


Suicide is a leading causing of death for adolescents in the United States (Heron, Reference Heron2019; Verlenden et al., Reference Verlenden, Fodeman, Wilkins, Jones, Moore, Cornett, Sims, Saelee and Brener2024) and rates increased in the first two decades of the 21st century (Hoffmann et al., Reference Hoffmann, Farrell, Monuteaux, Fleegler and Lee2020). Suicidality (i.e., having suicidal thoughts, making plans, and/or attempting suicide) affects communities of color (Ivey-Stephenson et al., Reference Ivey-Stephenson, Demissie, Crosby, Stone, Gaylor, Wilkins and Brown2020; Kann et al., Reference Kann, McManus, Harris, Shanklin, Flint, Queen and Ethier2018; Wolf et al., Reference Wolf, Rivara, Orr, Sen, Chapman and Woolf2024), including Latino youth (Miron et al., Reference Miron, Yu, Wilf-Miron and Kohane2019; Twenge et al., Reference Twenge, Cooper, Joiner, Duffy and Binau2019), yet research on potential physiological biomarkers of adolescent suicidality has predominantly utilized White, European-American samples, and been cross-sectional. Two longitudinal studies have examined changes over time in suicidal thoughts and behaviors (STB) in Mexican-origin youth in the US (Gonzalves et al., Reference Gonzalves, Ferrer, Robins, Guyer and Hastings2023; Lawson et al., Reference Lawson, Kellerman, Kleiman, Bleidorn, Hopwood and Robins2021), yet neither included neurobiological predictors of future STB. Given the role of stressors as a trigger for STB (Yildiz, Reference Yildiz2020), social exclusion paradigms have been used to induce moderate stress in adolescents and study differences in physiological stress responses between youths with and without STB (Chesin et al., Reference Chesin, Cascardi, Tsang and Smith2020). In accord with the developmental psychopathology framework and bioecological models of stress vulnerability (Cicchetti, Reference Cicchetti, Beauchaine and Hinshaw2008; Hankin & Abela, Reference Hankin and Abela2005; Miller & Prinstein, Reference Miller and Prinstein2019), this prospective study was conducted to identify the concurrent and predictive associations of autonomic nervous system (ANS) regulation with STB in Mexican-origin adolescents.
After first documenting the rates of STB in representative studies of Latino youth, we proceed to make the case for focusing on the ANS as a key component of the body’s stress-regulation system. We present evidence, and the limitations of existing evidence, for the associations between parasympathetic and sympathetic activity and suicidal ideation and attempts during adolescence. We propose that examining autonomic activity during experiences of social exclusion may be particularly salient for understanding the stress responses of Mexican-origin youths that may either exacerbate or mitigate their risk for STB. Subsequently, we test this proposition utilizing 11 years of data on STB throughout adolescence provided by Mexican-origin youths, from whom basal and reactive autonomic data were obtained at 17 years.
STB in Latino youth
In the second decade of the 21st century (the 2010s), which overlaps with most of the period of data collection for the current study, suicide was the third most prevalent cause of death for young adolescents (10–14 years), and the second leading cause of death for older adolescents (15–19 years), across all races/ethnicities (Hedegaard et al., Reference Hedegaard, Curtin and Warner2020; Wolf et al., Reference Wolf, Rivara, Orr, Sen, Chapman and Woolf2024), and for Latino youth specifically (Benton, Reference Benton2022; Miron et al., Reference Miron, Yu, Wilf-Miron and Kohane2019). Suicide rates for high-school aged youth increased by more than 60% over this time (Hoffmann et al., Reference Hoffmann, Farrell, Monuteaux, Fleegler and Lee2020), with suicide rates increasing most rapidly for Black and Latino youth (Wolf et al., Reference Wolf, Rivara, Orr, Sen, Chapman and Woolf2024), and especially for Latina girls (Benton, Reference Benton2022).
Far more adolescents seriously consider and attempt suicide than actually die by self-injury. In the 2019 national Youth Risk Behavior Survey, 18.8% of high school-aged (14–18 years) students reported past-year suicidal ideation, 15.7% reported having made a plan, 8.9% reported attempting suicide, and 2.5% reported having made an attempt that required medical treatment, with female students reporting higher rates of all forms of STB than male students (Ivey-Stephenson et al., Reference Ivey-Stephenson, Demissie, Crosby, Stone, Gaylor, Wilkins and Brown2020). A striking trend for racial and ethnic differences in the 2019 survey was that although White high school students reported higher past-year rates of suicidal ideation (19.1%) and making a plan (15.7%) than Latino (17.2%, 14.7%, respectively) and African American students (16.9%, 15.0%, respectively), White students had lower rates of suicide attempts (7.9%) and attempts requiring hospitalization (2.1%) than Latino (8.9%, 3.0%, respectively) and African American students (11.8%, 3.3%, respectively) (Ivey-Stephenson et al., Reference Ivey-Stephenson, Demissie, Crosby, Stone, Gaylor, Wilkins and Brown2020). Racially/ethnically minoritized female students drove the higher rates of these most serious suicidal behaviors. National statistics vary across time and behaviors, however, with some years of the survey reporting the highest rates of past-year suicidal ideation for Latina youth (e.g., 22% in 2017) (Villarreal-Otálora et al., Reference Villarreal-Otálora, Jennings and Mowbray2019). In prior work with the current sample of Mexican-origin youths (Gonzalves et al., Reference Gonzalves, Ferrer, Robins, Guyer and Hastings2023), 38% of girls and 17.5% of boys had reported STB at least once by 17 years. STB clearly constitute a major health concern for Latino youth, making it critically urgent to pursue research on factors associated with STB that could be targeted in prevention and intervention programs for this community.
Roles of the autonomic nervous system in stress regulation
There is a critical need for more research on proximal risk factors for adolescent suicidality, including physiological indicators of acute stress dysregulation (Miller & Prinstein, Reference Miller and Prinstein2019). The ANS is responsible for the body’s automatic and unconscious responses to the external environment via its parasympathetic (PNS) and sympathetic (SNS) branches. Sympathetic activation increases somatic arousal, preparing the body for assertive or defensive action through reaction or retreat (i.e., “fight or flight”; Hastings & Kahle, Reference Hastings, Kahle, LoBue, Pérez-Edgar and Buss2019). The PNS, often referred to as the “rest and digest” system, supports multiple responses and functions including calming, regulation, orientation, and engagement (Hastings & Kahle, Reference Hastings, Kahle, LoBue, Pérez-Edgar and Buss2019). There are multiple measures of parasympathetic and sympathetic activity; two that are widely used in developmental psychophysiology and developmental psychopathology are respiratory sinus arrhythmia (RSA) and skin conductance responses (SCR), respectively (Zisner & Beauchaine, Reference Zisner, Beauchaine and Cicchetti2016). As an index of high-frequency heart rate variability, RSA reflects the variability in cardiac interbeat intervals associated with the respiratory cycle. As an index of electrodermal activity (EDA), SCR reflect acute decreases in the skin’s resistance to electrical current, attributable to perspiration of the eccrine glands.
There is moderate rank-order stability of individual differences in RSA and SCR measures across development (El-Sheikh, Reference El-Sheikh2007; Tuvblad et al., Reference Tuvblad, Gao, Isen, Botwick, Raine and Baker2012; Weiner & McGrath, Reference Weiner and McGrath2017). Despite this, basal RSA (tonic, or baseline) increases over childhood, with rates of change slowing or plateauing in late childhood to mid-adolescence (Dollar et al., Reference Dollar, Calkins, Berry, Perry, Keane, Shanahan and Wideman2020). Acute parasympathetic changes (phasic, or reactivity to stimuli or tasks) decrease in magnitude from childhood to adulthood (Hastings & Kahle, Reference Hastings, Kahle, LoBue, Pérez-Edgar and Buss2019; Zisner & Beauchaine, Reference Zisner, Beauchaine and Cicchetti2016). Basal and reactive electrodermal indices of sympathetic activity increase across early childhood, but both basal and acute SCR begin to decrease after middle childhood (Reinhard et al., Reference Reinhard, Slyschak, Schiele, Andreatta, Kneer, Reif, Domschke, Gamer, Pauli, Deckert and Romanos2022; Widegren et al., Reference Widegren, Vegelius, Frick, Roy, Möller, Kleberg, Hoppe, Hjorth, Fällmar, Pine, Brocki, Gingnell and Frick2025). There is some evidence, however, that the developmental trajectories of acute autonomic reactivity are not linear. More specifically, adolescents have been shown to mount stronger autonomic responses than children to various challenge tasks, especially for indices of sympathetic activity (Allen & Matthews, Reference Allen and Matthews1997; Stroud et al., Reference Stroud, Foster, Papandonatos, Handwerger, Granger, Kivlighan and Niaura2009).
Parasympathetic and sympathetic arousal influence how individuals respond to environmental stressors, including their ability to withstand perceived challenges and threats (Hastings & Kahle, Reference Hastings, Kahle, LoBue, Pérez-Edgar and Buss2019; Porges, Reference Porges2007). Tonic or basal ANS measures reflect a person’s typical levels of parasympathetic and sympathetic activation prior to encountering a potentially evocative stimulus, whereas phasic or reactive measures indicate how ANS activity has changed in response to such stimuli; hence, tonic and phasic measures offer complementary insights into the psychophysiology underlying individual differences in behavior. Higher tonic RSA and moderate withdrawal of parasympathetic influence (decrease in RSA) in reaction to aversive stimuli are associated with better emotion regulation (Beauchaine, Reference Beauchaine2015; Hastings et al., Reference Hastings, Kahle, Han and Lagattuta2014; Miller & Prinstein, Reference Miller and Prinstein2019), whereas lower tonic RSA and both stronger (greater decrease) and weaker RSA withdrawal (no decrease, or increase) to aversive stimuli are associated with emotion dysregulation and psychopathology (Beauchaine, Reference Beauchaine2012, Reference Beauchaine2015). Considering the sympathetic branch, increased SCR is associated with stress, affect, and attention (Gualniera et al., Reference Gualniera, Singh, Fiori and Santosh2021), with mild sympathetic arousal supporting increased vigilance to environmental cues, and greater arousal indicating a “fight or flight” response (Hastings et al., Reference Hastings, Zahn-Waxler and Usher2007). Disproportionate sympathetic responsivity, whether over-or under-arousal, impairs an individual’s capacity to cope effectively with their present situation (Keller et al., Reference Keller, Hicks, Miller, Cacioppo, Tassinary and Berntson2000) and is linked with multiple mental health issues including anxiety and depression (Asbrand et al., Reference Asbrand, Blechert, Nitschke, Tuschen-Caffier and Schmitz2017; Blechert et al., Reference Blechert, Michael, Grossman, Lajtman and Wilhelm2007).
