


1. Introduction
Language comprehension develops during infancy and childhood, requiring the child to understand the sentences’ meaning and recognize inconsistencies in the discourse (Skeide & Friederici, Reference Skeide and Friederici2016). Previous studies report that auditory comprehension (AC) is an integrative process that involves the processing of linguistic and non-linguistic information, a claim supported by the ventral stream of the language network (Parker et al., Reference Parker, Luzzi, Alexander, Wheeler-Kingshott, Ciccarelli and Lambon Ralph2005; Saur et al., Reference Saur, Kreher, Schnell, Kümmerer, Kellmeyer, Vry, Umarova, Musso, Glauche, Abel, Huber, Rijntjes, Hennig and Weiller2008). AC also entails the consolidation of at least two processes: 1) language perception, which implies distinguishing between perceptual inputs such as words in all modalities and nonverbal stimuli (Federmeier et al., Reference Federmeier, Kutas and Dickson2016), and 2) word-meaning processing, which includes the detection of the match between an incoming word and representations stored in their mental lexicon (Coltheart et al., Reference Coltheart, Rastle, Perry, Langdon and Ziegler2001; Federmeier, Reference Federmeier2022). Thus, AC development requires the gradual acquisition of these abilities.
During the first year of life, infants’ language-perception abilities become tuned to the sounds of their native language, and they begin to establish their first lexical-semantic representations. (Friedrich & Friederici, Reference Friedrich and Friederici2005c). At 14 months old, infants exhibit efficient lexical priming (Friedrich & Friederici, Reference Friedrich and Friederici2005a). Around 18 months old, they undergo a burst of vocabulary, during which they learn multiple new words and combine them. (Golinkoff & Hirsh-Pasek, Reference Golinkoff, Hirsh-Pasek, Fletcher and Mac-Whinney1995; Silva-Pereyra et al., Reference Silva-Pereyra, Rivera-Gaxiola and Kuhl2005). Between 19 and 24 months, children develop the ability to integrate the meaning of words into a sentential context (Friedrich & Friederici, Reference Friedrich and Friederici2005c, Reference Friedrich and Friederici2005b). Around 30 months old, children can identify inconsistencies in the sentence’s meaning (Silva-Pereyra et al., Reference Silva-Pereyra, Rivera-Gaxiola and Kuhl2005), until they exhibit specialization and integration in brain structures at 6 or 7 years of age (Etchell et al., Reference Etchell, Adhikari, Weinberg, Leen Choo, Garnett, Ming Chow and Chang2016; Wang et al., Reference Wang, Wagley, Rice and Booth2021; Weiss-Croft & Baldeweg, Reference Weiss-Croft and Baldeweg2015) with language lateralization established by 5 years of age (Weiss-Croft & Baldeweg, Reference Weiss-Croft and Baldeweg2015). However, not all children acquire language comprehension skills due to multiple factors, including risk factors for atypical brain structure at birth.
1.1. Language development and risk factors for atypical brain structure
Infants who are born with pre- and perinatal risk factors for atypical brain structure usually exhibit lower gray matter and brain volumes (Foster-Cohen et al., Reference Foster-Cohen, Friesen, Champion and Woodward2010; Huang et al., Reference Huang, Zhu, Qu and Mu2016; Iwata et al., Reference Iwata, Bainbridge, Nakamura, Tamura, Takashima, Matsuishi and Iwata2010; Woodward et al., Reference Woodward, Anderson, Austin, Howard and Inder2006). For example, maternal diseases during pregnancy, such as thyroid dysfunction, epilepsy, asthma, preeclampsia, hypertension, maternal infections, or diabetes, are associated with reduced gray matter and cortical volume (Harmony, Reference Harmony2021; Huang et al., Reference Huang, Zhu, Qu and Mu2016; Mwaniki et al., Reference Mwaniki, Atieno, Lawn and Newton2012; Ye et al., Reference Ye, Luo, Huang, Li, Liu and Liu2022), while early or late maternal age has been linked to smaller infant brain volume (Doyle et al., Reference Doyle, Cheong, Burnett, Roberts, Lee and Anderson2015; Hackman & Farah, Reference Hackman and Farah2009; Howard et al., Reference Howard, Roberts, Lim, Lee, Barre, Treyvaud, Cheong, Hunt, Inder, Doyle and Anderson2011; Reidy et al., Reference Reidy, Morgan, Thompson, Inder, Doyle and Anderson2013; Richmond et al., Reference Richmond, Johnson, Seal, Allen and Whittle2016; Thompson et al., Reference Thompson, Kelly, Chen, Beare, Alexander, Seal, Lee, Matthews, Anderson, Doyle, Spittle and Cheong2019). Multiple studies have also reported that preterm infants display more acute maturational brain disturbances (Aarnoudse-Moens et al., Reference Aarnoudse-Moens, Weisglas-Kuperus, Van Goudoever and Oosterlaan2009; Feldman et al., Reference Feldman, Lee, Yeatman and Yeom2012; Harmony, Reference Harmony2021; Mwaniki et al., Reference Mwaniki, Atieno, Lawn and Newton2012; Reidy et al., Reference Reidy, Morgan, Thompson, Inder, Doyle and Anderson2013) characterized by decreased interhemispheric connections associated with the language system (Scheinost et al., Reference Scheinost, Chang, Lacadie, Brennan-Wydra, Constable, Chawarska and Ment2022), and abnormal extra-callosal connectivity between bilateral temporal regions, which have been positively correlated with language assessments during childhood (Barnes-Davis et al., Reference Barnes-Davis, Williamson, Merhar, Holland and Kadis2020). However, no studies have linked the neuropathological pattern observed on magnetic resonance imaging (MRI) with AC.
Prior studies have identified two main stressors of atypical brain development with long-term effects on cognition: the first is associated with maternal conditions during pregnancy, and the second is associated with the perinatal risk factors for atypical brain structure in infants (Mwaniki et al., Reference Mwaniki, Atieno, Lawn and Newton2012; Nilsen et al., Reference Nilsen, Ruiz and Tulve2020). For the first type of stressor, social factors, such as low parental socioeconomic status, have been associated with delayed cognitive development (Li et al., Reference Li, Yang, Li, Xie and Fang2022). However, no studies have examined the effects of this type of stressor on language development.
Conversely, perinatal risk factors for atypical brain structure in infants have been identified as crucial stressors for language development. For example, it has been reported that 40% of premature infants will display mild to moderate cognitive impairment, of which 48% born at less than 30 weeks’ gestational age will exhibit language impairments (Charkaluk et al., Reference Charkaluk, Rousseau, Benhammou, Datin-Dorrière, Flamant, Gire, Kern, Pierrat, Kaminski and Marret2019; C. E. Rogers et al., Reference Rogers, Lean, Wheelock and Smyser2018; E. E. Rogers & Hintz, Reference Rogers and Hintz2016), of which 26.7% may progress to delayed development of verbal expression, limited lexicon and grammatical complexity (Charkaluk et al., Reference Charkaluk, Rousseau, Benhammou, Datin-Dorrière, Flamant, Gire, Kern, Pierrat, Kaminski and Marret2019; Isotani et al., Reference Isotani, Azevedo, Chiari and Perissinoto2009). Even more alarming is that between 7 and 12 years of age, around 24% of children born preterm may display abnormal scores in basic language skills compared to their term peers (Luu et al., Reference Luu, Ment, Schneider, Katz, Allan and Vohr2009). Previous studies also suggest that prenatal and perinatal risk factors for atypical brain structure such as maternal conditions and infant risk factors for atypical brain structure may have a long-term effect, which may manifest when the child is required to exert more cognitive effort; for instance, a delay in language development by 24 months may only become apparent when the ability to integrate word meaning into a sentential context is required (Friedrich & Friederici, Reference Friedrich and Friederici2005a, Reference Friedrich and Friederici2005c) or when structural specialization and integration in the brain are needed at 6 or 7 years of age (Etchell et al., Reference Etchell, Adhikari, Weinberg, Leen Choo, Garnett, Ming Chow and Chang2016; Wang et al., Reference Wang, Wagley, Rice and Booth2021; Weiss-Croft & Baldeweg, Reference Weiss-Croft and Baldeweg2015).
