



Introduction
Exposure to trauma in early childhood has been shown to impact the developing brain, with extensive research demonstrating disruption of critical processes including executive functioning, episodic memory, emotion reactivity/emotion regulation, and reward processing, all of which rely on fronto-limbic networks (Cowell et al., Reference Cowell, Cicchetti, Rogosch and Toth2015; Gonzalez & Oshri, Reference Gonzalez and Oshri2019; Kavanaugh et al., Reference Kavanaugh, Dupont-Frechette, Jerskey and Holler2017; Stevens et al., Reference Stevens, Reddy, Kim, van Rooij, Ely, Hamann, Ressler and Jovanovic2018). However, it is still unclear how early in life these associations become apparent, and which components of neurocognitive and emotional processes are affected by trauma exposure, given that most research has been conducted with school-age children and adolescents and findings obtained from samples with young children have been mixed (Lund et al., Reference Lund, Toombs, Radford, Boles and Mushquash2020; Young-Southward et al., Reference Young-Southward, Eaton, O'Connor and Minnis2020). Furthermore, past studies with young children have assessed trauma without considering how nuances in operationalization and measurement of trauma exposure differentially affects neurocognitive and emotional processes, nor have neurocognitive and emotional processes been measured in comprehensive, yet discernible ways (i.e., the majority of studies in early childhood have employed broad measures of executive functioning, or examined only one specific component of executive functioning). Associations between early childhood trauma, executive functioning, episodic memory, and emotion reactivity/emotion regulation may also be dependent on other contextual factors early in development, consistent with a bioecological lens, yet few studies have measured the distinct influences of specific risk factors that exist beyond the individual level, such as socioeconomic adversity and parental depressive symptoms (Bronfenbrenner, Reference Bronfenbrenner1979). The current paper expands on prior work linking trauma exposure with neurocognitive and emotional processes in children by moving beyond both overly broad conceptualizations of these constructs, as well as more specific conceptualizations that fail to integrate potentially relevant variables.
Executive functioning (also known as cognitive control) is an umbrella term used to describe a collection of higher-order cognitive processes that facilitate goal-directed actions and behaviors and allow flexible adjustment of these behaviors based on the environment (Diamond, Reference Diamond2013; Miyake et al., Reference Miyake, Friedman, Emerson, Witzki, Howerter and Wager2000). These processes can be divided into three correlated, yet partially independent, components, including inhibitory control (i.e., the ability to suppress or control automatic or prepotent responses), cognitive flexibility (i.e., shifting between mental sets or tasks), and working memory (i.e., maintaining or manipulating information not perceptually present; Miyake et al., Reference Miyake, Friedman, Emerson, Witzki, Howerter and Wager2000). Episodic memory, while not considered a primary component of executive functioning, is another critical cognitive domain that involves acquiring, storing, and recalling new information, and is highly correlated with executive functioning generally and working memory specifically (McCabe et al., Reference McCabe, Roediger, McDaniel, Balota and Hambrick2010). Executive functioning plays an important role in an individual’s capacity to control their emotions. Emotion regulation, or the ability to modulate, manage, or organize emotions in order to meet environmental demands and achieve goals, is thought to occur by the prefrontal cortex exerting cognitive control over the amygdala, a central emotion processing structure in the brain (Kebets et al., Reference Kebets, Favre, Houenou, Polosan, Perroud, Aubry, Van De Ville and Piguet2021; Ochsner & Gross, Reference Ochsner and Gross2005; Pruessner et al., Reference Pruessner, Barnow, Holt, Joormann and Schulze2020). Executive functioning and emotion regulation are acknowledged as top-down processes given that they are effortful responses and are thought to rely heavily on prefrontal circuitry (Zelazo & Cunningham, Reference Zelazo, Cunningham and Gross2007). Emotion reactivity, a separate but related dimension, is defined as the expression of positive or negative affect in response to stimuli, and varies in its latency, intensity, and duration (Eisenberg et al., Reference Eisenberg, Fabes, Murphy, Maszk, Smith and Karbon1995; Gross & Thompson, Reference Gross, Thompson and Gross2007; Rothbart, Reference Rothbart, Kohnstamm, Bates and Rothbart1989). In contrast to executive functioning and emotion regulation, emotion reactivity is a bottom-up process that does not require conscious mental resources and is thought to be mediated by subcortical brain regions like the limbic system (Gross & Thompson, Reference Gross, Thompson and Gross2007). It is through successful management of emotion reactivity that adaptive emotion regulation occurs (Rydell et al., Reference Rydell, Berlin and Bohlin2003). Although emotion reactivity may primarily occur through bottom-up processes, and executive functioning and emotion regulation largely occur through top-down processes, these constructs are interconnected and implicated in the development of psychopathology (Ferrier et al., Reference Ferrier, Bassett and Denham2014; Graziano et al., Reference Graziano, McNamara, Geffken and Reid2013; Rydell et al., Reference Rydell, Berlin and Bohlin2003). Indeed, bidirectional associations between emotion reactivity/emotion regulation and executive functioning/episodic memory due to shared neurocircuitry have been described in the literature (Barch et al., Reference Barch, Harms, Tillman, Hawkey and Luby2019; Erk et al., Reference Erk, Von Kalckreuth and Walter2010; Pessoa, Reference Pessoa2009). (For a more comprehensive review of these neurocognitive and emotional constructs and processes, and their interrelations, see Nigg, Reference Nigg2017).
Deficits in executive functioning/episodic memory and emotion reactivity/emotion regulation underlie numerous psychiatric conditions, perhaps due to their fundamental role in learning and adaptation across contexts, their relative plasticity from infancy through early adulthood, and their sensitivity to environmental factors, including exposure to maltreatment and other traumatic life events (Zelazo, Reference Zelazo2020). As such, executive functioning and emotion reactivity/emotion regulation have been identified as possible transdiagnostic mechanisms linking early childhood trauma to general psychopathology across the lifespan (Fernandez et al., Reference Fernandez, Jazaieri and Gross2016; Weissman et al., Reference Weissman, Bitran, Miller, Schaefer, Sheridan and McLaughlin2019; Zelazo, Reference Zelazo2020). The identification of transdiagnostic factors, or constructs that contribute to the development and maintenance of multiple psychiatric conditions, has become a key focus in the field of developmental psychopathology given the potential for transdiagnostic factors to serve as effective, cross-cutting treatment targets (Conradt et al., Reference Conradt, Crowell and Cicchetti2021; Pacheco et al., Reference Pacheco, Garvey, Sarampote, Cohen, Murphy and Friedman-Hill2022; Vargas & Mittal, Reference Vargas and Mittal2021). For example, negative emotionality or emotion dysregulation may be identified earlier and more reliably in young children who do not always meet diagnostic criteria for psychiatric conditions but are at risk for later psychopathology, thereby allowing for preventive interventions focused on a critical mechanism (e.g., emotion regulation) implicated in the development of numerous psychiatric disorders (Beauchaine & Cicchetti, Reference Beauchaine and Cicchetti2019; Cludius et al., Reference Cludius, Mennin and Ehring2020; Fernandez et al., Reference Fernandez, Jazaieri and Gross2016). Thus, specifying transdiagnostic factors in early childhood is essential for preventing the development of psychopathology and problematic long-term outcomes, as well as for addressing current symptoms among children living in contexts of risk.
In this article, we examine cross-sectional associations between early childhood trauma and components of executive functioning (i.e., inhibitory control and cognitive flexibility), episodic memory, and emotion reactivity in a sample of young children admitted to a specialized, early childhood day treatment program (also referred to as a partial hospital program). This population is at high risk for current and future psychiatric disorders, yet vastly understudied. We chose to focus on emotion reactivity rather than emotion regulation as emotion reactivity is observable and thus more feasible to assess in young children. Emotion reactivity is also an important component of the ability to regulate an emotional reaction, and is more robustly associated with early childhood trauma, per a meta-analysis (see Lavi et al., Reference Lavi, Katz, Ozer and Gross2019).