The ANS has been conceptualized as a negative-feedback homeostatic regulatory system, in which greater sympathetic activity acts as an accelerator and greater parasympathetic activity as the brake, but prevailing theory posits that contributions of parasympathetic and sympathetic activation may act reciprocally, coactively, or even independently (Bertnson et al., Reference Berntson, Cacioppo and Quigley1993). In moderately stressful environments, modest sympathetic activation paired with mild parasympathetic withdrawal may be most adaptive, allowing individuals to actively engage with present stressors while maintaining effective regulation (Hastings & Kahle, Reference Hastings, Kahle, LoBue, Pérez-Edgar and Buss2019; Porges, Reference Porges2007). Hence, adolescents’ basal and acute stress responsive autonomic physiology facilitate different strategies for addressing environmental demands. It has been suggested that youth who fail to mount appropriate autonomic responses to challenges that support effective coping may be vulnerable to developing STB (Miller & Prinstein, Reference Miller and Prinstein2019).
Autonomic nervous system and STB
As cogently argued by Miller and Prinsten (Reference Miller and Prinstein2019), many of the germinal theories on suicidality shared themes of heightened affective distress and weakened emotion regulation as antecedents of STB, although these theories rarely made explicit connections to stress biology (but see Lineham, Reference Lineham1993). Neurobiological analogs of poor emotion regulation have been shown to characterize suicidal adults, compared to adults without STB, through relatively lower tonic and blunted reactivity of the SNS and PNS, or autonomic hypoactivity (McCall et al., Reference McCall, Rosenquist and Miller2022; Thorell, Reference Thorell2009). Yet, few of the existing neurobiological models of suicidality risk have been developmentally informed (Ludwig et al., Reference Ludwig, Roy, Wang, Birur and Dwivedi2017), despite adolescence being characterized by normative changes in stress-response systems, the onset or exacerbation of social stressors in family, peer and scholastic domains, and increasing prevalence of suicidal ideation and attempts (Miller & Prinstein, Reference Miller and Prinstein2019). In accord with bioecological and multi-level models of developmental psychopathology (Cicchetti, Reference Cicchetti, Beauchaine and Hinshaw2008; Cicchetti & Curtis, Reference Cicchetti and Curtis2007), autonomic indicators of biological vulnerability may increase susceptibility for a range of internalizing difficulties, including thoughts and actions of self-harm, during the adolescent period of increased stress (Hankin & Abela, Reference Hankin and Abela2005; Hastings et al., Reference Hastings, Kahle, Han and Lagattuta2014). Examining the autonomic biomarkers of suicidality risk in adolescence may benefit prevention and intervention programs, through the identification of biologically vulnerable youth who may be most in need of therapeutic attention, and by revealing tonic and reactive biomarkers that could be targeted to strengthen effective emotional and behavioral self-regulation through biofeedback and other therapies (Beauchaine et al., Reference Beauchaine, Hinshaw and Bridge2019; Miller & Prinstein, Reference Miller and Prinstein2019).
The limited extant developmental psychophysiology research, at first consideration, may appear to present a heterogenous set of autonomic correlates of STB in adolescents. This may be due, in part, to studies varying in their suicide criteria, such as targeting youths with suicidal ideation (e.g., Giletta et al., Reference Giletta, Hastings, Rudolph, Bauer, Nock and Prinstein2017), youths engaging in either suicidal or non-suicidal acts of self-harm (e.g., Crowell et al., Reference Crowell, Beauchaine, McCauley, Smith, Stevens and Sylvers2005), or youths reporting any thoughts or behaviors related to self-harm (e.g., Wielgus et al., Reference Wielgus, Aldrich, Mezulis and Crowell2016). Studies also have varied in their targeted ages of participants, from pre-teen (e.g., James et al., Reference James, Woody, Feurer, Kudinova and Gibb2017) to emerging adults (e.g., Chesin et al., Reference Chesin, Cascardi, Tsang and Smith2020). It is plausible that distinct aspects of suicidality may be associated differently with sympathetic and parasympathetic regulation, and that such patterns of biobehavioral coordination may change developmentally. Intriguingly, evidence for both specific and shared associations emerged in a meta-analysis of studies of the autonomic correlates of STB in individuals aged 25 years and younger (Bellato et al., Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023).
Across 10 studies, youths with STB evinced parasympathetic hypoactivity, as reflected in both lower basal and less reactive PNS activity, than youths without STB; these associations held across types of STB (ideation; suicidal self-harm; non-suicidal self-injury) and within both youth (7–17 years) and emerging adult (18–25 years) samples (Bellato et al., Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023). Conversely, across 6 studies of EDA, there were not robust associations between suicidality and measures of sympathetic activity, until Bellato and colleagues (Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023) examined types of STB. Samples that engaged in non-suicidal self-injurious behaviors evinced increased EDA, whereas samples with ideation alone or with broadly defined suicidality evinced reduced EDA, both relative to youths without STB. Collectively, these findings suggest that, like adults (McCall et al., Reference McCall, Rosenquist and Miller2022), youths with suicidal tendencies have suppressed parasympathetic activity, yet having greater versus less sympathetic activity may demarcate suicidal youths who are more versus less likely, respectively, to engage in self-harm.
Further support for a specific link between greater sympathetic reactivity and self-harm behaviors was found in an examination of older adolescents and emerging adults distinguished as engaging in either suicidal or non-suicidal self-harm in the past year, having self-harm ideation without action, or no evidence of self-harm thoughts or behaviors (Wetherall et al., Reference Wetherall, Cleare, Belkadi, Etherson, Loney, Mathew, Munro, Townsend, Nock, Ferguson and O’Connor2025). Although groups did not differ in basal EDA, adolescents who had engaged in active self-harm evinced significantly greater sympathetic reactivity in response to both physical (loud auditory tone) and social (Maastricht acute stress test) stressors, as shown through more SCR and higher skin conductance levels during the stress tasks. Sympathetic activation of the ideation group was intermediate to the other two groups, and not significantly different from that of adolescents without self-harm. These findings are notably different than those reported in studies of adults’ STB, which have consistently linked active suicidal behaviors with reduced SCR to stressors (McCall et al., Reference McCall, Rosenquist and Miller2022; Thorell, Reference Thorell2009). It has been suggested that the pathophysiology of suicidality may progress from hyperreactivity in adolescents to hyporeactivity in adults (O’Connor et al., Reference O’Connor, Ferguson, Green, O’Carroll and O’Connor2016; Wetherall et al., Reference Wetherall, Cleare, Belkadi, Etherson, Loney, Mathew, Munro, Townsend, Nock, Ferguson and O’Connor2025), a hypothesis that is in accord with some developmental elaborations of the allostatic load model (Blair & Raver, Reference Blair and Raver2012; Hastings et al., Reference Hastings, Guyer and Parra2022a).
It is important to note that the meta-analysis of Bellato and colleagues (Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023) considered associations between autonomic physiology and youths’ current or past STB. To our knowledge, there have been only two prospective longitudinal studies predicting youths’ future suicidality from baseline or reactive physiology. Giletta and colleagues (Reference Giletta, Hastings, Rudolph, Bauer, Nock and Prinstein2017) found that girls who evinced stronger parasympathetic reactivity, as shown by greater decreases in RSA to a public speaking task, were more likely to report suicidal ideation over the next 9 months (Giletta et al., Reference Giletta, Hastings, Rudolph, Bauer, Nock and Prinstein2017). Conversely, Wielgus and colleagues (Reference Wielgus, Aldrich, Mezulis and Crowell2016) found that weaker parasympathetic recovery from, but not reactivity to, a cognitive stressor predicted more suicidal and non-suicidal thoughts and behaviors 6 months later. Thus, although the meta-analysis showed that weaker parasympathetic activity is associated with current or past STB, the only two longitudinal studies of adolescents suggest that stronger or more prolonged parasympathetic reactivity may predict STB in the subsequent 6 to 9 months. Clearly, more research contrasting the concurrent and prospective associations between autonomic physiology and youth suicidality is needed.
Social exclusion as a stressor for Mexican-origin adolescents
Interpersonal adversity is a negative experience reliably associated with greater risk for psychopathology in adolescence (Platt et al., Reference Platt, Kadosh and Lau2013), including suicidality (Paul, Reference Paul2018). Social exclusion specifically is detrimental for adolescent wellbeing (Killen & Rutland, Reference Killen, Rutland and Ruck2011), can provoke feelings of social stress (Wang et al., Reference Wang, Braun and Enck2017), and confers risk for STB (Longobardi et al., Reference Longobardi, Morese and Fabris2020). Examining stress responses during social exclusion in Mexican-origin adolescents is apt, given the unfortunately common experience of racial and ethnic discrimination faced by Latino youth in the US (Benner & Graham, Reference Benner and Graham2011). Similar to other social stressor tasks used in previous studies of suicidality, using social exclusion to examine autonomic responses in a Mexican-origin adolescent sample could provide evidence for how particular stress responses are related to the likelihood of endorsing past or forthcoming suicidality in this understudied youth population.