1.2. Associating motor milestones with language development
Previous studies have shown that infants born with risk factors for atypical brain structure exhibit sequelae in motor development. For example, it is estimated that 31% of premature infants will develop some form of sequelae, of which 60% experience cognitive developmental delay, and 10% show signs of motor and coordination impairments (Mwaniki et al., Reference Mwaniki, Atieno, Lawn and Newton2012).
In this regard, recent studies suggest a link between early motor skills and later language development, a claim supported by the embodied cognition approach, which posits that infants develop language skills through ongoing interaction with their environment. As infants manipulate their environment, they learn to interact by using their body characteristics and the properties of objects, thereby increasing their understanding of the world (Gibson, Reference Gibson1988). Most studies have found that gross motor milestones are associated with later general cognitive development (Oudgenoeg-Paz et al., Reference Oudgenoeg-Paz, Mulder, Jongmans, van der Ham and Van der Stigchel2017). For instance, a study reported that higher postural control in infants born at term was associated with higher cognitive scores in the BSID (Wijnroks & Veldhoven, Reference Wijnroks and Veldhoven2003), while other studies also reported that general movements (GM), defined as whole-body movements involving the arms, legs, neck and trunk, are positively associated with later cognitive development (Bruggink et al., Reference Bruggink, Van Braeckel and Bos2010; De Bock et al., Reference De Bock, Will, Behrenbeck, Jarczok, Hadders-Algra and Philippi2017; Kodric et al., Reference Kodric, Sustersic and Paro-Panjan2010; Lundqvist-Persson et al., Reference Lundqvist-Persson, Lau, Nordin, Bona and Sabel2012). However, no studies have reported an association between gross motor skills and language development.
On the other hand, the link between fine motor skills and later cognitive development has been frequently associated with clinical diagnoses of autism or attention deficit hyperactivity disorder (ADHD), identifying a delay in fine motor skills that characterizes these pathologies. (Bowler et al., Reference Bowler, Arichi, Austerberry, Fearon and Ronald2024; Landa & Garrett-Mayer, Reference Landa and Garrett-Mayer2006; LeBarton & Landa, Reference LeBarton and Landa2019). However, only one study reported that fine and gross motor scores seem to predict vocabulary comprehension at 30 months (Andalò et al., Reference Andalò, Rigo, Rossi, Majorano and Lavelli2022), highlighting the importance of assessing the association between motor milestones and language development to inform multidisciplinary interventions for this at-risk population.
1.3. Psychometric tests as predictors of language development
Although multiple studies report long-term effects on cognition in infants born with risk factors for atypical brain structure, few have examined the psychometric tests that predict language development trajectories in this population. For example, a prior study reported that BSID has predictive validity for the mental and psychomotor developmental scales from 6 to 36 months (Lung et al., Reference Lung, Shu, Chiang, Chen and Lin2009), while in another research, the authors found that risk factors for atypical brain structure, such as neonatal sepsis and lower gestational age, predicted a decline in BSID-3 scores from 12 to 20 months (Greene et al., Reference Greene, Patra, Silvestri and Nelson2013). It is essential to develop a psychometric test to predict language development in infants with pre- and perinatal risk factors for atypical brain structure, thereby enabling earlier identification of atypical language development.
Moreover, AC is a language feature that is difficult to assess before 36 months of age. Nevertheless, few studies have examined AC in this population, even though identifying predictors of language development delay and implementing earlier interventions are necessary. Thus, this study had three primary aims: The first was to describe the early language development trajectories; the second was to determine the main predictors of AC development in this population; and the third, equally important, was to identify a predictive psychometric test for assessing behavioral performance in AC of 3-year-old children with prenatal and perinatal risk factors for atypical brain structure. In this exploratory study, we expected a delay in language development at 24 months of age due to increased environmental demands. Additionally, we expected that risk factors and MRI neuropathological patterns would be negatively associated with AC scores. In contrast, greater interaction with the environment (i.e., reaching fine and gross motor milestones earlier) might benefit AC development. Finally, given that prior studies suggest that BSID has predictive properties, we also expected earlier assessments with this test to predict the AC at 36 months of age.
2. Materials and methods
2.1. Participants
This longitudinal study selected 36-month-old children born with prenatal and perinatal risk factors for atypical brain structure, using MRI and conducting all evaluations from birth to 36 months of age. From an initial pool of 81 toddlers, a rigorous selection process was undertaken, resulting in the enrollment of 51 participants (28 females, 23 males). The exclusion of 30 participants was due to poor MRI quality. Participants also underwent clinical, anthropometric and motor assessments. Corrected age was used for all assessments. Individuals with incomplete evaluations, intraventricular hemorrhage, or abnormal baseline auditory function were excluded from this study. To ensure normal auditory function prior to inclusion, all infants underwent standard audiological assessments, including otoacoustic emissions (OAEs; amplitudes ranging from −10 dB SPL to +30 dB SPL) and tympanometry, which assessed cochlear and middle-ear function. The study was conducted following the Ethical Principles for Medical Research Involving Human Subjects established by the Declaration of Helsinki in 1964 and subsequently amended, and the International Ethical Guidelines for Health-related Research Involving Humans (2016) issued by the Council for International Organizations of Medical Sciences (CIOMS) and the World Health Organization (WHO). Written informed consent was obtained from the parents or legal guardians of all participants after explaining the study procedures, potential risks and their right to withdraw at any time without penalty.
2.2. Clinical and neuropsychological assessment
In this study, we collected data on prenatal and perinatal risk factors for atypical brain structure; anthropometric data at birth and at 36 months (including weight, height and body mass index (BMI)); and demographic information from participants and their parents, including parents’ age and educational level. Participants also underwent neuropsychological assessments using the Preschool Language Scale (PLS-5) (Zimmerman et al., Reference Zimmerman, Steiner and Pond2011) at 12, 24 and 36 months. BSID-2 (Bayley, Reference Bayley1993) and the MacArthur–Bates Communicative Development Inventories (MB-CDIs) (Jackson-Maldonado, Reference Jackson-Maldonado and Chappele2003) were included in the assessments at 12, 24 and 30 months. The PLS-5 in Spanish assesses infants’ and young children’s receptive and expressive language skills. It consists of two subscales: AC and expressive communication (EC). The BSID-2 is a standard series of measurements used to assess the infant’s development between 1 and 42 months, and it consists of the MDI and psychomotor development index (PDI), while the MB-CDI is an inventory of communicative development used to explore toddlers’ comprehension and production of words between 8 and 30 months.
2.3. Motor assessment
All participants were assessed monthly between 2 and 24 months by a neuromotor rehabilitation expert with extensive clinical and academic training in the management of pediatric patients at risk of neurological injury. The evaluator’s qualifications ensured that they had the necessary expertise in both therapeutic practices and newborn development, particularly in infants with neurological concerns.
During the assessment, the evaluator observed whether each infant displayed the expected postures, movements and motor responses for their corrected age. This included their ability to achieve gross motor milestones, such as head control, sitting, crawling and gait. Each evaluation took place when the infant was non-sick, awake, well-fed and rested, to ensure they were in the best condition for accurate assessment.
