


Introduction
Given the globally aging population, there is an increasing demand for health care services and long-term care (LTC) homes to support older adults who require assistance with day-to-day living (United Nations Department of Economic and Social Affairs, n.d.). Many older adults who live in LTC homes are at an increased risk for depression and social isolation (Boamah et al., Reference Boamah, Weldrick, Lee and Taylor2021). Moreover, many older adults in LTC experience physical limitations, such as reduced mobility, chronic illness, cognitive decline, and increased frailty, in addition to emotional and social concerns, all of which may contribute to a diminished quality of life (QoL) (Liu et al., Reference Liu, Kao and Ying2020; Qiao et al., Reference Qiao, Qiao, Tan, Chen, Peng, Mao, Zhao, Chen and Yao2025; Scocco et al., Reference Scocco, Rapattoni and Fantoni2006; Yuan et al., Reference Yuan, Lapane, Tjia, Baek, Liu and Ulbricht2021).
The World Health Organization (WHO) defines QoL as ‘an individual’s perception of their position in life in the context of the culture in which they live and in relation to their goals, expectations, standards, and concerns’ (WHO, 1995, p. 1403). Residents in LTC homes face a variety of challenges, such as loss of independence, loneliness, communication barriers, and systemic factors (e.g., location of LTC relative to friends and family) that may negatively impact their QoL (Boamah et al., Reference Boamah, Weldrick, Lee and Taylor2021). Accordingly, routine assessment and targeted interventions for individuals living in LTC to address these challenges are necessary (Arias-Casais et al., Reference Arias-Casais, Amuthavalli Thiyagarajan, Rodrigues Perracini, Park, van den Block, Sumi, Sadana, Banerjee and Han2022). Further, health-related quality of life (HRQoL), a subset of QoL, includes the impact of disease and treatment on disability, daily functioning, perceived health, and living a fulfilling life (Mayo, Reference Mayo2015). Given the likelihood that many older adults who live in LTC homes experience health concerns, understanding both QoL and its subset, HRQoL, and aiming to identify ways to improve these factors in older adults is paramount (United Nations Department of Economic and Social Affairs, 2020). In this paper, we use the term QoL to include central aspects of both QoL and HRQoL.
Traditional models of care often fall short in addressing the complex and interconnected needs of older adults in LTC, highlighting the need for more holistic approaches to promote well-being (Verbeek & Mitchell, Reference Verbeek and Mitchell2022). Dance is a holistic approach to care for older adults, as dance may be associated with a range of physical, emotional, cognitive, and social benefits (Clifford et al., Reference Clifford, Shanahan, McKee, Cleary, O’Neill, O’Gorman, Louw and Ní Bhriain2023; Waugh et al., Reference Waugh, Yourdan, Casale, Balaban, Cross and Merom2024). Dance intervention refers to ‘an organised form of physical activity associated with bodily movement in response to music in an improvised or choreographed style’ (Salihu et al., Reference Salihu, Wong, Bello and Kwan2021, p. 1333). In a meta-analysis, it was found that undertaking structured dance of any genre is equally as and occasionally more effective than other types of structured exercise for improving a range of health outcome measures, including cardiovascular health, range of motion, balance, and strength measures (Fong Yan et al., Reference Fong Yan, Cobley, Chan, Pappas, Nicholson, Ward, Murdoch, Gu, Trevor, Vassallo, Wewege and Hiller2018). For older adults with mild cognitive impairment, Alzheimer’s disease, and/or dementia, dance has been proposed as an effective, affordable, and engaging non-pharmacological treatment option, and may complement existing treatment approaches (Tao et al., Reference Tao, Awan-Scully, Ash, Pei, Gu, Gao, Cole and Baker2023). Dance interventions have the potential to improve health outcomes and foster meaningful social interactions, ultimately contributing to enhanced QoL (Barnstaple et al., Reference Barnstaple, Laurita-Spanglet, Fanning, Soriano and Hugenschmidt2024; Paglione et al., Reference Paglione, Kenny, McDonough, Din and White2024).
Although dance interventions have been explored in a variety of populations, their specific impact on QoL in LTC settings remains under-researched and not synthesized. Therefore, the objective of this systematic review was to identify, critically appraise, and synthesize the evidence on the effectiveness of dance interventions on QoL for older adults living in LTC.
Methods
Registration and protocol
This review was registered in the PROSPERO registry (CRD42024600978). The protocol is available from the corresponding author on reasonable request.
Framework
The Cochrane Handbook informed the conduct of this review (Higgins et al., Reference Higgins, Chandler, Cumpston, Li, Page and Welch2024). Reporting was compliant with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guideline (Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson, McDonald and Moher2021).
Patient and public involvement
This project has four patient partners (LR, PLC, EPJ, and KS) who identify as older adult women. LR and KS participate in dance, PLC engages in an active lifestyle, and EPJ is interested in this topic. LR and KS previously worked as nurses, PLC previously worked as a scientist, and EPJ previously worked as a social worker in geriatric assessment.
The project was conceptualized by two of the patient partners (LR and PLC) and successfully submitted to a funding opportunity for patient partner-initiated projects funded by the Strategy for Patient-Oriented Research-Evidence Alliance (SPOR EA; SPOR Evidence Alliance, n.d.). The SPOR EA is funded by the Canadian Institutes of Health Research and includes 400+ researchers, trainees, and patient partners, all engaged in promoting evidence-informed health policy and practice (Tricco et al., Reference Tricco, Zarin, Clement, Abou-Setta, Curran, LeBlanc, Li, Godfrey, Moffitt, Moher, Colquhoun, Graham, Florez, Wilhelm, Isaranuwatchaia, Mann, Hamilton, Srinivasan, Bornstein and Straus2022). The four patient partners have been involved in all aspects of the study as members of the research team, including developing the research question, refining the eligibility criteria, training in title/abstract screening, participating in full-text screening, developing the data extraction sheet, and contributing to the revision of this manuscript. The patient partners wrote the plain language summary that accompanies this manuscript (Supplementary Material I). Due to the significant patient partner involvement in this review, we have included an additional relevant reporting guidance: the short form of the Guidance for Reporting Involvement of Patient and the Public (GRIPP)-2 (see Supplementary Material II; Staniszewska et al., Reference Staniszewska, Brett, Simera, Seers, Mockford, Goodlad, Altman, Moher, Barber, Denegri, Entwistle, Littlejohns, Morris, Suleman, Thomas and Tysall2017).