To that end, in this study we used the social exclusion stressor task Cyberball (Williams & Jarvis, Reference Williams, Jarvis, Williams and Jarvis2006), a virtual ball-tossing game in which, across blocks of trials, participants become increasingly more excluded from play (i.e., the other avatars do not toss the ball to the player). Cyberball was designed to elicit feelings of exclusion, rejection, and ostracism, and it also can induce both sympathetic and parasympathetic activation (Holterman et al., Reference Holterman, Murray-Close and Breslend2016). Cyberball has been used to look at relations between stress physiology and suicidality. In response to a set of 3 tasks that included Cyberball, emerging adults with suicidal ideation were shown to evince less parasympathetic activation (smaller decreases, or increases, in RSA relative to basal) than those without suicidal ideation (Chesin et al., Reference Chesin, Cascardi, Tsang and Smith2020). In a study of family members related to a suicidal or non-suicidal adolescent, Kaufman et al. (Reference Kaufman, Crowell, Coleman, Puzia, Gray and Strayer2018) looked at family members’ RSA responses to Cyberball. Only family members of suicidal youths evinced decreased RSA during the latter half of the task, during which the most exclusion occurred; RSA of the two groups did not differ at baseline or during the earlier, primarily inclusive period of Cyberball.
Current study
Mexican-origin and other Latino adolescents are at risk for internalizing problems due to exposure to stressors such as ethnic discrimination (Brittian et al., Reference Brittian, Toomey, Gonzales and Dumka2013) and acculturation pressures (Wu et al., Reference Wu, Marsiglia, Ayers, Cutrín and Vega-López2020), suggesting it could be particularly important to gain insight into how their stress physiology is related to risk for STB. Considering the rise in suicidality amongst adolescents in the US, including in the Latino population (Benton, Reference Benton2022), measuring autonomic stress activity presents a unique opportunity to further examine whether unique biological markers are associated with past and prospective suicidality.
Given the documented associations between autonomic activity and STB, the current study measured both basal and task-responsive RSA and SCR in relation to past and subsequent suicidality in a sample of Mexican-origin adolescents. Prior work with this sample demonstrated that, compared to youths without reported STB, youths endorsing STB had lower effortful control and greater negative emotionality (Lawson et al., Reference Lawson, Kellerman, Kleiman, Bleidorn, Hopwood and Robins2021), lower familism and increased family conflict (Gonzalves et al., Reference Gonzalves, Ferrer, Robins, Guyer and Hastings2023), and were more likely to be female and US-born (Gonzalves et al., Reference Gonzalves, Ferrer, Robins, Guyer and Hastings2023). The present work evaluated how Mexican-origin adolescents’ basal and acute autonomic physiology may reveal patterns of responding to environmental demands that are associated with (1) prior history of suicidality and (2) subsequent reports of suicidality. Reasonably consistent findings in prior studies examining basal RSA and SCR reactivity in relation to adolescent STB supported making the following a priori hypotheses:
-
1. Mexican-origin youths with a history of STB were expected to evince lower basal RSA and less RSA activation than those without a history of STB.
-
2. Mexican-origin youths with a history of STB were expected to display fewer basal SCR and less SCR activation than those without a history of STB.
-
3. Tentatively, based on Giletta et al. (Reference Giletta, Hastings, Rudolph, Bauer, Nock and Prinstein2017), greater RSA activation was expected to predict greater likelihood of STB at follow-up.
-
4. Tentatively, based on Bellato et al. (Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023) and Wetherall et al. (Reference Wetherall, Cleare, Belkadi, Etherson, Loney, Mathew, Munro, Townsend, Nock, Ferguson and O’Connor2025), greater SCR activation was expected to predict greater likelihood of STB at follow-up.
Hypotheses 3 and 4 were tentative given the very limited prior research on prospective associations between autonomic physiology and STB. Recognizing that associations might differ for youths with suicidal ideation versus suicidal attempts (Bellato et al., Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023; Wetherall et al., Reference Wetherall, Cleare, Belkadi, Etherson, Loney, Mathew, Munro, Townsend, Nock, Ferguson and O’Connor2025), supplemental analyses were conducted that distinguished adolescents by type of STB. Multiple additional sensitivity analyses were conducted to determine the robustness of findings.
Method
Participants
Participants were 229 Mexican-origin adolescents (M = 17.16 years, SD = 0.44, 110 females) enrolled in a neurobiological sub-study of the California Families Project. The California Families Project began with 674 Mexican-origin families living in northern California with a child in fifth grade (M Age = 10.85 years, 50% female), drawn at random from school rosters during the 2006–2007 and 2007–2008 academic years. The sub-study was designed to examine neurobiological mechanisms in the etiology and development of depression in late adolescence. Thus, youths with elevated but sub-clinical depressive problems were oversampled from the full project sample, using counts of adolescents’ self-reported symptoms in 9th grade (ages 14–15) based on the Diagnostic Interview Schedule for Children-IV (DISC-IV; Shaffer et al., Reference Shaffer, Fisher, Lucas, Dulcan and Schwab-Stone2000) and the Anhedonic Depression and General Distress subscales of the Mood and Anxiety Symptom Questionnaire (Clark and Watson, Reference Clark and Watson1995). Scores above the sample median on any of these three measures indicated presence of risk for depression. A dichotomous recruitment variable referring to depression-risk (1 = scored above the median on any recruitment measure, n = 175; 0 = scored below the median on all measures, n = 54) was controlled for in analyses. No participants met diagnostic criteria for major depressive disorder based on the DISC-IV at the time of sample selection. The neurobiological sub-sample did not differ significantly from other participants in the larger study with respect to adolescent sex or age, or family income-to-needs ratios (all p > .05). Parents provided informed consent for their child’s participation and youths provided assent. This study was approved by the research site’s Institutional Review Board.
Procedure
For data collected as part of the larger California Families Project study, trained research staff interviewed participants in their homes in either Spanish or English, based on participant preference, annually from ages 10 to 19 years. Interviewers were all bilingual and most interviewers were of Mexican heritage. All youths elected to complete measures in English. Measures of STB were collected in the home visits, 7 of which preceded the neurobiological assessment (ages 10 to 16 years), and 3 of which followed it (ages 17 to 19 years; at 5, 17, and 31 months subsequently).
Youths’ neurobiological data were collected when participants were 16- to 17-years-old, between the seventh and eighth year of data collection for the California Families Project. Participants visited a university medical research facility with one parent and participated in a functional magnetic resonance imaging (fMRI) scan with simultaneous electrocardiogram (ECG) and EDA recordings. Over an hour after participants’ arrival, electrodes were affixed to the youths’ torso and hand, and after allowing several minutes for accommodation, baseline ECG and EDA were collected for 3 minutes while the participants were lying on the scanner bed, outside of the MRI scanner. Adolescents then completed a structural scan and a set of three tasks in the scanner; the second task was the social exclusion challenge, Cyberball (Eisenberger et al., Reference Eisenberger, Lieberman and Williams2003). After receiving instructions, participants played 12 rounds of Cyberball, including six Inclusion and six Exclusion rounds, always presented in the same pseudorandom order, with a brief inter-trial interval between each round. Throughout the Inclusion round, the other players were equally likely to throw the ball to the participant or each other. However, during Exclusion, near the beginning of the round, the other players stopped throwing the ball to the participant and continued throwing it only to each other. The rounds of the Cyberball task were configured to increase participants’ experiences of being excluded from play progressively over the task, but ending with an Inclusion round.
In addition to reporting STB during the home visits, youths reported on STB during a second medical research facility visit, providing a fourth assessment scheduled approximately 23 months following the initial neurobiological assessment. Thus, this assessment occurred between the aforementioned measures of STB in the annual home visits 17 and 31 months following the neurobiological assessment, providing a total of 4 measures of STB at 5, 17, 23, and 31 months after obtaining ECG and EDA data.
Measures
Suicidal thoughts and behaviors
To ensure discretion and given the sensitive nature of the STB questions, youths responded to the measures assessing STB without the help of the interviewers (i.e., youths reported their responses directly on a computer that was turned away from interviewers), apart from the administration of the clinical interview (e.g., DISC or DIS, depending on age).
History of STB. History of STB was captured by utilizing participants’ responses to two instruments, the NIMH Computerized Diagnostic Interview Schedule for Children (CDISC-IV; Shaffer et al., Reference Shaffer, Fisher, Lucas, Dulcan and Schwab-Stone2000), administered annually from ages 10 to 16 years, and a brief suicide questionnaire adapted from the Youth Risk Behavior Survey (YRBS; Brener et al., Reference Brener, Kann, Shanklin, Kinchen, Eaton, Hawkins and Flint2013), administered annually from ages 11 to 16. The CDISC-IV is a fully structured diagnostic interview designed for non-clinicians to measure common psychiatric symptoms in children (Shaffer et al., Reference Shaffer, Fisher, Lucas, Dulcan and Schwab-Stone2000). In the annual assessments when participants were in 5th through 11th grade, youths responded to two DISC-IV items assessing STB: “During the last year, (1) was there a time when you thought seriously about killing yourself? …, (2) have you tried to kill yourself?” (0 = no, 1 = yes). The YRBS questionnaire included three items to assess STB in the past 12 months: “Have you thought about committing suicide?”; “Have you made a plan for committing suicide?”; “Have you attempted suicide?” (1 = never, 2 = once, 3 = twice, 4 = 3 or more times).
After visits were completed and interviews were examined by research staff, parents were contacted if their child reported having any imminent thoughts of self-harm and/or suicide. Although study questions did not specifically probe for imminent risk, the study protocol dictated that if a youth spontaneously reported active suicidality, research staff should inform caregivers and make appropriate referrals to services. There were no occurrences of active suicidality.