The Psychomotor Development Assessment Form, developed in the Department of Neurohabilitation Therapy of the Neurodevelopment Unit of the Institute of Neurobiology at UNAM, was used as an assessment tool. This tool is based on neurodevelopmental assessment scales and methods (Gessel, Reference Gessel and Carmichael1954; Gessel & Amatruda, Reference Gessel and Amatruda1981; Katona & Berényi, Reference Katona and Berényi2001), and was divided into five subscales for the assessment of psychomotor development: gross motor, fine motor, cognitive, language and social perceptual. The results of these subscales are recorded monthly with a range of 0 to 4, indicating the following: 0 (Does not succeed); 1 (Tries but fails); 2 (In the process of development); 3 (Succeeds unskillfully); 4 (Normal). Once babies reached a score of 4 on both the gross and fine motor subscales, the corresponding age in months was considered the developmental milestone. To ensure the reliability of clinical assessments of gross and fine motor milestone records, intra- and inter-rater reliability were monitored through periodic training sessions to ensure that all raters adhered to the same guidelines and scoring criteria. Moreover, periodic checks were conducted to ensure that the scores remained consistent and accurate over time. All participants were treated using Katona Neurohabilitation to prevent neurological sequelae from birth to 6 months (Gonzalez-Moreira et al., Reference Gonzalez-Moreira, Harmony, Hinojosa-Rodríguez, Carrillo-Prado, Juárez-Colín, Gutiérrez-Hernández, Carlier, Cubero-Rego, Castro-Chavira and Fernández2023; Hinojosa-Rodríguez et al., Reference Hinojosa-Rodríguez, Jiménez, Colín, Moreira, Bautista and Harmony2020).
2.4. MRI acquisition
Children also underwent MRI scanning at 36 months old during natural sleep, following a protocol that included sleep deprivation and fasting to avoid sedation. Ear protection was provided. The MRI was performed on a Discovery MR750 3-Tesla system (GE Healthcare, WI, USA) using a 16-channel neurovascular head coil (HDNV). Anatomical images included coronal 3D T1-weighted SPGR, with repetition time (TR) = 6.072 ms, echo time (TE) = 2.428 ms, flip angle = 12°, 392 slices, slice thickness = 1 mm, spacing between slices = 0.5 mm, acquisition matrix = 256 × 256 (voxel size = 0.859 × 0.5 × 0.859 mm3); coronal 3D T2-weighted SE, with TR = 2500 ms, TE = 68.746 ms, flip angle = 90°, 196 slices, slice thickness = 1 mm, spacing between slices = 1 mm, acquisition matrix = 256 × 256, (voxel size = 0.859 × 1 × 0.859 mm3). MRI quality was controlled by an expert in magnetic resonance image acquisition, who performed volumetric segmentation during scanning to verify correct image acquisition. Images with movement or object artifacts were rejected, and those with magnetic field inhomogeneity after applying a resonator filter (GE Healthcare, WI, USA) using the software ‘Ready Wiew’ were also excluded from this study. After acquisition, the expert performed a double-anonymized visual inspection, and all neuropathological patterns were detected and registered according to the Krägeloh-Mann and Horber classification (Krägeloh-Mann & Horber, Reference Krägeloh-Mann and Horber2007). The MRI data also revealed that 50% of the participants showed structural alterations under this classification: 32.2% of them showed alterations in lateral ventricle (LV) and around 23.7% evidenced alterations in corpus callosum volumes and augmented subarachnoid space in frontal regions, which was consistent with a prior study in infants with atypical perinatal brain structure (Hinojosa-Rodríguez et al., Reference Hinojosa-Rodríguez, Jiménez, Colín, Moreira, Bautista and Harmony2020). Therefore, manual segmentation of the corpus callosum and LVs was performed from T1 and T2-weighted sequences. Volumes were estimated using the AW Volume Share 2 software from General Electric.
2.5. Data analysis methods
2.5.1. Descriptive data
We calculated frequencies, means and standard deviations for anthropometric, demographic, neuropsychological, motor and volumetric data for atypical brain volumes (the corpus callosum and the left and right LVs), as well as the prevalence of prenatal and perinatal risk factors for atypical brain structure.
2.5.2. Regression analysis
Predictors of language development. Regression analyses were performed to identify relationships between AC at 36 months and factors that might explain variance in language performance in our cohort. The linear regression model included the standard AC score (PLS-5) at 36 months as the dependent variable. Demographic information (sex, age, parents’ age and education level), anthropometric data (weight, height and BMI), risk factors for atypical brain structure, age in months of motor milestone achievement and volumes of the corpus callosum and the left and right LVs were included as independent variables. The linear regression analyses included multiple forward regressions to find a reduced model that best explained the data. A collinearity diagnostic for each regression model was performed using the following steps: correlation analysis, tolerance values, variance inflation factors and condition indices. Variables with values indicative of collinearity were excluded from the regression analyses.
Neuropsychological tests. Regression analyses were conducted separately to explore the best neuropsychological test predicting AC of the PLS-5 at 36 months. This included the standard AC score of the PLS-5 at 36 months as the dependent variable, and the neuropsychological assessments at 12, 24 or 30 months (i.e., PLS-5, BSID-2 and MB-CDIs) as independent variables. The linear regression analyses involved multiple forward regressions to find a reduced model that best explained the data. We removed factors with the highest p value until all factors were statistically significant. A p value <0.05 was considered statistically significant in all analyses.
3. Results
3.1. Descriptive results
Table 1 presents participants’ demographic, anthropometric and prenatal and perinatal risk factors for atypical brain structure. A total of 78.4% of participants were born preterm. Most patients presented with multiple risk factors, and there was a high prevalence of advanced resuscitation (See Table 1).
Demographic and anthropometric information, and distribution of prenatal and perinatal risk factors for atypical brain structure of the cohort
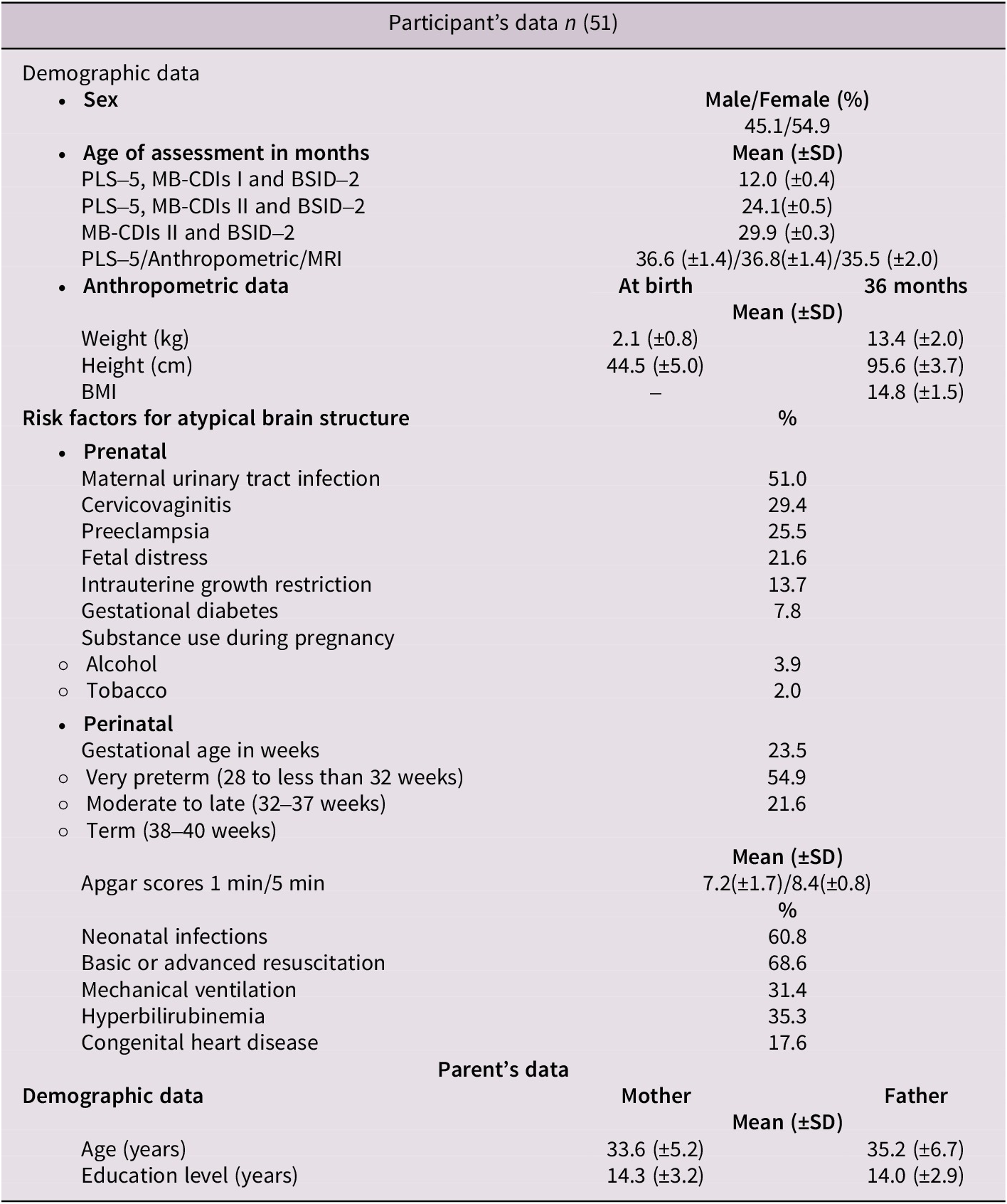
Note: SD = Standard Deviation, BMI = Body mass index.
