 24 , Reference Jazbec, Simić and Corović 25 , Reference Happonen, Läärä and Hiltunen 27 – Reference Sugiyama, Kuriyama and Akhter 30 , Reference Tamakoshi, Lin and Kawado 32 – Reference Gardener, Rundek and Wright 34 ) combined for moderate coffee (1–2 cups/d) v. low coffee consumption are shown in Fig. 3. The pooled RR was 0·92 (95 % CI 0·87, 0·98), which was weaker than the pooled RR for high v. low coffee consumption, but the inverse association was statistically significant. Compared with men (RR 0·92, 95 % CI 0·86, 0·98), women tended to have a lower risk of death (RR 0·87, 95 % CI 0·80, 0·94), but no significant difference by sex was found (P for men v. women = 0·48). The results of subgroup analyses for moderate v. low coffee consumption were similar to those of the analyses for high v. low coffee consumption, although the strength of the associations in each stratum was slightly weaker.

Fig. 3 Forest plot of the prospective cohort studies of total mortality for moderate (1–2 cups/d) v. low/no coffee consumption. RR, relative risk; NHS, Nurses' Health Study; HPFS, Health Professionals Follow-up Study. (A colour version of this figure can be found online at http://www.journals.cambridge.org/bjn).
Dose–response meta-analysis
A total of sixteen studies were included for the dose–response meta-analysis of coffee consumption and risk of death( Reference Kahn, Phillips and Snowdon 16 , Reference LeGrady, Dyer and Shekelle 19 , Reference Klatsky, Armstrong and Friedman 21 – Reference Iwai, Ohshiro and Kurozawa 24 , Reference Andersen, Jacobs and Carlsen 26 – Reference Gardener, Rundek and Wright 34 ). The pooled RR for a 1 cup/d increment of coffee consumption was 0·96 (95 % CI 0·94, 0·97; P< 0·001), which was similar for men (RR 0·94, 95 % CI 0·91, 0·97) and women (RR 0·95, 95 % CI 0·94, 0·97) (data not shown). However, we found some evidence of a non-linear association between coffee consumption and total mortality (P for non-linearity < 0·001), which supports the findings that high coffee consumption ( ≥ 5–9 cups/d) is not associated with a further reduced risk of death compared with moderately high coffee consumption ( ≥ 2–4 cups/d).
Decaffeinated coffee consumption and total mortality
In Supplementary Table 1 (available online), six studies that examined the association between decaffeinated coffee consumption and total mortality are listed out( Reference Andersen, Jacobs and Carlsen 26 , Reference Paganini-Hill, Kawas and Corrada 28 , Reference Lopez-Garcia, van Dam and Li29a,b , Reference Freedman, Park and Abnet 33 , Reference Gardener, Rundek and Wright 34 ). Since one study that showed an inverse association provided a forest plot without a risk estimate, only five studies were included for a small meta-analysis of decaffeinated coffee consumption and mortality( Reference Andersen, Jacobs and Carlsen 26 , Reference Paganini-Hill, Kawas and Corrada 28 , Reference Lopez-Garcia, van Dam and Li29a,b , Reference Gardener, Rundek and Wright 34 ). The pooled RR for high decaffeinated coffee consumption ( ≥ 2–4 cups/d) v. no coffee consumption was 0·86 (95 % CI 0·80, 0·92; P< 0·001) with no heterogeneity (P= 0·51; I 2= 0 %) (Supplementary Fig. 2, available online).
Publication bias
There was no indication of publication bias in the literature for the analyses of total mortality and high coffee consumption (Begg's P= 0·10; Egger's P= 0·14; Supplementary Fig. 3, available online) or moderate coffee consumption (Begg's P= 0·12; Egger's P= 0·23).
Discussion
To quantitatively assess the association between coffee consumption and total mortality, we conducted a meta-analysis of twenty prospective cohort studies, consisting of 129 538 cases of death among the 973 904 participants. The results support a significant inverse association between coffee consumption and risk of death. Overall, the risk of death decreased by 14 % for high (median of the highest categories: 5–6 cups/d) v. no or low (mostly less than 1 cup/d) coffee consumption. The reduced risk of death was similar for participants who drank ≥ 2–4 cups of coffee per d and those who drank ≥ 5–9 cups/d. Even consumption of one or two cups of coffee daily was associated with a lower risk of death (reduced by 8 %). Similar inverse associations were found for men and women, and limited data also suggested an inverse association between decaffeinated coffee consumption and mortality.
