Nutrition education interventions aim to help athletes align their dietary intake with current sports nutrition guidelines(Reference Alaunyte, Perry and Aubrey1,Reference Heaney, O’Connor and Michael2) . These interventions, incorporated into many elite institute, professional or collegiate sports programmes, vary widely from individual consultations to group education; some incorporate practical skills such as cooking or shopping(Reference Heaney, O’Connor and Michael2). Despite the time and cost associated with athlete education, there is limited information on how these nutrition interventions influence dietary intake. A number of reviews have evaluated the level of nutrition knowledge in athletes(Reference Heaney, O’Connor and Michael2,Reference Trakman, Forsyth and Devlin3) , and one published recently also reports on how this improves with nutrition education(Reference Tam, Beck and Manore4). Generally, the level of athlete nutrition knowledge varies widely amongst athlete groups(Reference Heaney, O’Connor and Michael2,Reference Trakman, Forsyth and Devlin3) , but improves, at least in the short term, even after brief nutrition education interventions(Reference Tam, Beck and Manore4). However, due to the wide range of knowledge assessment tools with limited validation, the authors were unable to identify the most effective nutrition education modality to improve nutrition knowledge in athletes(Reference Tam, Beck and Manore4).
Although it is often assumed that greater nutrition knowledge results in better dietary intake, evidence suggests other factors (e.g. taste, cost and convenience) are equally important(Reference Spronk, Kullen and Burdon5). Athletes may fail to meet their dietary intake due to the challenges in navigating specific barriers such as available time for food selection and preparation due to high daily training commitments, suppressed appetite between training sessions, food culture and traditions unique to their sport, religious or environmental considerations and the body composition and physique requirements required for success(Reference Alaunyte, Perry and Aubrey1,Reference Heaney, O’Connor and Michael2) . Observations made by coaches and sports dietitians indicate that athletes who possess confidence in their nutrition knowledge are more likely to incorporate this knowledge into their lifestyle by choosing appropriate foods to match their sport(Reference Alaunyte, Perry and Aubrey1,Reference Heaney, O’Connor and Michael2) . However, the effectiveness of different types of nutrition education interventions to promote change in the dietary intake of athletes has yet to be evaluated.
Therefore, the primary aim of this systematic review was to investigate the effectiveness of nutrition education interventions on change in dietary intake in athletes. The secondary aim was to compare the effectiveness of different education delivery modalities (e.g. group v. individual or in-person to virtual education modalities). Given the substantial professional and institutional investment in nutrition education for athletes, a comprehensive evaluation regarding its effectiveness to modify dietary intake is relevant to informing future best practice.
Methods
Search strategy
The systematic literature search to identify studies was conducted by one researcher (A. B.) from the earliest record until June 2019. Databases searched included PubMed, Embase, CINAHL and SPORTDiscus (EBSCOHost) using key words and controlled vocabulary, ‘athletes’, ‘sport’, ‘nutrition’, ‘diet’, ‘food’, ‘education*’, ‘programs*’, ‘counsel*’, ‘health education’, ‘intervention’, ‘strategy*’, ‘curriculum’, ‘lesson*’, ‘class’, ‘workshop*’, ‘program evaluation’, ‘dietary intake’, ‘energy intake’, ‘energy balance’, ‘behav*’, ‘feeding behavior’, ‘intake*’, ‘consumption’, ‘habits’, ‘patterns’, ‘practices’, ‘dietetics’, ‘food habits’, ‘caloric intake’. The full electronic search strategy is presented in online Supplementary Fig. S1. The search strategy was complemented by a hand search of studies referenced in similar reviews and included studies. This systematic review was registered on Prospero (CRD42018083952) and reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines(Reference Moher, Shamseer and Clarke6).
Eligibility criteria
Eligible study designs included randomised controlled trials, quasi-experimental and pre-post intervention studies. Abstracts and studies not reported in English were excluded. Studies of athletes, male and female aged between 12 and 65 years from all sports, and athletic levels were eligible for inclusion. Interventions including individual/group counselling/education, in-person or virtual (e.g. online/DVD) modalities were eligible if the primary outcome, change in dietary intake (energy, macronutrients, micronutrients and/or food groups, diet quality/index) was reported quantitatively.
Selection of studies and data extraction
After the search was conducted and duplicates removed, manuscript titles and abstracts were screened independently by two authors (A. B. and R. T.). Disagreements were resolved via discussion with a third author (G. C.). Full texts of all potentially eligible studies were reviewed independently by two authors (A. B. and R. T.). After identification of eligible full-text articles, data were extracted in duplicate (A. B. and R. T.). When relevant, paper authors were contacted (A. B.) and requested to supply additional/missing information. A computer program (WebPlotDigitizer, version 3.9) was used to calculate the mean and standard deviation of data reported in figures(Reference Rohatgi7).
Nutritional information extracted pre- and post-intervention included mean energy (kJ), macronutrient (g), micronutrient (mg/µg), food group(Reference Rohatgi7) and KIDMED diet quality/index (score of +1 or −1 totalling to a maximum 12)(Reference Rohatgi7). All nutrients were converted to SI units if reported otherwise. To manage table size in this review, only the micronutrients Fe and Ca were tabulated. Changes to other micronutrients were discussed only in the text. To compare changes, within- and when relevant, between-group (double-arm studies) effect size (ES) was calculated when relevant data (mean, sd or sem) were provided. The Hedges’ g (random model) ES was calculated using extracted data (mean, sd, sample size) in the Comprehensive Meta-Analysis version 2 software (Biostat, 2005), and were considered trivial (0·0–0·19), small (0·2–0·49), moderate (0·5–0·79) or large (≥0·8)(Reference Cohen8).
Calculation of energy, macronutrient and micronutrient values across studies
To assess the adequacy of reported dietary intakes, the recommended food group or recommended dietary intake (RDI)/RDA guidelines specific to the country were used, and for studies using diet quality/indexes, the recommended ranges for these parameters cited in the paper (a sixteen-item Mediterranean diet quality index). To assess the adequacy of energy intake, the types of methodology used to determine the estimated energy requirement (EER) of the participants could range from published energy requirement algorithms, general population energy requirement recommendations for ‘active’ or ‘very active’ individuals, or literature reported values for the sport/activity.
The classification of adequacy for macronutrients varied depending on the specific guidelines used in the paper. Historically, scientific opinion on this ranged over the period of time the studies were conducted, initially being recommended as a proportion of daily energy (protein 10–15 %; fat 20–30 % and carbohydrate ≥50–60 % of daily energy intake), later recognition that g/kg per d recommendations were more appropriate (protein 1·0–2·0 g/kg per d and carbohydrate 3–12 g/kg per d(Reference Thomas, Erdman and Burke9)). Where possible, g/kg per d calculations were undertaken if not reported in the paper to assist in evaluating the appropriateness of the older, percentage of energy recommendations. Micronutrient adequacy was based on the respective country RDI/RDA values. Historically, mean intakes which did not meet the RDI/RDA, but were a set proportion ranging between 70 and 100 % of the RDI/RDA for micronutrients were reported as ‘likely’ to be adequate in older nutrition literature, although this is not an established way of reporting dietary adequacy.
