The prevalence of obesity in children and adolescents has reached epidemic proportions worldwide and is associated with many co-morbidities( 1 – Reference Cattaneo, Monasta and Stamatakis 3 ). Paediatric obesity is closely linked to the so-called ‘obesogenic’ environment where a myriad of factors is conducive to eating too much and not moving enough, thereby promoting weight gain and ultimately overweight and obesity( Reference Swinburn, Egger and Raza 4 , Reference Swinburn, Sacks and Hall 5 ). Among the many factors that explain the susceptibility to gain weight, a better understanding of the link between eating behaviours and weight gain is of crucial importance to overcome the rising rates of obesity.
Obesity interventions have to consider individuals’ eating behaviours, especially those that have been associated with obesity and weight gain( Reference Gallant, Tremblay and Pérusse 6 , Reference Chaput, Leblanc and Pérusse 7 ). For example, dietary restriction can promote overeating in dietary restrained adolescents having disinhibited eating behaviour( Reference van Strien, Herman and Verheijden 8 ). Additionally, adolescents with high restrained eating behaviour scores are more likely to gain weight over time( Reference Snoek, Engels and van Strien 9 ). Properly assessing eating behaviours of children and adolescents remains challenging, however.
In 1985, Stunkard & Messick developed the Three-Factor Eating Questionnaire (TFEQ) as a self-reported scale based on the restraint( Reference Polivy and Herman 10 ) and latent obesity( Reference Meyer and Pudel 11 ) theories, to assess dietary restraint (restriction of food intake to control weight), disinhibition (tendency to overeat opportunistically) and hunger (responsiveness to internal hunger sensations). While this initial version of the TFEQ developed in adults has been shown to clearly link eating behaviours with weight gain and weight-loss success( Reference Bryant, King and Blundell 12 – Reference Stunkard and Messick 15 ), it has been recently revised into a shorter twenty-one-item version (TFEQr21) focusing on restraint, uncontrolled eating and emotional eating( Reference Cappelleri, Bushmakin and Gerber 13 ). In this last version, although the restraint dimension remains unchanged, uncontrolled eating refers to eating in response to food palatability and the likelihood to overconsume, and emotional eating represents the process to eat in response to negative moods( Reference Cappelleri, Bushmakin and Gerber 13 ).
Despite a significant body of literature regarding the utility of the TFEQ in adults( Reference Cappelleri, Bushmakin and Gerber 13 – Reference de Medeiros, Yamamoto and Pedrosa 18 ), the validity of this TFEQr21 remains to be tested among children and adolescents. Martín-García et al. ( Reference Martín-García, Vila-Maldonado and Rodríguez-Gómez 19 ) recently reported a strong association between body composition and cognitive restraint in 7–17-year-old Spanish youth using a modified version of the Spanish adult TFEQ. These results highlight the usefulness of the TFEQr21 in children, but only in a limited population. It thus remains important to develop and validate a specific version of the English TFEQr21 for children and adolescents to better characterize their eating behaviour traits and evaluate the impact of obesity interventions in this population.
The objective of the present study was to develop an adapted-version of the adult TFEQr21 to be used among children and adolescents (CTFEQr17) and to assess its psychometric properties and factor structure. We also examined the associations between the CTFEQr17 and BMI and food preferences as a secondary objective.
Methods
The process of developing and validating the CTFEQr17 comprised two phases: the CTFEQr17 was developed in phase 1 and validated in phase 2. Each phase is detailed below.
Phase 1: Development of the CTFEQr17
Participants
A sample of seventy-six children (thirty-nine boys and thirty-seven girls) recruited between 2013 and 2014 from primary and secondary schools in North and West Yorkshire, UK were interviewed to determine their understanding of the original TFEQr21( Reference Cappelleri, Bushmakin and Gerber 13 ) items and to develop the wording of the CTFEQr17 (mean age: 12·3 (sd 1·4) years; mean BMI: 19·1 (sd 2·5) kg/m2; mean BMI percentile: 59·4 (sd 25·8)). All children, their guardians and the school gave informed consent for participation. Children who had any known eating disorders or eating issues, or who had difficulties with reading were excluded from participation (n 5). These children were identified by parents and/or teachers. The project gained full ethical approval from the University of Bradford Ethics Committee.