A dichotomous STB score was derived from the two DISC-IV items in 5th grade, and the DISC-IV plus YRBS items in all subsequent years (i.e., 6th–11th grade). Participants’ affirmative responses to one or more of the items were scored as 1 (“yes”) for STB at that grade. Participants responding “never” or “no” to all items were scored as 0 (“no”) for STB at that grade. Finally, a bivariate History of STB variable was computed from the 7 assessments of STB from 10 to 16 years; participants were scored as 1 (“yes”) for History of STB if STB was present at one or more of the assessments, or 0 (“no”) if there was no indication of STB at any time from 5th through 11th grade.
Prospective STB. STB at follow-up were assessed using multiple instruments at four assessments over the 2.5 years following the autonomic physiology measurement. In home visits conducted through the larger California Families Project, all participants completed the DISC-IV at 5 months (M = 17.55 years, SD = 0.40) and the adult DIS-IV (Robins et al., Reference Robins, Cottler, Bucholz, Compton, North and Rourke1995) at 31 months (M = 19.73 years, SD = 0.44) after ANS was measured. Participants also completed the YRBS suicide items at the home visits occurring 5, 17 (M = 18.59 years, SD = 0.40), and 31 months subsequently. At 23 months following the physiology assessment (M = 19.05 years, SD = 0.59), participants returned to the same medical research facility and completed the Beck’s Depression Inventory (BDI; Beck et al., Reference Beck, Steer and Brown1996) and the Self-Injurious Thoughts and Behaviors Interview (SITBI; Nock et al., Reference Nock, Holmberg, Photos and Michel2007), each of which included multiple items that assessed STB. Across these four assessments, participants’ affirmative responses to one or more of the STB items on any of the instruments were scored as 1 (“yes”) for presence of STB, versus 0 (“no”). Finally, a bivariate Prospective STB variable was computed; participants were scored as 1 (“yes”) for Prospective STB if STB was present at one or more of the four assessments, or 0 (“no”) if there was no indication of STB at 5, 17, 23, and 31 months following the ANS data acquisition.
In addition to the STB protocols mentioned above, a clinical psychologist was on-call and available for consultation when participants endorsed STB on the BDI and SITBI measures. Additionally, for youths reporting imminent feelings of wanting to harm themselves, interviewers provided a mental health resource sheet and contracted the participant for safety until the youth could be transported to the nearest emergency department for evaluation. No youths died by suicide (or by any other cause) during the duration of the study.
Psychometric evaluation of the STB measures. The intra-class coefficients (ICC) for the items used to generate the STB scores across the 10 assessments from 11 to 19 years ranged from = 0.47 to 0.78 (M = 0.64) (see Supplemental Table 1). ICC could not be calculated for 10 years, as STB were assessed from only 2 items on the DISC. It should be noted that ICC and other reliability statistics have been shown to under-estimate true reliability when items have widely different variances (Mehta et al., Reference Mehta, Bastero-Caballero, Sun, Zhu, Murphy, Hardas and Koch2018; Metsämuuronen, Reference Metsämuuronen2023), as was the case for rarely endorsed items assessing suicide attempts compared to more frequently endorsed items assessing ideation and plans.
Next, we examined the STB measures’ factor structure and evidence for measurement invariance using confirmatory factor analyses (see Supplemental Information). Only 7 youths (3%) endorsed suicidal ideation at each of the first two assessments (10 and 11 years), and models including these assessments did not converge. A CFA including the 9 assessments of STB for ages 12 through 20 years had acceptable-to-good model fit statistics, CFI = 0.928, TLI = 0.920, RMSEA = 0.042, with all STB items loading highly on a single STB factor at each assessment (see Supplemental Table 2), indicating that the STB measures had configural invariance. We then ran a CFA model constraining item loadings to be equal across time points, but this model had significantly worse fit, X 2(9) = 49.427, p < .001, indicating a lack of evidence for the STB measures having metric invariance across assessments.
Physiological data processing
Respiratory sinus arrhythmia. ECG were collected simultaneously with the MRI scan using three electrodes on the chest connected with Biopac MRI compatible wireless signal logging (Biopac Systems, USA) through Siemens’ Physiological Monitoring Unit, with a sampling frequency of 400 Hz. Data were converted into an ASCII formatted string of amplitude values that then was fed into Mindware HRV (heart rate variability) software (Mindware Technologies, Gahanna, OH). The inter-beat-interval sequence was used to calculate RSA. Trained research assistants visually reviewed ECG data for accurate identification of R-spikes and corrected data when the automated program misinterpreted the R-spikes. RSA was calculated within the 0.12–0.40 frequency band. For the 3-min baseline recording, RSA was calculated in 30-s epochs, with the 6 epoch values then averaged to calculate basal RSA. For the Cyberball recording, RSA was calculated over the duration of each exclusion trial, which ranged from 22 to 32 s. The average of the RSA values for the 6 exclusion trials provided the measure of Cyberball social exclusion RSA. Inclusion trials were not included in these analyses. RSA data for 10 individuals during baseline and 27 during Cyberball were missing due to human error, equipment errors during sample collection, or high-frequency noise in the ECG signal caused by fMRI interference. RSA values are expressed in units of ln(ms2).
For sensitivity analyses (see below), RSA also was examined across the last half of the Cyberball task (Kaufman et al., Reference Kaufman, Crowell, Coleman, Puzia, Gray and Strayer2018). This period included 4 exclusion trials, 2 inclusion trials, and 5 inter-trial intervals (M = 212.65s, SD = 34.98). RSA was calculated in 30-s epochs, discarding final epochs that were shorter than 22 s; the epoch values then were averaged to calculate RSA across the latter half of Cyberball.
Skin conductance responses. EDA data were obtained before and during the MRI scan using two electrodes on the palm of the non-dominant hand using Biopac MP150 equipment and AcqKnowledge 4.1 software, with a gain of 10 μS (Biopac Systems, USA). To account for high-frequency noise in the fMRI signal, a rolling filter was applied using Mindware EDA software (Mindware Technologies, Gahanna, OH). For the 3-min baseline recording, including each 30-s segment, the number of nonspecific SCR with an amplitude change of 0.05 μS was counted (Braithwaite et al., Reference Braithwaite, Watson, Jones and Rowe2015) within each 30-s segment; these 6 values then were averaged to index basal SCR. For the Cyberball recording, SCR were counted within each Cyberball exclusion trial, and then the 6 values were averaged to index Cyberball social exclusion SCR. SCR data were missing for 7 youths during baseline and 15 during Cyberball.
Data analysis
Bivariate associations first were examined with zero-order correlations and t tests. Then, to test Hypotheses 1 and 2, we utilized two-way (2 × 2) mixed-design analyses of covariance (ANCOVA), with History of STB (prior disclosure of STB vs. no STB ever across 7 assessments from ages 10–16) treated as a between-subjects variable and ANS measurement (baseline vs. task) treated as a within-subjects variable. Separate ANCOVAs were conducted for RSA and SCR, examining whether having a prior history of suicidality was associated with participants’ autonomic stress physiology during baseline (prior to Cyberball) and social exclusion (during Cyberball). In each ANCOVA, we controlled for age, sex, depression recruitment status, antidepressant medication use, and body mass index (BMI) at the time of the physiology measurement.
To test Hypotheses 3 and 4, parallel two-way (2 × 2) mixed-design ANCOVA models were examined, with Prospective STB (disclosure of STB vs. no STB ever from 4 assessments across ages 17–19 years) treated as the between-subjects variable and the basal and task RSA and SCR measures examined in separate ANCOVAs. History of STB reported prior to the autonomic physiology assessment was included alongside the aforementioned 5 covariates. In addition, structural equation modeling (SEM) with a binary outcome was used as an alternative analysis to examine whether RSA and SCR at baseline and during Cyberball social exclusion made simultaneous and independent contributions to adolescents’ likelihood of Prospective STB. A dichotomous measure of Prospective STB (5–31 months following the ANS measurement) was regressed onto baseline and task scores (modeled as manifest predictors), as well as covariates. To examine whether the ANS variables accounted for a significant amount of the model variance, we ran three models: the 6 covariates only (Model 1); covariates plus basal RSA and SCR (Model 2); and covariates plus basal and social exclusion task RSA and SCR (Model 3) (see Figure 1).
Structural equation model predicting the presence versus absence of suicidal thoughts and behaviors in the 2.5 years following assessment of basal and Cyberball Exclusion RSA and SCR at 17 years, accounting for prior suicidality and demographic characteristics. Note. STB = suicidal thoughts and behaviors; RSA = respiratory sinus arrhythmia; SCR = skin conductance responses; BMI = body mass index; med use = use of antidepressant medication (0/1); recruit group = elevated depression scores at 14 years (0/1); history of STB = suicidal thoughts and behaviors reported from 10–16 years (0/1).

Figure 1. Long description
A diagram representing a structural equation model predicting the presence versus absence of suicidal thoughts and behaviors in the 2.5 years following assessment of basal and Cyberball Exclusion RSA and SCR at 17 years, accounting for prior suicidality and demographic characteristics. The diagram includes four main components under autonomic physiology: Basal RSA, Task RSA, Basal SCR, and Task SCR. These components are connected to a central box labeled Future STB. Additionally, there are covariates such as Age, Sex, BMI, Med use, Recruit group, and History of STB, which are also connected to Future STB. Arrows indicate the directional relationships between these components and Future STB.
Missing data and outliers. Data for all 229 youths were available for both STB variables (i.e., history of STB, and prospective STB). Across the covariates, missing data ranged from 0 to 4.4%. For the ANS (i.e., independent) variables, missing data range from 3.1% to 11.78%. To account for missing data in the independent variables (ANS variables) and covariates, we used full information maximum likelihood. To test for potential biases in the missing data, we ran Little’s (Reference Little1988) MCAR test and the data were determined to be treatable as missing completely at random, X 2 (67) = 62.43, p = .64. Model fit was evaluated using R-squared values across path analysis models.
Outliers (i.e., values greater than 3 standard deviations beyond the mean) in the dependent variables were winsorized to bring the values within 3 standard deviations of the mean. Descriptive statistics and repeated-measures ANCOVA analyses were run using SPSS 28. The path analysis was implemented using Mplus 8.0 (Muthén & Muthén, Reference Muthén and Muthén2017).
