


Introduction
Generally, a rise in the prevalence of common mental disorders (mood, anxiety, and substance use disorders) in the general population has been suggested in the past decade [Reference Grant, Chou, Saha, Pickering, Kerridge and Ruan1–Reference Slade, Vescovi, Chapman, Teesson, Arya and Pirkis7], although not always consistently for each disorder category [Reference Dobson, Vigod, Mustard and Smith6, Reference Slade, Vescovi, Chapman, Teesson, Arya and Pirkis7]. Recently, we confirmed an increase in 12-month prevalence of common mental disorders between 2007–2009 and 2019–2022 in the Netherlands, from 17.4 to 26.1%, as well as a rise in the prevalence of all main categories of common mental disorders [Reference ten Have, Tuithof, van Dorsselaer, Schouten, Luik and de Graaf8]. It is uncertain whether the observed rise in prevalence can, at least partly, be explained by a similar rise in the first incidence of these disorders. Findings of registration studies suggest this is the case, as they show a rise in health care use for people with incident depressive and anxiety disorders [Reference Momen, Beck, Lousdal, Agerbo, McGrath and Pedersen9–Reference Walrave, Beerten, Mamouris, Coteur, Van Nuland and Van Pottelbergh11], but this could also be due to changes in the health care system, such as improved accessibility or capacity of care.
Prospective studies in the general population are needed to examine the first incidence of disorders, but such studies are resource-intensive and scarce [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference de Graaf, ten Have, Tuithof and van Dorsselaer13]. The most recent prospective studies examining incidence rates of mental disorders in the general population observed a depression incidence varying from 1.52 to 2.05 cases per 100 person-years [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12–Reference Lehtinen, Sohlman, Nummelin, Salomaa, Ayuso-Mateos and Dowrick14]. For anxiety disorders, these rates range from 1.58 to 1.69 [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference de Graaf, ten Have, Tuithof and van Dorsselaer13]. For any substance use disorder, incidence is estimated at 0.97 [Reference de Graaf, ten Have, Tuithof and van Dorsselaer13] and at 1.66 for alcohol use disorder and 0.31 for drug use disorder separately [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12]. However, these prospective studies were performed more than a decade ago and thus predate the studies indicating a rise in the prevalence of mental disorders. Therefore, it remains unclear whether the incidence rates have actually increased as well.
Of the three above-mentioned prospective studies examining incidence rates, only two had a sufficient sample size to adequately examine determinants of incident common mental disorders. Their findings indicated that women have a higher incidence of mood and anxiety disorders, while men have a higher incidence of substance use disorders. Also, younger age was related to higher incidence rates than older age [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference de Graaf, ten Have, Tuithof and van Dorsselaer13]. Changes in sociodemographics, like no longer living with a partner and loss of a paid job, appeared to be stronger determinants than the corresponding sociodemographics [Reference de Graaf, ten Have, Tuithof and van Dorsselaer13]. Furthermore, these studies showed that it is important to study the association with prior other mental disorders, because incident disorders are often secondary [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference de Graaf, ten Have, Tuithof and van Dorsselaer13]. Determining whether these relationships can be replicated today is important, as it may help to target general prevention as well as prevention of psychiatric comorbidity.
Recent population-based findings on incidence rates and associated determinants are thus lacking, but registration studies have looked at the relationship over time between incidence rates and different subgroups. Specifically, a steeper increase in health care use by people with incident depressive and/or anxiety disorders was seen in the most deprived quintiles [Reference Dykxhoorn, Osborn, Walters, Kirkbride, Gnani and Lazzarino10] and among young adults [Reference Momen, Beck, Lousdal, Agerbo, McGrath and Pedersen9–Reference Walrave, Beerten, Mamouris, Coteur, Van Nuland and Van Pottelbergh11]. This latter finding is in accordance with the observed steeper increase in prevalence rate of a common mental disorder for younger adults in the general population [Reference ten Have, Tuithof, van Dorsselaer, Schouten, Luik and de Graaf8]. That prevalence study also showed a steeper increase for students compared to those with a paid job, and for those living in a city compared to nonurban residents. By examining whether changes in incidence rates over time are similar for different sociodemographic groups, insight can be gained into groups that have become more or less vulnerable over the past decade.
Aims of this article
In this article, we present incidence rates of DSM-5 mood, anxiety, and substance use disorders based on data from the third Netherlands Mental Health Survey and Incidence Study (NEMESIS-3). NEMESIS-3 is a population-based cohort of the Dutch general population aged 18–75 years, designed to provide up-to-date information on the prevalence and incidence of mental disorders in the general population. The associations of sociodemographic and mental health variables with the incidence will be examined to determine vulnerable groups.
Additionally, we assess changes over time in disorder incidence by comparing the DSM-IV incidence rates between the first two waves of NEMESIS-3 (i.e., wave 1 in 2019–2022 and wave 2 in 2023–2024) with those of NEMESIS-2 (i.e., wave 1 in 2007–2009 and wave 2 in 2010–2012), and to what extent these changes were similar for different sociodemographic groups.