Qualitative design
The children took part in one-to-one structured interviews with the researchers. The child was presented with the adult version of the TFEQr21( Reference Cappelleri, Bushmakin and Gerber 13 ) and was asked whether he/she understood each item, if he/she understood how to respond to each question and to put each item into his/her own words. The interviews allowed the researchers to determine the children’s understanding of each item. Sample percentages were calculated for correct understanding of each item. In addition, the wording the children used to describe each item was then used to develop the CTFEQr17. This was achieved by recording the most frequently used words and phrases for each item and adopting these words, and phrases, in the new items. The interviews were audio-recorded and transcribed for analysis. Two researchers independently analysed the children’s responses to try to reach a subjective consensus on the child responses.
Anthropometric measurements
Body weight was assessed using a Seca 877 weighing scale and was measured to the nearest 0·1 kg. Children wore loose and lightweight shorts and a T-shirt to be weighed. Height was measured while the child was barefoot, using a Leicester stadiometer, and was measured to the nearest 0·1 cm. BMI was calculated as [weight (kg)]/[height (m)]2. BMI percentiles were calculated using the WHO( Reference de Onis, Onyango and Borghi 20 ) criteria based on age and sex.
Phase 2: Validation of the CTFEQr17
A sample of 433 children (230 boys; mean age: 12·0 (sd 1·7) years; mean BMI: 19·7 (sd 4·5) kg/m2; mean BMI percentile: 57·6 (sd 30·9)) from primary and secondary schools in West Yorkshire and Lancashire, UK were recruited between 2016 and 2017. A sub-sample of forty-five children (twenty-three boys and twenty-two girls) took part in interviews to confirm their understanding of the CTFEQr17. All children, their guardians and the school gave informed consent for participation. Children who had any known eating disorders or eating issues, or who had difficulties with reading were excluded from participation (n 23). The project gained full ethical approval from the University of Bradford Ethics Committee.
Validation design
Children were asked to self-complete the CTFEQr17 and an adapted paper-based Leeds Food Preference Questionnaire (LFPQ), suitable for use with children( Reference Halford, Boyland and Cooper 21 ). The LFPQ consists of a list of common UK foods (e.g. crisps, strawberries, yoghurt, biscuits) and the child was asked to indicate if he/she would like to consume these foods. Responses were then coded and summed into preference for high-protein (eight items), high-fat (eight items), high-carbohydrate (eight items) and low-energy foods (eight items). Mean taste preference scores were also calculated for low-fat savoury foods (LFSA: twelve items), low-fat sweet foods (LFSW: five items), high-fat savoury foods (HFSA: eight items) and high-fat sweet foods (HFSW: seven items).
Anthropometric measurements
A sub-sample of children had their height and weight measured (131 boys and 122 girls). Anthropometric measures were taken using the same procedure as in phase 1.
Qualitative design
The children took part in structured one-to-one interviews with a researcher. They were presented with the CTFEQr17 and asked if they understood each item, understood how to respond to each question and asked to elaborate on what they thought each item meant, to confirm their understanding. Each interview lasted approximately 20 min. Interviews were audio-recorded and transcribed for analysis.
Statistical analysis
We calculated that a total sample of 338 would be sufficient (power ≈ 0·90, effect size=0·25, probability level=0·05) to run the planned analysis. An exploratory, varimax rotation, principal components factor analysis was carried out to determine the factor structure of the CTFEQr17. An item analysis was also conducted to confirm the internal consistency, item-convergent and item-divergent validity of the CTFEQr17 items. Bivariate correlations explored relationships between age and CTFEQr17 factors by sex, and ANOVA was used to determine differences between sex and age groups (7–10 years and 11–15 years) on each CTFEQr17 factor. Partial correlations, controlling for age, were used to examine relationships between CTFEQr17 factors and anthropometric measurements. Partial correlations, controlling for age and BMI, were also used to explore relationships between CTFEQr17 factors and food and taste preferences. Only correlations above 0·20 are reported. Groups were formed using a median split on cognitive restraint (CR), uncontrolled eating (UE) and emotional eating (EE) scale scores to create low and high CR groups (LCR and HCR), low and high UE groups (LUE and HUE) and low and high EE groups (LEE and HEE). ANCOVA was used to analyse differences in anthropometric measures (controlling for age) and in food and taste preferences (controlling for age and BMI) by sex and eating behaviour groupings. Effect size was measured through η 2. For the qualitative data, the children’s comments were used to determine their level of understanding of each item of the CTFEQr17 and percentages of the correctly understood items were calculated. Understanding of items between phase 1 and 2 was examined using t tests. The statistical software package IBM SPSS Statistics version 22 was used to conduct the analyses and the level of statistical significance was set at P<0·05 for all analyses.