There was some evidence of heterogeneity among the studies overall, but the observed heterogeneity seemed to be explained, partly by one study, which was targeted on a unique population of Adventist religious adherents in the USA( Reference Kahn, Phillips and Snowdon 16 ). This was the only study that showed a significant positive association between coffee consumption and total mortality among the studies included in the meta-analysis. The reason for the observed positive association is unclear, but it may be due to confounding from unhealthy lifestyles among subjects consuming high amounts of coffee based on the previous literature( Reference Je, Liu and Giovannucci 46 ). The study was adjusted for smoking status, but was not adjusted for other potential confounders such as alcohol consumption and BMI. In addition, some residual confounding may also have existed, since coffee consumption has been considered a bad behaviour by the Adventists, and thus they were less likely to follow other prescripts of the church as well, resulting in increased mortality among coffee drinkers.
The mechanisms of the long-term effects of coffee are unclear. Coffee is a complex mixture of biologically active substances that may have both beneficial and harmful effects on the health of humans. Studies have shown some negative health consequences of caffeine consumption, particularly in relation to CVD risk, including increased blood pressure( Reference Noordzij, Uiterwaal and Arends 2 , Reference Hartley, Lovallo and Whitsett 3 ). However, these effects seem to be acute, and habitual coffee drinkers develop partial tolerance to the effects of caffeine in coffee. For the long-term effects of coffee, coffee components other than caffeine may become more relevant to affect health outcomes. Coffee is one of the major sources of antioxidants in the diet( Reference Svilaas, Sakhi and Andersen 47 ). Phenolic compounds in coffee (e.g. chlorogenic, ferulic and p-coumaric acids) have strong antioxidant activities( Reference Gómez-Ruiz, Leake and Ames 13 ). Several studies have also found an inverse association between coffee consumption and blood concentrations of some inflammatory markers( Reference Lopez-Garcia, van Dam and Qi 48 ). Prolonged inflammation may contribute to atherosclerosis and IHD as well as cancers. In addition, the chlorogenic acid in coffee may decrease blood pressure by increasing NO levels( Reference Watanabe, Arai and Mitsui 49 ) and reduce the risk of diabetes mellitus by slowing the release of glucose into the blood stream after consumption of a meal and improving insulin sensitivity, along with other components in coffee including Mg, trigonelline and quinides( Reference van Dam and Hu 50 – Reference Tunnicliffe and Shearer 52 ). Long-term hyperinsulinaemia is related to an increased risk of tumorigenesis due to increased cell proliferation and reduced apoptosis and thus enhances cancer progression( Reference Giovannucci, Harlan and Archer 53 , Reference Inoue and Tsugane 54 ). Hypertension, diabetes, CVD, inflammatory diseases and cancers are important causes of mortality. Thus, the net long-term impact of coffee consumption may favour a decreased risk of death by delaying the progression of disease through the beneficial properties of coffee components.
Of the twenty studies included in the meta-analysis, some studies also reported risk estimates of deaths from CVD( Reference Leitzmann, Stampfer and Willett 12 – Reference Kleemola, Jousilahti and Pietinen 23 , Reference Jazbec, Simić and Corović 25 – Reference Happonen, Läärä and Hiltunen 27 , Reference Lopez-Garcia, van Dam and Li 29 – Reference de Koning Gans, Uiterwaal and van der Schouw 31 , Reference Freedman, Park and Abnet 33 , Reference Gardener, Rundek and Wright 34 ), which showed an inverse trend of coffee consumption overall, while one study that was conducted early in men showed an increased risk of CVD-specific deaths( Reference LeGrady, Dyer and Shekelle 19 ). Several studies also reported risk estimates of deaths from total cancer( Reference LeGrady, Dyer and Shekelle 19 , Reference Rosengren and Wilhelmsen 20 , Reference Klatsky, Armstrong and Friedman 21 , Reference Iwai, Ohshiro and Kurozawa 24 , Reference Andersen, Jacobs and Carlsen 26 , Reference Happonen, Läärä and Hiltunen 27 , Reference Lopez-Garcia, van Dam and Li 29 , Reference Sugiyama, Kuriyama and Akhter 30 , Reference Tamakoshi, Lin and Kawado 32 – Reference Gardener, Rundek and Wright 34 ) in addition to total mortality. Unlike for deaths from CVD, many of the studies showed no association between cancer deaths and coffee consumption overall, while some studies showed a non-significant inverse trend( Reference Happonen, Läärä and Hiltunen 27 ) or significant inverse associations, but in only women( Reference Sugiyama, Kuriyama and Akhter 30 , Reference Tamakoshi, Lin and Kawado 32 ). Interestingly, a study conducted in Japan showed a reduced risk of death in women only for colorectal cancer, but not for other cancers. The inverse association for total mortality that we found in the meta-analysis seems to be influenced mostly by the reduced risk of deaths from CVD. It seems possible that coffee consumption protects against death from specific types of cancers, but not against total cancer deaths. This may be attributed to the aetiological