Introduction
Tuberous sclerosis complex (TSC) is a rare, autosomal dominant genetic condition characterized by the presence of benign tumours (hamartomas) in multiple organs.Reference Northrup, Aronow and Bebin1 TSC is caused by pathogenic variants in the TSC1 or TSC2 genes, which encode for the proteins hamartin and tuberin, respectively. These pathogenic variants result in overactivation of the mechanistic target of rapamycin (mTOR) pathway.Reference Northrup, Aronow and Bebin1
Given the multisystemic nature of TSC, patients require coordinated care from multiple subspecialties, and TSC clinics are recommended.Reference Northrup, Aronow and Bebin1 Individuals with TSC often experience disrupted care delivery, and there may be barriers to completing surveillance tests, organizing care and transitioning.Reference Alsowat, Zak and McCoy2 TSC is also associated with increased healthcare utilization, costs and impacts on quality of life.Reference Northrup, Aronow and Bebin1 Herein, we describe the state of TSC care in Canada and explore existing challenges, as well as resources available for individuals with TSC and their caregivers. The views expressed in this paper are reflective of the opinion of TSC experts and advocates across Canada.
Methods
To better understand the status of TSC care delivery in Canada, a survey was distributed to Canadian TSC care providers to obtain the following information: the frequency of clinics, number of patients followed, subspeciality services/resources available and presence of a transition program.
TSC clinics in Canada
TSC clinics are an ideal resource for children and adults with TSC.Reference Northrup, Aronow and Bebin1 The care for people with TSC is generally best served in formal TSC clinics with a dedicated healthcare team. This allows for the development of clinical expertise and the local consolidation of additional resources. However, most people worldwide do not have access to specialized TSC clinics, and clinics can differ geographically. There are 11 TSC clinics in Canada (Table 2).
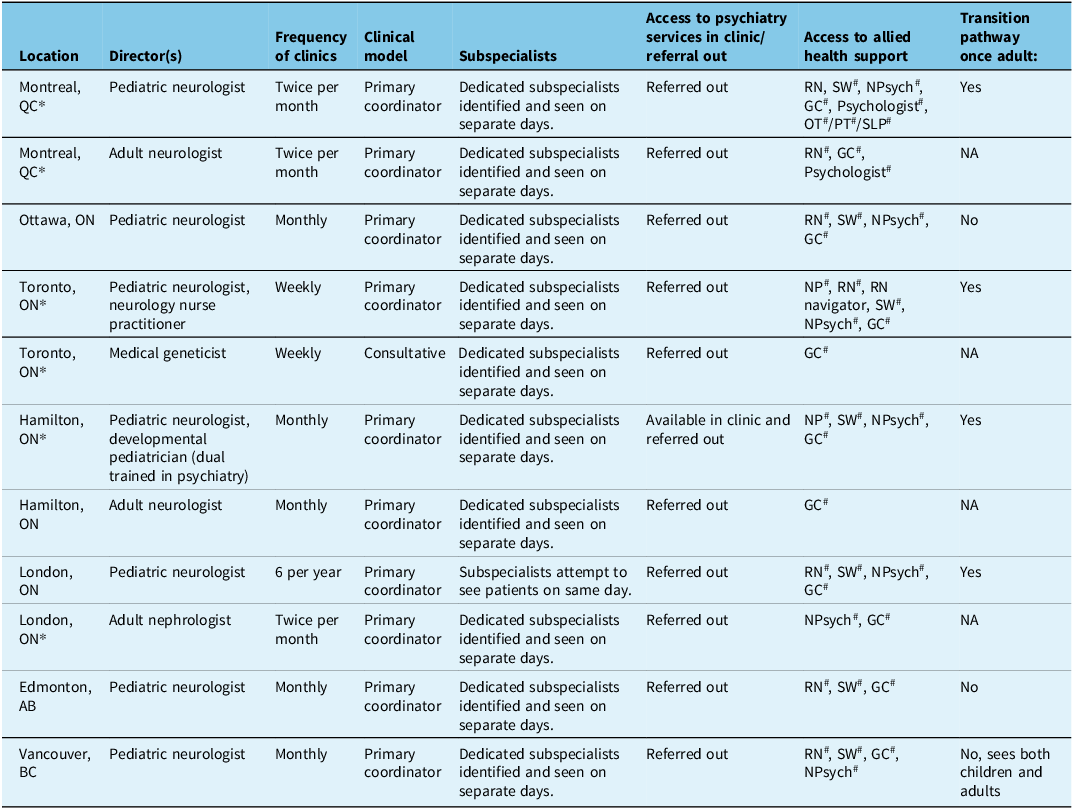
Table 2. Description of pediatric and adult TSC clinics in Canada
The TSC clinic structure varies depending on the location and resources available (Table 2). Most clinic directors are neurologists/epileptologists; however, some clinics are managed by nephrologists or geneticists. The TSC clinic typically acts as the primary healthcare coordinator, managing the screening for TSC manifestations and ensuring their initial and ongoing care. Clinics may also operate on a consultative basis where medical consultants carry out the screening tests. People with TSC are referred to TSC clinics by primary care providers, pediatricians or other specialists. The access to resources and support from nursing and other allied health professionals, such as social workers, genetic counselors and psychologists, is variable between clinics (Table 2). Only some pediatric TSC clinics have a standardized transition pathway.