Results
Phase 1: Development of the CTFEQr17
The qualitative data from the interviews with children revealed that there were a number of items in the TFEQr21( Reference Cappelleri, Bushmakin and Gerber 13 ) that the children had difficulty in understanding, particularly items 9, 17 and 21. To develop a more understandable questionnaire, these items were reworded, using the children’s own language, as ascertained from the interviews (see Appendix for the CTFEQr17). In addition, the children also deemed the response format of the TFEQr21 unclear and too complex; thus, the response format of the CTFEQr17 was altered to read ‘totally true’, ‘mostly true’ ‘mostly false’ and ‘totally false’, again utilizing the phraseology of the children from the interviews.
Phase 2: Validation of the CTFEQr17
Structure and internal consistency of the CTFEQr17
The data met the assumptions for factor analysis, with the Kaiser–Meyer–Olkin measure of sampling adequacy index=0·87 and a significant Bartlett’s test of sphericity (χ 2=2706·45, P<0·001), indicating that the correlations between items were sufficiently large for a principal component analysis. A varimax rotation principal component analysis initially revealed four factors with eigenvalue >1, which in combination explained 51·6 % of the variance. The factors of UE (items 3, 6, 8, 9, 12, 13, 15, 19 and 20) and EE (items 2, 4, 7, 10, 14 and 16) were retained as in the original TFEQr21. However, CR loaded into two factors: CR1 (items 1, 5 and 11) and CR2 (items 17, 18 and 21). The items in CR1 are related to current food restriction behaviour, whereas CR2 is related to more prospective food restriction behaviours. However, following the removal of weak items due to low inter-item and item-to-total correlations and Cronbach’s α increasing after item removal (17, 18, 19 and 21), a three-factor structure was revealed, which explained 53·5 % of the variance. The factors of UE (items 3, 6, 8, 9, 12, 13, 15 and 20), EE (items 2, 4, 7, 10, 14 and 16) and CR (items 1, 5 and 11) were retained to create a CTFEQr17.
Following an analysis of internal consistency, the CTFEQr17 had a Cronbach’s α of 0·85, with the factors of UE (α=0·85) and EE (α=0·83) showing similarly high scores. The factor of CR had Cronbach’s α=0·67, which, although lower than UE and EE, was deemed adequate. The item analysis also revealed that the factors had adequate to good inter-item correlations for CR (r=0·38–0·47), UE (r=0·32–0·58) and EE (r=0·36–0·59), showing that the items within each scale correlated with one another. The corrected item-to-total correlations were good; CR (r=0·46–0·52), UE (r=0·53–0·63) and EE (r=0·55–0·70), with the items correlating most strongly with their respective factors, supporting item-discriminant and convergent validity. The factor of UE correlated significantly with EE (r=0·47, P<0·001) only (Table 1).
Table 1 Rotated factor structure loading of the new Child Three-Factor Eating Questionnaire (CTFEQr17)
Children’s understanding of the items
The qualitative aspect of the analysis, concerning the children’s understanding of the questionnaire items, revealed a very good level of understanding of the CTFEQr17. More specifically, in comparison to the original TFEQr21, all items of the CTFEQr17 were more understandable (mean understanding of 95 % v. 81 % for the original TFEQr21; see Fig. 1), where items 2, 9, 10, 11 and 12 were significantly more understood (P<0·05) compared with the original TFEQr21.