Operationalizing trauma exposure
Operationalization of trauma exposure varies considerably across studies, and how trauma is characterized and assessed has important implications for whether neurocognitive, emotional, and behavioral effects are observed (Jackson et al., Reference Jackson, McGuire, Tunno and Makanui2019). Although the question of how to best operationalize trauma exposure is still being explored and debated (McLaughlin et al., Reference McLaughlin, Sheridan, Humphreys, Belsky and Ellis2021; Pollak & Smith, Reference Pollak and Smith2021; Smith & Pollak, Reference Smith and Pollak2021), one of the most longstanding methods for operationalizing trauma is summing the number of categories of traumatic life events that a person has experienced. Theory and empirical research point to synergistic effects of two or more traumatic life events; i.e., multiple negative life events may produce a greater combined effect than the sum of the individual events (Putnam et al., Reference Putnam, Harris and Putnam2013). Not only is experiencing multiple types of traumatic events in childhood more common than experiencing only one type of event (Finkelhor et al., Reference Finkelhor, Turner, Shattuck and Hamby2013; Jackson et al., Reference Jackson, McGuire, Tunno and Makanui2019; Turner et al., Reference Turner, Shattuck, Finkelhor and Hamby2016), cumulative trauma, also termed polyvictimization, is associated with more frequent, severe, and complex psychiatric outcomes in both children and adults (Ford & Delker, Reference Ford and Delker2018). Cumulative trauma has also been linked to emotion reactivity/emotion regulation difficulties in school-age children (Choi & Oh, Reference Choi and Oh2014; Hébert et al., Reference Hébert, Langevin and Oussaïd2018) and adolescents (Charak et al., Reference Charak, Ford, Modrowski and Kerig2019). Further, in a study of preschool-age children, effects of trauma on inhibitory control were more pronounced for a cumulative risk index including maltreatment, family turmoil, and socioeconomic status, than for each of these individual factors alone (Giuliano et al., Reference Giuliano, Roos, Farrar and Skowron2018). Although categorical approaches to trauma measurement, including cumulative risk indices or composites, have been helpful in establishing associations between trauma and neurocognitive and emotional outcomes in children, the field is generally moving in the direction of adopting dimensional approaches to trauma measurement, which may be more informative than assessing the sum total of children’s exposures to certain events (Pollak & Smith, Reference Pollak and Smith2021).
Examining dimensions of trauma exposure is increasingly recognized as equally if not more important than assessing cumulative trauma, given differential effects on outcomes. McLaughlin and colleagues (2021) have proposed investigating dimensions of threat versus deprivation within the realm of child maltreatment, for example, and have found differential effects of each dimension in multiple domains. For traumatic events that go beyond maltreatment, distinguishing between interpersonal versus non-interpersonal trauma may be useful. A robust body of research has demonstrated that interpersonal trauma (i.e., victimization that occurs in relationships, including sexual and physical abuse and witnessing relational violence) is associated with worse developmental outcomes than is non-interpersonal trauma (i.e., trauma that is not individually directed, such as experiencing a natural disaster or being in a car accident) (Badour et al., Reference Badour, Feldner, Babson, Smith, Blumenthal, Trainor, Bunaciu and Olatunji2011; Ford et al., Reference Ford, Gagnon, Connor and Pearson2011; Maughan & Cicchetti, Reference Maughan and Cicchetti2002). Numerous studies have established connections between interpersonal trauma and emotion reactivity/emotion regulation problems in school-age children and adolescents (see D’Andrea et al., Reference D’Andrea, Ford, Stolbach, Spinazzola and Van der Kolk2012 and Gruhn & Compas, Reference Gruhn and Compas2020 for reviews), and a growing number have linked interpersonal trauma to executive functioning deficits in these age groups as well (DePrince et al., Reference DePrince, Weinzierl and Combs2009; Musicaro et al., Reference Musicaro, Ford, Suvak, Sposato and Andersen2020; Nolin & Ethier, Reference Nolin and Ethier2007; van der Bij et al., Reference van der Bij, den Kelder, Montagne and Hagenaars2020). Differentiating between interpersonal versus non-interpersonal trauma has indeed been found to be useful; for example, in a study of school-age children and adolescents in outpatient and residential clinics, sluggish cognitive tempo – which has some overlap with components of executive functioning – was positively associated with interpersonal trauma but not non-interpersonal trauma (Musicaro et al., Reference Musicaro, Ford, Suvak, Sposato and Andersen2020). Interpersonal trauma may be especially salient for young children who rely completely on their relationships with caregivers, and thus are disproportionately exposed to these types of experiences (Hagan et al., Reference Hagan, Browne, Sulik, Ippen, Bush and Lieberman2017). Therefore, it is critical to test whether interpersonal, compared to non-interpersonal trauma, as well as cumulative trauma, differentially affect young children’s executive functioning and emotion reactivity, as this will contribute to a greater understanding of the impact of trauma on neurocognitive and emotional processes in this population. It should also be noted that interpersonal versus non-interpersonal trauma is one conceptualization, but there are many different dimensions that can, and should, be explored to contribute to a richer understanding of early childhood trauma exposure and relevant neurocognitive and emotional consequences (Smith & Pollak, Reference Smith and Pollak2021). For a more comprehensive understanding of the current thinking around categorical versus dimensional approaches to conceptualizing and operationalizing trauma exposure, see recent papers by Smith and Pollak (Reference Smith and Pollak2021), McLaughlin et al. (Reference McLaughlin, Sheridan, Humphreys, Belsky and Ellis2021), and Pollak and Smith (Reference Pollak and Smith2021).
Early childhood trauma and neurocognitive outcomes
Three systematic reviews have provided strong evidence for associations between traumatic life events experienced in childhood and general executive functioning deficits, as well as specific impairments in episodic memory, in primarily school-age children and adolescents (Lund et al., Reference Lund, Toombs, Radford, Boles and Mushquash2020; Su et al., Reference Su, D’Arcy, Yuan and Meng2019; Young-Southward et al., Reference Young-Southward, Eaton, O'Connor and Minnis2020). Although the majority of these studies have focused on maltreatment (e.g., sexual, physical, and emotional abuse; neglect) and institutionalization/foster care, other types of adversity have also been explored, including witnessing family violence and exposure to parental mental illness and substance use (Lund et al., Reference Lund, Toombs, Radford, Boles and Mushquash2020). Importantly, findings differ substantially based on which component of executive functioning is examined. For example, in some cross-sectional studies during middle childhood, children who had experienced early trauma had poorer working memory than those who had not, but exhibited no differences in cognitive flexibility (Augusti & Melinder, Reference Augusti and Melinder2013; Bücker et al., Reference Bücker, Kapczinski, Post, Ceresér, Szobot, Yatham, Kapczinski and Kauer-Sant'Anna2012). Conversely, other studies found associations between exposure to traumatic life events and both working memory and cognitive flexibility in school-age children (Carvalho et al., Reference Carvalho, Renner, Donat, de Moura, Fonseca and Kristensen2018; DePrince et al., Reference DePrince, Weinzierl and Combs2009; Perna & Kiefner, Reference Perna and Kiefner2013). Similarly, early childhood trauma was associated with inhibitory control in some cross-sectional studies during middle childhood (Carvalho et al., Reference Carvalho, Renner, Donat, de Moura, Fonseca and Kristensen2018; DePrince et al., Reference DePrince, Weinzierl and Combs2009; Nadeau & Nolin, Reference Nadeau and Nolin2013) but not others (Augusti & Melinder, Reference Augusti and Melinder2013; Bruce et al., Reference Bruce, Fisher, Graham, Moore, Peake and Mannering2013; Mezzacappa et al., Reference Mezzacappa, Kindlon and Earls2001). Though fewer studies have been conducted with early childhood populations, mixed findings on early childhood trauma and executive functioning capacities have also been found. For instance, several studies found differences in inhibitory control between maltreated and non-maltreated children (Fay-Stammbach et al., Reference Fay-Stammbach, Hawes and Meredith2017; Skowron et al., Reference Skowron, Cipriano-Essel, Gatzke-Kopp, Teti and Ammerman2014), while others did not (Cipriano-Essel et al., Reference Cipriano-Essel, Skowron, Stifter and Teti2013; Giuliano et al., Reference Giuliano, Roos, Farrar and Skowron2018). In one study, cumulative trauma in a sample of preschool-age children attending a community-based trauma clinic was unrelated to an executive functioning composite derived from a performance-based measure (Cohodes et al., Reference Cohodes, Chen, Lieberman and Bush2020). These results underscore the importance of: (1) conducting additional studies measuring multiple components of executive functioning and other cognitive factors at the same time in samples of young children, and in samples of young children with acute symptomatology, such as those admitted to partial hospital or inpatient programs, and (2) examining potential moderators of the association between early childhood trauma and executive functioning.