Data sources and strategy
We conducted searches in seven databases (Ovid MEDLINE, Ovid APA PsycINFO, Scopus, CINAHL EBSCO, Ovid Embase, SPORTDiscus EBSCO, and Ovid ERIC) and searched ClinicalTrials.gov to identify ongoing or unpublished trials related to dance interventions in LTC facilities. Relevant journals, reference lists of included studies, and relevant systematic reviews were manually searched to identify additional studies not captured through electronic searches. Searches were dated from inception until July 21, 2024 (see Supplementary Material III).
Search queries were developed in consultation with a research librarian and in collaboration with the research team. Search terms related to (a) dance and (b) LTC were combined using AND/ OR functions to develop the search strategy. The retrieved searches using these two terms were quite small. As such, we did not include ‘QoL’ or ‘HRQoL’ as search terms, as we did not want to further limit the studies retrieved.
We used the Peer Review of Electronic Search Strategies (PRESS) 2015 Evidence-Based Checklist to peer-review the final MEDLINE query (McGowan et al., Reference McGowan, Sampson, Salzwedel, Cogo, Foerster and Lefebvre2016; see Supplementary Material IV).
Eligibility criteria
We included studies that met the following criteria: (1) Older adults, of whom at least 50% of the sample were 60 years or older according to the United Nation’s definition of old age (United Nations High Commissioner for Refugees, 2024) living in LTC facilities (‘also known as nursing homes, personal care homes, residential care facilities, lodges, assisted living facilities and supportive housing’ and ‘extended care, chronic care or complex continuing care’ [Canadian Institute for Health Information, 2025]); (2) Dance interventions delivered by any health care provider, staff, or volunteer; (3) A comparison group (e.g., other physical activity interventions, pharmaceutical management, other recreation, recreational therapy programs, occupational therapy, or physical therapy activities); (4) QoL or HRQoL outcome measures; and (5) Randomized controlled trials, quasi-experimental studies, and observational studies. To support decisions about what constituted a QoL measure, we used the WHO (WHO, 1995) definition of QoL and the Mayo et al. (Reference Mayo2015) definition of HRQoL, both of which qualified for inclusion in our study and are outlined in our protocol. Overall, we took a liberal approach to decisions about QoL measures and included measures that had subscales for at least 2–3 of the domains of QoL in our frameworks. Exclusion criteria included studies of individuals younger than 60 years old or if they do not reside in a LTC facility, other physical activities if not delivered as part of a dance intervention, and studies without a comparison group.
Study selection
After removing duplicates, a two-step process was conducted in Covidence (Veritas Health Innovation, 2024). First, title/abstract screening was completed independently by three authors (AD, ZM, and HC). Pilot screening was performed on 50 articles to ensure a per cent agreement of >80% was achieved in the title and abstract screening phase. Discrepancies were resolved by consensus or by a third author (HC or AD). Second, full-text screening was completed independently by two authors, including patient partners (AD, HC, ZM, EPJ, LR, PC, and KS). For full-text screening, each of the patient-partners (EPJ, LR, PC, and KS) was paired with one of the study leads (AD or HC). Discrepancies were resolved by consensus or the involvement of a third reviewer (HC or AD).
Data extraction
Two authors (ZM and AD) independently conducted data extraction using pilot-tested and standardized extraction documents. Discrepancies were resolved by consensus or the involvement of a third author (HC). Extracted data included: authors, year of publication, country, sample size, study design, study-setting demographics (age, sex/gender, sample size), intervention characteristics, comparator characteristics, QoL and HRQoL outcome measure (name of scale, type, and relevant sub-scales), attendance rates, measurement of fidelity, use of theory (name of theory and how it was applied), proposed mechanisms of action, and results (descriptors, point estimates, and variability).
Risk of bias
Two authors (MLC and HAS) independently assessed the quality of evidence of the included studies using the Downs and Black Quality Assessment Tool (Downs and Black) (Downs & Black, Reference Downs and Black1998). Discrepancies were resolved through consensus. Downs and Black include 27 items that assess reporting transparency, external validity, internal validity (including bias and confounding), and power and can be used with intervention and non-intervention studies (Downs & Black, Reference Downs and Black1998). We modified the Downs and Black, in alignment with other researchers, to score item 27 as 0 (no power calculation reported) or 1 (power calculation reported) rather than the original (scored out of 32; item 27 scored from 0 to 5) (O’Connor et al., Reference O’Connor, Tully, Ryan, Bradley, Baxter and McDonough2015). The methodological quality score (out of 27) is calculated as poor (<7), limited (7–13), moderate (14–20), and strong >21 (Downs & Black, Reference Downs and Black1998; Jäkel & von Hauenschild, Reference Jäkel and von Hauenschild2011). Scores can range between 0 and 28.
We deviated from the risk of bias tools initially proposed in the protocol, as Downs and Black can be used for all study designs. Thus, we used the same tool to assess the risk of bias across all included studies.
Data synthesis and analysis
We presented a narrative summary of the evidence and created tables to summarize and categorize the extracted information based on the type of dance intervention. Due to the large heterogeneity of the data (e.g., different QoL outcome measures, populations, and dance types), performing a meta-analysis of the data was not possible. We used a descriptive quantitative analysis to identify the use of theory, mechanisms of action, and intervention attendance and fidelity.
Results
Study selection
The electronic database search identified 1,377 citations. After the removal of duplicates, 819 citations were reviewed in the title and abstract screening, of which 53 articles were selected for full-text screening. Following review of the full texts, eight articles met our inclusion criteria and were synthesized in the narrative review. However, following extraction, it was noted that two studies (Chang, Chen, et al., Reference Chang, Chen, Liu, Yong, Yang, Zhu, Wang and Yan2021; Chang, Zhu, et al., Reference Chang, Zhu, Zhang, Yong, Yang, Wang and Yan2021) included the same sample and outcome measures. As such, Chang, Chen et al. (Reference Chang, Chen, Liu, Yong, Yang, Zhu, Wang and Yan2021) was excluded, resulting in seven studies included in our review. A PRISMA diagram of the study selection process is presented in Figure 1 (Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson, McDonald and Moher2021).
PRISMA diagram.