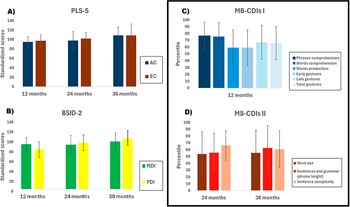
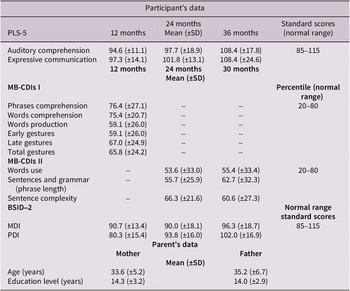
As can be seen in Figure 1 and Table 2 (as well as in Figure 1 in the Supplementary Material) all neuropsychological scores improved with age, except for the sentence complexity score, which declined slightly from 24 to 36 months of age (See Figure 1D, Table 2).
The bar graphs show the participants neuropsychological scores between 12 and 36 months of age. A) illustrates auditory comprehension (AC) and expressive communication (EC) scores of Preschool Language Scale (PLS-5) at 12, 24, and 36 months, B) shows the mental development (MDI) and psychomotor development indices (PDI) of Bayley Scales of Infant Development-2 (BSID-2) at 12, 24, and 30 months. In C) and D), the bar graphs represent all subtests of the MacArthur-Bates Communicative Development Inventories I and II (MB-CDIs I and II) at 12, 24, and 30 months.

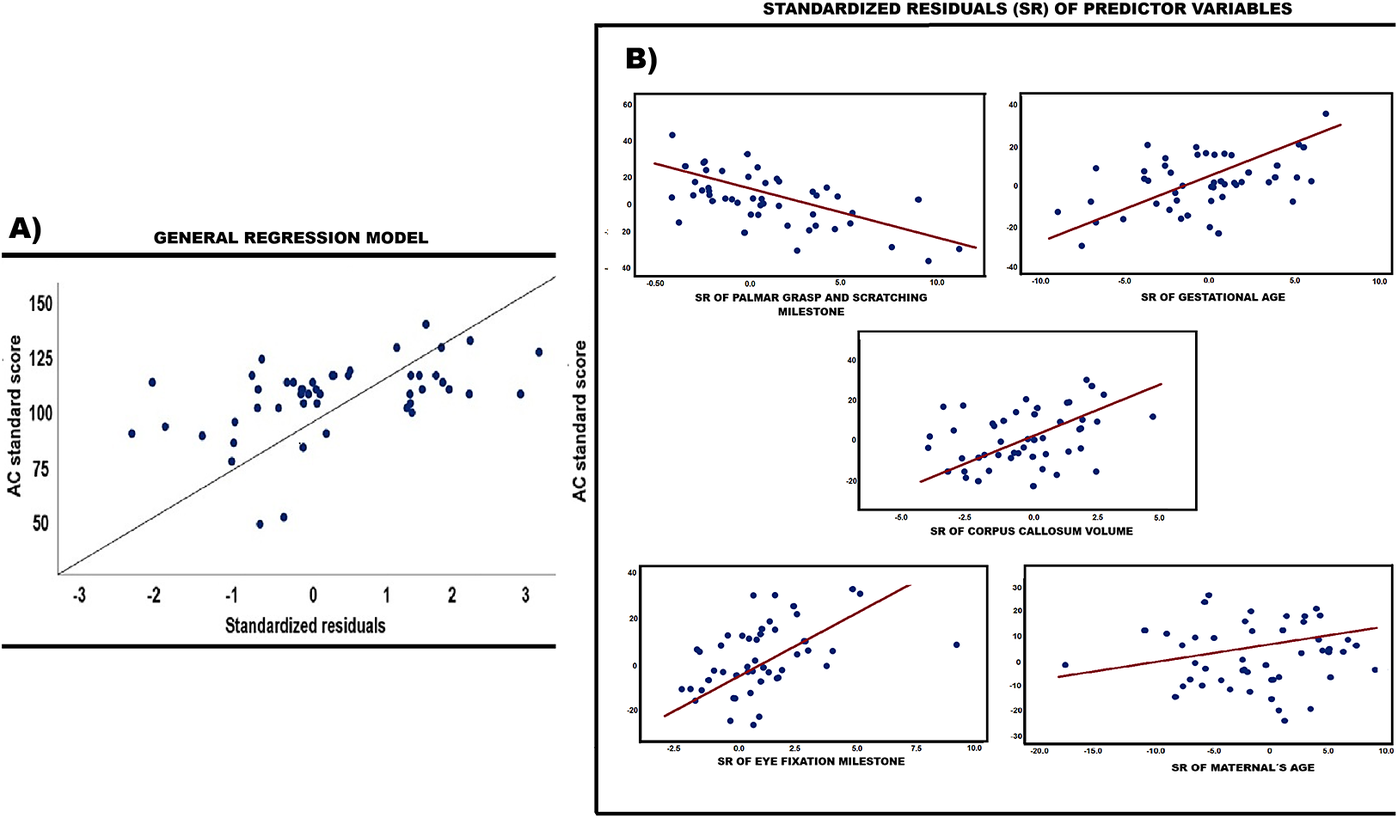
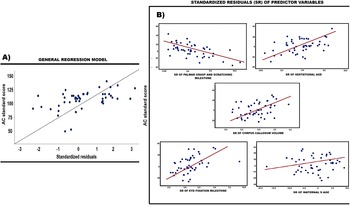
The scatter plots illustrate the relationship between the standardized score of auditory comprehension (AC) at 36 months and the standardized residuals (SR) of the regression model. A) shows the SR of the general regression model, whereas the scatter plots in B) illustrate the relationship between AC and the SR of predictor variables.