Methods
Study design
We used a multistage, stratified random sampling procedure for NEMESIS. First, a random sample of municipalities was drawn for both studies. Second, in NEMESIS-3 [Reference ten Have, Tuithof, van Dorsselaer, Schouten and de Graaf15], a random sample of individuals aged 18–75 years was drawn from the Dutch population register (Basisregistratie Personen; BRP). In NEMESIS-2 [Reference de Graaf, ten Have and van Dorsselaer16], a random sample of addresses of private households from postal registers was drawn. Next, a random individual aged 18–64 years was selected to be asked to participate, based on the most recent birthday at first contact within the household. In both studies, individuals with insufficient command of the Dutch language, as well as institutionalized individuals (i.e., those living in hostels, hospices, or prisons), were excluded. Individuals temporarily living in institutions were contacted to be interviewed after returning home.
For NEMESIS-3, the Medical Research Ethics Committee (METC Utrecht) stated that the Dutch Medical Research Involving Human Subjects Act (WMO) did not apply (reference number WAG/mb/19/017126, 15 May 2019). Therefore, no official approval was required under the WMO. The field procedures, information for respondents, and informed consent forms were assessed positively by the local Ethical Review Committee. NEMESIS-2 was approved by a medical ethics committee (the Medical Ethics Review Committee for Institutions on Mental Health Care, METiGG: reference number CCMO nr. NL18210.097.07) since it included saliva collection. In both studies, respondents provided written informed consent at each wave after receiving comprehensive written and verbal information about the study procedures.
Fieldwork
In NEMESIS-3, the baseline wave was performed from November 2019 to March 2022 (response rate 54.6%). Of the 6,194 respondents, 59 were deceased and, therefore, 6,135 were approached for follow-up ~3 years after baseline (January 2023 to November 2024). Of those, 4,688 (76.4%) were interviewed again (mean period between both interviews: 2 years and 310 days; mean interview duration: 76 minutes). Any mental disorder and any mood disorder in the 12 months before baseline were significantly associated with attrition at first follow-up, after controlling for sociodemographic characteristics [Reference ten Have, Tuithof, van Dorsselaer, Korteling and Luik17].
In NEMESIS-2, the baseline wave was performed from November 2007 to July 2009 (response rate 65.1%). Of the 6,646 respondents, 50 were deceased and, therefore, 6,596 were approached for follow-up ~3 years after baseline (November 2010 to July 2012). Of those, 5,303 (80.4%) were interviewed again (mean period between both interviews: 3 years and 7 days; mean interview duration: 84 minutes). No significant association was found between 12-month mental disorders at baseline and attrition at follow-up after controlling for sociodemographics [Reference de Graaf, van Dorsselaer, Tuithof and ten Have18].
To allow generalization of the data to the Dutch population at baseline, a weighting factor was constructed for each study, adjusting for selective nonresponse at baseline and attrition at follow-up. After weighting, the distribution of the sociodemographic characteristics at baseline of those who participated in the second wave came very close to that of the Dutch population at baseline [Reference ten Have, Tuithof, van Dorsselaer, Korteling and Luik17, Reference de Graaf, van Dorsselaer, Tuithof and ten Have18].
Diagnostic interview
The Composite International Diagnostic Interview (CIDI) 3.0 was used to ascertain DSM diagnoses of mood disorders (i.e., major depressive disorder, persistent depressive disorder/dysthymia and bipolar disorder); anxiety disorders (i.e., panic disorder, agoraphobia, social phobia, specific phobia and generalized anxiety disorder [GAD]) and substance use disorders (i.e., alcohol and drug use disorders) in both studies. The CIDI is a fully structured, lay-administered diagnostic interview, developed for use in the World Mental Health Survey Initiative [Reference Kessler and Ustün19]. This instrument has demonstrated good validity for assessing DSM-IV common mental disorders [Reference Haro, Arbabzadeh-Bouchez, Brugha, de Girolamo, Guyer and Jin20]. In NEMESIS-3, the CIDI version was slightly modified to enable both DSM-IV and DSM-5 diagnoses. Briefly, three types of changes were made in the CIDI 3.0: some less relevant questions were removed, a few referrals or skips were adjusted and some questions were added. Before omitting any question, changing any referral or skipping in the original CIDI 3.0 used in NEMESIS-2, we checked its effect on the prevalence rates within NEMESIS-2. These effects were only small and nonsignificant. A more detailed account of the changes is described elsewhere [Reference ten Have, Tuithof, van Dorsselaer, Schouten and de Graaf15]. Although the criteria for common mental disorders according to DSM-IV and DSM-5 are quite similar, the validity and reliability of our modified CIDI 3.0 to assess DSM-5 diagnoses have not been formally determined.
At baseline, a lifetime version of the CIDI assessed any prior occurrence of mental disorders. At follow-up, the CIDI assessed any occurrence of mental disorders since the baseline interview. A mental disorder developed between baseline and follow-up in those without a lifetime history of the respective disorder at baseline was considered first-incident. First incidence of a category of disorders was defined as the development of a disorder in a category (mood, anxiety or substance use disorder) between baseline and follow-up, among those who has never in their life experienced any separate disorder in that category at baseline. Following previous studies, first incidence was calculated without application of the DSM hierarchical rules [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference de Graaf, ten Have, Tuithof and van Dorsselaer13].
Determinants
Sociodemographic characteristics assessed at baseline were sex, age, education (primary or lower secondary; higher secondary; or higher vocational or university), living situation (with a partner or without), employment status (with a paid job or without), household income (lowest 25%; medium; or highest 25%) and urbanicity (rural or city). These sociodemographic characteristics were measured in the same manner in both NEMESIS studies to enable comparisons [Reference ten Have, Tuithof, van Dorsselaer, Schouten and de Graaf15, Reference de Graaf, ten Have and van Dorsselaer16].