Figure 1. Long description
At the top, two boxes: left, ‘Studies from databases/registers (n = 1377)' lists Scopus 424, Embase 396, C I N A H L 175, M E D L I N E 156, Psyc I N F O 52, Unspecified 174; right, ‘References from other sources (n = 0)'. Both flow to ‘References removed (n = 559)' with breakdown: Duplicates manually 18, by Covidence 541, by automation 0, other reasons blank. Downward, ‘Studies screened (n = 818)' splits right to ‘Studies excluded (n = 759)'. Down, ‘Studies sought for retrieval (n = 59)' splits right to ‘Studies not retrieved (n = 0)'. Down, ‘Studies assessed for eligibility (n = 59)' splits right to ‘Studies excluded (n = 52)' with reasons: Not English 4, Wrong setting 1, Wrong study design 12, Not dance intervention 14, Wrong patient population 1, Not quality of life 20. Down, ‘Studies included in review (n = 7)'.
Study characteristics
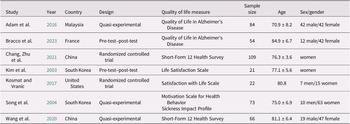
The included studies were published between 2003 and 2023 and were conducted in China (n = 2), South Korea (n = 2), France (n = 1), Malaysia (n = 1), and the United States of America (n = 1). Overall, 429 participants were included across all seven studies, of which 339 (79%) were female or women participants. The seven studies included two randomized controlled trials (Chang, Zhu, et al., Reference Chang, Zhu, Zhang, Yong, Yang, Wang and Yan2021; Kosmat & Vranic, Reference Kosmat and Vranic2017), three quasi-experimental (Adam et al., Reference Adam, Ramli and Shahar2016; Song et al., Reference Song, June, Kim and Jeon2004; Wang et al., Reference Wang, Yin, Meng, Shang, Meng, Zheng, Wang and Chen2020), and two pre-test–post-test (Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023; Kim et al., Reference Kim, June and Song2003). Table 1 presents a summary of the study characteristics. See Supplementary Material V for additional extracted information per A MeaSurement Tool to Assess systematic Reviews (AMSTAR)-2 (Shea et al., Reference Shea, Reeves, Wells, Thuku, Hamel, Moran, Moher, Tugwell, Welch, Kristjansson and Henry2017).
Study characteristics

Table 1. Long description
From the top row, column headers are Study, Year, Country, Design, Quality of life measure, Sample size, Age, and Sex or gender. Row 1: Adam et al., 2016, Malaysia, Quasi-experimental, Quality of Life in Alzheimer’s Disease, 84, 70.9 plus or minus 8.2, 42 male and 42 female. Row 2: Bracco et al., 2023, France, Pre-test post-test, Quality of Life in Alzheimer’s Disease, 54, 84.9 plus or minus 6.7, 12 male and 42 female. Row 3: Chang, Zhu et al., 2021, China, Randomized controlled trial, Short-Form 12 Health Survey, 109, 76.3 plus or minus 3.6, women. Row 4: Kim et al., 2003, South Korea, Pre-test post-test, Life Satisfaction Scale, 21, 77.1 plus or minus 5.6, women. Row 5: Kosmat and Vranic, 2017, United States, Randomized controlled trial, Satisfaction with Life Scale, 22, 80.8, 7 men and 15 women. Row 6: Song et al., 2004, South Korea, Quasi-experimental, Motivation Scale for Health Behavior and Sickness Impact Profile, 73, 75.0 plus or minus 6.9, 10 men and 63 women. Row 7: Wang et al., 2020, China, Quasi-experimental, Short-Form 12 Health Survey, 66, 81.1 plus or minus 6.4, 19 male and 47 female.
Risk of bias
The methodological quality of the included studies, based on the Downs and Black Quality Assessment Tool (Downs & Black, Reference Downs and Black1998), ranged from 10 (Kim et al., Reference Kim, June and Song2003) to 20 (Chang, Zhu, et al., Reference Chang, Zhu, Zhang, Yong, Yang, Wang and Yan2021; Wang et al., Reference Wang, Yin, Meng, Shang, Meng, Zheng, Wang and Chen2020). Five of the seven studies had a methodological quality score in the moderate range (14–20) (Adam et al., Reference Adam, Ramli and Shahar2016; Chang, Zhu, et al., Reference Chang, Zhu, Zhang, Yong, Yang, Wang and Yan2021; Song et al., Reference Song, June, Kim and Jeon2004; Wang et al., Reference Wang, Yin, Meng, Shang, Meng, Zheng, Wang and Chen2020). The remaining two studies had a methodological quality score in the low range (10–13) (Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023; Kim et al., Reference Kim, June and Song2003).
All studies reported their objectives, main outcome measures, and participant characteristics. All studies conducted their intervention in a natural setting (LTC). No studies reported on intervention adherence or compliance, and no studies concealed randomization from both participants and the intervention delivery team (e.g., health care staff). Chang, Zhu et al. (Reference Chang, Zhu, Zhang, Yong, Yang, Wang and Yan2021), who used a clustered randomized controlled trial study design, did not account for clustering in these analyses, affecting the strength and certainty of findings.
Dance intervention characteristics
Five of the seven studies tested a form of dance that they reported was targeted for a specific country or cultural group. Two utilized Chinese Square dance specifically as a popular form of dance for people in China (Chang, Zhu, et al., Reference Chang, Zhu, Zhang, Yong, Yang, Wang and Yan2021; Wang et al., Reference Wang, Yin, Meng, Shang, Meng, Zheng, Wang and Chen2020), two used Korean Dance Movement specifically targeted for people in Korea (Kim et al., Reference Kim, June and Song2003; Song et al., Reference Song, June, Kim and Jeon2004), and one used Poco-Poco dance as a common dance form in Malaysia (Adam et al., Reference Adam, Ramli and Shahar2016). In the remaining two, one chose Tango because they felt the movements would be effective (Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023), and the other chose Slow Waltz but did not report why (Kosmat & Vranic, Reference Kosmat and Vranic2017). Sessions ranged from one to four times per week, with most lasting 45–60 min. The total program duration ranged from 6 weeks (Adam et al., Reference Adam, Ramli and Shahar2016) to 24 weeks (Song et al., Reference Song, June, Kim and Jeon2004), with longer durations typically offering more complex or progressive activities.