Quality assessment
Study quality was independently assessed in duplicate by three researchers (A. B. all papers, H. O. and R. T. shared) using a modified version of the Downs and Black risk of bias rating tool(Reference Downs and Black10). The original tool consists of twenty-seven items that examine data reporting, external and internal validity, including bias and statistical power. In single-arm study designs, twenty of the twenty-seven items that logically applied were used. In double-arm study designs, twenty-four items were used. Item 18 addressed the validity and reliability of the tools used to measure dietary intake. This item was assessed as two parts as previously described by Spronk et al. (Reference Spronk, Kullen and Burdon5), where one point was awarded for appropriate choice of dietary method and another point for appropriate application. This approach was adopted with consideration of items 7·2–7·5 in the Academy of Nutrition and Dietetics Quality Criteria Checklist to accompany the Downs and Black tool and allowing for clarification when assessing quality ratings. Downs and Black score ranges were provided with corresponding quality levels based on the scoring methodology of the Downs and Black checklist. Quality levels for single-arm studies included: excellent (20–21), good (15–19), fair (12–14) and poor (<12) and for double-arm studies excellent (23–25), good (18–22), fair (14–17) and poor (<14). The maximum scores were 21 and 25 for single-arm and double-arm studies, respectively. Disagreement between authors was discussed to achieve consensus.
Results
Literature search and study selection
A total of 8004 articles were identified through the database search. After removal of duplicates, 6285 articles remained. Screening by title and abstract identified thirty-six articles for full-text review. After evaluation against inclusion and exclusion criteria, twenty-one articles were eligible for inclusion (Fig. 1). One additional article was identified by hand-searching references of included papers.
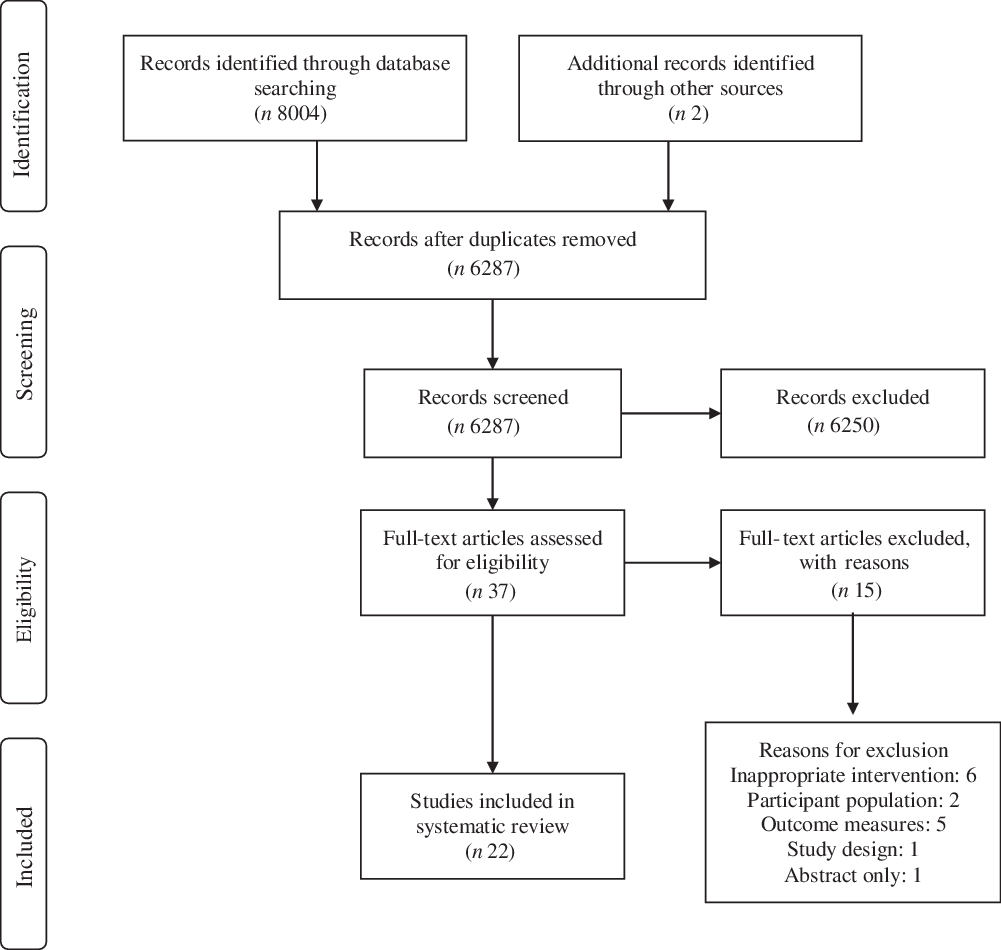
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart.
Study characteristics
Study characteristics were summarised into single-arm (intervention group only) and double-arm (intervention and control groups) studies (Table 1). The sample size across all studies ranged from 7 to 210 athletes (80·5 % female). Studies were conducted in the USA (n 14), Europe (n 5), Iran (n 1), Malaysia (n 1) and Brazil (n 1). The majority of studies involved mixed sports (n 9), with one of these mixed sport studies involving two population groups (mixed sport and ballet dancers). Team sports were represented in seven studies including volleyball (n 3), soccer, baseball, softball and handball (n 1 for all). Individual sports included swimming, ballet, track and field, canoeing and wrestling (n 1 for all). The mean age of athletes across all studies was 19·8 years. Athletic calibre included high school (n 3 studies), collegiate (n 4 studies), state (n 1 studies), national (n 10 studies) and international (n 4 studies) levels. Two studies involved athletes with physical disabilities(Reference Rastmanesh, Taleban and Kimiagar11,Reference Kandiah12) .