How many Canadians are followed in TSC clinics?
The estimated live birth prevalence of TSC is approximately 1:10 000.Reference Northrup, Aronow and Bebin1 With a total Canadian population of 41 million people (https://www.statcan.gc.ca/en/subjects-start/population_and_demography), 7 million of whom are under 18 years of age, the number of people with TSC in Canada is approximately 4,100 (697 children and 2,993 adults). This is in contrast with the 807 patients (452 children and 355 adults), which are followed in the listed 11 TSC clinics in Canada (Table 2). We estimate that only 32% (807/4,100) of Canadians with TSC are followed at specialized TSC clinics (only 12% [355/2,993] of adults). Therefore, in Canada, the treatment gap (difference between clinical need and services provided) is 70% for the entire TSC population, and for adults, it is close to 90%.Reference de Vries, Whittemore and Leclezio4 However, a paucity of recent epidemiological studies in TSC may account for some of this discrepancy (i.e., difference between the expected number of individuals to have TSC based on epidemiological data and the number of individuals identified in Canada).
Multiple factors may explain why many patients with TSC are not followed in specialized TSC clinics. These include a lack of diagnosis, a mild phenotype and/or an absence of local resources. Nonetheless, these numbers clearly support the need for more referrals to specialized centres, especially in the adult population.
How optimal screening/treatment impacts morbidity, mortality and healthcare utilization in TSC
Optimal surveillance of potential multi-organ complications is essential in TSC as it helps to decrease morbidity, mortality and healthcare utilization.Reference Northrup, Aronow and Bebin1 Epilepsy affects 70–90% of individuals, the majority with onset in the first 2 years of life.Reference Northrup, Aronow and Bebin1,Reference Nabbout, Belousova and Benedik5 Screening electroencephalogram examinations for the detection of epileptiform abnormalities and pre-emptive treatment with vigabatrin may reduce the risk of developing infantile epileptic spasms as shown in the PREVeNT trial.Reference Northrup, Aronow and Bebin1,Reference Bebin, Peters and Porter6 Although preventative vigabatrin did not delay the onset of drug-resistant epilepsy or improve neurodevelopmental outcomes in the PREVeNT trial, improvement in the overall care of people with TSC through novel research studies such as PREVeNT may improve overall health outcomes.Reference Bebin, Peters and Porter6 TAND are very common and encompass autism spectrum disorder (ASD), intellectual disability, mood disorders and attention deficit hyperactivity disorder. Early diagnosis of TAND facilitates early intervention and puts in place school supports that can improve the overall quality of life of the child and caregivers.Reference Northrup, Aronow and Bebin1,Reference de Vries, Heunis and Vanclooster3
Targeted therapy with mTOR inhibitors is effective for the treatment of subependymal giant cell astrocytomas (SEGAs), drug-resistant epilepsy, angiomyolipomas (AMLs), lymphangioleiomyomatosis (LAM) and facial angiofibroma.Reference Northrup, Aronow and Bebin1 SEGAs may lead to hydrocephalus requiring neurosurgical intervention, which can be avoided with early detection. Early treatment with an mTOR inhibitor can prevent growth or may shrink SEGAs. Early detection of enlarging AMLs and initiation of an mTOR inhibitor may prevent nephrectomy, hemorrhage and renal failure. Early identification of LAM may prevent deterioration in lung function.