All interventions included warm-up and cool-down segments, typically 5–15 min each. Main dance activities included choreography (e.g., slow waltz), movement routines (e.g., aerobic sequences), or traditional steps, often incorporating paired or group movements. Some interventions included social activities like greetings and small talk as a warm-up (Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023), while others focused on movement and range of motion as a warm-up (Song et al., Reference Song, June, Kim and Jeon2004). All dance interventions were delivered in person; however, the type of facilitator and extent of training varied across studies. Several programs were led by trained health or rehabilitation professionals, such as physical therapists (Adam et al., Reference Adam, Ramli and Shahar2016), nurse leaders (Kim et al., Reference Kim, June and Song2003), or trained instructors (Chang, Zhu, et al., Reference Chang, Zhu, Zhang, Yong, Yang, Wang and Yan2021). Others involved specialized personnel, including a dance pedagogist (Kosmat & Vranic, Reference Kosmat and Vranic2017) and a Korean dance expert (Song et al., Reference Song, June, Kim and Jeon2004). In some cases, nursing staff were trained to deliver the intervention following a ‘train-the-trainer’ model, where facilitators received therapeutic tango training and additional support from a dance movement therapist and musician (Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023). In Wang et al. (Reference Wang, Yin, Meng, Shang, Meng, Zheng, Wang and Chen2020), facility staff led the sessions; however, the authors did not detail specific training procedures. Overall, the level of facilitator expertise and documentation of training varied considerably between studies. See Table 2 for a complete summary of dance intervention characteristics.
Intervention characteristics
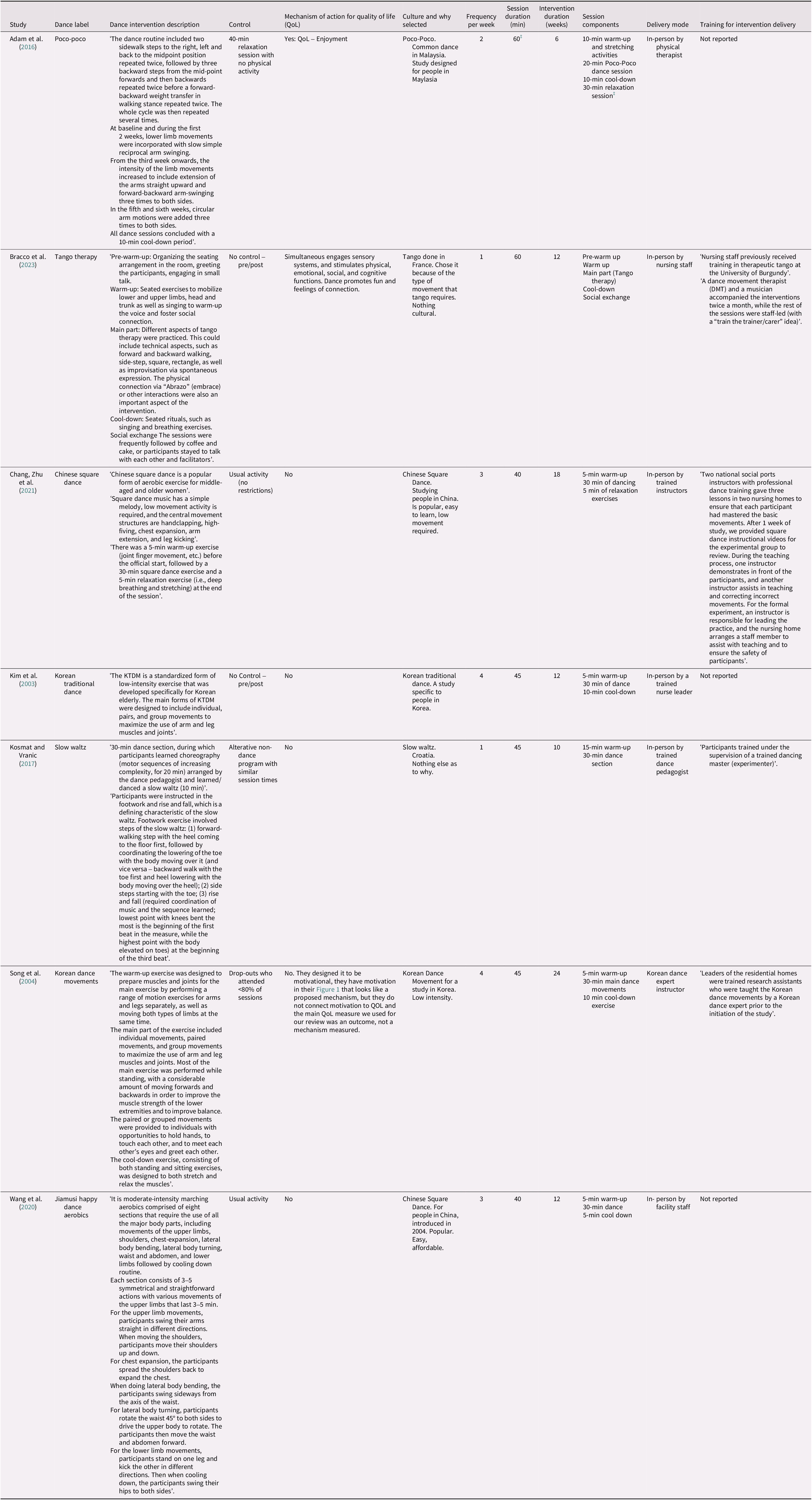
Table 2. Long description
The table contains twelve columns. From left to right, columns are Study, Dance label, Dance intervention description, Control, Mechanism of action for quality of life (QoL), Culture and why selected, Frequency per week, Session duration in minutes, Intervention duration in weeks, Session components, Delivery mode, and Training for intervention delivery. Each row details a different study: Adam et al. 2016 describes Poco-poco dance in Malaysia with two sessions per week, 60 minutes each, over 6 weeks, delivered in-person by a physical therapist, with no training reported. Bracco et al. 2023 covers Tango therapy in France, one session per week, 60 minutes, 12 weeks, delivered by nursing staff trained in therapeutic tango, with support from a dance movement therapist and musician. Chang, Zhu et al. 2021 presents Chinese square dance in China, three sessions per week, 40 minutes, 18 weeks, led by trained instructors with instructional videos and staff assistance. Kim et al. 2003 details Korean traditional dance, four sessions per week, 45 minutes, 12 weeks, delivered by a trained nurse leader, training not reported. Kosmat and Vranic 2017 describes Slow waltz in Croatia, one session per week, 45 minutes, 10 weeks, led by a trained dance pedagogist. Song et al. 2004 covers Korean dance movements, four sessions per week, 45 minutes, 24 weeks, led by a Korean dance expert instructor, with research assistants trained by the expert. Wang et al. 2020 presents Jiamusi happy dance aerobics in China, three sessions per week, 40 minutes, 12 weeks, delivered by facility staff. Each study row includes detailed descriptions of the dance routines, control conditions, mechanisms for quality of life, cultural context, session breakdowns, and delivery training. Footnotes clarify discrepancies in session duration reporting for Adam et al.