Changes in demographics between baseline and follow-up were included in both studies. These consider changes in one direction: no longer living with a partner (through divorce or death), no longer with a paid job, a substantial decrease in household income (i.e., a substantial decrease in income of respondent or, in case of a partner, a substantial decrease in income of the partner, or a decrease in both incomes) or to move house.
Regarding mental health, the presence of another main disorder category at baseline in the past 12 months was considered. For example, for incident mood disorder, the presence of baseline anxiety or substance use disorder in the past 12 months was examined.
Statistical analyses
First, incidence rates of DSM-5 disorders among persons at risk were described using frequency tables. As the exact dates of first diagnosis were not available, we assumed this date to be half the time between baseline and follow-up for each incident case [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference de Graaf, ten Have, Tuithof and van Dorsselaer13]. The incidence per 100 person-years at risk was then calculated by dividing the number of incident cases by the number of person-years at risk and multiplying this rate by 100. The number of person-years at risk for each non-incident case was the time elapsed between baseline and follow-up.
Second, logistic regression analyses were performed to examine the association between the determinants and first incidence of categories of DSM-5 disorders, expressed in odds ratios (OR) with 95% confidence interval (95% CI). These analyses were adjusted for sex, age and time between baseline and follow-up.
Third, incidence rates of DSM-IV mental disorders (mood, anxiety and substance use) of both studies were compared among the same age range of respondents (18–64 years). An increase or decrease in incidence rate of these disorders over time was calculated using logistic regression analyses with the first incidence of a disorder as the dependent variable and study as the independent variable. Two types of models were used. The first model only adjusted for time between baseline and follow-up. The second model additionally adjusted for differences in sociodemographic characteristics at baseline between both study samples (sex, age, education, living situation, employment status, household income and urbanicity).
Logistic regression models with marginal effects were used to analyze whether changes in incidence rates significantly differed across each sociodemographic characteristic and changes therein. We estimated additive interaction effects between study and each characteristic, adjusted for time between baseline and follow-up and other sociodemographics.
Results
Description of the sample
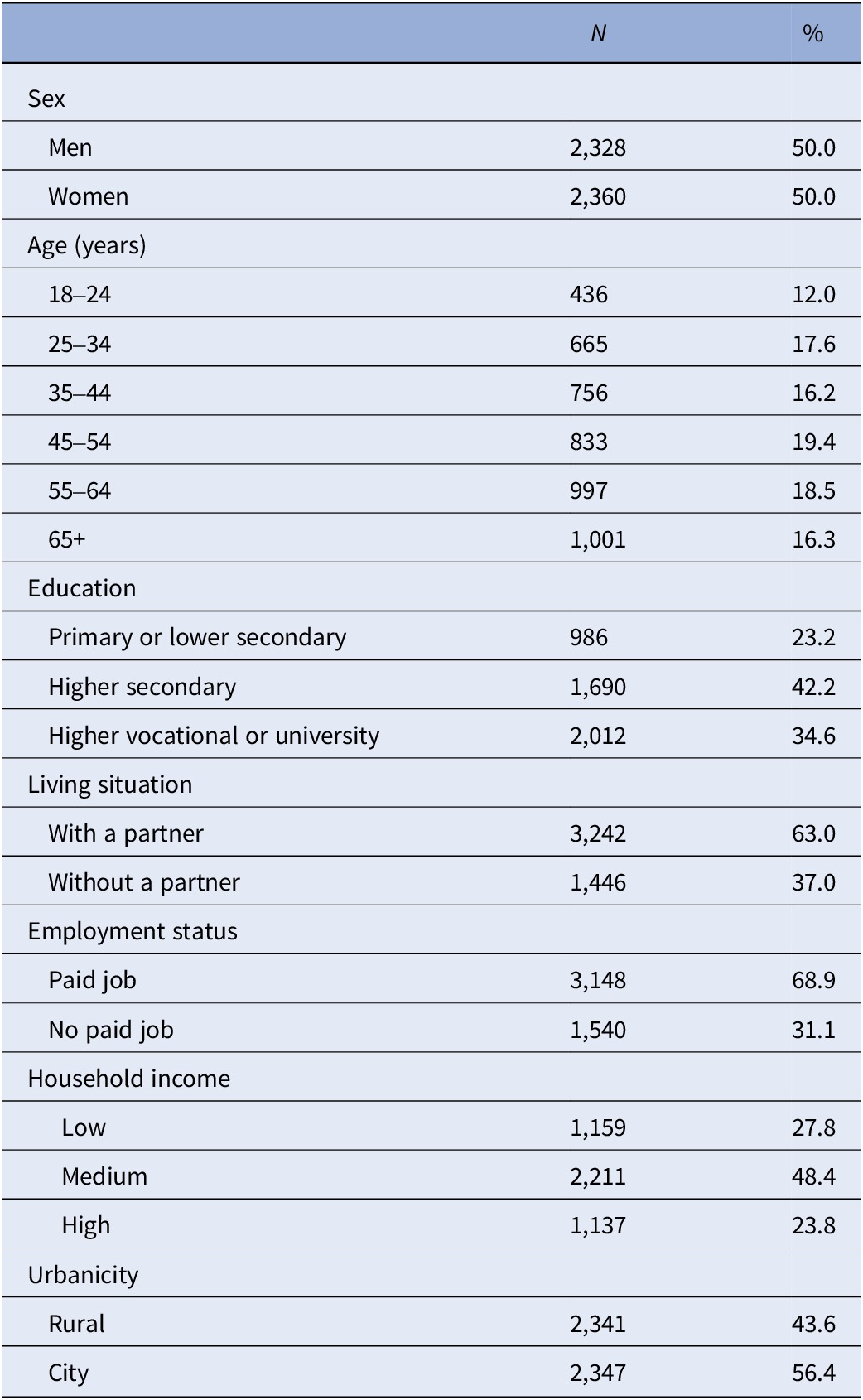
At baseline, the mean age of the sample was 46.2 years (standard error: 0.32). The sample included 50.0% women, 42.2% with higher secondary education, 63.0% living with a partner, 68.9% with a paid job and 56.4% living in the city (Table 1).