Early childhood trauma and emotion reactivity
There is extensive support in the literature for an association between early childhood trauma and emotion reactivity. Specifically, children who are exposed to trauma in early childhood tend to display high levels of negative emotionality (e.g., anger, sadness) in general, and in response to neutral or negative stimuli (McLaughlin & Lambert, Reference McLaughlin and Lambert2017; Weissman et al., Reference Weissman, Bitran, Miller, Schaefer, Sheridan and McLaughlin2019). In a meta-analysis conducted by Lavi and colleagues (2019), children who had experienced maltreatment were substantially more likely to display both high negative affect and low positive affect compared to children who had not experienced maltreatment. Effect sizes for these emotion reactivity constructs were stronger than effect sizes for emotion regulation (Lavi et al., Reference Lavi, Katz, Ozer and Gross2019). Given that children who have experienced maltreatment may experience negative emotions more intensely than their non-maltreated peers, maltreated children may have to exert greater effort to effectively modulate negative affect (Weissman et al., Reference Weissman, Bitran, Miller, Schaefer, Sheridan and McLaughlin2019), which has been found in a sample of maltreated adolescents (McLaughlin et al., Reference McLaughlin, Peverill, Gold, Alves and Sheridan2015). Thus, children who experience more intense negative emotions may have greater difficulties effectively regulating emotion, and impaired emotion regulation may result in higher levels of negative affect. Importantly, the relationship between early childhood trauma and emotion reactivity may be context dependent. For example, caregivers’ reactions to children’s expressions of emotion, along with caregivers’ own abilities to express and regulate emotions, may influence how children express and experience affect (Bariola et al., Reference Bariola, Gullone and Hughes2011; Gross & Cassidy, Reference Gross and Cassidy2019; Lobo & Lunkenheimer, Reference Lobo and Lunkenheimer2020; Morris et al., Reference Morris, Silk, Steinberg, Myers and Robinson2007). Examining trauma and emotion reactivity in samples of young children, along with potential moderating factors, is critical for understanding children’s development of self-regulatory capacities.
Family contextual factors as potential moderators
Existing research on early childhood trauma and neurocognitive and emotional processes has revealed mixed findings in samples of young children. Given the pivotal role of the family context in early childhood development (Bronfenbrenner, Reference Bronfenbrenner1979; Scheeringa & Zeanah, Reference Scheeringa and Zeanah2001), it is likely that these associations vary by family contextual influences. Family socioeconomic adversity and parental depression are two of the most studied contextual factors thought to impact neurodevelopment and child functioning. Regarding socioeconomic adversity, there is overwhelming evidence that, on average, children growing up in contexts of socioeconomic adversity fare worse in many domains than children who do not experience poverty and other resource inequities (Le Menestrel et al., Reference Le Menestrel and Duncan2019). Specifically, socioeconomic adversity is associated with components of executive functioning and emotional processing in samples of preschool- and school-age children (St. John et al., Reference St. John, Kibbe and Tarullo2019; Ursache & Noble, Reference Ursache and Noble2016; Zhang et al., Reference Zhang, Lee, White and Qiu2020), with the presence of socioeconomic-based disparities in executive functioning exhibiting small to medium effect sizes in a meta-analysis (Lawson et al., Reference Lawson, Hook and Farah2018). However, many studies have measured executive functioning using a composite score, so it is yet unclear how socioeconomic adversity affects specific components of executive functioning, especially in the presence of trauma (St. John et al., Reference St. John, Kibbe and Tarullo2019).
In addition to being one of the most prevalent mental health disorders, depression is particularly salient because it shapes a parent’s perception of themselves and others, and therefore changes how parents interact with their children in important ways that affect child development (National Research Council & Institute of Medicine, 2009). Early exposure to parental depressive symptoms has been shown to be related to deficits in children’s executive functioning at ages 5 and 6 (Hughes et al., Reference Hughes, Roman, Hart and Ensor2013; Wang & Dix, Reference Wang and Dix2017), and difficulties with emotion expression and regulation throughout early childhood (Blandon et al., Reference Blandon, Calkins, Keane and O’Brien2008; Granat et al., Reference Granat, Gadassi, Gilboa-Schechtman and Feldman2017; Maughan et al., Reference Maughan, Cicchetti, Toth and Rogosch2007; Priel et al., Reference Priel, Zeev-Wolf, Djalovski and Feldman2020). This may be because parental depressive symptoms interfere with sensitive and responsive parenting, and lead to restricted emotion expression, increased negative emotionality, and unpredictable shifts between withdrawal and anger in the parent, any of which may contribute to impairments in the child’s developing neurocognitive and emotional processes (Priel et al., Reference Priel, Zeev-Wolf, Djalovski and Feldman2020). In short, these studies reflect a need to examine family socioeconomic adversity and parental depressive symptoms in concert with early childhood trauma, as the interplay of these factors may affect young children’s executive functioning and emotion reactivity. It may be the combination of trauma and socioeconomic adversity, or trauma and parental depressive symptoms, that places some children at higher risk for problems compared to others. Specifically, exposure to trauma is more likely to be associated with negative outcomes in children in the presence of additional risk factors, including parental depressive symptoms and socioeconomic adversity. This may be due to the lack of supportive factors in both of these contexts (e.g., lack of access to a warm, nurturing caregiver who is emotionally attuned, responsive to their child’s needs, and able to support processing and coping with traumatic events; inequitable access to resources that support healthy functioning in times of difficulty, such as quality time with parents, which can be more difficult to come by in single parent households or households in which parents are struggling to make ends meet; Masten et al., Reference Masten, Lucke, Nelson and Stallworthy2021). The downstream impact of parenting behavior on child emotional and neurocognitive processes is beyond the scope of this paper, but identifying which aspects of parenting behavior hold particular importance for young children’s cognitive and emotional development in the context of trauma is a critical next step. For example, distinguishing between parental sensitivity when children are distressed versus when children are calm has important implications for children exposed to trauma, and such differences in parental sensitivity have been found to differentially affect child emotionality and other related outcomes (Leerkes & Zhou, Reference Leerkes and Zhou2018).
The present study
A fairly robust body of literature has demonstrated associations between early childhood trauma exposure and impaired neurocognitive and emotional processes, yet few of those studies have examined these relations within samples of young children, and results of those studies that have are conflicting (Cohodes et al., Reference Cohodes, Chen, Lieberman and Bush2020). Testing such associations in early childhood will provide important revelations about whether, when, and how trauma interferes with the healthy development of cognitive and self-regulatory processes. Executive functioning undergoes the greatest maturation when children are 3–7 years old, making this developmental period one of critical importance for neurocognitive and emotional processes (Best & Miller, Reference Best and Miller2010). Furthermore, it is unclear how associations between early childhood trauma and executive functioning and emotion reactivity are moderated by family contextual factors that have been shown to have effects in prior research, namely socioeconomic adversity and parental depressive symptoms. The presence of contextual factors may help explain mixed findings in previous studies. Given the limited evidence base for this age group, the primary aim of the current study was to utilize a sample of young children admitted to an early childhood day treatment program and examine cross-sectional associations between cumulative trauma (and interpersonal trauma) and components of executive functioning, episodic memory, and emotion reactivity, conceptualized using the National Institute of Mental Health Research Domain Criteria (RDoC). The RDoC framework relies on dimensions of functioning rather than categorical diagnoses, which allows for the identification of underlying commonalities across psychiatric conditions that are otherwise considered distinct; this approach is especially important in developmental research, wherein identifying transdiagnostic factors is a critical first step in preventing a range of psychiatric disorders (Pacheco et al., Reference Pacheco, Garvey, Sarampote, Cohen, Murphy and Friedman-Hill2022). The secondary aim of the study was to test whether family socioeconomic status and parental depressive symptoms were potential moderators.
Importantly, this study includes a broad array of traumatic experiences rather than maltreatment alone, and investigates the roles of cumulative trauma and interpersonal trauma to better understand how differing operationalizations of trauma exposure (e.g., a categorical versus dimensional approach) affect outcomes. Results may therefore be more applicable to community and treatment settings outside of child welfare-involved systems, and will be especially relevant to young children, for whom relational experiences hold great developmental significance. In addition, most studies have employed a composite score of executive functioning, or examined one component. Our inclusion of two components of executive functioning, as well as episodic memory and a cognitive composite score, paired with our use of well-validated and developmentally sensitive observational and performance-based measures, represents a rigorous approach to understanding processes that are central to children’s social-emotional well-being across development, and will aid in the prevention of psychopathology. Moreover, inhibitory control is measured using two different assessment tools (i.e., the NIH Toolbox Flanker task and the Lab-TAB Tower of Patience task), given that inhibitory control can be considered both a neurocognitive and emotional process. Employing two tools – one that assesses the neurocognitive aspects of inhibitory control through a computerized, individual task, and one that assesses the emotional aspects of inhibitory control through a relational task – allows for greater understanding of the associations between trauma exposure and this nuanced construct.
