


Stroke and dementia pose a significant threat to global public health. In addition to sharing common cardiovascular risk factors,Reference Sahathevan, Brodtmann and Donnan 1 , Reference Gardener, Wright, Rundek and Sacco 2 stroke has been shown to approximately double the risk of subsequent incident dementia.Reference Savva and Stephan 3 As stroke and dementia becomes more frequent with the aging population, widespread prevention initiatives are essential to combat the health and economic burden imposed by both cerebrovascular conditions.
We recently demonstrated a concomitant decline in stroke and dementia incidence in Ontario, Canada from 2002 to 2013 among those aged 80 years and older.Reference Cerasuolo, Cipriano and Sposato 4 This may be attributable to improved primary prevention targeting shared risk of factors of stroke and dementia, and to a decreased incidence of dementia directly related to the decreased incidence of stroke.Reference Cerasuolo, Cipriano and Sposato 4 Independent of changes in stroke incidence, improvements in acute stroke care and rehabilitation may also have contributed to a decline in the incidence of dementia. In order to further understand the relationship of stroke and dementia in the Ontario’s eldest population, this study examines temporal trends in the prevalence of stroke and dementia in those aged 80 years and older from 2003-04 to 2012-13.
We obtained data on the prevalence of stroke and dementia in Ontario through a publicly available online data portal managed by the Public Health Agency of Canada. 5 The Canadian Chronic Disease Surveillance System (CCDSS) monitors descriptive metrics of various health conditions using administrative health databases (e.g., health registries, hospital discharges, physician billing claims, and prescription dispenses).Reference Feely, Lix and Reimer 6 The accuracy of the validated diagnostic algorithms which identified cases for stroke and dementia are described elsewhere.Reference Jaakkimainen, Bronskill and Tierney 7 , Reference Hall, Mondor, Porter, Fang and Kapral 8 Prevalence was defined as all prevalent cases in a particular year of observation, divided by the total population with valid Ontario health insurance. 5 We reported crude stroke and dementia prevalence trends from fiscal years 2003-04 to 2012-13 in those aged at least 80 years, stratified by sex. Age-standardization was not completed owing to unavailability of more granular age strata. Crude rates were accompanied by 95% confidence intervals; significant trends were identified using the Kendall τ-b correlation coefficient. Analysis was completed using STATA 13.
From fiscal years 2003-04 to 2012-13 (Table 1), crude stroke prevalence increased 5.1% (163.4-171.8 per 1000 population, p=0.020) in women and 4.2% (182.2-189.8 per 1000, p=0.039) in men. Similarly, with a higher magnitude across the same timeframe, crude dementia prevalence increased by 21.0% (178.4-215.9 per 1000, p<0.001) in women and 24.0% (130.1-161.3 per 1000, p<0.001) in men. In each year from 2003-04 to 2012-13 (Figure 1), dementia prevalence was higher among women, whereas stroke prevalence was higher among men.
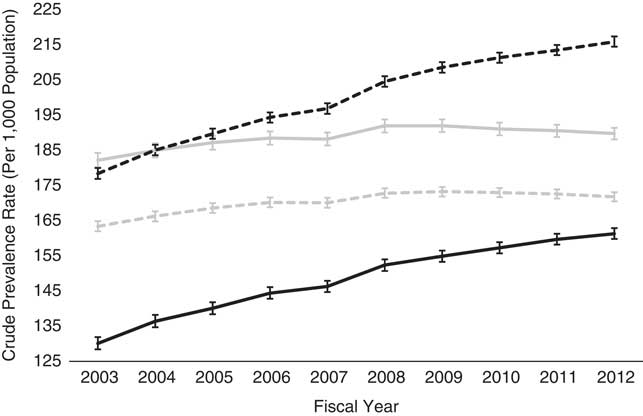
Figure 1 Temporal trends of crude stroke and dementia prevalence rates (per 1000 population) among those aged 80 years and older, fiscal years from 2003-04 to 2012-13. 5 Black lines represent dementia, and gray lines stroke. Dashed lines symbolize women, and solid lines men. Error bars represent 95% confidence intervals around point estimates. Refer to Table 1 for corresponding metrics.