‡ Adams et al. reported that the dance intervention was 60 min in duration; however, their explanation of the dance intervention totals 70 min.
Quality of life outcome characteristics
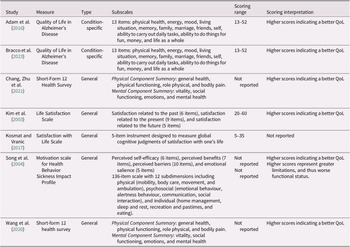
The studies utilized both condition-specific and general QoL measures to assess outcomes. Between studies, outcome measures were framed differently with respect to QoL; however, all outcome measures met our criteria for QoL/HRQoL. Condition-specific tools were used in two studies with adults living with Alzheimer’s disease (Adam et al., Reference Adam, Ramli and Shahar2016; Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023). The remaining five studies used general measures of QoL (and HRQoL), including the Short-Form 12 Health Survey (Chang, Zhu, et al., Reference Chang, Zhu, Zhang, Yong, Yang, Wang and Yan2021; Wang et al., Reference Wang, Yin, Meng, Shang, Meng, Zheng, Wang and Chen2020), the Life Satisfaction Scale (Kim et al., Reference Kim, June and Song2003), the Satisfaction with Life Scale (Kosmat & Vranic, Reference Kosmat and Vranic2017), the Motivation Scale for Health Behavior (Song et al., Reference Song, June, Kim and Jeon2004), and the Sickness Impact Profile (Song et al., Reference Song, June, Kim and Jeon2004). In general, higher scores indicated better QoL, although some studies did not report scoring ranges or interpretations (see Table 3).
Quality of life outcome characteristics

Table 3. Long description
The table contains seven rows, each corresponding to a different study, and six columns labeled Study, Measure, Type, Subscales, Scoring range, and Scoring interpretation. From top to bottom: Adam et al. 2016 and Bracco et al. 2023 both use the Quality of Life in Alzheimer’s Disease measure, condition-specific, with 13 subscales including physical health, energy, mood, living situation, memory, family, marriage, friends, self, daily tasks, fun activities, money, and life as a whole; scoring range is 13 to 52, higher scores indicate better quality of life. Chang, Zhu et al. 2021 and Wang et al. 2020 use the Short-Form 12 Health Survey, general type, with subscales divided into Physical Component Summary (general health, physical functioning, role physical, bodily pain) and Mental Component Summary (vitality, social functioning, emotions, mental health); scoring range not reported, higher scores indicate better quality of life. Kim et al. 2003 uses the Life Satisfaction Scale, general type, with subscales for satisfaction related to the past (6 items), present (9 items), and future (5 items); scoring range 20 to 60, higher scores indicate better quality of life. Kosmat and Vranic 2017 uses the Satisfaction with Life Scale, general type, a 5-item instrument for global cognitive judgments of life satisfaction; scoring range 5 to 35, scoring interpretation not reported. Song et al. 2004 uses two measures: Motivation scale for Health Behavior (subscales: perceived self-efficacy, benefits, barriers, emotional salience) and Sickness Impact Profile (136 items, 12 subdimensions including physical, psychosocial, and individual domains); scoring ranges not reported, higher scores indicate better quality of life for the motivation scale, but for the Sickness Impact Profile, higher scores represent greater limitations and worse functional status. Note at the bottom defines QoL as quality of life.
Note. QoL = quality of life.
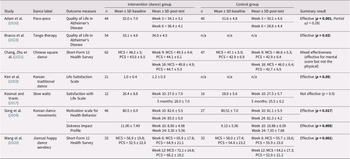
Results of the dance intervention
Across the seven studies, dance-based interventions generally showed positive effects on QoL and associated outcomes, including life satisfaction and health behaviour outcomes. In one study, Poco-Poco dance significantly improved QoL for individuals living with Alzheimer’s disease, with mean scores rising from 32.0 ± 7.0 at baseline to 36.4 ± 4.1 at Week 6 in the intervention group compared to a decline in the control group (p < 0.001, partial η2 = 0.29; Adam et al., Reference Adam, Ramli and Shahar2016). In another study, Tango therapy led to a significant improvement from a baseline of 33.1 ± 4.6 to 34.0 ± 4.5 post-intervention (p = 0.03; Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023).
In two studies, QoL was measured using the mental component scores (MCS) and physical component scores (PCS) from the Short-Form 12 (Chang, Zhu, et al., Reference Chang, Zhu, Zhang, Yong, Yang, Wang and Yan2021; Wang et al., Reference Wang, Yin, Meng, Shang, Meng, Zheng, Wang and Chen2020). Wang et al. (Reference Wang, Yin, Meng, Shang, Meng, Zheng, Wang and Chen2020) showed that Chinese square dance aerobics improved MCS at both 6 and 12 weeks (p = 0.03 and p < 0.001, respectively) and improved PCS at 12 weeks (p = 0.003). Both MCS and PCS were improved following a Chinese square dance intervention ([MCS: 9 weeks, p = 0.019; 18 weeks, p = 0.008]; [PCS: 9 weeks, p < 0.001; 18 weeks, p = 0.008]; Chang, Zhu, et al., Reference Chang, Zhu, Zhang, Yong, Yang, Wang and Yan2021).
In a study of Korean dance movements, health behaviour motivation improved from 80.5 ± 6.9 to 85.0 ± 6.0 at Week 24 (p = 0.017) and functional status as measured by the Sickness Impact Profile improved from 11.00 ± 7.48 to 5.30 ± 5.56 at Week 24 (p = 0.005; Song et al., Reference Song, June, Kim and Jeon2004). In a study of Korean traditional dance, Life Satisfaction Scores improved from 0.96 ± 0.4 to 1.17 ± 0.3 (p < 0.05; Kim et al., Reference Kim, June and Song2003). In contrast, a dance intervention that incorporated the slow waltz did not significantly affect Satisfaction with Life scores (p = 0.90; Kosmat & Vranic, Reference Kosmat and Vranic2017; see Table 4).