We hypothesized that children who had experienced more categories of traumatic life experiences (i.e., cumulative trauma) would show lower levels of inhibitory control, cognitive flexibility, episodic memory, and overall cognitive composite scores, higher levels of expressed negative affect at the omission of an expected reward and due to a perceived loss, and lower levels of expressed positive affect during a rewarding paradigm compared to children with fewer categories of traumatic life experiences. We also hypothesized that children who experienced interpersonal trauma would show lower levels of inhibitory control, cognitive flexibility, episodic memory, and overall cognitive composite scores, higher levels of expressed negative affect, and lower levels of expressed positive affect, than children who had not experienced interpersonal trauma. Finally, we hypothesized that these main effects would be qualified by interactions between each of the predictors and family socioeconomic adversity and parental depressive symptoms, such that children exposed to greater cumulative trauma or interpersonal trauma and higher levels of socioeconomic adversity or parental depressive symptoms would demonstrate lower levels of inhibitory control, cognitive flexibility, episodic memory, and overall cognitive composite scores, higher levels of expressed negative affect, and lower levels of expressed positive affect than children exposed to lower levels of socioeconomic adversity or parental depressive symptoms.
Method
Participants
Participants in this cross-sectional study included 90 4- to 7-year-old children, and their caregivers, attending a specialized, early childhood day treatment program (also referred to as a partial hospital program). Children admitted to this program presented with a variety of psychiatric concerns: acute aggression, threats to self and/or others, self-injurious behavior, highly uncooperative and oppositional behavior, severe and persistent tantrums, anxiety, and mood problems. To be eligible for this study, (1) the child’s caregiver had to be fluent in English, (2) the child could not be diagnosed with autism spectrum disorder, and (3) the child could not demonstrate a significant developmental delay as defined by a standard score of < 70 on the NIH Toolbox Picture Vocabulary Test. Seventy-four percent of children were male (26% female; 0% non-binary/other). Two percent of children were Asian, 8% were Black, 63% were White, 14% were multiracial, and 12% endorsed other races; 18% were Hispanic or Latino/a. Forty-four percent of children had internalizing symptoms in the clinical range (t-score ≥ 70) on the Child Behavior Checklist (CBCL; Achenbach & Edelbrock, Reference Achenbach and Edelbrock1991), while 72% had externalizing symptoms, and aggressive behaviors specifically, in the clinical range on the CBCL. Per case review, 29% of children had suicidal ideation in the past four weeks, 44% had suicidal ideation in their lifetime, 21% had lifetime suicidal behavior, and 48% had lifetime non-suicidal self-injury.
Most caregivers who served as the primary reporter for the study were biological mothers of the participating child (87%), followed by adoptive mothers (7%), biological fathers (3%), and finally “other” caregivers (2%). Of primary caregivers for the study (94% of whom identified as female), 6% had less than a high school degree, 20% had completed high school, 19% had completed a certificate program (e.g., cosmetology, certified nursing assistant), 27% had some postsecondary education, 21% had a bachelor’s degree, and 7% had a master’s degree or higher. Forty-six percent of primary caregivers were not employed, and 51% were single parents. Additionally, family income varied widely among participants, such that 11% of caregivers reported a total annual family income of less than $10,000, 21% reported an income of $10,000–$19,999, 15% reported $20,000–$29,999, 14% reported $30,000–$39,999, 4% reported $40,000–$49,999, 7% reported $50,000–$59,999, 1% reported $60,000–$69,999, 3% reported $70,000–$79,999, 4% reported $80,000–$89,999, 1% reported $90,000–$99,999, and 19% reported $100,000 or more.
Procedure
Caregivers were invited to participate in the study at the time of their child’s admission into the day treatment program. After the study was explained by research staff, caregivers provided written consent for themselves and their child to participate. Caregivers and children completed assessments shortly after admission, though in some instances child assessments were delayed due to behavioral challenges. All study procedures were approved by the Institutional Review Board at the medical center.
Measures
Demographics and family socioeconomic adversity
Caregivers reported on their child’s age, gender, race, and ethnicity, as well as on their own education level, employment status (not employed vs. employed), marital status (single vs. two-parent household), and family income. Consistent with prior research (e.g., Huffhines et al., Reference Huffhines, Coe, Busuito, Seifer and Parade2022; Tyrka et al., Reference Tyrka, Ridout, Parade, Paquette, Marsit and Seifer2015), indicators of socioeconomic risk (education ≤ high school diploma, non-employment, single parenthood) were summed to provide a parsimonious assessment of family socioeconomic adversity (possible scores ranged from 0 to 3).
Traumatic life events
Caregivers completed the Diagnostic Infant and Preschool Assessment (Scheeringa & Haslett, Reference Scheeringa and Haslett2010) interview to assess children’s lifetime exposure to traumatic events. The twelve possible categories of traumatic events included physical abuse, sexual abuse, witnessing violence, experiencing an accident (e.g., car crash), animal attack, man-made disaster, natural disaster, accidental burning, near drowning, life-threatening hospitalization/medical procedure, learning that one of these events happened to the caregiver, and “other” traumatic life event. Importantly, emotional abuse and emotional or physical neglect were not explicitly assessed. Cumulative trauma was computed by summing the number of categories that a child had experienced in their lifetime: 0, 1, or 2 or more categories. Interpersonal trauma was derived by the presence of sexual abuse, physical abuse, and/or witnessing violence (present = 1, absent = 0). Cumulative trauma and interpersonal trauma were used as predictors in separate models, but it should be noted that there is overlap in that the categories that composed interpersonal trauma (i.e., sexual abuse, physical abuse, witnessing violence) were also included in the cumulative trauma count.
Caregiver depressive symptoms
To assess depressive symptoms, caregivers completed the Center for Epidemiological Studies – Depression Scale (CES-D; Radloff, Reference Radloff1977). The CES-D is a 20-item scale which consists of a checklist of moods, cognitions, and feelings associated with depression (e.g., “I felt that people dislike me”). Scores range from 0 (rarely/never) to 3 (most of the time). This measure has shown excellent reliability and validity in previous studies with parents (Atkins, Reference Atkins2014; Ferro & Speechley, Reference Ferro and Speechley2013). In this study, internal consistency was adequate (α = .78). Total scores of 16 or higher generally represent the cutoff for clinically significant depressive symptoms. Caregivers with a score of 16 or above were coded as having clinically significant depressive symptoms present (1), while those with a score of 15 or below were coded as not having clinically significant depressive symptoms present (0). Fifty-eight percent of caregivers in this sample were at or above the clinical cutoff.
Executive functioning and episodic memory
Two components of executive functioning (inhibitory control and cognitive flexibility), as well as episodic memory and a composite of overall cognitive functioning were assessed in this study; each of these constructs falls under the RDoC domain of Cognitive Systems. The National Institutes of Health Toolbox for the Assessment of Neurological and Behavioral Function (NIH Toolbox) is a brief neuropsychological screening battery with tests for children under age 7, and 7 or older, and was used to measure neurocognitive processes (Gershon et al., Reference Gershon, Wagster, Hendrie, Fox, Cook and Nowinski2013). Each NIH Toolbox task was administered to the child using an electronic tablet, and instructions were provided both orally and visually. Standard scores were obtained for each task, and thus can be used across age groups. Inhibitory control was assessed with the Flanker Inhibitory Control and Attention Test (Flanker); in this task – which measures both speed and accuracy – children press a button to indicate whether an arrow (or other stimuli) that is in the middle of an arrangement is congruent or incongruent with the other arrows in the configuration. Cognitive flexibility was assessed with the Dimensional Change Card Sort Test (DCCST); this task assesses attentional flexibility to the switching of rules, and scores are based on accuracy and reaction time. Episodic memory was assessed using the Picture Sequencing Memory Test (PSMT); in this task, children must place pictures in a predefined, correct sequence after having previously seen the order before it is scrambled. Finally, an overall cognitive composite which is a combination of both fluid and crystallized abilities was derived from these three tests plus the Picture Vocabulary Test (TPVT), which is a measure of general vocabulary knowledge. The NIH Toolbox has demonstrated excellent validity and good test-retest reliability in other samples of young children, including those experiencing risk and adversity (Akshoomoff et al., Reference Akshoomoff, Beaumont, Bauer, Dikmen, Gershon, Mungas, Slotkin, Tulsky, Weintraub, Zelazo and Heaton2013; Distefano et al., Reference Distefano, Fiat, Merrick, Slotkin, Zelazo, Carlson and Masten2021).