Table 1. Participant, intervention and dietary analysis characteristics of included studies: single-arm and double-arm studies
(Mean values and standard deviations)
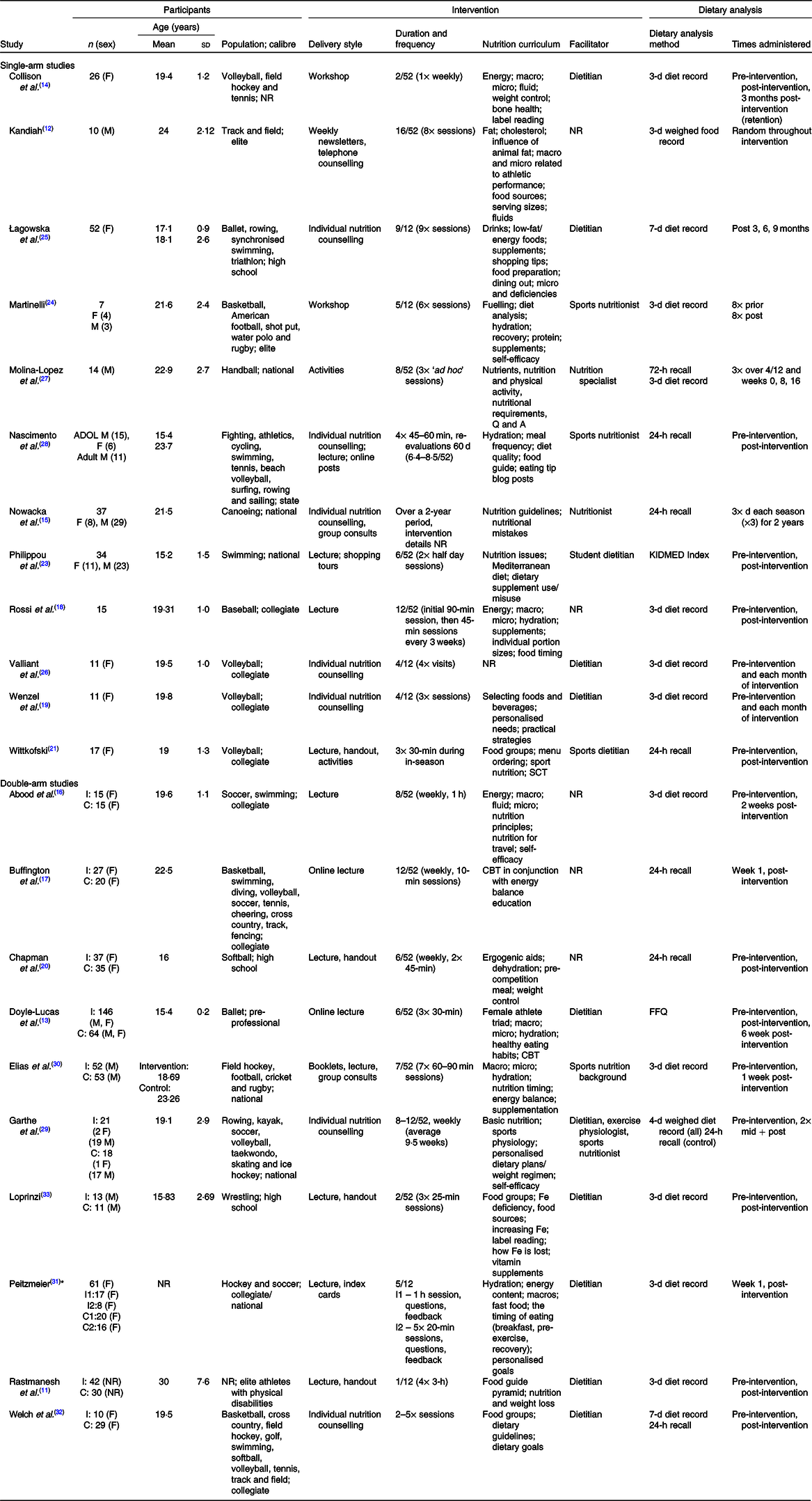
F, female; NR, not recorded; macro, macronutrients; micro, micronutrients; M, male; ADOL, adolescents; KIDMED Index, Mediterranean Diet Quality Index; SCT, social cognitive theory; I, intervention group; C, control group; CBT, cognitive behavioural theory.
* Peitzmeier(Reference Peitzmeier31) assessed two intervention and two control groups.
Intervention characteristics
Nutrition education modality
Various nutrition education modalities were utilised across the twenty-two included studies. Face-to-face group lectures (n 8 studies) and individual nutrition counselling (n 6) were most commonly used. Other modalities included group workshops/activities (n 4) or mixed methods (n 5), including lectures and handouts or lectures and individual counselling.
Nutrition education topics
Half of the studies (n 11) incorporated a combination of nutrition topics including energy, macronutrient, micronutrient and hydration principles; meal frequency and timing; and supplement use. Other topics incorporated food groups and dietary guidelines (n 2), nutrient recommendations (n 1), general sport nutrition principles (n 1), Fe (n 1), Mediterranean diet principles (n 1), and individual nutrition plans or weight control strategies (n 3). Self-efficacy, social cognitive or cognitive behavioural theory concepts to assist the athletes to make dietary change were included in 6/22 studies(Reference Doyle-Lucas and Davy13,Reference Collison, Kuczmarski and Vickery14) .
Duration and frequency of nutrition education
The nutrition education interventions ranged from 2 to 39 weeks in duration, with two studies (one single-arm, one double-arm) incorporating a follow-up period (6–16 weeks) and reported retention of dietary changes(Reference Doyle-Lucas and Davy13,Reference Collison, Kuczmarski and Vickery14) . One study assessed athlete dietary intake changes across two seasons, with the education delivered during the second season, however failed to describe the duration and frequency of the education programme(Reference Nowacka, Leszczyńska and Kopeć15). Session number varied from three (3/22 studies), 4–7 (13/22 studies), to more than seven (6/22 studies) sessions across the intervention period. Session duration ranged from 10 to 120 min with total intervention time ranging from 60 to 720 min.
Nutrition education facilitator
Most of the interventions (17/22) were delivered by a qualified (or student) nutrition professional with expertise described as, ‘dietitian’ (n 10), ‘sports or performance nutritionist/dietitian’ (n 4), ‘nutrition specialist/professional nutritionist’ (n 2) and student dietitian (n 1). The remaining studies (5/22) failed to report facilitator expertise(Reference Kandiah12,Reference Abood, Black and Birnbaum16–Reference Rossi, Landreth and Beam18) .
Diet methodology characteristics
Most studies (15/22) assessed dietary intake twice, immediately pre- and then post-intervention, with some (5/21) studies also conducting assessments during the intervention (data not extracted). Two studies did not disclose the number of dietary intake assessment sessions but did present pre- and post-intervention results(Reference Nowacka, Leszczyńska and Kopeć15,Reference Wenzel, Valliant and Chang19) . All studies utilised a valid diet method to collect nutrient intake; however, only 10/22 studies appropriately applied the methodology (i.e. appropriate sample size, population, duration, frequency and nutrients assessed)(Reference Nowacka, Leszczyńska and Kopeć15,Reference Wenzel, Valliant and Chang19–Reference Wittkofski21) .
Study quality
Methodological quality had a mean score of 12/21 (range 7–15) for single-arm studies and a mean score of 15/25 (range 11–20) for double-arm studies, representing poor study quality and fair study quality for single- and double-arm studies, respectively (online Supplementary Tables S1 and S2). Most reported their aims (21/22 studies), main outcomes (18/22 studies), described the main findings (19/22 studies) and used appropriate statistical tests (15/22 studies). The lowest ratings were for the recording of compliance to the education intervention and collection of dietary intake (5/22 studies). Ten of the studies appropriately applied the dietary methodology with limitations in application mostly due to small participant numbers and inappropriate measurement and number of collection days for specific micronutrients. For example, Fe intake was reported after only 3-d of measurement in a food diary that requires up to eleven recording days(Reference Capling, Beck and Gifford22).