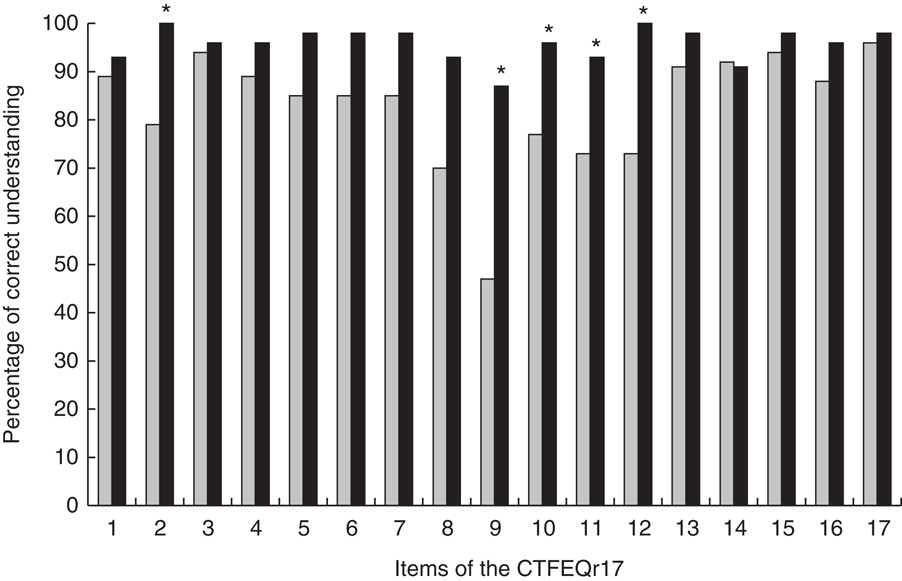
Fig. 1 Comparison of percentage correct understanding of items between the original Three-Factor Eating Questionnaire (TFEQr21; ![]() ) and the new Child Three-Factor Eating Questionnaire (CTFEQr17;
) and the new Child Three-Factor Eating Questionnaire (CTFEQr17; ![]() ) among a sub-sample of forty-five children and adolescents (twenty-three boys) recruited from primary and secondary schools in West Yorkshire and Lancashire, UK, in 2016–2017. *Understanding of the CTFEQr17 item was significantly higher than for the original TFEQr21 item (P<0·05)
) among a sub-sample of forty-five children and adolescents (twenty-three boys) recruited from primary and secondary schools in West Yorkshire and Lancashire, UK, in 2016–2017. *Understanding of the CTFEQr17 item was significantly higher than for the original TFEQr21 item (P<0·05)
Participant characteristics and CTFEQr17
For both boys and girls, UE correlated negatively with age (r=−0·32, P<0·001 and r=−0·25, P=0·001, respectively). CR correlated negatively with age for girls only (r=−0·21, P<0·01). No significant correlations for EE were found. Younger children scored higher on CR and UE (F (1,439)=4·56, P<0·05, η 2=0·01; and F (1,437)=34·61, P<0·001, η 2=0·07, respectively). Boys reported higher UE scores (F (1,437)=7·07, P<0·01, η 2=0·02). No differences by age and sex were found for EE (see Table 2).
Table 2 Factor scores on the new Child Three-Factor Eating Questionnaire (CTFEQr17), by age group and sex, among a sample of 433 children and adolescents (230 boys) recruited from primary and secondary schools in West Yorkshire and Lancashire, UK, 2016–2017

CR, cognitive restraint; UE, uncontrolled eating; EE, emotional eating.
* Boys had a significantly higher mean UE score compared with girls (P<0·001).
† Younger children had a significantly higher mean CR or UE score compared with older children (P<0·01).
CTFEQr17, body weight and BMI
After controlling for age, CR was found to correlate positively with weight (r=0·21, P<0·05), BMI (r=0·25, P<0·01) and BMI percentile (r=0·21, P<0·05) for girls only. No other associations were found.
Table 3 presents the participant characteristics by CTFEQr17 group. ANCOVA revealed that those with a HCR had a significantly higher weight (F (1,247)=8·29, P<0·01, η 2=0·04), BMI (F (1,247)=12·35, P=0·001, η 2=0·05) and BMI percentile (F (1,246)=8·41, P<0·01, η 2=0·04), regardless of sex. No significant differences between UE and EE groups and anthropometric measures were evident. Age was a significant covariate throughout these analyses (P<0·01).