Emotion reactivity
The preschool and school-age versions of the Laboratory Temperament Assessment Battery (Lab-TAB; Goldsmith & Rothbart, Reference Goldsmith and Rothbart1996) were used to assess dimensions of emotion reactivity. The RDoC construct of Inhibitory Control (associated with the RDoC domain Cognitive Systems) was assessed using the Tower of Patience, a task in which the child and experimenter take turns building a tower, and the child is increasingly delayed in their turn as the experimenter waits for longer time increments before adding a block. The RDoC construct of Frustrative Non-Reward (associated with the RDoC domain Negative Valence Systems) was assessed using the Attractive Toy in Transparent Box task. In this task, the experimenter locks an enticing toy in a clear box and provides the child with a set of keys to open the box; however, none of the keys fit. The RDoC construct of Loss (associated with the RDoC domain Negative Valence Systems) was assessed using the Box Empty task, wherein the child is told they will receive a gift but are instead given an empty box. The RDoC construct of Responsiveness to Reward (associated with the RDoC domain Positive Valence Systems) was assessed using the Popping Bubbles task, in which the experimenter blows bubbles and the child is encouraged to chase them and prevent them from touching the floor.
Lab-TAB tasks were coded using a system described in prior studies with young children (Dyson et al., Reference Dyson, Olino, Durbin, Goldsmith, Bufferd, Miller and Klein2015; Olino et al., Reference Olino, Klein, Dyson, Rose and Durbin2010). For the Tower of Patience task, two behavioral codes (compliance and impulsivity [reverse-scored]) were summed to create the composite variable of Inhibitory Control. Compliance scores ranged from 0 (extremely non-compliant) to 3 (extremely compliant), while Impulsivity scores ranged from 0 (not at all impulsive) to 3 (high impulsivity).
For the Attractive Toy in Transparent Box and Box Empty tasks, expression, intensity, and frequency of negative affect (anger and sadness) observed during each task was coded using facial, vocal, and bodily indicators. For facial codes, scores ranged from 0 (no facial affect) to 4 (six or more instances of low intensity, three or more instances of moderate intensity, or one or more instance of high intensity). For vocal codes, scores ranged from 0 (no vocal expression) to 3 (many low intensity vocalizations, two or more moderate intensity vocalizations, or one or more high intensity vocalizations). For body codes, scores ranged from 0 (body posture never reflects emotion) to 3 (many instances of low intensity, two or more instances of moderate intensity, or one or more instance of high intensity). This resulted in six codes (Facial Sadness, Vocal Sadness, Bodily Sadness, Facial Anger, Vocal Anger, Bodily Anger) for each task, which were then summed to create the composite variables of Frustrative Non-Reward and Loss. For the Popping Bubbles task, expression, intensity, and frequency of positive affect was coded using facial, vocal, and bodily indicators, in the same manner described above, with low scores reflecting low levels of positive affect and high scores reflecting high levels of positive affect, ranging from 0 to 3 or 4. Four codes (Facial Positive Affect, Vocal Positive Affect, Bodily Positive Affect, Anticipatory Positive Affect) were then summed to create the composite variable of Responsiveness to Reward.
Analytic preparation and plan
Statistical analyses were conducted using IBM SPSS Statistics 26. All study variables were inspected and deemed normal. Missing value analysis revealed 6% of values across all study variables were missing. Little’s (Reference Little1988) Missing Completely at Random test was nonsignificant, demonstrating that these data were missing completely at random; χ2 (127) = 137.65, p = .24. Markov Chain Monte Carlo multiple imputation methods were used to avoid power loss related to listwise deletion. As only 6% of total data values were missing, the standard five imputations were performed using all available study variables. The primary analyses for the study therefore used pooled parameter estimates generated by this procedure.
For the first aim of testing differences in executive functioning, episodic memory, and emotion reactivity outcomes by trauma exposure, we conducted a series of one-way ANCOVAs. Unadjusted and adjusted (controlling for child age and gender) analyses were conducted for each model. The first set of ANCOVAs included cumulative trauma (a three-level variable coded as exposure to 0, 1, or 2+ categories of traumatic events) as the fixed effect, and one outcome variable at a time. Following the same procedure, the second set of ANCOVAs included interpersonal trauma (coded as 0 = no interpersonal trauma and 1 = interpersonal trauma) as the fixed effect. Bonferroni corrections were employed for post hoc comparisons.
For the second aim of examining family socioeconomic adversity and parental depressive symptoms as potential moderators of associations between trauma exposure and executive functioning, episodic memory, and emotion reactivity outcomes, we conducted an additional series of ANCOVAs with two fixed factors and their interaction (cumulative trauma and interpersonal trauma as predictors, and family socioeconomic adversity and parental depressive symptoms as moderators). Again, both unadjusted and adjusted (controlling for child age and gender) analyses were conducted.
Results
Descriptive analyses
Descriptive statistics for study variables are presented in Table 1 and bivariate correlations are presented in Table 2. Regarding participants’ cumulative trauma exposure, 38.6% of children had experienced 0 types of traumatic events, 28.4% 1 type of traumatic event, and 33.4% 2 or more types of traumatic events. Of the children experiencing 2 or more types of traumatic events, 14.8% experienced 2 types, 14.8% 3 types, 1.1% 4 types, and 2.3% 5 types. Regarding participants’ interpersonal trauma exposure, 31.4% had experienced interpersonal trauma (i.e., physical abuse, sexual abuse, and/or witnessing violence). Regarding specific types of traumatic experiences, 10.3% of children experienced physical abuse, 4.6% experienced sexual abuse, 26.7% witnessed violence, 10.2% experienced an accident (e.g., car crash), 8% experienced an animal attack, 3.4% experienced a man-made disaster, 1.1% experienced a natural disaster, 4.6% experienced an accidental burning, 2.3% experienced a near drowning, 14.8% experienced a life-threatening hospitalization/medical procedure, 9.3% learned that one of these events happened to a caregiver, and 24.4% experienced another type of traumatic life event.
Table 1. Descriptive statistics for full sample

Table 2. Correlations among study variables

Note. Socioeconomic Adversity = Family Socioeconomic Adversity; Parental Depressive Symp. = Parental Depressive Symptoms. Inhibit. Control (Tower) = Inhibitory Control measured in LAB-Tab Tower of Patience. Inhibit. Control (Flanker) = Inhibitory Control measured in NIH Toolbox Flanker Inhibitory Control and Attention Test. *** p < .001, ** p < .01, *p < .05.
Primary analyses
Cumulative trauma and NIH toolbox-based neurocognitive outcomes: executive functioning, episodic memory, and cognitive composite
As shown in Table 3, analysis of variance revealed a significant main effect of cumulative trauma group (0, 1, or 2+ types of traumatic events) on episodic memory, F (2, 87) = 3.21, p = .046. However, this main effect was no longer significant when adjusting for age and sex, F (2, 85) = 2.85, p = .06. Given that age and sex were not significantly associated with episodic memory at the correlational level, post hoc comparisons using Bonferroni correction were conducted for the model without covariates. These comparisons showed significantly higher episodic memory scores in the 0 trauma group (M = 99.97, SE = 2.9) compared to the 2+ traumas group (M = 89.24, SE = 3.3; p = .049). The means for the 0 trauma and 1 trauma groups (p = .99) and 1 trauma and 2+ traumas groups (p = .22) did not differ from each other. Results also revealed a main effect of trauma group on the overall cognitive composite, F(2, 87) = 3.25, p = .044. This main effect remained significant when adjusting for age and sex, F(2, 85) = 3.28, p = .043. Post hoc comparisons using Bonferroni correction indicated a trend towards significance, such that cognitive composite scores in the 0 trauma group (M = 92.99, SE = 2.2) were higher than those of the 2+ traumas group (M = 85, SE = 2.4; p = .052). The means for the 0 trauma and 1 trauma groups (p = .99) and 1 trauma and 2+ traumas groups (p = .17) did not differ from each other. Main effects of trauma group on executive functioning components were not found.
Table 3. Results of analyses of variance for cumulative trauma and NIH toolbox-based outcomes

Interpersonal trauma and NIH toolbox-based neurocognitive outcomes: executive functioning, episodic memory, and cognitive composite
As shown in Table 4, analysis of variance revealed a significant main effect of interpersonal trauma group (interpersonal versus no interpersonal trauma) on the overall cognitive composite, F(1, 88) = 8.19, p = .005. This main effect remained significant when adjusting for age and sex, F (1, 86) = 9.39, p = .003. Post hoc comparisons using Bonferroni correction indicated significantly higher cognitive composite scores in the no interpersonal trauma group (M = 92.75, SE = 1.6) compared to the interpersonal trauma group (M = 83.81, SE = 2.4; p = .003). No other main effects of interpersonal trauma group on executive functioning or episodic memory were found.