Single-arm studies dietary outcomes
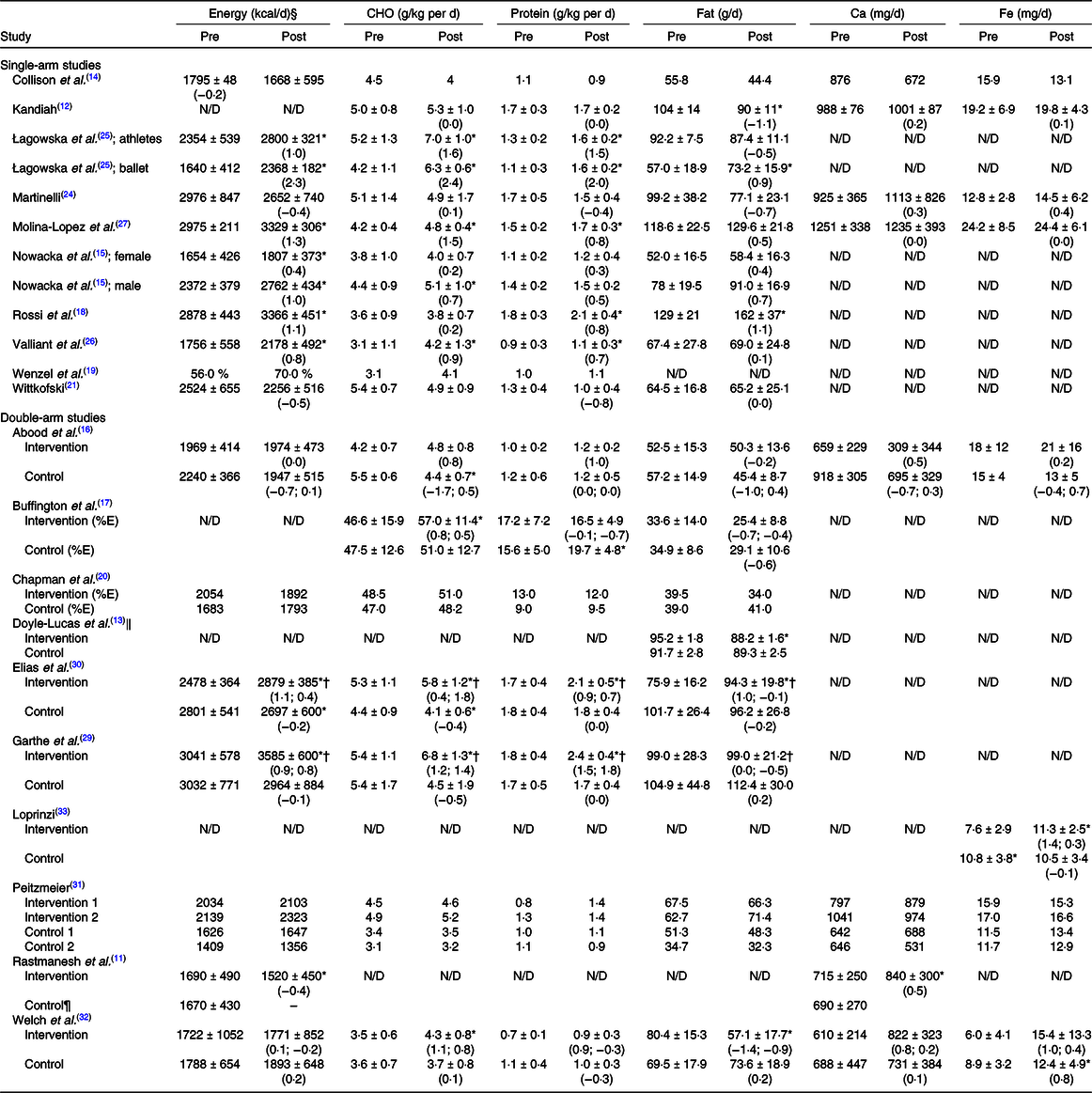
The single-arm studies (n 12) investigated the within-group changes in dietary intake pre- and post-nutrition intervention (Table 2). Of these studies, 9/12 reported changes in energy intake and 10/12 changes in macronutrients using predominantly 3-d diet records (n 6 studies), with a smaller number using 7-d diet records (n 1 study), 24-h recall (n 2 studies) or 72-h recall (n 1 study). Micronutrient intake was reported in 4/12 studies using predominantly 3-d diet records (n 3 studies) and one using 24-h recall (n 1 study). In 3/12 single-arm studies, food group intake was assessed(Reference Philippou, Middleton and Pistos23). Adherence to the Mediterranean diet using a diet index (KIDMED) was assessed in 1/12 studies(Reference Philippou, Middleton and Pistos23).
Table 2. Nutrient intake pre- and post-nutrition education for included single-arm and double-arm studies‡
(Mean values and standard deviations; mean values with their standard errors)
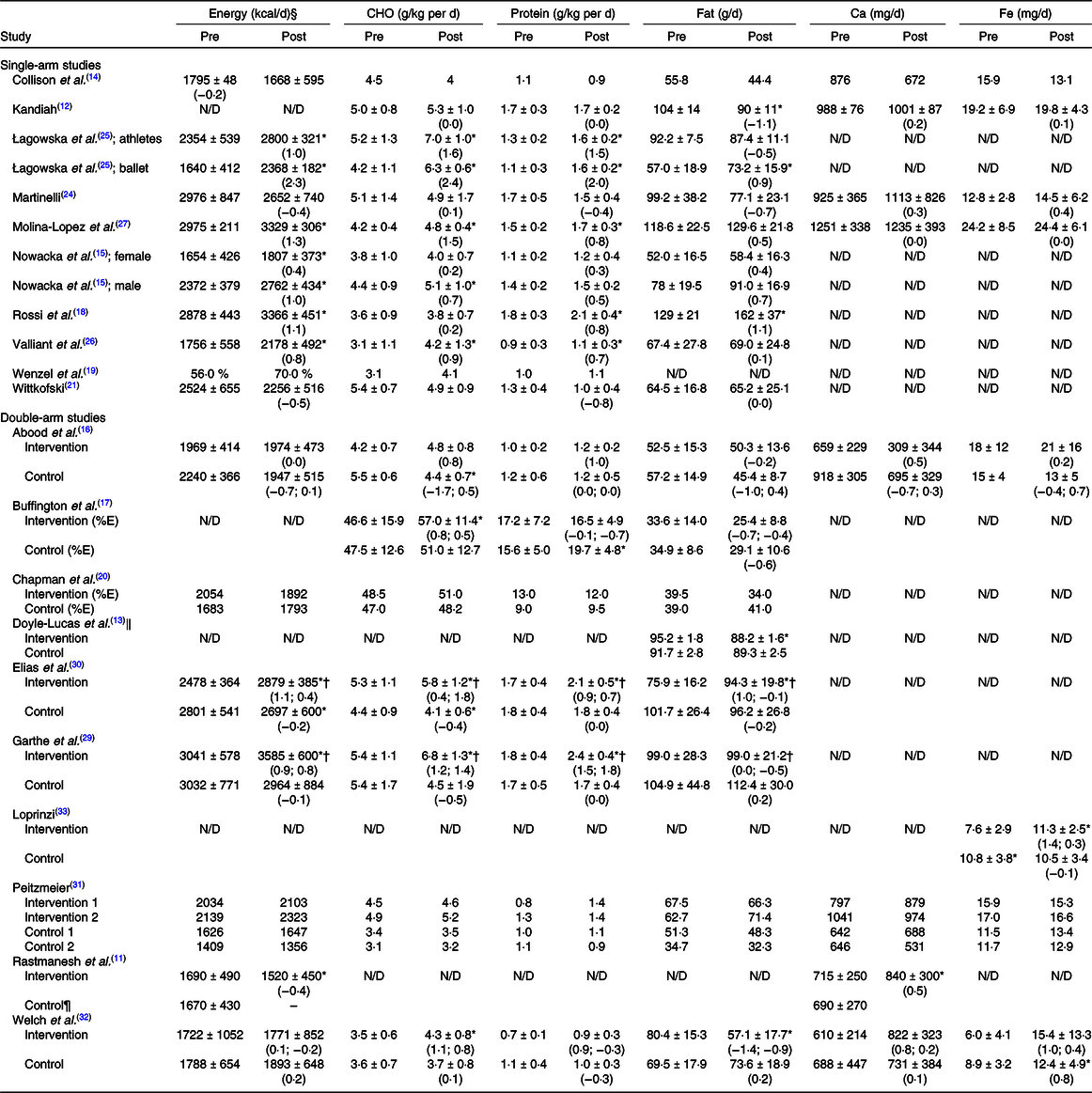
CHO, carbohydrate; N/D, not defined; %E, percentage energy.