Current challenges and gaps in TSC care in Canada
Internationally, a significant gap has been identified between TSC surveillance guidelines and what is actually available to individuals with TSC worldwide.Reference Stuart, Fladrowski and Flinn7 Key priorities to improve the gaps in care are (1) improved access to TSC expertise, (2) coordinated and integrated care and (3) implementation of the guidelines.Reference Stuart, Fladrowski and Flinn7 In Canada, there are similar challenges (Table 3), which include, but are not limited to, transition of children with TSC to adulthood (i.e., healthcare, occupational, social transitions, etc.) (action items 1 and 2), resources for TAND and mTOR inhibitor access/access to novel therapies (action items 1 and 3) and as discussed access to TSC clinics (action items 1 and 3).Reference Stuart, Fladrowski and Flinn7
Table 3. Summary of selected current gaps in TSC care and actions required
Transition
The transition period, generally defined as extending from age 12 to 21 years, can be difficult for people with TSC and their families. Difficulties related to transition include concerns regarding sexual health and family planning and social issues such as education, finding employment, obtaining a driver’s permit, navigating financial supports and transition to residential care for some.Reference Andrade, Bassett and Bercovici8 Given that most individuals with TSC have TAND and neurodevelopmental disorders and mental health challenges are common, transition programs should be adapted to the particular needs of patients and their caregivers and may need to start later and occur more slowly. A successful transition program extends across this transition period and helps provide patients and their families with the tools to allow them to attain their full potential and in turn lead to optimal quality of life.Reference Andrade, Bassett and Bercovici8 Transitions in rare diseases and developmental disabilities are often hindered by variability in care systems and policies, leading to fragmented support and delays. Unified transition models, developed with key stakeholders, are essential to ensure coordinated and comprehensive care for individuals, particularly in specialized areas like TSC.
A healthcare transition program for young people with TSC may overlap with local epilepsy clinic transition programs. Such transition programs may be organized in various ways. They may involve personalized teaching, often carried out by a nurse. In-person and online information sessions, addressing the needs of patients and their families, are a means of reaching a wider audience while requiring fewer resources. There are many social resources available (e.g., job training programs) to patients, and an organized transition program can ensure that patients are made aware of these. Transition readiness checklists are an efficient means to assess a person’s knowledge of issues relevant to young adulthood with a chronic condition. There are epilepsy-specific checklists that are recommended for any patient approaching the age of majority.Reference Andrade, Bassett and Bercovici8 Some centres have different transition programs for individuals who will be managing their own care versus those who will require substantial support from caregivers.
Access to TAND services
TAND affect 90% of individuals with TSC during their lifetime.Reference de Vries, Heunis and Vanclooster3–Reference de Vries, Whittemore and Leclezio4 These manifestations are categorized into six levels: behavioural, psychiatric, intellectual, academic, neuropsychological and psychosocial aspects.Reference de Vries, Whittemore and Leclezio4 Although distinct, these levels do not occur in isolation and tend to naturally group into seven “clusters,” reflecting the complexity of individual TAND profiles.Reference de Vries, Whittemore and Leclezio4 Among TSC clinics in Canada, there is variable access to TAND professionals, such as psychologists and social workers (Table 2). Individuals requiring assessment from psychiatry are referred to mental health services on a consultative basis. Moreover, individuals requiring therapies, such as occupational therapy, physiotherapy and speech and language therapy, are referred to local rehabilitation centres.
TAND manifestations are under-assessed/treated and under-researched. Several gaps in the delivery of care for TAND have been identified, which apply to Canada and internationally, as summarized below Reference Vanclooster, Bissell and van Eeghen9:
-
1. Under identification/assessment: Despite the prevalence of TAND, healthcare providers often overlook its impact, with fewer than 20% of patients receiving assessment or treatment.Reference de Vries, Whittemore and Leclezio4,Reference Vanclooster, Bissell and van Eeghen9 In Canada, this number is unknown.