Table 4. Results of analyses of variance for interpersonal trauma and NIH toolbox-based outcomes

Cumulative trauma and lab-TAB-based outcomes: emotion reactivity
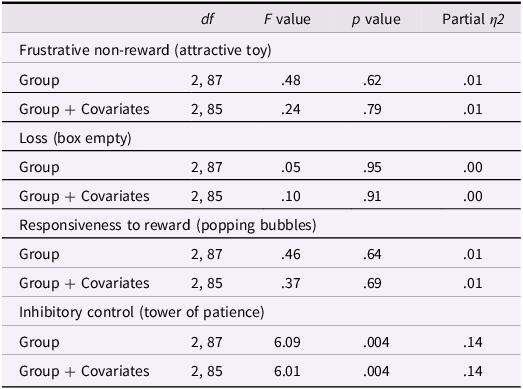
As shown in Table 5, analysis of variance revealed a significant main effect of cumulative trauma group (0, 1, or 2+ types of traumatic events) on inhibitory control measured during the Tower of Patience task, F(2, 87) = 6.09, p = .004. This main effect remained significant when adjusting for age and sex, F(2, 85) = 6.01, p = .004. Results showed higher levels of inhibitory control in girls compared to boys, F(1, 85) = 7.47, p = .008, and a positive association between child age and inhibitory control, F(1, 85) = 4.71, p = .03. Post hoc comparisons using Bonferroni correction indicated significantly higher levels of inhibitory control in the 0 trauma group (M = 3.49, SE = .22) compared to the 2+ traumas group (M = 2.55, SE = .25; p = .02), and higher levels of inhibitory control in the 1 trauma group (M = 3.70, SE = .26) compared to the 2+ traumas group (p = .006). The means for the 0 trauma and 1 trauma groups did not differ from each other, p = .99. The main effect of cumulative trauma group on each of the other Lab-TAB-based outcomes was not significant.
Table 5. Results of analyses of variance for cumulative trauma and lab-TAB-based outcomes
Interpersonal trauma and lab-TAB-based outcomes: emotion reactivity
As shown in Table 6, analysis of variance revealed a significant main effect of interpersonal trauma group (interpersonal versus no interpersonal trauma) on inhibitory control measured during the Tower of Patience task, F(1, 88) = 4.04, p = .048. This main effect remained significant when adjusting for age and sex, F(1, 86) = 4.14, p = .046. Results showed higher levels of inhibitory control in girls compared to boys, F(1, 86) = 6.82, p = .011, and a positive association between child age and inhibitory control, F(1, 86) = 4.33, p = .041. Post hoc comparisons using Bonferroni correction indicated significantly higher levels of inhibitory control in the no interpersonal trauma group (M = 3.44, SE = .18) compared to the interpersonal trauma group (M = 2.75, SE = .27; p = .046). The main effect of interpersonal trauma group on each of the other Lab-TAB-based outcomes was not significant.
Table 6. Results of analyses of variance for interpersonal trauma and lab-TAB-based outcomes

Interactions with family socioeconomic adversity and parental depressive symptoms
To examine contextual risk factors that may explain variation in associations between trauma exposure and neurocognitive and emotional processing outcomes, we tested interactions between the two grouping variables (cumulative trauma or interpersonal trauma) and two potential moderators (family socioeconomic adversity and parental depressive symptoms), with and without covariates. None of the tested interaction terms were associated with Lab-TAB-based or NIH Toolbox-based outcomes (results shown in Tables 7-10).
Table 7. Results of analyses of variance for cumulative trauma, moderators, and NIH toolbox-based outcomes

Table 8. Results of analyses of variance for interpersonal trauma, moderators, and NIH toolbox-based outcomes

Table 9. Results of analyses of variance for cumulative trauma, moderators, and lab-TAB-based outcomes

Table 10. Results of analyses of variance for interpersonal trauma, moderators, and lab-TAB-based outcomes

Discussion
The present study tests associations between early childhood trauma and components of executive functioning, episodic memory, and emotion reactivity in young children, representing a novel exploration of multiple interrelated neurocognitive and emotional processes implicated in the development of psychopathology. This study extends prior work that established general associations between trauma and neurocognitive functioning by exploring the nuance within and among these constructs (e.g., expanding how trauma and neurocognitive/emotional outcomes are operationalized and measured). Consistent with a bioecological approach, this study also sought to assess potential interactive effects between trauma and family contextual factors given the importance of context early in development (Bronfenbrenner, Reference Bronfenbrenner1979).
Extant research has demonstrated a link between trauma exposure in early childhood and deficits in neurocognitive and emotional processes in older children and adolescents, but few studies have examined these relations in a sample of preschool- to young school-age children, which constitutes a developmental period marked by rapid growth in executive functioning and social-emotional skills (Best & Miller, Reference Best and Miller2010). The present study also tested two operationalizations of trauma exposure (cumulative trauma and interpersonal versus non-interpersonal trauma) given their potential significance for an early childhood population. Rather than using a broad, all-encompassing measure of executive functioning, or examining only one facet of executive functioning (e.g., cognitive flexibility), as has been done in previous research, this study included multiple salient neurocognitive – as well as emotional – outcomes. Furthermore, this study used data collected in an early childhood day treatment program, rather than the child welfare system, which resulted in a broad array of traumatic experiences rather than a narrower focus on maltreatment, as well as exploration of neurocognitive and emotional processes in children with acute and severe clinical presentations who are at high risk for continued psychiatric symptomatology.
Our hypotheses were partially supported, as there was an association between cumulative trauma and episodic memory, and both cumulative trauma and interpersonal trauma and the overall cognitive composite. Results also indicated that both cumulative trauma and interpersonal trauma were related to inhibitory control, as assessed with the Tower of Patience Lab-TAB task. These findings add to our knowledge of how early trauma exposure is linked (or not linked) with neurocognitive and emotional outcomes during this sensitive developmental period. Surprisingly, family socioeconomic adversity and parental depressive symptoms were not found to add additional risk for impaired neurocognitive functioning.
Trauma and NIH toolbox-based neurocognitive outcomes
Inhibitory control and cognitive flexibility
We first hypothesized that cumulative and interpersonal trauma would be negatively associated with inhibitory control, cognitive flexibility, episodic memory, and overall cognition, assessed using the NIH Toolbox. Neither inhibitory control nor cognitive flexibility were related to whether children had experienced 0, 1, or 2 or more categories of traumatic events, or interpersonal versus non-interpersonal trauma. The lack of association between trauma and inhibitory control is in contrast to most studies conducted with school-age children and adolescents, wherein lower levels of inhibitory control were found in youth who were exposed to trauma compared to their non-exposed counterparts (van der Bij et al., Reference van der Bij, den Kelder, Montagne and Hagenaars2020). However, these results are consistent with some studies conducted with young children, which found no association between trauma and inhibitory control (Cipriano-Essel et al., Reference Cipriano-Essel, Skowron, Stifter and Teti2013; Giuliano et al., Reference Giuliano, Roos, Farrar and Skowron2018). One explanation for the lack of association between trauma and inhibitory control in this sample might be that there is a floor effect of inhibitory control in early childhood, given that many young children struggle to inhibit their responses at this developmental stage (Dowsett & Livesey, Reference Dowsett and Livesey2000; van der Bij et al., Reference van der Bij, den Kelder, Montagne and Hagenaars2020), and that may be especially true for children with acute behavioral concerns. Another possibility may be that inhibitory control measured via the Flanker task in the NIH Toolbox does not assess the more complex components of inhibitory control that map onto daily functioning in the lives of young children; to get a clearer picture of the effects of trauma on inhibitory control in this population, more emotionally salient and ecologically valid outcome measures may be helpful, such as the Tower of Patience task in the Lab-TAB battery (van der Bij et al., Reference van der Bij, den Kelder, Montagne and Hagenaars2020).
The non-significant association between trauma and cognitive flexibility also departs from prior research with school-age children demonstrating that greater trauma exposure is associated with reduced cognitive flexibility (Carvalho et al., Reference Carvalho, Renner, Donat, de Moura, Fonseca and Kristensen2018; DePrince et al., Reference DePrince, Weinzierl and Combs2009; Perna & Kiefner, Reference Perna and Kiefner2013). However, these results do mirror findings from a recent study of preschool-age children, which found no association between cumulative trauma and a measure of executive functioning that largely relied upon cognitive flexibility (Cohodes et al., Reference Cohodes, Chen, Lieberman and Bush2020). Such variability in findings could be due to several factors, one of which relates to the numerous cognitive flexibility paradigms and tasks that are available. A consensus neurocognitive battery for trauma research, similar to the MATRICS battery in schizophrenia (Nuechterlein et al., Reference Nuechterlein, Green, Kern, Baade, Barch, Cohen, Essock, Fenton, Frese, Gold, Goldberg, Heaton, Keefe, Kraemer, Mesholam-Gately, Seidman, Stover, Weinberger, Young and Marder2008), would likely help reduce the heterogeneity of neurocognitive findings.