Table 3 Body measurements, by groups of low/high factor scores on the new Child Three-Factor Eating Questionnaire (CTFEQr17) and sex, among a sample of 433 children and adolescents (230 boys) recruited from primary and secondary schools in West Yorkshire and Lancashire, UK, 2016–2017

CR, cognitive restraint; UE, uncontrolled eating; EE, emotional eating.
* Based on the World Health Organization criteria.
† Mean body measurement in the high CR, UE or EE group was significantly different compared with that in the low CR, UE or EE group (P < 0·05 to P < 0·001).
CTFEQr17, food and taste preferences
Younger children were found to have a higher food preference for all categories; high-carbohydrate foods (r=−0·33, P<0·001), high-fat foods (r=−0·24, P<0·001) and low-energy foods (r=−0·23, P<0·001). This was particularly so for younger girls compared with boys. BMI correlated negatively with high-carbohydrate food preference (r=−0·24, P<0·001). This association was found to be stronger in boys. No association between BMI percentile and food preference was found.
Partial correlations showed that UE was positively related to preferences for high-fat foods (r=0·26, P<0·001), high-protein foods (r=0·27, P<0·001) and high-carbohydrate foods (r=0·23, P<0·001). The relationships between UE and food preferences were found to be stronger in girls. Also, for EE significant relationships existed only for girls, for high-carbohydrate foods (r=0·25, P<0·01), high-protein foods (r=0·22, P<0·05) and high-fat foods (r=0·21, P<0·05). No significant correlations between CR and food preferences were found.
Food preferences were found to differ significantly between the CTFEQr17 groups (see Table 4). ANCOVA revealed for high-protein foods that the HUE group had a higher preference compared with the LUE group (F (1,241)=17·74, P<0·001, η 2=0·07). Boys consistently showed a higher protein preference, regardless of CR, UE and EE groups (F (1,242)=20·09, P<0·001, η 2=0·08; F (1,241)=14·98, P<0·001, η 2=0·06; and F (1,242)=18·28, P<0·001, η 2=0·07, respectively). Both the HUE and HEE groups reported a greater preference for high-fat foods (F (1,241)=16·79, P<0·001, η 2=0·07; and F (1,242)=5·45, P<0·05, η 2=0·02, respectively) and high-carbohydrate foods (F (1,241)=16·85, P<0·001, η 2=0·07; and F (1,242)=4·63, P<0·05, η 2=0·02, respectively). No differences were found for preference for low-energy foods. Age was a significant covariate throughout the analyses (P<0·001).
Table 4 Food and taste preferences, by groups of low/high factor scores on the new Child Three-Factor Eating Questionnaire (CTFEQr17) and sex, among a sample of 433 children and adolescents (230 boys) recruited from primary and secondary schools in West Yorkshire and Lancashire, UK, 2016–2017
CR, cognitive restraint; UE, uncontrolled eating; EE, emotional eating; LFSA, low-fat savoury; HFSA, high-fat savoury; LFSW, low-fat sweet; HFSW, high-fat sweet.
* Girls had a significantly different mean food/taste preference compared with boys (P < 0·05 to P < 0·001).
† Mean food/taste preference in the high CR, UE or EE group was significantly different compared with that in the low CR, UE or EE group (P < 0·05 to P < 0·001).
In terms of taste preference, younger children had a higher preference across most categories; LFSA (r=−0·25, P<0·001), LFSW (r=−0·23, P<0·001) and HFSW (r=−0·26, P<0·001). Taste preference was found to correlate more strongly for girls compared with boys. However, BMI was only found to correlate with taste preference in boys for HFSW foods (r=−0·24, P<0·01).
Partial correlations revealed that UE was positively correlated with preference for HFSA (r=0·31, P<0·001) and HFSW foods (r=0·27, P<0·001). When examined by sex, taste preference associations were stronger in girls: UE and EE with HFSW (r=0·38, P<0·001; and r=0·25, P<0·01, respectively) and HFSA foods (r=0·34, P<0·001; and r=0·20, P<0·05, respectively), and UE with LFSA foods (r=0·25, P<0·01). No taste preference associations were found with CR.