Dance intervention results by study
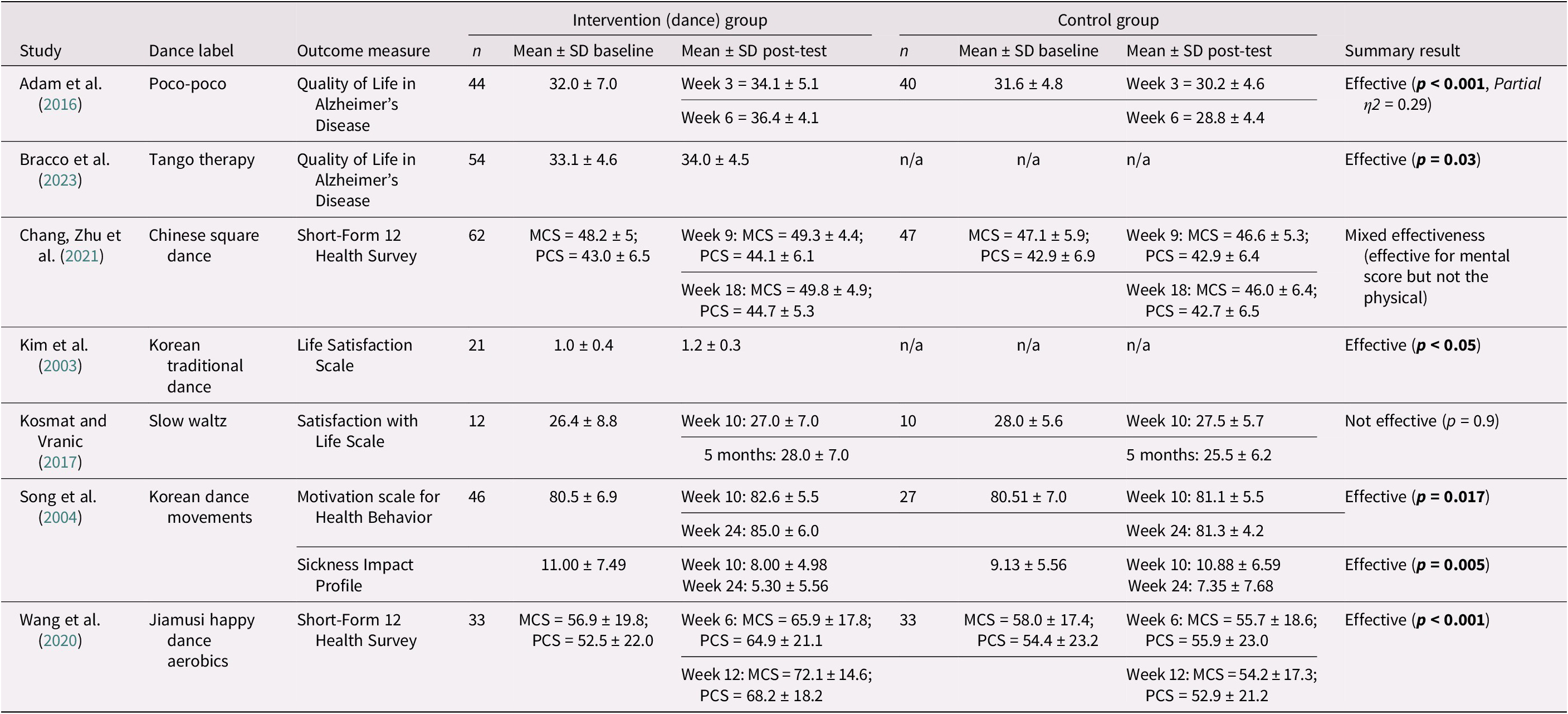
Table 4. Long description
The table contains nine columns: Study, Dance label, Outcome measure, Intervention group (n, mean plus or minus S D baseline, mean plus or minus S D post-test), Control group (n, mean plus or minus S D baseline, mean plus or minus S D post-test), and Summary result. From top to bottom: Adam et al. 2016, Poco-poco, Quality of Life in Alzheimer’s Disease, intervention n equals 44, baseline 32.0 plus or minus 7.0, week 3 34.1 plus or minus 5.1, week 6 36.4 plus or minus 4.1; control n equals 40, baseline 31.6 plus or minus 4.8, week 3 30.2 plus or minus 4.6, week 6 28.8 plus or minus 4.4; result: Effective, p less than 0.001, partial eta squared equals 0.29. Bracco et al. 2023, Tango therapy, Quality of Life in Alzheimer’s Disease, intervention n equals 54, baseline 33.1 plus or minus 4.6, post-test 34.0 plus or minus 4.5; control n not applicable; result: Effective, p equals 0.03. Chang, Zhu et al. 2021, Chinese square dance, Short-Form 12 Health Survey, intervention n equals 62, baseline M C S equals 48.2 plus or minus 5, P C S equals 43.0 plus or minus 6.5; week 9 M C S equals 49.3 plus or minus 4.4, P C S equals 44.1 plus or minus 6.1; week 18 M C S equals 49.8 plus or minus 4.9, P C S equals 44.7 plus or minus 5.3; control n equals 47, baseline M C S equals 47.1 plus or minus 5.9, P C S equals 42.9 plus or minus 6.9; week 9 M C S equals 46.6 plus or minus 5.3, P C S equals 42.9 plus or minus 6.4; week 18 M C S equals 46.0 plus or minus 6.4, P C S equals 42.7 plus or minus 6.5; result: Mixed effectiveness, effective for mental score but not physical. Kim et al. 2003, Korean traditional dance, Life Satisfaction Scale, intervention n equals 21, baseline 1.0 plus or minus 0.4, post-test 1.2 plus or minus 0.3; control n not applicable; result: Effective, p less than 0.05. Kosmat and Vranic 2017, Slow waltz, Satisfaction with Life Scale, intervention n equals 12, baseline 26.4 plus or minus 8.8, week 10 27.0 plus or minus 7.0, 5 months 28.0 plus or minus 7.0; control n equals 10, baseline 28.0 plus or minus 5.6, week 10 27.5 plus or minus 5.7, 5 months 25.5 plus or minus 6.2; result: Not effective, p equals 0.9. Song et al. 2004, Korean dance movements, Motivation scale for Health Behavior, intervention n equals 46, baseline 80.5 plus or minus 6.9, week 10 82.6 plus or minus 5.5, week 24 85.0 plus or minus 6.0; control n equals 27, baseline 80.51 plus or minus 7.0, week 10 81.1 plus or minus 5.5, week 24 81.3 plus or minus 4.2; result: Effective, p equals 0.017. Song et al. 2004, Sickness Impact Profile, intervention baseline 11.00 plus or minus 7.49, week 10 8.00 plus or minus 4.98, week 24 5.30 plus or minus 5.56; control baseline 9.13 plus or minus 5.56, week 10 10.88 plus or minus 6.59, week 24 7.35 plus or minus 7.68; result: Effective, p equals 0.005. Wang et al. 2020, Jiamusi happy dance aerobics, Short-Form 12 Health Survey, intervention n equals 33, baseline M C S equals 56.9 plus or minus 19.8, P C S equals 52.5 plus or minus 22.0; week 6 M C S equals 65.9 plus or minus 17.8, P C S equals 64.9 plus or minus 21.1; week 12 M C S equals 72.1 plus or minus 14.6, P C S equals 68.2 plus or minus 18.2; control n equals 33, baseline M C S equals 58.0 plus or minus 17.4, P C S equals 54.4 plus or minus 23.2; week 6 M C S equals 55.7 plus or minus 18.6, P C S equals 55.9 plus or minus 23.0; week 12 M C S equals 54.2 plus or minus 17.3, P C S equals 52.9 plus or minus 21.2; result: Effective, p less than 0.001. Notes: S D equals standard deviation, M C S equals mental component score, P C S equals physical component score, n slash a equals not applicable. Bolded values indicate statistical significance.