Episodic memory
Executive functioning deficits are often more robust than memory deficits after trauma (e.g., Gervasio et al., Reference Gervasio, Beatty, Kavanaugh, Cancilliere and Holler2022; Kavanaugh et al., Reference Kavanaugh, Dupont-Frechette, Jerskey and Holler2017); however, current findings in this sample of young children are somewhat inconsistent with this notion. Cumulative trauma, but not interpersonal trauma, was associated with episodic memory, such that children who had experienced no traumatic events had higher episodic memory scores than children who had experienced two or more categories of traumatic life events. This association was no longer significant when child age and gender were entered into the model, though notably these covariates were not correlated with episodic memory. The current findings are consistent with a small body of work with school-age children demonstrating that maltreatment may impair initial verbal and visual learning and encoding abilities, the latter of which aligns with the PSMT task used in the present study (Berthelot et al., Reference Berthelot, Paccalet, Gilbert, Moreau, Mérette, Gingras, Rouleau and Maziade2015, Kavanaugh et al., Reference Kavanaugh, Dupont-Frechette, Jerskey and Holler2017). Furthermore, in a recent study of a younger cohort of psychiatrically hospitalized children ages 7–12, a prior history of sexual abuse was associated with lower scores on measures of episodic and working memory, though the working memory finding was more robust (Gervasio et al., Reference Gervasio, Beatty, Kavanaugh, Cancilliere and Holler2022). Episodic memory, or the initial learning and encoding of verbal or visual information, is traditionally considered to be more dependent on executive functioning abilities such as inhibitory control (i.e., to be able to focus on stimuli or a task) and working memory (i.e., to be able to hold presented information in mind) than on non-executive functioning memory abilities such as delayed retrieval (McCabe et al., Reference McCabe, Roediger, McDaniel, Balota and Hambrick2010). It is therefore unclear whether the current findings related to episodic memory reflect risk for future or long-term executive functioning deficits, memory deficits, or a combination. Prospective, longitudinal studies should examine relations between episodic memory and components of executive functioning (e.g., inhibitory control and working memory) over the course of development, and specifically, whether executive/frontoparietal and memory/hippocampal vulnerabilities differ depending on the developmental period of trauma.
Cognitive composite
Both cumulative trauma and interpersonal trauma were associated with an overall cognitive composite score using the Flanker, DCCST, PSMT, and TPVT scores. More specifically, post hoc comparisons revealed a trend-level effect (p = .052) for cumulative trauma, such that young children who were exposed to no traumatic events had higher cognitive composite scores than children exposed to two or more categories of traumatic events. Post hoc comparison results were statistically significant for interpersonal trauma, such that children who were exposed to interpersonal trauma had lower cognitive composite scores than children not exposed to interpersonal trauma. Associations may have been driven by scores on the PSMT and TPVT as these tasks are more associated with global cognitive development than specific to one domain (e.g., executive functioning). This reflects research demonstrating that neurocognition is unified in early childhood and may not differentiate into separate neurocognitive domains until later in development (Mungas et al., Reference Mungas, Widaman, Zelazo, Tulsky, Heaton, Slotkin, Blitz and Gershon2013). Research should continue to explore developmental trajectories of cognition following trauma, including assessments of global cognition along with more specific components of cognition. Importantly, the current findings are consistent with a large body of research that has found associations between trauma and deficits in global cognition in preschool- and school-age children as well as adolescents (Young-Southward, 2020). This study expanded on these prior findings by specifying trauma exposures, indicating that cumulative trauma and interpersonal trauma may both be important for global cognitive abilities in young children.
Trauma and lab-TAB-based emotion reactivity outcomes
Inhibitory control
We also hypothesized that cumulative and interpersonal trauma would each be associated with lower levels of inhibitory control, higher levels of negative affect (i.e., frustrative non-reward, loss), and lower levels of positive affect (i.e., responsiveness to reward). Both cumulative and interpersonal trauma were associated with inhibitory control assessed during the Tower of Patience task. Children who had experienced either no traumatic events or one category of traumatic event had higher levels of inhibitory control than children who had experienced two or more categories of traumatic events, which supports the premise that cumulative trauma may be a salient predictor of neurocognitive and emotional outcomes (Putnam et al., Reference Putnam, Harris and Putnam2013). Likewise, children who had experienced a type(s) of non-interpersonal trauma, such as a car accident or natural disaster, had higher levels of inhibitory control than children who had experienced a type(s) of interpersonal trauma, including sexual abuse, physical abuse, and/or witnessing violence. This finding suggests that exposure to relationally based traumatic events may hold great import for young children’s capacities to control and inhibit responses, consistent with the early childhood literature (Hagan et al., Reference Hagan, Browne, Sulik, Ippen, Bush and Lieberman2017).
It is notable that early childhood trauma was associated with inhibitory control in the Tower of Patience task but not the NIH-Toolbox Flanker task; in fact, these two measures of inhibitory control were not correlated. These contrasting findings may be due to the nature of each task. The Tower of Patience is a relational task, wherein the child was playing a game with the examiner, and over time the examiner required the child to wait for longer and longer intervals before their next turn. Interestingly, this task may more closely represent a real-world situation that young children are often faced with at home and in early learning settings. The Flanker task, on the other hand, is an individual, computerized task that required the child to respond to a target stimulus while ignoring other distracting information. These results are consistent with research differentiating between “hot” versus “cool” executive functioning (Zelazo & Carlson, Reference Zelazo and Carlson2012). Cool executive functioning is thought to take place when the individual is engaging with abstract, decontextualized problems without a significant affective or motivational component, like the Flanker, while hot executive functioning operates in motivationally and emotionally significant situations, like the Tower of Patience (Zelazo & Carlson, Reference Zelazo and Carlson2012). Research has shown that impairments in hot executive functioning can occur in the absence of impairments of cool executive functioning, and vice versa; for example, within the early childhood realm, children were more likely to select a larger, delayed reward over a smaller, immediate reward when asked which reward the experimenter should choose (“cool” paradigm), but were more likely to choose the immediate reward when asked to choose for themselves (“hot” paradigm; Prencipe & Zelazo, Reference Prencipe and Zelazo2005). The current study provides additional support for hot versus cool inhibitory control processes in young children, extending this to the context of early childhood trauma. It may be that young children who have experienced more categories of trauma or interpersonal trauma display difficulties with inhibitory control in affectively relevant and relational contexts – situations that relate to everyday interactions with caregivers – but perform at a similar level as children who have experienced little or no trauma (or no interpersonal trauma) on tasks that do not elicit emotion or take place in a relational context. Future studies should continue to examine differences in hot and cool inhibitory control based on context in populations of young children exposed to trauma. Furthermore, this work supports the relevance of assessing differences in context while examining individual-level factors, which is in line with a bioecological viewpoint (Bronfenbrenner, Reference Bronfenbrenner1979). Use of the RDoC framework allowed for a more expansive view of individual neurocognitive and emotional processes, including inhibitory control, which includes both cognitive and emotional components, and opened the door for greater exploration of context by measuring inhibitory control using two different tasks – one relationally based and one individual. This study therefore represents one emerging example of how RDoC and bioecological frameworks can be integrated; future work should further consider how to bridge these frameworks.
Frustrative non-reward, loss, and responsiveness to reward
Surprisingly, both operationalizations of trauma were unrelated to emotion reactivity, including frustrative non-reward (e.g., excessive anger and/or sadness in response to thwarted attempts to obtain an expected reward), loss (e.g., excessive anger and/or sadness when faced with a disappointing outcome), and responsiveness to reward (e.g., positive affect in response to participating in a fun and engaging activity). This contrasts with prior research, primarily in samples of older children, which found higher levels of negative emotionality and lower levels of positive emotionality in school-age children and adolescents who had experienced trauma compared to those who had not (Lavi et al., Reference Lavi, Katz, Ozer and Gross2019; McLaughlin & Lambert, Reference McLaughlin and Lambert2017; Weissman et al., Reference Weissman, Bitran, Miller, Schaefer, Sheridan and McLaughlin2019). A possible explanation for the null findings in this study may be that the association between trauma and emotion reactivity is especially context dependent in early childhood. For instance, young children have been shown to display different emotional reactions and regulation strategies based on the emotional expressions of their caregivers, and caregivers’ reactions to children’s own emotional expressions (Bariola et al., Reference Bariola, Gullone and Hughes2011; Morris et al., Reference Morris, Silk, Steinberg, Myers and Robinson2007). In environments with caregivers who suppress or punish their own and others’ emotional expressions, children may learn to suppress emotion, or otherwise alter their expressions, as well (Gross & Cassidy, Reference Gross and Cassidy2019; Lobo & Lunkenheimer, Reference Lobo and Lunkenheimer2020). This has been shown to be the case in families with maltreatment histories especially (Gruhn & Compas, Reference Gruhn and Compas2020). In the current study, emotional reactivity was observed outside the home environment and without the presence of a caregiver or other adult who had a longstanding relationship with the child. Further research is needed to compare emotion reactivity in more naturalistic contexts, such as during caregiver-child interactions, with emotion reactivity in lab-based settings among young children with early trauma exposure. Caregiver emotionality and responses to child emotion must also be assessed to more fully understand associations between trauma exposure and emotion reactivity in early childhood as these factors may serve as important moderator variables.