The CTFEQr17 groups also discriminated between taste preferences (see Table 4). ANCOVA revealed that, irrespective of CR, UE or EE group, boys consistently had higher preferences for LFSA foods (F (1,241)=6·50, P<0·05, η 2=0·03; F (1,240)=4·23, P<0·05, η 2=0·02; and F (1,241)=6·02, P<0·05, η 2=0·02, respectively) and HFSA foods (F (1,242)=9·44, P<0·01, η 2=0·04; F (1,241)=6·70, P=0·01, η 2=0·02; and F (1,242)=8·71, P<0·01, η 2=0·04, respectively). The HUE group had a higher preference for LFSA foods (F (1,240)=9·24, P<0·01, η 2=0·04). In addition, those with a HUE and HEE had a higher preference for HFSA foods (F (1,240)=18·66, P<0·001, η 2=0·09; and F (1,242)=3·62, P=0·058, η 2=0·02, respectively) and HFSW foods (F (1,241)=18·60, P<0·001, η 2=0·07; and F (1,242)=8·45, P<0·01, η 2=0·03, respectively). Age was a significant covariate throughout the analyses (P<0·001).
Discussion
The main aim of the present work was to propose a validated adaptation of the TFEQr21 among children and adolescents. According to our results, the proposed CTFEQr17 successfully assesses psychological eating behaviour traits in children and adolescents, and shows associations with body weight, BMI and food preferences. These findings are supported by qualitative data showing that the children had a good understanding of the CTFEQr17 items, confirming the strength and usefulness of this tool.
CTFEQr17 and anthropometric measures
A high CR score was shown to be associated with a higher body weight, BMI and BMI percentile in girls. This finding supports previous work with adolescents by van Strein et al. ( Reference van Strien, Herman and Verheijden 8 ), Snoek et al. ( Reference Snoek, Engels and van Strien 9 ) and Martín-García et al. ( Reference Martín-García, Vila-Maldonado and Rodríguez-Gómez 19 ). Evidence also supports a stronger association between adverse weight regulation and dietary restraint in girls compared with boys( Reference Halberstadt, van Strien and de Vet 22 ). These seemingly counter-intuitive findings are explained well with the goal conflict theory( Reference Stroebe, van Koningsbruggen and Papies 23 ). This theory posits that weight regulation issues are a result of the conflict between the goal of weight control and the goal of eating enjoyment; the hedonic expectation of food often undermines the goal of weight control( Reference Veling, Aarts and Papies 24 ). In the current obesogenic environment, replete with palatable foods, the goal of eating enjoyment is more often primed, requiring a higher cognitive effort to maintain the goal of weight control( Reference Stroebe, van Koningsbruggen and Papies 23 ). Such cognitive effort can easily become more difficult to maintain when other issues (e.g. emotions, work) reduce cognitive capacity available, resulting in the goal of eating enjoyment becoming much easier to access( Reference Stroebe, van Koningsbruggen and Papies 23 ). As a consequence, a less healthy eating pattern can occur, leading to a susceptibility to weight gain( Reference van Strien, Herman and Verheijden 25 ).
Although the goal conflict theory supports our results, conflicting evidence exists, as restrained eating has also been associated with lower food intake and better weight regulation( Reference Kemps, Herman and Hollitt 26 – Reference Roberts, Campbell and Troop 28 ). This suggests that some individuals are better able to maintain their weight control goal in comparison to their eating enjoyment goal. Thus, the relationship between CR and weight is complex, and CR likely interacts with other eating behaviour traits (e.g. disinhibition) to produce differing influences upon body weight( Reference Gallant, Tremblay and Pérusse 6 , Reference Bryant, Kiezebrink and King 29 ). That CR was associated with a higher weight and higher BMI in this child and adolescent sample supports a large body of adolescent and adult data, suggesting the CTFEQr17 has successfully measured this psychological construct.