Baseline descriptives of the NEMESIS-3 sample of people aged 18–75 years at baseline, participating in both waves (n = 4,688)a

a In unweighted numbers and weighted percentages.
Incidence of DSM-5 disorders
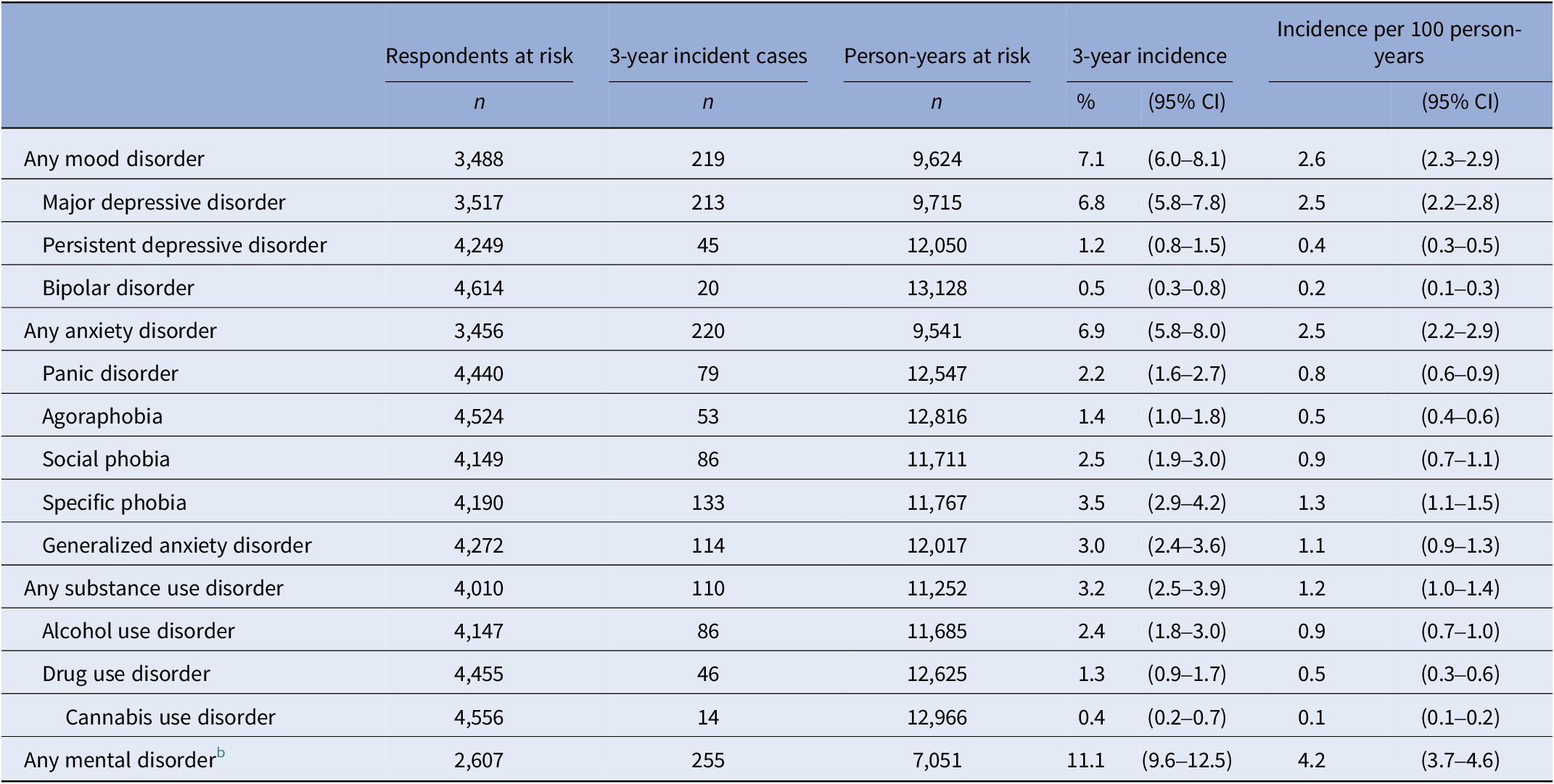
Of the people who never had a common mental disorder at baseline, 11.1% developed a DSM-5 mood, anxiety or substance use disorder in the 3-year period between baseline and follow-up (Table 2). This corresponds to an incidence rate of 4.2 cases per 100 person-years at risk.