Sensitivity analyses. Multiple sensitivity ANCOVAs were conducted to probe the findings of the main models. (a) To determine whether any relations between STB and RSA as assessed during the Cyberball Task were an artifact of examining RSA within non-consecutive Exclusion trials, ANCOVAs for History of STB and Prospective STB were conducted using RSA across the latter half of the Cyberball Task (Kaufman et al., Reference Kaufman, Crowell, Coleman, Puzia, Gray and Strayer2018). (b) As reports on the SITBI and BDI may have varied from reports on the measures used across all other assessments, ANCOVAs and SEM for Prospective STB were run with STB assessed from reports on the DIS and SUIC only. (c) As the majority of youths who reported STB endorsed suicidal thoughts (ideation, plans) without behaviors (attempts), ANCOVAs for History of STB and ANCOVAs and SEM for Prospective STB were run excluding any youths who endorsed one or more items indicating suicide attempts in any assessment (n = 204). Finally, (d) ANCOVAs were run to test whether RSA and STB measures differed between youths who reported an attempt at any time (n = 25), youths who reported suicidal thoughts but no attempts (n = 68), and youths who never reported any STB (n = 136) (Wetherall et al., Reference Wetherall, Cleare, Belkadi, Etherson, Loney, Mathew, Munro, Townsend, Nock, Ferguson and O’Connor2025). These analyses are presented in the Supplemental Information and summarized succinctly in Results.
Results
Descriptive statistics
Descriptive statistics and zero-order correlations of key study variables are presented in Table 1. RSA activity significantly decreased from baseline to the social exclusion task, paired t(193) = 10.86, p < .001, whereas there was not a significant change in SCR, paired t(205) = .45, p = .65. Table 2 presents descriptive statistics and t tests comparing basal and task physiological measures for youths who did versus did not report history of STB, and who did versus did not report prospective STB. Over 27% of youths (n = 62) had endorsed STB at least once between 5th and 11th grade. Almost exactly the same number (n = 61) reported STB at least once during the 4 follow-up assessments over the next 2.5 years, 30 (49%) of whom had prior history of STB and 31 (51%) of whom had not. Cumulatively, 40.6% (n = 93) of the youths reported STB over the 11 assessments from 10 to 20 years, including 68 (29.7%) who reported suicidal ideation and/or plans for self-harm, but did not engage in suicidal self-harm, and 25 (10.9%) who reported one or more suicide attempts, in addition to suicidal thoughts. In t tests (see Table 2), participants who reported histories of STB had significantly lower basal SCR than youths without history of STB. Youths who reported prospective STB tended to evince lower basal (p = .060) and higher task (p = .051) SCR, and had significantly higher task RSA, compared to adolescents who did not report STB over the 2.5 years of follow-up assessments.
Descriptive statistics and zero-order correlations of key study variables

Note. BMI = Body Mass Index, STB = suicidal thoughts and behaviors, RSA = respiratory sinus arrhythmia, SCR = skin conductance response. Sex was coded as 1 = female (n = 110), 0 = male (n = 119). Medication use was coded dichotomously, 0 = no, 1 = yes. All physiological measures were recorded when participants came to the lab for the fMRI scan. Both history of and prospective STB were scored dichotomously, no = 0, yes = 1. Significant correlations are in bold and denoted as *p < .05, **p < .01; borderline effects † p < .10.
Means, standard deviations, and t-tests of ANS variables by history of STB and prospective STB groups
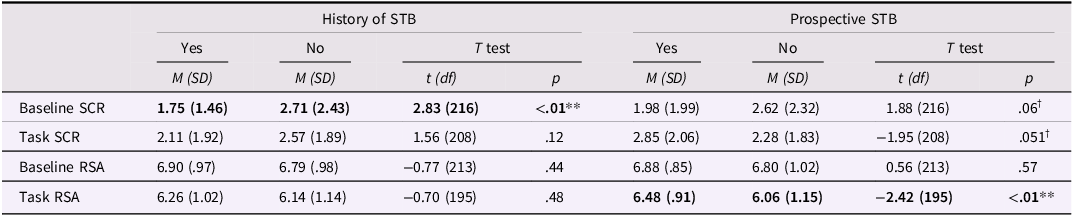
Note. ANS = autonomic nervous system, RSA = respiratory sinus arrhythmia, SCR = skin conductance response. Task refers to the Cyberball social exclusion trials. Both history of STB and prospective STB were scored dichotomously, yes = 1, no = 0. Significant correlations are in bold and denoted as **p < .01; borderline effects † p < .10.
History of STB predicting autonomic physiology
Hypothesis 1: RSA. Contrary to prediction, there were no significant main or interaction effects in the ANCOVA for RSA and history of STB. Adolescents with a history of STB did not differ in basal or task parasympathetic activity from youths without a history of STB.
Hypothesis 2: SCR. The ANCOVA for SCR revealed a significant main effect for history of STB, F(1,192) = 6.56, p < .05, partial η 2 = 0.03. As predicted, adolescents with a history of endorsing STB prior to the scan had overall lower SCR across baseline and social exclusion (M = 1.87, SD = 1.65; i.e., hypoactivation), compared to participants without a history of STB (M = 2.68, SD = 2.15). There also was a main effect of sex, F(1,192) = 4.64, p < .05, partial η 2 = 0.02, with male youths showing greater sympathetic arousal (M = 2.78, SD = 1.63) compared to female youths (M = 2.11, SD = 1.51).
Autonomic physiology prospectively predicting subsequent STB
Hypothesis 3: RSA. The ANCOVA for RSA revealed a significant measurement by prospective STB interaction, F(1,179) = 4.73, p < .05, partial η 2 = 0.03. Adolescents who did versus did not prospectively endorse STB did not differ in basal RSA, and contrary to predictions, youths who reported prospective STB had higher task RSA than did youths who did not endorse prospective STB (see Table 2). Considered another way, although RSA decreased significantly from baseline to social exclusion for both youths who endorsed prospective STB, paired t(52) = 3.81, p < .001, and those who did not endorse STB at follow-up, paired t(140) = 10.54, p < .001, the parasympathetic reactivity of the two groups differed significantly, t(192) = −2.228, p < .05. Youths who reported future suicidality had weaker parasympathetic reactivity than those who did not
Hypotheses 4: SCR. The ANCOVA for SCR revealed a significant measurement by prospective STB interaction, F(1,192) = 9.19, p < .01, partial η 2 = 0.05. Compared to participants who did not report future STB, those who went on to endorse future STB had lower basal SCR and, as predicted, higher task SCR (see Table 2). Considered another way, participants who went on to endorse STB evinced a significant increase in SCR from baseline to social exclusion, paired t(56) = −2.11, p < .05, whereas youths who did not endorse prospective STB showed a significant decrease in SCR from baseline to social exclusion, paired t(148) = 1.98, p = .050. The SCR reactivity of the two groups differed significantly, t(204) = −2.924, p < .01; youths who reported future suicidality had stronger sympathetic reactivity than those who did not.
Hypothesis 3 and 4: Path Analysis. Next, we implemented SEM with a binary outcome to examine basal and task RSA and SCR as simultaneous predictors of prospective STB over the 2.5 years following the physiology assessment (see Figure 1, Table 3). We ran three iterative models in a stepwise fashion to examine prediction of prospective STB from covariates alone (Model 1), covariates with basal ANS variables (Model 2), and covariates with basal and task ANS variables (Model 3). Model 1 produced a R 2 = .13; adding basal autonomic measures accounted for a non-significant unique 1% of variance in prospective STB, for R 2 = .14; and adding social exclusion autonomic variables accounted for a significant unique 12% of variance, for R 2 = .25.
Predictive associations between covariates, autonomic physiology scores, and prospective STB 5–31 months following the measurement of ANS activity: Results of path analysis with a binary outcome
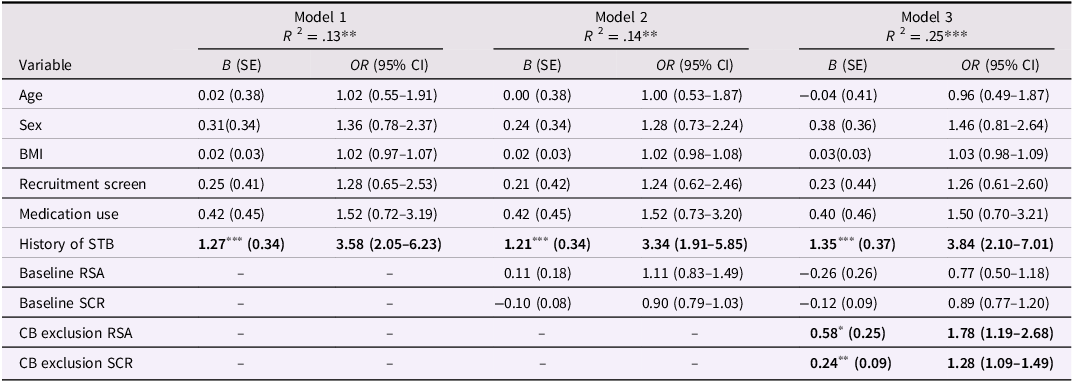
Note. STB = suicidal thoughts and behaviors; History of STB were scored as yes = 1, no = 0; RSA = respiratory sinus arrhythmia; SCR = skin conductance response; BMI = Body Mass Index; Sex was scored female = 1, male = 0; Recruitment Screen was scored as elevated depression scores = 1, lower depression scores = 0; Medication Use was scored as used antidepressants = 1, no antidepressant use = 0; CB = Cyberball. Significant effects in bold font, *p < .05, **p < .01., ***p < .001.