* Significant within-group (pre-post) difference (P < 0·05).
† Significant between-group (post-intervention) difference (P < 0·05).
‡ Results presented as mean values and standard deviations (within-group effect size; between-group effect size), where available.
§ To convert kcal to kJ, multiply by 4·184.
‖ Presented as mean values with their standard errors.
¶ No post-intervention assessment conducted.
Baseline dietary intakes did not always meet the nutrition targets identified by the researchers which were guided by their country’s RDI/RDA or relevant sports nutrition literature at the time. In the case of energy, a range of methods were used to identify the appropriate EER for the athlete population investigated. This included the use of general population-based energy requirements typically identifying a range of suitable energy intakes for ‘active’ or ‘very active’ individuals. Other studies used algorithms (e.g. Harris–Benedict or Nelson equations) or sport-specific energy requirements reported in the literature to calculate the appropriate level of energy for the study population (based on age, sex, weight and height). Training loads of participants were only detailed in 2/9 studies assessing energy intake, contributing to the poor quality of studies since training information is essential to evaluate athlete energy requirements(Reference Thomas, Erdman and Burke9).
Few (2/9) single-arm studies that assessed energy intake reported this to be within the researchers’ targeted EER at baseline(Reference Wittkofski21,Reference Martinelli24) . Of those studies identified as having a low mean participant energy intake at baseline, 6/7 reported a significantly higher post-intervention energy intake (ES 0·4–2·3; P ≤ 0·05), with only one(Reference Łagowska, Kapczuk and Jeszka25) falling within the researchers’ identified EER. The ES ranged from small to large. It is relevant to note that the study by Łagowska et al. (Reference Łagowska, Kapczuk and Jeszka25) involved both ballet dancers and female-athlete sub-groups, and although both observed significant increases and large ES, only the female-athlete sub-group met energy intakes within researchers’ range post-intervention (ES 1·0–2·3; P ≤ 0·001). Conversely, the remaining study (1/7) with low baseline energy intake reported a close to significant decrease further below the researchers identified EER post-intervention (ES −0·2; P = 0·05)(Reference Collison, Kuczmarski and Vickery14). All 7/9 studies where authors reported low baseline energy intakes assessed female athletes, with 1/7 including mixed-sex athletes(Reference Nowacka, Leszczyńska and Kopeć15). In 2/9 studies where authors reported energy intake met the EER at baseline, both reported non-significant decreases which fell below the targeted EER post-intervention (ES −0·4 to −0·5)(Reference Wittkofski21,Reference Martinelli24) .
Carbohydrate intake was assessed in 10/12 single-arm studies. At baseline, mean carbohydrate intake was deemed to be appropriate by the researchers’ (>50 % of energy or 6–10 g/kg per day) for the study population assessed in only 2/10 studies(Reference Collison, Kuczmarski and Vickery14,Reference Wittkofski21) . In the 8/10 studies where carbohydrate intake was identified to be below requirements at baseline, the range in mean intake (when able to be calculated) was 3·1–5·2 g/kg per d. Post-intervention, this increased to 3·8–7·0 g/kg per d, with 4/8 studies reporting significant increases in carbohydrate intake (ES 0·7–2·4; P < 0·05), yet still falling below the researchers’ recommendations. In the 2/10 studies deemed to have adequate carbohydrate intake at baseline based on percentage of energy, no significant changes in intake were observed post-intervention(Reference Collison, Kuczmarski and Vickery14,Reference Wittkofski21) .
Protein intake was reported in 10/12 single-arm studies and was deemed adequate according to author recommendations in 5/10 studies at baseline (1·1–1·7 g/kg per d, when able to be calculated)(Reference Nowacka, Leszczyńska and Kopeć15,Reference Rossi, Landreth and Beam18) . In the remaining studies identified as having inadequate protein intake at baseline, three also reported protein as inadequate post-intervention (1·1–1·6 g/kg per d), while the other two studies reported small to large increases to meet the targeted protein intake, ranging between 1·2 and 2·1 g/kg per d (ES 0·2–0·8)(Reference Nowacka, Leszczyńska and Kopeć15,Reference Rossi, Landreth and Beam18) . In the 5/10 studies reporting adequate protein intake at baseline, 4/5 studies maintained an adequate protein intake post-intervention between 0·9 and 1·7 g/kg per d, while one study reported a large reduction post-intervention, falling to the lower limit of the researchers’ recommendations (1·0 g/kg per d; ES −0·8)(Reference Wittkofski21).
Dietary fat intake was reported in 9/12 single-arm studies. Of these, 5/9 were reported at baseline to exceed researchers’ recommendations (20–30 % of energy), with the remaining four meeting this recommendation at 23–28 % of energy(Reference Collison, Kuczmarski and Vickery14,Reference Nowacka, Leszczyńska and Kopeć15,Reference Wittkofski21,Reference Łagowska, Kapczuk and Jeszka25) . Post-intervention, 3/5 studies that exceeded baseline recommendations reported non-significant decreases which fell within the recommended 20–30 % of energy(Reference Kandiah12,Reference Martinelli24,Reference Valliant, Emplaincourt and Wenzel26) , while the remaining two studies still exceeded 30 % of energy post-intervention(Reference Rossi, Landreth and Beam18,Reference Molina-Lopez, Molina and Chirosa27) .