-
2. Under treatment: TSC clinics in Canada have variable resources to help address TAND (Table 2), and wait times for neuropsychological/psychiatric services are often long (i.e., >12–24 months). Access to psychiatry services in TSC clinics is limited (Table 2). Only some clinics have access to neuropsychological testing (Table 2), testing through school boards is limited by long wait lists, and private evaluations are costly for families. Non-pharmacological interventions are limited, and remote interventions (i.e., tele-consultations, virtual care) are underutilized.Reference Vanclooster, Bissell and van Eeghen9
-
3. Cluster-specific gaps: Although the ASD–like cluster is well-researched, other clusters (such as scholastic difficulties) receive less attention. This imbalance leaves clinicians less equipped to manage the less-studied clusters.Reference Vanclooster, Bissell and van Eeghen9
-
4. Geographic disparities: Clinical and research TSC sites are predominantly located in high-income countries. This lack of representation from low- and middle-income countries hinders global efforts to improve TAND care.Reference Vanclooster, Bissell and van Eeghen9 In Canada, geographic disparities exist, and there are no TSC clinics located in Northern and/or remote communities. Indigenous people who may live in the most remote/underserved areas are most affected by these disparities.
-
5. Lack of research: While TAND research has increased, more studies are needed across the lifespan, particularly for adults who are currently underrepresented.Reference Vanclooster, Bissell and van Eeghen9
To bridge these gaps in Canada, it is essential to invest in provider education, engage patients through educational programs and prioritize TAND research across the lifespan.
mTOR inhibitor access
Reimbursement programs for mTOR inhibitors exist for TSC-related AML and SEGA, but not for the other manifestations of TSC (e.g., epilepsy, facial angiofibroma, LAM). These programs are variably accessible across Canada, leading to disparities in the care of individuals with TSC. mTOR inhibitors are costly ($172 Canadian dollars per day). In many provinces and territories, the cost of everolimus and sirolimus must be assumed by the patient or by private insurance. Public reimbursement is available in some locations, such as Ontario and Quebec, but not in others (e.g., Manitoba, Newfoundland). In Ontario, everolimus for AML is reimbursed if patients have coalescent/multifocal AMLs, show progression despite previous embolization/surgery and have documented clinical rationale against further invasive procedures. Reimbursement criteria for SEGA in Ontario state that surgical resection must be unfeasible due to the tumour’s characteristics or complications from previous surgeries. Initial approvals in Ontario are for one year, with renewals conditional upon tumour-response criteria. In Quebec, everolimus is reimbursed for those covered by the public drug coverage plan available to all residents. Accepted indications are renal AML that are at least 3 cm in diameter, a SEGA at least 1 cm and growing and drug-resistant epilepsy. Renewals in Quebec are required every 3–6 months.
Community resources
Given its multisystemic nature and need for lifelong surveillance, it is important that individuals with TSC and their caregivers are supported. In Canada, Tuberous Sclerosis Canada Sclérose Tubéreuse (TSCST) is a nonprofit, charitable organization that provides support and awareness for individuals with TSC and their caregivers, while also promoting research and educational initiatives. The TSC Alliance is a US-based but internationally recognized nonprofit organization that similarly provides support and advocacy for individuals living with TSC and their families and helps to drive TSC research. Both TSCST and the TSC Alliance aim to improve access and quality of care for individuals living with TSC. In Ontario, the Ontario TSC Network is a provincial entity composed of healthcare providers dedicated to improving the quality of life of children and adults. In collaboration with TSC Canada and colleagues at the Université de Montréal healthcare network, this initiative has created an educational series for individuals with TSC and their caregivers.





 You have
Access
You have
Access
Introduction
Tuberous sclerosis complex (TSC) is a rare, autosomal dominant genetic condition characterized by the presence of benign tumours (hamartomas) in multiple organs.Reference Northrup, Aronow and Bebin1 TSC is caused by pathogenic variants in the TSC1 or TSC2 genes, which encode for the proteins hamartin and tuberin, respectively. These pathogenic variants result in overactivation of the mechanistic target of rapamycin (mTOR) pathway.Reference Northrup, Aronow and Bebin1
Given the multisystemic nature of TSC, patients require coordinated care from multiple subspecialties, and TSC clinics are recommended.Reference Northrup, Aronow and Bebin1 Individuals with TSC often experience disrupted care delivery, and there may be barriers to completing surveillance tests, organizing care and transitioning.Reference Alsowat, Zak and McCoy2 TSC is also associated with increased healthcare utilization, costs and impacts on quality of life.Reference Northrup, Aronow and Bebin1 Herein, we describe the state of TSC care in Canada and explore existing challenges, as well as resources available for individuals with TSC and their caregivers. The views expressed in this paper are reflective of the opinion of TSC experts and advocates across Canada.