Note: SD = standard deviation; MCS = mental component score; PCS = physical component score; n/a = not applicable.
Bolded values are those with statistical significance.
Use of theory
No studies used theory to explore or explain the effect of dance interventions in LTC.
Mechanisms of action
Two studies proposed mechanisms of action for how dance interventions could affect QoL (Adam et al., Reference Adam, Ramli and Shahar2016; Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023). In the first, the mechanism proposed was enjoyment (Adam et al., Reference Adam, Ramli and Shahar2016). In the second, it was proposed that the simultaneous engagement of sensory systems and physical, emotional, social, and cognitive functions would improve QoL (Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023). In addition, that dance promotes fun and feelings of connection (Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023). In both cases, the mechanisms were proposed in the introduction and discussion of the articles. Neither of these studies specifically measured whether the mechanisms of action, as related to the dance intervention, affected QoL.
Attendance and fidelity
Four of the seven studies measured intervention attendance rates. Specifically, rates were 92% (Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023), 84% (Kim et al., Reference Kim, June and Song2003), 92% (Song et al., Reference Song, June, Kim and Jeon2004), and 80% (Wang et al., Reference Wang, Yin, Meng, Shang, Meng, Zheng, Wang and Chen2020). Three studies (Chang, Zhu, et al., Reference Chang, Zhu, Zhang, Yong, Yang, Wang and Yan2021; Kim et al., Reference Kim, June and Song2003; Wang et al., Reference Wang, Yin, Meng, Shang, Meng, Zheng, Wang and Chen2020) attended to the fidelity of the intervention by having facilitators train participants in the dance movements, with two of these (Kim et al., Reference Kim, June and Song2003; Wang et al., Reference Wang, Yin, Meng, Shang, Meng, Zheng, Wang and Chen2020) going further by monitoring the necessary dance movements during the intervention.
Discussion
This review found that dance-based interventions have the potential to enhance QoL (inclusive of HRQoL) in older adults living in LTC, including those living with Alzheimer’s disease. Across the seven studies, most interventions yielded positive effects on condition-specific or general QoL outcomes, with improvements observed in mental well-being, physical functioning, and life satisfaction. Notably, condition-specific measures, such as the QoL in Alzheimer’s Disease Scale, were effective in capturing changes in populations with cognitive decline (Adam et al., Reference Adam, Ramli and Shahar2016; Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023), while general tools like the Short-Form-12 Health Survey and Life Satisfaction scales provided a broader assessment of well-being in older adults living in LTC. The overall quality of evidence among the included studies was variable. Although some studies demonstrated strong reporting practices and clear intervention descriptions, many exhibited methodological weaknesses, including small sample sizes, lack of randomization, and limited control of confounding variables.
The diversity and complexity of dance practices across studies present additional challenges. Variations in dance genres, movement types, music selection, and program structure were often under-reported, hindering both replication and comparison. Adherence to published dance-based intervention reporting standards is recommended for future research (Barnstaple et al., Reference Barnstaple, Laurita-Spanglet, Fanning, Soriano and Hugenschmidt2024). Five of the seven included studies utilized a dance intervention designed for a specific country or cultural group. Previous dance intervention studies have highlighted the importance of utilizing a dance form that is culturally relevant to participants, as dance provides a platform for socialization, cultural connection, and may encourage participation in individuals who might otherwise refrain from physical activity (Belza et al., Reference Belza, Walwick, Schwartz, LoGerfo, Shiu-Thornton and Taylor2004; Fonseca et al., Reference Fonseca, Rueda and Cabanzo2025; Lukach et al., Reference Lukach, Jedrziewski, Grove, Mechanic-Hamilton, Williams, Wollam and Erickson2016; Sofianidis et al., Reference Sofianidis, Hatzitaki, Douka and Grouios2009). Regardless of whether a dance form is designed for a country or cultural group, the issue of standardizing dance movements when designing dance interventions remains a challenge (Barnstaple et al., Reference Barnstaple, Laurita-Spanglet, Fanning, Soriano and Hugenschmidt2024). Future research in this area will need to examine how design and data collection challenges can effectively be managed, including the range of individual health status, participant capacity for consent, treatment preferences, and limited staff availability (Lam et al., Reference Lam, Chow, Taylor, Chow, Lam, Bonin, Rowbottom and Herrmann2018).