Both UE and EE were found not to be related to anthropometric measures. This lack of association has also been found in adults( Reference Cappelleri, Bushmakin and Gerber 13 ). However, there is evidence suggesting that EE( Reference Anglé, Engblom and Eriksson 30 ), UE( Reference Martín-García, Vila-Maldonado and Rodríguez-Gómez 19 ,Reference de Lauzon, Roman and Deschamps 31 ) or both UE and EE( Reference Konttinen, Haukala and Sarlio-Lähteenkarva 32 , Reference Green, Schembre and White 33 ) are associated with higher weight and BMI in adolescents and adults. Where relationships have been found in adolescents( Reference Martín-García, Vila-Maldonado and Rodríguez-Gómez 19 ), the study sample consisted of overweight/obese and lean groups of children/adolescents. In the current study, children and adolescents were sampled from schools and not selected based on their weight status, thus having a lower proportion of overweight and obese participants. This could explain why associations with UE and EE were not found. In addition, where relationships have been found in adult samples, this has, at least partially, been attributed to food choice, whereby those with a higher UE and EE have a less healthful diet, higher energy intake and higher snack intake( Reference de Lauzon, Roman and Deschamps 31 , Reference Green, Schembre and White 33 ) and partake in less physical activity( Reference Green, Schembre and White 33 ). This suggests that the food preferences of UE and EE can impact adversely upon weight status.
CTFEQr17, food and taste preferences
Higher preferences for HFSA, HFSW, high-carbohydrate and high-fat foods were evident in those children who were characterized by higher UE and EE scores; this relationship was particularly strong in girls. This taste preference pattern reflects evidence from adult populations, which have shown a higher preference for high-fat foods in UE and EE adults( Reference Keskitalo, Tuorila and Spector 34 ). A preference for HFSW foods in individuals with a HEE has also been found to be particularly strong in women compared with men( Reference Keskitalo, Tuorila and Spector 34 ). This indicates that the taste preferences, and associated sex differences, found in adults are also found in children and adolescents, suggesting these preferences begin in childhood and persist into adulthood. Furthermore, UE and EE are characterized by eating in response to the palatability of food, eating opportunistically and eating in response to negative affect. Individuals with a HUE and HEE report a higher preference for high-fat (savoury and sweet) and high-carbohydrate foods( Reference Keskitalo, Tuorila and Spector 34 , Reference Camilleri, Méjean and Kesse-Guyot 35 ). These foods typically reflect highly palatable, energy-dense foods (e.g. crisps, sausage roll, biscuits, cakes). Due to their macronutrient content, these foods have a relatively low satiating ability( Reference Gerstein, Woodward-Lopez and Evans 36 ) and eating them can result in passive overconsumption( Reference Westerterp 37 ), increasing vulnerability to future weight gain( Reference Blundell and MacDiarmid 38 ). Indeed, this is reflected in adult data where UE and EE are related to higher body weight( Reference Konttinen, Haukala and Sarlio-Lähteenkarva 32 , Reference Green, Schembre and White 33 ).
Independently of CTFEQr17 scores, males were found to have a higher preference for high-protein, HFSA and LFSA foods. This pattern has previously been reported in children and adolescents( Reference Caine-Bish and Scheule 39 ) and adults( Reference Arganini, Saba and Comitato 40 ). In addition, younger children also reported higher food preferences than older children, regardless of gender; this has also been previously reported( Reference Caine-Bish and Scheule 39 ). Interestingly, food and taste preferences were more strongly related to psychological factors of the CTFEQr17 in girls than boys, whereas food preference was more strongly associated with anthropometric measures in boys. This is despite no difference in sex being reported for CR and EE, and boys scoring higher on the UE scale. Existing evidence purports that females tend to score more highly on CR, UE and EE in adolescents( Reference Vagstrand, Linne and Karlsson 41 ), on EE in adults( Reference Karlsson, Persson and Sjöström 14 , Reference Péneau, Ménard and Méjean 42 ) and on CR in adults( Reference Hainer, Kanesova and Bellisle 43 , Reference Provencher, Drapeau and Tremblay 44 ). Thus, females are reporting a higher influence of psychological eating behaviour traits over their eating behaviour. The reason for this sex difference is unclear and needs to be further elucidated.