Neuropsychological data of our sample
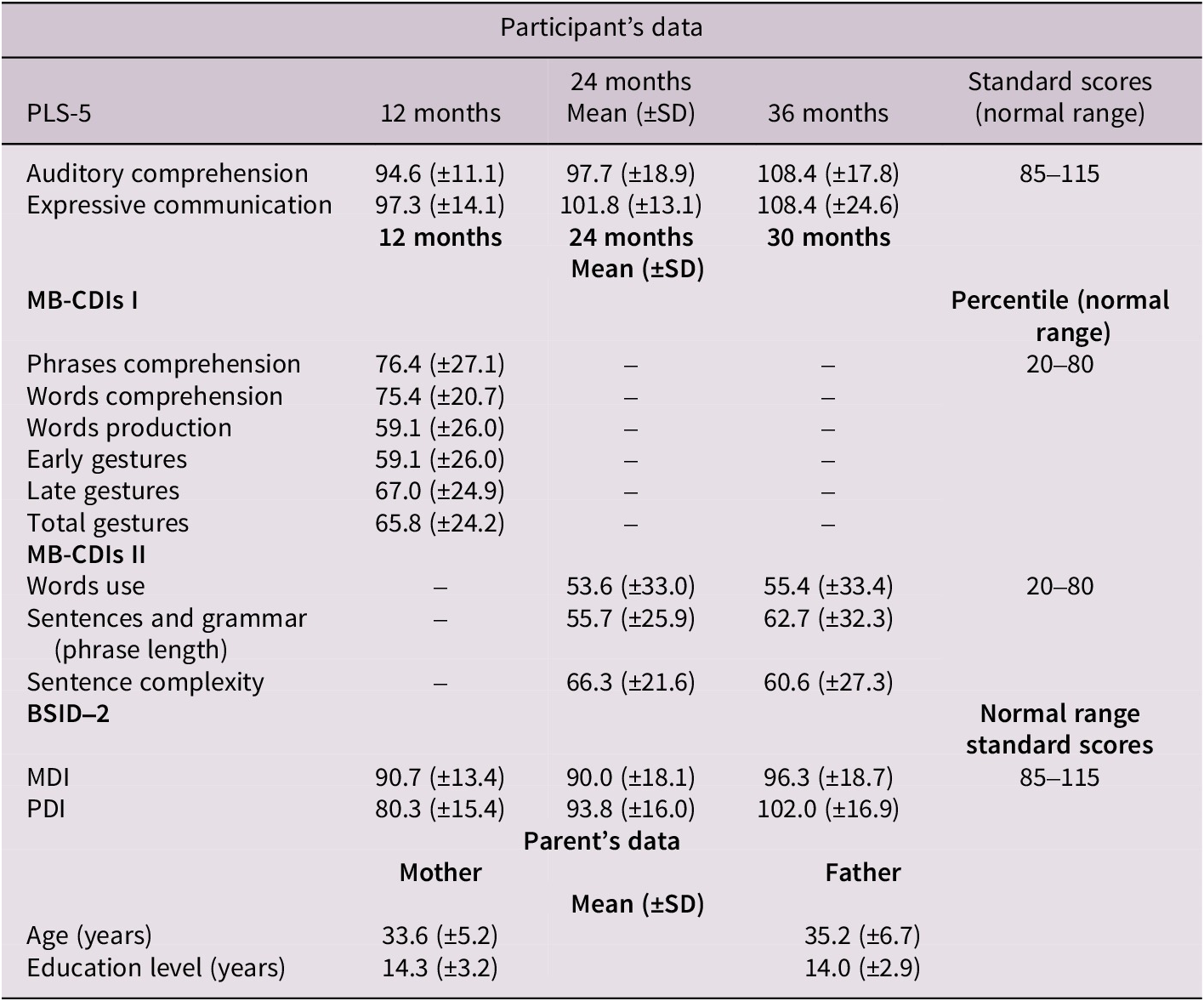
Note: SD = Standard Deviation, PLS-5 = Preschool Language Scale; MB-CDIs = MacArthur–Bates Communicative Development Inventories; BSID-2 = Bayley Scales of Infant Development-2; MDI, Mental Development Index; PDI, Psychomotor Development Index.
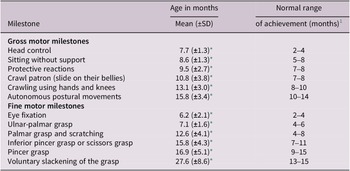
Table 3 presents the ages at which fine and gross motor milestones were achieved. Notably, the timing of achievement was later than that reported in typically developing populations (Bracewell & Marlow, Reference Bracewell and Marlow2002; Dalton, Reference Dalton2005; Katona, Reference Katona, Vietze and Vaughan1988; Knobloch, Reference Knobloch1961).
Participant’s age of achievement of gross and fine motor milestones
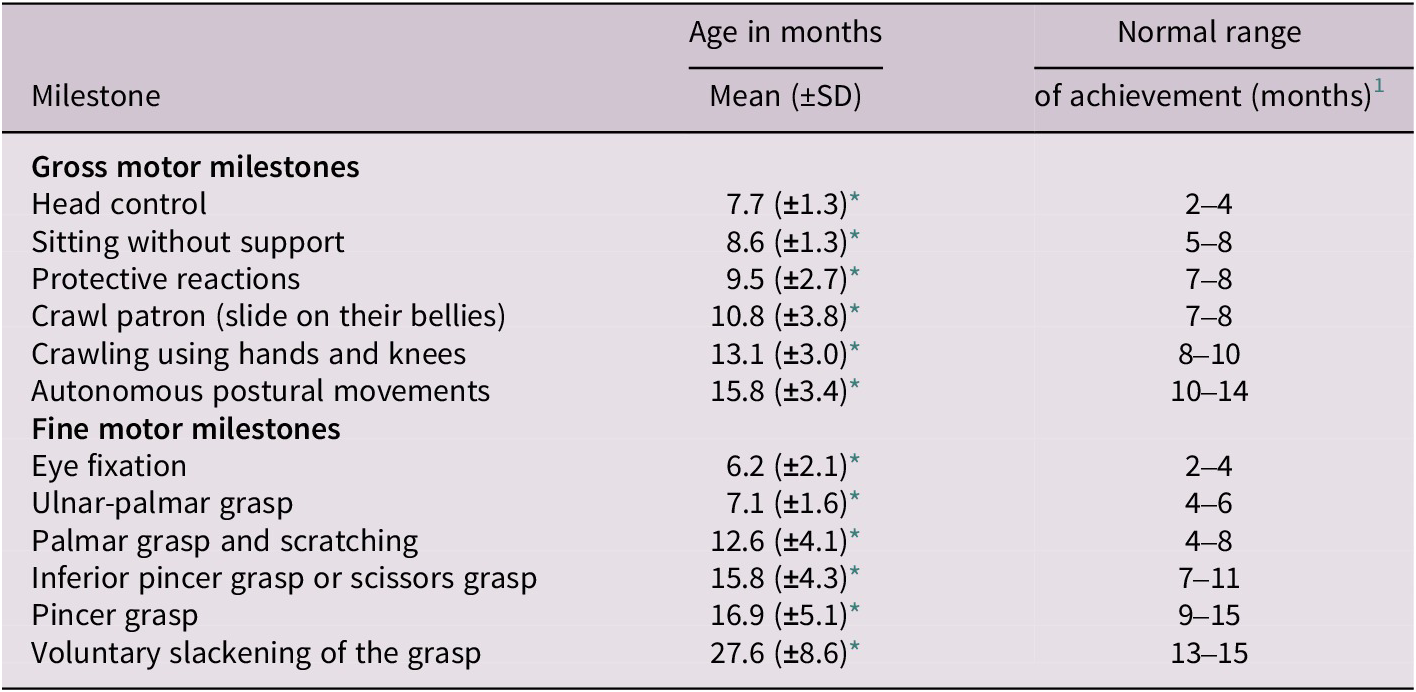
Note: SD = Standard Deviation;
* lower than normal range.