Fe and Ca were reported in 4/12 single-arm studies, with each of these meeting the researchers’ targeted recommendation of >70 % of the RDI/RDA at baseline. Two of these four studies reported non-significant increases for Fe and Ca post-intervention (ES: Fe 0·1–0·4; Ca 0·2–0·3)(Reference Kandiah12,Reference Martinelli24) . The remaining 2/4 studies showed no change in Fe intake(Reference Collison, Kuczmarski and Vickery14,Reference Molina-Lopez, Molina and Chirosa27) , and a decrease in Ca intake to <70 % of the RDI/RDA(Reference Collison, Kuczmarski and Vickery14). However, due to the fair quality of dietary methodology used for micronutrient assessment, these findings are questionable. Other micronutrients reported in 3/4 studies showed mostly adequate intakes at baseline and insignificant changes post-intervention(Reference Martinelli24,Reference Molina-Lopez, Molina and Chirosa27) . One study examined intake of dietary fibre, vitamin C and dietary cholesterol, with dietary cholesterol showing a significant reduction post-intervention(Reference Kandiah12).
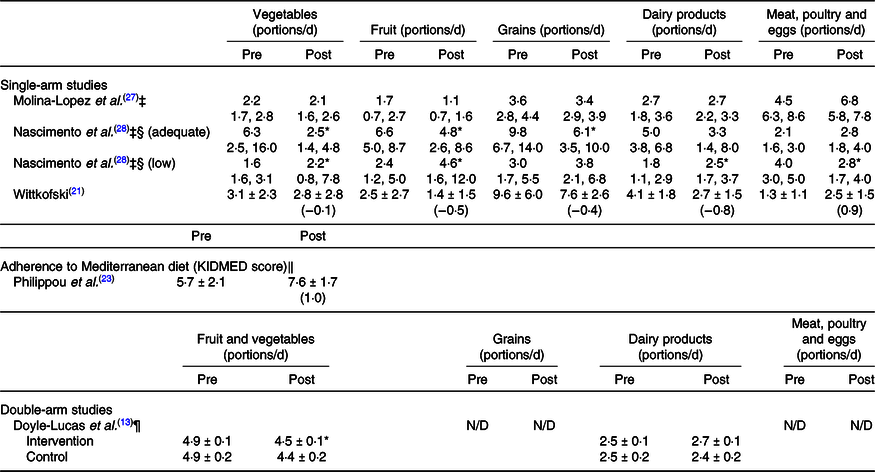
Change in food group consumption and adherence to the Mediterranean diet were assessed in 3/12 and 1/12 single-arm studies, respectively. One of the studies assessing food group consumption(Reference Nascimento, Silva and Ribeiro28) reported athletes (adults and adolescents) as low, adequate or high at baseline and post-intervention based on the Brazilian Food Pyramid Guide. A significant reduction post-intervention in vegetable, fruit and grain intake was reported in athletes classified as adequate at baseline for these food groups (P < 0·05), falling below recommended intakes for vegetables. No significant changes were reported for dairy, or meat and egg intake. For athletes classified as low intake for vegetables, fruit and dairy, significant increases were reported for these food groups (P < 0·05), achieving the recommended intake for fruits. A significant reduction in meat and egg intake was observed in athletes classified as high intake at baseline (P < 0·05); however, these athletes remained above recommended intakes for this food group. No significant change in grain intake was observed in those classified as low at baseline(Reference Nascimento, Silva and Ribeiro28). Another study assessing food groups(Reference Wittkofski21) reported participants met grains, vegetable and fruit groups at baseline, whilst dairy was reported as lower and meat serves higher than recommendations. Non-significant decreases were reported for vegetable, fruit and grain food groups post-intervention. Meat serves decreased to within the recommended intake (2·7 serves), while a large increase in milk intake to within the recommended range was observed post-intervention (2·5 serves; ES 0·9)(Reference Wittkofski21). The remaining study assessing food groups reported low fruit and grain intake, and high meat, poultry and egg intake, pre-intervention. These food groups remained outside of recommended intakes post-intervention(Reference Molina-Lopez, Molina and Chirosa27). One study investigated adherence to the Mediterranean diet, reporting a large increase in adherence post-intervention (ES 1·0)(Reference Philippou, Middleton and Pistos23).
Double-arm studies dietary outcomes
In the double-arm studies (n 10), energy intake was assessed in 7/10 studies, where 5/7 used 3–4-d food records, and 2/7 used 24-h recall (one study also used a 7-d food record). Macronutrients were measured in 8/10 studies (7/8 measuring carbohydrate and protein, and 8/8 dietary fat), where 4/8 used 3–4-d food records (one of these also used a 24-h recall), and 4/8 used 24-h recalls (two of these combined this with a 4- or 7-d food dairy). One study measured food groups in addition to dietary fat using an FFQ(Reference Doyle-Lucas and Davy13). Micronutrients were measured in 5/10 studies, using predominantly 3-d food records, with one study using a 7-d food record in addition to the 24 h recall. Identification of nutrition targets was similar to the single-arm studies. Other micronutrients reported in 3/10 studies showed mostly adequate intakes at baseline and insignificant changes post-intervention.
The control groups in the double-arm studies received no placebo or sham intervention and generally only experienced minimal, non-significant within-group changes to dietary intake. There were generally more positive changes in dietary intake within the intervention groups, although not all changes were significant or in the direction targeted. Within- and between-group changes in dietary intake are presented in Table 3. Sufficient information was provided in 6/10 double-arm studies to perform between-group analyses(Reference Garthe, Raastad and Refsnes29,Reference Elias, Saad and Taib30) , with 4/10 failing to provide sufficient data, reducing study quality(Reference Rastmanesh, Taleban and Kimiagar11,Reference Doyle-Lucas and Davy13,Reference Chapman, Toma and Tuveson20,Reference Peitzmeier31) .
Table 3. Diet quality pre- and post-nutrition education for included single-arm and double-arm studies†
(Mean values and standard deviations; mean values with their standard errors; mean values and 95 % confidence intervals)
N/D, not defined.
* Significant within-group (pre-post) difference (P < 0·05).
† Results presented as mean values and standard deviations (within-group effect size; between-group effect size), where available.
‡ Presented as mean values and 95 % confidence intervals.
§ Nascimento et al. (Reference Nascimento, Silva and Ribeiro28) classified participants as adequate or low based on meeting recommended food portion number (or adequate and high for meat and eggs).
‖ Adherence to the Mediterranean diet is described as poor (score: 0–3), medium (score: 4–7) or good (score: 8–12).
¶ Presented as mean values with their standard errors.
Energy intake was compared between-groups in 4/10 studies. Energy intake was significantly increased relative to control in two studies (ES 0·4–0·8; P < 0·05)(Reference Garthe, Raastad and Refsnes29,Reference Elias, Saad and Taib30) , while trivial, non-significant between-group differences in energy intake were observed post-intervention in two studies (ES −0·2 to 0·1; P > 0·05)(Reference Abood, Black and Birnbaum16,Reference Welch, Zager and Endres32) .