Three-year incidence rate and incidence per 100 person-years of DSM-5 mental disorders in the general population, aged 18–75 years at baseline, based on NEMESIS-3 (n = 4,688)a

a In unweighted numbers and weighted incidence rates and incidence per 100 person-years with 95% confidence intervals (95% CIs).
b Any mental disorder included any mood disorder, any anxiety disorder and/or any substance use disorder.
Of the main disorder categories, incidence was similar for any mood disorder (7.1%) and any anxiety disorder (6.9%), but lower for any substance use disorder (3.2%). Of the separate disorders, the highest incidence rates were observed for major depressive disorder (6.8%), specific phobia (3.5%), generalized anxiety disorder (3.0%), social phobia (2.5%) and alcohol use disorder (2.4%).
Determinants of the incidence of DSM-5 disorders
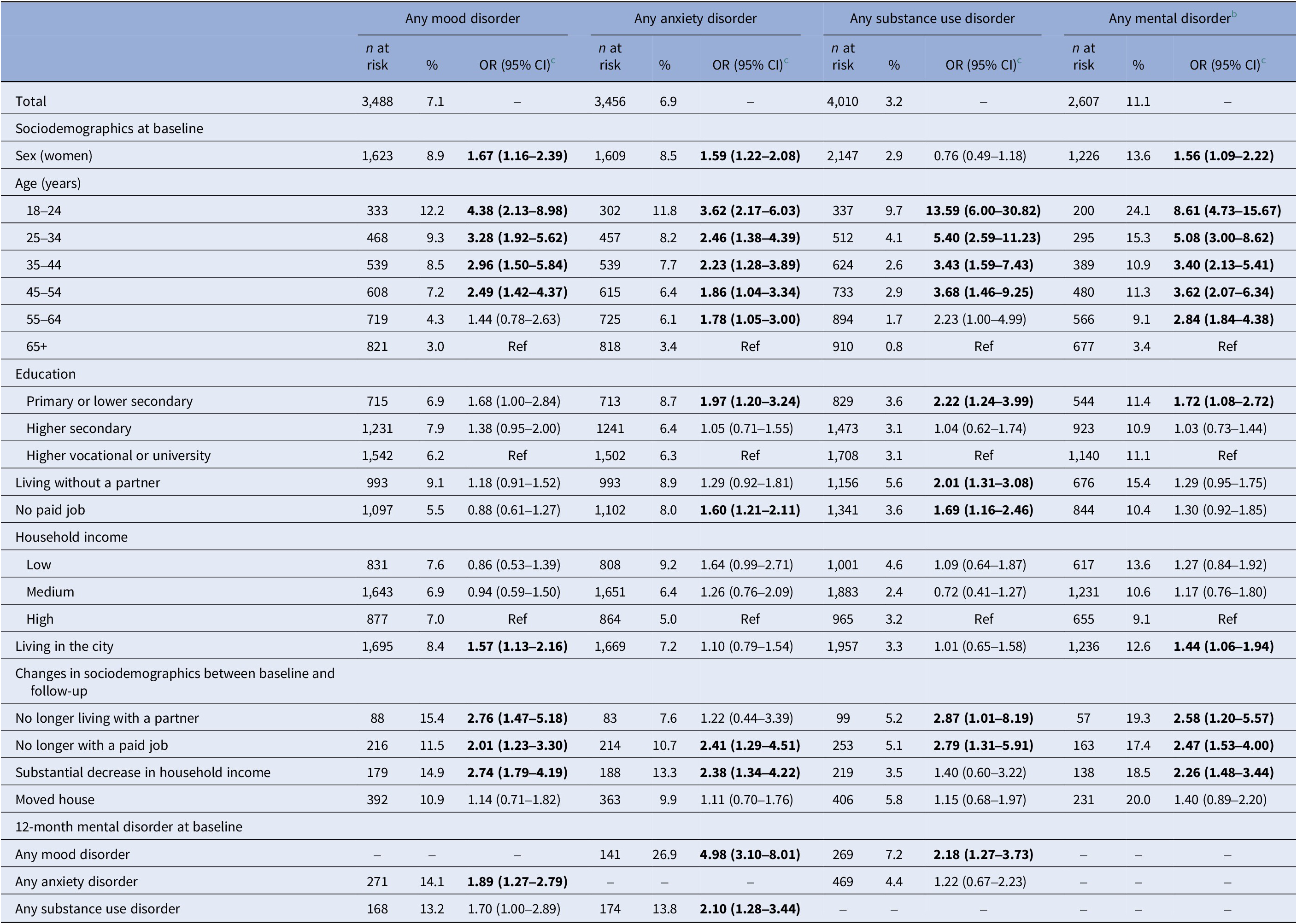
Women were more likely to develop any mental disorder than men (13.6% vs. 8.8%). While the incidence of mood and anxiety disorders was higher in women, no difference in sex was observed in substance use disorders (Table 3). Lower age was associated with a higher incidence of all disorder categories. For example, 24.1% of those aged 18–24 years at baseline developed any mental disorder versus 3.4% of those aged 65 years and older. Respondents living without a partner more often developed a substance use disorder than those living with a partner (5.6% vs. 1.9%). Compared to having a paid job, having no paid job was associated with a higher incidence of anxiety (8.0% vs. 6.5%) and substance use disorders (3.6% vs. 3.0%).