Methods
To better understand the status of TSC care delivery in Canada, a survey was distributed to Canadian TSC care providers to obtain the following information: the frequency of clinics, number of patients followed, subspeciality services/resources available and presence of a transition program.
Current TSC surveillance and management recommendations
International recommendations exist for the diagnosis and management of TSC and are followed by TSC clinics in Canada that receive official recognition by the TSC Alliance (Table 1).Reference Northrup, Aronow and Bebin1 The TAND Consortium has also published consensus recommendations for the identification and treatment of TSC-associated neuropsychiatric disorders (TAND).Reference de Vries, Heunis and Vanclooster3–Reference de Vries, Whittemore and Leclezio4 These recommendations emphasize the importance of regular monitoring, early intervention and the need for a multidisciplinary approach to care.Reference Northrup, Aronow and Bebin1,Reference de Vries, Heunis and Vanclooster3–Reference de Vries, Whittemore and Leclezio4
Table 1. Summary of current TSC surveillance and treatment recommendations [1]
Note: Table summarizing the Updated International TSC Diagnostic Criteria and Surveillance and Management Recommendations [1]. ACTH = adrenocorticotropic hormone; DRE = drug-resistant epilepsy; ECG = electrocardiogram; ECHO = echocardiogram; EEG = electroencephalogram; FEV1 = forced expiratory volume in one-second; GFR = glomerular filtration rate; LAM = lymphangiomyomatosis; mTORi = mechanistic target of rapamycin inhibitor; PFT = pulmonary function test; SEGA = subependymal giant cell astrocytoma; TSC = tuberous sclerosis complex; TAND = TSC-associated neuropsychiatric disorders; 6MWT = six-minute walk test.
TSC clinics in Canada
TSC clinics are an ideal resource for children and adults with TSC.Reference Northrup, Aronow and Bebin1 The care for people with TSC is generally best served in formal TSC clinics with a dedicated healthcare team. This allows for the development of clinical expertise and the local consolidation of additional resources. However, most people worldwide do not have access to specialized TSC clinics, and clinics can differ geographically. There are 11 TSC clinics in Canada (Table 2).
Table 2. Description of pediatric and adult TSC clinics in Canada
Note: AB = Alberta; BC = British Columbia; GC = genetic counselor; NA = not applicable; NP = nurse practitioner; NPsych = neuropsychologist; ON = Ontario; RN = registered nurse; SW = social worker; TSC = tuberous sclerosis complex.
*TSC clinics recognized by the TSC Alliance; # indicates that allied health have other roles outside the TSC clinic and are not only working in the TSC clinic.
The TSC clinic structure varies depending on the location and resources available (Table 2). Most clinic directors are neurologists/epileptologists; however, some clinics are managed by nephrologists or geneticists. The TSC clinic typically acts as the primary healthcare coordinator, managing the screening for TSC manifestations and ensuring their initial and ongoing care. Clinics may also operate on a consultative basis where medical consultants carry out the screening tests. People with TSC are referred to TSC clinics by primary care providers, pediatricians or other specialists. The access to resources and support from nursing and other allied health professionals, such as social workers, genetic counselors and psychologists, is variable between clinics (Table 2). Only some pediatric TSC clinics have a standardized transition pathway.
How many Canadians are followed in TSC clinics?
The estimated live birth prevalence of TSC is approximately 1:10 000.Reference Northrup, Aronow and Bebin1 With a total Canadian population of 41 million people (https://www.statcan.gc.ca/en/subjects-start/population_and_demography), 7 million of whom are under 18 years of age, the number of people with TSC in Canada is approximately 4,100 (697 children and 2,993 adults). This is in contrast with the 807 patients (452 children and 355 adults), which are followed in the listed 11 TSC clinics in Canada (Table 2). We estimate that only 32% (807/4,100) of Canadians with TSC are followed at specialized TSC clinics (only 12% [355/2,993] of adults). Therefore, in Canada, the treatment gap (difference between clinical need and services provided) is 70% for the entire TSC population, and for adults, it is close to 90%.Reference de Vries, Whittemore and Leclezio4 However, a paucity of recent epidemiological studies in TSC may account for some of this discrepancy (i.e., difference between the expected number of individuals to have TSC based on epidemiological data and the number of individuals identified in Canada).