1 (Bracewell & Marlow, Reference Bracewell and Marlow2002; Dalton, Reference Dalton2005; Katona, Reference Katona, Vietze and Vaughan1988; Knobloch, Reference Knobloch1961).
The main MRI neuropathological patterns were abnormal lateral LV and corpus callosum volumes. The participants exhibited greater right than left LV volume, which aligns with previous studies reporting increased ventricular volumes in infants and children with a clinical diagnosis of neurodevelopmental impairment (Harmony, Reference Harmony2021; Lind et al., Reference Lind, Parkkola, Lehtonen, Munck, Maunu, Lapinleimu and Haataja2011) (See Table 4).
Participants’ MRI volumes at 36 months

Note: SD = Standard Deviation, MRI = magnetic resonance imaging, LV = lateral ventricles.
3.2. Predictors of language development results
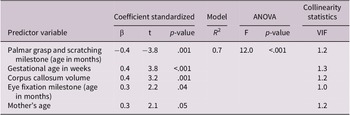
The regression analyses (sum of squares = 6533.9; root mean square = 1634.2; standardized residual (Kolmogorov–Smirnov test, p = 0.2; homoscedastic)) showed that gestational age in weeks and corpus callosum volume were positively associated with AC at 36 months, highlighting the importance of perinatal risk factors for atypical brain structure and neurological patterns in language development (Charkaluk et al., Reference Charkaluk, Rousseau, Benhammou, Datin-Dorrière, Flamant, Gire, Kern, Pierrat, Kaminski and Marret2019; C. E. Rogers et al., Reference Rogers, Lean, Wheelock and Smyser2018; E. E. Rogers & Hintz, Reference Rogers and Hintz2016), while the consolidation age of fine motor milestones was also linked to AC, as previous studies have reported (Andalò et al., Reference Andalò, Rigo, Rossi, Majorano and Lavelli2022; Yildiz et al., Reference Yildiz, Yildiz, Camli and Elbasan2025). An unexpected finding was that maternal age significantly predicted AC scores (see Table 5 and Figure 2A,B).
Predictor variables of AC at 36 months
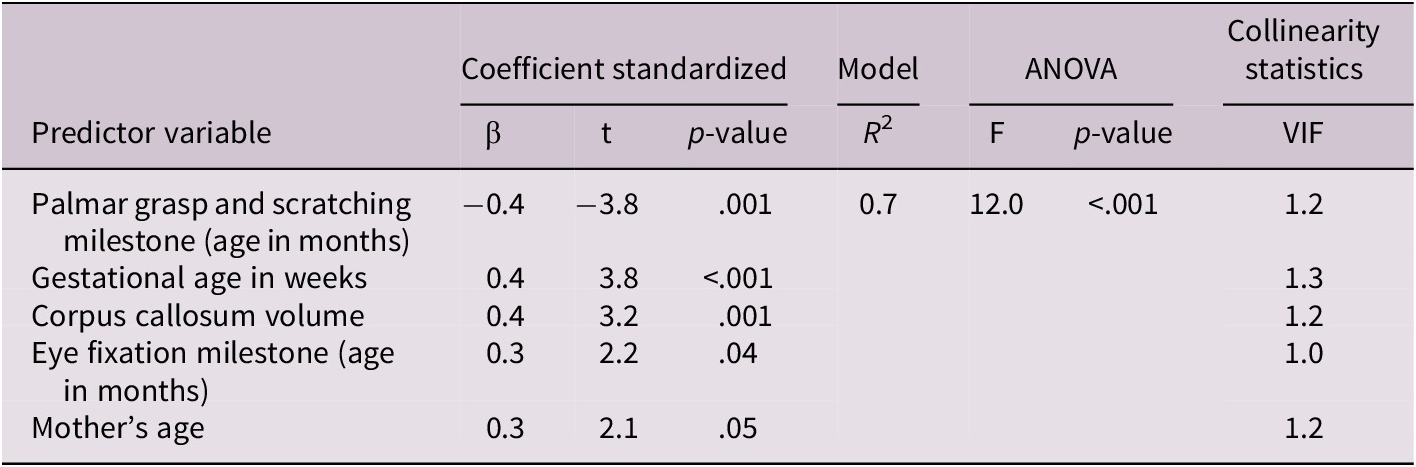
Note: AC = Auditory comprehension, VIF = Variance Inflation Factor.
3.3. Neuropsychological results
As shown in Table 6, the MDI of BSID-2 scores at 12 and 30 months predicted AC scores at 36 months.
Neuropsychological assessment predictors of AC at 36 months

Note: AC = Auditory comprehension, BSID-2 = Bayley Scales of Infant Development-2, MDI = Mental development index, PLS-5 = Preschool Language Scale, EC = Expressive communication, VIF = Variance Inflation Factor.
4. Discussion
The aim of this longitudinal study was threefold: first, to examine the early language development trajectories of infants born with pre- and perinatal risks for brain injury; second, to identify the primary factors predicting AC development in this population; and third, to determine a predictive psychometric test of behavioral performance for AC in children at 36 months of age. To achieve this, we employed a comprehensive set of demographic, clinical, neuropsychological, motor and neuroimaging data. In this exploratory study, with respect to the first aim, we expected to find a delay in language development at 24 months. For the second aim, we suggested that pre- and perinatal risk factors and MRI neuropathological patterns would be negatively associated with AC scores, whereas greater interaction with the environment (i.e., reaching fine and gross motor milestones earlier) might benefit AC development. For the third aim, given that prior studies suggest that BSID has predictive properties, we expected earlier assessments with this test to predict AC at 36 months of age. The results of our analysis first showed an age-related increase in AC scores (See Table 2), a decrease in grammatical complexity between 24 and 30 months of age (Charkaluk et al., Reference Charkaluk, Rousseau, Benhammou, Datin-Dorrière, Flamant, Gire, Kern, Pierrat, Kaminski and Marret2019; Isotani et al., Reference Isotani, Azevedo, Chiari and Perissinoto2009), and a PDI score lower than the normal range at 12 months, which matches the findings reported in prior studies in children with risk factors for atypical brain structure (Andalò et al., Reference Andalò, Rigo, Rossi, Majorano and Lavelli2022; Charkaluk et al., Reference Charkaluk, Rousseau, Benhammou, Datin-Dorrière, Flamant, Gire, Kern, Pierrat, Kaminski and Marret2019; Mwaniki et al., Reference Mwaniki, Atieno, Lawn and Newton2012). Regarding the second aim, our findings matched our expectations; gestational age in weeks and corpus callosum volume were positively associated with AC at 36 months, highlighting the importance of perinatal risk factors for atypical brain structure and MRI neuropathological patterns on language development (Charkaluk et al., Reference Charkaluk, Rousseau, Benhammou, Datin-Dorrière, Flamant, Gire, Kern, Pierrat, Kaminski and Marret2019; C. E. Rogers et al., Reference Rogers, Lean, Wheelock and Smyser2018; E. E. Rogers & Hintz, Reference Rogers and Hintz2016). Greater interaction with the environment also seems to benefit AC development by facilitating the attainment of fine motor milestones (Andalò et al., Reference Andalò, Rigo, Rossi, Majorano and Lavelli2022; Yildiz et al., Reference Yildiz, Yildiz, Camli and Elbasan2025). However, an unexpected finding was that maternal age significantly predicted AC scores, a finding that requires additional explanation. Finally, with respect to the third aim, we confirmed that BSID-2 scores at 12 and 30 months predicted AC scores at 36 months, which is in line with prior literature (Flynn et al., Reference Flynn, Huber and DeMauro2020; Lung et al., Reference Lung, Shu, Chiang, Chen and Lin2009). Our findings thus offer critical insights into the developmental characteristics of these infants and enhance our understanding of the interplay between early neurodevelopmental vulnerabilities and later language acquisition. They also underscore the importance of multimodal early assessment for identifying infants at risk of persistent language difficulties.