In all models, prior history of STB significantly increased the odds of reporting prospective STB. In Model 2, neither baseline SCR nor baseline RSA significantly predicted prospective STB. In the final model, both higher task SCR and higher task RSA were significantly predictive of increased likelihood of reporting STB at follow-up (see Table 3). Higher task SCR predicted a 28% increase in odds of subsequent STB, and higher task RSA predicted a 78% increase in odds of subsequent STB. Noting that, on average, Cyberball exclusion elicited parasympathetic withdrawal without sympathetic activation, this suggests that participants who displayed an opposite pattern of autonomic responses – smaller decreases in parasympathetic activity and larger increases in sympathetic activity during social exclusion trials, relative to baseline – were at greater risk for prospective suicidality 5 to 31 months later, supporting Hypotheses 4 but not Hypothesis 3.
Sensitivity analyses
-
a. In the ANCOVAs for RSA across the second half of the Cyberball task (Kaufman et al., Reference Kaufman, Crowell, Coleman, Puzia, Gray and Strayer2018) for history of STB and prospective STB, findings remained unchanged. History of STB prior to the physiological assessment was not associated with baseline or task RSA (see Supplemental Table 3), but the measurement by prospective STB interaction for RSA remained significant (see Supplemental Table 4). Higher RSA during the second half of Cyberball (i.e., less RSA suppression) predicted prospective STB over the next 2.5 years.
-
b. In the ANCOVAs for prospective STB measured using the YRBS and DISC/DIS only, the measurement by prospective STB interaction for RSA was slightly weaker, F(1,179) = 3.57, p = .060, partial η 2 = 0.02 (see Supplemental Table 5), and the measurement by prospective STB interaction for SCR remained significant (see Supplemental Table 6). The aforementioned associations of autonomic physiology with prospective STB did not change. Similarly, the Task RSA and Task SCR measures remained significant predictors of prospective STB in the SEM (see Supplemental Table 7).
-
c. The four ANCOVAs and SEM testing the hypotheses with only participants who never reported a suicide attempt (n = 204) are presented in Supplemental Tables 8 through 12. All the aforementioned findings of the main analyses remained significant, indicating that the described associations for basal and task autonomic measures pertained to past and future suicidal ideation, specifically.
-
d. Finally, descriptive statistics for the autonomic measures characterizing youths reporting suicide attempts at any time, youths reporting suicidal thoughts, and youths reporting no STB are presented in Supplemental Table 13, and the ANCOVAs comparing these groups for basal and task RSA and SCR are in Supplemental Tables 14 and 15. There were no significant effects in the ANCOVA for RSA. There was a significant measurement by Type of STB interaction for SCR, F(2,191) = 4.20, p < .05, partial η 2 = 0.04. Post-hoc Tukey’s tests showed that youths reporting attempts had lower basal SCR than youths reporting no STB, but no groups differed in task SCR. Considering SCR reactivity, youths reporting attempts tended to have greater sympathetic activation (SCR increase), paired t(119) = 1.971, p = .051, sympathetic activity did not change significantly for youths reporting ideation, paired t(63) = −0.692, ns, and youths reporting no STB tended to have sympathetic deactivation (SCR decrease), paired t(21) = −1.996, p = .059.
Discussion
Suicidal ideation and acts of self-harm were prevalent in this sample of Mexican-origin adolescents in Northern California. Across 11 assessments from ages 10 to 20 years, more than 40% (93/229) of youths reported STB at least once, with 48% (30/62) of those who reported STB prior to 17 years continuing to experience STB in emerging adulthood. Although no deaths by suicide (or other means) occurred over the study, almost 11% (25/229) of youths attempted suicide during their second decade of life. Although not directly comparable to past-year rates of suicidal thoughts and actions by Latino youth (Ivey-Stephenson et al., Reference Ivey-Stephenson, Demissie, Crosby, Stone, Gaylor, Wilkins and Brown2020; Villarreal-Otálora et al., Reference Villarreal-Otálora, Jennings and Mowbray2019), these high rates illustrate the importance of identifying factors conferring risk for suicidality in this community. Strikingly, our assessment of adolescents’ basal autonomic activity as well as autonomic responses to social exclusion, a potential stressor for this sample of Mexican-origin youth (Benner & Graham, Reference Benner and Graham2011), at 17 years distinguished both the youths with histories of prior suicidality, and those who went on to experience STB over the next 2.5 years, from youths who did not experience suicidality. To our knowledge, this is the first longitudinal study to document such associations of parasympathetic and sympathetic activity with suicidality in an exclusively Mexican-origin sample of adolescents. More importantly, our findings both converged with and diverged from patterns identified in prior psychophysiological studies of suicidality in samples of predominantly White youth (Bellato et al., Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023; Wetherall et al., Reference Wetherall, Cleare, Belkadi, Etherson, Loney, Mathew, Munro, Townsend, Nock, Ferguson and O’Connor2025), identifying multiple aspects of pathophysiology that could be targets of future work with this, and perhaps other, Latino communities.
Building on principles of developmental psychopathology and bioecological models of stress vulnerability (Cicchetti, Reference Cicchetti, Beauchaine and Hinshaw2008; Hankin & Abela, Reference Hankin and Abela2005), it has been proposed that maladaptive autonomic responses to challenges confer vulnerability to suicidality in adolescence (Miller & Prinstein, Reference Miller and Prinstein2019). Our demonstration that sympathetic hypoactivation across basal and task conditions was related to endorsing a history of suicidality replicates prior findings with youth (Bellato et al., Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023) and adult samples (McCall et al., Reference McCall, Rosenquist and Miller2022; Thorell, Reference Thorell2009). Conversely, there was no indication that basal or acute parasympathetic activity distinguished youth with versus without prior STB, unlike many prior studies with adolescents and adults (Bellato et al., Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023; McCall et al., Reference McCall, Rosenquist and Miller2022). Our study is the first to show that greater SCR activity paired with less RSA withdrawal to social exclusion, a pattern indicative of uncoupled sympathetic activation (Berntson et al., Reference Berntson, Cacioppo and Quigley1993, Reference Berntson, Norman, Hawkley and Cacioppo2008), predicted greater likelihood of future STB in the transition from late adolescence into early adulthood. Across the analyses, most relations of ANS measures with prior STB or future STB were consistently evident, with several associations becoming more robust as covariates were included in ANCOVA or SEM analyses. Supplemental analyses suggested that youth who reported having attempted suicide, such that their ideation advanced to engaging in self-harm behavior, may have been most prone to sympathetic hyperreactivity to social exclusion, a biobehavioral pattern that may distinguish those who attempt suicide in adolescence (Wetherall et al., Reference Wetherall, Cleare, Belkadi, Etherson, Loney, Mathew, Munro, Townsend, Nock, Ferguson and O’Connor2025) from adult attemptors, who often are found to have reduced SNS activity (McCall et al., Reference McCall, Rosenquist and Miller2022). Overall, our work provides further evidence for potential biomarkers of suicidality risk, extending prior research on developmental pathophysiology to include adolescents and emerging adults of Mexican origin.
The implications of our findings should be considered in the contexts of both the typical development of autonomic physiology in adolescence, and the nature of youths’ autonomic responses to the social exclusion task used in our study. Over the course of adolescence, one expects levels of basal SNS activity to decrease while basal PNS activity increases, contributing to tonic parasympathetic dominance (Dollar et al., Reference Dollar, Calkins, Berry, Perry, Keane, Shanahan and Wideman2020; Widegren et al., Reference Widegren, Vegelius, Frick, Roy, Möller, Kleberg, Hoppe, Hjorth, Fällmar, Pine, Brocki, Gingnell and Frick2025). At the same time, although the magnitude of acute ANS responses decreases somewhat over childhood, adolescents can have stronger autonomic, and particularly sympathetic, reactivity to challenge tasks than are observed in children (Allen & Matthews, Reference Allen and Matthews1997; Stroud et al., Reference Stroud, Foster, Papandonatos, Handwerger, Granger, Kivlighan and Niaura2009). In our sample, though, Cyberball evoked an average response of decreased RSA without change of SCR, or uncoupled parasympathetic withdrawal (Berntson et al., Reference Berntson, Cacioppo and Quigley1993). Although we did not examine youths’ subjective evaluations of their exclusion experiences, this dual-branch autonomic response may have prepared youths for attending to and engaging with the task rather than preparing for defense against a potential threat or stressor. Yet, there also was considerable variability in ANS responses. Adolescence has been characterized as a period of extensive neurobiological recalibration (Dahl & Gunnar, Reference Dahl and Gunnar2009) that may increase the likelihood of youth being susceptible to poorly regulated autonomic reactions to acute challenges. Consistent with this framing of developmental pathophysiology, the extent to which adolescents deviated from the average pattern of autonomic response to Cyberball exclusion, through either atypically subdued or exaggerated activity, appeared to reveal such contextually inappropriate stress responses that conferred risk for maladaptive cognitions and actions of suicidality (Miller & Prinstein, Reference Miller and Prinstein2019).