Multiple factors may explain why many patients with TSC are not followed in specialized TSC clinics. These include a lack of diagnosis, a mild phenotype and/or an absence of local resources. Nonetheless, these numbers clearly support the need for more referrals to specialized centres, especially in the adult population.
How optimal screening/treatment impacts morbidity, mortality and healthcare utilization in TSC
Optimal surveillance of potential multi-organ complications is essential in TSC as it helps to decrease morbidity, mortality and healthcare utilization.Reference Northrup, Aronow and Bebin1 Epilepsy affects 70–90% of individuals, the majority with onset in the first 2 years of life.Reference Northrup, Aronow and Bebin1,Reference Nabbout, Belousova and Benedik5 Screening electroencephalogram examinations for the detection of epileptiform abnormalities and pre-emptive treatment with vigabatrin may reduce the risk of developing infantile epileptic spasms as shown in the PREVeNT trial.Reference Northrup, Aronow and Bebin1,Reference Bebin, Peters and Porter6 Although preventative vigabatrin did not delay the onset of drug-resistant epilepsy or improve neurodevelopmental outcomes in the PREVeNT trial, improvement in the overall care of people with TSC through novel research studies such as PREVeNT may improve overall health outcomes.Reference Bebin, Peters and Porter6 TAND are very common and encompass autism spectrum disorder (ASD), intellectual disability, mood disorders and attention deficit hyperactivity disorder. Early diagnosis of TAND facilitates early intervention and puts in place school supports that can improve the overall quality of life of the child and caregivers.Reference Northrup, Aronow and Bebin1,Reference de Vries, Heunis and Vanclooster3
Targeted therapy with mTOR inhibitors is effective for the treatment of subependymal giant cell astrocytomas (SEGAs), drug-resistant epilepsy, angiomyolipomas (AMLs), lymphangioleiomyomatosis (LAM) and facial angiofibroma.Reference Northrup, Aronow and Bebin1 SEGAs may lead to hydrocephalus requiring neurosurgical intervention, which can be avoided with early detection. Early treatment with an mTOR inhibitor can prevent growth or may shrink SEGAs. Early detection of enlarging AMLs and initiation of an mTOR inhibitor may prevent nephrectomy, hemorrhage and renal failure. Early identification of LAM may prevent deterioration in lung function.
Current challenges and gaps in TSC care in Canada
Internationally, a significant gap has been identified between TSC surveillance guidelines and what is actually available to individuals with TSC worldwide.Reference Stuart, Fladrowski and Flinn7 Key priorities to improve the gaps in care are (1) improved access to TSC expertise, (2) coordinated and integrated care and (3) implementation of the guidelines.Reference Stuart, Fladrowski and Flinn7 In Canada, there are similar challenges (Table 3), which include, but are not limited to, transition of children with TSC to adulthood (i.e., healthcare, occupational, social transitions, etc.) (action items 1 and 2), resources for TAND and mTOR inhibitor access/access to novel therapies (action items 1 and 3) and as discussed access to TSC clinics (action items 1 and 3).Reference Stuart, Fladrowski and Flinn7
Table 3. Summary of selected current gaps in TSC care and actions required
Note: CADTH = Canadian Agency for Drugs and Technologies in Health; ECHO = Extensions for Community Healthcare Outcomes; TSC = tuberous sclerosis complex.
Transition
The transition period, generally defined as extending from age 12 to 21 years, can be difficult for people with TSC and their families. Difficulties related to transition include concerns regarding sexual health and family planning and social issues such as education, finding employment, obtaining a driver’s permit, navigating financial supports and transition to residential care for some.Reference Andrade, Bassett and Bercovici8 Given that most individuals with TSC have TAND and neurodevelopmental disorders and mental health challenges are common, transition programs should be adapted to the particular needs of patients and their caregivers and may need to start later and occur more slowly. A successful transition program extends across this transition period and helps provide patients and their families with the tools to allow them to attain their full potential and in turn lead to optimal quality of life.Reference Andrade, Bassett and Bercovici8 Transitions in rare diseases and developmental disabilities are often hindered by variability in care systems and policies, leading to fragmented support and delays. Unified transition models, developed with key stakeholders, are essential to ensure coordinated and comprehensive care for individuals, particularly in specialized areas like TSC.