Determinants of 3-year incidence of DSM-5 mental disorders in the general population, aged 18–75 years at baseline, based on NEMESIS-3 (n = 4,688)a

Significant values (<0.05) are highlighted in bold.
a In unweighted numbers at risk and weighted percentages and odds ratios (OR) with 95% confidence intervals (95% CIs).
b Any mental disorder included any mood disorder, any anxiety disorder and/or any substance use disorder.
c Adjusted for sex, age and time between baseline and follow-up.
All changes in sociodemographic characteristics were associated with a higher incidence of most disorder categories, except for having moved house (Table 3). Compared to those who remained living with a partner, those no longer living with a partner had a higher incidence of any disorder (19.3% vs. 8.7%). Those who no longer had a paid job also had a higher incidence of any disorder as compared to those who kept a paid job (17.4% vs. 10.8%), and those with a strong decrease in household income had a higher incidence compared to those without such a decrease (18.5% vs. 10.6%).
Also, having a mental disorder before baseline was associated with having an increased incidence of another mental disorder (Table 3). For example, having an anxiety disorder in the 12 months before baseline was associated with a higher incidence of a mood disorder (14.1% vs. 6.4% for those without a 12-month anxiety disorder at baseline). A current mood or substance use disorder at baseline was associated with a higher incidence of anxiety disorder (respectively 26.9% vs. 5.9 and 13.8% vs. 6.5%). Baseline mood disorder was also associated with a higher incidence of a substance use disorder (7.2% vs. 2.9%).
Changes in incidence rates of DSM-IV mental disorders over time
The 3-year incidence rates of any DSM-IV mood, anxiety or substance use disorder among 18- to 64-year-olds significantly and substantially increased from 8.5% in NEMESIS-2 to 14.0% in NEMESIS-3, and this change remained significant after controlling for differences in sociodemographic characteristics between the studies (Table 4). Changes were also seen for any mood disorder (from 4.9 to 8.0%), any anxiety disorder (from 5.0 to 8.1%) and any substance use disorder (from 2.5 to 4.6%).
Changes in 3-year incidence rates of DSM-IV disorders in the general population, aged 18–64 years at baseline, based on NEMESIS-2 (N = 5,303) and NEMESIS-3 (N = 3,687)a, b

Significant values (<0.05) are highlighted in bold.
a Weighted percentages and odds ratios (OR) with 95% confidence intervals (95% CIs).
b NEMESIS-2: waves in 2007–2009 and 2010–2012; NEMESIS-3: waves in 2019–2022 and 2023–2024.
c Adjusted for time between baseline and follow-up.
d Adjusted for time between baseline and follow-up and sociodemographic differences (sex, age, education, living situation, employment status, household income and urbanicity) between respondents of both NEMESIS studies.
e Any mental disorder included any mood disorder, any anxiety disorder and/or any substance use disorder.
Changes in sociodemographic correlates of incidence of DSM-IV mental disorders over time
A significantly stronger increase in the incidence of any DSM-IV disorder in the period between the two studies was found for those living in a city compared to nonurban residents (p = 0.026) and those who lost their paid job compared to those who kept a paid job (p = 0.034). No significant interaction effects were found for other sociodemographics or changes therein between the baseline and follow-up wave.
Sensitivity analyses
The 3-year incidence rate of any DSM-5 mental disorder did not differ significantly between respondents interviewed at baseline before or during the pandemic (10.7% pre-pandemic vs. 11.2% during the pandemic), also after controlling for differences in sociodemographic characteristics of the respondents interviewed in these periods (Supplementary Table). This was true for all main disorder categories.
Discussion
With prospective data from a representative sample of the general population, we showed that the first onset of mental disorders is not a rare phenomenon. More than 1 in 10 (11.1%) of those who never had a common mental disorder in their life developed a first incidence of a DSM-5 mood, anxiety or substance use disorder over 3 years in this population-based sample, aged 18–75 years. Women, younger adults and people with primary or lower secondary education, or those living in the city, had a higher incidence rate of any mental disorder. When comparing the incidence of any DSM-IV common mental disorder between NEMESIS-2 and NEMESIS-3, the incidence rate substantially increased over this 12-year period, from 8.5 to 14.0% among adults aged 18–64 years. An even stronger increase was found for those living in the city and for those who had lost their job (vs. those who kept their job).
We can only compare the incidence rates of this recent study with much older samples from other countries. This comparison shows that the incidence rates per 100 person-years for depression and anxiety disorders in this sample from the Netherlands are higher than those reported more than a decade ago in the United States and Finland [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference Lehtinen, Sohlman, Nummelin, Salomaa, Ayuso-Mateos and Dowrick14]. To allow comparison with previous estimations of international studies for substance use disorders, we performed post-hoc analyses to obtain DSM-IV incidence rates among 18- to 75-year-olds for substance use disorders. Although the incidence of DSM-IV substance use disorders used to be much lower in the Netherlands compared to the United States [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference de Graaf, ten Have, Tuithof and van Dorsselaer13], we now see a mixed picture: the incidence rate of alcohol use disorder is (still) lower (i.e., 1.13 per 100 person-years), while that of drug use disorder is higher (i.e., 0.55 per 100 person-years) than previously observed in the United States [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12]. Notably, given that the rise in the prevalence of common mental disorders has been observed in multiple Western countries [Reference Grant, Chou, Saha, Pickering, Kerridge and Ruan1–Reference Slade, Vescovi, Chapman, Teesson, Arya and Pirkis7] and that the Netherlands is mostly in the average range when compared to other European countries regarding other aspects, such as environmental or socioeconomic factors, and availability of mental health care [Reference Lopez-Morinigo, Fiorillo, Dom and Arango21, Reference Arango, Fiorillo, Dom and Lopez-Morinigo22], it is likely that the current observed increase in first incidence has occurred in other countries as well. However, this remains to be investigated.