Moderate to large increases in carbohydrate intake relative to control were reported in three (ES 0·5–0·8; P > 0·05)(Reference Abood, Black and Birnbaum16,Reference Buffington, Melnyk and Morales17,Reference Welch, Zager and Endres32) , and a significant, large increase reported in two studies (ES 1·4–1·8; P < 0·05)(Reference Garthe, Raastad and Refsnes29,Reference Elias, Saad and Taib30) . Similar variability was reported across studies with protein intake post-intervention. Two studies reported increases in intake relative to control (ES 0·7–1·8)(Reference Garthe, Raastad and Refsnes29,Reference Elias, Saad and Taib30) ; two others reported small to moderate reductions relative to control (ES −0·3 to −0·7)(Reference Buffington, Melnyk and Morales17,Reference Welch, Zager and Endres32) . One study reported no between-group difference (ES 0·0)(Reference Abood, Black and Birnbaum16). A moderate increase in fat intake relative to control was reported in one study (ES 0·4)(Reference Abood, Black and Birnbaum16), while trivial to large reductions relative to control were found in four studies (ES −0·1 to −0·9)(Reference Buffington, Melnyk and Morales17,Reference Garthe, Raastad and Refsnes29,Reference Elias, Saad and Taib30,Reference Welch, Zager and Endres32) ). Between-group differences in Ca intake were reported in 2/10 studies(Reference Abood, Black and Birnbaum16,Reference Welch, Zager and Endres32) , with small increases reported in both studies (ES 0·2–0·3). Small to moderate increases in Fe intake compared with control were reported in three studies (ES 0·3–0·7)(Reference Abood, Black and Birnbaum16,Reference Welch, Zager and Endres32,Reference Loprinzi33) .
The remaining four double-arm studies did not conduct between-group analyses or did not provide sufficient information for ES to be calculated, contributing to the poor study quality and difficulty in drawing firm conclusions. Within-group analysis was performed in one of these studies, indicating a moderate reduction in energy intake (ES −0·4), and a moderate increase in Ca intake (ES 0·5), post-intervention(Reference Rastmanesh, Taleban and Kimiagar11).
Discussion
This is the first systematic review to evaluate the effectiveness of nutrition education programmes on the dietary intake of athletes. Overall, the impact of nutrition education programmes was varied. Given the range of intervention modalities and durations, the limitations in the dietary assessment methodologies employed and the small number of studies conducting intervention-control comparison analyses, it is difficult to make firm conclusions as to the efficacy of the interventions or which interventions were best. Study quality was rated poor to fair-range, also indicating room for methodological improvement. Despite the significant investment in nutrition education of athletes, there is limited and generally low-quality evidence of the efficacy of interventions. Well-designed and rigorous research application is needed in this area to inform future best practice.
Of the twenty-two studies, more than half (n 12) had a single-arm design which assessed dietary intake pre- and post-intervention (Table 1). While there was some evidence of intervention benefit, many of the ES were trivial or small and not statistically significant (Tables 2 and 3). Carbohydrate intake in particular often failed to meet the researchers’ set targets, although with the age of the studies, many of these recommendations were outdated and likely inappropriate for the sports assessed(Reference Thomas, Erdman and Burke9). Remarkably, intervention time was only able to be calculated for 3/12 studies and ranged from 180–300 min (3–5 h), across a 2- to 39-week duration.
In the double-arm studies (Table 1), none of the control arms used an alternative or ‘sham’ intervention to manage differences in group attention. Control groups generally experienced minimal changes; however, a limitation present in several studies was the failure to perform analysis between intervention and control groups (4/10 studies). Analysis was primarily conducted within-groups and rendered the use of the control group to qualitative comparison only. Across the double-arm studies, only 2/10 reported consistent, significant dietary improvements with ES in the large range(Reference Garthe, Raastad and Refsnes29,Reference Elias, Saad and Taib30) . The remaining double-arm studies demonstrated inconsistent dietary outcomes, with calculated ES varying in both direction and magnitude. Aligning with the single-arm study results, carbohydrate intake often failed to reach the researchers’ targeted levels, although these may have been too high for the sports assessed(Reference Thomas, Erdman and Burke9). In several instances, the control group outperformed the intervention group with respect to increasing nutrient intake. Most (9/10) double-arm studies provided sufficient detail on the intervention time which ranged from 60 to 720 min (1–12 h) over 2–12 weeks.
Across all studies, most of the interventions focused on face-to-face group education, with some studies using resources such as handouts or emails to participants, and others using individual consults and meal plans. Most of the facilitators appeared to have training in nutrition/dietetics, although facilitator background/qualifications were not always provided. The heterogeneity of these factors in addition to the range in approaches used to assess dietary outcomes makes it impossible to discern the overall effectiveness of interventions, nor which interventions are superior for improving dietary intake in athletes.
Given the heterogeneity and limited quality of the included studies in this review, few conclusions can be drawn as to the effect of nutrition education on dietary practices of athletes. A summary table in the form of a checklist has been constructed by authors to aid discussion of relative strengths and limitations of included studies (Table 4). This aims to succinctly critique the common flaws observed, while also guiding future nutrition education research. The checklist, Dietary Intake and Nutrition Education Reporting for Sports, outlines factors which would inform stronger study design, methodology and reporting. Appraisal of the literature included in this review identified four areas common to nutrition education intervention studies which require attention: participant characteristics, targeted dietary outcomes of the intervention (and underpinning rationale), intervention characteristics and dietary methodology. These areas are described below, and in further detail in online Supplementary Table S3.
Table 4. Study design, methodology and reporting summary checklist of included studies (n 22), Dietary Intake and Nutrition Education Reporting for Sports (DINERS) checklist
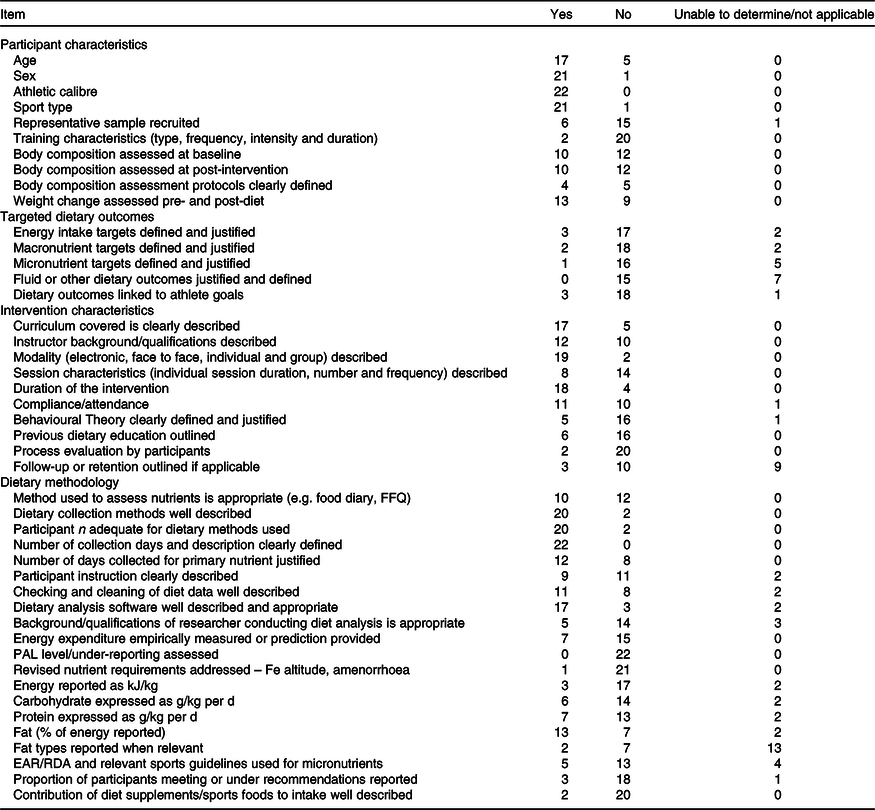
PAL, physical activity level; EAR, Estimated Average Requirement.