A healthcare transition program for young people with TSC may overlap with local epilepsy clinic transition programs. Such transition programs may be organized in various ways. They may involve personalized teaching, often carried out by a nurse. In-person and online information sessions, addressing the needs of patients and their families, are a means of reaching a wider audience while requiring fewer resources. There are many social resources available (e.g., job training programs) to patients, and an organized transition program can ensure that patients are made aware of these. Transition readiness checklists are an efficient means to assess a person’s knowledge of issues relevant to young adulthood with a chronic condition. There are epilepsy-specific checklists that are recommended for any patient approaching the age of majority.Reference Andrade, Bassett and Bercovici8 Some centres have different transition programs for individuals who will be managing their own care versus those who will require substantial support from caregivers.
Access to TAND services
TAND affect 90% of individuals with TSC during their lifetime.Reference de Vries, Heunis and Vanclooster3–Reference de Vries, Whittemore and Leclezio4 These manifestations are categorized into six levels: behavioural, psychiatric, intellectual, academic, neuropsychological and psychosocial aspects.Reference de Vries, Whittemore and Leclezio4 Although distinct, these levels do not occur in isolation and tend to naturally group into seven “clusters,” reflecting the complexity of individual TAND profiles.Reference de Vries, Whittemore and Leclezio4 Among TSC clinics in Canada, there is variable access to TAND professionals, such as psychologists and social workers (Table 2). Individuals requiring assessment from psychiatry are referred to mental health services on a consultative basis. Moreover, individuals requiring therapies, such as occupational therapy, physiotherapy and speech and language therapy, are referred to local rehabilitation centres.
TAND manifestations are under-assessed/treated and under-researched. Several gaps in the delivery of care for TAND have been identified, which apply to Canada and internationally, as summarized below Reference Vanclooster, Bissell and van Eeghen9:
1. Under identification/assessment: Despite the prevalence of TAND, healthcare providers often overlook its impact, with fewer than 20% of patients receiving assessment or treatment.Reference de Vries, Whittemore and Leclezio4,Reference Vanclooster, Bissell and van Eeghen9 In Canada, this number is unknown.
2. Under treatment: TSC clinics in Canada have variable resources to help address TAND (Table 2), and wait times for neuropsychological/psychiatric services are often long (i.e., >12–24 months). Access to psychiatry services in TSC clinics is limited (Table 2). Only some clinics have access to neuropsychological testing (Table 2), testing through school boards is limited by long wait lists, and private evaluations are costly for families. Non-pharmacological interventions are limited, and remote interventions (i.e., tele-consultations, virtual care) are underutilized.Reference Vanclooster, Bissell and van Eeghen9
3. Cluster-specific gaps: Although the ASD–like cluster is well-researched, other clusters (such as scholastic difficulties) receive less attention. This imbalance leaves clinicians less equipped to manage the less-studied clusters.Reference Vanclooster, Bissell and van Eeghen9
4. Geographic disparities: Clinical and research TSC sites are predominantly located in high-income countries. This lack of representation from low- and middle-income countries hinders global efforts to improve TAND care.Reference Vanclooster, Bissell and van Eeghen9 In Canada, geographic disparities exist, and there are no TSC clinics located in Northern and/or remote communities. Indigenous people who may live in the most remote/underserved areas are most affected by these disparities.
5. Lack of research: While TAND research has increased, more studies are needed across the lifespan, particularly for adults who are currently underrepresented.Reference Vanclooster, Bissell and van Eeghen9
To bridge these gaps in Canada, it is essential to invest in provider education, engage patients through educational programs and prioritize TAND research across the lifespan.
mTOR inhibitor access
Reimbursement programs for mTOR inhibitors exist for TSC-related AML and SEGA, but not for the other manifestations of TSC (e.g., epilepsy, facial angiofibroma, LAM). These programs are variably accessible across Canada, leading to disparities in the care of individuals with TSC. mTOR inhibitors are costly ($172 Canadian dollars per day). In many provinces and territories, the cost of everolimus and sirolimus must be assumed by the patient or by private insurance. Public reimbursement is available in some locations, such as Ontario and Quebec, but not in others (e.g., Manitoba, Newfoundland). In Ontario, everolimus for AML is reimbursed if patients have coalescent/multifocal AMLs, show progression despite previous embolization/surgery and have documented clinical rationale against further invasive procedures. Reimbursement criteria for SEGA in Ontario state that surgical resection must be unfeasible due to the tumour’s characteristics or complications from previous surgeries. Initial approvals in Ontario are for one year, with renewals conditional upon tumour-response criteria. In Quebec, everolimus is reimbursed for those covered by the public drug coverage plan available to all residents. Accepted indications are renal AML that are at least 3 cm in diameter, a SEGA at least 1 cm and growing and drug-resistant epilepsy. Renewals in Quebec are required every 3–6 months.