Compared to 12 years ago, a substantial increase in the incidence was observed for all three main categories of DSM-IV disorders, using similar research methods. That is, these are highly comparable samples randomly drawn from the general population in which structured diagnostic interviews were administered. Similar to the previously observed increase in prevalence between the NEMESIS studies, the rise in incidence between these studies cannot be attributed to the COVID-19 pandemic, changes in study methods (i.e., introduction of video calling in NEMESIS-3) or shifts in the population structure [Reference ten Have, Tuithof, van Dorsselaer, Schouten, Luik and de Graaf8]. Furthermore, this increase cannot be attributed to the small differences in the clinical assessment instrument used in NEMESIS-3 and NEMESIS-2, as in both studies, the DSM-IV diagnoses were based on the same questions and algorithms. Other research found no support for the hypothesis that improved attitudes toward mental illness and reduction of stigma explain the rise in mental health problems [Reference Gagné, Henderson and McMunn23]. Therefore, the current findings indicate that the observed rise in the prevalence of common mental disorders may, at least in part, reflect a genuine rise in their incidence. This stresses the need to implement public health strategies to prevent new cases.
Knowledge on determinants of disorder incidence may help to target prevention to vulnerable subgroups. Comparison of the determinants associated with a higher 3-year incidence rate of DSM-5 common mental disorders in NEMESIS-3 to those observed in two previous studies that examined incidence rates of DSM-IV mental disorders reveals a mixed picture. For some sociodemographics, the associations were broadly similar [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference de Graaf, ten Have, Tuithof and van Dorsselaer13]: sex (being a woman for any mood and any anxiety disorder), lower age and living alone (for substance use disorder). An equal number of associations with demographics now observed in NEMESIS-3 were not previously found: low educational level (for anxiety and substance use disorders) [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference de Graaf, ten Have, Tuithof and van Dorsselaer13], having no paid job (for anxiety and substance use disorders) [Reference de Graaf, ten Have, Tuithof and van Dorsselaer13] and living in the city (for mood disorder) [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference de Graaf, ten Have, Tuithof and van Dorsselaer13] were now also associated with higher incidence rates. Additionally, as in those previous studies, changes in sociodemographics [Reference de Graaf, ten Have, Tuithof and van Dorsselaer13] and a 12-month mood, anxiety or substance use disorder at baseline [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference de Graaf, ten Have, Tuithof and van Dorsselaer13] were clearly associated with higher incidence DSM-5 rates in the present study.
Notably, the high incidence rate among young adults (i.e., one in four 18- to 24-year-olds developed any mental disorder) indicates the need for prevention at an early age, for example, with school- and student-based interventions. These allow targeting mental health issues at an early age, and such interventions have been found (cost-)effective [Reference Khanh-Dao Le, Cuevas Esturas, Mihalopoulos, Chiotelis, Bucholc and Chatterton24, Reference Harrer, Adam, Baumeister, Cuijpers, Karyotaki and Auerbach25]. The high incidence rates of disorders in those with another mental disorder at baseline highlight the importance of preventive strategies in clinical practice. In the Netherlands, this is relevant for both general health care (GHC) and mental health care (MHC). The General Practitioner (GP) serves as the gatekeeper to MHC services, and over the past decade, the treatment of mental disorders within GHC has been strengthened through the introduction of the general practice mental health practitioner, who supports GPs in the care for patients with common mental health problems [Reference Nuyen, van Dorsselaer, Tuithof, Luik, Kroon and ten Have26]. Early monitoring of emerging symptoms in both GHC and MHC could help prevent the development of secondary disorders. This is important because such a development is not only clinically challenging – because it complicates diagnosis and treatment planning – but also costly, as it often leads to longer treatment durations, higher relapse rates and increased use of specialized services.