History of STB
Our first set of analyses examined whether participants with a history of STB differed in their physiological activity compared to their peers without prior STB. We found significantly lower SCR across baseline and task conditions in youth with histories of STB. A similar pattern of lower sympathetic activity has been reported in prior research with depressed and suicidal adults (Thorell, Reference Thorell2009; Thorell et al., Reference Thorell, Wolfersdorf, Straub, Steyer, Hodgkinson, Kaschka and Jandl2013), and with youths who predominantly reported suicidal ideation without self-harm behavior (Bellato et al., Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023), as was the case for the primary analyses of our sample. Thus, there is consistent evidence that low EDA is a biomarker of concurrent or past suicidal ideation in youth. Considering prior research and theory in developmental psychopathology, tonic and phasic sympathetic under-arousal may be associated with low behavioral inhibition (Beauchaine, Reference Beauchaine2001; El-Sheikh et al., Reference El-Sheikh, Kouros, Erath, Cummings, Keller and Staton2009), or diminished tendency to be vigilant and ability to increase attentiveness to acute cues of challenge or risk (McNaughton & Corr, Reference McNaughton and Corr2004), either of which act against youths’ abilities to curb impulsive behaviors with negative consequences. Impulsivity is well-established as a cognitive-behavioral process associated with youth suicidality (Cha et al., Reference Cha, Franz, Guzmán, Glenn, C., Kleiman and Nock2018; Kasen et al., Reference Kasen, Cohen and Chen2011). SNS hypoactivity also may reflect lower sensitivity to threat and increased drive to engage in risky or disruptive behavior to extinguish unpleasant feelings associated with low sympathetic arousal (Cappadocia et al., Reference Cappadocia, Desrocher, Pepler and Schroeder2009). Thus, weaker inhibitory stress-signaling implied by lower SCR across baseline and task conditions may have contributed to greater likelihood to engage in STB. Alternatively, it is possible that reduced sympathetic activity was not evident earlier in adolescence, when the STB were reported. Rather, sympathetic hypoactivity may have been akin to a physiological “scar” resulting from those aversive formative experiences (Yang et al., Reference Yang, Daches, George, Kiss, Kapornai, Baji and Kovacs2019). This alternative interpretation may be more compatible with the quite different association of SCR to exclusion with future STB, as discussed below, which calls into question whether SNS hypoactivity is a biomarker that precedes and predicts youth suicidality.
In contrast to previous research (Bellato et al., Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023), we did not observe significant associations of basal or social exclusion RSA with history of STB in our sample of Mexican-origin youths. The lack of association of parasympathetic responses to Cyberball with prior STB was maintained in the sensitivity analyses (Supplemental Table 3) examining RSA over the longer, contiguous latter half of the Cyberball task (Kaufman et al., Reference Kaufman, Crowell, Coleman, Puzia, Gray and Strayer2018), indicating that the non-significant findings were not an aberration resulting from our use of the six relatively brief and non-contiguous exclusion trials. There are several possible, albeit speculative, reasons for our surprising failure to replicate associations of parasympathetic activity with past STB.
First, considering both basal and task RSA, the temporal design of the study may have impacted the findings. Most prior studies of adolescent STB and RSA have recruited samples with currently or recently active suicidality (i.e., Crowell et al., Reference Crowell, Beauchaine, Hsiao, Vasilev, Yaptangco, Linehan and McCauley2012; Giletta et al., Reference Giletta, Hastings, Rudolph, Bauer, Nock and Prinstein2017; James et al., Reference James, Woody, Feurer, Kudinova and Gibb2017; Yang et al., Reference Yang, Daches, George, Kiss, Kapornai, Baji and Kovacs2019). In our study, adolescents were included in the “history of STB” group if they had endorsed STB at least once in the previous seven years. It is possible that lower basal and task RSA are associated with more proximal STB endorsement, but not with distally past tendencies that may have not been maintained.
Second, our choice of stressor task may not have been ideal. As with applications of psychophysiology to other topics of developmental inquiry (e.g., Obradović et al., Reference Obradović, Bush and Boyce2011), past studies of adolescent suicidality have varied greatly in their use of social, emotional and cognitive challenge tasks to evoke parasympathetic responses. Task demands affect the patterns of autonomic response that would be considered appropriate or healthy (Hastings & Kahle, Reference Hastings, Kahle, LoBue, Pérez-Edgar and Buss2019), such that one may not expect highly consistent associations between STB and parasympathetic reactivity across studies with different tasks. Compared to other procedures, it is possible that the Cyberball social exclusion task was not a congruous or appropriate stressor for identifying a reliable association of task-responsive parasympathetic activity with adolescents’ histories of STB. Supporting this interpretation is the fact that two prior studies that utilized Cyberball reported significant but opposite associations of suicidality with task RSA (i.e., less versus more parasympathetic activation) (Chesin et al., Reference Chesin, Cascardi, Tsang and Smith2020; Kaufman et al., Reference Kaufman, Crowell, Coleman, Puzia, Gray and Strayer2018). Such inconsistent findings call the efficacy of Cyberball for identifying the parasympathetic pathophysiology of concurrent and past suicidality into question.
Third, as noted previously, this is the first study to examine links between parasympathetic activity and suicidality in a 100% Latino sample, and very few studies of other aspects of psychopathology in Latino children and youth have involved parasympathetic measures. Most of these have examined RSA in infancy or toddlerhood and reported either non-significant associations with adjustment in early childhood (Somers et al., Reference Somers, Luecken, Spinrad and Crnic2019), or associations with externalizing but not internalizing problems (Somers, Reference Somers2025; Waters et al., Reference Waters, Boyce, Eskenazi and Alkon2015). In one prior analysis of the current sample, basal RSA at 17 years was not associated with concurrent depressive symptoms, although higher RSA predicted less depression 2 years later in boys only (Risbud et al., Reference Risbud, Guyer, Robins and Hastings2024). These findings stand in contrast to studies with other communities that suggest PNS measures are robustly associated with psychopathology (Beauchaine, Reference Beauchaine2015; Beauchaine & Thayer, Reference Beauchaine and Thayer2015). Given the limited literature extant, it would be premature to conclude that associations of parasympathetic regulation with current and past internalizing psychopathology are less robust in Mexican-origin and other Latino youth than other populations that have been studied. Rather, we reiterate calls for more pathophysiology research with diverse communities in order to avoid assumptions of biological universalism and instead to ascertain empirically where and why such commonalities do versus do not exist (Hastings et al., Reference Hastings, Guyer and Parra2022b).
Prospective STB
Participants who displayed lower basal sympathetic activity were more likely to endorse suicidality 5 to 31 months later, although this finding from the ANCOVA was not retained in the SEM analysis. Thus, low basal SCR not only distinguished between youths with current or past suicidality but also, perhaps to a lesser extent, predicted prospective STB. This suggests that tonic SNS hypoactivity may be a biomarker for future STB risk within the adolescent period, an association previously shown in studies of adults (Sarchiapone et al., Reference Sarchiapone, Gramaglia, Iosue, Carli, Mandelli, Serretti and Zeppegno2018; Thorell, Reference Thorell2009). Conversely, as was the case for prior STB, lower basal parasympathetic activity did not predict future STB. Prior research with adolescents has examined associations of basal RSA with youths’ current or past STB, but has not tested for prospective links (Bellato et al., Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023). Additional studies will be needed to determine whether tonic RSA is indicative of future risk for STB in other samples.
It was the measures of autonomic activity during the Cyberball exclusion trials that proved to be most strongly predictive of suicidal thoughts and actions occurring over the subsequent 2.5 years. Compared to youths who did not report future STB, those who did evinced elevated SCR and RSA during the task. When examined as reactivity relative to baseline, future STB was predicted by stronger than average SNS reactivity and weaker than average PNS reactivity, or uncoupled sympathetic activation (Berntson et al., Reference Berntson, Cacioppo and Quigley1993, Reference Berntson, Norman, Hawkley and Cacioppo2008). Sympathetic reactivity is a hallmark of stressful arousal, whereas parasympathetic withdrawal to many challenge tasks has been interpreted as indicative of better emotion regulation (Hastings & Kahle, Reference Hastings, Kahle, LoBue, Pérez-Edgar and Buss2019; Porges, Reference Porges2007). Hence, future STB was predicted by Mexican-origin youth physiologically responding to Cyberball exclusion as if it was a threat, rather than as an engaging activity. Mexican-origin youths are more likely to endure negative experiences related to social exclusion, such as ethnic discrimination or acculturative conflict, compared to their non-Latino peers (Hovey & King, Reference Hovey and King1996; Perez et al., Reference Pérez, Fortuna and Alegria2008). Possibly, youths who physiologically reacted to a computer game as threatening had experienced such ethnic stressors more often, or were otherwise primed to perceive them. Some prior studies also have shown that youths with current or recent STB have greater sympathetic reactivity (Nock & Mendes, Reference Nock and Mendes2008) and reduced parasympathetic reactivity (James et al., Reference James, Woody, Feurer, Kudinova and Gibb2017). Indeed, Yang and colleagues (Reference Yang, Daches, George, Kiss, Kapornai, Baji and Kovacs2019) found that this pattern of dual-branch autonomic reactivity distinguished depressed youths with histories of STB from depressed youths without STB and youths without psychopathology. Our findings suggest that weak PNS responses paired with strong SNS responses also may be a multisystem biomarker for prospective STB risk in late adolescence.
Physiological correlates of suicidal thoughts or behaviors?
The identified associations between autonomic physiology and Mexican-origin youths’ prior and future STB may have been most characteristic of youths with suicidal ideation that did not progress to attempting suicide; indeed, all findings were retained in analyses excluding the 25 youths who reported attempts. Intriguingly, the pathophysiology of suicidal ideation that we documented both overlapped with, and diverged from, the findings of the meta-analysis by Bellato and colleagues (Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023), which linked adolescent suicidal ideation with sympathetic hypoactivity. We showed that reduced SNS activity similarly characterized Mexican-origin youths with past ideation, but greater SNS reactivity distinguished those who reported ideation in future. Further, evincing greater SNS reactivity to Cyberball exclusion also characterized the 25 youths who ever reported a suicide attempt, paralleling the association of greater SNS with self-harm actions reported by both Bellato and colleagues (Reference Bellato, Admani, Deak, Farhat, Fontana Antunes de Oliveira, Vasconcelos, Malanchini, Shephard and Michelini2023) and Wetherall and colleagues (Reference Wetherall, Cleare, Belkadi, Etherson, Loney, Mathew, Munro, Townsend, Nock, Ferguson and O’Connor2025). Thus, despite the considerable evidence that tonic SNS hypoactivity may be a biomarker of suicidality across ages, it is possible that greater sympathetic reactivity may be a biomarker of risk for both suicide attempts and future suicidal ideation. Future work will be needed to substantiate this possibility, as it would inform targeted identification and prevention efforts with Latino youth, who are at higher risk of attempting suicide than are White youth (Ivey-Stephenson et al., Reference Ivey-Stephenson, Demissie, Crosby, Stone, Gaylor, Wilkins and Brown2020).