Participant characteristics
Adequate participant description is necessary as different interventions may be more efficacious at different age stages or levels of athletic calibre. While most studies in this review reported age and variance (17/22), sex (21/22), sport (21/22) and athletic calibre (22/22), only two studies adequately described training characteristics (inclusive of frequency, intensity, duration and type)(Reference Thomas, Erdman and Burke9). Detailed training information is necessary to evaluate athlete energy and nutrient requirements(Reference Thomas, Erdman and Burke9). Moreover, to make sense of current nutrition guidelines, body weight and composition is important, especially how these may change over the intervention period. Only ten and thirteen studies reported on body composition and body weight, respectively. Detailed protocols and error (e.g. technical error of measurement) associated with the assessment of body composition are also an important inclusion in the methods of the paper. Only four papers in this review provided such information(Reference Thomas, Erdman and Burke9).
Targeted dietary outcomes of the intervention
Defining intervention targets and desired dietary outcomes is essential for assessing intervention impact. Energy, macronutrient and micronutrient targets were defined and justified by only three(Reference Thomas, Erdman and Burke9), two(Reference Thomas, Erdman and Burke9) and one(Reference Thomas, Erdman and Burke9) studies, respectively. Given athlete dietary goals can vary over a season or even a training period, the goals of the athletes may warrant lower or higher intake of energy, macronutrients or micronutrients, which needs to be explained with a clear underpinning rationale provided(Reference Jeukendrup34).
Intervention characteristics
Intervention characteristics should be transparent. Details on the curriculum covered (17/22), the facilitator background and experience (12/22), modality of intervention used (individual or group, in-person or virtual) (19/22), as well as session duration, frequency and the total number of sessions (7/22) were not covered comprehensively across studies(Reference Jeukendrup34). The total amount of intervention minutes/hours should be provided. Participant attendance and compliance are also important and only half (11/22) of the studies examined these parameters. Underpinning behavioural theory and techniques are critical(Reference Teixeira and Marques35). Clearly, there is a robust body of research outlining how behavioural support is needed to facilitate dietary change, yet many of the studies did not describe use of these methods. Process evaluation including how the participants perceived the intervention is important for determining how well the intervention was received, and this was only examined in two studies. Lastly, sustained dietary change is also relevant when evaluating intervention efficacy, and only three of the included studies assessed this(Reference Rumbold, St Clair Gibson and Stevenson36,Reference Magkos and Yannakoulia37) . Clearly, financial or resource limitations may make follow-up after the intervention challenging.
Dietary methodology
A number of the included studies did not appropriately apply dietary methodology to their population, for example, 3–4-d food diaries are insufficient to examine intakes of micronutrients(Reference Basiotis, Welsh and Cronin38). In this case, combining methods such as using a FFQ for micronutrients with a food diary, which is better for quantifying energy and macronutrients, is recommended(Reference Rumbold, St Clair Gibson and Stevenson36,Reference Magkos and Yannakoulia37) , although the level of agreement of FFQ is limited at the individual rather than group level(Reference Fogelholm and Lahti-Koski39). The plausibility of data is also important, and potential under-reporting should be assessed(Reference Capling, Beck and Gifford22). This requires capture of training loads; technology such as accelerometers, heart rate monitors or Global Positioning System trackers may be helpful as doubly-labelled water is unlikely to be available or affordable in most situations(Reference Capling, Beck and Gifford22). Another major flaw in included papers was the reporting of mean intakes of energy and macronutrients which may be skewed by athletes with extremely high or low intakes(Reference Heaney, O’Connor and Gifford40). While mean intake can be useful, it is stronger to report the proportion of participants who reach the dietary targets as this facilitates a better assessment of intervention effectiveness in the cohort(Reference Heaney, O’Connor and Gifford40). Similarly, in the case of micronutrients, it would be useful to not only check the proportion of participants meeting the Estimated Average Requirement and RDI/RDA for their age and sex but also report the proportion of participants meeting other sports nutrition specific targets which may be higher than those for the general population(Reference Thomas, Erdman and Burke9). How the nutrient intake from dietary supplements contributes to intakes should also be detailed, and only two studies in this review reported on this(Reference Thomas, Erdman and Burke9). Finally, the rigour of data capture and the background/experience of the researcher conducting the dietary analysis (reported in 5/22 studies) is also relevant to the quality of the dietary outcomes. Use of self-report apps may make data capture easier but not necessarily accurate(Reference Chen, Berkman and Bardouh41).
Although the major limitation of this review is the quality of the literature that informs it, a major strength is the detailed synthesis of the studies and the construction of the Dietary Intake and Nutrition Education Reporting for Sports checklist table (Table 4) which succinctly summarises the strengths and limitations of the included studies while also guiding future research practice. Nonetheless, the authors acknowledge some limitations of this review including studies excluded if published in languages other than English which poses a risk of publication bias. Further, no meta-analysis was performed due to the heterogeneity of included studies.
In conclusion, there is limited research informing the efficacy of nutrition education interventions in athletes, and what is available is of poor to fair quality, reporting varied outcomes. The findings of the review highlight (1) the requirement for ongoing nutrition education of athletes as they commonly report energy and carbohydrate intakes below recommendations, and (2) the importance of carefully planning interventions to ensure meaningful outcomes is aligned with sport-specific nutritional requirements that can be clearly interpreted and subsequently reported by sports nutrition professionals and researchers. As nutrition education is a key strategy to enhance dietary intake in athletes and there is substantial investment in nutrition education interventions across the broader sporting context, there is a need for rigorous research in this area to inform best practice.
Acknowledgements
This paper is dedicated to the memory of Associate Professor Helen O’Connor, who sadly passed during the preparation of this manuscript.
No funding was supplied in production of this manuscript.
The study was designed by A. B., G. C. and H. O. C.; data were collected and analysed by A. B., R. T., H. O. C. and L. M.; data interpretation and manuscript preparation were performed by all authors; all authors (except H. O. C.) approved the final version of the manuscript.
The authors declare no conflicts of interest.
Supplementary material
For supplementary materials referred to in this article, please visit https://doi.org/10.1017/S0007114520003694