Interactions with family contextual factors
Although we were unable to examine the role of caregiver emotionality and parenting behavior in associations of early childhood trauma exposure and neurocognitive and emotional outcomes, we were able to examine other family contextual factors, including socioeconomic adversity and parental depressive symptoms. However, family socioeconomic adversity and parental depressive symptoms did not moderate associations between trauma and neurocognitive and emotional outcomes. This finding was contrary to hypotheses as well as prior literature focused on young children (Granat et al., Reference Granat, Gadassi, Gilboa-Schechtman and Feldman2017; Hughes et al., Reference Hughes, Roman, Hart and Ensor2013; Priel et al., Reference Priel, Zeev-Wolf, Djalovski and Feldman2020; St. John et al., Reference St. John, Kibbe and Tarullo2019; Ursache & Noble, Reference Ursache and Noble2016; Wang & Dix, Reference Wang and Dix2017). As described above, it is likely that caregiver emotionality and responses to child emotion are central to child emotional and behavioral functioning. These factors, as well as other dimensions of parenting, such as sensitivity and responsiveness, may be more proximally related to outcomes among young children than is socioeconomic status and parental mental health given that children observe and experience these parenting processes in their everyday lives, and parents often buffer children from their socioeconomic and psychiatric distress (Crockenberg & Leerkes, Reference Crockenberg and Leerkes2003; Norcross et al., Reference Norcross, Bailes and Leerkes2020; Zhou et al., Reference Zhou, Cao and Leerkes2017). Indeed, associations of socioeconomic adversity and parental depression with parenting behavior are not consistently observed, are often small in magnitude, and are frequently moderated by other factors (Bernard et al., Reference Bernard, Nissim, Vaccaro, Harris and Lindhiem2018; Roubinov & Boyce, Reference Roubinov and Boyce2017). From a bioecological perspective, parenting falls within the microsystem level, which is the layer closest to the individual, while socioeconomic adversity and parental depressive symptoms fall within the mesosystem or exosystem levels (Bronfenbrenner, Reference Bronfenbrenner1979). Future studies should move beyond socioeconomic status and parental mental health to examine aspects of parenting, including parental sensitivity, as potential moderators of the impact of trauma exposure in early childhood at the microsystem level.
Limitations and future directions
Although this study is a novel contribution to the literature on early childhood trauma exposure and interrelated neurocognitive and emotional processes in an understudied age group, its findings should be interpreted within the context of the study’s limitations. First, it is important to note that children in this sample had acute behavioral and emotional challenges and were from treatment-seeking families, and thus may not be representative of trauma-exposed children in the general population. More research with young children in other community-based and treatment settings will be beneficial. Second, while a strength of the study was testing multiple neurocognitive and emotional processes, including two components of executive functioning, the third component of executive functioning – working memory – was not assessed. Given the importance of working memory for overall executive functioning (Nigg, Reference Nigg2017), this component should be included in future studies. Third, and relatedly, this study took a less conservative univariate approach, rather than a multivariate approach. Due to the uniqueness of the sample and the relatively small size, generating hypotheses for future research is more likely to emerge from less strict analyses, i.e., individual test results presented with Bonferroni corrections and effect sizes. However, this approach does not account for covariance among outcome variables, and therefore, when replicating these results, future studies should consider taking a more conservative approach to analyses. Furthermore, we do encourage replication of these results given that this is best practice in the social sciences, especially given the current sample size. Fourth, this study is cross-sectional and therefore causal assumptions cannot be made. Future prospective, longitudinal studies should assess both trauma exposure and neurocognitive and emotional outcomes at multiple time points to clarify the role and timing of trauma exposure in the development of cognitive and affective abilities. Moreover, while all traumatic events measured in the study took place in early childhood, specific timing of events was not assessed. The developmental timing of trauma has been shown to be an important predictor of cognitive, behavioral, and emotional outcomes (Jackson et al., Reference Jackson, McGuire, Tunno and Makanui2019). For example, in one study, children who had experienced maltreatment in infancy had lower levels of inhibitory control and working memory compared to children who had experienced maltreatment in later developmental periods (Cowell et al., Reference Cowell, Cicchetti, Rogosch and Toth2015). Future studies should clearly identify in which developmental periods traumatic events occurred.
There are several other important limitations related to assessment, conceptualization, operationalization, and analysis of trauma exposure. Namely, children’s exposure to a number of different traumatic events was assessed through parent interview; while this is common in early childhood research, previous research has highlighted discrepancies between parent-report, child-report, multi-informant assessment, and case file coding methods (Cooley & Jackson, Reference Cooley and Jackson2022). Future studies should consider multiple approaches to assessing trauma exposure to obtain a more comprehensive understanding of children’s experiences. Beyond assessing the type of experiences that occurred, children’s interpretations and appraisals of their experiences may be more potent in predicting subsequent neurocognitive and emotional processes (Pollak & Smith, Reference Pollak and Smith2021). Although this study extended prior research by distinguishing between cumulative trauma and interpersonal trauma, which approximate categorical versus dimensional approaches, respectively, these conceptualizations are still limited. Specifically, the interpersonal trauma composite did not include emotional abuse or neglect, and other forms of neglect were not assessed at all, making it impossible to test a dimensional, threat versus deprivation model, or other more sophisticated conceptualizations (McLaughlin et al., Reference McLaughlin, Sheridan, Humphreys, Belsky and Ellis2021). Research should also move beyond a simple count of different types of exposures by incorporating severity, frequency, and duration into models (Jackson et al., Reference Jackson, McGuire, Tunno and Makanui2019). To this end, researchers may consider using person-centered analytic approaches, such as latent class analysis or latent profile analysis, which are particularly well-suited for elucidating patterns of trauma exposure, and may improve understanding of the combinations of exposure types, severities, and other characteristics that confer greatest risk for neurocognitive and emotional problems. Other contextual variables, including family risk factors like parental depression or socioeconomic adversity, could also be incorporated into classes or profiles using person-centered analytic approaches. In summary, assessment, conceptualization, operationalization, and analysis of trauma exposure is complex, and requires even greater thoughtfulness for the field to progress.
Conclusions
When study results are taken together, it is clear that exposure to trauma has differential effects on neurocognitive and emotional processes assessed in early childhood (i.e., trauma was generally associated with episodic memory, global cognitive ability, and inhibitory control measured in a relational task, but not cognitive flexibility, emotion reactivity, or inhibitory control measured in an individual, computerized task). The current findings highlight the importance of assessment context, suggesting that for young children with acute psychiatric presentations, trauma may be more likely to impair neurocognitive and emotional processes that take place within relationally significant, rather than decontextualized, contexts. These findings emphasize the value of investigating multiple neurocognitive and emotional processes simultaneously and across development – using relational and non-relational paradigms – to specify transdiagnostic targets for early intervention in young populations exposed to trauma (Pacheco et al., Reference Pacheco, Garvey, Sarampote, Cohen, Murphy and Friedman-Hill2022). Our results show that it may not be enough to simply identify inhibitory control as a potential transdiagnostic mechanism, for example, without also considering context; consideration of context will allow for the development of more specific and nuanced interventions, such as family-based treatments for helping young children develop inhibitory control skills within their interactions with others, which may reduce psychopathology and improve social-emotional and cognitive functioning.
Funding statement
This project was supported by the National Institute of Mental Health under grant number R21MH115514 (JB, AS). Dr Huffhines received support from the Eunice Kennedy Shriver National Institute of Child Health and Human Development under grant number K23HD107243 (LH). Dr Parade was supported by the National Institute of General Medical Sciences under Award Number P20GM139767 (SP). Dr Kavanaugh received support from the National Institute of Mental Health under grant number K23MH129853 (BK). This information or content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by the National Institutes of Health (NIH) or the U.S. Government.
Competing interests
The authors declare none.











 Open access
Open access