The findings of this review align with previous literature highlighting the potential benefits of non-pharmacologic interventions in improving QoL among older adults in LTC settings (Arias-Casais et al., Reference Arias-Casais, Amuthavalli Thiyagarajan, Rodrigues Perracini, Park, van den Block, Sumi, Sadana, Banerjee and Han2022). Further, dance-based interventions appear to promote multiple other outcomes in older adults, such as memory, cognition, anxiety, and depressive symptomatology (Salihu et al., Reference Salihu, Wong, Bello and Kwan2021; Tao et al., Reference Tao, Awan-Scully, Ash, Pei, Gu, Gao, Cole and Baker2023). However, dance may offer unique advantages by simultaneously integrating structured physical activity with psychological, cognitive, and social elements within a single intervention (Adam et al., Reference Adam, Ramli and Shahar2016; Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023; Kosmat & Vranic, Reference Kosmat and Vranic2017). The present findings align with previous systematic reviews on dance interventions in older adults that suggest dance may exert broader effects than just physical health outcomes, including across mental, emotional, and social dimensions of QoL (Fong Yan et al., Reference Fong Yan, Cobley, Chan, Pappas, Nicholson, Ward, Murdoch, Gu, Trevor, Vassallo, Wewege and Hiller2018, Reference Fong Yan, Nicholson, Ward, Hiller, Dovey, Parker, Low, Moyle and Chan2024; Salihu et al., Reference Salihu, Wong, Bello and Kwan2021; Tao et al., Reference Tao, Awan-Scully, Ash, Pei, Gu, Gao, Cole and Baker2023). Consequently, dance should be explored for its potential to support the physical, psychological, and social well-being of older adults living in LTC settings.
In our protocol, we proposed describing the cost of the dance interventions. However, none of the studies included in this review discussed the cost of the dance program. Understanding the direct (e.g., teaching time, equipment, music) and indirect (e.g., space rental) costs associated with the dance interventions is warranted when aiming to understand how feasible it is to operate dance interventions in LTC settings and how accessible the dance intervention is to older adults living in LTC. In future, it would be beneficial if the costs associated with the dance programs were disclosed as part of the research.
Across all included studies, the majority of participants were women and/or females, and two studies included only women/female participants. The trend towards more women/female participants aligns with the greater trend for increased dance participation by women/females/girls (Waugh et al., Reference Waugh, Yourdan, Casale, Balaban, Cross and Merom2024). As such, we are limited in our interpretation of findings when applying them to men/males. Plausible conclusions for the increased number of women/females in these studies could be that more women/females are living in LTC homes. For example, in Ontario, Canada, more than two-thirds of the residents are female (Ontario Health atHome, 2021). Another explanation could be due to sociocultural perspectives of dance, whereby in some cultures, dance is perceived to be an activity for girls, and thus not as accessible to boys (Oliver & Risner, Reference Oliver and Risner2017). Some dance choreographers and scholars have tried to ‘de-gender’ dance movements (Oliver & Risner, Reference Oliver and Risner2017), which might be a strategy to apply to dance interventions in LTC homes to increase men/male participation. Future research could explore how dance is perceived in relation to experiences of masculinity for older adults, including those living in LTC.
Among the included studies, none applied theory. There is increasing evidence to suggest that interventions developed with a theoretical foundation or framework are more effective than those lacking a theoretical base (Noar et al., Reference Noar, Benac and Harris2007). Although two studies (Adam et al., Reference Adam, Ramli and Shahar2016; Bracco et al., Reference Bracco, Cornaro, Pinto-Carral, Koch and Mourey2023) proposed potential mechanisms through which dance interventions might influence QoL, neither empirically tested these pathways. Consequently, this limits causal interpretations and the ability to validate theoretical assumptions. Understanding mechanisms is complex and requires dedicated approaches. Fancourt et al. (Reference Fancourt, Aughterson, Finn, Walker and Steptoe2021) reported 600 potential mechanisms, including biological, behavioural, psychological, and social processes across individual-, community-, and societal- levels that may influence how leisure-based interventions affect health and health behaviours; however, they did not measure the mechanisms. Examples of useful syntheses of mechanisms in arts-based interventions do exist (Dingle et al., Reference Dingle, Sharman, Bauer, Beckman, Broughton, Bunzli, Davidson, Draper, Fairley, Farrell, Flynn, Gomersall, Hong, Larwood, Lee, Lee, Nitschinsk, Peluso, Reedman and Wright2021). Many of the studies in our review stated the need for more research on mechanisms and an incomplete understanding of how dance interventions could facilitate QoL. Certainly, more dedicated attention needs to be paid to this area.
Implications for practice, policy, and future research
Dance can be a viable, adaptable intervention in LTC settings to support residents’ QoL. However, despite its promise, the current evidence is limited. Although one could argue that there is a need for larger, high-quality randomized controlled trials with standardized QoL outcomes, these more traditional approaches to improving study quality might not be feasible or even desired (Petts & McGill, Reference Petts and McGill2024). Like many arts-based interventions, the significant heterogeneity inherent in dance styles and approaches to teaching dance complicates standardization. The desire for choice when living in LTC and the (likely) need for multiple locations to meet sample size requirements make logistics and randomization a challenge. A developing argument is being made to consider alternative approaches to advancing dance research by integrating lived experiences in evaluation and employing more qualitative, co-creation, and mixed-methods approaches (Petts & McGill, Reference Petts and McGill2024).
Study limitations
This review was limited by the small number of available studies, many of which were of varying methodological quality. Few studies employed randomized controlled designs, and the frequent use of convenience samples introduced potential selection bias, limiting internal validity. As such, participants who elect to participate in optional dance classes or dance interventions within their LTC may have better mobility and a better mood state at onset, or may be motivated to improve their well-being or QoL through participation. The heterogeneity of intervention types, durations, and outcome measures further complicated comparisons and precluded formal meta-analysis. Consequently, the overall efficacy of dance interventions on QoL in LTC residents remains unknown. Additionally, there were some challenges in coming to a consensus on what measures constituted QoL, particularly for our patient partners. Using established definitions of QoL and HRQoL provided useful guidance, but there were times when a more robust approach to determining decisions regarding QoL measures would have been useful (Mayo, Reference Mayo2015; WHO, 1995).
Conclusion
Dance-based interventions show promise for improving QoL among residents of LTC facilities. However, significant variability in study design, intervention characteristics, and outcome measurement limits the ability to draw firm conclusions. More rigorous, theory-driven research is essential to better understand the role of dance in promoting holistic well-being in LTC settings and to inform effective dance program implementation.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0714980826100609.
Acknowledgements
We would like to acknowledge Sherrie Logan, who supported our patient partner team members in learning important skills on how to write a plain language summary. Sherrie’s generosity with her time and knowledge provided a valuable learning opportunity for our team. We thank Hoda Seens, Ph.D. (Western University, Canada), for the peer review of the submitted search strategy.
Competing interests
The authors declare none.




 Open access
Open access