Table 1 Crude prevalence rates (per 1,000 population) of stroke and dementia among those aged 80 years and older, fiscal years from 2003-04 to 2012-13 5
Crude prevalence rate per 1,000 population. Years are expressed fiscally – year 2003 denotes April 1, 2003 to March 31, 2004. LCL=lower 95% confidence limit; UCL=upper 95% confidence limit.
We found that the prevalence of both stroke and dementia increased between 2003-04 and 2012-13 in Ontario, Canada, and the magnitude of the increase in dementia prevalence was far greater than that of stroke. This was consistent with a worldwide study of dementia burden among 21 Global Burden of Disease regions that projected prevalence to approximately double every 20 years.Reference Prince, Bryce, Albanese, Wimo, Ribeiro and Ferri 9 Since the rate of increase in dementia prevalence greatly exceeds that of stroke, the increase in dementia prevalence cannot be fully explained by cerebrovascular mechanisms such as a prior stroke.Reference Hugo and Ganguli 10 , Reference Raz, Knoefel and Bhaskar 11 In addition, our observations may be a consequence of more patients suffering milder strokes but remain undiagnosed, and therefore the temporal trends of stroke prevalence are biased downward. Given the documented decline in stroke incidence,Reference Cerasuolo, Cipriano and Sposato 4 the steady increase in dementia prevalence suggests that people with dementia may be living longer with the disease or being diagnosed at a younger age.
The previously observed temporal decrease in stroke and dementia incidenceReference Cerasuolo, Cipriano and Sposato 4 may be in part because of primary prevention efforts of Ontario’s integrated stroke system—preventive measures are successfully targeting risk factors common to both stroke and dementia,Reference Sahathevan, Brodtmann and Donnan 1 , Reference Gardener, Wright, Rundek and Sacco 2 and the risk of dementia is further reduced by decreasing the incidence of stroke since stroke is known to double the risk of dementia.Reference Savva and Stephan 3 Yet, it is possible that a decrease in the incidence of stroke and/or dementia are caused by older individuals dying from other health conditions (i.e., heart failure, cancer, respiratory illness, etc.), potentially precluding a diagnosis of stroke and/or dementia. The current study serves to counter that hypothesis and instead suggests that the average life expectancy after stroke and/or dementia diagnosis is increasing. This may be because of improvements in acute stroke care, rehabilitation, and secondary prevention and treatment of comorbid conditions. However, since our analysis was based on crude metrics, the increase in prevalence is partly a consequence of Canada’s aging population.
Our study has limitations. Since more granular age strata among the elderly were not available, we did not report age-standardized metrics. Second, we used administrative data to identify cases, and may have underestimated prevalent dementia and stroke.Reference Lopez, McDade, Riverol and Becker 12 In addition, given the unavailability of individual-level data, the analytical scope was limited. We also did not provide information on the underlying reasons for the observed trends, pending further, more elaborate investigation using individual-level data sources.
This study provides novel information on the concurrent temporal trends of stroke and dementia prevalence in Ontario, Canada. Given the substantial increases in dementia prevalence in women and men from 2003-04 to 2012-13, we speculate that improved stroke prevention, acute stroke care, and rehabilitation may have prolonged survival following a diagnosis of stroke or dementia. More importantly, we provide evidence for the increasing burden of stroke and dementia in Ontario, Canada, like other high-income countries, and must prepare for this impending public health concern with the potential for high consumption of health system resources. Future research should evaluate the clinical benefit of stroke-related health system investments on subsequent cognition.
Acknowledgments
The authors thank Catherine Pelletier and Cynthia Robitaille (Public Health Agency of Canada) for their assistance with navigating the Canadian Chronic Disease Surveillance System (CCDSS), and their insightful comments on this manuscript.
Statement of Authorship
JOC and VH conceived the study idea. JOC drafted all manuscript versions and conducted the statistical analyses. LEC and VH supervised the study. JOC, MRA, MKK, LEC, and VH interpreted results, critically reviewed the manuscript for important intellectual content, and approved final version of this manuscript.
Disclosures
JC, MRA, MK, LC, and VH have nothing to disclose.