Strengths and limitations
A strength of the present study is that the CTFEQr17 was both statistically and qualitatively verified as valid. The development of the CTFEQr17 involved creating accessible items by using the children’s/adolescent’s own phraseology ascertained from interviews. This produced a questionnaire that was highly understandable for children and adolescents. However, although associations between the CTFEQr17 and food and taste preferences were found, measurement of actual food intake was not carried out. Food preferences and the relationship between ‘liking’ and ‘wanting’ of foods have been found to be related to food intake( Reference Finlayson and Dalton 45 ) as well as associated with TFEQ factors in adults( Reference Finlayson, Bordes and Griffioen-Roose 46 ), thus an examination of this relationship in children and adolescents would be beneficial. A further limitation of the study is that body composition was not assessed, with research suggesting measurement of actual body composition is more accurate in determining relevant relationships than BMI( Reference Prentice and Jebb 47 , Reference Wells, Coward and Cole 48 ). Research by Martín-García et al. ( Reference Martín-García, Vila-Maldonado and Rodríguez-Gómez 19 ) also found an association between fat mass and CR in children and adolescents, therefore further exploration of this is of interest. Furthermore, although our sample size was adequate for the intended analysis, there was a larger proportion of secondary-school children; further consideration of the CTFEQr17 in primary-school children would be interesting. However, our sample did reflect that which was used to validate the Spanish TFEQr21C( Reference Martín-García, Vila-Maldonado and Rodríguez-Gómez 19 ).
Conclusion
The CTFEQr17 shows good internal consistency and is suitable for use in children and adolescents. The factor of CR was found to be associated with higher body weight, BMI and BMI percentile, thus those children who were larger showed more restrictive eating behaviours. Both UE and EE were associated with a higher preference for HFSA and HFSW foods, which is consistent with adult data and demonstrates that children with these eating behaviour traits have less healthy food preferences. Furthermore, a sex difference in the relationships between CTFEQr17 factors, anthropometric measurements and food preferences was apparent, whereby a stronger relationship was observed in girls. Collectively, the CTFEQr17 appears to be a valid and suitable tool to measure eating behaviour traits in children and adolescents.
Acknowledgements
Acknowledgements: The authors would like to thank the schools that participated in this study (Falinge Park High School, South Craven Secondary School, Otley All Saints Church-of-England Primary School, Sutton Church-of-England Primary School). They also thank the research assistants for helping with data collection (Matt Haigh, Amirah Akhtar, Naila Anjum, Alya Ponsford, Maria Rehmat, Sara Aslam, Anam Ayaz-Shah, Victoria Marshall, Paulina Jozwiak). Financial support: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Conflict of interest: The authors have no financial relationships relevant to this article or conflicts of interest to disclose. Authorship: E.B. designed the study, collected and analysed the data, and wrote the paper; D.T., J.-P.C., V.D., J.E.B. and N.A.K. advised on the design and contributed to the write-up. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the University of Bradford Ethics Committee. Verbal informed consent was obtained from all subjects. Verbal consent was witnessed and formally recorded.
Appendix
The Child Three-Factor Eating Questionnaire (CTFEQr17)
The items have been coded as in the original TFEQr21( Reference Cappelleri, Bushmakin and Gerber 13 ).
1. I eat small portions of food to help control my weight. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
2. I start to eat when I feel worried. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
3. Sometimes when I start eating, it seems I can’t stop. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
4. When I am sad, I usually eat too much. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
5. I don’t eat some kinds of food because they can make me fat. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
6. When I am next to someone who is eating, I also feel like eating. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
7. When I feel angry, I need to eat. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
8. I often get so hungry that I feel like I could eat loads of food without getting full. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
9. When I am hungry, I feel like to have to eat all of the food on my plate in one go, without stopping. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
10. When I feel lonely, I make myself feel better by eating. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
11. I eat less than I want at meal times to stop myself putting on weight. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
12. When I smell or see my favourite food, I find it hard to stop myself from eating it, even if I’ve just finished a meal. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
13. I’m always hungry enough to eat at any time. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
14. If I feel nervous, I try to calm myself down by eating. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
15. When I see something that looks delicious, I get so hungry that I have to eat it right away. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
16. When I feel really upset, I want to eat. Totally true (=4); mostly true (=3); mostly false (=2); totally false (=1).
17. How often do you feel hungry? Only at mealtimes (=1); sometimes between meals (=2); often between meals (=3); almost always (=4).