4.1. Comprehensive characterization of our sample
Although most language and cognitive measures in Figure 1 and Table 2 showed consistent improvement with age, a notable exception was the sentence complexity score, which declined slightly from 24 to 36 months. This deviation is particularly relevant since this population is expected to develop the ability to integrate word meaning in sentential contexts (Friedrich & Friederici, Reference Friedrich and Friederici2005c), which will progress to the identification of discourse incongruencies (Silva-Pereyra et al., Reference Silva-Pereyra, Rivera-Gaxiola and Kuhl2005), also contributing to the development of grammatical complexity. Our findings suggest that individuals born with prenatal and perinatal risk factors for brain injury exhibit more failures in grammatical complexity than in AC itself, which matches the findings of a prior study (Isotani et al., Reference Isotani, Azevedo, Chiari and Perissinoto2009). We propose that our study’s population may be more vulnerable to subtle disruptions in working memory, which may be related to their white matter abnormalities and may also affect vocabulary and phrase length production (Luu et al., Reference Luu, Ment, Allan, Schneider and Vohr2011; Marchman et al., Reference Marchman, Adams, Loi, Fernald and Feldman2016). In addition, given that previous studies also suggest that grammatical complexity typically accelerates between 30 and 36 months in low-risk populations (Huttenlocher et al., Reference Huttenlocher, Vasilyeva, Cymerman and Levine2002; Jackson-Maldonado, Reference Jackson-Maldonado and Chappele2003), its decline may reflect early neurodevelopmental challenges that this population might be unable to overcome.
We also found that our participants exhibited delayed achievement of gross and fine motor milestones and lower PDI scores at 12 months compared with normative developmental trajectories reported in non-pathological populations (Bracewell & Marlow, Reference Bracewell and Marlow2002; Dalton, Reference Dalton2005; Katona, Reference Katona, Vietze and Vaughan1988; Knobloch, Reference Knobloch1961). Our findings were consistent with previous studies reporting that one of the main sequelae of prenatal and perinatal risk factors for atypical brain structure is delayed neuromotor development, even in the absence of overt cerebral palsy (Bracewell & Marlow, Reference Bracewell and Marlow2002; Mwaniki et al., Reference Mwaniki, Atieno, Lawn and Newton2012; Sanchez et al., Reference Sanchez, Spittle, Cheong, Thompson, Doyle, Anderson and Morgan2019). In our study, the delay in motor milestones likely reflects early functional disruptions in sensorimotor integration and postural control, potentially stemming from subclinical perinatal neurological compromise. Moreover, the later emergence of complex fine motor skills, such as the pincer grasp and voluntary release, suggests prolonged maturation of corticospinal and cerebellar systems, which are crucial for precise motor coordination and are particularly vulnerable to early injury or immaturity (Pannek et al., Reference Pannek, Scheck, Colditz, Boyd and Rose2014).
Complementing the behavioral findings, the neuroimaging data revealed an increased right LV volume compared to the left, a pattern frequently observed in infants with developmental vulnerabilities or subtle white matter abnormalities (Lind et al., Reference Lind, Parkkola, Lehtonen, Munck, Maunu, Lapinleimu and Haataja2011; Thompson et al., Reference Thompson, Warfield, Carlin, Pavlovic, Wang, Bear, Kean, Doyle, Egan and Inder2007, Reference Thompson, Lee, Egan, Warfield, Doyle, Anderson and Inder2014). Neuropathological patterns such as enlarged ventricles may reflect reduced periventricular white matter volume or disturbances in cerebrospinal fluid dynamics, both of which are associated with altered neurodevelopmental outcomes (Inder et al., Reference Inder, Warfield, Wang, Hüppi and Volpe2005). Moreover, volumetric asymmetries in the ventricles have been linked to early disruptions in hemispheric development and lateralization, potentially influencing motor and cognitive profiles later in life (Gilmore et al., Reference Gilmore, Knickmeyer and Gao2018; Harmony, Reference Harmony2021). These structural findings support the hypothesis that delayed motor milestone attainment and language development difficulties in this cohort may be underpinned by neuroanatomical differences traceable to early brain development. Together, the cognitive, motor and MRI profiles underscore the importance of longitudinal neurodevelopmental monitoring in this high-risk population.
4.2. Predictors of AC at 36 months
An expected finding was that fine motor skills predicted AC at 36 months (Gonzalez et al., Reference Gonzalez, Alvarez and Nelson2019; Winter et al., Reference Winter, Stoeger and Suggate2021; Yildiz et al., Reference Yildiz, Yildiz, Camli and Elbasan2025). In this regard, typical language development has been associated with motor abilities through at least two hypotheses: 1) the speech–motor integration or shared activation hypothesis, and 2) the functionalist hypothesis. The first hypothesis suggests that the motor systems (premotor and primary motor cortices) contribute to processing perceptual skills that support language–motor abilities (Galantucci et al., Reference Galantucci, Fowler and Turvey2006; Hickok & Poeppel, Reference Hickok and Poeppel2007). This hypothesis also proposes that fine motor skills and vocabulary utilize similar underlying brain structures and processes, such as the Broca’s area, the cerebellum and the prefrontal cortex (Winter et al., Reference Winter, Stoeger and Suggate2021). At the same time, the second hypothesis ascribes a special role to motor development in new learning opportunities that involve interacting with objects, the environment and caregivers (Gonzalez et al., Reference Gonzalez, Alvarez and Nelson2019).
In our study, we found that an earlier consolidation age for the palmar grasp and scratching milestones was associated with higher AC scores, which aligns with the second hypothesis, which posits the importance of object manipulation in world understanding. These results also align with previous studies reporting an association between suboptimal infant neuromotor development and delays in language acquisition (Bartha-Doering et al., Reference Bartha-Doering, Schwartz, Kollndorfer, Fischmeister, Novak, Langs, Werneck, Prayer, Seidl and Kasprian2021) and those identifying fine motor skill milestones as predictors of later typical language outcomes in early infancy and childhood (Andalò et al., Reference Andalò, Rigo, Rossi, Majorano and Lavelli2022; Yildiz et al., Reference Yildiz, Yildiz, Camli and Elbasan2025). However, the positive association between AC and the ocular fixation milestone, measured in months, requires additional clarification. For this AC predictor, we propose at least two explanations. One might be that the ocular fixation milestone in our sample reflects a mix of involuntary and voluntary attention. Involuntary attention initially depends on the orienting network and is strongly influenced by environmental factors. This type of attention becomes more voluntary around the 1-year mark (Garon et al., Reference Garon, Bryson and Smith2008). Given that both types of attention appear in the first year, the infants might be exhibiting different forms of attention, as reflected in the ocular fixation milestone. On the other hand, the second explanation suggests that the meaning of spoken language may influence ocular fixation control during assessment (Allopenna et al., Reference Allopenna, Magnuson and Tanenhaus1998; Huettig & Altmann, Reference Huettig and Altmann2005). Between 6 and 12 months, infants should comprehend at least 6 to 13 words (Jackson-Maldonado, Reference Jackson-Maldonado and Chappele2003); therefore, the gaze might be directed towards the objects to which individual words refer in an accompanying visual display. Participants might be more likely to fixate on a known object when hearing part of or the entire word associated with it than on unrelated stimuli (Allopenna et al., Reference Allopenna, Magnuson and Tanenhaus1998; Huettig & Altmann, Reference Huettig and Altmann2005). The positive association between the age of the ocular fixation milestone and AC may then be explained by the increased knowledge or comprehension of new words acquired at 6 months. Moreover, because infants’ comprehension is an age-related process, they should be forced to fixate their gaze on the known word as age increases.