heterogeneity of cancers when all types are grouped together, suggesting that the effect of coffee varies by cancer site. For example, recent epidemiological studies have shown stronger inverse associations of coffee consumption with the risk of liver cancer( Reference Sang, Chang and Li 55 ), endometrial cancer( Reference Je and Giovannucci 43 ) and colorectal cancer( Reference Tian, Wang and Hong 56 ), while no significant association with coffee consumption has been found for breast cancer( Reference Li, Ren and Qin 57 ). Thus, the overall effect may depend on the population rates for these specific cancers. The recent largest prospective US cohort study of the National Institutes of Health–American Association of Retired Persons (NIH-AARP) Diet and Health Study( Reference Lopez-Garcia, van Dam and Li 29 ) included in the present meta-analysis has shown inverse associations of coffee consumption with total and disease-specific deaths (including those from heart disease, respiratory diseases, diabetes and infections), but not with deaths due to cancers. In that study, inverse associations for total mortality were similar regardless of the predominant type of coffee consumed (caffeinated or decaffeinated) or across many subgroups. For cancer deaths, it is also possible that the residual confounding effects of smoking, alcohol or other unhealthy lifestyle factors related to coffee consumption may still exist, which are likely to obscure the beneficial effects of coffee consumption.
On the other hand, some factors related to health status may confound the association between coffee consumption and total mortality more inversely than the true association. There is a possibility that subclinical diseases lead to a reduction in coffee consumption, i.e. those in the lowest category of coffee consumption had more past disease history than those who were in the higher categories of coffee consumption, causing an elevation in risk among low/non-coffee drinkers. However, the risk estimate from the present meta-analysis limited to studies that had adjusted for health status( Reference Kahn, Phillips and Snowdon 16 , Reference Vandenbroucke, Kok and van 't Bosch 18 – Reference Rosengren and Wilhelmsen 20 , Reference Woodward and Tunstall-Pedoe 22 – Reference Jazbec, Simić and Corović 25 , Reference Happonen, Läärä and Hiltunen 27 – Reference Sugiyama, Kuriyama and Akhter 30 , Reference Tamakoshi, Lin and Kawado 32 – Reference Gardener, Rundek and Wright 34 ) was not attenuated, but remained essentially the same. A study conducted in Japan attempted to examine the reverse causation with exclusion of death that occurred within 2–8 years from baseline and did not alter the relationship between coffee consumption and all-cause mortality( Reference Tamakoshi, Lin and Kawado 32 ). Similarly, the large US cohort studies of NHS and HPFS conducted sensitivity analyses to evaluate the robustness of their inverse findings( Reference Lopez-Garcia, van Dam and Li29a,b ). They carried out several analyses by excluding individuals in the lowest category of coffee consumption, excluding those who reduced their coffee consumption in the 10 years preceding the study or excluding those who died within the first 4 years of follow-up. As a result of the analyses, all the estimates remained similar to those in the main analyses. The observed findings seem to suggest that the difference in health at baseline did not explain the observed inverse association.
We attempted to conduct an exploratory meta-analysis of total mortality in relation to decaffeinated coffee consumption, and the results showed similar inverse associations with no heterogeneity. The largest US cohort study indicated a significant inverse association for high coffee consumption ( ≥ 4 cups/d) v. no coffee consumption, but it was not included in the meta-analysis due to insufficient data( Reference Freedman, Park and Abnet 33 ). Another recent study carried out by Gardener et al. ( Reference Gardener, Rundek and Wright 34 ) reported a hazard ratio of 0·88 (95 % CI 0·88, 0·97) for consumption of one cup of decaffeinated coffee per day.
The present meta-analysis has several strengths. First, to the best of our knowledge, this is the first meta-analysis to investigate the long-term effect of coffee consumption on mortality. Second, all the studies included in the meta-analysis had a prospective design excluding recall and selection bias, which could be of concern in case–control studies. For practical and ethical reasons, the prospective design may be the best study design to investigate varying amounts of coffee consumption for a long period of time until many subjects die. Third, a large number of total cases were included in the meta-analysis, which increased statistical power to quantitatively assess the association of total mortality with coffee consumption. In addition, a relatively large number of studies allowed us to conduct subgroup analyses by geographical region, follow-up time, sex and confounder adjustment. Fourth, in addition to the large sample size, many of the studies had relatively long follow-up durations, which allowed observing the long-term effects of coffee consumption on mortality. Lastly, we found little evidence of publication bias, which could be of concern in a meta-analysis of published literature.