Understanding the substantial increase in incidence rate now compared to 12 years ago is complex. Design-related factors are unlikely to account for this rise. Societal changes, such as individualization of society [Reference Santos, Varnum and Grossmann27] or global challenges [Reference Cosh, Ryan, Fallander, Robinson, Tognela and Tully28], may offer explanations, but the present study was not designed to examine these. However, some insight was gained by investigating whether the strength of the association between sociodemographic risk factors and incidence of mental disorders changed between the two study periods. First, people living in the city had a stronger increase in the incidence of any mental disorder over the past decade than those living in rural areas. This is in line with the previously observed stronger increase in the prevalence of mental disorders among those living in the city [Reference ten Have, Tuithof, van Dorsselaer, Schouten, Luik and de Graaf8]. Possibly, living in the city is associated with more disadvantages today than before. A stronger increase in incidence was also observed in those who lost their paid job between baseline and follow-up, compared to those who kept their job. As it is not clear what came first, job loss or first incidence of a mental disorder, this finding is difficult to interpret. Job loss can be a stressful life event that may have preceded the disorder [Reference Flint, Bartley, Shelton and Sacker29, Reference Butterworth, Leach, Pirkis and Kelaher30], but it could also have been the result of the newly risen disorder [Reference Wichers, Maes, Jacobs, Derom, Thiery and Kendler31–Reference Olesen, Butterworth, Leach, Kelaher and Pirkis33]. Notably, the NEMESIS-2 study was performed during the economic crisis when loss of work was more common than in recent years when unemployment rates are at a historical low [34] and thus less the norm. Possibly, this could explain why the impact of job loss on incidence rates was found to be stronger in NEMESIS-3 than in NEMESIS-2. Of note, whereas previous research observed that younger adults had a stronger increase in the prevalence of mental disorders in the general population [Reference ten Have, Tuithof, van Dorsselaer, Schouten, Luik and de Graaf8] and in registered incidence of these disorders in general and mental health care [Reference Momen, Beck, Lousdal, Agerbo, McGrath and Pedersen9–Reference Walrave, Beerten, Mamouris, Coteur, Van Nuland and Van Pottelbergh11], the present findings suggest that this is not due to a stronger increase in incidence rates in the general population as no age differences were found. Perhaps, younger individuals experience a more chronic course of the disorders these days, which subsequently leads to a greater need for care. Additional research is needed to better understand this.
This study has several strengths. With prospective data from a sample representative of the Dutch population, we assessed the first incidence of DSM-5 common mental disorders with a structured diagnostic interview. Differences between incidence rates now and 12 years ago were examined with two highly comparable samples randomly drawn from the general population. Also, a wide range of determinants was considered, improving our ability to interpret the observed rise in incidence rates.
Some limitations of the study should be mentioned. First, while the CIDI 3.0 assesses DSM-IV mood, anxiety and substance use disorders with generally good validity [Reference Haro, Arbabzadeh-Bouchez, Brugha, de Girolamo, Guyer and Jin20], the validity and reliability of our slightly modified CIDI 3.0 to assess DSM-5 diagnoses have not been formally investigated [Reference ten Have, Tuithof, van Dorsselaer, Schouten and de Graaf15]. Second, our incidence rates are based on lifetime disorders at baseline and 3-year disorders at follow-up. Especially, the validity of lifetime disorders can be biased because of retrospective recall, resulting in underreporting [Reference Moffitt, Caspi, Taylor, Kokaua, Milne and Polanczyk35]. The presented incidence rates could therefore be somewhat overestimated [Reference Chou, Mackenzie, Liang and Sareen36]. As this bias is similar in both NEMESIS studies, the observed changes over time are unlikely to be affected. Third, this study determined 3-year incidence rates with two waves and, therefore, has no exact moment of onset. For each incident case, the number of person-years at risk was assumed to be half the time between baseline and follow-up. Although it is unclear to what extent this assumption is valid, it does correspond with what has been done in previous research [Reference Grant, Goldstein, Chou, Huang, Stinson and Dawson12, Reference de Graaf, ten Have, Tuithof and van Dorsselaer13] and, therefore, makes a comparison between the studies possible. Fourth, survey nonresponse and attrition could lead to bias in incidence estimates: in line with an international trend toward declining response rates in all types of surveys [Reference de Leeuw, Hox and Luiten37], the nonresponse and attrition rates in NEMESIS-3 were larger than in NEMESIS-2. Because the data were weighted for nonresponse and attrition, we assume that this had a limited effect on the incidence rates and risk associations reported here. Fifth, although the sample was representative of the Dutch population on most parameters, those with insufficient mastery of Dutch, those with no permanent residential address and those who were long-term institutionalized were excluded from participation.
To conclude, the present study shows a substantial rise in the first incidence of common mental disorders. This implicates a need for enhanced prevention programs and preventive measures aimed at reducing the incidence rates and thus the burden of mental disorders for the individual and society as a whole. These activities should be focused on those with higher DSM-5 incidence rates, that is younger people, those with primary or lower secondary education and those experiencing negative changes in sociodemographics, such as loss of a partner or a substantial decrease in household income. Also, those living in the city and those who lost their job seem to have become more vulnerable over the past decade, possibly due to a heightened sensitivity to broader societal developments. Lastly, the elevated risk of secondary disorders underscores the importance of monitoring emerging symptoms of other disorders in clinical practice to reduce the likelihood of psychiatric comorbidity.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1192/j.eurpsy.2026.10161.
Data availability statement
The data on which this manuscript is based are not publicly available. However, data from NEMESIS are available upon request. The Dutch Ministry of Health financed the data, and the agreement is that these data can be used freely under certain restrictions and always under the supervision of the Principal Investigator (PI) of the study. Thus, some access restrictions do apply to the data. The PI of the study is the last author of this article and can at all times be contacted to request data. At any time, researchers can contact the PI of NEMESIS and submit a research plan, describing its background, research questions, variables to be used in the analyses and an outline of the analyses. If a request for data sharing is approved, a written agreement will be signed stating that the data will only be used for addressing the agreed research questions described and not for other purposes.
Acknowledgments
The authors declare none.
Financial support
The third Netherlands Mental Health Survey and Incidence Study (NEMESIS-3) was conducted by the Netherlands Institute of Mental Health and Addiction (Trimbos Institute) in Utrecht. Financial support has been received from the Ministry of Health, Welfare and Sport. The funding source had no further role in study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Competing interests
The authors declare none.




 Open access
Open access
Comments
No Comments have been published for this article.