Community resources
Given its multisystemic nature and need for lifelong surveillance, it is important that individuals with TSC and their caregivers are supported. In Canada, Tuberous Sclerosis Canada Sclérose Tubéreuse (TSCST) is a nonprofit, charitable organization that provides support and awareness for individuals with TSC and their caregivers, while also promoting research and educational initiatives. The TSC Alliance is a US-based but internationally recognized nonprofit organization that similarly provides support and advocacy for individuals living with TSC and their families and helps to drive TSC research. Both TSCST and the TSC Alliance aim to improve access and quality of care for individuals living with TSC. In Ontario, the Ontario TSC Network is a provincial entity composed of healthcare providers dedicated to improving the quality of life of children and adults. In collaboration with TSC Canada and colleagues at the Université de Montréal healthcare network, this initiative has created an educational series for individuals with TSC and their caregivers.
Conclusion
Important strides have been made in the care of individuals with TSC in Canada with the development of several TSC clinics nationally. Our data suggest, however, that the majority of Canadian patients with TSC are not followed in a dedicated TSC clinic, and there is a significant treatment gap (for adults, close to 90%). There are persistent challenges related to transition, access to mTOR inhibitors and management of TAND. A national effort is required to improve and standardize access to care, treatments and resources for individuals with TSC and their caregivers in Canada (Table 3). Furthermore, a more systematic collection of data in the future will enable our group to better understand the care needs of individuals with TSC across Canada.
Acknowledgments
We would like to thank the TSC families who have inspired and supported our work.
Author contributions
RW, MNN, LS, AVA, MBC, EJD, CE, JF, AAH, RHK, CK, PhMa, PaMa, KM,, ASM, ET, MV, CW, MZ and MRK contributed to the planning of the article, writing of the original draft (divided into sections) and revising the final draft.
Funding statement
There are no funding sources to declare. We affirm that we have read the journal’s policies on ethical publishing.
Competing interests
Robyn Whitney: RW received consulting fees from Jazz Pharmaceuticals and Takeda Pharmaceuticals.
Maryam Nabavi Nouri: MNN received consulting fees from Jazz Pharmaceuticals.
Lauren Sham: No disclosures.
Andrea V Andrade: AVA received consulting and speaker fees from Jazz Pharmaceuticals.
Mary B. Connolly: MBC received consulting fees from Jazz Pharmaceuticals and UCB. Research grant from Dravet Syndrome Foundation, NIH, CIHR, SickKids Foundation and BC Children’s Hospital Research Institute. Site PI or Co-PI on studies in drug-resistant epilepsy from Xenon Pharmaceuticals Inc., Zogenix International Inc., Eisai Inc., Epygenix Therapeutics Inc., Takeda Pharmaceuticals Inc., Marinus Pharmaceuticals Inc. Grin Therapeutics Inc. and Jazz Pharmaceuticals Inc.
Elizabeth J Donner: ED received consulting fees from Jazz Pharmaceuticals, Takeda and UCB.
Cathy Evanochko: CW received honoraria from Jazz Pharmaceuticals.
Jennifer Flinn: No disclosures.
Andrew A. House: AAH received consulting fees from Baxter Canada, AstraZeneca Canada and Paladin Labs Inc.
Raymond H. Kim: No disclosures.
Christine Kowal: No disclosures.
Philippe Major: PM received consulting fees from Eisai, UCB and Jazz Pharmaceuticals.
Paula Marques: PM received consulting fees from Jazz Pharmaceuticals.
Katherine Muir: KM received consulting fees from Jazz Pharmaceuticals.
Ana Suller Marti: ASM received consulting fees from Jazz Pharmaceuticals and Paladin.
Elisabetta Trinari: No disclosures.
Mila Valcic: No disclosures.
Colin Wilbur: No disclosures.
Maria Zak: No disclosures.
Mark Keezer: MK reports unrestricted educational grants from UCB, Eisai, Jazz Pharmaceuticals and Paladin, as well as research grants for investigator-initiated studies from UCB and Eisai.