The present meta-analysis also has several potential limitations. First, a meta-analysis itself cannot solve confounding problems that could be inherent in the original studies, which may, in part, explain the observed findings. Usually, known and measured factors such as smoking status or alcohol consumption can be removed through statistical methods, as most of the studies included in the present meta-analysis did. All the studies adjusted for a strong confounder, smoking status, and the additional analysis carried out in the present meta-analysis limited to studies that had adjusted for at least alcohol consumption and BMI showed similar results. Nevertheless, we cannot rule out the possibility that unmeasured factors such as psychosocial factors associated with coffee drinking might have affected the inverse associations of coffee consumption and mortality. Since many people tend to use coffee shops as meeting places, those who report consuming coffee frequently are more likely to have a good social network. Thus, the effect of psychosocial factors related to coffee consumption should be assessed. Second, misclassification of coffee consumption categories may have occurred in the original analysis of each study and thus the meta-analysis, given that coffee consumption was assessed by self-report and, moreover, assessed at a single time point for most of the studies. Among the studies, two studies carried out in the USA for men (HPFS) and women (NHS) updated information on coffee consumption every 4 years during 18 and 24 years of follow-up, respectively( Reference Lopez-Garcia, van Dam and Li29a,b ). Except for the two studies, the others assessed coffee consumption at baseline only. However, misclassification of coffee consumption categories would have probably led to the underestimation, rather than to overestimation, of results, and thus the association between coffee consumption and risk of death may be even stronger. We found a slightly stronger inverse association in studies with relatively short follow-up durations. This may be related to less exposure misclassification in studies with short follow-up durations, which reduces the possibility of subjects altering their coffee consumption during follow-up. Third, the cut-offs for high exposure categories varied among the studies included in the meta-analysis, ranging from 2 to 9 cups/d. Even in the same geographical region, each country used different highest categories. For the highest categories of coffee consumption, studies carried out in Europe used >2–9 cups/d, those in the USA used 3–6 cups/d and those in Japan used 2–4 cups/d. We found no significant difference in the pooled RR stratified by cut-offs for the highest category (2–4 v. 5–9 cups/d), which might suggest that heavy coffee consumption ( ≥ 5 cups/d) seems not to provide further benefits against death compared with moderately high coffee consumption (2–4 cups/d). Of the studies included in the meta-analysis, two used 1 or 2 cups/d as a reference( Reference Jacobsen, Bjelke and Kvale 17 , Reference LeGrady, Dyer and Shekelle 19 ), and the other studies used 0 or < 1 cup/d as a reference. After the exclusion of the two studies, the pooled RR remained similar (RR 0·85, 95 % CI 0·79, 0·91). Finally, different brewing methods and varying cup sizes might have attenuated the results.
Conclusions
Both moderate coffee consumption and high coffee consumption were associated with significantly lower total mortality, compared with low/no coffee consumption. People who consumed ≥ 5–9 and ≥ 2–4 cups/d of coffee had similar risk reductions of mortality, suggesting little further benefits of heavy consumption of coffee with regard to death. Since research on coffee and disease has mostly focused on individual conditions and diseases, it might be meaningful to examine whether long-term coffee consumption can decrease the risk of death from a public health perspective. Indeed, due to the observational nature of the prospective cohort studies included in the meta-analysis, it is not possible to conclude that the inverse association between coffee consumption and mortality reflects cause and effect. However, based on the health benefits of coffee components (e.g. antioxidants including polyphenols), the relationship between coffee consumption and total mortality might be causal. Further large prospective studies that carefully adjust for all the potential confounders including factors related to social interaction should be conducted.
Supplementary material
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/S0007114513003814
Acknowledgements
The authors thank Youngyo Kim, B.S., a research assistant, for data management.
The present study was supported by a grant from the Kyung Hee University in 2012 (KHU-20121690). The sponsor had no role in the design or conduct of the study, collection, management, analysis, or interpretation of the data, or the preparation, review and approval of the manuscript.
The authors' contributions are as follows: Y. J. and E. G. were responsible for the study concept and design; Y. J. and E. G. acquired the data; Y. J. and E. G. analysed and interpreted the data; Y. J. drafted the manuscript; E. G. was responsible for the critical revision of the manuscript for important intellectual content; Y. J. obtained funding for the study; Y. J. carried out the statistical analyses. All the authors read and approved the final version submitted for publication.
None of the authors has any conflicts of interest to declare.