As hypothesized, we found that greater gestational age was a predictor of higher AC scores, consistent with prior studies in premature infants, which report that this population exhibits lower language skills (Isotani et al., Reference Isotani, Azevedo, Chiari and Perissinoto2009; Luu et al., Reference Luu, Ment, Schneider, Katz, Allan and Vohr2009; Mwaniki et al., Reference Mwaniki, Atieno, Lawn and Newton2012; C. E. Rogers et al., Reference Rogers, Lean, Wheelock and Smyser2018). Although we supposed that the MRI neuropathological pattern would be associated with the AC score, we did not directly hypothesize an association between AC and corpus callosum volume. However, this finding was expected based on previous studies, which describe an association between brain volumes and cognitive scores in infants with prenatal and perinatal risk of atypical brain structure (Foster-Cohen et al., Reference Foster-Cohen, Friesen, Champion and Woodward2010; Huang et al., Reference Huang, Zhu, Qu and Mu2016; Iwata et al., Reference Iwata, Bainbridge, Nakamura, Tamura, Takashima, Matsuishi and Iwata2010; Woodward et al., Reference Woodward, Anderson, Austin, Howard and Inder2006). Moreover, a previous study reports a positive correlation between the volume of the posterior corpus callosum and verbal fluency and vocabulary, and between the volume of the anterior corpus callosum and verbal span in healthy children (Bartha-Doering et al., Reference Bartha-Doering, Schwartz, Kollndorfer, Fischmeister, Novak, Langs, Werneck, Prayer, Seidl and Kasprian2021). This not only aligns with our findings but also highlights the significance of the corpus callosum in integrating information from both hemispheres, particularly in language network connectivity, in infants born with pre- and perinatal risk of atypical brain structure.
Although we hypothesized that maternal age would be a predictor of AC scores at 36 months, our findings did not support this hypothesis or prior studies reporting that advanced maternal age would be linked to brain development abnormalities and cognitive development delays (Doyle et al., Reference Doyle, Cheong, Burnett, Roberts, Lee and Anderson2015; Hackman & Farah, Reference Hackman and Farah2009; Howard et al., Reference Howard, Roberts, Lim, Lee, Barre, Treyvaud, Cheong, Hunt, Inder, Doyle and Anderson2011; Reidy et al., Reference Reidy, Morgan, Thompson, Inder, Doyle and Anderson2013; Richmond et al., Reference Richmond, Johnson, Seal, Allen and Whittle2016; Thompson et al., Reference Thompson, Kelly, Chen, Beare, Alexander, Seal, Lee, Matthews, Anderson, Doyle, Spittle and Cheong2019). Instead, we found that maternal age was positively associated with AC scores, consistent with other studies that relate maternal age to typical language development. For example, Muluk et al. (Reference Muluk, Bayoǧlu and Anlar2014) reported a positive correlation between mothers’ age and language comprehension in 36-month-olds, with children of older mothers exhibiting higher scores in word definition and object identification skills. The authors propose that this relationship may be accounted for by the amount of maternal attention devoted to infants’ development, which is greater in aged mothers. This explanation is also supported by other studies, which describe the importance of recurrent maternal stimulation of infants at birth through her voice, gestures and smile in improving infants’ AC (Brignoni-Pérez et al., Reference Brignoni-Pérez, Morales, Marchman, Scala, Feldman, Yeom and Travis2021; Soberón et al., Reference Soberón, Mónica Carlier, Jiménez, Harmony and Cycyk2019). We add that greater maternal age may be associated with a higher level of commitment to caregiving and support for child language development.
4.3. Psychometric test for assessing AC
Finally, we observed that MDI scores of BSID-2 at 12 and 30 months were the strongest predictors of standardized AC scores at 36 months, which matches previous studies describing the BSID-2 as one of the most widely reported tools for developmental assessment for infants and children with or without risk factors for atypical brain structure (Cirelli et al., Reference Cirelli, Bickle Graz and Tolsa2015; Flynn et al., Reference Flynn, Huber and DeMauro2020). Our findings are consistent with a previous study, which also reports that BSID scores may predict cognitive functioning at school age (Greene et al., Reference Greene, Patra, Silvestri and Nelson2013; O’Shea et al., Reference O’Shea, Joseph, Allred, Taylor, Leviton, Heeren, Douglass, Frazier, Jara and Kuban2018), and add to prior literature the predictive value of BSID for AC development (Lung et al., Reference Lung, Shu, Chiang, Chen and Lin2009).
Our results highlight the crucial role of early neurodevelopmental assessments in identifying infants at higher risk of later cognitive and communicative difficulties. When standardized, developmentally appropriate tools such as the BSID-2 are applied systematically, they can serve not only as diagnostic instruments but also as valuable predictors of later functional outcomes. Early identification enables the timely implementation of individualized interventions that support cognitive and communicative development during sensitive periods of brain plasticity. Moreover, using validated tools enhances the specificity of developmental surveillance and reduces the risk of overlooking subtle deficits, which might only become clinically evident at later stages. This highlights the importance of strengthening routine pediatric follow-up protocols by incorporating comprehensive developmental assessments, particularly in populations with prenatal and perinatal risk factors, to facilitate earlier access to support services and optimize long-term outcomes.
5. Conclusions
We concluded that AC is influenced by motor development and caregivers’ interactions, which facilitate new learning opportunities that enable interaction with the environment, thereby affecting language comprehension. In addition, perinatal risk factors for atypical brain structure, such as prematurity and MRI neuropathological patterns, play an adverse role in this cognitive development, particularly atypical brain structure associated with this clinical condition, including corpus callosum volume, which appears to affect AC.
Our findings also emphasize the need for early and comprehensive developmental assessments using validated tools, such as the BSID-2, to detect subtle delays and predict later cognitive outcomes. Early identification of at-risk infants enables targeted interventions during sensitive developmental periods, thereby improving adaptive trajectories and long-term functional outcomes in children exposed to early neurological compromise.
The present study has inherent limitations. Most importantly, due to the longitudinal nature of our findings, they cannot be extrapolated to the general population with risk factors for atypical brain structure, as our sample is small and all participants received Katona Neurohabilitation treatment to prevent neurological sequelae. Additionally, a group with typical development was not included in this study. Moreover, for our sample, we lacked data on attention assessment, mothers’ intelligence and other social or cognitive variables. We also used traditional anthropometric measures to assess the participants. Body composition measures (e.g., energy X-ray absorptiometry) are commonly employed; however, they may provide more nuanced metrics for studies examining the impact of specific anthropometric predictors on maturation and cognitive function in children. Therefore, interpretations of this study should be carried out carefully, as it aims to identify predictors of language development; multiple factors were not considered.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/langcog.2026.10073.
Data availability statement
The data are available in the following link: https://figshare.com/s/a30cbffda6dde05d93c7
Acknowledgements
The authors would like to acknowledge the participation of the following individuals: Teresa Álvarez, Paulina Álvarez, Silvia Ruiz Tovar, Dulce Bautista Aguilar, Yeni Almaraz, Adrián Elías Jiménez and Consuelo Pedraza. We are especially grateful to the children and their families who participated in this study.
Funding statement
This research was supported by PAPIIT IT 200223 and CONAHCYT number CF-2023-I-220.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have influenced the work reported in this paper.






 Open access
Open access