Limitations
Although this study had many strengths, there are some important limitations. First, our primary analyses of youths’ RSA utilized their physiology within the six relatively brief and non-contiguous episodes of Cyberball social exclusion. Computation of RSA may produce less reliable estimates during brief trials if these periods do not include a sufficient number of respiratory cycles (Zisner & Beauchaine, Reference Zisner, Beauchaine and Cicchetti2016). Further, our examination of only exclusion trials was distinct from most prior examinations of parasympathetic regulation during Cyberball, which have used longer periods of Cyberball including exclusion, inclusion, and inter-trial intervals (e.g., Kulakova et al., Reference Kulakova, Graumann, Cho, Deuter, Wolf, Roepke, Otte and Wingenfeld2024; Lambe et al., Reference Lambe, Craig and Hollenstein2019; Seah & Friedman, Reference Seah and Friedman2024). Therefore, we also examined RSA over the longer and contiguous latter half of Cyberball, paralleling Kaufman et al. (Reference Kaufman, Crowell, Coleman, Puzia, Gray and Strayer2018). The primary findings were sustained; RSA during the latter half of Cyberball was not associated with history of STB, but higher RSA during this extended period predicted future STB. Given that parasympathetic responses could be expected to vary across periods of inclusion, exclusion, and inactivity between trials (Hastings & Kahle, Reference Hastings, Kahle, LoBue, Pérez-Edgar and Buss2019), studies using extended periods of Cyberball could be characterized as examining RSA in a para-social game with varying demands on participants. Our examination of RSA specifically within non-consecutive exclusion trials may have offered an advantage for interpretability. However, further empirical testing would be needed to confirm this point, and we recommend that future studies configure Cyberball to have inclusion and exclusion rounds of 30s or longer to facilitate more robust measures of heart rate variability.
Second, there were low reliability statistics for several of the measures of STB. This may have been an artifact of the low rates of endorsement of items assessing suicide attempts, and hence the very different variances of items assessing ideation versus attempt (Mehta et al., Reference Mehta, Bastero-Caballero, Sun, Zhu, Murphy, Hardas and Koch2018; Metsämuuronen, Reference Metsämuuronen2023). Psychometric analyses using CFA confirmed that, from age 12 years onwards, all items loaded on a single factor, and these STB measures had configural invariance. Nonetheless, it will be important for future studies to replicate the current findings with more robust measures of suicidality, such as clinical interviews. Third, the adolescents who participated in this study were exclusively Mexican-origin and one cannot generalize these findings to adolescents of other Latino backgrounds, given the heterogeneity of different cultures and practices within the broader US Latino communities (Roth et al., Reference Roth, Musci and Eaton2019). Fourth, when measuring both prior and prospective STB, our analysis allowed for endorsements that were both years in the past and years in the future, respectively. Forthcoming work should identify more proximal risk factors associated with imminent STB, as most adolescent research has focused on distal predictors which are often transdiagnostic rather than specific to suicidality (Cha et al., Reference Cha, Franz, Guzmán, Glenn, C., Kleiman and Nock2018; Miller & Prinstein, Reference Miller and Prinstein2019).
Conclusion
In conclusion, adolescence represents a developmental period of heightened risk for interpersonal stress (McLaughlin & Nolen-Hoeksema, Reference McLaughlin and Nolen-Hoeksema2012; Parker et al., Reference Parker, Rubin, Price, DeRosier, Cicchetti and Cohen1995), physiological dysregulation (Crowell et al., Reference Crowell, Baucom, Yaptangco, Bride, Hsiao, McCauley and Beauchaine2014), and suicidality (Miller & Prinstein, Reference Miller and Prinstein2019). There is limited research studying possible biomarkers for increased suicide risk in youth, and scant work examining the links between psychophysiology and STB in Latino youth. The current study demonstrated that Mexican-origin adolescents with tonically low levels of sympathetic activity and who responded to an acute social exclusion task as if it was a threatening stressor were most vulnerable for STB. Future research should continue to investigate the interplay between sympathetic and parasympathetic acute stress responses, rather than examining each branch in isolation. Failing to account for activity across the complete autonomic stress system offers only partial answers in the search for reliable biomarkers of youth suicidality.
Despite growing concern for adolescent suicidality, researchers’ ability to predict STB, including suicide deaths, remains remarkably inadequate (Franklin et al., Reference Franklin, Ribeiro, Fox, Bentley, Kleiman, Huang, Musacchio, Jaroszewski, Chang and Nock2017). Understanding and identifying the autonomic correlates of youth suicidality provides generative avenues for objective and early identification of developing STB. As measurement of ANS physiology is non-invasive, can be obtained during brief periods like clinic visits, and increasingly is being incorporated into widely used wearable technologies (Hang et al., Reference Hang, Hastings, Hostinar, LoBue, Perez-Edgar and Bussin press), indices like SCR and RSA may be viable targets for identification of at-risk youth. With the effectiveness of biofeedback techniques for changing physiological regulation and reactivity, interventions with suicidal youth also may be able to focus on these autonomic biomarkers to reduce future risk. Youth suicidality is complex, implicating factors across social, cultural, and neurobiological contexts (Miller & Prinstein, Reference Miller and Prinstein2019), and utilizing physiological indices of risk may advance the efforts toward prevention and early intervention.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579426101680.
Acknowledgments
The authors wish to thank the participating families, and the University of California students and staff who contributed to data collection.
Funding statement
This research was supported by National Institutes of Health (Grant Nos. R01MH098370, Drs. Amanda Guyer and Paul Hastings, and R01DA017902, Dr. Richard Robins).
Competing interests
There are no conflicts of interest to report. The research reported in this manuscript was included in a chapter of the first author’s dissertation, which is available at this location: https://escholarship.org/content/qt4hk373cf/qt4hk373cf.pdf?t=rljiec
Preregistration statement
This study was completed as part of a doctoral dissertation that was approved by a faculty committee but not formally preregistered.
Data availability statement
We are not legally or ethically allowed to publicly post data for this project because the participants in the study have not given informed consent to have their personal data publicly shared, and we do not have IRB approval to post data publicly.
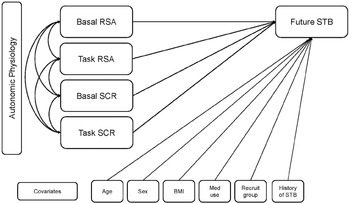
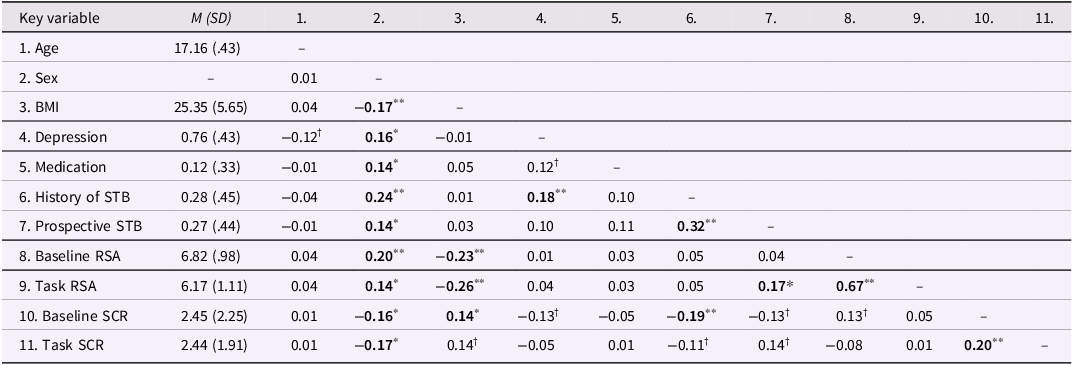
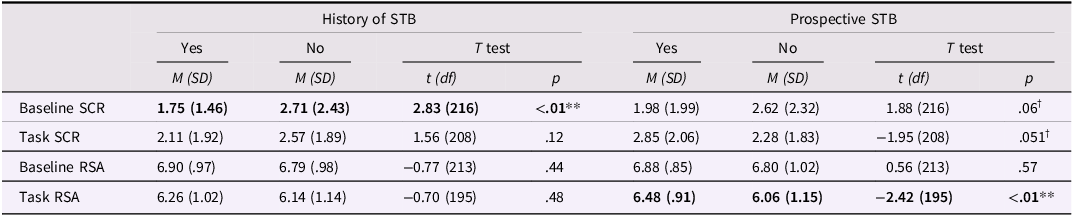
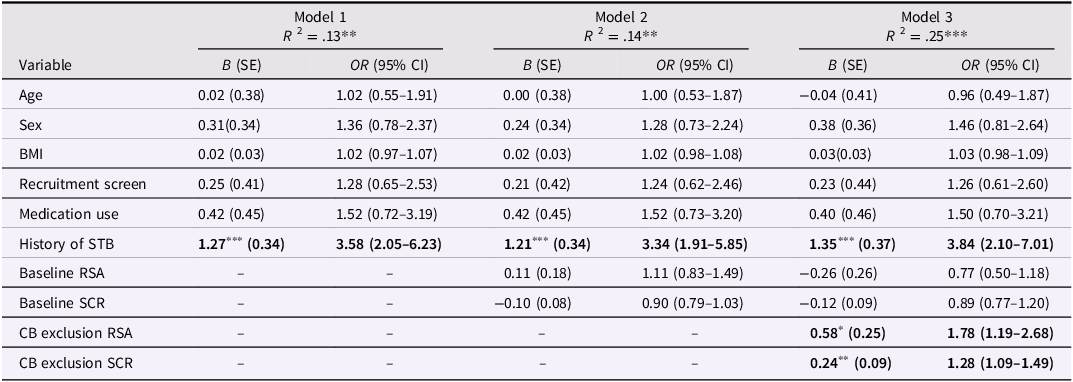



 Open access
Open access